Embed Size (px)
Citation preview

Health Care Sector in India: Some Key Issues
VR MuraleedharanDept of Humanities and Social Sciences
Indian Institute of Technology Madras

Outline
• The Fundamental challenge in public finance
• Basic Features of Indian Health Care Sector– Status of Health– Access to health care (use of health care
services)– Cost of health care
• Distribution of Benefits of Public Spending• Key Policy Questions

Fundamental Challenge in Public Finance
• How much should the government spend for health care? – role of government in financing and providing health care to the people
• How should the benefits of public spending (on healthcare) should be distributed across various socio-economic groups? Who deserves how of much of financial support for health care?
Fundamental principle: A rupee spent on one person is a rupee denied to another person.

Objectives of Healthcare System
• Improve health status
• Provide protection against financial risks arising from illnesses – poverty reduction strategy
• Institute mechanisms to meet “legitimate” expectations of patients

Health Status Indicators

321 131 5274 261 96 Per-capita spending in international dollars (PPP)
17.1 6 23.1 10 4.4 Government health spending to total government spending (%)
69.7 48.7 44.9 33.7 21.3 Government share of Total Expenditure (%)
4.4 3.7 14.6 5.8 4.8 Health expenditure as % of GDP
99 97 99 97 43 Births by skilled attendants
94 99 93 84 67 Fully Immunized (%)
26 15 8 37 87 Under-5 mortality /1000 live-births
15 82<30 68IMR/1000 live-births
Thailand
Sri Lank
a USA China India Indicator
Health Status Indicators: India in comparison with other countries





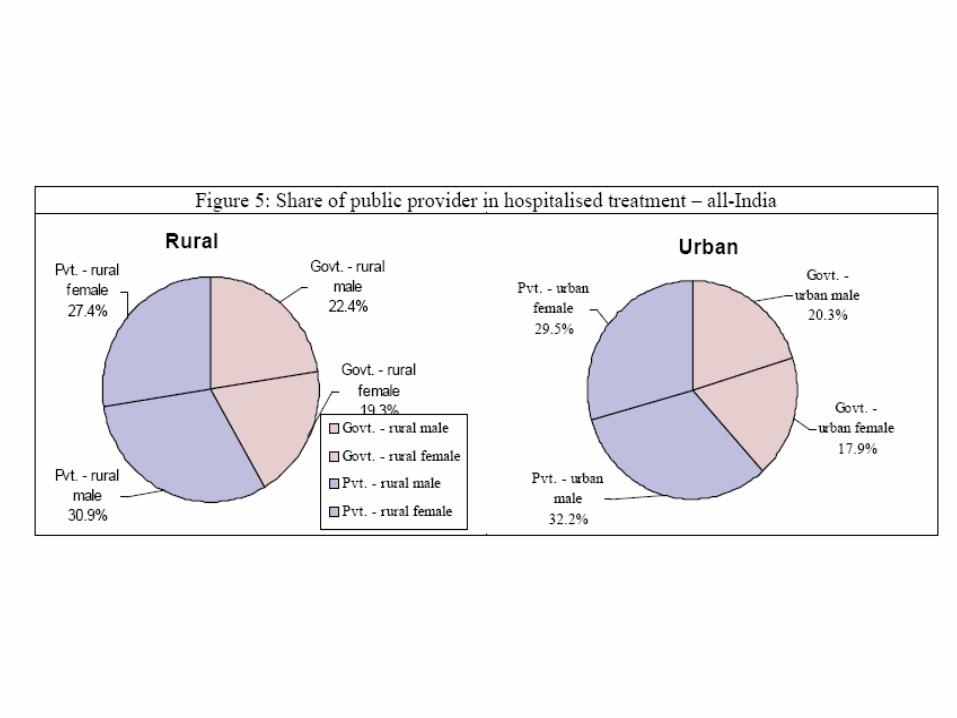
Use of Health Care Services
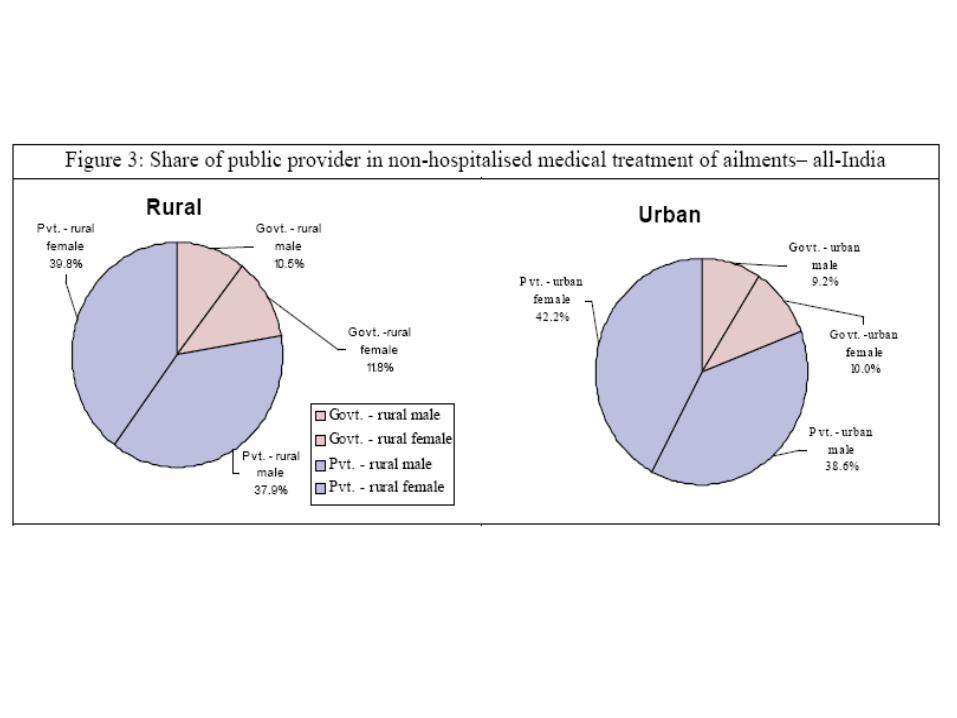
Dependence on Public and Private Providers:


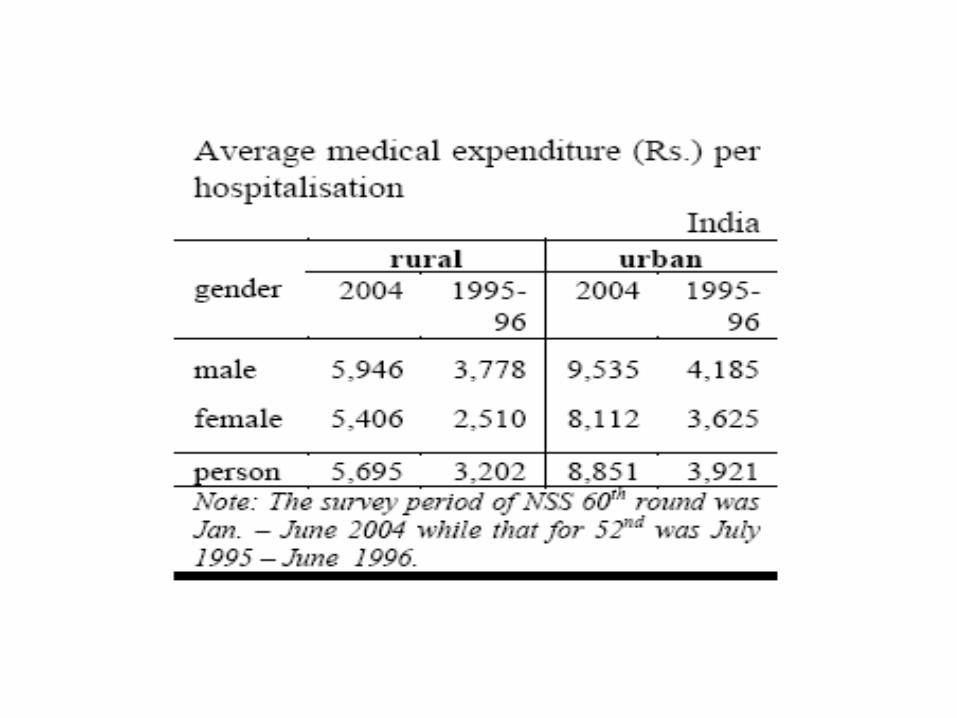
Costs of Health Care
Financial Burden of Ill-health





