Embed Size (px)
Citation preview

David W. Willis, M.D., FAAP Director of the Division of Home Visiting and Early
Childhood Systems (DHVECS)
Maternal and Child Health Bureau
Health Resources and Services Administration
Department of Health and Human Services
Health Equity and Young Children:
Overview of Federal and State Contexts BUILD: Health Equity and Young Children Conference
May 30, 2013
1

Take Home Messages
• Building health and health equity are key MCH
strategic priorities
• The emphasis on the Prenatal-to-Three period is
required for building health and education
readiness for the next generation of children
• The ACA and the President’s Early Learning
Agenda have created an unprecedented
opportunity united and coordinated with
unified vision
2

A League Table of Child Well-Being
Source: UNICEF, 2013
3

Health inequalities can be seen as
an outcome of…
Social Inequalities
4

What causes health inequities? “The social determinants of health are mostly responsible
for health inequities - the unfair and avoidable
differences in health status seen within and between
countries. The structural roots of health inequities lie
within education, taxation, labor and housing markets,
urban planning, government regulation, health care
systems, all of which are powerful determinants of
health, and ones over which individuals have little or no
direct personal control but can only be altered through
social and economic policies and political processes.”
WHO Commission on the Social Determinants of Health
5

“Social Determinants of Health” Social-Physical-Economic-Services Determinants
• Income & income inequality
• Education
• Race/ethnicity/gender & related discrimination
• Built Environment
• Stress
• Social support
• Early child experiences
• Employment
• Housing
• Transportation
• Food Environment
• Social standing
6

Differential Universality On average, disadvantaged children (neighborhoods)
have poorer outcomes. However, most vulnerable
children are in the populous middle class.
Socioeconomic
Disadvantage Socioeconomic
Advantage
Clyde Hertzman, MD
7

Genetics:Orchid-Dandelion Hypothesis “Biological Sensitivity to Context”
W. Thomas Boyce, M.D., 2008
• Plasticity hypothesis, sensitivity hypothesis, or
differential-susceptibility hypothesis
• Gene x Environment Interactions
• Gene variants (orchid genes) • SERT gene – depression/anxiety – 25% population
• Alleles:
• S/S, S/L
• L/L
• DRD4 gene – externalizing behaviors and antisocial risk, ADHD, risk –
20% population
“Risk becomes possibility”
“Vulnerability becomes plasticity and responsiveness”
8

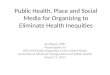
9 Wilkinson & Pickett, The Spirit Level
Index of: • Life expectancy • Math & Literacy • Infant mortality • Homicides • Imprisonment • Teenage births • Trust • Obesity • Mental illness
– incl. drug & alcohol addiction
• Social mobility
www.equalitytrust.org.uk
Health and social problems are worse in more unequal countries
Inde
x of
hea
lth a
nd s
ocia
l pro
blem
s

10
Significant Adversity
Supportive Relationships, Stimulating Experiences, and Health-Promoting Environments
Healthy Developmental Trajectory
Impaired Health and Development
Traditional Framework Guiding Early Childhood Policy and Practice
Source: Harvard

Environment of Relationships
Physical, Chemical & Built Environments
Nutrition
Gene-Environment Interaction
Physiological Adaptations & Disruptions
Biological Embedding During Sensitive Periods
Cumulative Effects Over Time
Foundations of Healthy Development and Sources of Early Adversity
Health-Related
Behaviors
Educational Achievement & Economic Productivity
Physical & Mental Health
Lifelong Outcomes
How Early Experience Gets Into the Body
A Biodevelopmental Framework
11

12
A large portion of many health, safety and prosperity conditions is attributable to Adverse Childhood Experience. ACE reduction reliably predicts a decrease in all of these conditions simultaneously.
POPULATION ATTRIBUTABLE
RISK

Social-
economic
environment
Genetic,
Prenatal and
Neurodevelop-
mental Factors
Attachment and
Relational
Patterns
(ACE Scores)
LIFE COURSE Drivers of Developmental Trajectories
• Neurodevelopmental
• Social-economic
• Relational
Relational Health 13

Relational Health
14
14

We’re in the “building health and
developmental assurance”
business…
Physical health
Developmental health
Relational health
15

“Innovation lies at the intersection
between early childhood systems and
child health”
Jack Shonkoff, M.D, 2011 Harvard’s Center on the Developing Child
16

17
New Protective Interventions
Building an Enhanced Theory of Change that Balances Enrichment and Protection
Significant Adversity
Healthy Developmental Trajectory
Supportive Relationships, Stimulating Experiences, and Health-Promoting Environments
Source: Harvard Center on Developing Child

Pediatric and
OB
Practitioners
CHC’s
Economic
Assistance (TANF,
WIC, Foodstamps)
Child Care
Centers
Head
Start
Family
Resource
Centers
Others
CBO’s
An Early Childhood System
Families
Home
Visiting
Programs
Subsidized
Child Care
Early
Interv.
18

