Embed Size (px)
Citation preview

259
SUMMARYHealth literacy is a relatively new concept in health pro-motion. It is a composite term to describe a range of out-comes to health education and communication activities.From this perspective, health education is directed towardsimproving health literacy. This paper identifies the failingsof past educational programs to address social and eco-nomic determinants of health, and traces the subsequentreduction in the role of health education in contemporaryhealth promotion. These perceived failings may have led tosignificant underestimation of the potential role of healtheducation in addressing the social determinants of health. A‘health outcome model’ is presented. This model highlightshealth literacy as a key outcome from health education.Examination of the concept of health literacy identifies
distinctions between functional health literacy, interactivehealth literacy and critical health literacy. Through thisanalysis, improving health literacy meant more than trans-mitting information, and developing skills to be able toread pamphlets and successfully make appointments. Byimproving people’s access to health information and theircapacity to use it effectively, it is argued that improvedhealth literacy is critical to empowerment. The implicationsfor the content and method of contemporary health edu-cation and communication are then considered. Emphasisis given to more personal forms of communication, andcommunity-based educational outreach, as well as thepolitical content of health education, focussed on betterequipping people to overcome structural barriers to health.
Health literacy as a public health goal: a challenge forcontemporary health education and communicationstrategies into the 21st century
DON NUTBEAM Department of Public Health and Community Medicine, A27, University of Sydney, NSW 2006, Australia
HEALTH PROMOTION INTERNATIONAL Vol. 15, No. 3© Oxford University Press 2000 Printed in Great Britain
Key words: empowerment; health education; health literacy; health outcomes
INTRODUCTION
Health literacy is a relatively new concept inhealth promotion. In this paper it is used as acomposite term to describe a range of outcomesto health education and communication activities.From this perspective, health education is directedtowards improving health literacy. This paperexplores the place of health education in con-temporary health promotion, before examiningin greater detail the definition and usefulness ofthe concept of health literacy. In doing so, thispaper attempts to promote renewed attention tothe role of health education and communication
in health promotion and disease prevention, andadvocates improvements in the sophistication ofcontemporary health education strategies.
HEALTH EDUCATION ANDCONTEMPORARY HEALTHPROMOTION
Education has been an essential component ofaction to promote health and prevent diseasethroughout this century. Campaigns to promotematernal and child health, to prevent com-municable disease, and to promote immunization

and other preventive health services have a longhistory. In developing countries, health educationdirected towards these goals remains a funda-mental tool in the promotion of health andprevention of disease.
In developed countries, during the 1960s and1970s this early experience in health campaigningwas directed towards the prevention of non-communicable disease by promoting healthylifestyles. Many of these early campaigns werecharacterized by their emphasis on the trans-mission of information, and were based upon arelatively simplistic understanding of the relation-ship between communication and behaviourchange. Over time, it became apparent that cam-paigns which focussed only on the transmissionof information and failed to take account of thesocial and economic circumstances of individualswere not achieving the results which had beenexpected in terms of their impact on health be-haviour. Many health education programs emerg-ing during the 1970s were found to be effectiveonly among the most educated and economicallyadvantaged in the community. It was assumedthat these groups had higher levels of educationand literacy, personal skills and economic meansto receive and respond to health messages com-municated through traditional media.
As a tool for disease prevention, healtheducation was considerably strengthened by the development of a new generation of moresophisticated, theory-informed interventionsduring the 1980s. These programs focussed onthe social context of behavioural decisions, andfocussed on helping people to develop personaland social skills required to make positive healthbehaviour choices. This type of program waspioneered through school-based health educationprograms directed towards preventing teenagesubstance misuse, and subsequently has beenapplied in other settings (Glanz et al., 1997).
Several theories of behaviour change weredeveloped during this period to guide educationalprograms. Examples include Azjen and Fishbein’stheory of planned behaviour, and Bandura’s sociallearning theory (Ajzen and Fishbein, 1980;Bandura, 1986). These theories have helped toidentify and explain the complex relationshipsbetween knowledge, beliefs and perceived socialnorms, and provide practical guidance on thecontent of educational programs to promote be-havioural change in a given set of circumstances.
