Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Health communication method and primary care seekingafter screening for early type 2 diabetes in a Japanesehealthcare setting
Rie Ueki • Masao Ichikawa • Yuri Hiranuma •
Takashi Naito • Takami Maeno • Taiga Shibayama
Received: 1 July 2013 / Accepted: 16 September 2013 / Published online: 15 October 2013
� The Japan Diabetes Society 2013
Abstract
Objective Whereas many people at high risk of devel-
oping type 2 diabetes are detected through screening in a
Japanese healthcare setting, they do not necessarily seek
primary care for diagnosis and treatment in the early stages
of the disease. This study aimed to identify the most
effective health communication method for the diabetes
screening report to encourage primary care consultation.
Methods This facility-based cohort study involved 1,128
Japanese participants identified from the routine diabetes
screening database from 2003 to 2009 who were consid-
ered to be at high risk of type 2 diabetes. Multiple logistic
regression analyses were performed to estimate the relative
effectiveness of the health communication method—a let-
ter or an interview—regarding the likelihood of seeking
primary care. The study controlled for sex, age, family
history of diabetes, perceived symptoms, recommendation
for diabetes care, undergoing treatment for other diseases,
detection of comorbidity, request for referral to a specialist,
and counseling by a public health nurse or dietician after
screening.
Results The proportion of participants who sought pri-
mary care after screening was 7 %. Those who received
feedback on diabetes screening via physician interview
were more likely to seek primary care consultation (odds
ratio 2.6, 95 % confidence interval 1.2–5.6).
Conclusion Health communication in the form of an
interview with a physician after diabetes screening may
encourage people at high risk of type 2 diabetes to seek
primary care, yet very few seek primary care in the early
stage of the disease. Therefore, more effective communi-
cation methods are needed.
Keywords Health communication �Type 2 diabetes �Screening � Primary care � Cohort study
Background
In Japan, the number of people with type 2 diabetes is
increasing as a result of lifestyle changes and aging of the
population. In 2007, the Japanese Ministry of Health,
Labour and Welfare (MHLW) estimated that approxi-
mately 8.9 million Japanese out of the total population of
127 million were affected by diabetes [1] and that lifestyle-
related diseases, including diabetes, accounted for about
60 % of all mortality and one third of all medical expen-
ditures [2, 3]. Since 2000, the MHLW—under the National
Health Promotion Movement in the 21st Century (Health
Japan 21)—has striven to reduce the burden of lifestyle-
related diseases by encouraging routine screenings for
these diseases [3, 4]. Under Health Japan 21, priority is
given to preventing and controlling type 2 diabetes and its
associated complications. In 2008, the MHLW required
health insurers to provide screening and counseling/guid-
ance specifically focused on metabolic syndrome [3].
Consequently, the number of people who had a screening
for diabetes increased from 45 million to 60 million during
R. Ueki (&)
Doctoral Program in Nursing Sciences, Graduate School of
Comprehensive Human Sciences, University of Tsukuba,
1-1-1 Tennodai, Tsukuba, Ibaraki 305-8575, Japan
e-mail: [email protected]
M. Ichikawa � T. Maeno � T. Shibayama
Faculty of Medicine, University of Tsukuba, 1-1-1 Tennodai,
Tsukuba, Ibaraki 305-8575, Japan
Y. Hiranuma � T. Naito � T. Maeno
Total Health Evaluation Center Tsukuba, 1-2 Amakubo,
Tsukuba, Ibaraki 305-0005, Japan
123
Diabetol Int (2014) 5:122–128
DOI 10.1007/s13340-013-0143-x

the last decade [5]. Today, many people who are at high
risk of type 2 diabetes are detected in Japanese healthcare
settings through diabetes screening, which examines fast-
ing plasma glucose (FPG) and glycosylated hemoglobin
(HbA1c) [1, 5, 6].
Whereas diabetes screening should lead those at high
risk to seek primary care for diagnosis and treatment, this
does not happen in many cases [1, 7, 8]. Previous studies
suggest that such patients might not be aware of the
importance of primary care because they have no notice-
able symptoms [8]. In addition, the screening reports were
not communicated well enough to prompt such patients to
seek primary care in the early stages of the disease [4, 6].
In Japan, the common methods of communicating the
screening reports are by letter, or by interview with a
physician at the health checkup in the healthcare setting.
