Embed Size (px)
DESCRIPTION
Published annually this publication provides detailed facts and figures about healthcare in Ireland and the pharmaceutical and healthcare industry both nationally and globally across the following areas: Healthcare Today, Self-Care Today, Demographic Trends, Healthcare Tomorrow, The Medicines Industry, Medicines in the Community and Medicines and Global Health
Citation preview

Healthcare Facts and Figures
2009

All facts and figures were correct at time of going to print (February 2009)

The Irish Pharmaceutical HealthcareAssociation (IPHA) represents theinternational research-basedpharmaceutical industry in Ireland. Its member companies include bothmanufacturers of prescriptionmedicines and non-prescription orconsumer health care medicines.
IPHA
2009 Healthcare Facts and Figures
1

2
IntroductionAs outlined in this latest edition of Healthcare Facts and Figures the
cost of developing a new medicine has increased from €149 million in
1975 to €1,059 million in 2006. It is also taking longer to bring a new
medicine from the laboratory to a patient.
As impressive as advances in pharmaceuticals have been, our work is
far from over. Thousands upon thousands of people with serious
diseases and conditions, and a healthcare system struggling with
rising costs can benefit from new medicine discoveries.
In this context it must be recognised that it is the medicines of today
that inevitably pay for the medicines of tomorrow.
We are on the verge of a new era of personalised and tailored
medicine that holds great promise for patients and the healthcare
system. That promise, however, is not a given and depends on
sustained, substantial investment in R&D, a supportive public policy
environment and an appropriate regulatory framework.

2009 Healthcare Facts and Figures
3
New medicines help patients to recover from ill health, faster and
more fully. They make it possible to prevent or slow the development
of many diseases, turning for example, previously fatal illnesses into
manageable chronic conditions and helping avoid the discomfort of
invasive surgery. They also offer cost savings and improve efficiency,
delivering financial benefits to the whole healthcare system, through
optimal management and reduction of treatment times,
hospitalisation and time off work. These advances have immeasurably
improved the lives of Irish patients, as well as their families and care
givers.
The encouragement of innovation in medicines, in how we deliver
medicines and in how we deliver healthcare is central to the
improvement of our healthcare system, of patient health and of our
country’s economic development and needs to continue to be
rewarded.
Dr Gerald Farrell
IPHA President

4
Healthcare Today 6Public Expenditure on Health 1998-2009
Health Expenditure as a % of GDP 2007
State Expenditure on Medicines 2000-2007
Pharmaceutical Expenditure as a % of Healthcare Expenditure inSelected Countries
Pharmaceutical Expenditure per Capita in Western Europe 2007
Number of Day Cases Treated in Ireland 1997-2007
Self-perceived Health Status by Age Group 2007
Prevalence and Burden of Chronic Disease
Self-Care Today 16Self Medication Market in Ireland 2007
OTC Medicines as a % of the Total Pharmaceutical Market 2007
Demographic Trends 20Population projections 2006-2036
Comparison of Age-Related Public Expenditure
Main Causes of Death in Ireland 2007
Healthcare Tomorrow 26Evolution of Innovative Medicines
Medicines Life Cycle
Cost of Developing an Innovative Medicine
Benefits of Innovative Medicines
Contents

2009 Healthcare Facts and Figures
5
Need for Continued Medicines Innovation
Business Sector R&D in Ireland
Changes in Location of Pharmaceutical Industry Research Sites in thePeriod 2001 – 2006
The Medicines Industry 36Leading Pharmaceutical Companies by Sales in Ireland and Globally
Distribution of Global Pharmaceutical Sales by Region
9 of the World’s Top 15 Medicines are Produced in Ireland
World Trade in Pharmaceuticals 2006
Medicines in the Community 42Community Medical Schemes Expenditure 2007
GMS Scheme Expenditure and % Growth Rate 1998-2007
Ageing of the GMS Scheme 1994-2007
Drugs Payment Scheme Expenditure 1999-2007
High Tech Scheme Expenditure 1999-2007
Long Term Illness Scheme Expenditure 1999-2007
Making Headroom for Innovation
Medicines and Global Health 52Industry Supported Public-Private Partnerships in the Developing World
Number of Positive Health Interventions made in the Developing World
Map of Pharmaceutical Locations in Ireland 56

