Embed Size (px)
Citation preview

0066-4308/96/0201-0113$08.00 113
Annu.Rev. Psychol. 1996.47:113–42Copyright© 1996by AnnualReviewsInc. All rightsreserved
HEALTH PSYCHOLOGY:Psychological Factorsand PhysicalDiseasefrom thePerspectiveof HumanPsychoneuroimmunology
Sheldon Cohen andTracyB. Herbert
Department of Psychology, Carnegie Mellon University, Pittsburgh, Pennsylvania15213
KEY WORDS: stress,social support, personality, upperrespiratory infection, immune function
ABSTRACT
This review addresses the importance of studies of human psychoneuroimmu-nology in understanding the role of psychological factors in physical il lness.First, it provides psychologically and biologically plausible explanations forhowpsychological factorsmight influence immunity andimmunesystem–me-diated disease.Second, it coverssubstantial evidencethat factorssuch asstress,negative affect, clinical depression, social support, and repression/denial caninfluenceboth cellular and humoral indicatorsof immunestatus and function.Third, atleastin thecaseof thelessseriousinfectiousdiseases(colds, influenza,herpes), it considersconsistent and convincing evidenceof linksbetween stressandnegative affect and diseaseonset and progression.Althoughstill early in itsdevelopment, research alsosuggests a role of psychological factors in autoim-munediseases. Evidencefor effectsof stress, depression, andrepression/denialononsetandprogressionof AIDS andcanceris lessconsistentand inconclusive,possibly owingtomethodological limitationsinherent in studyingthesecomplexill nesses, or because psychological influences on immunity are not of themagnitudeor typenecessary to alter thebody’s responsein thesecases.What ismissing in this literature, however, is strong evidence that the associationsbetween psychological factors and disease that do exist are attributable toimmunechanges.

CONTENTSINTRODUCTION..................................................................................................................... 114WHAT IS PSYCHONEUROIMMUNOLOGY?...................................................................... 114WHAT IS IMM UNE FUNCTION?.......................................................................................... 115
TheImmuneSystem............................................................................................................. 115Testsof ImmuneFunction ................................................................................................... 115Immunity and Disease......................................................................................................... 117
HOW COULD PSYCHOLOGICAL FACTORSINFLUENCEIMM UNITY ANDDISEASE?........................................................................................................................ 118
DO PSYCHOLOGICAL FACTORSINFLUENCE IMM UNITY AND DISEASE?............. 119Stress.................................................................................................................................... 119Affect.................................................................................................................................... 122Interpersonal Relationships................................................................................................. 124Personali ty........................................................................................................................... 127
DO PSYCHOLOGICAL FACTORSINFLUENCE IMM UNE SYSTEM–MEDIATEDDISEASE?........................................................................................................................ 127
Infectious Disease................................................................................................................ 128Autoimmune Diseases.......................................................................................................... 131Cancer ................................................................................................................................. 133
CONCLUSIONS....................................................................................................................... 136
INTRODUCTION
Much of psychoneuroimmunology’s popularity with both the public andthepsychologicalcommunity derivesfrom its promiseto exploreandexplainthecommonbelief that our personalitiesandemotionsinfluenceour health.Candepression,anxiety, psychologicaldistress,social support,or an optimisticview alterourability to resistinfection,autoimmunediseases,or cancer?Whatare the biological pathwaysthroughwhich psychological characteristicsandstatesyield physicalchanges?Canwe alter immunity andhencediseasesus-ceptibility throughpsychological intervention? Severalhundredstudiespub-lishedin the pastdecadeaddressthe relationof psychological characteristicsand statesto immune function and to healthoutcomesthought to be deter-mined by immune alterations.In this chapterwe highlight what we havelearnedaboutthe importanceof immunity asa link betweenthemind andthebody.
WHAT IS PSYCHONEUROIMMUNOLOGY?
Psychoneuroimmunology (PNI) is the studyof the interrelations betweenthecentralnervoussystem andtheimmune system.Theterminterrelationsis usedbecausethe assumption is that the relationsarebidirectional. Work with ani-malshasadvancedour understandingof this bidirectionality andhasprovidedevidencefor nervesconnectingthe central nervoussystem(CNS) and theimmunesystem(e.g. Feltenet al 1985), for neuroendocrine-inducedaltera-tions of specificimmune functions(e.g.Shavitet al 1984),andfor the exist-
114 COHEN & HERBERT

enceof chemicalscalledcytokinesthat areproducedby the immunesystem,crossthe blood-brainbarrier, and alter the function of the CNS (review inRabinetal 1989).An importantstepin establishingthattheCNS and immunesystem interact wasaccomplishedby psychologistsworkingwith animalmod-elswho demonstratedthat immunesystemchangecouldbeinducedby classi-cally conditioned stimuli (review in Ader &Cohen1993).
The interestsof psychoneuroimmunologistsworking with humansoverlapwith thoseof animalresearchers,but humanpsychoneuroimmunologists’ em-phasesaredifferent.Examplesof overlapin focusincludestudiesof classicalconditioning of humanimmune response(e.g. Bovbjerg et al 1990, Buske-Kirschbaumet al 1992)anddemonstrationsof immune-systemeffectson theCNSasreflectedin humanperformance(Smithet al 1988).Themostobviousdifference,however,is that the humanliteratureis primarily concernedwithbehaviorand psychologicaltraits and statesas drivers of CNS and immuneresponse.Themajor foci of humanstudiesincludeestablishingwhetherthereis an associationbetweenpsychologicaltraits andstatesandimmunity, whatthebiological andbehavioralpathwaysarethatareresponsible for suchrela-tions,andwhetherpsychologically inducedchanges inimmunity are responsi-ble for changesin susceptibility to immunesystem–mediateddisease.
WHAT IS IMMUNE FUNCTION?
The ImmuneSystem
Theimmune systemprotectsthebody from damageby invadingmicroorgan-isms—bacteria,viruses, fungi, and parasites.These foreign materials arecalled antigens.Most immune systemcells are locatedin the bonemarrow,thymus,lymph nodes,spleen,tonsils,appendix,andPeyer’s patches(clumpsof immunetissuein the small intestines).Becausethere is no easyway toaccessthecellsof theseorgans,PNI work with humansis primarily limited tothestudyof immuneprocessesoccurringin circulatingperipheralblood.Cir-culatingbloodtransportsimmune componentsbetweenorgansof theimmunesystemand sites of inflammation. Componentsof the immune systemthatcirculatein blood (e.g.sometypesof white blood cellsandantibody)surveyfor andcombatagainstinvadingantigens.Therefore,peripheralbloodplaysakey role ininflammatory and immune processes.
Testsof Immune Function
In this section,we describethe immunesystemtestsmostcommonly usedinhumanPNI research.Most of the testsevaluatethe role of immunecells inperipheral blood.
PSYCHOLOGICAL FACTORSAND DISEASE 115

ENUMERATIVE TESTS Theenumerativeassaymostoftenusedinvolvessimplycountingthenumbersor percentagesof differentkindsof white bloodcells intheperipheralblood.Thewhite bloodcellsrelevantto this chapterareneutro-phils, monocytes,and lymphocytes,including naturalkiller (NK), T, and Blymphocytes. Quantifying the numberof circulating cells is important bothbecausethe body cannotrespondadequatelyto antigenicresponsewithout aminimumnumberof eachtypeof immunecell andbecauseanoptimal responserequiresa balanceof the variouscell types.Both increasesanddecreasesinnumbersof circulatingcellssuggestalterationsin theimmunesystem.However,thechangesfoundin thePNI literatureareusuallyquitesmall,andwhetherthesechanges indicatecompromised immune functionis theoretically unclear.
FUNCTIONAL TESTS Immuneresponsecanbedivided into cellular immunity,in which immune cells directly combatantigens,and humoral immunity, inwhich products ofimmunecells (e.g.antibody) combat antigens. Althoughthecellularandhumoralsubsystemsworktogetherin manyinstances,thefunctionaltestswe describe primarilyexplore theintegrityof oneor the other.
Lymphocytesarethekeycellscontrolling theimmuneresponse.Theabilityof thesecells to proliferaterapidly in the face of an antigenicchallengeisessentialto anadequateresponse.Lymphocyteproliferationis atestof cellularimmunity thatexamineshow effectively stimulated lymphocytes divide. Lym-phocytesarestimulatedthroughincubationwith substances(mitogens)capa-ble of nonspecifically inducingT or B lymphocytesto divide. It is assumedthat greaterproliferation indicatesmore effective cell function. Commonlyusedmitogensincludephytohemagglutinin(PHA), concanavalinA (Con A),and pokeweed mitogen (PWM).
NK cells may be thought of as serving a survei l lance function; theycan detectandkill damagedor altered(e.g.infectedor cancerous)cells.TheNK cell cytotoxic activity assay, another test of cellular immunity, is usedto determinehow effectively NK cells kill transformedcells. In this assay,immunecells are incubatedwith tumor cells andtumor-cell killing is meas-ured.
The functional testsdescribedup to this point are in vitro tests;cells areremoved fromthe body andtheir functionis studied inthelaboratory.Threeinvivo teststhatassessthefunctionof cells in thelivi ng organismarealsousedin this literature. One, thequantificationof antibodies(Ab) to herpesviruses,isusedto indirectly assesscellular immunecompetence(e.g.Glaser& GottliebStematsky1982).Almost everyonehasbeenexposedto thecommonherpes-viruses.Theseviruses differ from most other known viruses in that afterexposure,theyarepresentin thebodyall of the time, althoughoften in latentstates.When the immunesystemis suppressed,latentvirus replicates.Anti-bodiesare proteinmoleculesproducedby the immunesystemthat havethe
116 COHEN & HERBERT

ability to attachto a specificantigen,mark it for destruction,andpreventitfrom causinginfection.Ab is producedin responseto theherpesviral replica-tion, and the amountof Ab producedfluctuatesin relation to the amountofvirus produced.Hence higher levelsof herpesvirus Ab areinterpreted asindirectevidence of compromised cellularimmunefunction.
A moredirecttestof cellularimmunity is thedelayed-typehypersensitivityresponse.In this test,small amounts ofantigenareintroducedby injection intothe skin. A hypersensitivity responseis one in which swelling and rednessoccurat thesiteof injection. Theinflammationis generatedby thereactionoftheantigenwith antigen-specificT lymphocytes.Inflammation is expectedinresponseto the antigens,andthe largerthe inflammation, the more“compe-tent” thecellularimmunesystemis assumedto be.
Finally, in an in vivo testassessingthecompetenceof thehumoralarmofthe immune system, individuals are inoculated with an antigen, and theamountof Ab producedin responseto that specific antigenis quantified.Depending on thespecific type ofAb, it canbequantifiedfrom eitherblood ormucosalsecretions(e.g. saliva,nasaldischarge).The more Ab producedinresponseto anantigen,themore“competent”thehumoralsystemis assumedto be.
ImmunityandDisease
The immunesystem’s defenseagainstinvading microorganisms is composedof a complex cascadeof events.Moreover, the exact natureof any givenimmuneresponsevarieswith the invadedorganism’s historyof exposure,thetype of antigen,andthe routeof entry into the body.Practically,humanPNIresearchersare limited to assessinga small number of rough markersofimmunefunction rather than anything that resemblesa true estimateof thebody’s ability to resistdisease.For theseandotherreasonsaddressedlater(seethesectionentitled“Do Psychological FactorsInfluenceImmuneSystem–Me-diatedDisease?”),PNI studieswith immune (but not disease)outcomes areinformativeabouttheinterrelationamongbehavior,theCNS,andtheimmunesystem,but do not necessarilyindicatechangesin resistanceto disease.In thesectionsthat follow, we first discussstudieson therelationsbetweenpsycho-logical factorsand immunity, and thenstudiesof the relationsbetweenpsy-chologicalfactorsandtheonsetandprogressionof immunesystem–mediateddisease.Thereviewis limi tedto studiesof thepsychological factorsthathavereceivedthemostattention, including stressfullife events,clinical depression,negativeaffect,socialsupport,and repression/denial.
PSYCHOLOGICAL FACTORSAND DISEASE 117