During the same period, social marketingevolved as a technique for influencing social norms
and behaviours in populations (Andreasen,1995). Social marketing has encouraged creativeapproaches to the analysis of issues and the de-velopment of programs, especially in relation tothe communication of information. As a conse-quence, health education programs have evolvedin their sophistication, reach and relevance to awider range of groups in populations.
Despite this progress, interventions whichhave relied primarily on communication and edu-cation have mostly failed to achieve substantialand sustainable results in terms of behaviourchange, and have made little impact in terms ofclosing the gap in health status between differentsocial and economic groups in society.
ADDRESSING SOCIALDETERMINANTS OF HEALTH
In the 19th century public health action resultedfrom a need to address the devastating effects of the living and working conditions imposed on populations during the industrial revolution.The initial focus of public health action was,therefore, on the social and environmental deter-minants of the health of the population. By thelate 20th century, however, there had been a shiftin the emphasis of public health action towardmodifying individual risk behaviours.
However, recent epidemiological analysis ofhealth, disease and disability in the populationsof most developed countries confirms the role of social, economic and environmental factors indetermining increased risk of disease and adverseoutcomes from disease (Townsend et al., 1988;Harris et al., 1999). Health status is influenced byindividual characteristics and behavioural pat-terns (lifestyles) but continues to be significantlydetermined by the different social, economic andenvironmental circumstances of individuals andpopulations. The relationships between thesesocial factors and health, although easy to observe,are less well understood and much more difficultto act upon. Consequently they have been givenmuch less attention as a basis for public healthintervention than have individual behaviours inthe recent past.
As the effects on population health of eco-nomic, social and environmental policies adoptedin developed nations in the late 20th centurybegin to emerge and are better understood, there has been renewed interest among publichealth practitioners in acting to influence these
260 D. Nutbeam

determinants of health. This renewed interestwas reflected through the Ottawa Charter forHealth Promotion (World Health Organization,1986) and more recently confirmed in the JakartaDeclaration (World Health Organization, 1997).Through the Charter, health promotion has cometo be understood as public health action which is directed towards improving people’s controlover all modifiable determinants of health. Thisincludes not only personal behaviours, but alsothe public policy, and living and working con-ditions which influence behaviour indirectly, andhave an independent influence on health.
This more sophisticated approach to publichealth action is reinforced by accumulated evi-dence concerning the inadequacy of overlysimplistic interventions of the past. To take a con-crete example, efforts to communicate to peoplethe benefits of not smoking, in the absence of awider set of measures to reinforce and sustainthis healthy lifestyle choice, are doomed to fail-ure. A more comprehensive approach is requiredwhich explicitly acknowledges social and environ-mental influences on lifestyle choices andaddresses such influences alongside efforts tocommunicate with people. Thus, more compre-hensive approaches to tobacco control are nowadopted around the world. Alongside efforts tocommunicate the risks to health of tobacco use,these also include strategies to reduce demandthrough restrictions on promotion and increasesin price, to reduce supply by restrictions on ac-cess (especially to minors), and to reflect socialunacceptability through environmental bans.This more comprehensive approach is not onlyaddressing the individual behaviour, but alsosome of the underlying social and environmentaldeterminants of that behaviour.
It is now well understood from experiences in addressing specific public health problems oftobacco control, injury prevention and pre-vention of illicit drug use, and the more generalchallenge of achieving greater equity in health,that education alone is generally insufficient toachieve major public health goals.
As a result of the failings of educational pro-grams in the past, the role of health education asa tool in the ‘new public health’ promoted by theOttawa Charter has been somewhat downplayed.Health education has often been considered in arather limited way as contributing only to im-provements in individual knowledge and beliefsabout risk factors for disease, and as having onlya limited role in promoting behaviour change in
relation to those risk factors. This may have hadthe unintended consequence of underestimatingthe role of health education, and fails to properlycapture the potential of health education as a toolto support a full range of contemporary publichealth interventions. The failings identifiedabove reflect both an oversimplistic analysis ofthe determinants of health, and of the use ofinappropriate measures of outcome.
HEALTH LITERACY AS AN OUTCOMEOF HEALTH PROMOTION
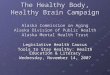
In the recent past, considerable attention has beengiven to analysing the determinants of health,and to the definition of outcomes associated with health promotion activity. This has led to thedevelopment hierarchies of ‘outcomes’ fromhealth interventions, which illustrate and explainthe linkages between health promotion actions,the determinants of health, and subsequenthealth outcomes. Figure 1 provides a summaryoutcome model for health promotion (Nutbeam,1996).
