Embed Size (px)
Citation preview

HEALTH SYSTEM WATCH 2/2002 1
II/Summer 2002
HEALTH SYSTEM WATCH Supplement of the journal Soziale Sicherheit
Health System Watch is produced by the Institute for Advanced Studies/Institut für Höhere Studien
(IHS) - IHS HealthEcon and edited by the Hauptverband der österreichischen
Sozialversicherungsträger (Federation of Austrian Social Security Institutions)
Resource consumption in the EU: Allocation is more than financing – payment mechanisms
in Social Health Insurance Countries
Focus: Physicians and cities: a close link
Maria M. Hofmarcher, Christine Lietz, Monika Riedel*
Resource consumption In order to finance the health system in the best possible way, both economic and fairness aspects have to be taken into consideration. However, the way of financing alone does not indicate whether the allocation (i.e. the distribution of funds) is efficient or not. How funds are distributed and used is determined by the demand for health services as well as the supply, which in turn depends on the level of a society’s development. In developed countries, the major part of resources is spent on the following three sectors: hospitals, care provided by generalists or specialists, and medicines. In many cases up to 50 per cent of the total health budget is spent on hospital care. Costs, efficiency and quality are considerably influenced by the mechanisms of paying the individual health service providers.
Physicians and cities In Austria, the physician density, and in particular the density of physicians, who have a contract with the social health insurance, is low compared to Germany and France. Even Vienna has a lower physician density than Hamburg, Berlin, Lyon and Paris. What these five cities do have in common is the fact that their ratio of physicians per inhabitant is higher than that of the rest of the respective country. In Austria this difference is greater than in Germany, with Vienna having 72% more physicians per inhabitant than the rest of the country. In the two French cities - Lyon and Paris - the gap is even more pronounced: Paris, for example, has two-and-a-half times more physicians than the rest of France. In cities, also the health insurance’s per-capita spending for medical services is higher than in the country. In this case, however, the difference is not as big as with the density of physicians.
* With special thanks to Gerald Röhrling for his assistance and Martina Szucsich for translation

HEALTH SYSTEM WATCH 2/2002 2
Resource consumption in the EU: Allocation is more than financing - payment mechanisms in Social Health Insurance countries
Mixed financing as a rule without exceptions In none of the developed countries public financing taps only one single source. In countries with
social security systems the major part of public expenditure on health is financed by contributions,
the rest by taxes. To what extent each of these two financing sources come into play varies from
country to country: While in France the main part (95%) of public spending on health is financed by
health insurance contributions, in Austria it is only 66%. Germany is in between with 90%.
Health insurance contributions can be considered as a general tax that has been specially adapted
to the financing of health care and corresponds to a fixed percentage of a beneficiary's income, the
amount being limited by an upper level. The contributions' amount as well as the defined services
are determined on the basis of certain laws, which substantiate a social contract providing services
in terms of non-cash benefits and/or money for all those who necessitate them, independently of
their incomes.
It is difficult to compare the individual contribution rates since they differ considerably from each
other, even within public health insurance companies. While in Austria people employed have to pay
approximately 7% (blue collar workers: 7.6%, white collar workers: 6.9%, civil servants: 7.1%), in
Germany they pay on the average 14% for public health insurance. In France, people employed pay
13.55%. In Austria, employers and employees to equal parts share the contribution. In France,
employers pay 12.8%, employees 0.75%. Unlike in Austria and Germany, where contributions are
paid up to a monthly gross income of € 3.226,67 (Austria) and € 3.375 (Germany), respectively, there
is no income ceiling.
Be it taxes or contributions....
Contrary to Social Health Insurance (SHI) countries tax financed health care systems depend on the
overall amount of tax revenues collected by the state. . This means the health care system is
constantly competing for public funds1.
Health insurance contributions - levied as a certain percentage of the income - have the properties of
an income tax. Nevertheless they are used only for specified services and are in most cases levied
and administered by self-governing bodies that have their own balance and budget rules.
Contributions and services therefore cannot be changed by simple government measures. A
1 A five-year investment plan of the British National Health Care System (NHS) provides for raising the health budget by 40 million Pounds (65 billion Euro) in order to lift health care spending to the European average level. In the preceding discussions some rather extraordinary suggestions were made, like the transfer of funds from the defense budget and the ministry of internal affairs to the health budget. (The plan is now to finance health care by raising national insurance by 1%.) Cf. Moore, W.: NHS to receive an extra £40bn over next five years, BMJ 2002;324:993 (27 April) and Appleby J., Boyle S.: Blair's billions: where will he find the money for the NHS?, BMJ 2000;320:865-867 (25 March).

HEALTH SYSTEM WATCH 2/2002 3
legislative process, requiring certain rules of decision-making among the interest groups, precedes
every single adjustment of contribution rates or services. Contributions can seem more attractive
than uncommitted taxes if the impression can be created among the people that their money is spent
and administered to their benefit by non-government organisations.
Yet, contribution-based financing is mostly linked to the occupational status substantiating an
entitlement. Thus, unlike with systems that are financed by taxes there is no basic right to health
care provision in SHI-countries 2.
... economic consequences of financing on competitiveness are likely ...
Income and consumption taxes are the usual sources for financing public duties. The amount of
taxes available depends however on short - and long-term economic growth cycles. In times of
recession, tax revenues may dec rease and the competition for public funds increase. Profits in
general are more sensitive to an economic downturn than wages. The economic effect health
systems that are financed by taxes may generate depends considerably on what kind of tax is used.
Economic theory is based on the assumption that high taxes decrease labour supply by diminishing
the income available. Empirical evidence, on the other hand, indicates that the income elasticity of
labour supply (at least with men) is low3. High labour costs in turn may diminish a country's
competitive ability on the international level and slow down investments and growth. With the
growing globalisation of the economy, such considerations are becoming ever more important.
An important social aspect of taxation is the question of who carries the tax burden. A tax system is
considered vertically just if people with higher incomes have to pay more. Horizontal justice would
mean that persons suffering from certain disadvantages (e.g. health problems) pay lower taxes than
those without these disadvantages. Vertical justice tends to be higher in systems that are financed by
progressive income taxes including profit taxation. Only in such comprehensive tax systems it can be
guaranteed that taxes rise with rising income. Horizontal justice is generally given if tax contributions
are made by a broad basis, including the whole population. It may however suffer if revenues are
solely drawn from consumption taxes. For instance, the value-added tax on drugs, affects only those
who suffer from health problems. In addition to that, consumption taxes like the value-added tax
might endanger vertical justice since persons with lower incomes spend a larger share for
consumption goods, whereas persons with higher incomes have a higher propensity to save.
Horizontal justice is even more threatened if fund raising is decentralised too much: wealthier regions
are able to contribute more than poor regions. As a consequence the central state often has to take
complicated adjustment measures, which might reduce the transparency of allocating funds to the
health sector.
2 In France, a quasi-basic right was created in 2000 by introducing a comprehensive right to health care provision; cf. Yukata I., Jacobzone S, Lenain P.: The Changing Health System in France, OECD Working Papers No. 269, 2000. 3 Cf. e.g.. Leibfritz W., Thornton J., Bibbee A.: Taxation and Economic Performance, OECD 1997, Economics Department Working Papers No.176

