Embed Size (px)
DESCRIPTION
Health Roundtable Qld Chapter Meeting Latest Developments in ABF Member Perspective. Dr Andrew Johnson Townsville Health Service District. Latest District Developments. ABF Model released Purchasing Framework negotiations finalised - PowerPoint PPT Presentation
Citation preview

Health RoundtableQld Chapter Meeting
Latest Developments in ABFMember Perspective
Dr Andrew Johnson
Townsville Health Service District

Latest District Developments
• ABF Model released
• Purchasing Framework negotiations finalised
• Financial Plan including Demand Management Strategies developed
• District ABF Plan being developed
• Institute / service level specific strategies being formulated and implemented
• Routine reporting mechanisms established

Demand Management StrategiesPurchasing Framework
1. Out of Scope Activities (male ster / vein strip & lig)– District communication strategy to be developed– Where clinically indicated procedure is required, second
medical opinion will be sought and if concurred opinion → procedure undertaken
2. Own Source Revenue– PHI target: 80% (currently 46%)– Bulk billed clinics target: 27% (currently 18%)

3. Relative Utilisation (↓ or ↑ serving population)– District plan to be developed:
• Rebalance relative utilisation of approx three clinical services• Develop work program for priority areas identified by clinicians
and worthwhile for local population
4. Outpatient Ratios (repeat to new attendances)– Negotiated local targets for following clinic types:
• General paediatrics / paediatric surgery• General surgery• Thoracic medicine
Demand Management StrategiesPurchasing Framework

5. Potentially Avoidable Adms (uncomp cellulitis)– New ED short stay beds model of care includes
treatment of cellulitis patients– Corporate supportive of this model, targets endorsed:
• Short stay outliers admissions (ED) = 33%• Treatment provided outside hospital setting = 47%• Overnight acute admissions = 20%
6. Mode of Treatment (in-centre vs home dialysis)– Integrated Planning and Policy Executive Committee– NQ benchmarks of 40% home and 60% in-centre
Demand Management StrategiesPurchasing Framework

7. Quality and Safety (falls, PU, HAI, treatment inj)– Clinical Improvement & Redesign Unit monitoring volume
of pressure ulcers → developing reduction strategies– Review medical records → process changes required?– Review "Medicare Never Events" (US based study) →
isolate further hospital treatment injuries for review
8. Activity Growth– Indexed areas → accepted corporate rate– Non-indexed areas → demand management strategies
Demand Management StrategiesPurchasing Framework

Current ABF Governance
• ABF (Casemix) Management Group– Nominated Institute representatives meet monthly– Operationally focussed (not generally clinical)– Forum for sharing ABF information and experiences
• ABF Management Group – Education Sessions– Attendees as above, meet monthly (alternate fortnight)– Education session topics based on:
• Identified issues• Corporate developments• Attendee feedback