These models generally distinguish betweendifferent levels of outcome. At the end-stage ofinterventions are ‘health and social outcomes’,usually expressed in terms of mortality, mor-bidity, disability, dysfunction, quality of life andfunctional independence.
Intermediate outcomes represent the deter-minants of these health and social outcomes.Personal behaviours, e.g. smoking or physicalactivity may increase or decrease the risk of illhealth, and are summarized as ‘healthy life-styles’. ‘Healthy environments’ consist of theenvironmental, economic and social conditionsthat can both impact directly on health, as well as support healthy lifestyles, e.g. by making itmore or less easy for an individual to smoke (as described above), or adopt a healthy diet.Access to, appropriate provision and appropriateuse of health services are acknowledged asimportant determinants of health status, and arerepresented as ‘effective health services’ in thismodel.
Health promotion outcomes represent thosepersonal, social and structural factors that can bemodified in order to change the determinants ofhealth (i.e. intermediate health outcomes). Theseoutcomes also represent the most immediatetarget of planned health promotion activities.Within this level of the model, ‘health literacy’
Health literacy as a public goal 261

262 D. Nutbeam
Fig. 1: An outcome model for health promotion.
Health and socialoutcomes
Social outcomesmeasures include: quality oflife, functional independence,equity
Health outcomes measures include: reducedmorbidity, disability, avoidablemortality
Healthy lifestylesmeasures include:tobacco use, foodchoices, physicalactivity, alcohol andillicit drug use
Effective healthservices measures include:provision ofpreventive services,access to andappropriateness ofhealth services
Healthyenvironmentsmeasures include:safe physicalenvironment,supportive economicand social conditions,good food supply,restricted access totobacco, alcohol
Intermediate healthoutcomes (modifiabledeterminants ofhealth)
Health promotionoutcomes (interventionimpact measures)
Health literacymeasures include:health-related,knowledge attitudes,motivation,behaviouralintentions, personalskills, self-efficacy
Social action andinfluencemeasures include:communityparticipation,communityempowerment, socialnorms, public opinion
Healthy publicpolicy andorganizationalpracticemeasures include:policy statements,legislation, regulation,resource allocation,organizationalpractices
Health promotionactions Education
examples include:patient education,school education,broadcast media andprint mediacommunication
Social mobilizationexamples include:communitydevelopment, groupfacilitation, targetedmass communication
Advocacyexamples include:lobbying, politicalorganization andactivism, overcomingbureaucratic inertia

refers to the personal, cognitive and social skillswhich determine the ability of individuals to gainaccess to, understand, and use information topromote and maintain good health. These in-clude such outcomes as improved knowledge andunderstanding of health determinants, andchanged attitudes and motivations in relation to health behaviour, as well as improved self-efficacy in relation to defined tasks. Typicallythese are outcomes related to health educationactivities.
The model also distinguishes two other typesof health promotion outcome. ‘Social action andinfluence’ describes the results of efforts toenhance the actions and control of social groupsover the determinants of health—illustrated byefforts to work effectively with to promote thehealth of marginalized groups. ‘Healthy publicpolicy and organizational practices’ are the resultof efforts to overcome structural barriers to health—typically the outcome of political advocacy andlobbying which may lead to legislative change.Success in the introduction of tobacco controllegislation in many countries represents a con-temporary example of an outcome from effectivepublic health advocacy.
The health promotion actions in the modelinclude education for health, efforts to mobilizepeople’s collective energy, resources, skills to-wards the improvement of health, and advocacyfor health. A typical health promotion programmight consist of interventions targeted at allthree of the factors identified as health pro-motion outcomes above. For example, a programto promote healthy eating might consist of effortsto educate people about basic food groups, todevelop practical skills in food preparation andselection, and different actions to improve accessto healthier food choices through supply-sideintervention. These could include, e.g. efforts toimprove the food choices available in school andworksite canteens, and interventions with foodretailers to improve the supply and promotion ofhealthier food choices.