HOW COULD PSYCHOLOGICALFACTORS INFLUENCEIMMUNITY AND DISEASE?
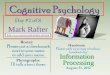
Figure1 presentsa simplified view of how psychological factorsmight alterimmunity anddiseasesusceptibility. As discussedabove,psychologicalvari-ablesmay influence immunity through direct innervation of the CNS andimmunesystemsor throughhormonalpathways.Behavioralchangesthatareassociatedwith personalitycharacteristicsor thatoccurasadaptationsor cop-ing responsesin the faceof stressfuleventsor negativeemotionalstatesmay
Figure 1 Pathwaysthroughwhichpsychological factorsmight influenceonsetandprogressionofimmune system–mediateddisease.For simplicity, arrowsaredrawn in only one direction, frompsychologicalcharacteristics todisease. Nolackof alternative pathsis implied.
118 COHEN & HERBERT

also influenceimmunity. For example,personsexperiencingnegativeaffectoftenengagein poorhealthpractices,suchassmoking,poordietarypractices,and poorsleeping habits (Cohen & Williamson 1988), which may haveimmu-nosuppressiveeffects (Kiecolt-Glaser& Glaser1988).
DO PSYCHOLOGICAL FACTORS INFLUENCEIMMUNITY AND DISEASE?
Stress
Stressful lifeevents arecommonly believed to alter immunity and hencesusceptibility to immunesystem–mediateddisease.When demandsimposedby eventsexceed individuals’ abiliti es to cope,a psychologicalstressresponsecomposedof negativecognitive and emotionalstatesis elicited. It is theseresponsesthatarethought to influenceimmune function throughtheir effectson behavioralcopingand neuroendocrineresponse.
NATURALISTIC STRESSORS In a seriesof studies,Glaser,Kiecolt-Glaser,andcolleaguesinvestigatedtheimpactof medicalschoolexaminationson medicalstudents’ cellularimmunefunction.In thetypicalstudy,students’ psychologicalstress levelsandimmuneresponseswere assessed duringa low-stressbaselineperiod (e.g. just following vacation)and againduring a seriesof importantexams.Studentsreportedmorestressduringexamsandshoweda decreaseinthe function of a rangeof indicatorsof cellular immuneresponse,includingdecreasedNK activity(Kiecolt-Glaseretal1984,Glaseretal1986),lymphocyteproliferation(Glaseret al 1985b,1987,1993),lymphocyteproductionof thechemicalmessengergammainterferon(Glaseret al 1986,1987),aswell asanincreasein production of antibodyto herpesviruses(Glaseret al 1985a,1987,1991).
In a studyof therole of positive (e.g.accomplishing a goal,experiencingagood interactionwith their bosses)and negative(e.g. losing keys, havingarguments)daily eventsin humoralimmunity, Stoneet al (1994)hadcommu-nity volunteersingesta capsulecontainingan innocuousnovel proteindailyfor 12 weeks.The proteinactedas an antigento which the immune systemrespondedby producingantibody. To evaluatethe role of daily eventsinantibodyproduction,volunteersalso completeddaily diariesand gavedailysalivasamplesthatwereusedto assessamountsof secretoryImmunoglobulinA (sIgA) antibodyproducedin responseto thenovelantigen.Thereportingofmoredesirableeventswasconcurrentlyrelatedto greatersIgA antibodypro-duction, and the reporting of more undesirableeventswas relatedto less.Desirableeventswerealsoassociatedwith increasesin sIgA productionovertwo subsequentdays.Thesedataprovideevidencefor the role of day-to-day
PSYCHOLOGICAL FACTORSAND DISEASE 119

eventsin immuneregulationaswell assuggestthebenefitof positiveeventsinhealthoutcomes.
Two studiesexploredthe impact of perceivedstress on thebody’s ability toproduceantibodies (developimmunity) in responseto the standardseriesofthreehepatitisB vaccinations.Glaseret al (1992)did not find a prospectiverelation between negativeaffect and seroconversion(initial productionofhepatitisB antibodies)in responseto the first injection. They did, however,find that thosewho did not seroconvertwere more stressreactive(reportedmorestressin responseto a subsequentexamperiod)thanthosewho serocon-verted. In contrast,Jabaaijet al (1993) found that greaterperceivedstressassessedafter the secondhepatitisB vaccinationwas associatedwith lessantibodyproduction(amongthosewho seroconverted)in responseto thethirdinjection. It is unclear,however,whetherthesedifferencesin antibodylevelaregreatenoughto influencethe degreeof protectionagainstinfection pro-videdby thevaccination.
Stressfuleventsthat last for a longerterm,e.g.monthsor evenyears,havesimilar potential to influencethe immunesystem. Oneexampleis the setofstudiesassessingstresseffectson residentsof theareasurroundingtheThreeMile Island(TMI) nuclearpowerplant.TMI wasthesiteof a seriousaccidentin 1979,andthedistressamongarearesidentshasremainedhigh (Baumet al1985).Recently,almost10 yearsafter the accident,McKinnon et al (1989)found moreantibodyto herpesvirusesin TMI residentsthan in demographi-cally matchedcontrol-group residents,suggesting lowercellularimmunecom-petence inthe former.
Studieson the impactof the chronicstressassociatedwith caregivingforrelativeswith Alzheimer’s disease(AD) reportmixed results.Kiecolt-Glaseret al (1987b)found that caregivingwasassociatedwith distressandelevatedlevels of herpesvirusantibody.The caregiversdid not differ from the low-stresscontrolgroup,however,in avarietyof healthbehaviorsthoughtto affectcellular immunity. In contrast,in a similar study,Irwin et al (1991)foundnodifferencein NK activity betweencaregiversandcontrols.Finally, Esterling etal (1994b)comparedAD caregivers,former AD caregivers(i.e. thosewhoseAD relativehaddiedat leasttwo yearspreviously),andcontrols.Formerandcurrent caregiversdid not differ from eachother and had poorer NK-cellresponseto stimulatory chemicalsthanthecontrol group.Thesedatasuggestthatpsychological andimmunologicalconsequencesof chronicstressorsmaypersistbeyondthe cessationof theactual stressor.
If stressis reliably associatedwith immune change,can stress-reductioninterventionsprevent that change? The few existing studiesare less thanconvincingin thatregard.However,only oneactuallyaddressedtheeffective-nessof an intervention in the faceof a commonstressfulevent.In this study,medicalstudentsweretrainedin relaxationtechniquesjust prior to first-year
120 COHEN & HERBERT

exams.The interventiondid not influencestress-inducedchangesin cellularimmunefunction (Kiecolt-Glaseret al 1986).In a secondstudyof relaxationtraining in medical students,neither the training nor immune measurementcoincided with a common stressful event (McGrady et al 1992),but re-searchersdid find increasedlymphocyte proliferationin responseto PHA andCon A in the relaxationgroupfollowing the four-weekintervention. Finally,elderlyadultsresidingin ageriatriccarefacility whoweretrainedin relaxationtechniquesshowedimprovedcellular immune response,including increasedNK activity and decreasedlevels of herpesantibody (Kiecolt-Glaseret al1985).Work on relaxationtrainingasa stress-reducinginterventionis incon-clusive.However,the literaturesuggeststhatrelaxationtrainingmaybesuffi-cient to temporarily alter the relation betweenusual backgroundlevels ofstressand immune response,but not sufficient to influence stress-inducedperturbationsin immunity caused by externalstressors.
ACUTE STRESSORS IN THE LABORATORY Severalstudieshave assessedtheeffectsof acute(i.e. lasting5–20minutes)psychological stressors(e.g.speechtask,Stroopcolor word interferencetask,mentalarithmetic) on immunere-sponse.The most consistentimmune changesfollowing stressorexposureincludeincreasedNK andsuppressor/cytotoxic T cell numbersanddecreasedproliferativeresponsesto mitogens,particularlyPHA (e.g.Herbertet al 1994,Manucket al 1991,Naliboff et al 1991,Zakowskiet al 1992).Onestudyhasshownthatimmunechangesin bothcell numbersandfunctioncanbefoundassoonasfive minutesafter theonsetof thestressor(Herbertet al 1994).Mostimmuneparametersreturnto arestinglevelby onehourfollowing thecessationof the stressor(Kiecolt-Glaseret al 1992),althoughsomeevidenceindicatesthatNK activity remainsdepressedfor aslongas48 hours(Sieberetal 1992).Moreover,stress-elicitedimmuneresponsesfoundin thelaboratoryareat leastpartly attributable to a dispositional style of respondingto stress.This issuggested by dataindicating that stress-inducedimmune responses arereliableacrosstime and tasks(Marslandet al 1995).The existenceof dispositionalimmunereactivestylesallowsthepossibility thatgreaterimmunereactivitymayplacepeopleatrisk for stress-elicitedimmunerelateddisease(Boyceetal1995,Cohen& Manuck1995).
Laboratorystudiesare ideal for exploring biologic mechanisms linkingpsychologicalstressto immunechange.For example,Manuck et al (1991)concludedthat individualscharacterizedby high sympathetic nervoussystem(SNS) activation (i.e. large increasesin blood pressure,heartrate,and SNShormonesepinephrineandnorepinephrine)in the faceof acutestressorsalsoshowedthe largestimmune changes.Thosedemonstrating litt le or no sympa-thetic reactivity showedlittle or no change.This result hasbeenreplicatedseveraltimes (Bachenet al 1995,Herbertet al 1994,Zakowskiet al 1992).
PSYCHOLOGICAL FACTORSAND DISEASE 121

The correlations between sympathetic and immune response suggestthatstress-elicitedSNS responsemay drive the immune changes.However,thisevidence ismerely correlationalanddoes notestablisha causal chain.
Two recentexperimentalstudieshaveattemptedto provideevidencethatwould allow a causalinferenceregardingthemediating role of theSNSin therelationbetweenacutestressandimmunechange.Thesestudiesaresimilar toearlierwork in thatpersonsexposedto stressorsarecomparedto thosenot soexposed.However, thesestudiesalso include a secondfactor. Subjectsareadministeredeitherplacebosor pharmacologicalagents that prevent hormonesproducedby the SNSfrom binding to andthereforeinteractingwith immunecells(adrenergicblockers).If theeffectsof stresson cellularimmunefunctionaremediatedby theSNS,the pharmacologicalagentsshouldeffectively elimi-natestress-inducedchangein the immunesystem. In onestudy,Bachenet al(1995)demonstratedthat administeringthe adrenergicblocker labetalolpre-ventedstress-inducedincreasesin NK-cell numberand NK activity andde-creasesin lymphocyteproliferation in responseto mitogen.Benschopet al(1994)havealsoshownthat the adrenergicblockerpropranololpreventsthestress-inducedincrease inNK-cell numberand NK activity. Both studiesthereforesuggestthattheseimmunechangesarecausedby sympathetic activa-tion followingstressorexposure.TheinterpretationthattheSNSis theprimarymediatorof theseeffectsis alsosupportedby studiesthat investigate stress-in-duced immune changes inthe contextof otherkey hormonalsystems involvedin immune regulation.For example,studieshave failed to implicate eithercortisol (Manucket al 1991;Zakowskiet al 1992,1994)or opioids(Naliboffet al 1995)in acutestress-inducedsuppressionof eitherlymphocyteprolifera-tion or NK-cell activity.
Although laboratorystressstudiesprovidevaluableinformation, importantquestionsremainunanswered.For example,to what extentdo acutestressoreffectsfoundin thelaboratorysimulatemorechronicreal-lifestressfulevents,andis laboratoryimmunereactivitya dispositional markerof susceptibility tostress-eliciteddisease(Boyce etal 1995,Cohen& Manuck 1995)?
Affect
Researchon the role of negativeaffect in immune responsehasfocusedonclinical depression.However,recentwork examinesrelationsbetweendiffer-ent affective states,both negativeand positive, and immune responseinhealthypopulations.
DEPRESSIVE DISORDERS Investigation of theimmunologiccorrelatesof clini-cal depressionhasreceivedconsiderableattention.A recentmeta-analysis ofover 40 studies shows thatwhen comparedto healthy controls, clinicallydepressedindividualshaveloweredproliferative responseto PHA, ConA, and
122 COHEN & HERBERT