Two major Health Policy Challenges
•Reduce inequity in health status –Social and economic strata
•Reduce the impoverishing effects of catastrophic health expenditures

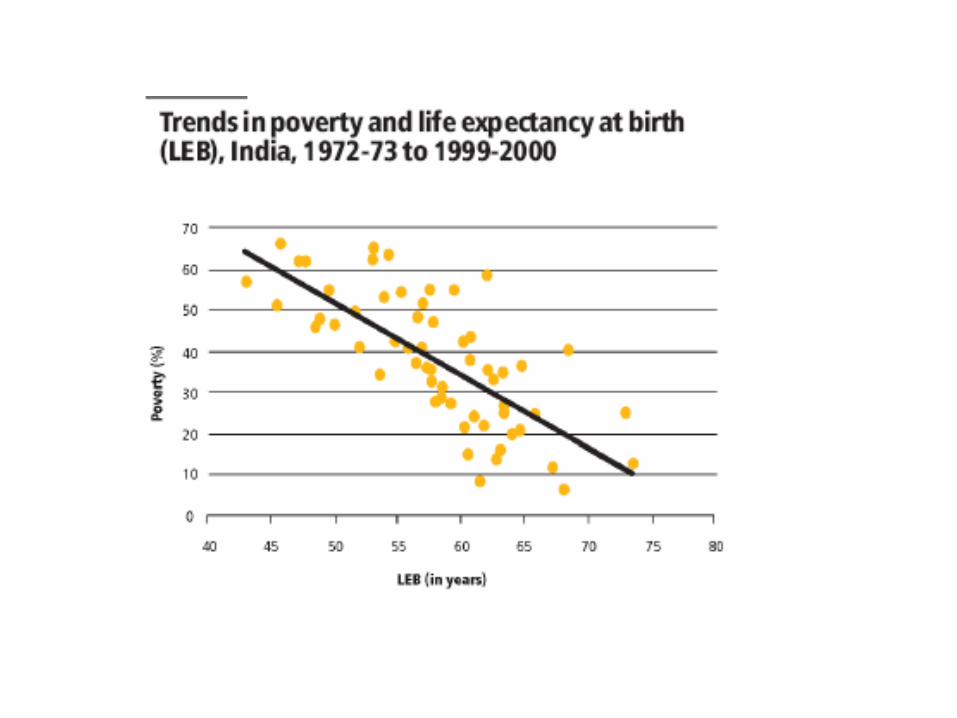
Income inequality and health statusRecent Evidence
•Increase in Income, Education, Health Personnel exert a statistically significant negative impact on health status (IMR)
But
•Increases in income inequality cause health status (IMR) to increase.
(evidence holds good for both high income and low income countries)
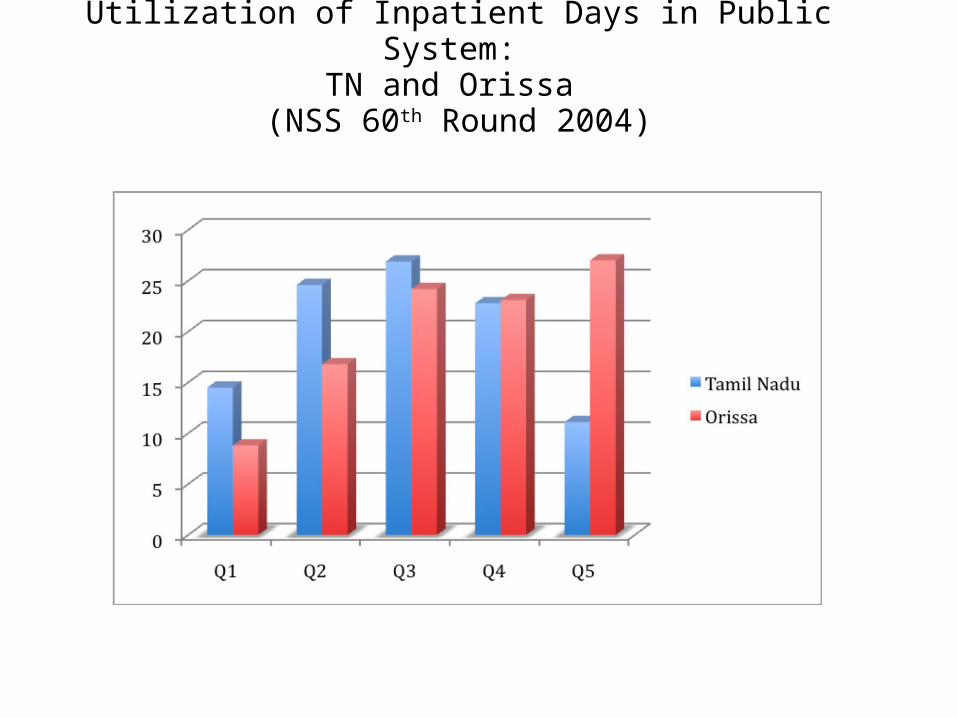
Utilization of Inpatient Days in Public System: TN and Orissa
(NSS 60th Round 2004)