HEALTH SYSTEM WATCH 2/2002 4
... and will finally depend on the balance of power in practice
In general employees carry the major burden of contribution payments in the medium run even if
employers share the rates, the latter in fact being able to shift the burden onto wages. The
magnitude of this shift depends on the labour market conditions and, above all, on the power of trade
unions. Even if a complete shift of the employers‘ contributions is not possible, part of it is likely to be
passed onto prices, which can in turn impair the competitiveness. It is difficult to assess these effects
on economies growth dynamics. Nevertheless it is often argued that social security systems are to a
certain extent automatic stabilisers that help to compensate for a decrease in demand during times
of recession and thus to slow down the economic downturn4.
Allocation is more than financing The sole way how funds are collected and administered does not give any information about the
efficiency of the allocation (i.e. the distribution of funds). The distribution and use of funds is mainly
determined by demand and to a certain extent also by the supply of health services provision, which
in turn is determined by the level of a society's development.
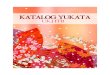
Figure 1: Expenditure on health according to the main functions, 1998 or most recent year
available
53 51 4845
40
31
19 18 1713 12 12
2217 16 14 13 12
8
35 34
8 11
0
10
20
30
40
50
60
Net
herla
nds
Sw
itzer
land
Aus
tria
Fra
nce
Isra
el
Bel
gium
Ger
man
y
Luxe
mbo
urg
Aus
tria
Sw
itzer
land
Ger
man
y
Bel
gium
Luxe
mbo
urg
Fra
nce
Net
herla
nds
Fra
nce
Isra
el
Bel
gium
Aus
tria
Ger
man
y
Luxe
mbo
urg
Net
herla
nds
Sw
itzer
land
hospital sector physician services drugs
in %
of t
otal
exp
endi
ture
on
heal
th
SHI, weighted average
SHI = Social Health Insurance Countries Hospital care: Belgium, Switzerland 1997; Austria: fund hospitals; health care spending according to official ESVG 95 method Physician services: Belgium: only public spending Drugs: Belgium 1997 Sources: WHO Health for all database, January 2002; OECD Health Data, August 2001; BMAGS; Statistik Austria; IHS HealthEcon 2002.
4 Vgl. Nowotny, E., Scheer, C., Walther, H.: Der öffentliche Sektor: Einführung in die Finanzwirtschaft (3., neubearb. und erw. Aufl.), Springer-Verlag, Berlin, 1996

HEALTH SYSTEM WATCH 2/2002 5
Figure 2: Health care spending in % of the GDP, 1998 or most recent year available
3,55,3
3,9 4,2 4,63,0 3,3 3,9
1,8
1,7
1,9
1,4 1,1 0,7
1,1 1,11,5
0,7
1,3
0,8
1,5 2,10,9
1,4 0,5
1,1
0,7
4,12,4
3,0 2,0
2,53,1
3,31,5
2,8
0
2
4
6
8
10
12
Ger
man
y
Sw
itzer
land
SH
I, w
eigh
ted
aver
age
Fra
nce
Net
herla
nds
Bel
gium
Isra
el
Aus
tria
Luxe
mbo
urg
in %
of G
DP
othersdrugsphysician serviceshospital care
SHI = Social Health Insurance Countries Hospital care: Belgium, Israel 1997; Austria: fund hospitals; Israel: Hospitals and research Physician services: Belgium: only public spending; Israel: private physicians (29,4%) and dental care (70,6%), 1997 Drugs: Israel: budget spending for drugs, 1997 Sources: OECD Health Data, June. 2001; Israel: Central Bureau of Statistics; IHS HealthEcon 2002.
In all health systems hospital care, physician services and drug consumption utilize the major share
of resources. In some cases up to 50% of health care spending is used for hospital care (cf. table 1),
which in all countries utilizes most resources5. This is why cost containment measures in health
policies focus on this sector not only in Austria, but also on an international level. The availability of
data and information in this sector is comparably sound. Despite considerable efforts not even the
experienced international organisations like the OECD have succeeded in comprehensively
documenting the consumption of resources in the sectors of general practitioners and specialists.
For 1999, the spending for generalist and specialist care are recorded for only six EU countries,
including Austria (cf. annexed table A1). As for public health, including health promotion and
prevention, the availability of data is even less satisfactory6.
Social health insurance countries show signs of ageing...
Countries with social security systems particularly focus on the curative sector. Public health as a
strategy of strengthening prevention and health promotion, on the other hand, is poorly developed,
which is a problem considering today’s demand for interventions to reduce premature morbidity and
mortality. Moreover, the compilation and processing of epidemiological and biostatistical data is not
only dissatisfactory, but in some cases like e.g. in Austria also split up between regions.
5 Since the Austrian health expenditures are likely to be underestimated, the share spent on hospitals (48%) is probably overestimated. Cf. Pichler, E., Walter, E.: Finanzierung des österreichischen Gesundheitswesens, Industriewissenschaftliches Institut, Vienna, March 2002. 6 The handbook of the System of Health Accounts developed by the OECD assumes a calculation of these expenditures. Up to now, Germany, the Netherlands and Switzerland are the only European countries that have implemented this system.

