Embed Size (px)
Citation preview
headacheheadache
Headache is one of the commonest Headache is one of the commonest neurological complain reported at neurology neurological complain reported at neurology clinicclinic
path physiologypath physiology
Intracranial pain sensitive structures includeIntracranial pain sensitive structures include: the : the arteries of the circules of willis &the first few arteries of the circules of willis &the first few centimeters of their median sized branchescentimeters of their median sized branches
Meningeal arteriesMeningeal arteries
Large veins &dural venous sinusesLarge veins &dural venous sinuses
Extra cranial sensitive structures: Extra cranial sensitive structures: external carotid arteires, scalp ,neck external carotid arteires, scalp ,neck muscle ,skin & cutaneous nerves, cervical nerve muscle ,skin & cutaneous nerves, cervical nerve &nerve roots, mucosa of the sinus &teeth ..&nerve roots, mucosa of the sinus &teeth ..
Case historyCase history
25 y old f with h/o : ER h/o sever 25 y old f with h/o : ER h/o sever headache ,diffuse ,dull in nature ,not relived by headache ,diffuse ,dull in nature ,not relived by analgesia,aggrevated by analgesia,aggrevated by cough ,sneezing.cough ,sneezing.
Assosiated with vomitingAssosiated with vomiting No other neurological symptoms.No other neurological symptoms. She gave h/o of chronic infrequent She gave h/o of chronic infrequent
headache ,which tension type and less sever, headache ,which tension type and less sever, relieved by analgesiarelieved by analgesia
She is singleShe is single Recently She was following with dermatology Recently She was following with dermatology
doctor and he gave her tablets for facial peelingdoctor and he gave her tablets for facial peeling
O/EO/E
Neurological exam :Neurological exam : HF:NHF:N Speech :normalSpeech :normal Cranial nerves: Cranial nerves: fundoscopic fundoscopic
exam:papilledemaexam:papilledema Motor, sensory, coordination :normal Motor, sensory, coordination :normal

Is this headache serious?Is this headache serious?
headacheheadache
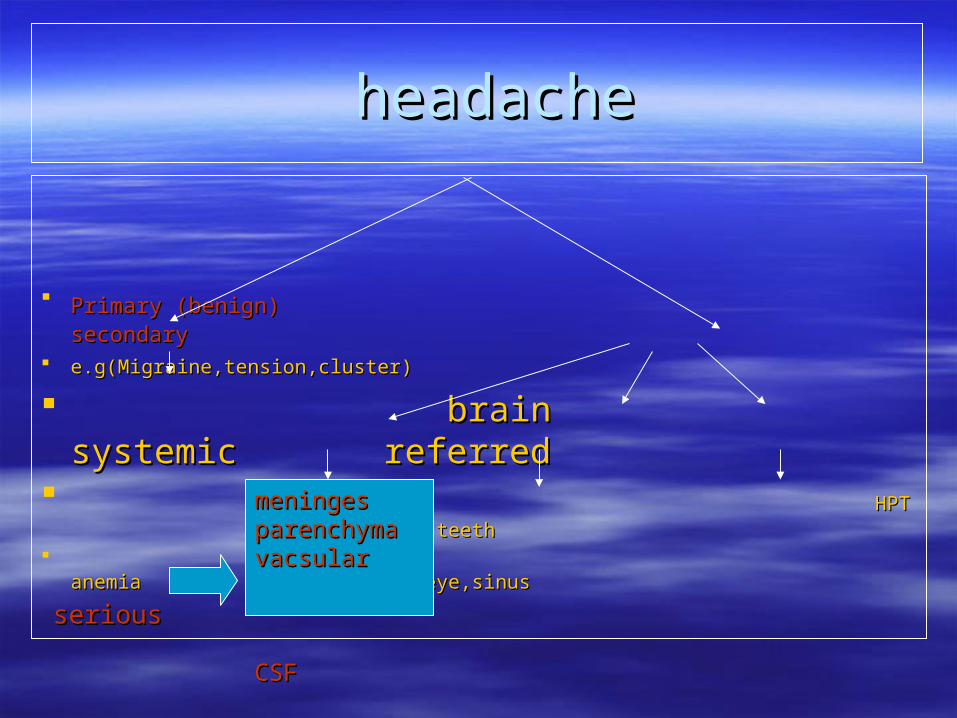
Primary (benign)Primary (benign) secondary secondary e.g(Migraine,tension,cluster) e.g(Migraine,tension,cluster)
brain systemic referred brain systemic referred HPT ear,teethHPT ear,teeth
anemia eye,sinusanemia eye,sinus
serious serious
meningesmeninges parenchyma parenchyma vacsular vacsular CSFCSF
Secondary causes (serious) Secondary causes (serious)
Structural causesStructural causes MeningesMeninges: meningitis: meningitis parenchyma parenchyma : encephalitis ,abscess, tumor: encephalitis ,abscess, tumor VascularVascular: hemorrhage, venous thrombosis, : hemorrhage, venous thrombosis,
giant cell arteritiesgiant cell arterities CsfCsf: increase CSF pressure : increase CSF pressure
(hydrocephalus ,pseudotumor (hydrocephalus ,pseudotumor cerebri) ,decrease CSF pressure…leak cerebri) ,decrease CSF pressure…leak
Careful history and examination should be Careful history and examination should be done to differentiate between benign and done to differentiate between benign and serious headacheserious headache

Age Age
Migraine headacheMigraine headache: child hood or early : child hood or early adulthoodadulthood
Giant cell arteritis:Giant cell arteritis: >50 y >50 y