PWM; loweredNK activity; highernumbersof circulatingwhite blood cells(primarily neutrophilsand monocytes); and lowerednumbersof NK, B, T,helperT, andsuppressor/cytotoxic T cells(Herbert& Cohen1993a).Longitu-dinaldataalsosuggestthatwhenpeoplerecoverfromdepression,decreasedNKactivity isnolongerevident(Irwin etal1992).Therelationsbetweendepressionand immuneoutcomesarestrongestin both older andhospitalizedsamples.However,it remainsunclearwhetherthis is becausethesegroupssuffer frommoreseveredepressionor whetherageor hospitalizationotherwisemoderatethe relationbetweendepressionand immunity.
Although thesefindings are reliable acrossstudiesincludedin the meta-analysis,thereis variability in results.Onereasonfor thevariability is meth-odological:Fewresearchgroupshaveachievedhigh-quality designs.To limitvariability, patientsmustbe assessedwhen they aredrug free, they must becarefully age- and sex-matchedwith comparisonsubjects,and appropriatecontrols mustbeused todeal with the day-to-dayvariability of immuneassays(Schleiferet al 1993).Onestudy,now a classic,that achievedthesegoalsisalsooneof thelargestandmostcarefully controlledstudies of clinicalpopula-tionsto date.Schleiferet al (1989)foundthat,consistentwith themeta-analy-sis, depression was associated with immunosuppression primaril y amongolder patientsand hospitalized patients.
As discussed earlier, relations between depression and immunity maysometimesbeattributableto behavioralfactors.Depressedpersonssleepless,exerciseless,havepoorerdiets,smokemore,andusealcoholandotherdrugsmoreoften thando nondepressedpersons(Gregory& Smeltzer1983,Grun-berg& Baum1985).Although manystudiesnow focuson physically healthy,drug-freesubjects,relationsbetweenhealthbehaviorsanddepressionor im-munity are generallynot assessed.The few studiesthat includedstatisticalcontrolsfor healthpracticessuchasweightandrecentweightloss(Schleiferetal 1989), cigaretteuse, and alcohol consumption (Irwin et al 1987, 1990)suggestthat thesehealthpracticesdo not accountfor alterationsin immunefunctionamongdepressed persons.
MOOD What do we know aboutthe relationbetweennormalfluctuationsinmoodandimmuneresponse?Relativelylitt le. Moreover,moststudiesaddressrelationsbetweennegativemoodstatesandimmunity,with only scatteredworkaddressingtherole of positive moods.A recentmeta-analysisof this literaturesuggeststhat depressedmood in nonclinical samplesis associatedwith de-creasedproliferativeresponsesto mitogensanddecreasedNK activity (Herbert& Cohen1993a).However,the effect sizesareconsiderablysmaller(in fact,abouthalf thesize)thanthosefoundfor clinical depression.Only a handfulofstudiesinvestigaterelationsbetweenanxietyandimmunity.Thesestudiesfound
PSYCHOLOGICAL FACTORSAND DISEASE 123

thatanxiousmoodis associated withdecreased NK activity(Lockeet al1984)anddecreasedproliferativeresponseto bothPHA andConA (Linn etal 1981).
Severalstudiesexaminethe associationsof positive and negativemoodstateswith immune outcomes.For example,a daily diary studyexaminedtherelationsbetweenpositive andnegativemoodstatesandantibodyresponsetoan orallyingestednovel antigen overeightweeks(Stoneet al1987). Antibodylevels were higher on days when respondentsreportedhigh positive moodstatesandlower on dayswhentheyreportedhigh negativemoodstates.Theseresultswerereplicatedin a subsequentstudy that monitoredmoodandanti-bodylevels overa 12-week period (Stoneet al 1994).
In a handfulof experimentalstudies,specificaffectivestateswereinducedin healthy subjectsand the subsequentacuteimmune changeswere docu-mented.For example,Knapp et al (1992) had subjectsrecall positive andnegativeexperiencesto induce“positive” and “negative” mood states.Bothpositiveandnegativemoodswereassociatedwith decreasedproliferativere-sponsesto PHA andincreasednumbers ofneutrophils.Similar immuneeffectsof positive and negativemood were attributedto the fact that all subjectsreportedincreasedlevelsof excitement(arousal)during themoodinductions,regardless of thevalence of themood.
Futtermanet al (1994)usedactorsin a within-subjectsdesignandinducedmood using written scenariosthat depictedfour different emotionalstates:high-arousalpositive, high-arousalnegative,low-arousalpositive, and low-arousalnegative.Although NK activity wasnot associatedwith moodcondi-tion, the proliferative response of lymphocytesto PHA was differentiallysensitiveto moodvalence.That is, proliferationincreasedfollowing positivemoodsand decreased followingnegativemoods.
Thusdifferentmoodsmaybeassociatedwith differentimmuneresponses.Clear interpretationof this work is impededby a lack of consensuson thedimensions in which moodshouldbeclassified.However,existingwork sug-geststhat the dimensions of valenceand arousalmay be importantonesinrelatingmoodsto immunefunction.
InterpersonalRelationships
Substantialevidenceimplicatesinterpersonalrelationshipsin themaintenanceof health (Cohen1988, Houseet al 1988). A seriesof prospectivestudiesshowsthat belonging to a strongsocialnetwork is associatedwith longevity(reviewedby Houseet al 1988) and that perceptionsof availablesupportprotectpersonsfrom the pathogenic effectsof stressfulevents(reviewedbyCohen& Will s 1985).Whatis not clear,however,is theextentto which theseeffectsaremediatedby support-inducedchangesin immunefunction.Recentstudiesof loneliness,separationanddivorce,perceptionsof support,anddis-
124 COHEN & HERBERT

closureof traumatic events havebegun to elucidate theimpactof interpersonalrelationshipson immunity and immune system–mediated illness.
In their studiesof first-year medicalstudents, Kiecolt-Glaserand Glaser(Glaseret al 1985a,Kiecolt-Glaseret al 1984) found that personshigher inself-reportedlonelinesshadlowerNK activity andhigherlevelsof herpesvirusantibody than thosewho describedthemselves as less lonely. In a relatedstudy, lonelier psychiatric inpatients hadpoorerNK cell function and lowerproliferativeresponsesto PHA thandid patientswho reportedlessloneliness(Kiecolt-Glaseret al 1984). Becauselonelinessis generallyassociatedwithpsychologicaldistressand negativeaffect (Peplau& Perlman1982), theserelationsmight be explicable in the sameterms as the effects of negativeemotionsdescribed above.
Thereis substantial evidencethat poorermarital relationsandmarital dis-ruption(separationanddivorce)areassociatedwith poorerhealth(Verbrugge1979).Recentwork hassearchedfor potentialeffectsof marital discordonimmunefunction. Kiecolt-Glaseret al (1987a)found that 16 separatedanddivorced(S/D) womenhadhigherlevelsof herpesantibody, a lower percent-ageof NK cells, andlower lymphocyteproliferativeresponseto PHA andConA thana comparisongroupof 16 marriedwomen.In a similar study,Kiecolt-Glaseret al (1988) found that 32 S/D men reportedhaving more infectiousillnessesandhadhigherlevelsof herpesantibodythantheir 32 marriedcoun-terparts.Finally, a study that categorizednewlywedcoupleson the basisofobservedinteractions(Kiecolt-Glaseret al 1993)foundthat thosewho exhib-ited more negativeor hostile behaviorsshowedgreaterdecreasesover 24hours inNK activity and proliferativeresponseto PHA and ConA.
Perceivedavailability of socialsupporthasalsobeenassociatedwith im-munefunction.A studyof 256 elderlyadults(Thomaset al 1985)found thatbloodsamplesfrom personsreportingtheyhadconfidingrelationshipsprolif-eratedmore in responseto PHA thansamplesfrom thosewithout confidingrelationships. Moreover,this relationwasunchangedby controlling for psy-chologicaldistressandhealthpractices.Similar resultswerefound in a studyof 23 spousesof patientswith cancer(Baronet al 1990).Six differentprovi-sionsof social support(including emotionaland instrumental forms of sup-port) were associatedwith higher NKactivity and betterproliferative responseto PHA (butnot to ConA). Betterimmune response amongsupportedpersonscould not be explainedby greaterdepressionor morenumerousstressfullifeeventsamongthosewith lesssocial support.Glaseret al (1992) found thatmedicalstudentsreportingmoreavailablesocialsupportproducedmoreanti-bodyin responseto a hepatitis Bvaccinationthanthose reporting less support,but two studiesof HIV-positive menwere less successful inestablishingrelationsbetweensocialsupport andimmunity (Goodkin etal 1992,Perryetal1992).However,HIV infectioncompromisesthe immunesystemto a degree
PSYCHOLOGICAL FACTORSAND DISEASE 125

soseverethat therelatively small effectsof socialsupport onimmune functionmightbeundetectable.
Many of the beneficial healtheffects of interpersonal relationships areattributedto receiptor availability of emotional support—someoneto talk toaboutproblems(Cohen& Wills 1985).A relatedliteraturehasexaminedthepotential health benefits associated with persons’ disclosure of traumaticevents.Pennebakerand his colleagues(Pennebaker& Beall 1986) reportedthat collegestudentsinstructedto write about both the emotionsand factsassociatedwith a traumaticeventhad fewer subsequentvisits to the healthcenterthan those instructed to writeaboutemotionsor factsalone.In a follow-up studyof therole the immune systemmight play in thebeneficial processoftraumadisclosure (Pennebakeret al 1988), 50 healthyundergraduateswereassignedto write abouteitherpersonalandtraumaticeventsor trivial topics.Theywrotefor 20 minutesa dayon four consecutivedays.Immunologic datawerecollectedbeforethestudybegan(baseline),at theendof theintervention,andat six-weekandfour-monthfollow-ups.Blood drawnfrom subjectswhowrote abouttraumaticeventswasmoreresponsiveto PHA (but not Con A).Therewerenorelationsbetweendisclosureandalcoholintake,caffeineintake,or exerciseover the courseof the study.In addition, subjectsrevealingtrau-maticeventsmadefewervisits to thehealthcenterin thesix weeksfollowingthe interventionthan did membersof the control group. Unfortunately, thedatado not supportanimmunepathwaybecausethelymphocyteproliferationdatawerenot correlatedwith health-centervisits. This absenceof correlationalsosuggeststhat increasesin healthcentervisits may be driven by psycho-logical influenceson decisionprocessesratherthan by influenceson actualillness(Cohen& Will iamson1991).
Researchon how social-supportinterventionsaffect immune systemfunc-tion in stressedsamplesis in its infancy.Existing studiesprovideonly sugges-tive evidence.Threevisits a weekfor a monthby collegestudentsto geriatric-homeresidentsresultedin no detectableeffectson residents’ cellular immuneresponse(Kiecolt-Glaseret al 1985);nor did an intervention (of unspecifiedlength) that providedemotional supportand information about finding newjobs modify the decreasein lymphocyteproliferation to PHA sufferedby agroupof Swedishwomenwhowereunemployedfor overninemonths (Arnetzetal 1987). However,asix-sessiongroupinterventionwith melanoma patientswasassociatedwith decreasedpsychological distressandincreasedNK activ-ity six monthsaftertheintervention (Fawzyet al 1993).This intervention wasrun by professionalfacilitatorsandincludedsuchelementsasstressmanage-ment training and educationabout cancer.How to designappropriateandeffectivesocialsupportinterventionsis a controversialandasyet unresolvedquestion.Appropriatedesigndependson definitions of socialresourcesto be
126 COHEN & HERBERT