HEALTH SYSTEM WATCH 2/2002 6
Public health in Austria is rooted in the Sanitation law of the Empire (Reichssanitätsgesetz) of 18707,
which is still valid today, defining the major tasks of sanitary surveillance and epidemics hygiene. A
modern public health system has to meet additional requirements such as health monitoring, health
promotion for the total population and, above all, for socially disadvantaged groups. The Austrian
system is at present on its way to become compatible with these tasks.
In France, the health reform of 1996 is considered a step towards public health, creating the
possibility to form managed care networks, so-called "réseaux". In these networks, a group of health
care providers work to provide and co-ordinate the care and health promotion for a certain group of
patients (who generally suffer from the same disease, like e.g. diabetes). Due to the possibility of
negotiating with social health insurance funds, the law enables the network to offer and reimburse for
services that normally do not fall under the social security service catalogue. Such services might be
patient information or nutritional counselling. However, only few people have made use of this
possibility so far8.
... and are closely connected with the private sector
One of the major characteristics of SHI-countries is the private provision of medical services.
Physicians offer services against payment of fees fixed by law or the administration, their amount
usually being the result of negotiations between health insurance companies and health care
providing organisations. The results of these negotiations are always contracts establishing a
public/private partnership between the private provider and the public payer. In this context, the
contracts have to be designed to guarantee both a reasonable remuneration of physicians and an
optimum of care provided for patients. One of the major problems in this context is the so-called
asymmetrical information9: Due to their lack of specialised knowledge, patients and health insurance
companies only have a limited possibility to examine what the physicians do. This means it cannot
be verified whether a physician takes the proper efforts or not. Therefore, physicians´ payments may
be higher than the corresponding services provided as profit-oriented physicians have an incentive to
restrict their efforts10.
Overview of payment mechanisms Although the development of a country's health system can be explained by its specific history and
the normative principals of health and social policies, which are derived from it, the relative
magnitude of the individual fields of services does not considerably differ between developed
countries (cf. annexed tables A1-A3). Differences are, among other things, due to the individual
7 Sablik, K.: Das Gesetz zur Organisation des öffentlichen Sanitätsdienstes in Österreich von 1870, zur Entstehungs-geschichte des Reichssanitätsgesetzes vom 30. April 1870, communication by the Austrian sanitary administration, volume 71, 1970, issue 6-7. 8 Cf. Hofmarcher, M.M., Durand-Zelinsiki, I.: Contracting and Paying Providers in Social Health Insurance Countries in Western Europe, edited by: European Observatory on Health Care Systems 2002, (being published) 9 Vgl. McGurie Th. G.: Physician Agency, in Culyer A. J., Newhouse J. P. (Ed): Handbook of Health Economics, Volume 1A: 462-517, Elsevier 2000. 10 Gaynor M., Mark T.: Physician contracting with health plans: a survey of the literature, Carnegie Mellon University, Pittsburgh, Pennsylvania, June 1999.

HEALTH SYSTEM WATCH 2/2002 7
payment mechanisms. Table 1 shows an overview of payment mechanisms in the fields of public
hospitals, generalist and specialist care as well as drugs for Austria, Germany and France.
Table 1: Payment mechanisms in Austria, Germany and France
Public hospitals Generalist and specialist
care
Drugs
Austria Per case flat rates (LKF
system), partly global budgets
Fee for service and lump
sums, physicians‘ fees
negotiated with individual
sickness funds
Degressive plan scheme
containing maximum mark-up
rates for wholesale and
pharmacy margins
France Global budgets fixed yearly
by the authorities, monthly
instalments to the hospitals
by the social health insurance
Fee for service, approx. for ¾
of physician’ centrally
determined, for ¼ fees are
determined by the market
National budgets for drugs,
two (degressive) mark-up
rates for wholesale and
pharmacy margins
Germany Per case flat rates, extra fees
(for special services and per
diem rates
A DRG system to be
introduced in 2003/2004
Global reimbursement
(amount determined by fee
for services and lump sums)
for all contract physicians of a
federal state; distribution
among physicians by point
system (EBM)
Since 1.1.2002 quality and
quantity-based target
agreements between health
insurers and physician
association; degressive
scheme containing maximum
mark-up rates for wholesale
and pharmacy margins Sources: European Observatory on Health Care Systems: Health Care Systems in Eight Countries: Trends and Challenges, April 2002 Rosian I., Habl C., Vogler S. Weigl M.: Arzneimittel, Steuerung der Märkte in der EU, ÖBIG, May 2001 Webpage AOK-Bundesverband: http://212.227.33.34/bundesverband Yukata I., et al, op.cit.; IHS HealthEcon 2002.
Different payment mechanisms...
The way health care providers are remunerated can considerably influence their behaviour. Empirical
studies have shown that payment mechanisms have a measurable influence on 11
- the form of treatment (e.g. medical vs. surgical treatment),
- the quality and quantity of medication,
- the number of treatments per physician visit or hospital day,
- the length of stay in hospital,
- the decision between out-patient or in-patient treatment of certain diseases,
- the naming of a disease and the severity degree physicians accord to it,
- the frequency of referrals to specialists and of laboratory tests.
11 Cf. Hsiao W.C., Roberts M.J., Berman P.A., Reich M.R.: Getting Health Reform Right, Harvard University, October 2000

HEALTH SYSTEM WATCH 2/2002 8
Below, the six most frequently applied payment mechanisms in the health care sector are described.
In practice, these methods are mostly combined instead of using only one of them in order to live up
to the specific requirements of the individual health care system and sector.
- Fee for service remuneration:
the single consultations or treatments such as injections, measuring the blood pressure,
laboratory tests, X-ray examinations etc. are paid.
- Per-case flat rate:
A certain package of services is paid. In the case of hospitals, for example, the stay there is paid,
regardless of its length and the treatments performed.
- Per-diem rate e:
Per diem rates are predominantly applied in the hospital sector. A certain sum has to be paid per
hospital day.
- Per capita flat rate:
A fixed sum is paid per patient and time unit (e.g. one year, a quarter or one month) regardless of
the treatment performed.
- Wages:
Particularly in the hospital sector physicians often receive annual wages.
- Global budget:
This method is often applied for paying hospital services. Hospitals receive a budget – generally
for one year – and have to provide care for all patients of a certain catchment area.
... exercise different kinds of influence on the providers’ behaviour The various payment mechanisms not only offer different "rewards“, but also influence the decision
of who has to bear the financial risk. In the case of per-capita flat rates, for example, physicians are
faced with the financial risk created by the unpredictable health condition of their patients. If an
influenza epidemic breaks out, they have to provide more services while their fees remain the same.
In the case of fee for service remuneration, this risk is born by the patients or their insurers. Tables 2
and 3 show the incentives the various payment mechanisms used with physicians or hospitals can
trigger.

HEALTH SYSTEM WATCH 2/2002 9
Table 2: Payment mechanisms for hospitals and their incentives
Payment
mechanism
Increasing the
number of
patients
Reducing the
number of
treatments per
reimbursement unit
Coding a disease
more severe than it
actually is
Choosing
healthier
patients
Fee for service
remuneration yes no yes no
Per case flat rate
(e.g. LKF) yes yes yes yes
Per-diem rate yes yes no no
Per-capita flat
rate yes yes no yes
Global budget no - - yes
Sources: Hsiao W.C., et al, op.cit., IHS HealthEcon 2002.
Table 3: Payment mechanisms for physicians and their incentives
Payment mechanism Increasing the
number of
patients
Reducing the
number of
treatments per
reimbursement unit
Coding a disease
more severe than it
actually is
Choosing
healthier
patients
Fee for service
remuneration yes no yes no
wages no - - yes
Wages + bonus for
number of patients yes - - yes
Per capita flat rate yes yes no yes
Sources: Hsiao W.C., et al, op.cit., IHS HealthEcon 2002.
If service provision is reimbursed on a fee for services basis, it is more attractive for physicians to
rate the disease in front of the patient or the insurer as more serious than it actually is, since a higher
degree of severity justifies more treatment episodes (which can be reimbursed separately). Unlike
most other payment mechanisms, this one constitutes no incentive for physicians to treat healthier
persons - on the contrary: patients who are more seriously ill need treatment more often and
therefore increase the physicians‘ income.
The system of per case flat rates is often applied in the hospital sector and consists in the payment
per hospital stay. It comprises a high risk for the hospitals since the amount reimbursed does not
depend on the severity of the case. This is why there is a tendency to reduce the number of
comprehensive and expensive treatments as far as possible and to choose healthier patients.