Compared with a letter, an interview should be a more
effective method because it allows prompt face-to-face
feedback with a professional [9]. Previous studies found
that mass screening reports were better communicated by
interview than by sending a letter [10, 11]. Among people
with impaired glucose tolerance, interviews by healthcare
providers after a screening reportedly had a greater effect
than a letter with regard to changes in lifestyle, including
weight control and improved diet [6, 12].
However, it is uncertain whether an interview would
encourage people to seek primary care in the early stages of
the disease. In this study, we investigated whether people
identified to be at high risk of type 2 diabetes at screening
were more likely to seek primary care if the screening
results were communicated by interview than by letter.
Methods
Study design and setting
We conducted a facility-based cohort study in a Japa-
nese healthcare setting of adults at high risk of type 2
diabetes. They were identified through annual diabetes
screenings included in their routine health checkups at
the Total Health Evaluation Center Tsukuba, located
approximately 50 km northeast of the Tokyo metro-
politan area covering a population of approximately
216,000.
Participants
Study participants were adults who were identified
through annual screening programs to be at high risk of
developing type 2 diabetes. We found 4,513 such people
in the database of the Total Health Evaluation Center,
Tsukuba, for the years 2003 through 2009; of these indi-
viduals, 3,385 who had been undergoing treatment for
diabetes were excluded. Consequently, 1,128 adults, (957
men and 171 women) aged 54 ± 7.9 years [mean ±
standard deviation (SD), range 31–84] were assessed
(Fig. 1).
Individuals were informed that their anonymous data
would be used in this study but could be withdrawn at any
time. The research ethics committees of both the Health
Evaluation Center Tsukuba and the Graduate School of
Comprehensive Human Sciences at the University of
Tsukuba approved the study.
People had annual diabetes screenings at the Total Health Evaluation Center Tsukuba for the years 2003 through 2009 (n=59,674)
Those who without risk of type 2 diabetes (n=55,161)
People at a high risk of type 2 diabetes: FPG ≥ 7.0 mmol/L or HbA1c (JDS) ≥ 6.5 % coexistent with FPG ≥ 7.0 mmol/L (n=4,513)
Those who had been undergoing treatment for diabetes (n=3,385)
Participants (n=1,128) a
: 957 men and 171 women aged 31-84 years
Health communication methods after diabetes screening b
Letter group (n=242) Interview group (n=886)
Fig. 1 Process of sampling. aStudy participants were adults who had annual diabetes screenings and identified to be at a high risk of type 2
diabetes. bHealth communication methods were by letter or interview, depending upon the particular scheme ordered by each health insurer
Health communication for type 2 diabetes 123
123

Diabetes screening and health communication methods
A high risk of diabetes at screening was assessed according
to the criteria of the Committee of the Japan Diabetes
Society (JDS), namely, FPG C 7.0 mmol/L or HbA1c C
6.5 % (JDS) coexistent with FPG C 7.0 mmol/L [13, 14].
HbA1cwas determined by the standard measurement
method [13–15]. Screenings were conducted during routine
health checkups for adults as required by health insurers
according to the national health promotion policy. Blood
pressure and anthropometric measurements, chest X-ray,
electrocardiography and blood tests were also performed.
A physician communicated results by letter or interview to
all individuals. The communication method depended upon
the health checkup scheme ordered by each health insurer.
According to the guidelines [13], the physician should
assess the results and communicate the following com-
ments to the individual, as appropriate: no problem; in need
of a change of lifestyle; in need of further examination; in
need of medical treatment [4, 13]. It was expected that at-
risk individuals would thus change their lifestyle habits
according to appropriate health guidance [4], and they
could obtain lifestyle counseling from a public health nurse
or dietitian if they asked for it in advance of attending the
screening. For this study, we focused on the comments ‘‘in
need of further examination’’ and ‘‘in need of medical
treatment.’’ The physician communicated the comments by
letter or interview to those at high risk of diabetes and
recommended seeking primary care for confirmatory
diagnosis and treatment of diabetes within 1 month. Both
communication methods included the same type of infor-
mation and differed only in form. In both methods, the
participants received screening test results along with their
reference ranges and advice to improve on the results. The
letter was sent out a few days after the screening; the
interview was conducted for about 10 min at the physical
examination by a physician after the end of screening. In
the interview, questions and answers were possible, unlike
in the letter. The forms of communication methods were
uniform for each health insurer.
