Embed Size (px)
Citation preview
DOI: 10.1051/odfen/2014006 J Dentofacial Anom Orthod 2014;17:304� RODF / EDP Sciences
1
Article received: 16-12-2013.Accepted for publication: 12-02-2014.
Healing processes following toothextraction in orthodontic cases
N. Cohen1, J. Cohen-Levy2
1 DDS, PhD University Lecturer, Paris 7 University, Private Practice at 10 rue Margueritte,
75017 Paris
2 DDS, PhD Former University Hospital Dental Assistant of the Hospitals of Paris,
Private Practice at 255 rue Saint-Honore, 75001 Paris
ABSTRACT
This article reviews the normal and pathological healing processes that takeplace after tooth extraction in orthodontic cases, and their associatedcomplications within the mucosa or alveolar socket, such as gingival clefts orbone defects. The general and local factors that are involved in such deficienthealing cases are detailed, in parallel to surgical procedure to enhance ridgepreservation or to ‘regenerate’ tissues. The relationships between theorthodontist and periodontist are underlined, because both praticioners assesspatient’s risk factors and follow him during this treatment stage.
KEY WORDS
Dental extraction, atraumatic extraction, healing, alveolar socket, bone regenerationtechniques, graft
INTRODUCTION
Extraction is a procedure that is currentlyperformed in orthodontics, either in thecontext of early treatment (serial extrac-tions, germectomies), for adolescents withsevere crowding or protrusion/overjet, orfor adult patients who have fewer possibili-ties for expanding the arch.
The consequences of this ‘‘simple’’ pro-cedure have not always been accuratelyassessed, whereas many mucosal and oss-eous complications may show up after theextraction: bone resorption with collapse ofthe alveolar process, a gingival cleft or
gingival recession in the area surroundingthe extraction site. Besides the potentialesthetic repercussions, these periodontaldefects also give rise to a clinical problemwith achieving some orthodontic move-ments, such as complete closure of thespace or uprighting a root.
Each individual has his own capacity toheal, that is determined by his biotype andbiological profile, consisting of cytokinesand inflammation mediators4,5,14,25,29,49,52.The various processes involved mayadditionally be altered by ageing, or by a
Address for correspondence:
Nicolas Cohen10, rue Margueritte – 75017 [email protected]
Article available at http://www.jdao-journal.org or http://dx.doi.org/10.1051/odfen/2014006

general illness. The potential for localhealing also depends on acquired fac-tors, and especially by the cause ofthe extraction (following trauma, en-dodontic lesion, periodontal lesion oron the contrary extraction of ahealthy tooth for orthodontic pur-poses).
This article provides a bibliographi-cal review on normal and pathological
post-extractional healing and on thedistinctive characteristics of extrac-tions in orthodontics, followed by apresentation of the techniques thatallow for preservation (atraumatic ex-tractions) or osteomucosal regenera-tion (grafts, biomaterials andmembranes).
POST-EXTRACTIONAL HEALING
Normal healing19
Any surgical procedure disruptstissue homeostasis. The slightestepithelial tissue breakdown is a portalof entry for micro-organisms, that arelikely to spread. The danger is de-tected by the cells present in the tis-sues that release inflammatorymediators and that organize a line ofdefense.
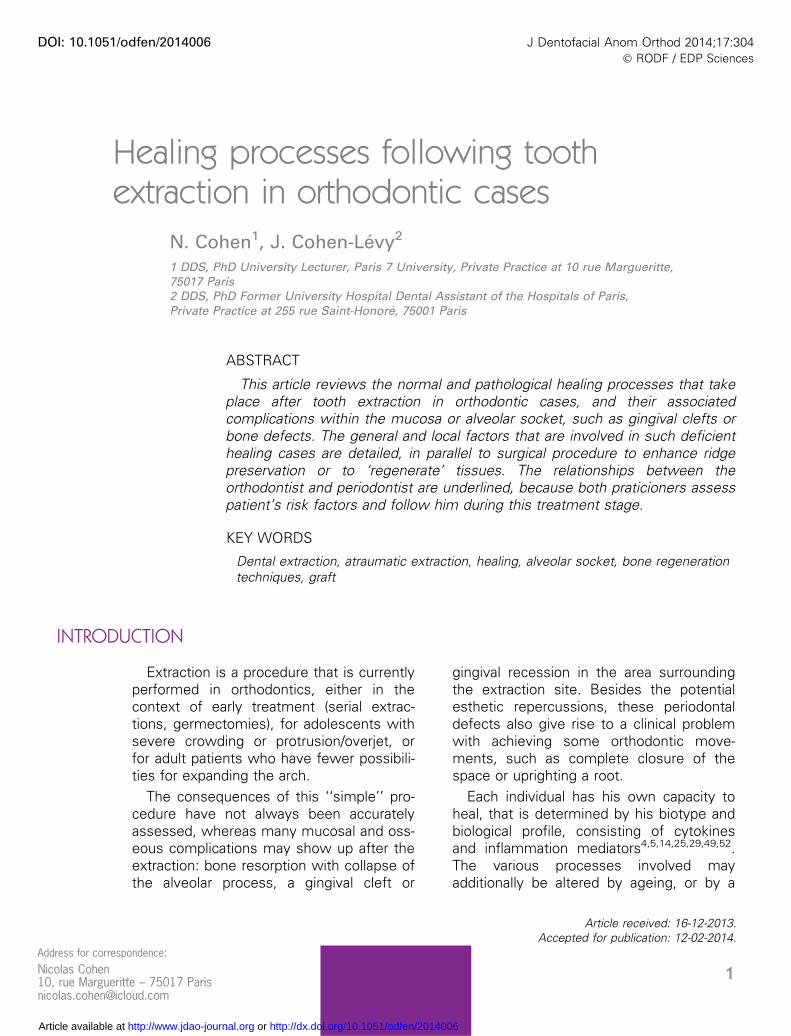
Depending on the clinical situation,there are then four possible re-sponses: a ‘‘normal’’ repair, a defec-tive healing, an excessive scarring ora regeneration. This last way of heal-ing, with ad integrum restoration ofthe mucosal and osseous volumes,can only be achieved with a period-ontal surgical intervention (Fig. 1).
Healing takes place in threestages, an inflammatory phase, aproliferative phase and a matura-
tion phase (Fig. 2). They have beenwidely described histologically butbio-molecular research has advancedour macroscopic understanding ofthe healing process.
This process is initiated as soon asblood platelets come into contactwith collagen connective tissue,
while blood fills in the empty socket.This creates a platelet aggregationthat forms a clot (erythrocytes andleukocytes embedded in a fibrin gel).The clot controls the bleeding, butalso serves as a support to the suc-cessive stages of cicatrization. Theplatelets produce growth factors andmediators (cytokines) involved inangiogenesis, the Platelet-Derived-Growth-Factor (PDGF) and the Trans-forming-Growth-Factor-beta (TGF-b).The PDGF is linked to the attractionof the neutrophils and the macro-phages, and influences the activity ofthe smooth muscles and the mito-genic properties of the fibroblasts.The TGF-b also signals the attractionof the macrophages, that stimulatesthem to secrete cytokines such asthe Fibroblast-Growth-Factor (FGH),the PDGF, the Tumor Necrosis Fac-tor-a (TNF-b), and interleukin-1 (IL-1).
The dental socket is next rapidlycolonized by granulation tissue, con-sisting of neo-vascular tissues,inflammatory cells and erythrocytes,that virtually replace the entire clotwithin a week. The next stage iscalled the provisional matrix, wherethe mesenchymal cells are organized
N. COHEN, J. COHEN-LEVY
2 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
Regeneration(identical replacement of gingival
and osseous tissues)
ExtractionNormal repair
Excessive scarring(fibrosis, hyperplasia,
cheloid)
Defective repair
(tissue loss)
Figure 1Types of post-extractional healing: normal healing, pathological and procedure-assisted techniques for regeneration.
Inflammation
CoagulumInflammationEpithelialization
NeovascularizationMatrix synthesisFormationContraction of the lesions Maturation
Proliferation
RemodelingApoptosisCollagen synthesis
Lesion 1 10 30 100
Figure 2Tissue phenomena of cicatrization over time.
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 3

into a dense network, within the col-lagen fibers and the vessels; themineralization progressively begins,that resembles the fingerlike forma-tion of immature bone within thematrix, embedded in ‘‘primaryspongy cell culture‘‘. This immaturebone is progressively remodeled intotrabecular bone and spongy bone
(trabeculae of mineralized bone, withsecondary osteons, surrounded bymedular spaces rich in vessels, adi-pocytes, mesenchymal and inflam-matory cells).