HEALTH SYSTEM WATCH 2/2002 10
Moreover, it is tried to reduce the length of stay in order to be able to increase the number of patients
and thus of reimbursed cases. If there are similarly defined cases (like e.g. mania without psychotic
symptoms and mania with psychotic symptoms, respectively) that are reimbursed differently, there is
a tendency to code those connected with a higher reimbursement.
Per-diem rates also predominantly occur in the hospital sector. They encourage prolonging the
length of stay, while avoiding expensive and complicated kinds of treatment, as well as the
enlargement of bed capacities in order to be able to keep more patients as long as possible.
Per capita flat rates favour a large number of patients. Since physicians and hospitals, respectively,
carry the fi nancial risk of the treatment of severe diseases, they have an incentive to pick healthier
patients in order to prevent expensive and labour-intensive treatment procedures.
Global budgets focus on motivating hospitals to apply the resources available as economically as
possible. With this form of payment hospitals bear however the financial risk of various uncertainties
such as the number of treatment episodes, costs of the individual treatment, length of stay per
patient, the number of patients etc. This is why hospitals under global budgets have an incentive to
keep case- and workload low.
Physicians who receive a fixed income face a low financial risk and therefore have no financial
motivation to keep the number of treatment episodes and patients low. What they are, on the other
hand, interested in is reducing their working burden and effort. Introducing a bonus or overtime
premium system can solve this dilemma.
The arguments stated above do not imply that physicians are only out for their own interests and try
to exploit the system as far as possible. It goes without saying that they are as well interested in the
well being of their patients. In order to guarantee the best possible payment scheme, health
insurance companies as payers have to consider the individual incentives that are generated by
different payment mechanisms. This is the more important as even the most altruistic physician
wants to earn a living.

HEALTH SYSTEM WATCH 2/2002 11
Focus: Physicians and cities: A close link*
The market of medical care, particularly the one in Social Health Insurance (SHI) countries, is characteristically split up into three main participants: physicians (supply), patients (demand) and
health insurance companies (payers). In their role as experts, physicians influence the patients’ demand for health services, which they in turn provide. By doing so they pursue in most cases not only altruistic aims, but also a target income. In the relation between social health insurers and
patients there is an incentive for patient to over-use services since their marginal cost of consumption is zero. Due to this tendency as well as an international increase in the number of physicians, health insurers as payers have to implement certain measures to regulate the amount
and price of the health care provided. Otherwise, the number of services as well as costs would explode. A high physician density may lead to higher costs than desirable. . At the same time it may guarantee high quality of health care provided for the population.
In addition to the difficulty of determining the optimal physician density, the question of regional
distribution arises. A public health system has the duty to ensure that medical care is regionally balanced and available for the whole population. If on the other hand care is provided for the respective surroundings, a regional concentration of health care providers on urban centres might
however be favourable from an overall economic point of view.
Compared to the rest of Austria, Vienna has a relatively large number of contract physicians, particularly specialists. From the point of view of health policy it is of interest to find out whether such
a difference in physician density between cities and the country also exists in other European states.
For comparing Vienna‘s physician density on a European level, cities and countries, respectively, with similar characteristics as Vienna or Austria should be chosen. Germany and France are, like Austria, SHI-countries and provide comparably high living standards. Like Vienna, the cities Lyon
and Hamburg have a medical university, and, with a population of one and a half million, Hamburg is similar to Vienna in terms of population. Despite all this, big cities cannot be tarred with the same brush. While Vienna with its more than one million inhabitants is Austria’s only metropolis, Germany
has several cities with populations exceeding one million. In addition to that, the population of Vienna accounts for a fifth of the entire population of Austria, whereas the inhabitants of Hamburg make up only 2% of the German population. France, on the other hand, is more like Austria, Paris with its
slightly more than two million inhabitants being the only metropolis. Considering all these facts, it is reasonable to include not only Lyon and Hamburg, but also Berlin and Paris into the comparison.
What makes a physician is defined differently
Even if physician densities are compared with those of other SHI-countries like Germany and
France, institutional differences regarding health care provision have to be taken into account. In
Austria and Germany, e.g., health care provision is based on benefits in-kind. This means persons
covered by health insurance are entitled to medical treatment, which is made possible by contracts
* With special thanks to the Physicians’ Chamber for Vienna for permitting us to summarize findings in the research report: Felderer, B., M.M.Hofmarcher, Ch. Lietz, M. Riedel, Ärztedichte im urbanen Umfeld (Physician density in urban settings), Institute for Advanced Studies, Vienna März 2002.

HEALTH SYSTEM WATCH 2/2002 12
between health insurers and health care providers. In France with its principle of cost reimbursement
the situation is different. Insured patients have to pay the physician’s fee which they are later (partly)
reimbursed for.
Unlike Germany and France, sickness fund patients in Austria are additionally provided with
physicians who do not hold a contract but may be seen by each enrolee at any time. Similar to
France, this means when consulting those physicians, patients can submit the receipt to the health
insurance and will be partly reimbursed for the physician’s fee. In Germany nearly all non-hospital
physicians are contracted, whereas in Austria only approximately two thirds of office-based
physicians have a contract with at least one insurance company. Ambulatory care provided by
outpatient departments of hospitals or outpatient clinics partly owned by the insurance companies
are further typically Austrian institutions. In 2000 approximately 15% of all ambulatory care cases
were treated in outpatient departments of hospitals and 2.4% in specialised outpatient clinics of
health insurance companies 12.
Austria has a relatively low physician density...
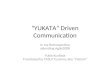
With 304 physicians per 100,000 inhabitants (considering all active physicians) Austria has a lower
physician density than Germany with 336 and France with 311 physicians per 100,000 inhabitants.
Austria’s density of agreed physicians (87 per 100,000 inhabitants) is clearly lower than the one in
Germany with a ratio of 153 (cf. figure 3). These striking differences in the number of contract
physicians can probably only partially be explained by the differences between the individual health
care systems described above.
In France contract physicians as we know them do not exist, since there are no contracts between
physicians and health insurance companies, as mentioned above. The ratios of physicians per
100,000 inhabitants indicated in figure 3 as 200 refer to office-based physicians. Comparing the
numbers with those of Austria and Germany is reasonable because in France patients can choose
their physician. This means the importance of office-based physicians in France in terms of care
provision is similar to that of contract physicians in Austria and Germany. Nevertheless, differences
between the systems of the individual countries must not be completely disregarded in such a
comparison13.
12 On the difficulty of comparing cases or case figures of the individual settings, cf. Hofmarcher, M.M., Riedel, M.: Health System Watch IV, Winter 2001/2002: Gesundheitszustand in der EU: Die EU wächst zusammen. Schwerpunktthema: Arztpraxis oder Spitalsambulanz: Ein Fall ist nicht ein Fall. 13 The number of office-based and registered physicians in France is the same per definition. In Germany, office-based and registered physicians are two different groups, but, as mentioned above, only few office-based physicians without contract exist. Therefore both groups have the same physician density (153).