Current ABF Governance
• Potential Bedday Savings Reports– Top 5 DRGs per Institute based on HRT data– Shows number of cases, monthly and YTD ALOS– Coloured coded to show improvement or ↑ ALOS
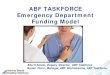
HEALTH ROUNDTABLE IDENTIFIED POTENTIAL BED DAY SAVINGS
- The Relative Stay Index (RSI) is used for comparison with peers. The RSI is based on subgroupings within DRG families - by DRG, emergency/elective, admit source, age group, complexity and destination.- Peers have been identified as Hospitals with a similar casemix to The Townsvil le Hospital
DRG Family Code and Name
Potential Annual BedDay Savings
TTHEpisodes
TTHALOS
ExemplarALOS
TTH RSI
Exemplar RSI
All HRT ALOS
Institute Target ALOS
May
201
0
Jun
201
0
Jul 2
010
Au
g 2
010
Sep
201
0
Oct
201
0
No
v 2
010
De
c 20
10
Jan
2011
Feb
201
1
Mar
201
1
Ap
r 20
11
TO
TA
L
Av
g M
on
th12
m A
LO
S
Institute of Cardiac Services Institute of Cardiac Services
F10 - PERC CORONY INTERVENT+AMI 498 119 5.3 3.3 143% 87% 3.8 TBA 22 5.4 12 4.9 17 3.6 18 5.2 13 13.8 26 4.5 17 4.0 28 3.8 20 5.4 27 4.4 18 5.7 18 4.3 236 19.7 5.1
F42 - CRC DSRD-AMI+INVAS INVEST PR 430 176 4.4 2.3 119% 87% 3.6 TBA 23 3.4 21 4.9 18 5.5 24 2.8 44 5.7 36 4.8 27 4.1 28 4.5 35 3.9 27 5.0 36 3.4 29 4.8 348 29 4.4
F74 - CHEST PAIN 419 649 0.9 0.5 112% 71% 0.6 TBA 94 1.4 85 1.4 110 1.4 94 1.5 123 1.4 116 1.3 107 1.3 99 1.2 93 1.2 79 1.2 100 1.5 106 1.5 1206 101 1.4
F41 - CRC DSRD+AMI+INVAS INVEST PR 405 90 5.8 3.7 133% 82% 4.5 TBA 9 9.3 19 6.9 19 5.4 7 6.3 20 5.7 12 4.8 18 4.8 14 7.7 8 6.3 5 4.0 14 4.5 7 6.1 152 12.7 5.9
F71 - N-MJR ARRHYTHM & CONDCTN DSRD 323 147 3.1 1.6 113% 73% 2.1 TBA 21 4.8 17 3.6 25 3.8 29 4.1 27 3.7 23 2.6 24 2.8 19 2.3 16 3.2 19 2.4 18 2.5 12 4.2 250 20.8 3.4
Institute of Emergency and Medical Services Institute of Emergency and Medical Services
I68 - NON-SURG SPINAL DISORDERS 599 196 3.7 1.9 124% 72% 2.5 TBA 29 4.1 37 1.6 39 2.8 21 5.3 35 3.4 39 3.4 32 2.9 29 7.6 21 3.4 38 5.6 24 6.3 29 2.1 373 31.1 3.9
B70 - STROKE 535 105 9.2 5.4 101% 73% 7.0 TBA 17 10.4 23 9.2 28 10.8 17 9.2 17 5.9 30 8.9 12 4.8 14 11.6 20 8.8 13 5.1 19 6.5 23 7.3 233 19.4 8.4
X60 - INJURIES 466 232 2.7 1.3 139% 87% 1.7 TBA 34 1.8 39 3.2 38 2.4 37 2.6 25 2.5 46 1.8 46 5.3 40 2.8 43 3.2 46 3.5 36 1.4 45 2.0 475 39.6 2.8
E65 - CHRNIC OBSTRCT AIRWAY DIS 454 204 5.2 3.9 95% 74% 5.0 TBA 18 7.0 28 4.0 31 4.5 36 6.5 31 8.5 33 4.1 42 5.7 40 3.6 19 5.6 52 5.6 36 5.3 34 6.8 400 33.3 5.5
B78 - INTRACRANIAL INJURY 278 45 8.2 5.0 132% 83% 5.8 TBA 4 14.0 8 8.5 9 7.1 9 12.8 14 5.9 2 3.0 5 10.2 8 7.8 9 7.6 6 6.2 11 13.5 10 10.5 95 7.92 9.1