provided,thenatureof thepopulation,thesourceof thesupport,strategiesforstructuringgroupinteraction,andthe durationof the intervention.
Personality
The study of the role of personalityin healthhasa long history (Friedman1990).However,relationsbetweenpersonalitycharacteristicsand immunityhavereceivedlitt le attention. Personalitycharacteristicscorrelatedwith meas-ures of immune statusinclude power motivation (e.g. Jemmott et al 1983,1990),pessimistic style (Kamen-Siegelet al 1991),andrepression(Esterlinget al 1993).We limi t our discussion to repression/denial becauseit hasbeenstudiedin relationboth to immunefunctionandto immunesystem–mediateddisease [acquired immunodeficiencysyndrome(AIDS) andcancer].
Repression/denialrepresentsa copingstrategyagainstthreateninginforma-tion and is characterizedby denial or minimization of distressand negativeemotions.Repressorsreactto stressfulstimuli with higherautonomic arousalthan personsreportinghighanxietyor distress(Weinbergeretal 1979).
Esterling et al (1993) found no associationof repressionwith herpesvirusantibodieswhenrepressionwasoperationalizedin termsof a low score intraitanxietyanda high scorein defensiveness.However,higherscoreson a per-sonality inventoryassessingrepressionwereassociatedwith the suppressionof cellular immunefunctionasindicatedby higherlevelsof herpesvirusanti-bodyin two independentsamples(Esterlingetal 1990,1994a).Theserelationsheldevenaftercontrolling for medicationuseanda rangeof healthpractices.In contrast,Antoni et al (1990) found that gay maleswho wereaboutto betestedfor HIV statuswho scoredhigher ona denialcopingscale had agreaterproliferative responseto PHA. This work suggeststhe possibility of a linkbetween repression/denialand cellularimmuneresponsebutalso suggests thatthe scale usedto measure repression/denialis important.
DO PSYCHOLOGICAL FACTORS INFLUENCE IMMUNESYSTEM–MEDIATED DISEASE?
Invasionof the body by a disease-causingagentis not sufficient causefordisease.Diseaseoccurswhen host defensesare compromisedor unabletorecognizetheforeignmaterial.This is why psychological variablesthat influ-enceimmunity havethe potential to influencethe onsetand progressionofimmunesystem–mediateddiseases.What is lessclearis whetherpsychologi-cally inducedchangesin immunity areof the magnitude or type that wouldalter the ability of the body to fight disease(Cohen& Willi amson1991,Laudenslager1987,O’Leary 1990).Below, we review a selectionof studiesthataddressestherole of psychological factorsin theonsetandprogressionofinfectiousdiseases,autoimmunediseases,andcancer.We limit ourselvespri-
PSYCHOLOGICAL FACTORSAND DISEASE 127

marily to prospectiveor intervention studiesandto studiesin which diseaseoutcomesare biologically verifiedor physiciandocumented.
InfectiousDisease
UPPERRESPIRATORY INFECTIONS (URI) Early prospectivework by Meyer &Haggerty (1962)indicatedthatbothdisruptivedaily events andchronic familystresswereassociatedwith greaterrisk for upperrespiratoryinfections. Similarresultswere reportedby Grahamet al (1986). Measuresof life stresswerecollectedfrom membersof 94familiesbeforeandduringasix-month periodinwhichdiarydataonsubjects’ respiratorysymptomswerecollecteddaily.Illnessepisodeswere validatedby noseand throat cultures.Although high- andlow-stressgroupswerealmostidenticalwith respecttodemographicsandhealthpractices,thehigh-stressgroupsexperiencedmoreverified episodesof illnessand moredays withsymptoms ofrespiratory illness.
In a studyof susceptibility to influenza(Cloveretal 1989),246individualsin 58 familiescompletedinstruments assessingfamily relationshipsandindi-vidual stressfullife eventsprior to thestartof flu season.Stressed(“rigid andchaotic”)familiesshowedgreaterincidenceof diseasethannonstressed(“bal-anced”)families.However,illnesswasnot relatedto individual stressfullifeevents.
Increasedincidence ofURI under stressin thesestudies maybeattributableto stress-inducedincreasesin exposureto infectious agentsrather than tostress-inducedimmunosuppression.For example,personsunderstressoftenseek out others, which increases the probabilityof exposure. Aseries ofstudiesusinga procedurethroughwhich volunteersareintentionally exposedto a virus (viral-challengetrials) providescontrol for exposure.In thesepro-spectivedesigns,psychologicalfactorsareassessedbeforevolunteersarein-tentionally exposedto an upper respiratoryvirus. Whetheror not personsdevelopbiologically verified clinical illnessoverthecourseof 7 to 10 daysofquarantineis thenassessed asthe dependentvariable.
Three recent viral-challenge trialssuggest interestingrelations betweenpsychologicalstress and URIsusceptibility. In a study of 394volunteers(Cohenet al 1991,1993),measuresof stressfullife events,perceivedstress,and negativeaffect all predictedthe probability of developinga cold, withgreaterstress linearly relatedto greaterprobability. TherelationsthatCohen etal reportedwere found consistently acrossfive different URI viruses.More-over, theseresultscould not be explainedby stress-eliciteddifferencesinhealthpracticessuchassmoking andalcoholconsumption or in thenumbersof variouswhite blood cell populations or total (nonspecific)antibodylevels.It is interesting to notethat stressfullife eventspredictedsusceptibility inde-pendentlyof (and througha different biological mechanismthan) perceived
128 COHEN & HERBERT

stressandnegativeaffect. In anotherstudy,Stoneet al (1992)replicatedtherelationbetweenstressfullife eventsandsusceptibility to URI andidentifiedthesamebiological pathwayas inthe workof Cohenet al (1993).Finally, in aviral-challengestudy examiningpredictorsof diseaseseverity (rather thanepisodeonset),Cohenet al (1995a)found that state(but not trait) negativeaffect measuredjust prior to viral exposurewasassociatedwith moreseverecoldsandinfluenzaasmeasuredby the amountof mucusproducedover thecourse of theillness.
In sum,bothstressfullife eventsandpsychologicalstress(perceptionsandnegativeaffect) areassociatedwith increasedsusceptibility to upperrespira-tory infections.Theseeffectsarenot generallyexplicablein termsof stress-elicited changesin health behaviors.However, neither is there any directevidenceyet that increasedsusceptibility is attributableto stress-inducedim-munosuppression.
HERPESVIRUS INFECTIONS Herpesviruses are thought to be responsible forcold sores,genitallesions,infectiousmononucleosis,andmononucleosis syn-dromeanddeafnessin neonates(Kiecolt-Glaser& Glaser1987).Herpesvirusesdiffer from most other knownvirusesin thatafterexposure,theyarepresentinindividuals all the time, althoughoften in latentstates.The cellular immuneresponseplaysa key role both in protectionfrom initial herpesvirusinfectionandin keepinglatentherpesvirusesfrom becomingactive(Glaser& Gotlieb-Stematsky1982). As discussedearlier, one explanationfor the increaseinherpesvirusantibodiesoftenassociatedwith stressfulconditionsis that stresssuppressescellular immune function,which allowsthe latentvirus to becomeactive. Isstress associated with arecurrenceof clinical disease (lesions) afteraperiod ofherpesvirus latency?
In a seriesof studiesof studentnursesconductedin the 1970s,negativemoodsat the beginningof the school year were generallyassociatedwithgreaternumbersof subsequentepisodesof verified oral herpes(Friedmannetal 1977,Katcheret al 1973,Luborskyet al 1976).Similar evidencefor stress-inducedrecurrenceis providedby bothretrospective(e.g.Kemenyet al 1989)andprospective studiesof genitalherpes(Goldmeier & Johnson 1982,McLar-non& Kaloupek1988;seecritiquesin Cohen& Wil liamson1991).A recentstudyof 125 collegestudentsprovidesan eleganttestof the role of stressinherpesrecurrencethroughan examinationof severalspecific causalmodels(Hoon et al 1991).This work indicatesthat stressincreasesvulnerability toillnessin general(nonherpes)andthat it is this increasein nonspecificvulner-ability that resultsin herpesrecurrence.Hoon et al did not addressthephysi-ologicalbasisfor thisvulnerability, butbecause theillnessvulnerability meas-urewasheavily influencedby highly prevalentinfectiousdiseases(coldsandinfluenza), animmunebasisis plausible.
PSYCHOLOGICAL FACTORSAND DISEASE 129

In sum,herpesstudiesgenerallysupporta relationbetweennegativeemo-tional statesand diseaserecurrence.However, the evidenceis not entirelyconsistent,and methodological limi tationswarrantcautiousinterpretation oftheseresults.Moreover,existing work doesnot establishthe extentto whichsuch effects are mediatedthroughimmune or behavioralpathways.
AIDS Not all personsexposedto theHIV virus becomeinfected.After expo-sure,both thenumberof yearsto manifestationof clinical symptoms andtheseverityof illnessatall stagesof AIDS varytremendously. Poornutrition,druguse, repeatedHIV exposure, and otherconcurrentviral infections canallaccelerateHIV diseaseprogression.However, even after thesefactors areaccountedfor, agooddealof variability in responseto thevirus is unexplained.Psychologicalvariablesarethoughtto contribute to hostresistanceto theHIVvirus by altering relevantbehavioralpracticesand hormonal and immuneenvironments(Baum & Nesselhof1988,Kemeny1994,Schneidermanet al1994).
Studiesof therolesof stressandnegativeaffect in theprogressionof HIVinfectionareinconsistent in their conclusions.Buracket al (1993)found thatHIV-positive gay men who were depressedat baselineshowedgreaterde-clines than a nondpressedcontrol group in numbersof T-helper cells (animportantprognostic indicator of HIV) overa subsequentperiodof five years.However,depressionwas not associatedwith either the onsetof AIDS ormortality. In contrast,in anotherstudyof HIV-positivegaymen,Lyketsosetal(1993)foundno associationbetweendepressionandchangesin T-helpercellcounts,AIDS onset,or mortality overa subsequentperiodof eightyears.In arecentstudy (Kemeny et al 1995), HIV-positive men who recently lost anintimatepartnerto AIDS showedanincreasein levelsof animmunemarkerofdiseaseprogression(serumneopterin)as well as a decreasein lymphocyteproliferation in responseto PHA. Neither immunechangewasexplicableintermsof useof recreationaldrugs,alcohol,or smoking. Finally, Kessleret al(1991)did not find correlationsbetweenrecentlossesor stressfullife eventsduring the six monthsprior to baselineandtwo diseaseoutcomes—T-helpercell countandonsetof symptoms associatedwith AIDS over the subsequenttwo to threeyears.All of thesestudiescanbefaultedfor focusingon baselinestressanddepressionaspredictorsof the long-termcourseof disease.Thesevariables arenot stable over time and thereis aneedto examinetriggers closerto thetimeof diseaseonset(Cohen etal 1995b).
Investigations of the role of denial in AIDS areinconsistent. Ironsonet al(1994) studied disease progressionin initially asymptomatic HIV-positivemeninvolved in a behavioralintervention program.Personswho deniedtheirdiagnosisdid poorly on markersof diseaseprogressiononeyearlater (poorerPHA-stimulatedproliferation and greaterdecline in T-helper cells) and re-
130 COHEN & HERBERT