Data
We examined longitudinal participant data at baseline and
at 1-year follow-up. The database stored laboratory data,
records of physical assessment by a physician, and the
medical questionnaires completed by study participant self-
report regarding health status and medical histories. Our
main outcome was whether participants sought primary
care for type 2 diabetes within 1 year after their diabetes
screening. Data regarding other factors known to be related
to seeking primary care were also collected: sex [8, 11];
age [8, 11]; family history of diabetes [8]; self-reported
perceived symptoms, such as thirst [8, 16, 17]; whether
recommended to seek immediate medical treatment or
further examination for diabetes [11, 16]; whether under-
going treatment for any diseases other than diabetes [8,
17]; whether diseases other than diabetes were detected
through other screenings at the same time [16]; whether the
participant requested a physician to issue the referral letter
to a diabetes care specialist [11]; and whether the partici-
pant received counseling by a public health nurse or die-
titian other than a physician after the screening [6]. FPG,
HbA1c, and clinical data including body mass index (BMI)
were also obtained. HbA1c value was eventually presented
as a National Glycohemoglobin Standardization Program
(NGSP) equivalent value calculated using the formula;
HbA1c (%) = 1.02 9 HbA1c (JDS) (%) ? 0.25 (%) [18].
Statistical analysis
The proportion of individuals who sought primary care
after screening was compared between the interview and
letter groups. We also made comparisons between groups
regarding sex, age; family history of diabetes (yes/no),
perceived symptoms (any/none), recommendation for dia-
betes care (medical treatment/further examination),
undergoing treatment for other diseases (any/none),
comorbidity detected at screening (any/none), request for
referral to a specialist (yes/no), counseling by a public
health nurse or dietitian (yes/no), and clinical data
including FPG (mmol/L), HbA1c (%), and BMI (kg/m2).
Multiple logistic regression analyses were performed to
estimate the relative effect of the communication method
in terms of seeking primary care, adjusting for the above
factors. The adjusted odds ratio (OR) and its 95 % confi-
dence interval (CI) were obtained. Statistical significance
was considered as P \ 0.05. All analyses were performed
by SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
Results
Of the 1,128 participants, 242 (21 %) were in the letter
group and 886 (79 %) in the interview group. The number
of people who sought primary care after the screening was
84 (7 %): 8 (3 %) in the letter group and 76 (9 %) in the
interview group. There were 41 (4 %) who received the
comment ‘‘in need of medical treatment for diabetes’’ and
1,087 (96 %) who were recommended to have a further
diagnostic examination for diabetes in primary care. In
those who received the comments ‘‘in need of medical
treatment’’: FPG and HbA1c were higher, at 9.9 mmol/L
and 8.6 %, respectively, compared with the group ‘‘in need
of further examination’’: FPG 7.9 mmol/L, HbA1c 6.6 %.
Table 1 shows participant characteristics at baseline. In the
124 R. Ueki et al.
123

letter group, FPG was higher than in the interview group,
and 121 (50 %) of the letter group were aware of some
symptoms compared with 338 (38 %) in the interview
group. Compared with the interview group, a higher pro-
portion of the letter group had other diseases detected at
screening. Conversely, a higher proportion of the interview
group requested a referral to a specialist in diabetes care
(8 % vs. 2 %) and received counseling by a public health
nurse or dietitian (20 % vs. 3 %). There were no significant
differences between groups in terms of sex, age, HbA1c,
BMI, family history of diabetes, recommendation for dia-
betes care, and undergoing treatment for other diseases.