6
Healthcare• The last decade has seen an unprecedented increase in health
expenditure following a period of cutbacks and stagnation in the1980’s and the early 1990’s. Public expenditure on health will havealmost quadrupled in the period 1998 to 2009.
• Healthcare expenditure in Ireland, relative to other EuropeanStates, is coming from a low base. Irish expenditure in 2007, as apercentage of GDP, is the lowest alongside Luxembourg in the EU.
• The Irish healthcare system remains a mix between publicexpenditure (75%) and private expenditure (25%). Over 50% ofthe population now have some form of private health insurance.
• The numbers employed in the health services increased by over60% between 1997 (68,084) and 2007 (111,505).
• State expenditure on medicines has increased in tandem with theincrease in public expenditure on healthcare. Medicines accountfor just 14.7 % of total healthcare expenditure – a small but vitalcomponent.
• Irish consumption of medicines remains amongst the lowest inWestern Europe. Growth in the Irish market has to be viewedagainst this background and against the ever-increasing sumsbeing invested to improve public health.

Today
2009 Healthcare Facts and Figures
7
• The pharmaceutical industry has recognised that the State faces achallenge in funding healthcare going forward and has agreedrobust, cost effective arrangements for the supply of medicines tothe health services. The State has estimated that thesearrangements will result in savings of €300 million in the Statemedicines bill in the period through to September 2010, savingswhich will provide the State with the monies to fund newtherapies which offer hope to patients of longer, healthier, moreactive lives.

8
Public Expenditure on Health 1998-2009
0
2
4
6
8
10
€ (B
illio
ns)
12
14
16
18
1998
Source: Department of Health and Children Statistics * Budget provision for 2009
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009*
4.1
4.9
5.7
7.2
8.4
9.1
10.1
11.9
13.1
15.1
16.216.34

9
Health Expenditure as a % of GDP 2007
0 2 4 6%
8 10 12
Source: OECD Health Data 2007 (e) Estimate
7.5
7.5
8.2
8.4
8.4
8.9
9
9.1
9.2
9.5
10.1
10.2
10.4
10.6
11.1
11.3
Ireland
Luxembourg
Finland
Spain
UK
OECD
Italy
Greece
Sweden
Denmark
Austria
Portugal
Belgium
Germany
France
Switzerland

10
State Expenditure on Medicines 2000-2007
0
200
400
600
800
1000
€ (
Mill
ions
)
% G
row
th
1200
1400
1600
1800
2000
Source: GMS/PCRS Annual Reports from 2000– 2007. The GMS figure excludes VAT and the Hi-Tech Scheme figure excludes patient care fees.
2001 2002 2003 2004 2005 2006
565
718
867
120221
27
22
17
18
11
15
11
1332
1529
20070
5
10
15
20
25
301701
1022
Euro (Millions)
% Growth Rate

11
Pharmaceutical Expenditure as a % ofHealthcare Expenditure in Selected Countries2006
0 5 15%
252010
Source: OECD In Figures 2008* IPHA calculation
14.6
21.7
21.3
20
17.6
17.6
16.9
16.4
14.8
14.7
13.3
12.4
8.5
Spain
Portugal
Italy
Greece
OECD
Belguim
France
Germany
Ireland*
Finland
Sweden
Austria
Denmark

12
Pharmaceutical Expenditure per Capita in Western Europe2007
0 100 300US Dollars ($)
500400 600 700200
Source: OECD Health Data 2008
276
320
351
366
380
384
399
404
409
436
441
467
498
509
515
589
Denmark
Ireland
Sweden
UK
Finland
Netherlands
Norway
OECD
Austria
Switzerland
Portugal
Luxembourg
Germany
Italy
Spain
France

0
100,000
200,000
300,000
400,000
500,000
600,000
Source: Department of Health and Children Health Statistics 2005; HSE Annual Reports 2006 – 2007
1997 1999 2001 2003 2005 2007
249,000
297,000
358,000
449,000
512,000
590,000
13
Number of Day Cases Treated in Ireland 1997-2007

14
Self-perceived Health Status byAge Group 2007
0
10
20
30
40
50%
60
70
80
90
100
Source: Health Status and Health Service Utilisation Q3 2008, Central Statistics Office * SLAN 2007 Report (Survey of Lifestyle, Attitude & Nutrition)
18-24 25-34 35-44 45-54 55-64 65-69 70+ All
Bad/Very Bad Fair Good Very Good
This is in a country where 1 in every 4 persons is obese andevery 2nd person is overweight*.