Human studies on post-extractionalhealing have demonstrated thatmineralization begins at the end ofthe first week; between the 2nd and4th week, the bony appearance ofthe clot has disappeared, with theproliferation of granulation tissue andthe provisional matrix; and between6 and 8 weeks, most of the granula-tion tissue has been replaced bythe provisional matrix (approximately60%) and with immature bone (ap-proximately 40% along the outerwalls of the alveolus). The osseousformation has not been completed24 weeks after extraction.
The dynamics of post-extractionalhealing depend on the mucous tis-sues and underlying bone tissuewhose cells do not regenerate at thesame rate. The principles of period-ontal regeneration were establishedon the basis of this principle.
The principle of guided tissueregeneration (GTR), developped byNyman in 198738, is based on theprinciple of selective recolonization ofthe detoxified radicular surfaces, bypreventing, with the help of amembrane (resorbable or not), the
invasion of the site by epithelial andconnective cells. This allows forcementogenesis when teeth are pre-sent and osteogenesis when theyare not. This osteogenesis can onlytake place if the osteoblasts havetime to form a bony network and ifosteogenesis is not inhibited by con-tact with the fibroblasts. The need to‘‘filter’’ the cells that penetrate intothe zone of regeneration must nothowever impede the expression ofthe inflammatory factors since theyare required for healing.
Mucosal healing
The epithelialization of the extractionsite is founded on the migration and di-vision of the cells of the basal stratum,starting from the areas bordering thewound. It begins within 12 hours fol-lowing surgery. The healing is distinc-tive in the buccal cavity since it is aseptic and humid site with a very highrate of regeneration. The speed of themucosal healing has therefore beencompared to that of the skin, andseems to be faster, due to certain bio-logical factors, whose production var-ies with the individual and the siteunder consideration.
Several studies, initiated by the re-search of Graves et al., on healing inmice, have shown the the IL-1 wasessential for buccal healing but notfor that of the skin21. Similarly, theexpression of the the TGF-b appearsto modulate the ability to heal in thebuccal cavity due to its chemotacticproperties16,59. Given that thesemediators are expressed differentlybased on the individual, it is concei-vable that they will be good markers
N. COHEN, J. COHEN-LEVY
4 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases

in the future for assessing the riskfor defective healing.
Since we still have no predictivetest to date for inflammatory media-tors involved in healing, cliniciansswitched to clinical and macroscopiccorrelations. The pre-surgical evalua-tion of soft tissues is especially im-portant, because the periodontaltypology provides some basis forprognosis. Today it is recognized thata fine biotype is a surgical risk factor;manipulating soft tissues poses a riskand their capacity to heal and to re-generate seem to be reduced due tothe small amount of underlying con-nective tissue.
Bone healing
In most situations, an extractioninduces bone resorption, that is al-ways more significant on the buccalside2,4,12,25,52. This resorption leadsto a reduction in vertical height of theridge53 and a lingual displacement ofits axis4,5.
However, regardless of the surgicaltechnique used, a loss of volume inthe transverse and vertical directionis evident22,49. The systematic reviewof Hammerle et al.22 calculates thehorizontal loss to be 3.8 mm and thealveolar height to be 1.24 mmsix months after extraction. A num-ber of authors have then suggestedthat we perform, in cases oftri-dimensional loss, bone regenera-tion procedures3,20,32,50,55,60, andthey describe the implementation ofmembranes to avoid collapse ofthe ridge17,43, the use of graftsof autogenous bone, allografts20,60 or
xenografts3,7,12. These studies wereconducted before implant restoration,therefore, their conclusions cannotbe extrapolated to orthodontic treat-ment today.
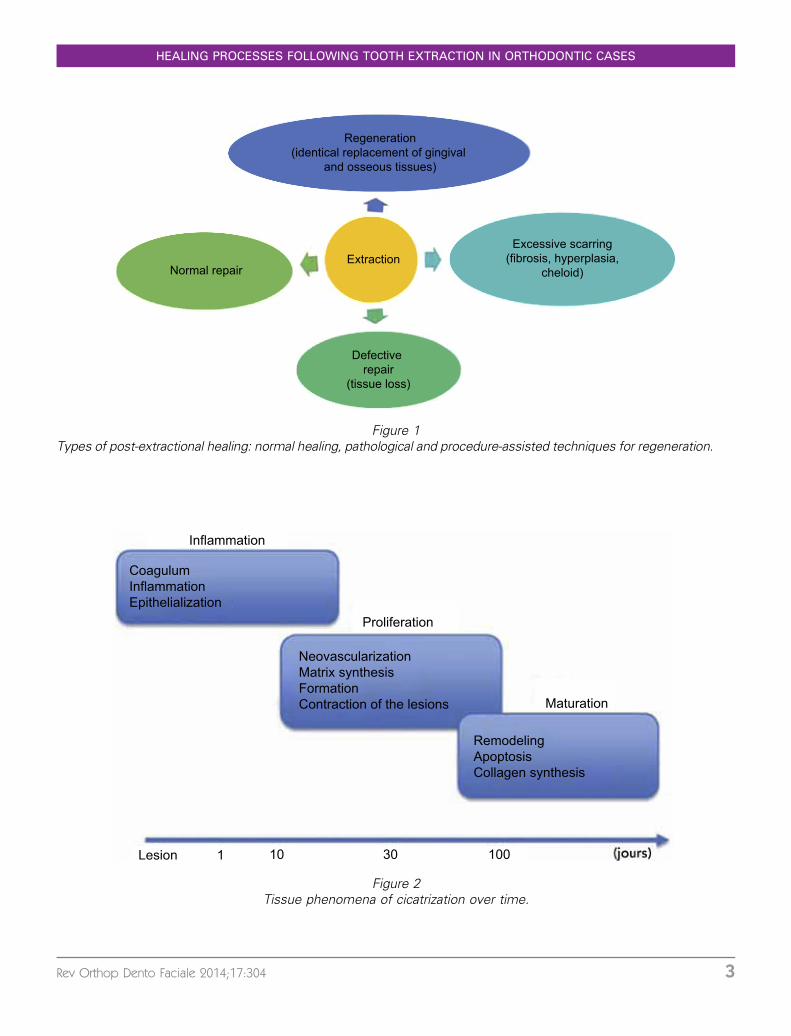
In the clinical case presented infigure 3 (a to j), the female patient,23 years of age who benefitted froman orthodontic treatment that in-volved extraction of premolars, pre-sented with a vertical fracture of apermanent first molar, that needed tobe extracted. The intraoral clinicalviews at 8 weeks post extraction(Fig. 3 a, b) and photos of the flapwhile it was trimmed (Fig. 3 c) clearlyshow the failure of the healing andthe tridimensional loss of volume, ina patient who was however young,in good health and a non-smoker.Taking into account the prolapsed si-nus and the low residual volume, wedecided on a regenerative therapy in-cluding bone substitution material(Bio-Oss�, distributed by GeistlichTM,Fig. 3 d), placement of a membrane(Fig. 3 e and f). Protecting the mem-brane against the risk of exposurewas ensured by sutures, ensuring aclosure of the gingival edges withoutexcessive traction (Fig. 3 g). The sec-tional views (cone beam computer-ized tomography CbCt) show thedefective tridimensional bone healingbefore regeneration (8 weeks afterextraction) (Fig. 3 h and i), and makesit possible to monitor the quality ofhealing (Fig. 3 h).
A systematic review conducted byVittorini et al.56 analyzed the differenttechniques of extraction and ofpreservation of the dental socket inhumans. They selected 424 scientific
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 5
Figure 3a) Occlusal view of the natural post-extractional healing of the patient after 8 weeks. b) Palatal view. c) Occlusalview after the the flap has been trimmed: lack of bone neoformation. d) Application of Bio-OssTM. e) Applicationof a membrane (Bio-GuidTM). f) Final positioning and testing of the membrane. g) Sutures. h) Post-operative conebeam reconstruction. i) Axial cut of the same day examination. j) Immediate post-operative view.
N. COHEN, J. COHEN-LEVY
6 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
articles and compared the use withthe non-use of post-extractional re-generative techniques. In every case,regeneration promoted the preserva-tion of the bone volume. It wasdifficult to compare the various tech-niques that were used, but it seemsthat the implementation of a mem-brane may increase the quality of thehealing. Manipulating the tissues(separating the flap or labial tractionof the flap) appears to limit the lossof bone volume56.
Pathological healing
Infectious complications
Infectious complications can occurwhen the formation of coagulumdoes not take place or is altered byearly fibrinolysis. They are caused bya bacterial colonization of the clot orby an inflammatory process entailinga massive migration of granulocytes.The relation between the operativetrauma and the site infection has alsobeen demonstrated and is attributedespecially to exposing the bone toolong during surgery, to drilling with-out irrigation, or to poor infectioncontrol6,23.