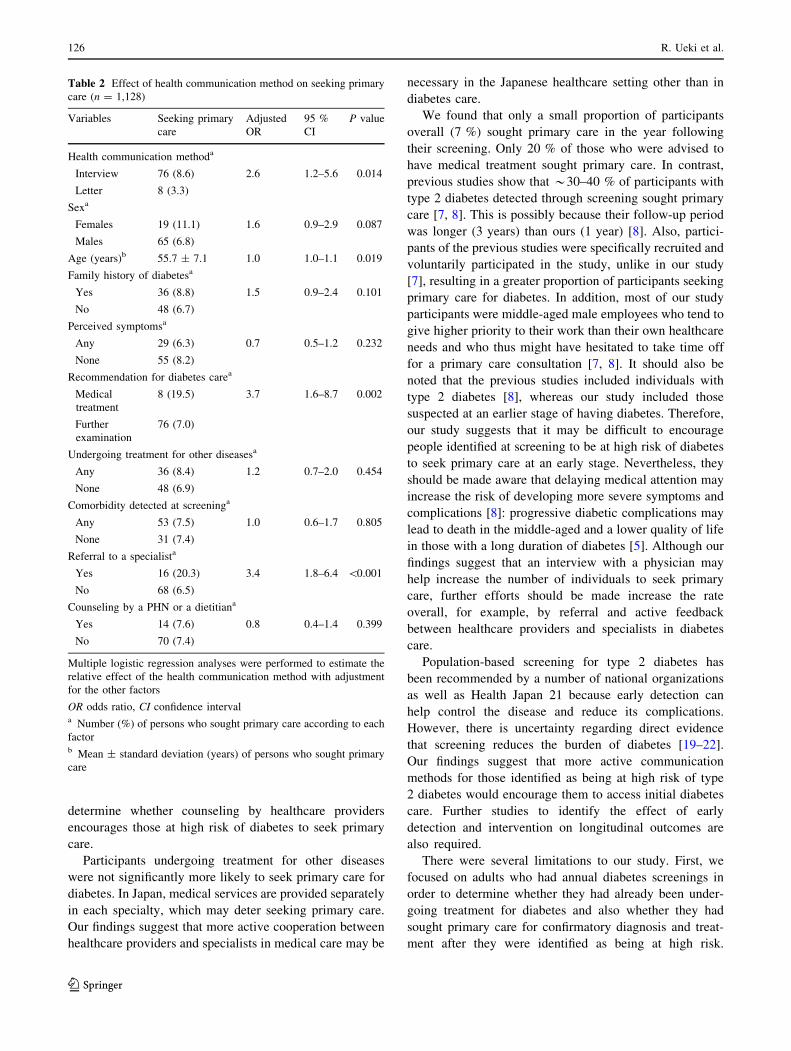
Table 2 shows the relative effect of the communication
method and other factors known to have an effect on
seeking primary care. The interview group was more likely
to seek primary care than the letter group (OR 2.6, 95 % CI
1.2–5.6). A recommendation for medical treatment (OR 3.7,
95 % CI 1.6–8.7) and request for referral to a specialist (OR
3.4, 95 % CI 1.8–6.4) were related to seeking primary care.
Discussion
As hypothesized, participants who received communication
of the results of their diabetes screening in an interview were
more likely to seek primary care than those who received the
information in a letter. An interview may therefore be more
effective in motivating high-risk individuals to seek primary
care after their screening. This finding is supported by pre-
vious studies showing that interviews achieve better patient
understanding of the results of mass screening compared
with communication by letter [9–11].
Besides the communication method, content also influ-
enced individuals in seeking primary care. Those recom-
mended to undergo medical treatment were more likely to
seek primary care than those recommended to undergo a
further examination, possibly because they were convinced
that their condition was serious enough to require prompt
medical attention [11, 16]. In addition, their seeking pri-
mary care may have been further influenced by referral to a
specialist in diabetes care [11]. However, referral to a
specialist was only provided to those who requested it
when the physician informed them about their screening
report, and thus, they may have been more highly moti-
vated to seek such care.