Utilization of Maternity Services in Public System: TN and Orissa (NSSO 60th Round, 2004)

How Much Do Governments Spend on Health Care?
And
How much Should Government Spend?
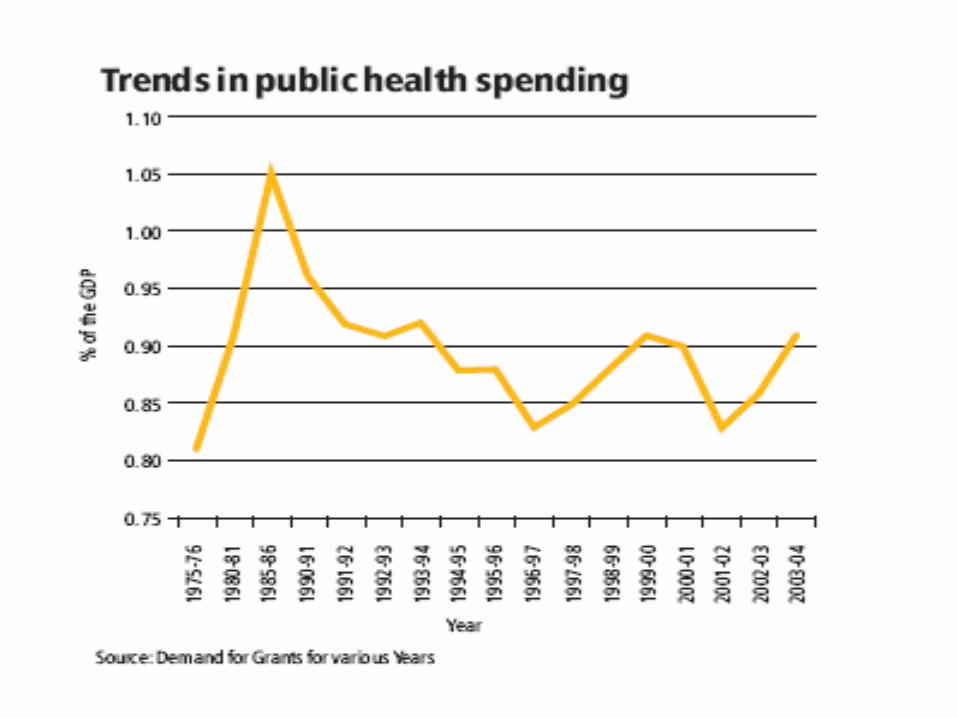