The different intervention strategies also meanthat a wide range of potential measures of healthpromotion outcomes can be considered as evi-dence of success in the short term. Some of theseare listed in the model in Figure 1.
Figure 1 also provides the bridge between anintervention (described as health promotionactions) and the goal of an intervention (modi-fication of the determinants of health). Thesehealth promotion outcomes are the bridge
between what we do and what we are trying toachieve in health promotion interventions.
Use of this model places health education andcommunication into the wider context of healthpromotion, and highlights health literacy as a keyoutcome from health education. In this context,how we define and measure health literacy isboth dictated by and influential on the contentand methods of health education.
WHAT IS HEALTH LITERACY?
The term health literacy has been used in thehealth literature for at least 30 years (Ad HocCommittee on Health Literacy, 1999). In theUnited States in particular the term is used todescribe and explain the relationship betweenpatient literacy levels and their ability to complywith prescribed therapeutic regimens (Ad HocCommittee on Health Literacy, 1999). Thisapproach infers that ‘adequate functional healthliteracy means being able to apply literacy skillsto health related materials such as prescriptions,appointment cards, medicine labels, and direc-tions for home health care’ (Parker et al., 1995).Research based on this definition has shown, e.g.that poor functional health literacy poses a majorbarrier to educating patients with chronic diseases(Williams et al., 1998), and may represent a majorcost to the health care industry through inadequateor inappropriate use of medicines (NationalAcademy on an Aging Society/Center for HealthCare Strategies, 1998).
However, this fundamental but somewhatnarrow definition of health literacy misses muchof the deeper meaning and purpose of literacy for people. The field of literacy studies is alivewith debate about different ‘types’ of literacy andtheir practical application in everyday life. Oneapproach to classification simply identifies typesof literacy not as measures of achievement inreading and writing, but more in terms of what it is that literacy enables us to do (Freebody andLuke, 1990).
Basic/functional literacy—sufficient basic skills inreading and writing to be able to function effect-ively in everyday situations, broadly compatiblewith the narrow definition of ‘health literacy’referred to above.Communicative/interactive literacy—more ad-vanced cognitive and literacy skills which,together with social skills, can be used to actively
Health literacy as a public goal 263

participate in everyday activities, to extractinformation and derive meaning from differentforms of communication, and to apply newinformation to changing circumstances.Critical literacy—more advanced cognitive skillswhich, together with social skills, can be appliedto critically analyse information, and to use thisinformation to exert greater control over lifeevents and situations.
Such a classification indicates that the differentlevels of literacy progressively allow for greaterautonomy and personal empowerment. Progres-sion between levels is not only dependent uponcognitive development, but also exposure todifferent information/messages (communicationcontent and method). This, in turn, is influencedby variable personal responses to such communi-cation—which is mediated by personal and socialskills, and self-efficacy in relation to definedissues.
By contrast to the definition of functional healthliteracy above, WHO defines health literacy morebroadly, as follows (Nutbeam, 1998).
Health literacy represents the cognitive and socialskills which determine the motivation and ability ofindividuals to gain access to, understand and useinformation in ways which promote and maintain goodhealth.
Health literacy means more than being able to readpamphlets and successfully make appointments. Byimproving people’s access to health information andtheir capacity to use it effectively, health literacy iscritical to empowerment.
This definition reflects elements of the two othertypes of literacy described above—interactiveand critical literacy. It also significantly broadensthe scope of the content of health education andcommunication, indicates that health literacymay have both personal and social benefits, andhas profound implications for education andcommunication methods.
In terms of ‘content’, efforts to improvepeople’s knowledge, understanding and capacityto act, should not only be directed at changingpersonal lifestyle or the way in which people use the health services. Health education couldalso raise awareness of the social, economic andenvironmental determinants of health, and bedirected towards the promotion of individual andcollective actions which may lead to modificationof these determinants.
In terms of ‘health benefit’, such a definitionimplies that health literacy is not only a personalresource which leads to personal benefits, e.g.healthier lifestyle choices and effective use ofavailable health services. It also implies that the achievement of higher levels of healthliteracy among a greater proportion of thepopulation will have social benefits, contributing,e.g. by enabling effective community action forhealth, and contributing to the development ofsocial capital.