New onset headache in elderly should be New onset headache in elderly should be always a concernalways a concern
Onset Onset
Headache of many years duration &with Headache of many years duration &with little changes is almost always of benign little changes is almost always of benign origin origin
New onset headache in old age or New onset headache in old age or increasingly sever headache ….increasingly sever headache ….seriousserious headache..headache..
Hyperacute : SAHHyperacute : SAH
periodicity: periodicity:
episodic headache is benignepisodic headache is benign Migraine ,Cluster headache Migraine ,Cluster headache
a daily constant headache ..tension typea daily constant headache ..tension type
durationduration
Migraine: 4-72 hMigraine: 4-72 h Cluster:1/2-2hCluster:1/2-2h Tension headache :build up over hours lasts Tension headache :build up over hours lasts
days to yearsdays to years
Location Location
unilateral headache:migraine,cluster,temporal unilateral headache:migraine,cluster,temporal arterities . arterities .
TensionTension headache : generalized ,frontal or headache : generalized ,frontal or posterior cervical regionposterior cervical region
Carotid dissection commonly present with Carotid dissection commonly present with neck,face,and head pain usually ipsilateral to the neck,face,and head pain usually ipsilateral to the dissection dissection
Local pain :superfacial structuresLocal pain :superfacial structures
Nature Nature
Nature: Nature: throbbing: vascular throbbing: vascular Tension :fullness, tightness, pressure like Tension :fullness, tightness, pressure like
aura,& associated symptomsaura,& associated symptoms
migrainemigraine: : aura;aura; focal cerebral symptoms focal cerebral symptoms associated with lasts from 20-30 min, precedes associated with lasts from 20-30 min, precedes the headachethe headache
Sensory, motor,autonomic,..Sensory, motor,autonomic,.. ClusterCluster headache: ptosis,lacrimation, conjuctival , headache: ptosis,lacrimation, conjuctival ,
nasal congestionnasal congestion Headcahe +fever …..infectionHeadcahe +fever …..infection Transient visual obscuration, diplopia,tinnitus …Transient visual obscuration, diplopia,tinnitus …
increase intracranial pressureincrease intracranial pressure
aura,& associated symptomsaura,& associated symptoms
Jaw clawdication: temporal arteritisJaw clawdication: temporal arteritis
Headache: progressive+ central nervous Headache: progressive+ central nervous symptoms is suggestive …structural brain symptoms is suggestive …structural brain lesion lesion
Aggravating & relievingAggravating & relieving
AggravatingAggravating Cough, straining……intracranial pressure Cough, straining……intracranial pressure Activity., stress…..migraine, tension typeActivity., stress…..migraine, tension type Sitting: CSF hypotensionSitting: CSF hypotension Relieving:Relieving: Rest…….migraine,tension Rest…….migraine,tension
Drug historyDrug history
Oral contraceptive… Cerebral vein Oral contraceptive… Cerebral vein thrombosis, migraine thrombosis, migraine
Steroid withdrawal pseudotumor cerebriSteroid withdrawal pseudotumor cerebri Retin A tablets Retin A tablets
Warfarin : HgeWarfarin : Hge
Postpartum : cerebral venous thrombosisPostpartum : cerebral venous thrombosis
Recurrent abortionRecurrent abortion
FHFH
migrainemigraine
examexam