HEALTH SYSTEM WATCH 2/2002 13
Figure 3: Physician density in Austria, Germany and France
304
171
87
336
153 153
311
200 200
0
50
100
150
200
250
300
350
400
active physicians office-based physicians contract physicians
phys
icia
ns p
er 1
00,0
00 in
habi
tant
s
Austria Germany France
Sources: Austria: ÖBIG, Association of Austrian insurance companies, Statistik Austria Germany: KBV, Federal Chamber of Physicians France: STATISS (DRASS, DREES) Reference year: 1999; IHS HealthEcon 2002.
... which also applies to Vienna
In Vienna there are less active physicians per capita than in Hamburg, Berlin, Lyon and Paris. As far
as contract physicians, particularly specialists, are concerned, Vienna clearly lags behind Hamburg
and Berlin. The two French cities have a higher physician density than the other cities, with Paris
showing particularly high ratios (cf. figure 4)
Figure 4: Physician density in Vienna, Hamburg, Berlin, Lyon and Paris
457
250
117
483
208 187
482
204 194
539
364 364
770
434 434
0
100
200
300
400
500
600
700
800
900
active physicians office-based physicians contract physicians
phys
icia
ns p
er 1
00,0
00 in
habi
tant
s
Vienna Hamburg Berlin Lyon Paris
Sources: Austria: ÖBIG, Association of Austrian Insurance Companies, Statistik Austria Germany: KBV, Federal Chamber of Physicians France: STATISS (DRASS, DREES), DDASS du Rhône Reference year: 1999; IHS HealthEcon 2002.

HEALTH SYSTEM WATCH 2/2002 14
Cities have a considerable physician surplus ...
In all five cities the physician density is clearly higher than in the surrounding area or the rest of the
country, respectively. Paris ranks first in terms of physician density with over two-and-a-half times
more active physicians per capita than France. Lyon ranks second, Vienna third immediately after
the two French cities, but clearly in front of Hamburg and Berlin. Vienna has 72% more active
physicians per capita than the rest of Austria, in Hamburg and Berlin the number is approximately
45% higher than for entire Germany. Regarding agreed physicians, the gap is less profound, but with
47% more physicians per capita in Vienna still obvious (Hamburg: 23%, Berlin: 29%) (cf. figure 5).
The fact that it is Vienna and Paris that have particularly high physician densities is probably a kind
of "metropolis effect“: Both cities are singular in terms of number of inhabitants within the two
countries.
Figure 5: Comparison of physician densities in cities and the country
172% 164%147%145% 137%
123%146%
135% 128%
174% 183% 183%
262%
227% 227%
0%
50%
100%
150%
200%
250%
300%
actice physicians office-based physicians contract physicians
ratio
Vienna / Austria (without Vienna) Hamburg / Germany (without Hamburg)
Berlin / Germany (without Berlin) Lyon / France (without Lyon)Paris / France (without Paris)
Sources: Austria: ÖBIG, Association of Austrian Insurance Companies (Verband der Versicherungsuntern. Österreichs), Statistik Austria Germany: KBV, Federal Chamber of Physicians France: STATISS (DRASS, DREES), DDASS du Rhône Reference year: 1999; IHS HealthEcon 2002
... even when considering the care provided to surrounding areas The assumption that cities have higher physician densities because they also provide care for their
surroundings can be examined by comparing the surroundings with the entire state. The assumption
proves absolutely true if the physician density of the city and its surroundings is exactly the same as
that of the rest of the country14. In the case of Austria, the physician density of Vienna, Lower Austria
14 This implies that a city provides care only for its own surroundings. The inhabitants of the province of Vorarlberg, e.g., are not supposed to consult a specialist in Vienna. This care provision for the surroundings however seems to play a minor role among office-based physicians.

HEALTH SYSTEM WATCH 2/2002 15
and Burgenland, the two provinces being defined as catchment area of Vienna, would have to
correspond to the density of western Austria (which is Austria without Vienna, Lower Austria and
Burgenland).
As shown in figure 6, the cities’ higher physician densities can hardly be explained exclusively by
providing care for the surrounding regions. Vienna and its surrounding provinces Lower Austria and
Burgenland have 30% more active physicians and 22% more contract physicians per capita than the
rest of Austria. For Paris and its surroundings the situation is similar. In German cities and their
surroundings the gap is less pronounced, but still obvious. All this shows that despite a rather
generous definition of the surroundings – the provinces Lower Austria and Burgenland being quite a
large catchment area for Vienna - the cities‘ higher physician densities are unproportionally high.
Figure 6: Care provision for the surroundings: Comparison of physician densities in the
surroundings and the country
130%
143%
122%125%135%
124% 124%
108%
114%118% 110%112%117%109%109%
0,000
0,200
0,400
0,600
0,800
1,000
1,200
1,400
1,600
active physicians office-based physicians contract physicians
ratio
Vienna+Lower A.+Burgenland / (rest of) Austria Hamburg+Schl.-Holst. / (rest of) GermanyBerlin+Brandenburg / (rest of) Germany Rhône (incl.Lyon) / (rest of) FranceÎle-de-France (incl.Paris) / (rest of) France
Sources: Austria: ÖBIG, Association of Austrian Insurance Companies, Statistik Austria Germany: KBV, Federal Chamber of Physicians France: STATISS (DRASS, DREES), DDASS du Rhône Reference year: 1999; IHS HealthEcon 2002
Other possible reasons for the disparities between cities and the country
Disparities between the physician densities of cities and the country depend to a large extent on the
individual physician‘s choice of location. This can in turn be influenced by different motivations and
circumstances: A high demand for medical care caused by a higher number of potential patients in a
certain location justifies a higher physician density. Generally it may be assumed, that the better the
medical infrastructure (comprising e.g. a teaching hospital, continuous education programmes etc.),
the greater the motivation to choose a certain location.