ported more symptoms two years later. Immune function at one year wasassociatedwith symptoms at a two-yearfollow-up, but no direct testof im-munemediation of the associationbetweendenial and symptoms was con-ducted.In contrast,Reedetal (1994)reportedthatHIV-positive gaymenwhorefuseto accepttheir diseaseandits implicationslive ninemonthslongerthanthosewho realisticallyaccept them.
Finally, in a singlestudyof socialsupport(Theorellet al 1995),48 hemo-philiac patientswho wereinfectedwith theHIV virus werefollowed for fiveyears.Those who reportedless accessto emotional supportatbaselineshoweda greaterdeclinein T-helpercellsoverthecourseof thestudythanthosewithstronger support systems. There were no diff erences between groups innumberof symptoms of AIDS or inrates of mortality.
INTERVENTIONS Two studiesinvestigatedthepotentialimpactof stressman-agementinterventionson immune markersof AIDS progression.A studyofmendiagnosedwith HIV infection(Coateset al 1989)foundno differences inT-helpercell numbersor lymphocyte proliferation betweentreatedand un-treatedpatients.In a studyof individuals’ responsesto beingdiagnosedHIVpositive (Antoni et al 1991),thosewho receivedstressmanagementprior tonotification respondedwith a betterimmune status(greaterT-helperandNKcell numbersandgreaterPHA-stimulatedlymphocyte proliferation) thanno-treatmentcontrols.Both of thesestudieshad small samplesizesand shortfollow-ups, and neitherpreselectedparticipantsfor particularvulnerabilities(e.g.depression).Interventionwork is of great theoreticaland practicalimpor-tance and further studies usingvariousproven approaches aswell as improvedmethodologies shouldbe the highestpriority.
Evidence reported aboveis at bestmixedin its supportfor aroleof psycho-logical variablesin the progressionof HIV infections.Investigations of therole of psychological factorsin AIDS, however,posedifficult methodologicalchallenges.Time sinceinfection is usually indeterminable;thereis difficultyin controlling for effectsof medication; and the work publishedto datehaslackedsufficient time-linesfor assessingmortality. Furtherwork attendingtothe stability of the psychological predictors,recognizingthat psychologicalfactorsmay havedifferent influenceson different stagesof disease,and as-sessingalternativeexplanationsfor relationswould be welcome.
Autoimmune Diseases
In autoimmunedisease,thebodybeginsto attackits owncellsandorgans.Theimmune systemproducesantibodies that attack its own tissues (autoanti-bodies),andT lymphocytes fail to discriminateself from nonselfandattacknormalbodytissue(Rabinetal 1989).Autoimmunedisordersincluderheuma-toid arthritis (RA), insulin-dependentdiabetes,lupus,Gravesdisease,inflam-
PSYCHOLOGICAL FACTORSAND DISEASE 131

matoryboweldisease,andmultiple sclerosis.Each isassociatedwith differentorgansandwith somewhatdiffering immuneprocesses.Most of thework ontherole of psychological factorsin autoimmunediseasehasinvolvedpatientswith RA. The primary symptom of RA is inflammation of the joints, andprogressionof thediseaseleadsto erosionof cartilageand finallyto joint-cav-ity destruction.
Numerousclinical observationsand severalretrospectivestudies suggestthat psychologicalfactors,includingstressful lifeevents(Homo-Delarcheetal1991,Rimón etal 1977)andless-supportiveatmospheres(DeVellisetal 1986,Moos& Solomon1964),play a role in theonsetandexacerbationof autoim-munediseases.More impressive are studiesevaluatingthe effectivenessofcognitive-behavioral interventions on RA progression (review in Young1992).Although not all interventionsaresuccessfulin affectingdiseaseout-comes(e.g. Parker et al 1988, Strausset al 1986), many have been.Forexample,Bradleyetal (1987)assignedRA patientsto oneof threegroups.Thefirst was a cognitive-behavioralprogramconsistingof biofeedbacktraining,RA education,relaxationtraining,behavioralgoal setting,anduseof self-re-wards.The secondincluded a social supportcondition consistingof smallgroup meetingswith family membersor friends to discussRA education,currentcopingstrategies,andthe developmentof improvedcopingmethods.The third group was a no-treatmentcontrol. Comparedwith the other twogroups, the patientsassigned to the cognitive-behavioral program showedgreaterreductionsin pain intensity, inflammation, andserumlevelsof rheu-matoid factor (a markerof diseaseprogression)immediately posttreatment.However,these benefits wereno longerevident sixmonths later.O’Leary etal(1988) also useda cognitive-behavioral interventionand compareddiseaseoutcomesof patientsundergoingthe intervention with patientsassignedto acontrolgroupthat receivedonly printedinformation (i.e. a bibliotherapycon-trol). Thetreatmentgroupmetonceeach weekfor two hoursovera five-weekperiod,and assessmentsof diseaseoutcomewere madeimmediately beforeand after the five weeksof intervention. When comparedwith the controlgroup, patientsreceiving the cognitive-behavioralinterventionreportedre-ducedpain,andrheumatologistswho wereblind to patientgroupassignmentfound improved jointconditions amongthesepatients.
Finally, Radojevicet al (1992)conducteda six-week-longintervention andassignedRA patientsto oneof four groups:cognitive-behavioralinterventionwith family support,cognitive-behavioralinterventionalone,educationwithfamily support,or a no-treatmentcontrol group.The family supportcompo-nentof the interventiondiffereddependingon thecondition,althoughin bothgroups family membersattendedthe meetings.In the cognitive-behavioralintervention,family supportconsistedof learninghow RA affectsthe familyenvironmentandhow thefamily canassistthepatientin copingwith painand
132 COHEN & HERBERT

in helpingthe patientto increasehis/herfunctioning. In the educationgroup,patientsreceivedemotionalsupport from family during sessionsand wereencouragedto discussillness-relatedproblemsbetweensessionswith theirfamily members.Regardlessof whether family supportwas available,RApatients in the cognitive-behavioral interventions showedimprovement injoint exam,reducedswelling severity,and fewer swollen joints two monthsafter the intervention, comparedwith the othertwo groups.
At this point it is unclear why someinterventions withRA patientsresultedin improved health and others did not,although possible reasons includedifferencesin patientadherenceto the interventions’ requirements;differingamountsof practiceto maintaingains;or differencesin suchpatientcharac-teristicsas severityof disease,amountof disability, and sex (Young 1992).Moreover,noneof the existingwork directly addresseshow (i.e whetherbymeansof immunechanges,behavioralchanges,etc)psychological factorsalterdisease progression.
Cancer
Cancercomprisesa largeandheterogeneousgroupof diseasescharacterizedby the uncontrolled proliferationof cells. Because the immunesystem isthought to play importantroles in tumor surveillanceand in preventingtheprogressionandmetastaticspreadof tumors, psychologicalfactorsassociatedwith immunity areconsideredpotentialcontributorsto canceronsetandpro-gression(Andersonet al 1994).The immune function emphasizedas a linkbetweenpsychological factorsandcanceris NK activity. The presumedim-portance of NKactivity is based on thecombination of reliable findingsassociatingpsychologic variables with NK activity (Herbert & Cohen1993a,b) andon the association of depressedNK activity andincreasedmetas-tases inanimal models (Gorelik & Herberman 1986).However, differentcancersareverydifferentdiseases,andimmuneandpsychological factorsmayplay a role in some butnot in others(Holland 1990, Rabinet al 1989).Similarly, psychological andimmuneprocessesmay vary at different phasesof tumorgrowth—tumor induction,growth,and metastases(Sklar & Anisman1981).
We reviewedwork suggestingthat both depressedaffect andclinical de-pressionhavebeenassociatedwith changesin immune function (includinglower NK activity). Depressionhasalsoreceivedconsiderableattentionasacontributor to cancer;however,the resultsare not entirely consistent.Thiswork includesprospectiveepidemiological studiesof initially healthypersonsthat predictsubsequentcancerincidenceandmortality aswell asstudiesthatpredict survivalamongdiagnosedcancerpatients.
PSYCHOLOGICAL FACTORSAND DISEASE 133

Evidencefrom prospectiveincidenceandmortality studiesis mixed. In a20-yearfollow-up of 2020 men who completedthe MinnesotaMultiphasicPersonalityInventoryin 1957–1958, thosewith higherdepressionscoreshadtwice therisk of dying of cancer 17(Shekelleetal 1981)and20 years (Perskyet al 1987)later thandid their lessdepressedcounterparts.Theseeffectswerenonspecificto siteor typeof cancerandcouldnot beexplainedby differencesin healthpractices.It is interestingto note that whena formula wasusedtocalculatewhetherpatientswere“clinically depressed”from the self-reportedscale,no relation to cancerwas found (Bieliauskas & Garron1982). Gros-sarth-Maticeket al (1983,1985) found that personswith long-lasting hope-lessnessand depressionwere more likely than those neither hopelessnordepressedto developcancerovera 10-yearfollow-up. This relationwasinde-pendentof a seriesof biological predictorsof diseaseonset.Several10- to20-year prospective studies have failed to find that clinical depression asassessedby self-report depression scalesplaced people atrisk for eithercancerincidenceor cancermortality (Hahn& Petitti 1988,Kaplan& Reynolds1988,Zondermanet al 1989).Depressionhas,however,beenassociatedwith mark-ers of diseaseprogression(Levy et al 1985) andshorter survival amongpatientsdiagnosedwith cancer (e.g. Derogatiset al 1979, Weisman& Worden1975).
Why are existing data inconsistent? Work on the role of depressionincancerincidenceand mortality has focusedon undifferentiatedcancerout-comes,andgreateremphasison specificdiseasetypesandsitesmaybeneces-saryto clarify this literature.Thetemporalinstability of bothdepressiveaffectandclinical depressionandthepossible roleof moreacutedepressiveepisodesin canceronset and progression alsoneed to be recognized(Cohen etal1995b). This requiresrepeatedmeasuresof depressionover the courseoflongitudinal studiesaswell astestingat shorterintervalsbetweendepressionand diseaseonset.
Evidencediscussedaboveaddressedtherole of interpersonalrelationshipsand support in immunity. Among cancerpatients,greateraccessto socialsupporthasbeen associated with better prognostic indicators(Levy et al1985)and longer survival (Funch & Marshall 1983, Weisman & Worden 1975).However,theeffectsof socialsupporton survivalmayoccurfor youngerbutnot for older women(Funch& Marshall 1983),and both diseaseonsetandmortality may be associatedwith social isolation amongwomenbut not men(Reynolds& Kaplan1990).This work is consistentwith otherresearchon therole of social supportand suggeststhat different social structuresand re-sourcesmayhavedifferent implicationsfor differentpopulations,particularlyas defined bygender and age.
Finally, a 15-yearstudysuggeststhat patientswho respondto nonmetas-tatic breastcancerwith afighting spirit or with denial haveless recurrenceand
134 COHEN & HERBERT