In terms of ‘method of education’ and com-munication, such a definition provides a challengeto communicate in ways that invite interaction,participation and critical analysis. This is verysimilar to the style of education for ‘criticalconsciousness’ advocated and popularized by theBrazilian educator, Paulo Freire (Freire, 1970).
Health literacy is clearly dependent upon levelsof fundamental literacy and associated cognitivedevelopment. Individuals with undevelopedskills in reading and writing will not only haveless exposure to traditional health education, butalso less developed skills to act upon the in-formation received. For these reasons, strategiesto promote health literacy will remain inextric-ably tied to more general strategies to promoteliteracy. But beyond this fundamental linkbetween literacy and health literacy, much of therichness of health literacy implied by the WHOdefinition is missed in approaches to the pro-motion of functional health literacy as describedabove.
Having emphasized this fundamental relation-ship, however, it is important to recognize thathigh literacy levels (assessed in terms of ability toread and write) are no guarantee that a personwill respond in a desired way to health educationand communication activities. By contrast, Freire,and those that have modelled their education pro-grams on his methods (Wallerstein and Bernstein,1988), have shown that working to raise the‘critical consciousness’ of those with little or noskills in reading and writing can undertakeactivities and achieve outcomes which are closelyaligned to the definition of critical literacydescribed above.
A MODEL OF HEALTH LITERACY
Notwithstanding the strong links betweenliteracy and health literacy, it is essential toconsider the challenges for health education and
264 D. Nutbeam

communication programs which are inherent inthe definition above. Table 1 summarizes some ofthe implications for health promotion action. Itdescribes four different dimensions, i.e.: theeducational goal; the content of a particular formof activity; the outcome expected; and the actionswhich could be taken by health workers.
Level 1, ‘functional health literacy’ reflects theoutcome of traditional health education based on the communication of factual information onhealth risks, and on how to use the health system.Such action has limited goals directed towardsimproved knowledge of health risks and healthservices, and compliance with prescribed actions.Generally such activities will result in individualbenefit, but may be directed towards populationbenefit (e.g. by promoting participation in im-munization and screening programs). Typicallysuch approaches do not invite interactive com-munication, nor do they foster skills developmentand autonomy. Examples of this form of actioninclude the production of information leaflets,and traditional patient education.
Level 2, ‘interactive health literacy’ reflects theoutcomes to the approach to health educationwhich have evolved during the past 20 years. Thisis focussed on the development of personal skillsin a supportive environment. This approach toeducation is directed towards improving personalcapacity to act independently on knowledge,specifically to improving motivation and self-confidence to act on advice received. Again, muchof this activity will result in individual benefit,rather than population benefit. Examples of thisform of action can be found in many contem-porary school health education programsdirected towards personal and social skilldevelopment and behavioural outcomes.
Level 3, ‘critical health literacy’ reflects thecognitive and skills development outcomes whichare oriented towards supporting effective socialand political action, as well as individual action.Within this paradigm, health education mayinvolve the communication of information, anddevelopment of skills which investigate thepolitical feasibility and organizational possibil-ities of various forms of action to address social,economic and environmental determinants ofhealth. This type of health literacy can be moreobviously linked to population benefit, alongsidebenefits to the individual. Health education inthis case would be directed towards improvingindividual and community capacity to act onthese social and economic determinants of health.
Relating this interpretation of the term ‘healthliteracy’ to the outcome model in Figure 1 illus-trates both lateral and vertical relationshipsbetween education, health literacy and the otherhealth promotion outcomes. For example, on avertical plane, improved health literacy mayenable healthy lifestyle choices, and supporteffective use of health services, including com-pliance with treatment regimes. Laterally, edu-cational programs directed at achieving criticalhealth literacy will improve capacity for socialaction which may in turn be directed towardschanging public policy and organizational prac-tices related to health. Examples of this form ofaction can be found in many community develop-ment programs. Through this route health edu-cation can be directed towards achieving changein the social, economic and environmental deter-minants of health which may benefit the healthof whole populations, alongside more typical pro-grams directed at individual lifestyles and healthsystem use.