• Chronic diseases such as diabetes, hypertension, heart disease andstroke are a large and growing burden on the health of Irish peopleand the Irish healthcare system. In the United States it is estimatedthat chronic diseases are responsible for about two-thirds of the risein healthcare spending over the last 15 to 20 years.
• The rising prevalence of chronic disease is partly the result of apopulation that is ageing and increasingly obese.
• Today, approximately 25% of the Irish population have a chronicdisease accounting for 78% of the country’s healthcare spending.
• Approximately 80% of GP consultations and 60% of hospital daysare related to chronic disease and their complications making thosepeople the most frequent users of healthcare in Ireland.
• 2 out of 3 patients admitted as medical emergencies haveexacerbations of chronic disease and 60% of deaths are as a resultof a chronic disease.
• Chronic diseases can be disabling and reduce a person’s quality oflife, especially if left undiagnosed or untreated. For example, every30 seconds, somewhere in the world a lower limb is amputated as aconsequence of diabetes.
• There is a significant increase predicted in chronic disease due to theestimated doubling of the elderly population over the next 30 years.This has implications for the healthcare system, if the current trendscontinue, bed requirements in hospitals will increase by 50-60%over the next 15 years.
• Many of the consequences and costs of chronic disease areavoidable through screening, early intervention, behaviour changeand the elimination of key risk factors such as poor diet, inactivityand smoking.
2007 2008 Healthcare Facts and Figures
15
Prevalence and Burden of Chronic Disease

Self-Care• Consumers want to actively manage their own health and are
taking greater individual responsibility for their healthcare andhealth choices.
• The health, social and economic benefits of responsible self-medication are well known and have been extensively reported.1
– Patients and consumers benefit due to wellness, enhancedproductivity and improved health in terms of prevention andincreased patient satisfaction as a result of being able toobtain the correct medication directly.
– Employers gain by having employees attend work when theymight otherwise have stayed at home.
– General Practitioners save time which enables them to betteruse that time for those patients with complicated or seriousillnesses. A recent report estimated that 51.4 million GPconsultations in the UK were solely for minor ailments. Itestimated that this represented 18% of a GP’s workload.Furthermore it estimated that the total cost to the NHS ofthese consultations was €2.5 billion and 80% of this cost(€2.15 billion) related to the cost of the GP’s time.2 It alsopresents more of an opportunity for doctors to educatepatients about common ailments and diminishes patientexpectations of a prescription for every visit.
– Pharmacists play a more active advisory role using their skilledknowledge of medicines and expertise in advising onsymptoms.
– Consumers pay less visits to accident and emergencydepartments and doctor surgeries. This in turn reduces thenumber of prescriptions, most of which are paid for, directly orindirectly, by the State.
161 E.g. Guiding Principles in Self-Medication: WSMI: http://www.wsmi.org/publications.htm 2 Minor ailments cost the NHS £2 billion/year. Pharm J 2008; 280:1090

2009 Healthcare Facts and Figures
Today• The Association of the European Self-Medication Industry (AESGP)
has estimated that savings of over €75 million annually could beachieved in Ireland if self-medication was practised more widely.The savings could then be put to better use elsewhere in thehealthcare system.
• Self-medication is an important element of the total Irish marketfor pharmaceutical products. The leading areas of the marketinclude analgesics (23%), cough and cold treatments (17%) and vitamins and minerals (12%).
17

18
Self Medication Market in Ireland 2007
Source: IMS Health, 2008 * At consumer price level
Analgesics 23%
Cough & Cold 17%
Vitamins & Minerals 12%
Digestives & Intestinal Remedies 10%
Skin Treatment 10%
Smoking Cessation 7%
Others 22%
Total Market: €315 m*

2007 2008 Healthcare Facts and Figures
19
0 2 6%108 12 14 16 18 204
Source: AESGP Economic and Legal Framework for Non-Prescription Medicines 2008
7.5
8.2
8.9
9.3
10.9
11.2
12.1
12.3
15.1
16.0
16.0
17.3
19.1
Portugal
Spain
Denmark
Sweden
Finland
Italy
Austria
Netherlands
Belgium
Ireland
Germany
UK
France
OTC Medicines as a % of the TotalPharmaceutical Market 2007

