Embed Size (px)
Citation preview

Health Reform Monitoring Survey -- Texas

InMarch2015,near thecloseof theHealthInsuranceMarketplace’ssecondopenenrollmentperiod,wesurveyedadultTexansages18to64tounderstand who remained uninsured and why,and to identify the differences, if any, in thecharacteristicsoftheuninsuredpopulationbeforethe opening of the Marketplace in September2013,andMarch2015.Oursurveyindicatesthatthe 16.9% of adult Texans who remain uninsured are more likely to be Hispanic, middle aged,lowincomeandwithoutacollegedegree. Thiscorrespondswiththepre-Marketplacedatawhichindicatedthatthesesamegroupsweremorelikelytouninsuredin2013.Themajority(57.1%)oftheremaininguninsuredcitedcostsasthebiggestfactorintheirlackofinsurance,andalsoreportedthattheprospectofafinewasnotanimportantconsiderationtothem.
ABOUT THE SURVEY
TheHealthReformMonitoringSurvey(HRMS)isaquarterlysurveyofadultsages18-64thatbeganin2013.ItisdesignedtoprovidetimelyinformationonimplementationissuesundertheACAandtodocumentchangesinhealthinsurancecoverageandrelatedhealthoutcomes.HRMSprovidesquarterlydataonhealthinsurancecoverage,access,useofhealthcare,healthcareaffordability,andself-reportedhealthstatus.TheHRMSwasdevelopedbytheUrbanInstitute,conductedbyGfK,andjointlyfundedbytheRobertWoodJohnsonFoundation,theFordFoundation,andtheUrbanInstitute. Rice University’s Baker Institute and The Episcopal Health Foundation are partneringtofundandreportonkeyfactorsaboutTexansobtainedfromanexpanded,representativesampleofTexasresidents(HRMS-Texas).TheanalysesandconclusionsbasedonHRMS-Texasare thoseof the authors and do not represent the view of the Urban Institute, the Robert Wood JohnsonFoundationortheFordFoundation.InformationaboutthesampledemographicsofthecohortisavailableinIssueBrief#1.ThisIssueBriefisasummaryofdataextractedfromtheHRMSSurveyinTexasthatwasadministeredinMarch2015.WewillcontinuetoreportonsurveydatathroughadditionalIssueBriefsandfuturesurveys.
Issue Brief #13: Characteristics of Uninsured Texans as of March 2015
2 HEALTHREFORMMONITORINGSURVEY--TEXAS2 HEALTHREFORMMONITORINGSURVEY--TEXAS
AT A GLANCE
Texas’ uninsured population remains primarily Hispanic, middle aged,low income and without a college degree
Costs of insurance remain the biggest barrier for uninsured Texans
Texans who gained coverage between 2013 and 2015 are healthier than the remaining uninsured
July, 2015
Elena Marks, JD, MPH, Vivian Ho, Ph.D., and Philomene Balihe, MPH

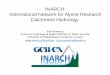
CHARACTERISTICS AND CHANGES IN RATES OF THE UNINSURED IN TEXAS, SEPTEMBER 2013 TO MARCH 2015 As we reported in Issue Brief #11, from September 2013 to March 2015, Texas experiencedanoverallreductionintherateofuninsuredresidentsages18-64of7.7percentagepoints,from24.6%to16.9%(a31%decrease).Forthisbrief,welookedatthecharacteristicsoftheremaining16.9%ofuninsuredadultTexansasofMarch2015andcompared themto the24.6%uninsuredadults as of September 2013. In Table 1, we examine the proportion of the uninsured in 2013and 2015 who are in various demographic or socioeconomic categories. At both points in time,theuninsuredareprimarilymiddleaged(31-49),Hispanic,lowincome(atorbelow138%ofthefederalpovertylevel),andnotcollegeeducated.
Table 1: Proportions of Uninsured Adult Texans by Demographic and Socioeconomic Category,
September 2013 and March 2015
HEALTHREFORMMONITORINGSURVEY--TEXAS 3