HEALTH SYSTEM WATCH 2/2002 16
A further factor physicians consider when choosing a certain location is the personal quality of life.
Physicians in rural areas often have to care for a relatively large catchment area, whereas physicians
in cities can share stand-by and emergency services with their colleagues and other providers. In
France, for example, the coast region and large cities have high physician densities, whereas some
rural regions are nearly underprovided for.
The cities‘ surplus is almost exclusively due to the surplus of specialists...
Vienna has twice as many specialists per capita than the rest of Austria. In Paris the number is even
three times, in Lyon two-and-a-half times as high as in France. Hamburg and Berlin each have one-
and-a-half times more specialists than Germany. The density of general practitioners, on the other
hand, is not that much higher than in the rest of the country. At least this is the case for Vienna,
Hamburg and Berlin (cf. figure 7).
Figure 7: Comparison of general practitioners and specialists in cities and the entire state
0,0
0,5
1,0
1,5
2,0
2,5
3,0
3,5
generalpractitioners
specialists generalpractitioners
specialists generalpractitioners
specialists
active physicians office-based physicians contract physicians
ratio
Vienna / Austria (without Vienna) Hamburg / Germany (without Hamburg)Berlin / Germany (without Berlin) Lyon / France (without Lyon)Paris / France (without Paris)
Sources: Austria: ÖBIG, Association of Austrian Insurance Companies, Statistik Austria Germany: KBV, Federal Chamber of Physicians France: STATISS (DRASS, DREES), DDASS du Rhône Referenc e year: 1999; IHS HealthEcon 2002
... and can be observed for all specialities
The higher specialist density in Vienna can be observed in almost all specialities. Except in the fields
of neurology and psychiatry, in Vienna there are at least two-and-a-half times more contracted
specialists per capita than in Austria. Vienna is particularly well equipped with contract specialists in
physical medicine, whose number is ten times higher than in the rest of Austria. The number of
contracted radiologists and orthopaedists is more than three times as high as the value for entire
Austria. In dentistry, which is most important in terms of quantity, Vienna has 70% more contracted
specialists than the rest of the country.

HEALTH SYSTEM WATCH 2/2002 17
Is Vienna overprovided or Austria underprovided for?
Despite its surplus of physicians compared with the rest of Austria, Vienna has a lower physician
density than Hamburg and Berlin. This may suggest that Austria‘s rural regions are provided with
much less contracted specialists per capita than rural regions in Germany. The German Land
Schleswig-Holstein, for example, has a density of contract specialists that is almost three times as
high as that of Lower Austria and Burgenland.
Per capita spending for medical care is higher in cities... The health insurers‘ per-capita spending15 for cities is higher than their spending for the country. In
Vienna, per-capita spending is 17% higher than in the rest of Austria. With this value Vienna ranks
second after Paris with a 26% difference. In Hamburg, the expenditure is 11%, in Berlin 7% higher
than in the rest of Germany (cf. figure 8).
... but less pronounced than the physician surplus ... As for the health insurance companies‘ per-capita spending for medical services, the difference
between cities and the country is less pronounced than that of physician density. In Vienna, the
contract-physician density is 47% higher than in the country, whereas the health insurance’s per-
capita spending is “only“ 17% higher than in the rest of Austria (cf. figure 8).
Figure 8: Medical-care spending vs. physician density in cities and in the country
Vienna /Austria
Hamburg /Germany
Berlin /Germany
Paris /France
S1 S2
147%123% 128%
227%
117% 111% 106%126%
0,000
0,500
1,000
1,500
2,000
2,500
ratio
Sources spending: Austria: Annual reports of the regional health insurance companies (GKK), Statistisches Handbuch der österreichischen Sozialversicherung (statistical handbook of the Austrian social insurance); Germany: federal health monitoring; France: CREDES: Eco-Santé 2001 (demo version); Reference year: 1998; France: projection of the year 1990–1995 Sources density of registered physicians: Austria: ÖBIG; Germany: KBV; France: STATISS (DRASS, DREES); Reference year: 1999
15 The values indicated for Austria refer to the expenditure of the nine regional health insurance companies, which cover approx. 80% of insured Austrians. For Germany, the expenditure of the general local health insurance companies (AOKs) is indicated, the AOKs covering the majority (almost 40%) of Germans with national insurance. The values for France correspond to the expenditure of the „Régime Géneral“, the health insurance for employees, which covers approx. 80% of the population. Since the health insurance companies effect the expenditure, the per-capita calculations refer to the number of sickness fund enrolees (exclusive the dependents)

HEALTH SYSTEM WATCH 2/2002 18
... which has its reasons
The higher density of specialists in big cities is indeed justified, particularly if there is a medical
university like in Vienna. In Austria, approximately one third of physicians who carry out research
work in teaching hospitals do this in Vienna, and more than half of medical students study there. The
proximity to research locations makes Vienna attractive both for physicians working in the field of
research and their colleagues who can benefit from further education facilities they find there.
Moreover, social bounds established during their studies and training period might facilitate the
exchange of professional experience. Furthermore, the university infrastructure offers an easier
access to state-of-the-art medical-technological equipment, for approximately one third of large
medical devices in Austria are located in Vienna.
All this combines to facilitate the physicians‘ work and to guarantee high quality of care to the benefit
of the patients. The disadvantage of a higher physician density is however the higher per-capita
spending of the health care system, which has been shown by empirical studies also in other
countries. To a certain extent, this phenomenon is also a consequence of the demand created by the
supply.

