Embed Size (px)
Citation preview

Health-e-Access: Improving Care for
Rochester’s Vulnerable Children
Kenneth McConnochie, MD, MPH

Research and Program Funding
• US Dept of Commerce Technology Opportunities Program• Robert Wood Johnson Local Initiative Funding Partners Program• Rochester Area Community Foundation• Maternal and Child Health Bureau R40 MC03605 • Agency for Healthcare Research and Quality R01 HS15165
Disclosure
N. Herendeen, K. McConnochie and N. Wood held equity positions in TeleAtrics, Inc., a vendor of telemedicine equipment, hosting and support services

Health-e-Access
• when and where you need it
• by people you know and trust
Providing Healthcare …

Problem
Large socioeconomic and city-suburban disparities in morbidity burden and in access to care.

Rochester’s Inner City Children:Sociodemographic Comparisons
Inner CityUnits West East Suburb+
Total population N 32,136 50,395 30,270 Population < 18 y N 10,917 17,783 8,417 Black or African American % 70.5 50.2 2.2Hispanic or Latino (of any race) % 8.8 27.9 1.3Median household income $ 20,585 20,559 87,126 Families below federal poverty level % 30.6 34.0 1.0Families w children < 5y below poverty level % 48.8 52.8 0.9Families on public assistance % 20.5 21.0 0.5Educational attainment (among age > 25 y)
High school graduate or higher % 63.1 58.8 96.0Bachelor's degree or higher % 9.8 7.7 63.1
Comparisons Based on 2000 US Census+ County's most affluent suburb

Hospitalization Among Rochester’s Children < 24 months old
• 1990 – 1991• Areas defined by zip codes • Relative Risk: rates compared to baseline rate • Baseline (1.0) = Pittsford• Highest rates = 14605, 14621• Inner city relative risk > 5.0

Greater Morbidity Burden or Lower Utilization/Admission
Threshold?• 5-fold greater admission rate for asthma• Asthma severity indicators demonstrate no city
vs. suburban difference in:– Severity at time of admission– Severity during hospital stay
• Conclusion: Much higher severity adjusted rates (much greater morbidity burden)

Working Women’s Options

Health-e-Access as a Solution
• Overview - how it works
• Brief history
• Service provided and it impact

Childcare/School Clinician site
secure webconnection
Video conference window -view at clinician site
Video conference window -view at child site

Diagnostic Quality Observations

Service Provided
• First telemedicine visits May 2001• > 6500 visits since then• 96% completion rate
(Among visits initiated, 96% have diagnosis and management decisions and treatment based entirely on telemedicine visits.)
• 4701 children enrolled in Health-e-Access at any time
• Among children with a participating primary care practice, 83% continuity. (Visit completed by that practice.)

0
5
10
15
20
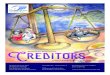
Child Care Absence Due to Illness Before and After Telemedicine
Da
ys
Ab
se
nt
Du
e t
o Il
lne
ss*
* Absence from child care due to illness, in mean days absent per week per 100 registered child-days.
Jan
July
Dec
After
Before
Net impact of telemed:63% reduction
Pediatrics May 2005

Parent Satisfaction%
of
fam
ilie
sBased on interviews with parent after first use of telemedicine. N = 229.
0
10
20
30
40
50
60
70
80
90
100
ED
Allowed to stay at work*
Would choose child carewith telemed over one without
Saved parent trip to:
Pri
mar
yC
are
Ph
ysic
ian
After hours
YesYes
* Estimated time saved = 4.5 hours per telemed visit

Impact on Pattern of Care for Acute Illness
• 6 year cohort study
• Observations from May 2001 through October 2007

Children and Child-Months Studied
ChildrenIntervention Group
4,701
2446 Insurance claims not available1039 Failed inclusion criteria
1,216 Children meeting all criteria for analysis
Child-Months
Matched ComparisonIntervention Control
19,652 19,652
Children enrolled at any time in Health-e-Access child care or elementary school program

Comparability:Control vs. Intervention Groups
• Optimal match Intervention and Control child-months differ only on
availability of telemedicine • Actual match
Perfect match on age, sex, month of year (illness season), zipcode of residence, socioeconomic area, insurance type
School-age children – comparable exposure to peers Preschool children – 100% of intervention children in
large childcare programs. Less so for control children. This introduces a conservative bias (against effect of telemed) when looking at overall utilization.