4 HEALTHREFORMMONITORINGSURVEY--TEXAS
Thereareinterestingchangesinthemake-upoftheremaininguninsuredwithinsomeofthesegroups,notwithstandingtheabove-notedconsistencies.Thepercentageofuninsuredwhoareolderadults,ages50-64,declinedconsiderablyfrom2013to2015,whilethepercentageofthoseages18-30and31-49whowereuninsuredrose,relativetotheolderadults.Thisisbecausethereductioninratesofuninsuredfortheoldestgroupdeclinedatagreaterratethantheotheragegroups.Thiswasanexpectedoutcomeofthepre-existingdispositionofolderadultstowardhealthcoverageandthe favorablepricingofplans for thispopulationbecauseof theAffordableCareAct’s ratebandrules.WhilethemajorityoftheremaininguninsuredadultsarestillHispanic,Hispanicsactuallyexperiencedthegreatestpercentagedecreaseintherateofuninsuredduringthisperiodoftime,adropof37.8percent.Notsurprisingly,thelowestincomeadultscompriseanincreasinglylargepercentageof theuninsured in2015as compared to2013,becausemostof themwere ineligibleforcoverageopportunitiesintheMarketplace.TheACAofferedcoveragetothisgroupthroughanoptionalMedicaidexpansion,butbecauseTexasdidnotexpandMedicaid,thelowestincomeTexanswerenoteligibleforACAcoverage.
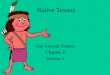
Wealsocomparedtheself-reportedhealthstatusofuninsuredTexansinSeptember2013andMarch 2015 to learn whether the remaining uninsured were more or less healthy than the pre-Marketplaceuninsured. Figure 1belowcontainsthatdata.Thepercentageofuninsuredindividualsreportingexcellenthealthwasrelativelyunchangedbetween2013and2015.Theshareofuninsuredineitherfairorpoorhealthalsodidnotchangesignificantlyovertime.However,thepercentageuninsured in very good health declined significantly (from 29.9% to 17.2%) between 2013 and2015,andthepercentageofuninsuredreportingthemselves ingoodhealthrose(from38.7%to49.8%).Thesechangessuggestthatthosewhowereabletogaincoveragesince2013arehealthieronaveragethanthosewhoremainuninsured.Theseresultsareconsistentwithresearchstudiesshowingastrongcorrelationbetweenincomeandhealthstatus.Theuninsuredinfamiliesearning100%+ofthefederalpovertylevelwereabletopurchaseinsuranceusingsubsidiesprovidedbytheAffordableCareAct.However,thelowestincomefamilies,whoarelikelytohaveworsehealthstatus,havenoaccesstosubsidies.TheACAintendedtogivethepoorestindividualsMedicaidcoverage,butTexashasnotelectedtheMedicaidexpansionofferedbythelaw.
Figure 1: Self-reported health status of adult Texans, September 2013 and March 2015
*Mar2015estimatedifferssignificantlyfromSep2013at.05level,usingtwo-tailedz-tests.

HEALTHREFORMMONITORINGSURVEY--TEXAS 5
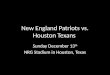
We asked those who remained uninsured in March 2015 why they did not have insurance andwhether the prospect of a tax penalty impacted their coverage decisions. As shown in Figure 2below,themajority(57.1%)citedthecostofinsuranceastheprimaryreasonfornotbeingcovered.Not surprisingly, as shown in Figure 3 below, nearly half of respondents (47.4%) reported thatthepossibilityofafinewas“nottooimportant”or“notatallimportant”tothem.Asmallbutnotinsignificant percentage of uninsured respondents, 17.3%, reported that they did not want healthinsurance.
Figure 2: Primary Reasons Adult Texans are Uninsured, March 2015
Figure 3: Importance of the Possibility of a Fine to Uninsured Adult Texans, March 2015

6 HEALTHREFORMMONITORINGSURVEY--TEXAS
Looking Ahead Inournextbrief,wewill explore thedifferences inaccess tocareamong insuredanduninsuredTexasadults.
ABOUT THE AUTHORS
Elena Marks, JD, MPH, isthePresidentandChiefExecutiveOfficerofTheEpiscopalHealthFoundationandanon-residentfellowinhealthpolicyatRiceUniversity’sBakerInstituteforPublicPolicy.
Vivian Ho, PhD, is the James A. Baker III Institute Chair in Health Economics, aprofessorintheDepartmentofEconomicsatRiceUniversity,andaprofessorintheDepartmentofMedicineatBaylorCollegeofMedicine.
Philomene Balihe, MPH,isadataanalystattheEpiscopalHealthFoundation.
TheauthorsgratefullyacknowledgetheassistanceofMeeiHsiangKu-GotoandAlitheaMcFarlaneand the financial supportof themembersof theBaker Institute’sHealthPolicyForum.
The core HRMS is supported by the Robert Wood Johnson Foundation, the FordFoundation,andtheUrbanInstitute.WeappreciatetheUrbanInstitute’swillingnesstocollaborateonexpandingtheHRMSsampletosupportestimatesforTexas.