HEALTH SYSTEM WATCH 2/2002 19
Table A1: Expenditure on hospital care spending in per cent of total expenditure on health Index EU15=100 1990 1995 1996 1997 1998 1999 1990 1995 1996
Austria*** 43,4 44,6 43,4 49,0 48,2 48,6 108 113 112 Belgium 32,8 33,3 34,4 34,6 n.av. n.av. 82 84 89 Denmark 56,7 55,0 55,3 54,7 54,3 53,9 141 139 143 Germany 34,7 34,7 34,1 33,6 34,0 n.av. 87 88 88 Finland 44,7 42,0 41,8 41,4 41,1 40,7 112 106 108 France 46,0 45,5 45,5 45,4 44,6 43,8 115 115 118 Greece 28,4 24,8 3) n.av. n.av. n.av. n.av. 71 63 n.av. Ireland** 52,4 53,3 52,0 52,3 50,1 n.av. 131 135 135 Italy 42,7 44,8 41,7 42,6 41,4 41,3 107 113 108 Luxembourg 26,4 31,3 32,4 36,0 30,7 29,8 66 79 84 Netherlands 50,5 50,6 51,1 52,8 52,8 52,7 126 128 132 Portugal** 29,5 33,6 35,7 n.av. n.av. n.av. 74 85 93 Sweden** 49,8 42,1 n.av. n.av. n.av. n.av. 124 106 n.av. Spain 44,1 45,2 44,8 n.av. n.av. n.av. 110 114 116 United Kingdom** 29,2 29,5 25,3 26,1 n.av. n.av. 73 74 66
EU15* 40,1 39,6 38,6 n.av. n.av. n.av. 100 100 100 EU12* 41,1 40,7 40,3 n.av. n.av. n.av. 102 103 105
Switzerland 49,5 50,7 50,9 50,8 50,3 n.av. 124 128 132 USA 44,9 43,1 42,7 42,1 41,3 40,5 112 109 111
Bulgaria 53,0 2) 59,0 n.av. n.av. n.av. n.av. 132 149 n.av. Estonia n.av. n.av. n.av. n.av. n.av. 35,4 n.av. n.av. n.av. Latvia 78,0 62,0 58,0 56,7 51,6 51,9 195 157 150 Lithuania n.av. n.av. n.av. n.av. 41,6 n.av. n.av. n.av. n.av. Malta n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. Poland** 34,8 1) 33,7 33,1 34,7 31,7 31,3 n.av. 85 86 Romania n.av. 59,0 58,0 63,0 n.av. n.av. n.av. 149 150 Slovakia 32,1 43,0 44,0 44,8 48,2 47,0 80 109 114 Slovenia 42,9 49,1 49,7 48,9 47,2 47,7 107 124 129 Czech Republic n.av. 29,6 33,8 35,6 35,4 35,1 n.av. 75 88 Turkey 33,4 28,7 28,2 28,8 29,3 n.av. 83 72 73 Hungary 59,7 54,8 53,1 n.av. n.av. n.av. 149 138 138 Cyprus n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av.
*Average weighted on the total health care spending **Only public spending *** Spending for fund hospitals 1)1991, 2)1992, 3)1994 Sources : WHO Health for all database, January 2002; OECD Health Data, August 2001 for Ireland, Portugal, Sweden, United Kingdom, USA and Poland; Health Care Systems in Transition (HiT) for Lithuania and Switzerland; Austria: Federal Ministry of Social Security and Generations, health care spending according to Statistik Austria, Jänner 2002; IHS HealthEcon 2002.

HEALTH SYSTEM WATCH 2/2002 20
Table A2: Expenditure on pharmaceuticals in per cent of total expenditure on health Index EU15=100 1990 1995 1996 1997 1998 1999 1990 1995 1996 1997 1998
Austria 13,2 10,4 10,6 12,9 14,1 n.av. 81 64 65 78 84 Belgium 15,5 16,2 15,4 16,1 n.av. n.av. 95 100 94 97 n.av. Denmark 7,5 9,1 8,9 9,0 9,2 9,0 46 56 55 54 55 Germany 14,3 12,3 12,4 12,2 12,7 n.av. 88 76 76 74 76 Finland 9,4 14,0 14,4 14,8 14,6 15,1 58 86 88 89 87 France 20,0 21,0 21,0 21,3 21,9 22,8 123 129 129 129 130 Greece 14,5 17,3 17,9 17,2 14,7 13,5 89 107 110 104 87 Ireland 11,1 9,5 9,5 9,3 9,9 n.av. 68 59 58 56 59 Italy 21,2 20,9 21,1 21,4 21,9 22,1 130 129 129 129 130 Luxembourg 14,9 12,0 11,5 12,6 12,3 11,7 91 74 70 76 73 Netherlands 9,1 10,4 10,4 10,3 10,8 11,0 56 64 64 62 64 Portugal 24,9 25,2 26,3 26,9 25,8 n.av. 153 155 161 162 153 Sw eden 8,0 12,5 12,9 12,8 n.av. n.av. 49 77 79 77 n.av. Spain 17,8 19,6 20,0 20,7 n.av. n.av. 109 121 122 125 n.av. United Kingdom 13,6 15,4 15,7 16,3 n.av. n.av. 83 95 96 98 n.av.
EU15* 16,3 16,2 16,3 16,6 16,8 n.av. 100 100 100 100 100 EU12* 17,2 16,6 16,7 16,9 17,0 n.av. 105 102 102 102 101
Switzerland 8,2 7,7 7,6 7,7 7,6 n.av. 50 47 47 46 45 USA 9,2 8,9 9,2 9,6 10,1 11,0 56 55 56 58 60
Bulgaria 12,3 17,4 23,5 23,4 23,8 n.av. 75 107 144 141 141 Estonia n.av. n.av. 17,0 17,0 16,6 22,7 n.av. n.av. 104 103 99 Latvia n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. Lithuania n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. Malta 16,0 15,0 15,0 22,0 n.av. n.av. 98 92 92 133 n.av. Poland 12,6 15,6 8,9 n.av. n.av. n.av. 77 96 55 n.av. n.av. Romania 11,0 1) 17,0 19,0 17,0 20,0 n.av. 68 105 116 103 119 Slovakia 16,8 28,0 30,1 29,7 28,7 28,3 103 173 184 179 171 Slovenia 10,4 18,9 17,4 17,9 18,9 19,0 64 116 107 108 112 Czech Republic 21,0 25,6 25,5 25,3 25,5 27,0 129 158 156 153 152 Turkey 20,5 30,1 26,3 27,8 34,7 n.av. 126 186 161 168 207 Hungary 5,0 25,0 26,3 26,4 26,5 25,5 31 154 161 159 158 Cyprus n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av.
* Average weighted on the total health care spending 1)1992 Sources: WHO Health for all database, January 2002; OECD Health Data, August 2001 for the USA; Health Care Systems in Transition (HiT) for Bulgaria, Malta, Poland and Slovakia; IHS HealthEcon 2002.