Institute of Mental Health Institute of Mental Health
U67 - PERSONLTY DSRD&ACUTE REACTIONS 413 83 6.8 3.7 116% 74% 4.3 TBA 14 5.8 8 23.9 10 6.7 15 8.9 15 7.8 13 3.8 17 3.1 13 10.8 13 24.9 11 2.5 12 3.4 14 3.6 155 12.9 8.2
U63 - MAJOR AFFECTIVE DSORDERS 269 66 14.3 12.0 83% 71% 13.9 TBA 12 27.1 7 8.9 9 11.3 12 28.8 11 10.8 14 13.3 7 5.4 13 11.2 10 7.3 8 35.4 18 12.9 12 20.1 133 11.1 16.2
Institute of Surgery Institute of Surgery
I08 - OTHER HIP & FEMUR PROC 738 58 15.6 9.0 126% 75% 10.8 TBA 4 32.0 12 14.2 9 17.7 10 26.8 10 8.5 12 10.8 11 13.5 6 20.5 13 9.8 19 14.2 13 16.5 9 11.9 128 10.7 15.1
I12 - INFC/INFM BONE/JNT+MISC PR 463 47 15.2 7.4 115% 78% 12.6 TBA 4 6.0 12 15.4 7 6.1 11 6.5 3 28.3 12 24.2 7 15.9 7 16.9 11 8.3 5 6.2 10 10.9 3 14.7 92 7.67 13.1
I03 - HIP REVISION OR REPLACEMENT 329 41 11.5 6.4 121% 79% 7.8 TBA 9 9.3 9 12.9 5 9.6 6 9.5 6 12.5 9 13.0 9 14.8 6 6.3 6 14.7 7 12.3 9 9.0 10 9.0 91 7.58 11.1
K01 - DIABETIC FOOT PROCEDURES 310 17 20.5 12.5 123% 68% 16.6 TBA 5 11.6 4 24.8 2 22.5 0 0.0 1 1.0 2 11.0 6 21.7 6 25.3 3 41.0 2 22.0 4 10.8 3 27.3 38 3.17 21.0
B02 - CRANIOTOMY 269 68 11.4 9.0 100% 83% 10.8 TBA 10 15.3 15 11.4 8 13.8 14 10.0 11 11.5 15 10.5 9 11.9 11 11.5 10 13.9 11 12.2 17 14.8 9 8.2 140 11.7 12.1
Institute of Womens & Childrens Health Institute of Womens & Childrens Health
O66 - ANTENATAL & OTH OBSTETRIC ADM 815 367 2.0 0.9 149% 67% 1.1 TBA 71 1.7 36 1.9 61 2.3 58 2.2 71 2.4 50 2.8 62 1.9 64 2.5 48 1.6 54 1.5 82 2.8 53 2.2 710 59.2 2.2
O01 - CAESAREAN DELIVERY 685 338 5.0 3.6 100% 80% 4.5 TBA 43 3.3 44 4.6 63 5.4 59 4.2 53 4.5 54 5.8 47 5.0 62 4.7 63 4.0 64 5.1 71 5.0 51 3.9 674 56.2 4.7
P66 - NEO,ADMWT 2000-2499G-SG OP 543 80 10.2 6.7 113% 76% 9.6 TBA 4 13.0 12 10.0 13 7.5 14 10.1 7 18.6 16 7.6 9 12.9 9 20.1 12 10.1 8 14.0 7 12.4 11 12.8 122 10.2 11.7
O60 - VAGINAL DELIVERY 409 830 2.1 1.9 88% 77% 2.4 TBA 138 2.2 131 2.3 150 2.2 155 2.3 133 1.9 138 2.0 123 2.1 133 2.2 144 2.0 109 2.0 146 2.1 138 2.6 1638 137 2.2
P65 - NEO,ADMWT 1500-1999G-SG OP 374 39 24.4 16.0 113% 90% 21.5 TBA 5 44.6 3 17.7 2 21.5 10 27.0 9 26.2 5 15.2 7 23.0 5 32.2 7 31.9 3 41.3 4 44.0 8 28.9 68 5.67 29.1
- Showing: Number of cases | ALOS
Greater than 10% over Jul10-Dec10 ALOS x.x
Greater than Jul10-Dec10 ALOS, but less than 10% over x.x
The above table represents 6 months of casemix data analysed by the Health Roundtable (Jun10-Dec10) For comparison to target ALOS when targets are agreed Less than Jul10-Dec10 ALOS x.x
Townsville Hospital Relative Stay Index compared to QLD peers