There can be simple, granuloma-tous and dry alveolitits, that presentwith pain two to four days after sur-gery. Another classification based onthe the duration of healing27, includesalveolar osteititis, suppurative osteiti-tis, necrotic osteititis and fibroushealing. With dry osteititis (or fibrino-lytic or dry socket), the socket ap-pears bare, with white greyish and
bloodless walls39; with suppurativealveolitis, the blood clot is disorga-nized and purulant, typically with yel-low greenish appearance. The painis intense, and must be treatedpromptly.
Women are affected by infectionssignificantly more frequently thanmen15. This has shown to be relatedto the intake of oral contraceptives27.
Additionally, the frequency of al-veolitis increases with age. They arerarely found in children, seeminglybecause there is better vasculariza-tion.
Smokers are more prone to infec-tion28,29. The operative technique andsurgical instruments used for an os-teotomy are also a factor. As a resultof the use of drills fitted with an in-ternal cooling system for osteo-tomies30, infection complicationsappear less frequently. The experi-ence of the surgeon, the use of achlorhexidine mouthwash prior to theprocedure11 might also have an im-pact on the frequency of infections.
The use of antibiotics
A recent Cochrane review evalu-ated 18 studies, with a total of 2,456participants who received antibiotics(different types and dosages) or aplacebo, immediately before or afterextraction of the wisdom teeth. Theyconcluded that there was enoughscientific evidence showing that anti-biotics administered just before and/or after a surgical procedure reducedthe risk for infection, pain and drysocket after extraction but that the
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 7
use of antibiotics also triggers moresecondary effects (generally brief andminor) in these patients34.
Complications linked to takingmedications
All the drugs that are going toalter one of the physiological phasesof healing are likely to expose patientsto some complications (inflammatoryphase and anti-inflammatory treat-ments, vascular and proliferative phaseand anti-angiogenic treatments...).
Corticosteroids for example, admi-nistered systemically and in strongdoses, delay healing. This affectis basically linked to their anti-inflam-matory action (decrease of leukocytemigration, lymphocyte inhibition, de-crease in macrophage phagocytosis,decrease in the production of antibo-dies and the appearance of antigens)and also related to the inhibiting actionon fibroblastic proliferation, collagensynthesis and epithelialization. This de-layed healing, with a more random re-generation phase, has been shown invitro and in vivo30.
Complications related to apathological condition
It is generally recognized that somepatient profiles entail difficulties withhealing. For example, patients with type2 diabetes fall into this category. Theypresent with the modifications of theexpression of certain mediators such asTGF-b that are essential for healing59.Controlling glycemia appears to be fun-damental for normal healing, becausehyperglycemia alters the leukocytefunctions, decreases phagocytosis andchemiotactism, and increases the risk
for infection. For these patients, healingcan turn out to be very unpredictable.
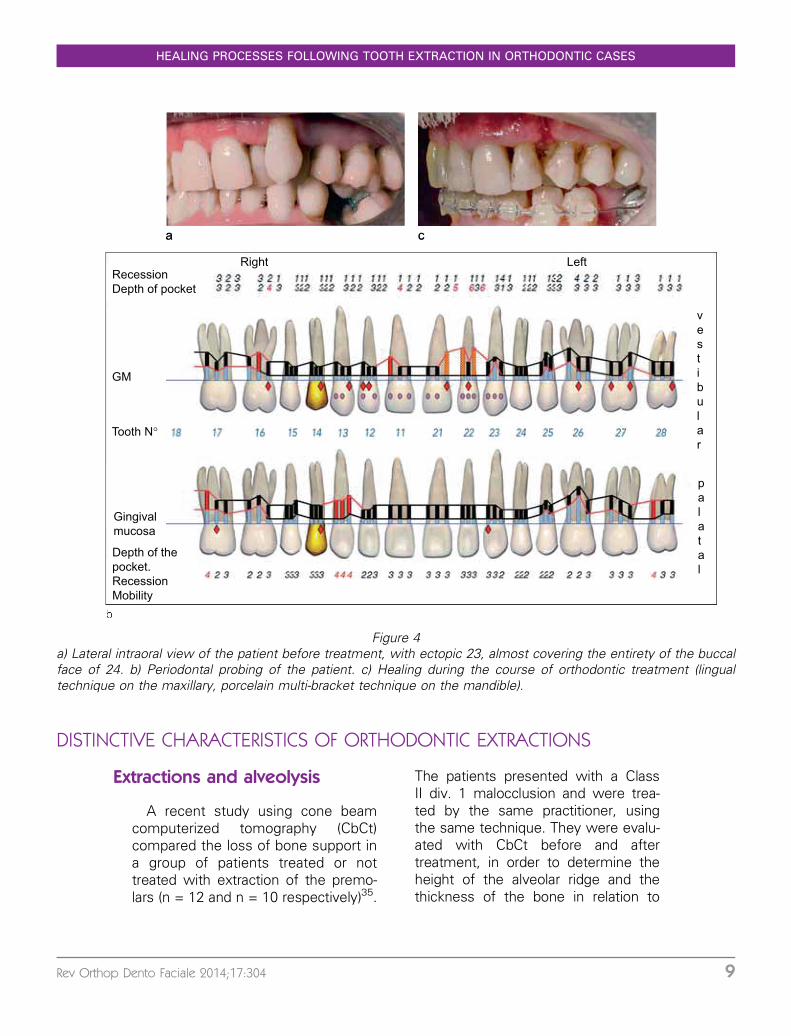
For the case shown in figure 4a,the patient, 50 years of age, presentswith type 2 diabetes, and withdifficulty in controlling plaque, withsevere maxillary crowding, 23 and 24practically overlapped each other. Hepresented with chronic adult period-ontitis with severe localized inflam-mation (Fig. 4 b). The orthodontictreatment plan chosen involved theextraction of 23, that presented withsevere buccal recession. Healingoccurred with invagination of the buc-cal mucosa, even though there wasno orthodontic movement for closingthe gap underway (Fig. 4 c.).
Patients with immuno-deficiency,whether they are infected with thehuman immuno-deficiency virus (HIV),have cancer or are taking immunosup-pressive drugs, almost always system-atically present with defective healing.With these patients, we observe achange in the quality of the inflamma-tory phase, a decrease in resistance toinfections as well as the debridementof necrotic debris.
The lack of oxygenation or perfu-sion of tissues is also one of themain factors responsible for the delayin healing. In a hypoxic environment,the deposition of collagen on the ma-trix is initially slowed then interruptedif hypoxia continues. Therefore, pa-tients who previously had oral radia-tion treatment or anti-angiogenictreatments are particularly at risk.The bone tissue when exposed toheavy doses of radiation undergoesirreversible changes with narrowingof the blood vessels, that thendecrease the flow of blood to thetissues.
N. COHEN, J. COHEN-LEVY
8 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
DISTINCTIVE CHARACTERISTICS OF ORTHODONTIC EXTRACTIONS
Extractions and alveolysis
A recent study using cone beamcomputerized tomography (CbCt)compared the loss of bone support ina group of patients treated or nottreated with extraction of the premo-lars (n = 12 and n = 10 respectively)35.
The patients presented with a ClassII div. 1 malocclusion and were trea-ted by the same practitioner, usingthe same technique. They were evalu-ated with CbCt before and aftertreatment, in order to determine theheight of the alveolar ridge and thethickness of the bone in relation to
a c
Right LeftRecessionDepth of pocket
GM
Tooth N°
vestibular
Gingivalmucosa
Depth of the pocket.RecessionMobility
palatal
Figure 4a) Lateral intraoral view of the patient before treatment, with ectopic 23, almost covering the entirety of the buccalface of 24. b) Periodontal probing of the patient. c) Healing during the course of orthodontic treatment (lingualtechnique on the maxillary, porcelain multi-bracket technique on the mandible).
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 9
the cemento-enamel junction. Theauthors found a decrease in the buc-cal-lingual alveolar dimensions in bothgroups, with no significant differencebetween them. On the other hand, thebone loss was significantly greater inthe group treated with extractions, inthe extraction site, and the distal regionon the maxillary canines showed themost variation.
Extraction and gingival clefts/fissures57
The development of a gingival clefton a site subjected to orthodonticspace closure following extraction isa fairly common occurrence. Theirfrequency has been estimated to be35%45,46. In a study carried out byRobertson et al.46, forty patients trea-ted with extraction of the premolarswere examined in order to analyzethe presence and distribution of gin-gival clefts, defined as an invagina-tion of interproximal tissues withepithelial spikes (mesial and distal) ofat least 1 mm. Fourteen of the fortypatients presented with cleft on oneor several of the premolar extractionsites, while no cleft was evident inthe premolar zones of the controlgroup of patients i. e. patients treatedwithout extractions.