A previous study showed that counseling by a public
health nurse after screening promoted a healthier lifestyle
[6]. However, in our study, the relative effect of counseling
by healthcare providers other than a physician was not
significant. Since 2008, specific health checkups and
counseling guidance focusing on metabolic syndrome have
been promoted through Health Japan 21 with the aim of
preventing lifestyle-related diseases [3]. In our study, we
could not determine the effect of specific counseling
because there were not enough data from the start of this
counseling program. Further studies are required to
Table 1 Characteristics of participants at baseline
Total Letter group Interview group P value
Number 1,128 242 886
Sex, malesa 957 (84.8) 204 (84.3) 753 (85.0) 0.763
Age (years)b 53.9 ± 7.9 54.1 ± 7.7 53.8 ± 8.0 0.515
FPG (mmol/L)b 8.0 ± 1.5 8.5 ± 1.9 7.9 ± 1.4 \ 0.001
HbA1c (%)b,c 6.7 ± 1.1 6.9 ± 1.1 6.7 ± 1.1 0.428
BMI (kg/m2)b 25.3 ± 3.6 25.6 ± 4.0 25.2 ± 3.5 0.131
Family history of diabetesa 411 (36.4) 87 (36.0) 324 (36.6) 0.880
Perceived symptomsa 459 (40.7) 121 (50.0) 338 (38.1) 0.001
Recommendation for diabetes carea
Medical treatment 41 (3.6) 10 (4.1) 31 (3.5) 0.698
Further examination 1087 (96.4) 232 (95.9) 855 (96.5)
Undergoing treatment for other diseasesa 431 (38.2) 79 (32.6) 352 (39.7) 0.052
Comorbidity detected at screeninga 709 (62.9) 177 (73.1) 532 (60.0) \0.001
Referral to a specialista 79 (7.0) 5 (2.1) 74 (8.4) \0.001
Counseling by a PHN or a dietitiana 185 (16.4) 6 (2.5) 179 (20.2) \0.001
FPG fasting plasma glucose level, HbA1c glycolated hemoglobin, BMI body mass index, PHN public health nursea Number (%); differences between interview and letter group calculated using the v2 testb Mean ± standard deviation; differences between interview and letter group calculated using Student’s t testc HbA1c (%) estimated as a National Glycohemoglobin Standardization Program equivalent value (%) calculated by the formula: HbA1c
(%) = 1.02 9 HbA1c (Japan Diabetes Society) (%) ? 0.25 (%)
Health communication for type 2 diabetes 125
123
determine whether counseling by healthcare providers
encourages those at high risk of diabetes to seek primary
care.
Participants undergoing treatment for other diseases
were not significantly more likely to seek primary care for
diabetes. In Japan, medical services are provided separately
in each specialty, which may deter seeking primary care.
Our findings suggest that more active cooperation between
healthcare providers and specialists in medical care may be
necessary in the Japanese healthcare setting other than in
diabetes care.
We found that only a small proportion of participants
overall (7 %) sought primary care in the year following
their screening. Only 20 % of those who were advised to
have medical treatment sought primary care. In contrast,
previous studies show that *30–40 % of participants with
type 2 diabetes detected through screening sought primary
care [7, 8]. This is possibly because their follow-up period
was longer (3 years) than ours (1 year) [8]. Also, partici-
pants of the previous studies were specifically recruited and
voluntarily participated in the study, unlike in our study
[7], resulting in a greater proportion of participants seeking
primary care for diabetes. In addition, most of our study
participants were middle-aged male employees who tend to
give higher priority to their work than their own healthcare
needs and who thus might have hesitated to take time off
for a primary care consultation [7, 8]. It should also be
noted that the previous studies included individuals with
type 2 diabetes [8], whereas our study included those
suspected at an earlier stage of having diabetes. Therefore,
our study suggests that it may be difficult to encourage
people identified at screening to be at high risk of diabetes
to seek primary care at an early stage. Nevertheless, they
should be made aware that delaying medical attention may
increase the risk of developing more severe symptoms and
complications [8]: progressive diabetic complications may
lead to death in the middle-aged and a lower quality of life
in those with a long duration of diabetes [5]. Although our
findings suggest that an interview with a physician may
help increase the number of individuals to seek primary
care, further efforts should be made increase the rate
overall, for example, by referral and active feedback
between healthcare providers and specialists in diabetes
care.
Population-based screening for type 2 diabetes has
been recommended by a number of national organizations
as well as Health Japan 21 because early detection can
help control the disease and reduce its complications.
However, there is uncertainty regarding direct evidence
that screening reduces the burden of diabetes [19–22].
Our findings suggest that more active communication
methods for those identified as being at high risk of type
2 diabetes would encourage them to access initial diabetes
care. Further studies to identify the effect of early
detection and intervention on longitudinal outcomes are
also required.
There were several limitations to our study. First, we
focused on adults who had annual diabetes screenings in
order to determine whether they had already been under-
going treatment for diabetes and also whether they had
sought primary care for confirmatory diagnosis and treat-
ment after they were identified as being at high risk.