HEALTHREFORMMONITORINGSURVEY--TEXAS 7
METHODOLOGY
Eachquarter’sHRMSsampleofnonelderlyadults is drawn from active KnowledgePanel®members to be representative of the USpopulation. In the first quarter of 2013, theHRMS provided an analysis sample of about3,000 nonelderly (age 18–64) adults. Afterthat,theHRMSsamplewasexpandedtoprovideanalysis samples of roughly 7,500 nonelderlyadults,withoversamples added tobetter tracklow-incomeadultsandadults in selected stategroupsbasedon (1) thepotential forgains ininsurancecoverage in thestateunder theACA(asestimatedby theUrbanInstitute’smicrosimulationmodel)and(2)statesofspecificinteresttotheHRMSfunders. Althoughfreshsamplesaredrawneachquarter,thesameindividualsmaybeselectedfordifferentroundsofthesurvey.Becauseeachpanelmemberhasauniqueidentifier,itispossibletocontrolfortheoverlapinsamplesacrossquarters.ForsurveysbasedonInternetpanels,theoverallresponserateincorporatesthesurveycompletionrateaswellastheratesofpanelrecruitmentandpanelparticipationovertime. The American Association for Public Opinion Research (AAPOR) cumulativeresponserate for theHRMSis theproductof thepanelhouseholdrecruitmentrate,thepanelhouseholdprofilerate,and theHRMScompletionrate—roughly5percenteachquarter. While low, this response rate does not necessarily imply inaccurate estimates; asurvey with a low response rate can still be representative of the sample population,althoughtheriskofnonresponsebiasis,ofcourse,higher.All tabulations fromtheHRMSarebasedonweightedestimates.TheHRMSweightsreflect the probability of sample selection from the KnowledgePanel® and post-stratification to the characteristics of nonelderly adults and children in the UnitedStatesbasedonbenchmarksfromtheCurrentPopulationSurveyandthePewHispanicCenter Survey. Because the KnowledgePanel® collects in-depth information onpanelmembers,thepost-stratificationweightscanbebasedonarichsetofmeasures,includinggender,age,race/ethnicity,education,householdincome,homeownership,Internetaccess,primarylanguage(English/Spanish),residenceinametropolitanarea,andregion.Giventhemanypotentialsourcesofbiasinsurveydataingeneral,andindatafromInternet-basedsurveysinparticular,thesurveyweightsfortheHRMSlikelyreduce,butdonoteliminate,potentialbiases. TheSeptember2013HRMShasadesigneffectof1.47fornonelderlyadults,andasamplingmarginoferrorfora50percentstatisticwith95percentconfidenceof+/-1.3forthenonelderlyadultsample.ThedesigneffectfortheTexasdatainMarch2015is2.184andtheMOEis+/-3.7.ThesurveyfieldedfromMarch5-30.
Health Reform Monitoring Survey -- Texas

Foundedin1993,the JAMES A. BAKER III INSTITUTE FOR PUBLIC POLICYhasestablisheditselfasoneof thepremiernonpartisanpublicpolicy thinktanks in thecountry.Theinstituteranks9thamonguniversity-affiliatedthinktanksworldwide,18thamongU.S.thinktanksandfourthamongenergyresourcethinktanks,accordingtoa2014studybytheUniversityofPennsylvania’sThinkTanksandCivilSocietiesProgram.AsanintegralpartofRiceUniversity,oneofthenation’smostdistinguishedinstitutionsofhighereducation,theBakerInstitutehasastrongtrackrecordofachievementbasedontheworkofitsendowedfellows,Ricefacultyscholarsandstaff.LocatedinHouston,Texas,thenation’sfourth-largestcityandtheenergycapitaloftheUnitedStates,aswellasadynamicinternationalbusinessandculturalcenter,theBakerInstitutebringsauniqueperspectivetosomeofthemostimportantpublicpolicychallengesofourtime.
Contact information can be found at: http://bakerinstitute.org
THE EPISCOPAL HEALTH FOUNDATION isanewlyestablishedentitywith$1billioninassetsdedicated to improving thehealthandwell-beingof thepeople andcommunities in theEpiscopalDioceseofTexas.TheFoundationembracestheWorldHealthOrganization’sbroad,holisticdefinitionofhealth:a stateofcompletephysical,mentalandsocialwell-beingandnotmerely theabsenceofdisease. The Foundation’s work includes research, grant-making and other initiatives aimed attransformationalchange.
Contact information can be found at: http://www.episcopalhealth.org
SuggestedCitation:
MarksE,HoV,BaliheP.
JamesA.BakerIIIInstituteforPublicPolicy,RiceUniversity,
TheEpiscopalHealthFoundation,
Health Reform Monitoring Survey – Texas,
Issue Brief #13:
Characteristics of Uninsured Texans as of March 2015
©2015JamesABakerIIIInstituteforPublicPolicy,EpiscopalHealthFoundation