Their etiology is still uncertain to-day. Some authors suggest that, forthe affected sites, the transeptal fi-bers are disorganized and not regen-erating57, since the invagination isdeveloping passively by the foldingof the gingival tissues; histologicalstudies have demonstrated the pre-sence of an epithelial hypoplasia,while the connective tissues present
with a decrease in collagen and an in-crease in glycoaminoglycanes. An-other hypothesis concerning theorigin of these fissures is that thereis a break in the gingival fibers, fol-lowed by a pathological bone remo-deling with loss of the corticalbone42.
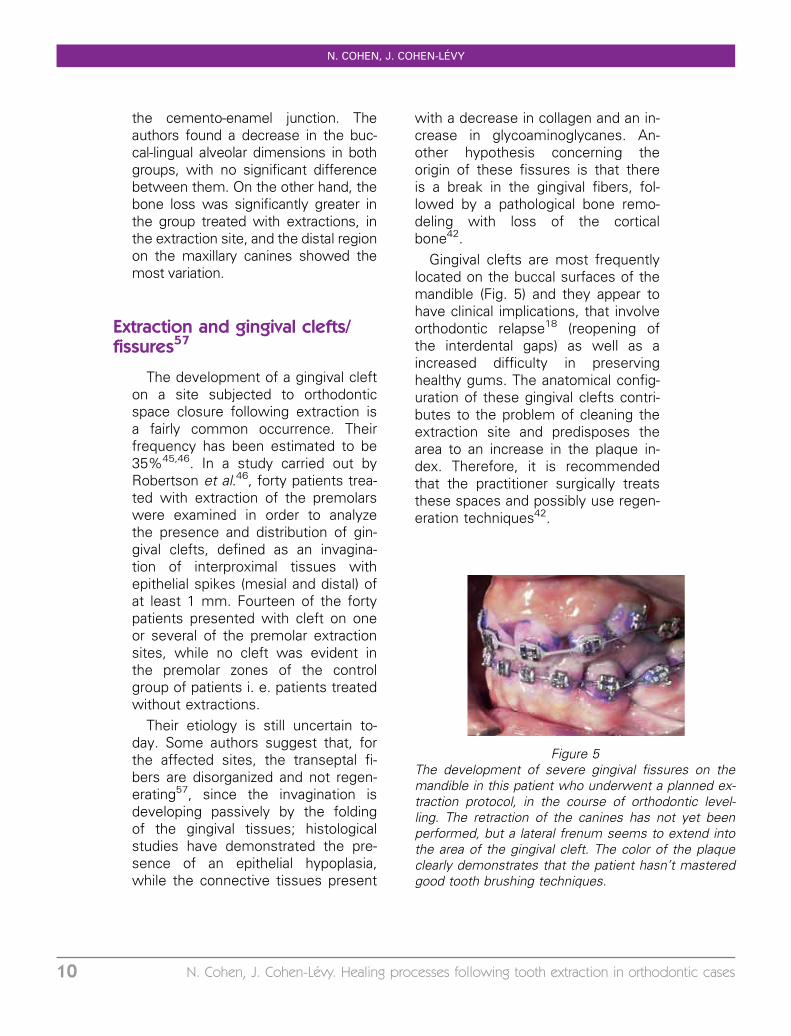
Gingival clefts are most frequentlylocated on the buccal surfaces of themandible (Fig. 5) and they appear tohave clinical implications, that involveorthodontic relapse18 (reopening ofthe interdental gaps) as well as aincreased difficulty in preservinghealthy gums. The anatomical config-uration of these gingival clefts contri-butes to the problem of cleaning theextraction site and predisposes thearea to an increase in the plaque in-dex. Therefore, it is recommendedthat the practitioner surgically treatsthese spaces and possibly use regen-eration techniques42.
Figure 5The development of severe gingival fissures on themandible in this patient who underwent a planned ex-traction protocol, in the course of orthodontic level-ling. The retraction of the canines has not yet beenperformed, but a lateral frenum seems to extend intothe area of the gingival cleft. The color of the plaqueclearly demonstrates that the patient hasn’t masteredgood tooth brushing techniques.
N. COHEN, J. COHEN-LEVY
10 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
The treatment of gingival clefts(without an osseous deficit) has beenascribed to the cold blade or the elec-tric cautery: the incision begins apicallyat points marking the depth of the cleftand is directed coronally towards apoint situated between the base of thecleft and the osseous crest. The oss-eous exposure is avoided at all costs,so that the incision attempts to recre-ate as much as possible an ‘‘ideal’’ gin-gival festoon. The excessive tissuesare resected and a pack is applied toenhance healing.
In the case illustrated in figure 6, anadolescent during the course of pre-surgical orthodontic treatment, thatconventionally implies the extraction ofthe maxillary second premolars and ofthe mandibular first premolars, camein for treatment of this type of gingivalcleft (Fig. 6 a, b and c), with a very in-flammed periodontium and high plaqueindex. Following a cone beam xray(6 d, panoramic reconstructions, 6 eaxial cut and dentoaxial recontructions),it appears that the mucosal cleft hasbeen complicated by mesial alveolarclefts on the first molars and severeroot resorption, which will make themanagement and the prognosis forthe adjacent teeth more difficult, eventhough the tooth vitality tests were po-sitive.
A case report described the use ofguided tissue regeneration for thesecases of gingivo-osseous clefts afterorthodontic closing of space42.
Impact of the timing oforthodontic treatment followingextraction
Depending upon the author, thetooth adjacent to the extraction site
may be moved into mature healingbone, or just the contrary, immedi-ately following extraction, while thehealing process is still underway.Based on the animal model, historicalstudies done by Bauerle8 and thenMurphey36 have reported a fasterpace of healing in the bone inrelation to the corresponding extrac-tion site.
Araujo, in 2001, developed ananimal model where he appliedorthodontic forces on the teeth adja-cent to the extraction site that wasfilled with Bio-Oss�1. He showedthat the teeth could be moved threemonth after packing the socket, thatnew formations (resorption/apposi-tion) could take place without affect-ing the quality of newly formedbone.
The authors emphatically insist onthe need to adapt the therapy to thespeed of resorption of the materialand to its properties for remodeling,for angio-genesis, osteo-inductionand osteo-conduction44. Cardaropoliet al. have shown the resorption ca-pacity of this material after 14 dayshave passed13. These findings arestill debatable and there seems tobe agreement that the longer themovement is delayed, the lesserthe risk44.
Impact of the location of theextraction site
The incisors have a thin buccal cor-tical bone, their roots may be promi-nent and sometimes outside of theosseous envelope (check to see ifthere were any prior orthodontictreatments to expand the shape ofthe arch); sometimes, when the
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 11
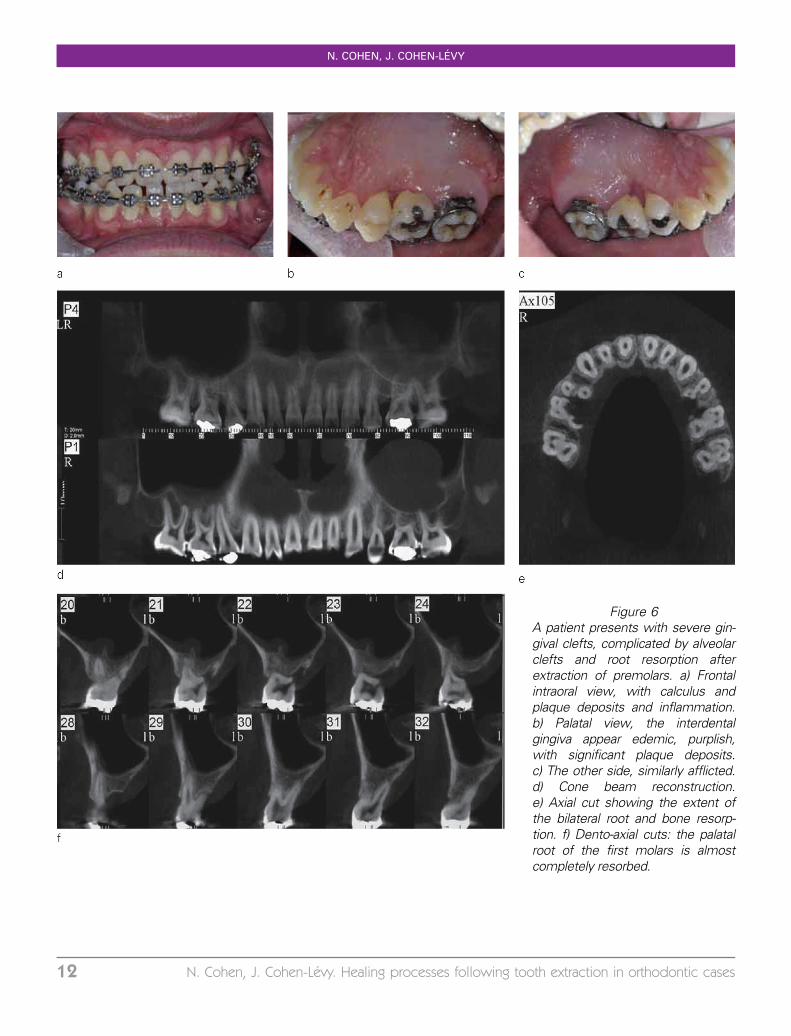
Figure 6A patient presents with severe gin-gival clefts, complicated by alveolarclefts and root resorption afterextraction of premolars. a) Frontalintraoral view, with calculus andplaque deposits and inflammation.b) Palatal view, the interdentalgingiva appear edemic, purplish,with significant plaque deposits.c) The other side, similarly afflicted.d) Cone beam reconstruction.e) Axial cut showing the extent ofthe bilateral root and bone resorp-tion. f) Dento-axial cuts: the palatalroot of the first molars is almostcompletely resorbed.