Demograp• The population of the Republic of Ireland increased by nearly
325,000 in the four year period April 2002 to April 2006. Havingonly recently passed 4 million, the population is set to exceed 5million within the next 15 years and projected to rise to 5.8m by2036.
• With an average age of 35.6 years Ireland has a relatively youthfulage structure; however this is set to change. Those aged 65 andover will account for 20% of the population (1.14 million) by 2036as against just 11% of the population (430,000) in 2001 and thenumber of those aged 80 and over is set to treble from a 2001level of 98,000 to 320,000 in 2036. These changes will havesignificant implications for public spending and in particularhealthcare expenditure as the elderly typically require 2–5 timesas many resources as those under 65.
• The life expectancy of those over the age of 65 has improvedsignificantly in recent years but remains low by comparison to ourWestern European neighbours.
• Circulatory diseases continue to be the principal cause of death inIreland and along with cancer account for nearly two thirds of alldeaths.
• Approximately one in five deaths in Ireland is of a person agedless than 65 years old.
20

2009 Healthcare Facts and Figures
21
hic Trends

22
Population Projections 2006-2036
0
1
2
3
4
5
6
Mill
ions
Year
2006
Source: Central Statistics Office
2011 2016
All
2026 2031 2036
4,200,0004,500,000
4,900,000
5,100,000
5,400,000
5,600,0005,800,00
466,000 531,000 631,000 741,000 866,000
1,002,0001,140,000
Over 65’s

23
Comparison of Age-Related PublicExpenditure
Years
Source: The impact of ageing on public expenditure: projections for the EU25 Member States on pensions, health care, long term care, education and unemployment transfers (2004-2050), European Commission 2006
Ireland
Female
Male
0
2000
4000
6000
7000
60-64 yrs
25181939
70-74 yrs
3854
2914
80-84 yrs
5392
4052
90-94 yrs
6110
4604
0
2000
4000
6000
7000
1000
3000
5000
1000
3000
5000
euro
euro
60-64 yrs
28002117
70-74 yrs
4514
3365
80-84 yrs
6034
4472
90-94 yrs
6567
4964
EU 15

24
Main Causes of Death in Ireland2007
Source: Central Statistics Office
Cancer 29%
Respiratory Diseases 14%
Injury and Poisoning 5%
Other causes 17%
Circulatory Diseases 35%
Other Circulatory Diseases 10%
Stroke 7%
Heart Disease 18%

25

• Research and development of new medicines offers hope to anageing population of a longer healthy life, well beyond that ofprevious generations. For example, there are currently over 750medicines in development to combat cancer, 547 for neurologicalconditions and 303 for rare diseases.
• Research based pharmaceutical companies are the engines ofmedicines innovation. They have discovered and developed over90% of all new medicines made available to patients worldwideover the last twenty years.
• The discovery, development, testing and gaining of regulatoryapproval for new medicines has become an even more highlycomplex, lengthy, risky and expensive process. Each success is builton many, many prior failures. On average only one or two of every10,000 promising molecules will successfully pass extensive tests andstringent regulatory requirements and go on to be approved asmedicines, which are suitable for use in patients. As such the cost ofdeveloping a medicine has gone from €149 million in 1975 to€1,059 million in 2006.
• It takes an average 10 to 12 years to develop a new medicine fromthe time it is discovered to when it passes the regulatory standardsof safety, quality and efficacy and is available to patients. Once onthe market the average medicine has only 8 to 10 years of effectivepatent protection left before facing generic competition. Only threeout of ten marketed medicines produce revenues that match orexceed their R&D costs before they lose patent protection.
• The European pharmaceutical industry employed over 107,000people in R&D in 2007 and spent a total of €24.8 billion on suchwork.
Healthcare
26

2009 Healthcare Facts and Figures
Tomorrow
27
• Innovation is central to the creation of the knowledge basedeconomy of the 21st century. In Ireland pharmaceutical industryR&D is responsible for 20% of all business R&D. If innovation is toflourish then it must be rewarded. Whilst Ireland retains a pro-innovation outlook this is increasingly not the case in Europegenerally with patient access to new medicines via Statereimbursement systems being delayed or even denied entirely. As a result of this less favourable climate for innovation more andmore pharmaceutical companies, including European ones, are deciding to locate new R&D facilities outside Europe.