Table 2 Effect of health communication method on seeking primary
care (n = 1,128)
Variables Seeking primary
care
Adjusted
OR
95 %
CI
P value
Health communication methoda
Interview 76 (8.6) 2.6 1.2–5.6 0.014
Letter 8 (3.3)
Sexa
Females 19 (11.1) 1.6 0.9–2.9 0.087
Males 65 (6.8)
Age (years)b 55.7 ± 7.1 1.0 1.0–1.1 0.019
Family history of diabetesa
Yes 36 (8.8) 1.5 0.9–2.4 0.101
No 48 (6.7)
Perceived symptomsa
Any 29 (6.3) 0.7 0.5–1.2 0.232
None 55 (8.2)
Recommendation for diabetes carea
Medical
treatment
8 (19.5) 3.7 1.6–8.7 0.002
Further
examination
76 (7.0)
Undergoing treatment for other diseasesa
Any 36 (8.4) 1.2 0.7–2.0 0.454
None 48 (6.9)
Comorbidity detected at screeninga
Any 53 (7.5) 1.0 0.6–1.7 0.805
None 31 (7.4)
Referral to a specialista
Yes 16 (20.3) 3.4 1.8–6.4 \0.001
No 68 (6.5)
Counseling by a PHN or a dietitiana
Yes 14 (7.6) 0.8 0.4–1.4 0.399
No 70 (7.4)
Multiple logistic regression analyses were performed to estimate the
relative effect of the health communication method with adjustment
for the other factors
OR odds ratio, CI confidence intervala Number (%) of persons who sought primary care according to each
factorb Mean ± standard deviation (years) of persons who sought primary
care
126 R. Ueki et al.
123

Therefore, those who did not have annual diabetes
screenings were not considered. However, the proportion
of those identified to be at high risk and who attended
health checkups the next year was 61 % in our target
population, which is similar to the annual uptake rate of
general health checkups reported in the national survey
[23]. Moreover, this proportion did not largely differ
between letter and interview groups (58 % vs. 62 %), so
our findings should not be greatly distorted. Second, par-
ticipants were restricted to employees and their family
members, and most were men. Thus, findings of this study
might not be generalizable to women and those who do not
have or cannot afford to have diabetes screening. Finally,
work-related factors that may affect seeking primary care,
such as workload [7] and capacity and willingness of
employers to play a role in their employees’ health man-
agement [10, 16], were not considered in our analysis
because that information was not available in the database.
If we could estimate the relative effect of work-related
factors, it would be useful for advising employers to sup-
port their employees’ health care.
In conclusion, an interview with a physician after dia-
betes screening has the potential to encourage people at
high risk of type 2 diabetes to seek primary care. How-
ever, as the overall proportion seeking primary care is
very low in the early stages, more active support and
cooperation between healthcare teams should be
considered.
Acknowledgments We are grateful to Dr. Katsuya Yamazaki of
Kawai Clinic for his comments on an earlier draft.
Conflict of interest None.
References
1. Ministry of Health, Labor and Welfare. Outline of results from
2007 National health and nutrition survey. http://www.mhlw.go.
jp/english/wp/wp-hw3/dl/2-064_065.pdf (2012). Accessed 15 Oct
2012.
2. Ministry of Health, Labor and Welfare. Health statistics in Japan
2007. http://www.mhlw.go.jp/english/database/db-hss/dl/hs2007a.
pdf (2012). Accessed 15 Oct 2012.
3. Ministry of Health, Labor and Welfare. Measures for National
Health Promotion. http://www.mhlw.go.jp/english/wp/wp-hw2/
part2/p3_0024.pdf (2012). Accessed 15 Oct 2012.
4. Fukuda H, Shinsho F. Accuracy of health examination results
self-reported by Japanese participants. J Public Health (Oxf).
2007;29:316–20.
5. Ministry of Health, Labor and Welfare. Annual Health, Labor and
Welfare Report 2007–2008. http://www.mhlw.go.jp/english/wp/
wp-hw2/part2/p2c1s3.pdf (2012). Accessed 15 Oct 2012.
6. Sakane N, Sato J, Tsushita K, Tsujii S, Kotani K, Tsuzaki K, et al.
Japan diabetes prevention program (JDPP) research group.
Prevention of type 2 diabetes in a primary healthcare setting:
three-year results of lifestyle intervention in Japanese subjects
with impaired glucose tolerance. BMC Public Health. 2011;
11(1):40.
7. Tsuda K, Tsutsumi A, Kawakami N. Work-related factors asso-
ciated with visiting a doctor for a medical diagnosis following a
worksite screening for diabetes mellitus in Japanese male
employees. J Occup Health. 2004;46:374–81.
8. Oishi M. JDNR group: application of a computerized information
system for diabetic network research in Japan. In: Aoki N, Akazawa
Y, Laporte R, editors. e-Health for diabetes in the Western Pacific:
proceedings of the 1st International Conference on the Western
Pacific diabetes information network (WPDIN) held in Kyoto on 14
November 1999. Amsterdam: Elsevier; 2000. p. 77–83.