N. COHEN, J. COHEN-LEVY
12 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
mandibular symphysis is narrow withsignificant lingual repositioning, lin-gual cortical bones may be, conver-sely, thinned out (‘‘shaped like acomma’’).
The canines are the longest teethin the arch, and the maxillary caninesare the pillars of the face, and main-tain close relations with the nasalfossa and the maxillary sinus, thatthey juxtapose. They are coveredwith a thin film of cortical bone,where fenestrations and dehiscencesare generally present. Their extractioninvolves a significant risk for osseouscollapse.
The maxillary premolars and mo-lars, located close to the sinus, mayfor certain patients present a risk fororal sinus communication. With re-gard to mandibular premolars andmolars that are located in less vascu-larized and thicker bone, the risk forinfection complications is greater.
Impact of a supracrestal gingivalfibrotomy
Various factors may affect thespeed of the orthodontic movement,such as bone density, periodontal andosseous metabolism, or the appliedforce. Kaira et al. performed uilateralsupracrestal fibrotomies in a group of14 subjects, from 13 to 22 years ofage, who were treated by the pre-programmed edgewise technique, andwhose treatment was carried out withextractions on the maxillary and man-dibular arches. The retraction wasachieved with non-frictional mechanicalforce, using T-shaped loops, and eachpatient was his own witness (treatedside/control side). The average differ-ence measured 0.36 mm on the maxil-lary arch and 0.60 mm on themandibular arch, but there was no clearevidence of any significant differencewhen a fibrotomy was performed26.
ASSESSING THE POTENTIAL FOR INDIVIDUAL TISSUE REPAIR
From the very first consultation, thevarious risk factors can be evaluated.Some factors are directly accessible,either with the medical history ques-tionnaire that allows the practitioner toassess any possible alteration in overallhealing process, or during the clinicalexamination (visual inspection, period-ontal probing, xrays).
Other considerations, such as thebiological factors for healing (inflam-matory profile, cytokines...), are stillnot part of the diagnostic examina-tion, but are particularly important fortissue repair.
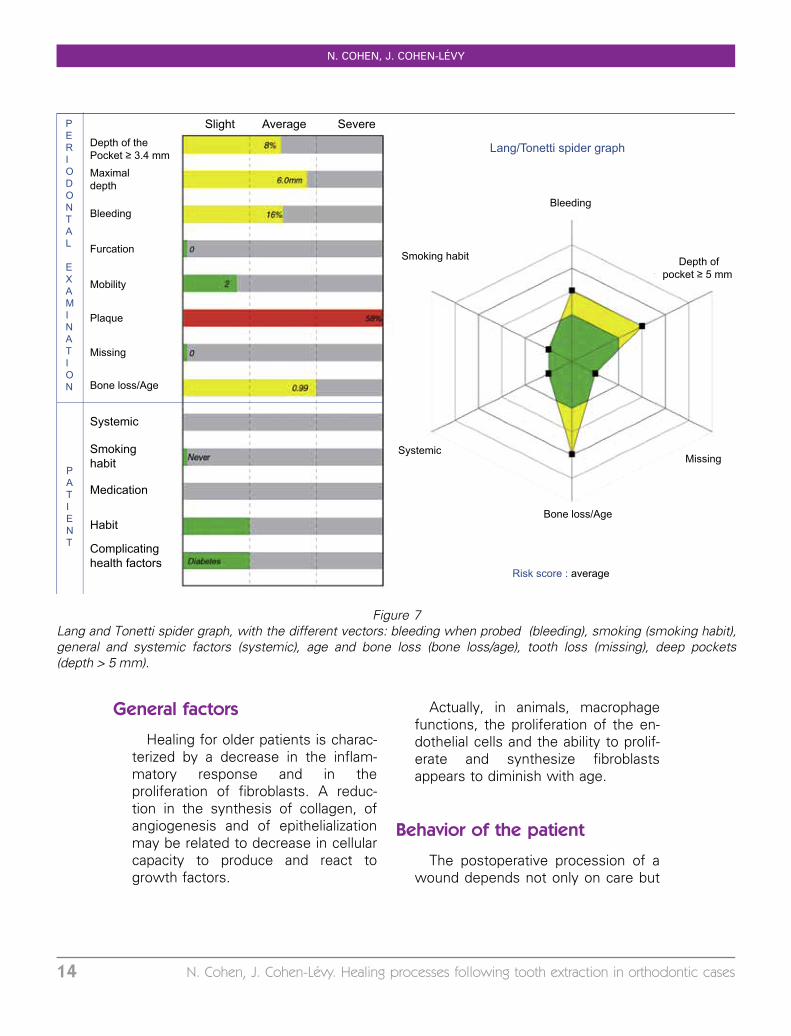
Lang and Tonetti31 have synthe-sized the clinical factors by develop-ing an assessment diagram forpatients in periodontal maintenance.This diagram, presented as a ‘‘spiderdiagram’’, illustrated in figure 7, is aneasy to use visual aid for practitioner/patient communication. It is usefulfor changing parameters, since someof them can be altered (smoking, pla-que control). The role of the ortho-dontist is crucial for making thepatient aware of the need to quitsmoking before extraction and for re-viewing a post-operative checklist.
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 13
General factors
Healing for older patients is charac-terized by a decrease in the inflam-matory response and in theproliferation of fibroblasts. A reduc-tion in the synthesis of collagen, ofangiogenesis and of epithelializationmay be related to decrease in cellularcapacity to produce and react togrowth factors.
Actually, in animals, macrophagefunctions, the proliferation of the en-dothelial cells and the ability to prolif-erate and synthesize fibroblastsappears to diminish with age.
Behavior of the patient
The postoperative procession of awound depends not only on care but
Slight Average SevereDepth of the Pocket ≥ 3.4 mmMaximaldepth
Bleeding
Furcation
Mobility
Plaque
Missing
Bone loss/Age
PATIENT
PERIODONTAL EXAMINATION
Systemic
Smokinghabit
Medication
Habit
Complicatinghealth factors
Lang/Tonetti spider graph
Risk score : average
Systemic
Depth ofpocket ≥ 5 mm
Bleeding
Bone loss/Age
Missing
Smoking habit
Figure 7Lang and Tonetti spider graph, with the different vectors: bleeding when probed (bleeding), smoking (smoking habit),general and systemic factors (systemic), age and bone loss (bone loss/age), tooth loss (missing), deep pockets(depth > 5 mm).
N. COHEN, J. COHEN-LEVY
14 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
also on the behavior of the patient.Excessively rinsing the mouth on theday of the operation, tobacco or alco-hol consumption (see supra), as wellas exerting strenuous physical effortcan lead to the loss of the coagulumand consequently infection.
Plaque index
The oral cavity is a septic healingenvironment, like the skin, that hasboth a positive and negative side: thepresence of bacteria is a source ofinflammation that can modulate the re-pair process by immediately recruitingspecific effectors. However, excessivecontamination of the wounds is asource of healing failure. Therefore, werecommend that when the orthodon-tist uses esthetic composite ‘‘shells’’,bonded to hide the extraction socket,so as not to press the shell against themucosa and impede brushing thatcould promote the build-up of plaqueand food deposits.
Tobacco
Smoking, that leads to both hypox-emia and hypoxia, is also responsiblefor healing failure. Nicotine produces
vasoconstriction, increases the sticki-ness of plaque and the risk for ministrokes and ischemia.