28
Evolution of Innovative Medicines Co
mpl
exity
1890 1900 1910 1920 1930 1940 1950Accumulated Knowledge of Human, Cell and Molecular Biology
1960 1970 1980 1990 2000 2010
Source: Boston Consulting Group
SerendipitousObservation
Aspirin
Sulfonamides
Antibiotics
Antihypertensives
Tranquilizers
Anti-arthritis
Beta-blockers
Cancer therapies
CNS drugs
Treatment forautoimmune disease
Focus onTissue Biochemistry
Focus onCell Biochemistry
Focus onMolecular Structure

29
Medicines Life Cycle
Researchphase
10,000 molecules screened
From concept to product:steps in the genesis of a medicine
100 molecules tested
10 candidate molecules1 medicine
Testphase
5 years0 15 years 20 years
Patent filing Patent expiry
10 years R&D 2 to 3 years
Developmentphase
AdministrativeProcedures Commercialisation phase
10 years
Source: LEEM

30
Cost of Developing an InnovativeMedicine
0
200
400
800
600
1000
1200
€ (M
illio
ns)
1975
Source: J.A DiMasi and H.G. Grabowski, ‘The Cost of Biopharmaceutical R&D: Is Biotech Different?, Price of Innovation: New Estimates of Drug Development Costs’, Managerial and Decision Economics 28 (2007) : 469- 479
1987 2001
149
344
868
2006
1,059

31
Benefits of Innovative Medicines
Beta Blockers
Source: Adapted from an ABPI Report (2004) The Human and Economic Value of Pharmaceutical Innovation and Opportunities for the NHS: Blood Pressure Lowering Treatment Trialists’ Collaboration (2000) The Lancet. See also IFPMA: The Value of Innovation (2008).
23% reduction in long term risk of death
Improved bypass operation survival rates
22% reduction in risk of death from heart attack and stroke
30% reduction in stroke events
29% reduction in coronary heart disease events
CalciumAntagonists
39% reduction in stroke events
28% reduction in major cardiovascular events
CombinationTherapy
72-80% reduction in risk of death when using acombination of anti-platelets, beta blockers, ACE inhibitorsand statins
AceInhibitors
60% reduction in risk of heart attack
30% reduction in risk of death
17-30% reduction in stroke events
Statins

32
Need for Continued MedicinesInnovation
HIV/AIDSPrevention
Medicines exist (R&D to improve their utility for patients)
Medicines exist (R&D to overcome emerging challenges e.g. drug resistance)
No medicines (R&D to bridge the gap)
Treatment Cure
Tuberculosis
Malaria
Childhood Diseases
Respiratory Infections
Cancers
Neuropsychiatric Disorders
Cardiovascular Diseases
Diabetes
Respiratory Diseases
Source: IFPMA, The Value of Innovation (2008)

33
Business Sector R&D in Ireland
Source: Forfás Research and Development Statistics in Ireland, 2006 – at a glance
Electrical/Electronic equipment 21%
Pharmaceuticals 20%
Instruments 9%
Food, Drink & Tobacco 5%
Software/Computer related 30%
Other services 4%
Chemicals 3%
Other sectors 8%

34
Changes in Location ofPharmaceutical Industry ResearchSites in the Period2001-2006
0
2
4
6
10
14
8
12
16
18
Europe
Note: Data collected from 22 global pharmaceutical companiesSource: IMI, EFPIA Research Directors Group, IFPMA
USA
New Research Sites
Num
ber P
harm
aceu
tical
Indu
stry
Res
earc
h Si
tes
Asia
Closed Research Sites

35

The Medic• The international research-based pharmaceutical industry is
critical to the health of the nation as it plays a vital role in theIrish economy.
• More than 120 pharmaceutical companies have a presence inIreland, of which 13 of the world’s top 15 pharmaceuticalcompanies have substantial operations. The industry directlyemploys over 24,500 people, half of whom are third levelgraduates, with as many again employed in the provision ofservices to the sector. The industry contributes approximately €3billion annually in taxes to the State.
• Pharmaceutical production in Ireland currently generates nearly50% of the country’s exports and 11% of its Gross DomesticProduct which contribute to making Ireland the largest netexporter of medicines in the world.
• Nearly €7 billion has been invested by the pharmaceutical sectorover the last nine years in a period when job growth in the sectorhas averaged 1,000 annually. According to IDA Ireland thereplacement value of the investment by the pharmaceuticalsector in the Irish economy is over €40 billion.
36

2009 Healthcare Facts and Figures
37
ines Industry• The market for pharmaceuticals continues to grow as outlined in
the next section on Medicines in the Community and there areopportunities for the industry to develop its operations in Irelandstill further.