CONCLUDING REMARKS—NEW OILINTO OLD LANTERNS
Health literacy is a concept that is both new andold. In essence it involves some repackaging ofestablished ideas concerning the relationshipbetween education and empowerment. Edu-cation for health directed towards interactive andcritical health literacy is not new, and has formedpart of social mobilization programs for manyyears. There are many contemporary examples of education being used as a powerful tool forsocial mobilization with disadvantaged groups in both developed and developing countries.Indeed those in developed countries may do well to retrace the roots of contemporary health education in community developmentprograms, and learn from their currentapplication in health development projects indeveloping countries.
Disappointingly, the potential of education asa tool for social change, and for political actionhas been somewhat lost in contemporary healthpromotion. Close attention to the impact ofpublic policy decisions on health, and the need tocreate supportive environments for health mayhave had the unintended consequence of leadingto structural interventions ‘on behalf’ of people—health promotion which is done ‘on’ or ‘to’people, rather than ‘by’ or ‘with’ people. In turn,
Health literacy as a public goal 265

266 D. Nutbeam
Tabl
e 1:
Lev
els
of h
ealt
h lit
erac
y
Out
com
e
Hea
lth
liter
acy
leve
l C
onte
ntIn
divi
dual
ben
efit
Com
mun
ity/
soci
al
Exa
mpl
es o
f ed
ucat
iona
l act
ivit
yan
d ed
ucat
iona
l goa
lbe
nefi
t
Fun
ctio
nal h
ealt
h lit
erac
y:Tr
ansm
issi
on o
f fa
ctua
l Im
prov
ed k
now
ledg
eIn
crea
sed
part
icip
atio
nTr
ansm
it in
form
atio
n th
roug
h co
mm
unic
atio
n of
in
form
atio
n on
hea
lth
of r
isks
and
hea
lth
in p
opul
atio
n he
alth
exis
ting
cha
nnel
s, op
port
unis
tic
info
rmat
ion
risk
s an
d he
alth
ser
vice
s se
rvic
es, c
ompl
ianc
epr
ogra
ms
(scr
eeni
ngin
ter-
pers
onal
con
tact
, and
utili
zati
onw
ith
pres
crib
ed
imm
uniz
atio
n)av
aila
ble
med
iaac
tion
s
Inte
ract
ive
heal
th li
tera
cy:
As
abov
e an
dIm
prov
ed c
apac
ity
toIm
prov
ed c
apac
ity
toTa
ilor
heal
th c
omm
unic
atio
n to
deve
lopm
ent
of p
erso
nal
oppo
rtun
itie
s to
dev
elop
act
inde
pend
entl
y on
infl
uenc
e so
cial
nor
ms,
spec
ific
nee
d; f
acili
tati
on o
fsk
ills
skill
s in
a s
uppo
rtiv
e kn
owle
dge,
impr
oved
inte
ract
wit
h so
cial
com
mun
ity
self
-hel
p an
d so
cial
envi
ronm
ent
mot
ivat
ion
and
grou
pssu
ppor
t gr
oups
; com
bine
self
-con
fide
nce
diff
eren
t ch
anne
ls f
orco
mm
unic
atio
n
Cri
tica
l hea
lth
liter
acy:
A
s ab
ove
and
prov
isio
nIm
prov
ed in
divi
dual
Impr
oved
cap
acit
y to
Pro
visi
on o
f te
chni
cal a
dvic
e to
pers
onal
and
com
mun
ity
of in
form
atio
n on
soc
ial
resi
lienc
e to
soc
ial
act
on s
ocia
l and
supp
ort
com
mun
ity
acti
on,
empo
wer
men
tan
d ec
onom
ican
d ec
onom
ic
econ
omic
det
erm
inan
tsad
voca
cy c
omm
unic
atio
n to
dete
rmin
ants
of
heal
th,
adve
rsit
yof
hea
lth,
impr
oved
com
mun
ity
lead
ers
and
and
oppo
rtun
itie
s to
co
mm
unit
y po
litic
ians
; fac
ilita
te c
omm
unit
yac
hiev
e po
licy
and/
or
empo
wer
men
tde
velo
pmen
tor
gani
zati
onal
cha
nge

health education has been limited to inter-personal communication and media campaignsdirected towards individual behavioural out-comes and health services use.
If achieving health literacy as defined by WHOis to be a goal, some rediscovery of the import-ance of health education needs to occur, togetherwith a significant widening of the content andmethods used. This poses a real challenge forcontemporary health education and the type ofinformation/education/communication programswhich are widely supported by development anddonor agencies—many of which are directed onlytowards achieving functional health literacy asdescribed above.