If we take another look at the re-port from the French National Insti-tute of Health (HAS)24, it appears,accordingly to the panel of expertson perioperative smoking, ‘‘that theproven benefits of quitting smokingpreoperatively vary based on howsoon before surgery it stops: quitting6 to 8 weeks before a procedure re-moves the risk of surgical complica-tions due to smoking; 3 to 4 weeksbefore surgery, it improves the out-come for all parameters; even whenit occurs 12 to 48 hours before sur-gery, it lowers the amount of carbonmonoxide and enhances oxygenation.By continuing to abstain from smok-ing during the time required for heal-ing (2-4 months) and possibly forbone consolidation improves surgicaloutcomes’’.
Gingival biotype
The concept of biotype wasfirst described by Ollson andLindhe40 who compared it to dentalmorphology. They differentiate a thin
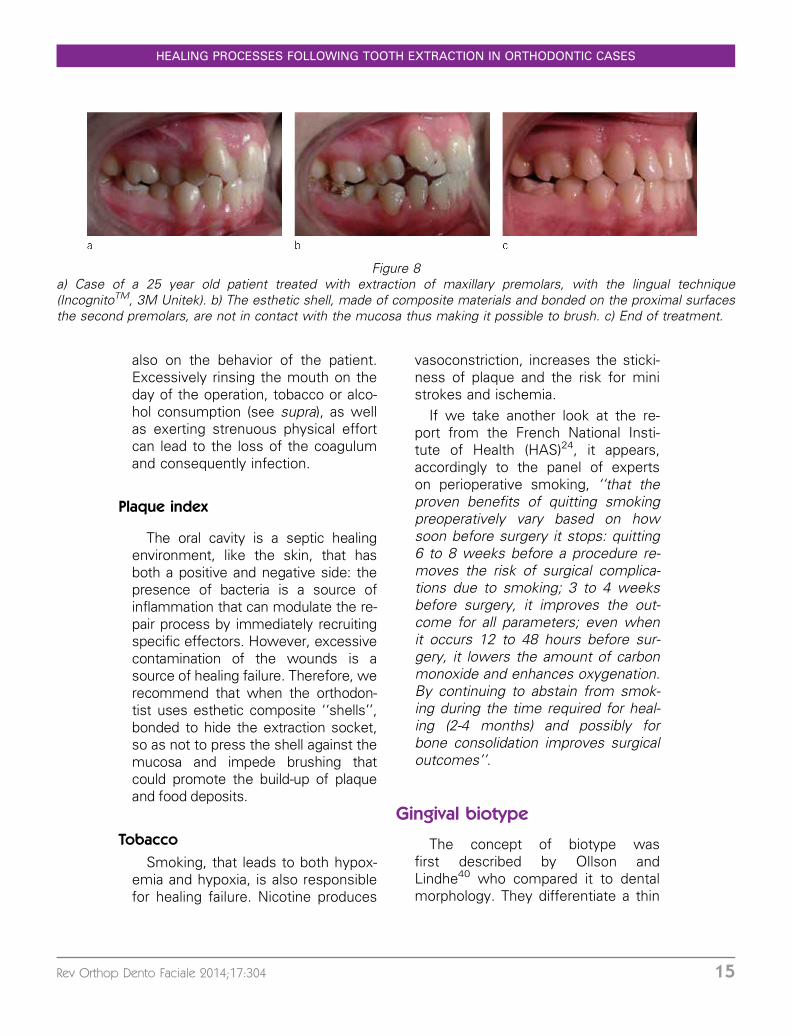
Figure 8a) Case of a 25 year old patient treated with extraction of maxillary premolars, with the lingual technique(IncognitoTM, 3M Unitek). b) The esthetic shell, made of composite materials and bonded on the proximal surfacesthe second premolars, are not in contact with the mucosa thus making it possible to brush. c) End of treatment.
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 15
periodontal type, associated with anarrow and triangular coronal anato-my, from a thick periodontium that isassociated with a wide and roundedcoronal anatomy.
The profile of the gingival mucosacan be assessed directly: color, thick-ness, surface appearance, inflamma-tory condition of the marginal gingivaand mucosa.
The thickness of the gingival mu-cosa can be evaluated by the visibi-lity of the periodontal probe and thetransparency of the tissue when it isinserted into the sulcus28. From asurgical perspective, a fine biotype iseven harder to manage since it isassociated with dental malpositions,due to severely reduced interdentalsepta.
Factors related to the surgicaltechnique
These techniques, developed forextraction protocols followed by im-mediate implants, known as atrau-matic extractions47,58 are intended topreserve the alveolus and especiallythe buccal bone surfaces that areparticuliarly thin on the anterior teeth.These techniques might possibly lim-it post-extractional bone resorption,and therefore prevent any change inthe heights of the gingival collarswhen the prosthetic device is inplace.
Atraumatic extractions
The principle behind atraumatic ex-tractions is to pull the root on a verti-cal axis, and therefore avoid largemovements during luxation.
A syndesmotomy is performed,then the root canal is prepared byusing a bit with a smaller diameterthan that of the auto thread-formingscrews which are secondarily em-bedded into the canal. A wrench,manual or digital, makes it possibleto regulate the torque force of thescrew.
The screw is next connected to a me-tal cable and to a pulley system, thatdistributes the support on the entire halfof the dental arch. A drawback of thissystem is that it can only be applied onmonoradicular teeth, to straight roots(given the direction of the traction),with, for example, a risk for fracturingthe apex of the lateral incisors that pre-sent with a thin apical distal curvature.In addition, the appliance is cumber-some, and is not suitable for patientswhose mouth does not open wide.
Using periotomes33,51
Periotomes are surgical instrumentswith a thin blade, that are inserted intothe sulcus, and guided towards theroot, on a slightly oblique axis, so as toprogressively widen the periradicularspace. The instrument is insertedaround the root and continues verticallyusing axial pressure. A periotome isused to cut the periodontal ligament fi-bers, and to dilate the alveolus, butalso to eliminate any suction effect byallowing air to penetrate. In mostcases, the use of dental forceps is notnecessary.
Piezoelectric osteotomy10,41
The basic principle of piezosurgeryis to use the properties of ultrasoundwaves to section bone tissue, that
N. COHEN, J. COHEN-LEVY
16 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
is approximately five times morepowerful than other scalers.