Source: 1 IMS Health Data Dec 2008 2 IMS Health Data Dec 2008 Note: “Merck & Co., Inc.” has its headquarters in Whitehouse Station, NJ, USA and operates in most countries outside the U.S., including Ireland, as Merck Sharp & Dohme.
By Rank
1. Pfizer
2. AstraZeneca
3. GlaxoSmithKline
4. sanofi-aventis
5. Wyeth
6. Roche
7. Novartis
8. Merck Sharp & Dohme
9. Abbott
10. Lilly
By Rank
1. Pfizer
2. GlaxoSmithKline
3. Novartis
4. sanofi-aventis
5. AstraZeneca
6. Johnson & Johnson
7. Roche
8. Merck & Co.
9. Abbott
10. Lilly
Ireland Top 101 Global Top 102
38
Leading Pharmaceutical Companiesby Sales in Ireland and Globally

39
Distribution of Global Pharmaceutical Salesby Region
Source: IMS Midas, Dec 2007
Europe 31%
Asia (excl. Japan), Africa and Australia 9%
Japan 9%
North America 46%
Latin America 5%
2007 Global Sales€663.50 billion

40
9 of the world’s top 15 medicines areproduced in Ireland
Source: IPHA Analysis. Rankings based on IMS Health Data, Dec 2008
Rank Medicine Company
1. Lipitor Pfizer
5. Enbrel Wyeth
7. Zyprexa Eli Lilly
8. Remicade Centocor
9. Singulair Merck Sharp & Dohme
10. Risperdal Janssen Pharmaceuticals
12. Takepron Takeda
13. Effexor XR Wyeth
15. Actos Takeda

41
World Trade in Pharmaceuticals2006
Source: International Trade Centre, a joint agency of the World Trade Organisation and the United Nations (http://www.intracen.org/dbms/country/CA_CtryIndex.Asp?CT=372)
Country Exports $ Imports $ Balance $
Ireland 12,734 1,753 10,981
Switzerland 20,663 10,292 10,371
Germany 32,243 24,622 7,621
UK 18,508 12,679 5,829
France 18,023 12,231 5,792
Sweden 6,350 2,362 3,988
Belgium 28,410 25,679 2,731
Austria 3,861 2,781 1,080
Netherlands 9,046 8,937 109
Italy 9,727 9,949 -222
Spain 5,338 6,951 -1,613
Japan 1,878 5,753 -3,875
USA 19,129 32,318 -13,189

Medicines in
42
Expenditure on the community medicines schemes has risen steadilyin recent years. The factors behind that growth include:
• Ireland’s rapidly increasing and ageing population as outlined inthe section on Demographic Trends.
• The development of new treatments becoming available and morepatients availing of them: for example in the areas of preventativemedicine and the long-term treatment of chronic illness. Thenumber of patients registered under the High Tech Scheme in 2007was 41,500, a five fold increase on the figure in 1997 (8,250).
• The introduction of Government initiatives to improve publichealth: the cardiovascular and the cancer strategies were launchedwith a view to improving poor health outcomes in these diseaseareas. They have resulted in more people being treated andnaturally an increase in the utilisation of medicines. For examplethe prescribing frequency of cardiovascular system medicationunder the GMS Scheme increased from 3.6 million in 1996 to 11.1million in 2007 (an increase of 208%).
• Epidemiological evolution: the increased incidence of chronic andnon-communicable diseases is generally quite costly to treat.Ireland has one of the highest incidences of asthma in the world,currently 12%, and increasing levels of diseases like diabetes andobesity.
• State decisions on eligibility and administration of the communitydrug schemes: The granting of medical cards to everyone over 70and the introduction of the Drug Payment Scheme resulted insubstantial growth in the State bill. For example the Deloittereview of the Governance and Accountability Mechanisms in theCommunity Drug Schemes (2003) noted that the provision ofmedical cards to the over 70s cost an additional €126m in the firstfull year of the arrangement in 2002. It also noted that the numberof claimants under the DPS increased by 40% between 2000 and2002.

