Embed Size (px)
DESCRIPTION
Health Psychology. Chapter 3: Seeking Health Care. I. Theories of Healthy Behaviors. Health Belief Model Theory of Reasoned Action Theory of Planned Behavior Self-Regulation Theory Precaution Adoption Process Model Transtheoretical Model. Health Belief Model. Susceptibility to disease - PowerPoint PPT Presentation
Citation preview
Health Psychology
Chapter 3: Seeking Health Care

I. Theories of Healthy Behaviors
• Health Belief Model
• Theory of Reasoned Action
• Theory of Planned Behavior
• Self-Regulation Theory
• Precaution Adoption Process Model
• Transtheoretical Model
Health Belief Model
• Susceptibility to disease
• _____________ of disease
• Benefits of behaviors
• Barriers to behaviors
• Problems: ignores SES, ethnicity, access to health care, social norms, good intentions
Theory of Reasoned Action
• Attitude toward behavior• Subjective norm
– DFN: perception of social pressure
• Motivation to comply• ___________________
• Prob: ignores ethnicity, SES, access to health care
Theory of Planned Behavior
• Theory of Reasoned Action
+ Perceived ______________

Self-Regulation Theory(Bandura’s social cognitive theory)
• Behavior• Environment all interact• Personal Factors
– e.g., cognition
• DFN: reciprocal determinism = interaction of factors, all have effects on ______________________

Precaution Adoption Process Model (Weinstein’s)
• 7 stages:– ________________– aware but believe not at risk (optimistic bias)– accept personal risk & idea of precaution– action– (believe action is unnecessary)– made changes– maintain changes

Transtheoretical Model (Prochaska’s)
• 5 stages of behavior change:– precontemplation– contemplation– preparation– action– ___________________

II. Seeking Medical Attention
• DFN: Illness behavior = ______________, determining health status
• DFN: Sick role behavior = ____________, trying to get well
A. Illness Behavior
• Personal reluctance– don’t want to see a doctor
• Social & demographic factors– Less likely to see dr: men, poor, young,
*Tuskegee
• ______________________– visible, severe, interfering, persistent
• Personal view of illness
Views of Illness
• Develop as we mature:– “magic”– contagion– personal _______________________– interaction of bio, psych, & social
Conceptualizing Illness(Leventhal)
• 4 components:– identify/label– time course (of disease & tx)– consequences– cause
• People feel less anxious & helpless when they _________________
B. Sick Role Conceptualizations
• Parson’s- Typical __________________:– can’t be blamed for being sick– relieved of normal responsibilities– will try to get well
• Segall’s (alternative ideas)– right to make health decisions– right to be relieved of normal responsibilities– duty to use variety of health care resources
C. Choosing a Practitioner
• What’s important?– ___________________– ___________________– ___________________

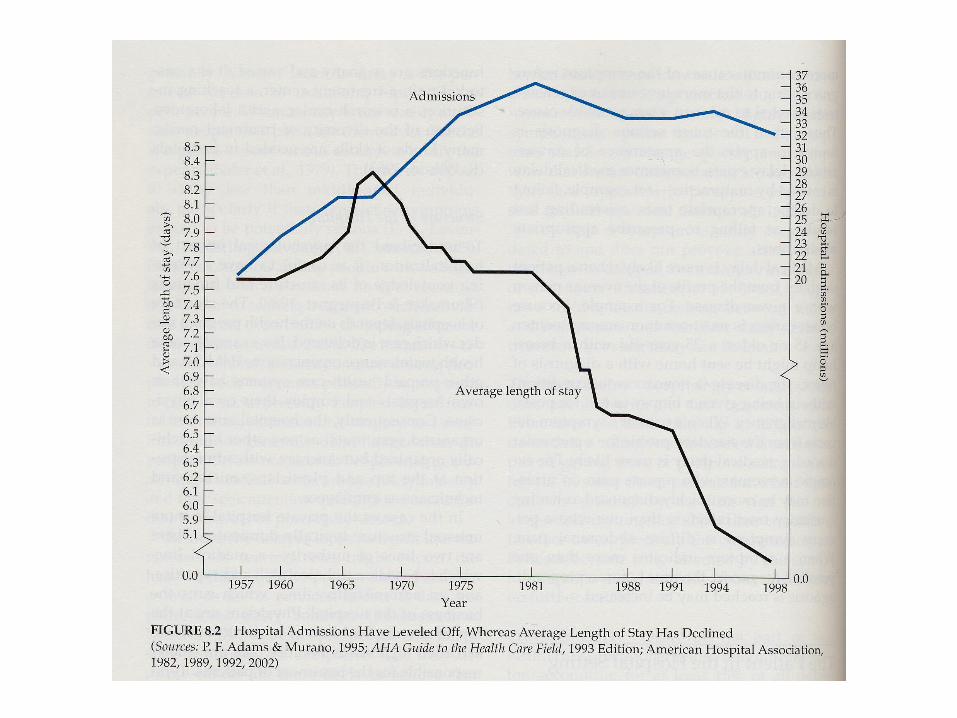

III. Being in the Hospital
A. The Hospitalized Patient Role
• Nonperson Tx = ______________
• Lack of info– Leventhal’s 4
• Loss of control– __________________ = every aspect of
person’s life is managed (e.g., eating, sleeping, schedule)

“Good” vs. “Bad” Patient
• Good: – quiet– submissive– obedient
• Pros: maybe better care, well liked, expect.s
• Cons: helplessness, uninvolved, pt & staff may miss info

• Bad: – demanding– insist on info– aware of rights
• Pros: may be a psych. healthy response, better informed
• Cons: rebellious self-sabotage, staff angry & ignoring

Stressful Medical Procedures- Coping
• Information
• Relaxation Training
• _______________