This device features a high tensionand sinus wave high frequency elec-tric field generator. The inserts, adap-
table to the type of procedure,vibrate at ultrasonic speed, in therange of 28 to 36 kHz, and make itpossible to section hard tissues. Theultrasonic waves are capable of
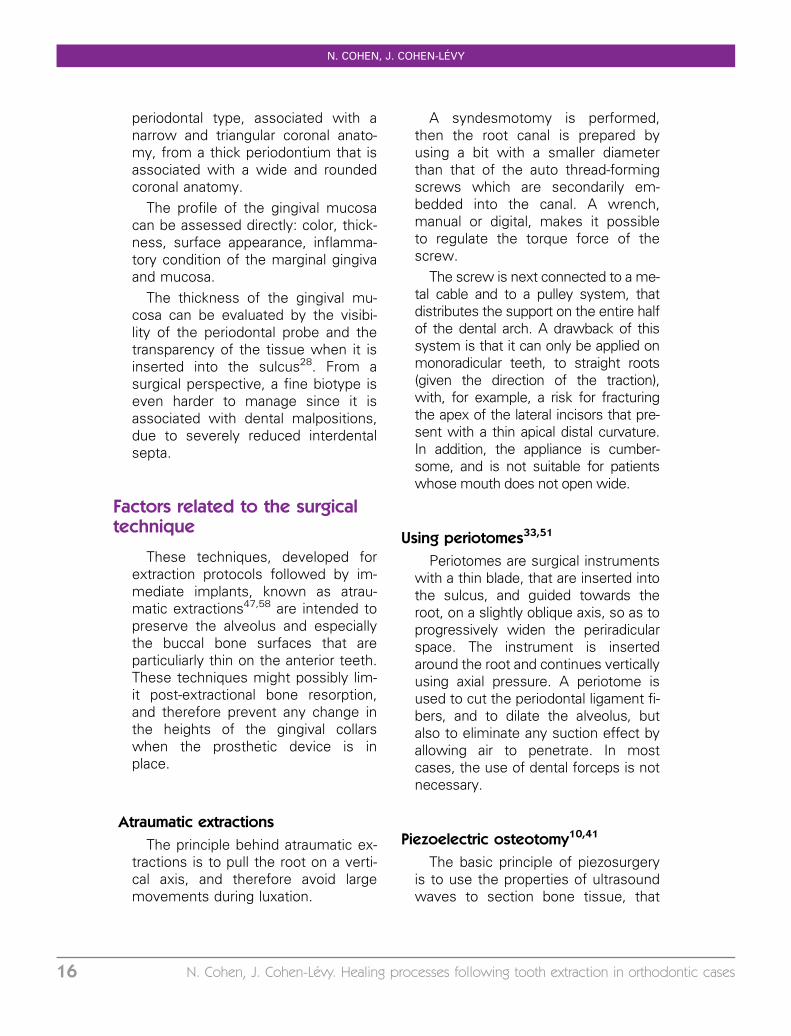
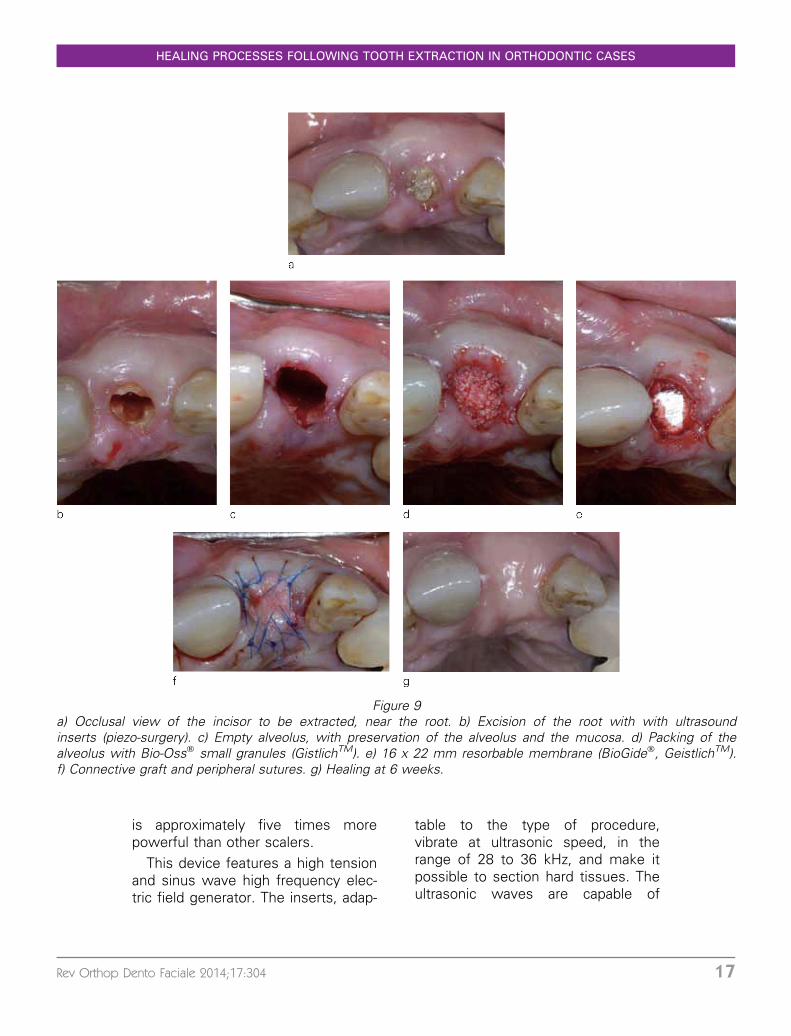
Figure 9a) Occlusal view of the incisor to be extracted, near the root. b) Excision of the root with with ultrasoundinserts (piezo-surgery). c) Empty alveolus, with preservation of the alveolus and the mucosa. d) Packing of thealveolus with Bio-Oss� small granules (GistlichTM). e) 16 x 22 mm resorbable membrane (BioGide�, GeistlichTM).f) Connective graft and peripheral sutures. g) Healing at 6 weeks.
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 17
breaking particles into a suspensionand of destroying bacterial mem-branes, thus helping to reduce therisk for site contamination.
It is reported that procedures car-ried out with piezosurgery lower therisk for post surgical trauma48.
In the case illustrated in figure 9,the extraction of a maxillary incisor,fractured at level of the alveolar ridge,was performed after sectioning of theroot by using piezosurgical inserts(Fig. 9 a, b, c). An alveolectomy wouldhave had harmful consequences forany future restoration and so, to avoidthis, regeneration techniques were uti-
lized not only for the hard tissues – bio-material and membrane (Fig. 9 d, e),but also for the mucosal tissues, usinga connective tissue graft (Fig. 9 f). Therestoration of the volumes before im-plant therapy is very evident (Fig. 9 g),in this patient with a high smile lineand significant esthetic needs.
Healing may be accelerated withthe use of some of the latest surgicaltechniques, that help promote vascu-larization and limit the developmentof necrosis. However, the outcomesare only predictable when the riskfactors are under control.
CONCLUSION
Extractions may cause severecomplications, and this happens, per-haps more often than we think, assome radiological studies haveshown. Even though the surgicaltechnique may be partially responsi-ble for bone loss, other factors canalso be identified.
We are not saying that practi-tioners should systematically use sur-gical techniques for regeneration,but, on the other hand, we need tobe particularly attentive to risk factors
related to the extraction site (extrac-tions of mandibular incisors or ofmaxillary premolars), to the biotypeand to the medical condition of pa-tients (immunosupression, diabetesetc.). As orthodontists, we can try toevaluate and reduce some of the fac-tors involved in pathologic healing,such as plaque control and the useof tobacco.
BIBLIOGRAPHY
1. Araujo MG, Carmagnola D, Berglundh T, Thilander B, Lindhe J. Orthodonticmovement in bone defects augmented with Bio-Oss. An experimental study in dogs.J Clin Periodontol 2001;28:73-80.
2. Araujo MG, Lindhe J. Dimensional ridge alterations following tooth extraction.An experimental study in the dog. J Clin Periodontol 2005;32:212-218.
3. Artzi Z, Nemcovsky CE. The application of deproteinized bovine bone mineral forridge preservation prior to implantation. Clinical and histological observations in acase report. J Periodontol 1998;69:1062-1067.
Conflicts of interest: The author declares noconflict of interest.
N. COHEN, J. COHEN-LEVY
18 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
4. Atwood DA. Postextraction changes in the adult mandible as illustrated by microra-diographs of midsagittal sections and serial cephalometric roentgenograms.J Prosthet Dent 1963;13:810-824.
5. Atwood DA. Some clinical factors related to rate of resorption of residual ridges.1962. J Prosthet Dent 2001;86:119-125.
6. Aydintug YS, Bayar GR, Gulses A, Misir AF, Ogretir O, Dogan N. Clinical study onthe closure of extraction wounds of partially soft tissue-impacted mandibular thirdmolars. Quintessence Int 2012;43:863-870.
7. Baldini N, De Sanctis M, Ferrari M. Deproteinized bovine bone in periodontal andimplant surgery. Dent Mater 2011;27:61-70.
8. Bauerle JR. When do we treat? Chronicle 1969;33:209-210.9. Blum IR. Contemporary views on dry socket (alveolar osteitis): a clinical appraisal of
standardization, aetiopathogenesis and management: a critical review. Int J OralMaxillofac Surg 2002;31:309-317.
10. Blus C, Szmukler-Moncler S. Atraumatic tooth extraction and immediate implantplacement with Piezosurgery: evaluation of 40 sites after at least 1 year of loading.Int J Periodontics Restorative Dent 2010;30:355-363.
11. Bonine FL. Effect of chlorhexidine rinse on the incidence of dry socket in impactedmandibular third molar extraction sites. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 1995;79:154-157; discussion 157-158.
12. Cardaropoli G, Araujo M, Lindhe J. Dynamics of bone tissue formation in toothextraction sites. An experimental study in dogs. J Clin Periodontol 2003;30:809-818.
13. Cardaropoli D, Re S, Manuzzi W, Gaveglio L, Cardaropoli G. Bio-Oss collagen andorthodontic movement for the treatment of infrabony defects in the esthetic zone.Int J Periodontics Restorative Dent 2006;26:553-559.
14. Carlsson GE, Persson G. Morphologic changes of the mandible after extraction andwearing of dentures. A longitudinal, clinical, and x-ray cephalometric study covering5 years. Odontol Rev 1967;18:27-54.
15. Cohen ME, Simecek JW. Effects of gender-related factors on the incidence of loca-lized alveolar osteitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79:416-422.
16. Cox DA, Maurer T. Transforming growth factor-beta. Clin Immunol Immunopathol1997;83:25-30.
17. de Molon RS, Avila ED, Cirelli JA, Mollo-Jr FD, Andrade MF, Barros-Filho LA.A Combined Approach for the Treatment of Resorbed Fresh Sockets AllowingImmediate Implant Restoration. A 2-Year Follow-Up. J Oral Implantol 2013.