2009 Healthcare Facts and Figures
the CommunityThe growth in medicine expenditure also has to be seen in the context of the factthat Ireland historically has one of the lowest levels of consumption of medicinesper head of population, so it is only to be expected that spending on medicines willincrease as the healthcare system endeavours to improve life expectancy andquality of life. It also has to be seen in the context of the large scale and ongoingincreases in Irish health spending.
43

44
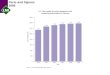
Community Medical Schemes Expenditure2007
0
150
75
300
225
450
600
375
525
750
900
975
1050
675
825
€ (M
illio
ns)
Long TermIllness Scheme
Source: HSE Primary Care Reimbursement Service Annual Report 2007 The GMS Scheme figures exclude VAT and the High Tech Scheme figures exclude patient care fees.
124
High TechScheme
239
Drug PaymentScheme
307
General MedicalServices (GMS) Scheme
1029

45
GMS Scheme Expenditure and % Growth Rate1998-2007
00
100
200
300
400
500
600
700
800
900
1000
1100
5
10
20
15
30
25
€ (M
illio
ns)
1998
Source: GMS (Payments) Board Annual Reports 1998 – 2005 HSE Primary Care Reimbursement Service Annual Reports 2006 & 2007 Figures excluding VAT.
1999 2000 2001 2002 2003 2004 2005 2006
252
11 12
17
28
27
1817
8
14.8
283
332
426
540
639
749
816
922
2007
1029
Euro (Millions)
% Growth Rate
11.6%
Gro
wth
The Scheme provides free medical services to persons who would nototherwise be able, without undue hardship, to afford such services.

46
Ageing of the GMS Scheme1994-2007
Source: GMS (Payment) Board Annual Reports 1994-2005 HSE Primary Care Reimbursement Service Annual Reports 2006 & 2007
1994 1,287,000 36.0% 297,000 23.1%
2000 1,148,000 30.3% 323,000 28.1%
2004 1,149,000 29.3% 383,000 33.3%
2007 1,276,000 30.1% 416,000 32.6%
Total No. of Eligible Persons
Year As a % of the Population
Total No. Aged 65 years+
65+ as a % of Eligible Persons
While the overall numbers eligible for medical cards has fallen since1994, the number of cardholders aged 65 and over has increased bynearly 36% (a trend significantly accentuated by the granting ofmedical cards to everyone over 70 years old in 2001).

47
Drugs Payment Scheme Expenditure1999-2007
0
25
50
75
100
125
150
175
200
225
250
275
300
325
€ (M
illio
ns)
1999
Source: GMS (Payment) Board Annual Reports 1999-2005 HSE Primary Care Reimbursement Service Annual Reports 2006 & 2007
105
2000
141
2001
178
2002
192
2003
204
2004
224
2005
247
2006
283
2007
307

48
High Tech Scheme Expenditure1999-2007
0
50
100
150
200
250
€ (M
illio
ns)
1999Source: GMS (Payment) Board Annual Reports 1999-2005 HSE Primary Care Reimbursement Service Annual Reports 2006 & 2007 Figures exclude patient care fees. The number of patients registered under the Scheme has increased from just over 8,000 in 1998 to nearly 41,500 in 2007.
40
2000
49
2001
61
2002
80
2003
104
2004
141
2005
169
2006
207
2007
239
Developments in biotechnology and therapeutics have given rise tothe introduction of medicines for the treatment of medicalconditions, many of which previously had either no effectivetreatment or required extended in-patient hospital care. Under theScheme these medicines are dispensed by the community pharmacist.

49
Long Term Illness Scheme Expenditure1999-2007
0
20
40
60
80
100
120
140
€ (M
illio
ns)
1999
Source: GMS (Payment) Board Annual Reports 1999-2005 HSE Primary Care Reimbursement Service Annual Reports 2006 & 2007
34
2000
42
2001
52
2002
62
2003
73
2004
86
2005
101
2006
115
2007
124
The Long Term Illness Scheme is for persons who suffer from one or moredefined long term illnesses. It gives such persons the right to obtain,irrespective of income, relevant medication free of charge.