HEALTH SYSTEM WATCH 2/2002 21
Table A3: Expenditure on physician services in per cent of total expenditure on health 1990 1995 1996 1997 1998 1999
Austria 18,3 18,2 17,7 19,4 19,2 19,0 Belgium** 18,6 15,3 15,9 n.av. 12,8 12,8 Denmark 15,8 16,0 15,7 15,7 15,7 15,2 Germany 17,7 16,7 16,4 17,0 17,0 n.av. Finland 25,1 24,7 24,6 24,2 24,4 24,4 France 11,8 11,7 11,6 11,7 11,7 11,7 Greece 12,4 10,8 3) n.av. n.av. n.av. n.av. Ireland 15,1 2) n.av. n.av. n.av. n.av. n.av. Italy 19,7 21,8 3) n.av. n.av. n.av. n.av. Luxemburg 21,6 14,2 3) 12,6 13,2 12,2 n.av. Netherlands 9,1 8,1 3) 8,0 7,8 7,7 7,8 Portugal n.av. n.av. n.av. n.av. n.av. n.av. Sweden 14,4 12,4 3) n.av. n.av. n.av. n.av. Spain 16,2 1) 15,5 2) n.av. n.av. n.av. n.av. United Kingdom 14,9 14,8 3) n.av. n.av. n.av. n.av.
EU15* n.av. n.av. n.av. n.av. n.av. n.av. EU12* n.av. n.av. n.av. n.av. n.av. n.av.
Switzerland 17,5 17,5 17,3 17,5 17,7 n.av. USA 23,1 22,7 22,5 22,4 22,6 22,7
Bulgaria n.av. n.av. n.av. n.av. n.av. n.av. Estonia n.av. n.av. n.av. n.av. n.av. n.av. Latvia n.av. n.av. n.av. n.av. n.av. n.av. Lithuania n.av. n.av. n.av. n.av. n.av. n.av. Malta n.av. n.av. n.av. n.av. n.av. n.av. Poland n.av. n.av. n.av. n.av. n.av. n.av. Romania n.av. n.av. n.av. n.av. n.av. n.av. Slovakia n.av. n.av. n.av. n.av. n.av. n.av. Slovenia n.av. n.av. n.av. n.av. n.av. n.av. Czech Republic n.av. n.av. n.av. 24,5 22,9 22,0 Turkey n.av. n.av. n.av. n.av. n.av. n.av. Hungary n.av. n.av. n.av. n.av. n.av. n.av. Cyprus n.av. n.av. n.av. n.av. n.av. n.av.
1)1991, 2)1992, 3)1994 * weighted on the total health care spending; **only public spending Source: OECD Health Data, August 2001; IHS HealthEcon 2002.

HEALTH SYSTEM WATCH 2/2002 22
Table A4: Characteristic features of care provision, 1999 or most recent year available Admission rate in per
cent Average length of
stay in days Treated cases/bed FTE staff per bed Physicians per
1,000 inhabitants Dentists per
1,000 inhabitants Pharmacists per 1,000 inhabitants
Physician's visits per capita
Austria 27,7 a) ** 7,9 42,5 2,1 3,0 0,5 0,5 6,7 Belgium 19,8 c) 11,4 a) 38,1 b) 1,5 h) 4,1 0,7 a) 1,4 a) 7,9 Denmark 19,0 a) 7,3 a) 54,9 a) 3,5 b) 2,8 0,9 0,5 5,8 Germany 21,6 a) 12,0 a) 30,1 1,5 3,5 0,8 0,6 6,5 c)
Finland 27,3 10,5 30,8 d) 2,1 g) 3,1 0,9 1,5 4,3
France 22,8 d) 10,8 b) 48,9 1,1 3,2 0,7 1,0 6,5 c)
Greece 15,0 d) 8,6 b) 30,9 i) 1,4 e) 4,3 1,1 n.av. n.av.
Ireland 14,8 a) 7,6 46,6 3,1 2,3 0,5 0,8 n.av.
Italy 17,6 a) 8,0 a) 36,2 a) 2,2 a) 5,7 0,6 1,0 6,0
Luxemburg 19,4 e) 15,3 c) n.av. n.av. 2,5 0,6 0,7 a) 2,8 a)
Netherlands 9,6 a) 13,1 26,8 a) 2,5 b) 3,1 0,5 0,2 5,8
Portugal 12,0 a) 9,0 a) 37,8 a) 3,1 a) 3,2 0,4 b) 0,8 3,4 a)
Sweden 18,0 c) 7,5 c) 42,0 c) n.av. 3,1 1,5 a) 0,7 2,8 b)
Spain 11,4 c) 10,0 c) 35,5 c) 1,6 c) 3,1 b) 0,4 g) 0,7 n.av.
United Kingdom 15,1 a) 9,8 c) 60,2 a) 3,7 a) 1,6 f) 0,4 0,6 g) 5,4 a)
EU 15* 18,1 10,2 40,7 2,1 3,4 0,6 0,8 6,0 EU 12* 18,7 10,4 36,6 1,7 3,8 0,6 0,8 6,2
Switzerland 17,0 a) 14,0 a) 21,5 i) 2,0 g) 3,4 0,5 a) 0,6 a) 11,0 g)
USA 12,5 7,0 38,9 4,6 2,7 a) 0,6 a) 0,7 c) 5,8 c)
Bulgaria 15,8 11,9 21,1 n.av. 3,4 0,6 0,2 5,7
Estonia 19,6 9,9 28,2 n.av. 3,1 0,7 0,6 6,3
Latvia 22,1 11,8 25,4 n.av. 3,1 0,5 n.av. 7,0
Lithuania 24,5 11,3 28,1 n.av. 3,9 0,6 0,6 4,5
Malta 20,2 b) 4,6 b) n.av. n.av. 2,6 0,4 1,8 n.av. Poland 13,8 a) 9,3 26,1 n.av. 2,3 0,3 0,5 5,3 Romania 20,7 9,5 n.av. n.av. 1,9 0,2 0,1 8,0
Slovakia 19,4 10,4 26,0 n.av. 3,2 0,5 0,4 13,5
Slovenia 16,6 9,0 30,9 n.av. 2,2 0,6 0,3 6,8
Czech Republic 19,4 11,6 30,4 n.av. 3,1 0,6 0,5 12,3 Turkey 7,6 6,0 36,4 1,5 1,3 0,2 0,3 2,1 Hungary 25,4 9,2 33,5 1,3 3,6 0,6 0,5 21,1 Cyprus n.av. n.av. n.av. n.av. n.av. n.av. n.av. n.av.
Accession13* 14,1 8,4 31,3 n.av. 2,1 0,3 0,4 6,1 MOEL10* 18,1 9,9 27,3 n.av. 2,6 0,4 0,4 8,6
a) 1998; b) 1997; c) 1996; d) 1995; e) 1994; f) 1993; g) 1992; h) 1991; i)1990 *average weighted on the population 1999, **cases Sources: WHO health for all database, January 2002; OECD Health data, August 2001 for cases/bed, FTE staff and physician's visits and USA all codes Health Care Systems in Transition (HiT) for admission rate and average length of stay in Malta; M. Schneider, G. Cerniauskas, L. Murauskiene: Health Systems of Central and Eastern Europe for treated cases and physician's visits in BUL, EST, LAT, LIT, POL, ROM, SLK and SLO; IHS HealthEcon 2002.