RESULTS:Attributes of Child-Months Studied
Variables Categories N %Visits/100/
year**Visits/100/
year**Age (months)
Preschool (< 5 yr) 13,187 33.6 82.4 431.3Young school-age (5 thru 8 yr) 15,821 40.3 34.8 238.9Older school-age (9 thru 12 yr) 10,296 26.2 35.2 245.1
Sex Female 20,151 51.3 48.9 299.9
Male 19,153 48.7 53.0 310.5Insurance type
Commercial , Child Health Plus 8,245 21.0 17.2 252.7Medicaid Managed Care 31,059 79.0 59.9 319.0
Illness Season ++Low: Months 7 thru 12 17,158 43.7 44.9 258.6
High: Months 13, 1 thru 6 22,146 56.3 55.6 341.1Socioeconomic area +++
Inner city 23,751 60.4 57.2 306.5Rest of city 11,145 28.4 51.4 308.2
Suburb 4,408 11.2 15.6 289.9All Child-Months 39,304 100.0 50.9 305.1
Distributions+ among 39,304 matched child-
months
ED Utilization
Overall Utilization
Child-months in category
+ All differences in utilization rates among categories for each variable are statistically significant at the .0001 level or better, except as noted.++ Rates differ at the .006 level of significance.+++ Difference in rates not statistically significant.* Overall utilization = all visits of any type (office, ED, or telemedicine) for illness.** Projected visits per 100 children per year

RESULTS:Telemed Impact on Utilization Patterns
0
50
100
150
200
250
300
350
Control Intervention
An
nu
al v
isit
s p
er
10
0 c
hild
ren
Telemed
ED
OfficeIllness
• 3.3% fewer office visits for illness• 23.7% fewer ED visits• 22.9% more illness visits overall

RESULTS:Fewer ED Visits
0
10
20
30
40
50
60
70
Control Intervention
An
nu
al E
D v
isit
s p
er
10
0 c
hild
ren 23.7%
reduction

IMPLICATIONS FOR PAYERS:Break-Even Ratio
Units of:• Cost - overall illness visits increased • Effectiveness - ED visits avoided
Unit Values:• Cost indicator - $51
(mean payment per telemed visit)• Effectiveness indicator - $355
(mean payment per ED visit avoided)
Break-Even Ratio: 355 ÷ 51 = 7:1 (visits increased to ED visits avoided)
Observed Ratio: 5:1

Summary: Impact of Health-e-AccessHealth-e-Access
• Large reduction in absence due to child illness (63% for inner city child care)
• 96% of visits completed• 87% continuity• 23.7% drop in ED visits• 22.9% increase in all visits for illness• Net cost reduction by replacing
expensive ED visits with low-cost primary care (via telemed)

• Social and economic benefits accrue from extraordinary access
• Reduced economic burden of health services
IMPLICATIONS

CONSERVATIVE BIAS
• Exclusion of short-term users from analysis
• Estimate for ED-related payment is low
• Telemedicine not available evenings, weekends, holidays, school vacations.

PATIENT-TO-PROVIDER TELEMDCINE: Next Steps - Organizational
Expansion of insurance reimbursement beyond limits of the Demonstration Project
Reimbursement for telemedicine “infrastructure fee”
Mobile telemedicine units• Telephone management as the gateway to
telemedicine• After-hours neighborhood access sites• Health-e-Access lines of communication

PATIENT-TO-PROVIDER TELEMDCINE: Next Steps - Programmatic
Telemedicine access for developmentally challenged children and adults
Teledentistry Behavioral health • Chronic illness prevention and management• Primary care for deaf population• Elder care • ED diversion through EMS-based mobile
telemed units

Under-Utilization by Inner City Children?
Socioeconomic area N %Visits/100/
year*Visits/100/
year*+ ++
Inner city 23,751 60.4 57.2 306.5Rest of city 11,145 28.4 51.4 308.2
Suburb 4,408 11.2 15.6 289.9
39,304 100.0 50.9 305.1
ED Utilization
Overall Utilization
Child-Months Studied
* Visits per 100 children per year.+ P < .001++ Difference in rates not statistically significant.

What does it take to keep Health-e-Access going?
Components of the infrastructure• Technical• Personnel – triage role, trouble
shooting, roaming telehealth assistants (roaming CTAs)
Cost of the infrastructure