longer li ves than patientswith stoic acceptance(fatalism) or helplessre-sponses(Greer 1991). Partial replicationsof this work have beenreported(Dean& Surtees1989,DiClemente& Temoshok1985).Greer(1991)cautionsthat theseresultshavebeenfound in thecontextof breastandcervicalcancerand thatgeneralizationsto other cancers are notwarranted.
Althoughtherearemanyconsistenciesin thesecorrelationalliteratures,asawhole theymustbeviewedin light of severalconcerns andqualifications. Theproblemsassociatedwith cancer(e.g.undetectedpremorbidstates,difficultyin quantifying severityatanystage,differencesin biology of different tumors,difficulty in assessingand controlling for medicationand compliancewithmedicalregimens)makeit difficult (andoften impossible) to designstudiesthat eliminateimportant alternativeexplanations. Correlations may be spuri-ous—i.e.derivedfrom other variablessuchas toxic workplaces,viruses,orchronicinfectionsthat influencebothpsychological characteristicsandcancer(Sklar & Anisman 1981). Moreover,althoughpsychological variablesmayaffect survival, the contribution is relatively small and is overshadowedbybiologicalfactors.Hencepsychological variablesareleastlikely to play a rolein laterandmoreseriousstagesof disease(e.g.Cassilethetal 1985,Jamison etal 1987).
INTERVENTIONS Tworecentinterventionstudiesprovidethemostprovocativeandconvincing evidencefor a role of psychologicalfactorsin cancerprogres-sion.In one(Fawzyetal1993),66malignant-melanomapatientswererandomlyassignedto eitheraninterventionorano-treatmentcontrolgroup.Theinterven-tioncombinededucation,stressmanagement,copingskills,anddiscussionwithpatientsandfacilitatorsandconsisted of six 90-minutesessions.Six monthsafter the intervention ended,participantsin the intervention group showedreducedpsychologic distress, enhanced immune function(increasedNK activ-ity), andchangesin immunecell counts(decreasedT cells,increasedlympho-cytes)whencomparedwith patients inthecontrolgroup.Theinterventionalsodecreasedrecurrence and increased survivalas assessedsix yearslater. Altera-tions in immuneoutcomes,however,did not explainthe intervention’s effecton mortality. In the other interventionstudy(Spiegelet al 1989),58 patientswith metastaticbreastcancer wererandomlyassignedto eitheran interventionorano-treatmentcontrolgroup.Theinterventionconsistedof weekly90-minutemeetings forone year. The highly structuredmeeting focusedon variousproblemsassociatedwith terminalillnessandonwaysto improverelationships.Tenyearslater,therewasan18-monthsurvivaladvantageassociatedwith theintervention.No immunemeasures wereassessed. Thesestudiesareconceptu-ally importantbecausetheyareexperimentaldemonstrationsof thesignificanceof psychologicalfactors,andtheyarepracticallyimportantbecausetheysuggesta significantrole for psychologicalinterventionsin cancersurvival.Ongoing
PSYCHOLOGICAL FACTORSAND DISEASE 135

attemptsto replicateandextendthiswork will helpusevaluatetheirvalidity aswell asidentify behavioralandimmunemechanismsresponsiblefor reportedoutcomes.
CONCLUSIONS
The literaturediscussedin this chapteris in manyways impressive.First, itprovidespsychologically andbiologically plausible explanations for how psy-chological factorsmight influence immunity and immune system–mediateddisease.Second,it providessubstantial evidencethatpsychological factorscaninfluencebothcellularandhumoralindicators of immunestatusandfunction.Third, at leastin the caseof the lessseriousinfectiousdiseases(colds,influ-enza,herpes),it includesconsistentandconvincingevidenceof links betweenstressanddiseaseonsetandprogression.Although still early in its develop-ment, researchon autoimmune diseases(at least on RA) also suggeststhepotentialrole of psychological factors.Evidencefor effectsof psychologicalfactorson AIDS andcanceris lessconsistentandinconclusive.This may bebecauseof methodological limitations inherentin studying thesecomplexillnesses,or it maybebecausepsychological influenceson immunity arejustnot of the magnitudeor type necessaryto alter the body’s responsein thesecases.Furtherdevelopmentandevaluationof psychosocial interventionsmaybethebestapproachfor providing evidencethatallowsclearcausalinferenceandat the sametime hasclinical implications.What is missing in this litera-ture,however,is strongevidencethat theassociationsbetweenpsychologicalfactorsanddiseasethatdo existareattributableto immunechanges.Many ofthe relationsreportedin this chaptermay be attributable to psychologicallyinducedchangesin healthbehaviors(e.g.healthpracticessuchassmokingandalcohol consumption, or degreeof adherenceto medical regimens);bettermeasurementandcontrolof thesevariablesareessential.Moreover,theinclu-sion in future studiesof immune measuresbasedon the role of the immunesystemin the specific diseaseunderstudy may help provide evidencefor adirect linkamongpsychological factors,immunity, anddisease.
ACKNOWLEDGMENTS
Drs. CohenandHerbert’s contributionsweresupportedby a ResearchScien-tist DevelopmentAward (K02MH00721)and a grant (MH50430) from theNational Institute of Mental Health, respectively.We are indebtedto Drs.AndrewBaum,BruceRabin,andMario Rodriguezfor their commentson anearlierdraft andto JanetSchlarbandSusanKravitz for their aid in preparingthe chapter.
136 COHEN & HERBERT

Any Annual Reviewchapter, aswell asany arti clecited in an Annual Reviewchapter,may bepurchased fromthe Annual ReviewsPreprints and Reprints service.
1-800-347-8007; 415-259-5017; email: [email protected]
LiteratureCited
Ader R, Cohen N. 1993. Psychoneuroimmu-nology: conditioning andstress.Annu. Rev.Psychol. 44:53–85
Anderson BL, Kiecolt-Glaser JK, Glaser R.1994. A biobehavioral model of cancerstressanddiseasecourse.Am.Psychol. 49:389–404
Antoni MH, August S, LaPerriereA, BaggettHL, Kli masN, et al. 1990. Psychologicaland neuroendocrine measures related tofunctional immune changesin anticipationof HIV-1 serostatus noti f ication. Psy-chosom.Med.52:496–510
Antoni MH, Baggett HL, Ironson G, LaPerri-ereA, AugustS, et al. 1991. Cognitive-be-havioral stress management interventionbuf fers distress responses and immu-nologic changes following notification ofHIV-1 seropositivity. J. Consult. Clin. Psy-chol. 59:906–15
Arnetz BB, WassermanJ, Petrini B, BrennerS-O,Levi L, et al. 1987. Immune functionin unemployed women. Psychosom. Med.49:3–12
Bachen EA, Manuck SB, Cohen S, MuldoonMF, Raible R, et al. 1995. Adrenergicblockage ameliorates cellular immune re-sponsesto mental stressin humans.Psy-chosom.Med.In press
Baron RS, Cutrona CE, Hicklin D, RussellDW, Lubaroff DM. 1990. Social supportand immunefunction among spousesofcancerpatients. J. Pers.Soc. Psychol. 59:344–52
Baum A, Nesselhof EA. 1988. Psychologi-cal researchand the prevention, etiology,and treatment of AIDS. Am. Psychol. 43:900–6
Baum A, Schaeffer MA, LakeCR,Fleming R,CollinsDL. 1985. Psychological and endo-crinological correlatesof chronic stressatThreeMile Island. In Perspectiveson Be-havioral Medicine, ed. R Wi l l i ams,2:201–17. SanDiego: Academic
Benschop RJ, Nieuwenhuis EES, TrompEAM, Godaert GLR, Baili eux RE, vanDoornen LJP. 1994. Effects of ß-adrener-gic blockadeon immunologic and cardio-vascular changesinducedby mental stress.Circulation89:762–69
BieliauskasLA, Garron DC. 1982. Psychologi-cal depressionandcancer.Gen.Hosp. Psy-chiatr. 4:187–95
Bovbjerg DH, Redd WH, Maier LA, HollandJC, Lesko LM, et al. 1990. Anticipatory
immune suppression andnauseain womenreceiving cyclic chemotherapyfor ovariancancer. J. Consult. Clin. Psychol. 58:153–57
Boyce WT, ChesneyM, Alkon A, TschannJM, AdamsS, et al. 1995. Psychobiologicreactivity to stressand childhood respira-tory il lnesses.Psychosom.Med.In press
Bradley LA, YoungLD, AndersonKO, TurnerRA, Agudelo CA, et al. 1987. Effects ofpsychological therapyon pain behavior ofrheumatoid arthritis patients: treatmentout-come and six-month followup. Arthrit isRheum.30:1105–14
Burack JH, Barrett DC, Stall RD, ChesneyMA, Ekstrand ML, CoatesTJ. 1993. De-pressivesymptoms and CD4 lymphocytedecline among HIV-i nfected men. J. Am.Med.Assoc.270:2568–73
Buske-Kirschbaum A, Kirschbaum C, StierleH, Lehnert H, HellhammerD. 1992. Con-ditionedincreaseof naturalkillercell activ-ity (NKCA) in humans.Psychosom.Med.54:123–32
CassilethBR, Lusk EJ,Mil ler DS, Brown LL,Mi ller C. 1985. Psychosocial correlatesofsurvival in advancedmalignantdisease.N.Engl. J. Med.312:1551–55
Clover RD, Abell T, BeckerLA, Crawford S,Ramsey JCN. 1989. Family functioningandstressas predictors of influenza B in-fection. J. Fam.Pract. 28:535–39
CoatesTJ, McKusick L, Kuno R, Stites DP.1989. Stress reduction training changednumberof sexualpartners but not immunefunction in men with HIV. Am. J. PublicHealth 79:885–87
Cohen S. 1988. Psychosocial models of therole of social support in the etiology ofphysicaldisease.Health Psychol. 7:269–97
Cohen S, Doyle WJ, Skoner DP, FiremanP,GwaltneyJM Jr, NewsomJT. 1995a. Stateand trait negative affect as predictors ofobjective andsubjective symptoms of res-piratory viral infections. J. Pers.Soc. Psy-chol. 68:159–69
CohenS,Kessler RC, Underwood Gordon LG.1995b. Strategies for measuring stressinstudies of psychiatric and physical disor-ders. In Measuring Stress: A Guide forHealth and Social Scientists,ed. S Cohen,RC Kessler, L Underwood Gordon, pp.3–26. NewYork: Oxford
CohenS, Manuck SB. 1995. Stress,reactivityanddisease. Psychosom.Med.In press
PSYCHOLOGICAL FACTORSAND DISEASE 137