Trends in Per-Capita Public Expenditure
Rs. 64 (1991-92)
Rs.184 (2001-02)
Rs.214 (2003-04)
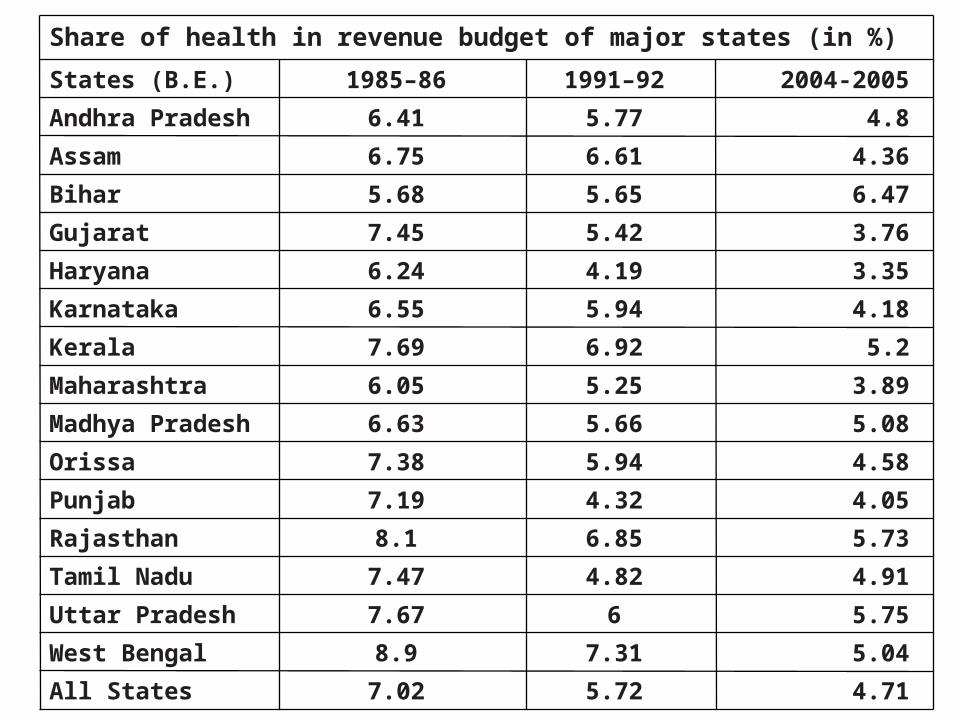
4.71 5.72 7.02 All States
5.04 7.31 8.9 West Bengal
5.75 6 7.67 Uttar Pradesh
4.91 4.82 7.47 Tamil Nadu
5.73 6.85 8.1 Rajasthan
4.05 4.32 7.19 Punjab
4.58 5.94 7.38 Orissa
5.08 5.66 6.63 Madhya Pradesh
3.89 5.25 6.05 Maharashtra
5.2 6.92 7.69 Kerala
4.18 5.94 6.55 Karnataka
3.35 4.19 6.24 Haryana
3.76 5.42 7.45 Gujarat
6.47 5.65 5.68 Bihar
4.36 6.61 6.75 Assam
4.8 5.77 6.41 Andhra Pradesh
2004-2005 1991–92 1985–86 States (B.E.)
Share of health in revenue budget of major states (in %)

Evidently,
government’s spending spent is
LOW

Policy Options
How should the health care system be organized? –(Financing and Provision) –
•Public vs Pvt sector •PPP strategy?

PPP or PPM? Some Common Questions
• Why PPP?
• How to assess whether PPP works well?
• Conditions for PPP’s success?
• What is PPP?

Why PPP? : Some Familiar Answers
• Private sector already widely present – utilize their resources for improving public health
• Better delivery system – better geographical access
• Lack of funds in public sector to expand; will outsourcing reduce public expenditure?
• Peoples’ dependence on private sector and better satisfaction.

35
“Nature” of participation: examples
Financial Non-Philanthropic
• Joint ventures
• Subsidies and concessions to private sector
Philanthropic Contributions
• BGF
• Local Industrialists’ contributions (TN)
• Drugs (from MNCs – case of DEC for Filariasis)
Non-financial
Philanthropic
• In-kind contributions
Community labour for construction of PHC (TN);
Non-philanthropic
Health Camps by corporate hospitals

36
“Forms” of participation: examples
Curative /Diagnostic Services
• Hiring clinical staff (OBGYN/Anesthetists/ medical officers)
• Blindness Control
• Hiring nursing staff
• Contracting-out of laboratory work
Preventive /Promotive
Services
• HIV-AIDS – role of NGOS
• TB control: role of NGOs, Hospitals, Private practitioners, Microscopy centres

37
“Forms” of participation : examples
Supportive services
• Ambulance• Catering• Security• Laundering
Rehabilitative
• Mental health programme?
• Reconstruction of cleft formation (BGF)
Policy Justifications for PPP
• PPP is not an end in itself.
• PPP should eventually: – Reduce cost of care– Improve access to care– Improve quality of care– Reduce inequality in health status
(geographic, gender, socio-economic groups)

Thank You