Current ABF Governance
• Bed Utilisation Report– Based on Relative Stay Index– Shows beds required if state and HRT ALOS met– Supports decisions about bed allocations based on
current need and efficiency
Revision 2.6 (DRAFT)
Report NotesData Source
- Data extracted from Transition II. This report can be re-produced for different time periods- Bed days are counted against the primary doctor unit the patient was under the care of for each day of their stay and are fractional
ie. If a patient was admitted at midday and stayed overnight, that day would count as 0.5 bed days
Data Inclusions- Inpatient episodes for the full calandar year 2010 (01/01/2010 through 31/12/2010)- Ward bed allocation figures as at December 2010 - overnight beds only- Bed numbers are derived using the formula: (Bed Days / days in period)- 3mths refers to Oct10 -> Dec10, 6mths refers to Jul10 -> Dec10, 12mths refers to Jan10 -> Dec10- [Beds used if Casemix] is based on state peer average length of stay (including critical care, SNAP and non-acute bed days)- Health RoundTable average is derived by applying the casemix adjusted average length of stay across the entire Health RoundTable membership to each separation / DRG
Data Exclusions- Excludes all same day cases from the following wards:
TBC, TBIR, TCLD, TDIA, TDSU, TEND, THMU, TMDP, TNLUQ, TODU, TOT, TPAEDB, TRAD, TSPN, TWCCand all cases in TDSUE, as these wards to not have any overnight beds
- Excludes all usage by Emergency and Palliative Dr Units, which in effect excludes the Emergency Short Stay and Palliative Care wards- The following institutes have been excluded from this report: Institute of Primary Health and Ambulatory Care, Institute of Mental Health Services, Institute of Support Services- The casemix and Health RoundTable average lengths of stay were not applied for Z-coded acute DRGs (Other health factors), Uncoded episodes and Non-Acute episodes
Total bed days used by inpatients
Bed days divided by number of days in period
to give a daily average
% Utilisation of all beds used at The Townsville
Hospital
% Utilisation of beds allocated to wards in
Institute
If Casmix state ALOS was achieved for each
inpatient episode, this many beds would be
required
Beds needed if Health RoundTable Average Met
over 12 months
3mths 6mths 12mths 3mths 6mths 12mths 3mths 6mths 12mths 3mths 6mths 12mths 3mths 6mths 12mths 3mths 6mths 12mths
Institute of Cardiac Services 3,492 6,846 13,141 38.0 37.2 36.0 10.4% 10.2% 10.0% 105% 103% 100% 34.8 33.2 31.9 37.8 36.9 35.5
Institute of Emergency & Medical Services 12,411 25,500 50,900 134.9 138.6 139.5 37.0% 38.0% 38.8% 93% 96% 96% 118.8 123.2 123.2 123.2 125.9 124.3
Institute of Surgery 8,767 17,627 34,144 95.3 95.8 93.5 26.1% 26.3% 26.0% 99% 100% 97% 99.3 96.6 91.7 91.8 90.2 86.9
Institute of Women's & Children's Services 6,602 13,143 25,253 71.8 71.4 69.2 19.7% 19.6% 19.2% 90% 89% 86% 66.4 64.5 62.2 68.5 67.7 65.8
Townsville Cancer Centre 2,264 3,930 7,844 24.6 21.4 21.5 6.7% 5.9% 6.0% 98% 85% 86% 17.3 14.7 14.5 21.1 18.3 17.8
Grand Total 33,536 67,053 131,304 364.5 364.4 359.7 100.0% 100.0% 100.0% 95.4% 95.4% 94.2% 336.7 332.2 323.5 342.3 339.1 330.1
Clinical Information ServicesTownsville Health Service District
Performance & Reporting UnitPh: 4796 1037
THE TOWNSVILLE HOSPITAL BED UTILISATION REPORT
DOCTOR UNIT Vs WARD ALLOCATION, BY INSTITUTEOCT10-DEC10 (3mths) / JUL10-DEC10 (6mths) / JAN10-DEC10 (12mths)
DRAFT
Institute (Ward) Bed Allocations as at December 2010
Beds Allocation382 100%
Institute of Cardiac Services 36 9.4%Institute of Emergency & Medical Services 145 38.0%Institute of Surgery 96 25.1%Institute of Women's & Children's Services 80 20.9%Townsville Cancer Centre 25 6.5%

2011/12 District ABF Plan
• “Funding Better Care” Governance Committee– Clinical leadership group– TOR developed– Inaugural meeting → August / September
• Data Integrity and Improvement Group– Data management group– TOR developed– Currently calling for nominations– Inaugural meeting → August

2011/12 District ABF Plan
• ABF Training and Education Proposal– Executive overview sessions for all staff– Staff group specific information sessions for all staff– Routine information sessions & attendance at meetings
• Institute / clinical specialties– Developing initiatives to:
• Achieve Purchasing F’work / Demand Management strategies• Improve ABF awareness• Increase ABF knowledge base

2011/12 District ABF Plan
• Expanding current routine reporting:– Analyse and monitor throughput for Demand
Management indicators– Develop mechanisms for early identification of issues
• Causal feedback needs to be supplied • Issue resolution strategies to be formally tabled and monitored
– Distribute and discuss information at existing Executive and Institute management meetings

Challenges
• “We’ve heard it all before…..”
• Clinical engagement
• Limited resources – District and Corporate
• Recruitment and retention of skilled staff

Questions / Comments