Cohen S, Tyrrel l DAJ, Smith AP. 1991.Psychological stressand susceptibil ity tothe common cold. N. Engl. J. Med. 325:606–12
CohenS, Tyrrell DAJ, Smith AP. 1993. Nega-tive li fe events, perceived stress,negativeaffect, and susceptibil ity to the commoncold. J. Pers.Soc. Psychol. 64:131–40
Cohen S, Williamson GM. 1988. Perceivedstressin a probability sampleof the UnitedStates.In The Social Psychologyof Health,ed. S Spacapan, S Oskamp, pp. 31–67.Newbury, CA: Sage
Cohen S, Will iamsonGM. 1991. Stressandinfectious disease in humans. Psychol.Bull. 109:5–24
Cohen S, Wills TA. 1985. Stress,social sup-port, andthebufferinghypothesis.Psychol.Bull. 2:310–57
DeanC, SurteesPG. 1989. Do psychologicalfactors predict survival in breastcancer?J.Psychosom.Res.33:561–69
Derogatis LR, Abeloff MD, Melisaratos N.1979. Psychological coping mechanismsandsurvival time in metastatic breastcan-cer.J. Am.Med.Assoc.242:1504–8
DeVellis RF, DeVellis B, McEvoy H, SauterSV, Harring K, Cohen JL. 1986. Predictorsof pain andfunctioning in arthritis. HealthEduc. Res.:Theory Pract. 1:61–67
DiClemente RJ, Temoshok L. 1985. Psycho-logicaladjustment to having cutaneous ma-lignantmelanomaasa predictor of follow-up clinical status. Psychosom.Med. 47:81(Abstr.)
Esterling BA, Antoni MH, FletcherMA, Mar-gulies S, SchneidermanN. 1994a. Emo-tional disclosure through writing or speak-ing modulateslatentEpstein-Barr virus an-tibody titers.J. Consult. Clin. Psychol. 62:130–40
Ester l i ng BA , A ntoni M H, K umar M ,SchneidermanN. 1990. Emotional repres-sion, stressdisclosure responses,and Ep-stein-Barr viral capsidantigen titers. Psy-chosom.Med.52:397–410
Ester l i ng BA , A ntoni M H, K umar M ,Schneiderman N. 1993. Defensiveness,trait anxiety, andEpstein-Barr viruscapsidantigen antibody titers in healthy collegestudents.Health Psychol. 12:132–39
Esterling BA, Kiecolt-GlaserJK, Bodnar JC,Glaser R. 1994b. Chronic stress, socialsupport, and persistent alterations in thenatural killer cell responseto cytokines inolderadults.Health Psychol. 13:291–98
FawzyFI, FawzyNW, Hyun CS, ElashoffR,Guthrie D, et al. 1993. Malignant mela-noma: effectsof anearlystructuredpsychi-atric intervention, coping, and aff ectivestateon recurrence and survival six yearslater. Arch.Gen.Psychiatr. 50:681–89
FeltenDL, FeltenSY, CarlsonSL, OlschowkaJA, Livnat S. 1985. Noradrenergic sympa-
thetic innervationof lymphoid tissue.J. Im-munol. 135:755S–65S
Friedmann E, Katcher AH, Brightman VJ.1977. Incidenceof recurrentherpeslabialisandupper respiratory infection: a prospec-tive study of the influenceof biologic, so-cial andpsychologic predictors.Oral Surg.Oral Med.Oral Pathol. 43:873–78
FriedmanHS. 1990. Personality and Disease.NewYork: Wiley
FunchDP,Marshall J. 1983. The role of stress,social support and agein survival frombreastcancer.J. Psychosom.Res.27:77–83
FuttermanAD, KemenyME, Shapiro D, FaheyJL. 1994. Immunologicalandphysiologicalchanges associated with induced positiveand negative mood. Psychosom.Med. 56:499–511
GlaserR, Gottlieb-StematskyTE. 1982. Hu-man Herpesvirus Infections: Clinical As-pects.New York: MarcelDekker
Glaser R, Kiecolt-Glaser JK, Bonneau RH,MalarkeyW, Kennedy S, HughesJ. 1992.Stress-inducedmodulation of immune re-sponseto recombinanthepatitis B vaccine.Psychosom.Med.54:22–29
Glaser R, Kiecolt-Glaser JK, Speicher CE,Holliday JE.1985a. Stress,loneliness,andchanges in herpesvirus latency. J. Behav.Med.8:249–60
Glaser R, Kiecolt-Glaser JK, Stout JC, TarrKL, Speicher CE, Holl iday JE. 1985b.Stress-relatedimpairments in cellular im-munity. Psychiatr. Res.16:233–39
GlaserR, PearsonGR,BonneauRH, EsterlingBA, AtkinsonC, Kiecolt-GlaserJK. 1993.Stressand the memory T-cell responsetothe Epstein-Barr virus in healthy medicalstudents.Health Psychol. 12:435–42
GlaserR, PearsonGR, JonesJF, Hil lhouse J,KennedyS, et al. 1991. Stress-relatedacti-vation of Epstein-Barr virus. Brain Behav.Immun. 5:219–32
GlaserR, Rice J, Sheridan J, Fertel R, StoutJC,et al. 1987. Stress-relatedimmunesup-pression: health implications. Brain Behav.Immun. 1:7–20
GlaserR, Rice J, SpeicherCE, Stout JC,Kie-colt-GlaserJK. 1986. Stressdepressesin-terferon production by leukocytes con-comitant with a decreasein natural killercell activity. Behav. Neurosci.100:675–78
GoldmeierD, JohnsonA. 1982. Doespsychiat-ric il lness affectthe recurrencerateof geni-tal herpes?Br. J. Vener.Dis. 54:40–43
Goodkin K, Blaney NT, FeasterD, FletcherMA, Baum A, et al. 1992. Active copingstyle is associated with natural killer cellcytotoxicity in asymptomatic HIV-1 sero-positive homosexual men. J. Psychosom.Res.36:635–50
Gorelik E, HerbermanR. 1986. The role ofnatural killer “NK” cells in the control oftumor growth and metastatic spread. In
138 COHEN & HERBERT

Cancer Immunology: Innovative Ap-proachesto Therapy,ed.R Herberman, pp.151–76. Boston: Martinez Nijhoff
GrahamNMH, Douglas RB,Ryan P. 1986.Stressandacute respiratory infection. Am.J. Epidemiol. 124:389–401
GreerS. 1991. Psychological responseto can-cer andsurvival. Psychol. Med.21:43–49
Gregory MD, SmeltzerMA. 1983. Psychiatry:Essentials of Clinical Practice. Boston:Lit tle,Brown
Grossarth-MaticekR, KanazirDT, Schmidt P,Vetter H. 1985. Psychosocial and organicvariablesaspredictors of lung cancer,car-diacinfarctandapoplexy: somedifferentialpredictors.Pers. Individ. Differ. 6:313–21
Grossarth-Maticek R, Kanazir DT, Vetter H,Schmidt P.1983. Psychosomatic factors in-volved in the processof cancerogenesis.Psychother.Psychosom.40:191–210
GrunbergNE, Baum A.1985. Biological com-monalities ofstressandsubstanceabuse.InCoping and Substance Use, ed. S Shiff -man, TA Wills, pp. 25–62. San Diego:Academic
Hahn RC, Petitti DB. 1988. Minnesota Mul-tiphasic Personalit y Inventory–rated de-pression andthe incidenceof breastcancer.Cancer61:845–48
Herbert TB, Cohen S. 1993a. Depression andimmunity: ameta-analytic review.Psychol.Bull. 113:472–86
Herbert TB, CohenS.1993b. Stressandimmu-nity in humans: a meta-analytic review.Psychosom.Med.55:364–79
Herbert TB, Cohen S, Marsland AL, BachenEA, Rabin BS, et al. 1994. Cardiovascularreactivity and thecourse of immune re-sponse to an acutepsychological stressor.Psychosom.Med.56:337–44
Holland JC. 1990. Behavioral and psychoso-cial risk factors in cancer:humanstudies.In Handbook of Psychooncology—Psycho-logical Careof thePatientwith Cancer,ed.JCHolland, JH Rowland, pp. 705–26. NY:Oxford Univ. Press
Homo-DelarcheF, Fitzpatrick F, Christeff N,Nunez EA, Bach JF, Dardenne M. 1991.Sex steroids, glucocorticoids, stress andautoimmunity. J. Steroid Biochem.Molec.Biol. 40:619–37
Hoon EF, Hoon PW, Rand KH, Johnson J,Hall NR, EdwardsNB. 1991. A psycho-be-havioral model of genital herpes recur-rence.J. Psychosom.Res.35:25–36
HouseJS,Landis KR, Umberson D. 1988. So-cial relationships and health. Science241:540–45
Ironson G, FriedmanA, Kli masN, Antoni M,Fletcher MA, et al. 1994. Distress,denialand low adherenceto behavioral interven-tions predict fasterdiseaseprogressioningaymeninfectedwith humanimmunodefi-ciencyvirus.Int. J. Behav. Med.1:90–105
Irwin M, Brown M, PattersonT, Hauger R,Mascovich A, GrantI. 1991. NeuropeptideY andnaturalkillercell activity: findings indepressionandAlzheimercaregiver stress.FASEBJ. 5:3100–7
Irwin M, Lacher U, Caldwell C. 1992. Depres-sion andreducednaturalkillercytotoxicity:a longitudinal study of depressedpatientsand control subjects. Psychol. Med. 22:1045–50
Irwin M, PattersonT, Smith TL, Caldwell C,Brown SA, et al. 1990. Reduction of im-mune function in li fe stress anddepression.Biol. Psychiatr. 27:22–30
Irwin M, Smith TL, Gillin JC.1987. Low natu-ral killer cytotoxicity in major depression.LifeSci.41:2127–33
Jabaai j L , Grosheide PM, Hei j tink RA,Duivenvoorden HJ, Ballieux RE, Vinger-hoets AJJM. 1993. Influenceof perceivedpsychological stressand distresson anti-body responseto low doserDNA hepatitisB vaccine.J. Psychosom.Res.37:361–69
JamisonRN, Burish TG, Wallston KA. 1987.Psychogenic factors in predicting survivalof breastcancerpatients. J. Clin. Oncol.5:768–72
JemmottJB III, Borysenko JZ, Borysenko M,McClelland DC, ChapmanR, et al. 1983.Academic stress, power motivation, anddecreasein secretion rateof salivary secre-tory immunoglobulin A. LancetI:1400–2
JemmottJB III, Hellman C, Locke SE, KrausL, Wil liamsRM, Valeri CR. 1990. Motiva-tional syndromes associated with naturalki l ler cell activity. J. Behav. Med. 13:53–73
Kamen-Siegel L, Rodin J, Seligman MEP,Dwyer J. 1991. Explanatory style andcell-mediated immunity in elderly men andwomen. Health Psychol. 10:229–35
KaplanGA, ReynoldsP.1988. Depression andcancermortality and morbidity: prospec-tive evidence from the Alameda Countystudy. J. Behav.Med.11:1–13
KatcherAH, BrightmanVJ, Luborsky L, ShipI. 1973. Prediction of the incidenceof re-current herpeslabialis andsystemic il lnessfrom psychological measures.J. Dent. Res.52:49–58
KemenyME. 1994. Stressfulevents, psycho-logical responses,andprogressionof HIVinfection. In Handbook of Human Stressand Immunity, ed. R Glaser, J Kiecolt-Glaser,pp. 245–66. New York: Academic
KemenyME, CohenF, ZegensL. 1989. Psy-chological and immunological predictorsof genital herpes recurrence.Psychosom.Med.51:195–208
KemenyME, Weiner H, DuranR, Taylor SE,VisscherB, Fahey JL. 1995. Immune sys-temchangesfollowing the death of a part-ner in HIV positive gay men.Psychosom.Med.In press
PSYCHOLOGICAL FACTORSAND DISEASE 139