v/s: v/s: fever ,BPfever ,BP General: General: sinus tendernesssinus tenderness Eye ,throat ,ear examEye ,throat ,ear exam
examexam
Normal examNormal exam: benign headache: benign headache
PapilledemaPapilledema: increased intracranial pressure: increased intracranial pressure
Focal neurological findingFocal neurological finding……serious……serious
Complicated migraineComplicated migraine….neurological signs….neurological signs
Horner syndromeHorner syndrome: cluster headache: cluster headache
Scalp tenderness,Scalp tenderness, pulslesspulsless: temporal arteritis: temporal arteritis
Is this headache serious?Is this headache serious? Characteristics of headache with serious underlying pathology Characteristics of headache with serious underlying pathology History :History : Explosive onset and severe at onsetExplosive onset and severe at onset No similar headaches in the pastNo similar headaches in the past you have a constant headache, which is gradually getting worse;you have a constant headache, which is gradually getting worse; Altered mental statusAltered mental status Age over 50Age over 50 ImmunosuppressionImmunosuppression
Physical examination :Physical examination : Neurologic abnormalities Neurologic abnormalities Decreased level of consciousnessDecreased level of consciousness MeningismusMeningismus PapilledemaPapilledema
Work upWork up
If history and exam is suggestive of serious If history and exam is suggestive of serious headacheheadache
Brain image: CT brain, mri brainBrain image: CT brain, mri brain
If suspect cerebral vein throbosis..CT If suspect cerebral vein throbosis..CT venogram ,MRVvenogram ,MRV
if fever or ? SAH …LPif fever or ? SAH …LP
Go back to the caseGo back to the case
Case historyCase history
25 y old f with h/o : ER h/o sever 25 y old f with h/o : ER h/o sever headache ,diffuse ,dull in nature ,not relived by headache ,diffuse ,dull in nature ,not relived by analgesia,aggrevated by analgesia,aggrevated by cough ,sneezing.cough ,sneezing.
Assosiated with vomitingAssosiated with vomiting No other neurological symptoms.No other neurological symptoms. She gave h/o of chronic infrequent She gave h/o of chronic infrequent
headache ,which tension type and less sever, headache ,which tension type and less sever, relieved by analgesiarelieved by analgesia
She is singleShe is single Recently She was following with dermatology Recently She was following with dermatology
doctor and he gave her tablets for facial peelingdoctor and he gave her tablets for facial peeling
O/EO/E
Neurological exam :Neurological exam : HF:NHF:N Speech :normalSpeech :normal Cranial nerves: Cranial nerves: fundoscopic fundoscopic
exam:papilledemaexam:papilledema Motor, sensory, coordination :normal Motor, sensory, coordination :normal
Work upWork up
CT brain : normalCT brain : normal MRI brain:NMRI brain:N MRV: NMRV: N LP: increased CSF pressure, protein, LP: increased CSF pressure, protein,
glu,cell count were normalglu,cell count were normal
Pseudo tumor cerebriPseudo tumor cerebri ( Idiopathic Intracranial Hypertension )( Idiopathic Intracranial Hypertension )
Home message Home message
Careful history and exam including Careful history and exam including (opthalmoscopic) exam is the key to (opthalmoscopic) exam is the key to differentiate benign from serious headache.differentiate benign from serious headache.