Pursuing the goal of improved health literacywill also require more overt alliances betweenhealth and education sectors in pursuing the goalof improved literacy levels in the population.This applies at local, national and internationallevels—emphasizing, e.g. the need for improvedalliances between WHO and UNESCO, at aninternational level, and clearer understandingbetween agencies at the most local level (StLeger and Nutbeam, 2000).
Improving health literacy in a populationinvolves more than the transmission of healthinformation, although that remains a fundamentaltask. Helping people to develop confidence to acton that knowledge and the ability to work withand support others will best be achieved throughmore personal forms of communication, andthrough community-based educational outreach.If we are to achieve the ultimate goal that isreflected in that definition of health literacy—trying to promote greater independence andempowerment among the individuals and com-munities we work with—we will need to acknow-ledge and understand the political aspects toeducation, focused on overcoming structuralbarriers to health.
Address for correspondence:Don NutbeamDepartment of Public Health and Community
MedicineA27, University of SydneyNSW 2006Australia
REFERENCES
Ad Hoc Committee on Health Literacy for the AmericanCouncil on Scientific Affairs, American Medical Asso-ciation (1999) Health Literacy: Report of the Council onScientific Affairs. Journal of the American MedicalAssociation, 281, 552–557.
Ajzen, I. and Fishbein, M. (1980) Understanding Attitudesand Predicting Social Behaviour. Prentice-Hall, Engle-wood Cliffs, NJ.
Andreasen, A. R. (1995) Marketing Social Change: Chang-ing Behaviour to Promote Health, Social Development,and the Environment. Jossey-Bass, San Francisco, CA.
Bandura, A. (1986) Social Foundations of Thought andAction: A Social Cognitive Theory. Prentice-Hall,Englewood Cliffs, NJ.
Freebody, P. and Luke, A. (1990) ‘Literacies’ programs:debates and demands in cultural context. Prospect, 5,7–16.
Freire, P. (1970) Pedagogy of the Oppressed. Continuum/Seabody, New York.
Glanz, K., Lewis, F. M. and Rimer, B. K. (1997) HealthBehaviour and Health Education: Theory, Research andPractice. Jossey-Bass, San Francisco, CA.
Harris, E., Sainsbury, P. and Nutbeam, D. (eds) (1999)Perspectives on Health Inequity. Australian Centre forHealth Promotion, Sydney.
National Academy on an Aging Society/Center for HealthCare Strategies (1998) Low health literacy skills increaseannual health care expenditures by $73 billion. Center forHealth Care Strategies Fact Sheet, Washington DC.
Nutbeam, D. (1996) Health outcomes and healthpromotion: defining success in health promotion. HealthPromotion Journal of Australia, 6, 58–60.
Nutbeam, D. (1998) Health promotion glossary. HealthPromotion International, 13, 349–364.
Parker, R. M., Baker, D. W., Williams, M. V. and Nurss, J. R.(1995) The test of functional health literacy in adults: a new instrument for measuring patient’s literacy skills.Journal of General Internal Medicine, 10, 537–541.
St Leger, L. and Nutbeam, D. (2000) Finding commonground between health and education agencies to im-prove school health: mapping goals, objectives, strategies,and inputs. Journal of School Health, 70.2, 45–50.
Townsend, P., Davidson, N. and Whitehead, M. (1988)Inequalities in Health (The Black Report and the HealthDivide). Pelican, London.
Wallerstein, N. and Bernstein, E. (1988) Empowermenteducation: Freire’s ideas adapted to health education.Health Education Quarterly, 15, 379–394.
Williams, M. V., Baker, D. W., Parker, R. M. and Nurss, J. R.(1998) Relationship of functional health literacy topatient’s knowledge of their chronic disease: a study of patients with hypertension and diabetes. Archives ofInternal Medicine, 158, 166–172.
World Health Organization (1986) Ottawa Charter forHealth Promotion. World Health Organization, Geneva.
World Health Organization (1997) Jakarta Declaration onLeading Health Promotion into the 21st Century. WorldHealth Organization, Geneva.
Health literacy as a public goal 267