Kessler RC, Foster C, Joseph J, Ostrow D,Wortman C, et al. 1991. Stressful lif eevents and symptom onset in HIV infec-tion. Am.J. Psychiatr. 148:733–38
Kiecolt-Glaser JK, Cacioppo JT, MalarkeyWB, GlaserR. 1992. Acute psychologicalstressorsand short-term immune changes:what,why, for whom, andto whatextent?Psychosom.Med.54:680–85
Kiecolt-Glaser JK, Fisher LD, Ogrocki P,Stout JC, Speicher CE, GlaserR. 1987a.Marital quality, marital disruption, andim-mune function. Psychosom.Med.49:13–34
Kiecolt-Glaser JK, Garner W, Speicher CE,PennGM, HollidayJ, Glaser R.1984. Psy-chosocial modifi ersof immunocompetencein medical students. Psychosom.Med. 46:7–14
Kiecolt-GlaserJK, GlaserR. 1987. Psychoso-cial influenceson herpes virus latency. InViruses,Immunity and Mental Disorders,ed.E Kurstak,ZJ Lipowski, PV Morozov,pp. 403–11. New York: Plenum
Kiecolt-GlaserJK, GlaserR. 1988. Methodo-logical issues in behavioral immunologyresearchwith humans.Brain Behav. Im-mun. 2:67–68
Kiecolt-GlaserJK, GlaserR, Shuttleworth EC,Dyer CS,Ogrocki P, SpeicherCE. 1987b.Chronic stress and immunity in famil ycaregiversof Alzheimer’s diseasevictims.Psychosom.Med.49:523–35
Kiecolt-GlaserJK, GlaserR, Strain E, Stout J,Tarr K, et al. 1986. Modulation of cellularimmunity in medical students. J. Behav.Med.9:5–21
Kiecolt-GlaserJK, GlaserR, Will iger D, StoutJ, MessickG, et al. 1985. Psychosocial en-hancement of immunocompetence in ageriatric population. Health Psychol. 4:25–41
Kiecolt-Glaser JK, Kennedy S, Malkoff S,Fisher L, Speicher CE, Glaser R. 1988.Marital discord and immunityin males.Psychosom.Med.50:213–29
Kiecolt-Glaser JK, Malarkey WB, Chee M,Newton T,Cacioppo JT,et al. 1993. Nega-tive behavior during marital conflict is as-sociatedwith immunological down-regula-tion. Psychosom.Med.55:395–409
Knapp PH, Levy EM, Giorgi RG, Black PH,Fox BH, HeerenTC. 1992. Short-termim-munological effects of induced emotion.Psychosom.Med.54:133–48
Laudenslager ML. 1987. Psychosocial stressand susceptibil ity to infectious disease.InViruses,Immunity and Mental Disorders,ed.E Kurstak,ZJ Lipowski, PV Morozov,pp. 391–402. New York: Plenum
Levy S, HerbermanR, Maluish A, Schliew B,LippmanM. 1985. Prognostic risk assess-ment in primary breastcancerby behav-ioral and immunological parameters.Health Psychol. 4:99–113
Linn BS, Linn MW, JensenJ. 1981. Anxietyandimmune responsiveness.Psychol. Rep.49:969–70
Locke SE, Kraus L, LesermanJ, Hurst MW,HeiselJS,Will iamsRM. 1984. Li fe changestress,psychiatric symptoms, and naturalkiller cell activity. Psychosom. Med. 46:441–53
Luborsky L, Mintz J, Brightman VJ, KatcherAH. 1976. Herpes simplex virus andmoods:a longitudinal study. J. Psychosom.Res.20:543–48
Lyketsos CG, Hoover DR, Guccione M, Sen-terfitt W, Dew MA,et al.1993. Depressivesymptoms as predictors of medical out-comesin HIV infection. J. Am. Med. As-soc.270:2563–67
Manuck SB, Cohen S, RabinBS, MuldoonMF, BachenEA. 1991. Individual differ-ences in cel lular immune response tostress.Psychol. Sci. 2:111–15
Marsland AL, Manuck SB, FazzariTV, Stew-ard CJ, Rabin BS. 1995. Stabili ty of indi-vidual differences in cellular immune re-sponsesto acute psychological stress.Psy-chosom.Med.57:295–98
McGradyA, ConranP, Dickey D, GarmanD,Farris E, Schumann-Brzezinski C. 1992.Theeffectsof biofeedback-assistedrelaxa-tion on cell mediated immunity, cortisol,andwhite blood cell count in healthy adultsubjects.J. Behav. Med.15:343–54
McKinnon W, Weisse CS, Reynolds CP,BowlesCA, BaumA. 1989. Chronic stress,leukocyte subpopulations, andhumoral re-sponse to latent viruses.Health Psychol.8:389–402
McLarnon LD, Kaloupek DG. 1988. Psycho-logical investigation of genital herpes re-currence: prospective assessmentandcog-nitive-behavioral intervention for a chronicphysical disorder. Health Psychol. 7:231–49
Meyer RJ, Haggerty RJ. 1962. Streptococcalinfections in fami l ies. Pediatrics 29:539–49
Moos RH,Solomon GF.1964. Personality cor-relates of the rapidity of progression ofrheumatoid arthritis. Ann. Rheum. Dis. 23:145–51
Naliboff BD, Benton D, SolomonGF, MorleyJE, Fahey JL, et al. 1991. Immunologicalchanges in young and old adults duringbrief laboratory stress.Psychosom. Med.53:121–32
Naliboff BD, Solomon GF, Gilmore SL, Ben-ton D, Morley JE, FaheyJL. 1995. Theeffectsof theopiateantagonistnaloxoneonmeasuresof cellular immunity during restand brief psychological stress. J. Psy-chosom.Res.In press
O’Leary A. 1990. Stress,emotion, andhumanimmune function. Psychol. Bull. 108:363–82
140 COHEN & HERBERT

O’Leary A, Shoor S, Lorig K, Holman HR.1988. A cognitive-behavioral treatmentforrheumatoid arthriti s. Health Psychol. 7:527–44
Parker JC, Frank RG, Beck NC, Smarr KL,Buescher KL, et al. 1988. Pain manage-ment in rheumatoid arthriti s patients: acognitive-behavioral approach. Arthrit isRheum.31:593–601
PennebakerJW,BeallSK. 1986. Confronting atraumatic event: toward an understandingof inhibition anddisease.J. Abnorm. Psy-chol. 95:274–81
Pennebaker JW, Kiecolt-GlaserJK, GlaserR.1988. Disclosuresof traumasandimmunefunction: health implications for psycho-therapy. J. Consult. Clin. Psychol. 56:239–45
PeplauLA, PerlmanD, eds.1982. Loneliness:A Source Book of Current Theory, Re-search,and Therapy.New York: Wiley
PerryS, FishmanB, JacobsbergL, FrancesA.1992. Relationships over 1 year betweenlymphocyte subsetsandpsychosocialvari-ablesamong adults with infection by hu-man immunodeficiency virus. Arch. Gen.Psychiatr. 49:396–401
PerskyVW, Kempthorne-RawsonJ, ShekelleRB. 1987. Personality and risk of cancer:20-year follow-up of the Western ElectricStudy. Psychosom.Med.49:435–49
Rabin BS, Cohen S, Ganguli R, Lysle DT,Cunnick JE. 1989. Bidirectional interactionbetween the central nervous system andimmune system. Crit. Rev. Immunol. 9:279–312
Radojevic V, Nicassio PM, Weisman MH.1992. Behavioral intervention with andwithout family support for rheumatoid ar-thritis. Behav. Ther.23:13–30
ReedGM, KemenyME, Taylor SE,Wang HJ,Visscher BR. 1994. Realistic acceptance asa predictor of decreasedsurvival time ingay men with AIDS. Health Psychol. 13:299–307
Reynolds P, KaplanGA. 1990. Social connec-tions and risk for cancer:prospective evi-dencefrom theAlamedaCounty study. Be-hav. Med.16:101–10
RimónR, Belmaker RH,EbsteinR. 1977. Psy-chosomatic aspectsof juvenile rheumatoidarthritis. Scand. J. Rheum.6:1–10
Schleifer SJ, Eckholdt HM, Cohen J, KellerSE. 1993. Analysis of partial variance(APV) as a statistical approachto controlday to day variation in immune assays.Brain Behav. Immun. 7:243–52
Schleifer SJ, Keller SE, Bond RN, Cohen J,Stein M. 1989. Major depressive disorderand immunity: role of age,sex, severity,andhospitalization. Arch. Gen.Psychiatry46:81–87
SchneidermanN, Antoni M, Ironson G, Kli -masN, LaPerriere A, et al. 1994. HIV-1,
immunity, and behavior. In Handbook ofHuman Stressand Immunity, ed.R Glaser,J Kiecolt-Glaser,pp. 267–300. New York:Academic
Shavit Y, Lewis JW, TermanGW, Gale RP,Liebesking JC. 1984. Opioid peptidesme-diate the suppressive effect of stressonnaturalkillercell cytotoxicity. Science223:188
Shekelle RB, Raynor WJ Jr,Ostfeld AM, Gar-ron DC, BieliauskasLA, et al. 1981. Psy-chological depression and seventeen-yearrisk of death from cancer. Psychosom.Med.43:117–25
Sieber WJ,Rodin J,Larson L, Ortega S,Cum-mings N, et al.1992. Modulation of humannatural killer cell activity by exposure touncontrollable stress.Brain Behav. Immun.6:141–56
Sklar LS,Anisman H. 1981. Stressandcancer.Psychol. Bull. 89:369–406
Smith AP, Tyrrell DAJ, Al-Nakib W, CoyleKB, Donovan CB, et al. 1988. The effectsof experimentally inducedrespiratory virusinfections on performance. Psychol. Med.18:65–71
Spiegel D, Bloom J, KraemerH, Gotthel E.1989. Effect of psychosocial treatmentonsurvival of patients with metastatic breastcancer.Lancet2:901
StoneAA, BovbjergDH, NealeJM, Napoli A,Valdimarsdottir H, et al. 1992. Develop-ment of common cold symptomsfollowingexperimental rhinovirus infection is relatedto prior stressful li fe events. Behav. Med.8:115–20
Stone AA, Cox DS, Valdimarsdottir H, Jan-dorf L, NealeJM. 1987. Evidence that se-cretory IgA antibody is associated withdaily mood. J. Pers. Soc. Psychol. 52:988–93
Stone AA, Neale JM, Cox DS, Napoli A,Valdimarsdotti r H, Kennedy-Moore E.1994. Daily events are associated with asecretory immuneresponseto anoral anti-genin men.Health Psychol. 13:440–46
StraussGD, SpiegelJS,DanielsM, SpiegelT,Landsverk J, et al. 1986. Group therapiesfor rheumatoid arthritis. Arthrit is Rheum.29:1203–9
Theorell T, Blomkvist V, Jonsson H, Schul-manS, Berntorp E, StigendalL. 1995. So-cial support and the development of im-mune function in human immunodefi-ciency virus infection. Psychosom. Med.57:32–36
ThomasPD,Goodwin JM, Goodwin JS.1985.Effect of social support on stress-relatedchangesin cholesterol level, uric acidlevel,andimmune function in anelderly sample.Am.J. Psychiatr. 142:735–37
Verbrugge LM. 1979. Marital status andhealth. J. MarriageFam.41:267–85
Weinberger DA, Schwartz GE, Davidson RJ.
PSYCHOLOGICAL FACTORSAND DISEASE 141

1979. Low-anxious, high-anxious, and re-pressive coping styles: psychometric pat-terns andbehavioral andphysiological re-sponsesto stress.J. Abnorm. Psychol. 88:369–80
Weisman A, Worden J. 1975. Psychologicalanalysis ofcancerdeaths.Omega: J. DeathDying6:61–75
Young LD. 1992. Psychological factors inrheumatoid arthritis. J. Consult. Clin. Psy-chol. 60:619–27
ZakowskiSG,CohenL, Hall MH, WollmanK,
Baum A. 1994. Dif ferential effectsof ac-tive andpassive laboratory stressors on im-mune function in healthy men. Int. J. Be-hav. Med.1:163–84
Zakowski SG,McAll ister CG, Deal M, BaumA. 1992. Stress, reactivity, and immunefunction in healthy men. Health Psychol.11:223–32
ZondermanAB, Costa PT, McCraeRR. 1989.Depression as a risk for cancermorbidityandmortality in a nationally representativesample.J. Am.Med.Assoc.262:1191–95
142 COHEN & HERBERT