Birth
Early Infancy
Late Infancy
Early Toddler
Late Toddler
Early Preschool Late Preschool
Age 6 mo 12 mo 18 mo 24 mo 3 yrs 5 yrs
Dev
elop
men
tal P
rogr
ess
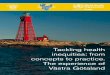
Strategies to Improve
Developmental Trajectories
“At Risk”
Trajectory
“High risk”
Trajectory
“Healthy”
Trajectory
What will push children in red and yellow categories towards green?
Reading to childx
Pre-school Appropriate Discipline
Health Services
Anticipatory Guidance
Parent Responsiveness
Language Stimulation
High quality ECE
Home visiting
Specialized services
19

MIECHV Maternal Infant and Early Childhood Home Visiting
• Section 2951 of the Affordable Care Act of 2010
• Amends Title V of the Social Security Act to add Section 511: Maternal, Infant, and Early Childhood Home Visiting Programs (MIECHV)
• A collaboration between MCHB and ACF
• $1.5 billion over 5 years
• Grants to states • 3% set-aside for grants to Tribes & Tribal Organizations
• 3% set-aside for research, evaluation, and TA)
20

21

MIECHV Opportunities
• Advance the field of maternal and early childhood heath and development
• Translate science into policy • Demonstrate a data collection framework to drive
Quality Improvement practices • Impetus for frontier, rural and urban infrastructure • Catalyst for collaboration and partnerships • Systems integration of HV with early intervention
• Early Childhood Comprehensive Systems (ECCS) • Medical home • Early child care and education
22

MIECHV Priority Populations • Families in at-risk communities
• Low-income families
• Pregnant women under age 21
• Families with a history of child abuse or neglect
• Families with a history of substance abuse
• Families that have users of tobacco in the home
• Families with children with low student achievement
• Families with children with developmental delays or Disabilities
• Families with individuals who are serving or have served in the Armed
Forces, including those with multiple deployments
continued
23

Home Visiting Program Goals
Improvements in:
• Prenatal, maternal, and newborn health
• Child health and development, including the
prevention of child injuries and maltreatment
• Parenting skills
• School readiness and child academic achievement
• Family economic self-sufficiency
• Referrals for and provision of other community
resources and supports
Reductions in crime and/or domestic violence
24

AAP Building Bridges Among Health and
Early Childhood Systems Project 2013
Goals • Establish collaborative leadership for EBCD
message carrying
• Emphasize the importance of “First 1000 Days”
across all EC systems
• Establish collaborations that yield linkages
between expanding medical home and EC
activities and programs
• Focus on “crossing the data divide” and
intentionally building health and developmental
capacity
25

26
5 Critical Components
Medical Homes/ Health Care
Early Care and Education
Social-Emotional Development/Mental Health
Family Support Services
Parent Education
ECCS Critical Components

New ECCS Grant Opportunity
• Requires:
• Partnership with Early Childhood System teams
and, preferably, state AAP Chapter
• Strategy choices:
• Mitigation of toxic stress and trauma in infancy
and early childhood
• Coordination of the expansion of developmental
screening activities in EECC settings
• Improvement of state infant/toddler child care
quality initiatives by incorporating 10 or more
Caring for Our Children: National Health and Safety Performance Standards
27

Breakthrough Early Childhood Activities
• Project LAUNCH (SAMHSA)
• MIECHV (Maternal Infant and Early Childhood Home Visiting)
• Help Me Grow
• ECCS (Early Childhood Comprehensive Systems)
• Race to the Top States
• TECCS (Transforming Early Childhood Community Systems)
• Place- Based Initiatives
• California: First 5 Alameda County, Magnolia Place
• Children’s Service’s Council Palm Beach County
• Promise Neighborhoods (US Department of Education)
• Magnolia Place
28

29

Project LAUNCH: Dual Focus: Systems Change
Forging partnerships: public,
private, parents
Uniting around a common vision
for young child wellness
Scanning, planning, and
evaluating progress
Improving policies and practices,
smart spending, integrated data
systems and common outcomes
Young Child
Wellness Councils
30

New Opportunities for
Collaborative Partners Yields new partners and innovation
• Health Reform
• Trauma informed systems / ACE scoring
• Triple Aim
• Information technology / unified data sets
• ReadyNation – ROI, workforce development
• Early education readiness as health outcome
31

The Five Conditions of
Collective Impact Success • Common agenda – shared vision
• Shared Measurement – collecting data and measuring
results consistently
• Mutually Reinforcing Activities – differentiating while
still coordinated
• Continuous Communication – consistent and open
communication
• Backbone Organization – for the entire initiative and
coordinate participating organizations and entities
Source: J. Kania and M. Kramer, 2011 32

It’s all about: • Building health, First 1000 Days
• “Building brains, forging futures!”
• The earliest relationships and their sturdiness
• Breaking the generational transmission of abuse, ACE
transmission and toxic stress mitigation
• Partnerships and shared values of communities of all
agencies that becomes a collective impact approach
• A culture of quality, measurement and accountability
• Population approaches and management upstream
• Driving innovation in all we do
• Proven, wise and sustainable investments for young
children’s future
33

Take Home Messages
• Building health and health equity are key MCH
strategic priorities
• The emphasis on the Prenatal-to-Three period is
required for building health and education
readiness for the next generation of children
• The ACA and the President’s Early Learning
Agenda have created an unprecedented
opportunity united and coordinated with
unified vision
34

Contact Information
David W. Willis, MD, FAAP
Director, Division of Home Visiting
and Early Childhood Systems
Maternal and Child Health Bureau, HRSA
301-443-8590
35