18. Edwards JG. The prevention of relapse in extraction cases. Am J Orthod1971;60:128-144.
19. Farina RT, Trombelli L. Wound healing of extraction sockets. Endodontic Topics2011;25:16-43.
20. Froum S, Cho SC, Rosenberg E, Rohrer M, Tarnow D. Histological comparison ofhealing extraction sockets implanted with bioactive glass or demineralized freeze-dried bone allograft: a pilot study. J Periodontol 2002;73:94-102.
21. Graves DT, Nooh N, Gillen T, Davey M, Patel S, Cottrell D et al. IL-1 plays a criticalrole in oral, but not dermal, wound healing. J Immunol 2001;167:5316-5320.
22. Hammerle CH, Araujo MG, Simion M, Osteology Consensus G. Evidence-basedknowledge on the biology and treatment of extraction sockets. Clin Oral ImplantsRes 2012;23 Suppl 5:80-82.
23. Harder S, Egert C, Wenz HJ, Jochens A, Kern M. Influence of the drill material andmethod of cooling on the development of intrabony temperature during preparationof the site of an implant. Br J Oral Maxillofac Surg 2013;51:74-78.
24. Haute autorite de sante. Arret de la consommation de tabac : du de pistage individuelau maintien de l’abstinence en premier recours. Recommandations de bonnepratiques 2013; Argumentation scientifique:1-559.
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 19
25. Johnson K. A study of the dimensional changes occurring in the maxilla followingtooth extraction. Aust Dent J 1969;14:241-244.
26. Kalra A, Jaggi N, Bansal M, Goel S, Medsinge SV, Abraham R et al. Comparison ofrate of canine retraction into recent extraction site with and without gingivalfiberotomy: a clinical study. J Contemp Dent Pract 2013;14:419-426.
27. Klammt J, Gansicke A, Gansicke W, Kunkel J, Muller U, Pingel G. [Risk of alveolitisafter dental extraction]. Stomatol DDR 1985;35:586-593.
28. Kois JC, Kan JY. Predictable peri-implant gingival aesthetics: surgical and prosthodonticrationales. Pract Proced Aesthet Dent 2001;13:691-698; quiz 700, 721-692.
29. Kuboki Y, Hashimoto F, Ishibashi K. Time-dependent changes of collagen crosslinksin the socket after tooth extraction in rabbits. J Dent Res 1988;67:944-948.
30. Kylmaniemi M, Oikarinen A, Oikarinen K, Salo T. Effects of dexamethasone and cellproliferation on the expression of matrix metalloproteinases in human mucosalnormal and malignant cells. J Dent Res 1996;75:919-926.
31. Lang NP, Tonetti MS. Periodontal risk assessment (PRA) for patients in supportiveperiodontal therapy (SPT). Oral Health Prev Dent 2003;1:7-16.
32. Lekovic V, Kenney EB, Weinlaender M, Han T, Klokkevold P, Nedic M, et al. A boneregenerative approach to alveolar ridge maintenance following tooth extraction.Report of 10 cases. J Periodontol 1997;68:563-570.
33. Levitt D. Atraumatic extraction and root retrieval using the periotome: a precursor toimmediate placement of dental implants. Dent Today 2001;20:53-57.
34. Lodi G, Figini L, Sardella A, Carrassi A, Del Fabbro M, Furness S. Antibiotics toprevent complications following tooth extractions. Cochrane Database Syst Rev2012;11:CD003811.
35. Lombardo L, Bragazzi R, Perissinotto C, Mirabella D, Siciliani G. Cone-beamcomputed tomography evaluation of periodontal and bone support loss in extractioncases. Prog Orthod 2013;14:29.
36. Murphey WH, Jr. Oxytetracycline microfluorescent comparison of orthodonticretraction into recent and healed extraction sites. Am J Orthod 1970;58:215-239.
37. Muska E, Walter C, Knight A, Taneja P, Bulsara Y, Hahn M, et al. Atraumatic verticaltooth extraction: a proof of principle clinical study of a novel system. Oral Surg OralMed Oral Pathol Oral Radiol 2013;116:e303-310.
38. Nyman S, Gottlow J, Lindhe J, Karring T, Wennstrom J. New attachment formationby guided tissue regeneration. J Periodontal Res. 1987;22(3):252-4.
39. Oginni FO, Fatusi OA, Alagbe AO. A clinical evaluation of dry socket in a Nigerianteaching hospital. J Oral Maxillofac Surg 2003;61:871-876.
40. Olsson M, Lindhe J. Periodontal characteristics in individuals with varying form of theupper central incisors. J Clin Periodontol 1991;18:78-82.
41. Pavlikova G, Foltan R, Horka M, Hanzelka T, Borunska H, Sedy J. Piezosurgery in oraland maxillofacial surgery. Int J Oral Maxillofac Surg 2011;40:451-457.
42. Pinheiro ML, Moreira TC, Feres-Filho EJ. Guided bone regeneration of a pronouncedgingivo-alveolar cleft due to orthodontic space closure. J Periodontol 2006;77:1091-1095.
43. Pinho MN, Roriz VL, Novaes AB, Jr., Taba M, Jr., Grisi MF, de Souza SL. Titaniummembranes in prevention of alveolar collapse after tooth extraction. Implant Dent2006;15:53-61.
44. Reichert C, Wenghofer M, Gotz W, Jager A. Pilot study on orthodontic space closureafter guided bone regeneration. J Orofac Orthop 2011;72:45-50.
45. Rivera Circuns AL, Tulloch JF. Gingival invagination in extraction sites of orthodonticpatients: their incidence, effects on periodontal health, and orthodontic treatment.Am J Orthod 1983;83:469-476.
46. Robertson PB, Schultz LD, Levy BM. Occurrence and distribution of interdental gingi-val clefts following orthodontic movement into bicuspid extraction sites. J Periodontol1977;48:232-235.
N. COHEN, J. COHEN-LEVY
20 N. Cohen, J. Cohen-Levy. Healing processes following tooth extraction in orthodontic cases
47. Saund D, Dietrich T. Minimally-invasive tooth extraction: doorknobs and strings revis-ited! Dent Update 2013;40:325-326, 328-330.
48. Sivolella S, Berengo M, Bressan E, Di Fiore A, Stellini E. Osteotomy for lower thirdmolar germectomy: randomized prospective crossover clinical study comparing piezo-surgery and conventional rotatory osteotomy. J Oral Maxillofac Surg 2011;69:e15-23.
49. Tallgren A. The continuing reduction of the residual alveolar ridges in completedenture wearers: a mixedlongitudinal study covering 25 years. J Prosthet Dent1972;27:120-132.
50. Ten Heggeler JM, Slot DE, Van der Weijden GA. Effect of socket preservationtherapies following tooth extraction in non-molar regions in humans: a systematicreview. Clin Oral Implants Res 2011;22:779-788.
51. Thomson PJ. Minimising trauma in dental extractions: the use of the periotome.Br Dent J 1992;172:179.
52. Ulm C, Solar P, Blahout R, Matejka M, Gruber H. Reduction of the compact and can-cellous bone substances of the edentulous mandible caused by resorption. Oral SurgOral Med Oral Pathol 1992;74:131-136.
53. Van der Weijden F, Dell’Acqua F, Slot DE. Alveolar bone dimensional changes ofpost-extraction sockets in humans: a systematic review. J Clin Periodontol2009;36:1048-1058.
54. Vergara JA, Caffesse RG. Preservation of esthetics with implant dentistry: a clinicalreport. Clin Implant Dent Relat Res 2002;4:200-211.
55. Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C, Sanz M. Surgical protocolsfor ridge preservation after tooth extraction. A systematic review. Clin Oral ImplantsRes 2012;23 Suppl 5:22-38.
56. Vittorini Orgeas G, Clementini M, De Risi V, de Sanctis M. Surgical techniques foralveolar socket preservation: a systematic review. Int J Oral Maxillofac Implants2013;28:1049-1061.
57. Wehrbein H, Bauer W, Diedrich PR. Gingival invagination area after space closure: ahistologic study. Am J Orthod Dentofacial Orthop 1995;108:593-598.
58. Weiss A, Stern A, Dym H. Technological advances in extraction techniques andoutpatient oral surgery. Dent Clin North Am 2011;55:501-513.
59. Yamano S, Kuo WP, Sukotjo C. Downregulated gene expression of TGF-beta indiabetic oral wound healing. J Craniomaxillofac Surg 2013;41:e42-48.
60. Zubillaga G, Von Hagen S, Simon BI, Deasy MJ. Changes in alveolar bone height andwidth following post-extraction ridge augmentation using a fixed bioabsorbablemembrane and demineralized freeze-dried bone osteoinductive graft. J Periodontol2003;74:965-975.
HEALING PROCESSES FOLLOWING TOOTH EXTRACTION IN ORTHODONTIC CASES
Rev Orthop Dento Faciale 2014;17:304 21