9. Arnold E. Developing therapeutic communication skills in the
nurse-client relationship. In: Interpersonal relationships profes-
sional communication skills for nurses. 5th ed. St. Louis: Saun-
ders Elsevier; 2003. p. 199-228.
10. Irie M, Nagata S, Miyata M, Ikeda M, Hirayama S. Psychosocial
evaluation on the correct recollection of periodic medical
checkups of workers. 2. Long-term change in the recalled results
of medical checkups. Sangyo Eiseigaku Zasshi. 1998;40(3):
75–84 (in Japanese).
11. Adachi Y, Matsumoto K, Konishi K, Yokota T, Irisawa Y, Ikuta
J, et al. Referral compliance improved by a letter of introduction
to a specific physician following mass screening. Nihon Kosyu
Eisei Zasshi. 1988;36(7):413–9 (in Japanese).
12. Alberti ZP, Shaw J. International diabetes federation: a consensus
on type 2 diabetes prevention. Diabet Med. 2007;24(5):451–63.
13. Japan Human Dry Dock Association. A small committee report for the
guideline in regard to determination of health screening tests results.
Off J Jpn Soc Human Dry Dock. 2002;17(2):14–30 (in Japanese).
14. The Committee of the Japan Diabetes Society on the diagnostic
criteria of diabetes mellitus, Kuzuya T, Nakagawa S, Satoh J,
Kanazawa Y, Iwamoto Y, Kobayashi M, et al. Report of the
Committee on the classification and diagnostic criteria of diabetes
mellitus. Diabetes Res Clin Pract. 2002;55(1):65–85.
15. The Committee of the Japan Diabetes Society on the diagnostic
criteria of diabetes mellitus, Seino Y, Nanjo K, Tajima N, Ka-
dowaki T, Kashiwagi A, Araki E, et al. Report of the Committee
on the classification and diagnostic criteria of diabetes mellitus.
Diabetol Int. 2010;1:2–20.
16. Shimizu M, Izumi Y, Takahashi M, Ogushi Y. Analysis of factors
which affects movement after health examinations. In: 17th
JCMI. http://www.med.shimane-u.ac.jp/jcmi97/paper/S54.htm (1997).
Accessed 15 Oct 2012 (in Japanese)
17. Yamaguchi N, Okubo T, Yamamura J, Takahashi K, Nakamura
R, Funatani F. A prospective study of access to medical services
following a community-based screening program. Nihon Koshu
Eisei Zasshi. 1990;37(4):281–8 (in Japanese).
18. Kashiwagi A, Kasuga M, Araki E, Oka Y, Hanafusa T, Ito H,
Committee on the Standardization of Diabetes Mellitus-Related
Laboratory Testing of Japan Diabetes Society, et al. International
clinical harmonization of glycated hemoglobin in Japan: from
Japan diabetes Society to national glycohemoglobin standardi-
zation program VALUES. Diabetol Int. 2012;3(1):8–10.
19. Rahman M, Simmons RK, Hennings SH, Wareham NJ, Griffin SJ.
Effect of screening for type 2 diabetes on population-level self-
related health outcomes and measures of cardiovascular risk: 13-year
follow-up of the Ely cohort. Diabet Med. 2012;29(7):886–92.
20. Rahman M, Simmons RK, Hennings SH, Wareham NJ, Griffin S.
How much does screening bring forward the diagnosis of type 2
diabetes and reduce complications? Twelve year follow-up of the
Ely cohort. Diabetologia. 2012;55(6):1651–9.
Health communication for type 2 diabetes 127
123

21. Waugh N, Scotland G, McNamee P, Gillett M, Brennan A,
Goyder E, et al. Screening for type 2 diabetes: literature review
and economic modeling. Health Technol Assess 2007; 11(17).
22. International diabetes federation. Global guideline for type 2
diabetes. http://www.idf.org/global-guideline-type-2-diabetes-
2012 (2013). Accessed 14 Feb 2013.
23. Ministry of Health, Labor and Welfare. Summary report of
comprehensive survey of living conditions 2010. http://www.
mhlw.go.jp/english/database/db-hss/dl/report_gaikyo_2010.pdf
(2010). Accessed 26 Aug 2013.
128 R. Ueki et al.
123





