50
Creating Headroom for Innovative Medicines
Per Item Cost on GMS Scheme is stabilising while the DPS and LTIScheme is reducing
0
15
20
25
30
35
40
45
50
55
2000 2001 2002 2003 2004 2005 20072006
42.1
27
11.5
45
29
13
48
31.9
14.2
50
34
15.8
51
35.75
16.9
52
36.25
17.2
53.5
37.1
18.1
53
36.25
18.5
Long Term Illness SchemeDrugs Payment SchemeGMS Scheme
Source: HSE Corporate Pharmaceutical Unit, 2008
€

51

• Of the 340 medicines on the World Health Organisation (WHO)essential drugs lists, 95% of them have no patents. This meansthat there is no patent obstacle preventing cheap generic copiesof the vast majority of essential medicines being produced locallyfor poor people in developing countries. But those people are notgetting them.
• Patents do not prevent access to medicines. The real barrierhindering access to treatments is in fact a lack of the basichealthcare infrastructure required to get existing medicines topeople. Other factors such as a lack of access to basics like food,decent housing and clean water, armed conflict, corruption,bureaucracy and the lack of simple prevention measures likecondoms and mosquito nets, unfortunately mean that poorhealth is endemic for the world's poorest people.
• Pharmaceutical companies globally are currently involved in morethan 150 health partnerships and programmes in the developingworld which are designed primarily to improve access tomedicines and other aspects of healthcare. Seventy-eight of theseinvolve capacity building activities. These include the provision ofbasic health education, encouraging behavioural change, traininghealth personnel, mounting prevention campaigns, as well asproviding infrastructure for delivering healthcare services.
• In the period 2000 to 2008, the industry provided enough healthinterventions – medicines, vaccines, equipment, health educationand training – to help nearly 1.75 billion people in developingcountries.
Medicinesand
52

2009 Healthcare Facts and Figures
Global Health• The industry has made available medicines, vaccines, equipment,
training and health education worth $9.2 billion, of which $2.7 billionwas in 2007 alone, to the developing world since the United Nationsannounced the Millennium Development Goals.
• Pharmaceutical companies are involved in 67 R&D programmes, upfrom 58 in 2007, for neglected tropical diseases and other diseases ofthe developing world such as malaria, sleeping sickness, dengue feverand chagas disease.
53
© BMS – www.securethefuture.com

54
Industry Supported Public-PrivatePartnerships in the Developing World
0 10 30Number of public-private partnerships
5040 6020
Source: IFPMA Partnerships to Help Build Healthier Societies in the Developing World 2007 www.ifpma.org/healthpartnerships
ChronicDiseases
Child &Maternal
VaccinePreventable
TropicalDisease
Tuberculosis
Malaria
HIV/Aids
11
17
10
19
13
13
52

2007 2008 Healthcare Facts and Figures
Number of Positive Health Interventionsmade in the Developing World
0
50
100
150
200
250
300
Mill
ions
of p
eopl
e po
tent
ailly
reac
hed
350
400
2000 2001 2002 2003 2004 2005 2006 2007
Other health interventions + education + trainingMedicines, Vaccines & Diagnostics - no profitMedicines, Vaccines & Diagnostics - donated
A positive health intervention is: (a) the delivery of sufficient medicine to cure one person of one disease, (b) the provision of a course of therapy sufficient to manage one disorder in one person for one year, (c) provision of sufficient vaccine to immunise one person against one disease for at least one year, or (d) delivery of a proven program of health education or training to one person. These metrics were used because, while companies know the number of doses they make available, they have a less precise view of the number of patients actually treated. Source: IFPMA www.ifpma.org/healthpartnerships


Open...to see the foot-print of Ireland’s phar-maceutical industry.

DublinAbbott Laboratories A Menarini Pharmaceuticals Alliance PharmaceuticalsAmgenArchAstellas PharmaAstraZeneca PharmaceuticalsBayer Consumer CareBayer Schering PharmaBiogen IdecBoehringer IngelheimBOCBristol Myers SquibbPharmaceuticalsCelgeneCephalon PharmaCovidienEisaiEli Lilly & CompanyForest LaboratoriesGlaxoSmithKlineGlaxoSmithKline ConsumerHealthcareGrunenthal PharmaHelsinn Birex TherapeuticsIpsen PharmaceuticalsJanssen-CilagLabopharm EuropeLEO PharmaHenkel LoctiteLundbeck MEDAMcNeil HealthcareMerck SeronoMSDMundipharmaNovartisNovartis Consumer HealthNovo NordiskNycomedOrganon LaboratoriesPfizer HealthcarePierre FabreProctor & GambleReckitt BenckiserRehelsRoche ProductsRottapharmsanofi-aventisSanofi Pasteur MSDSchering Plough PharmaceuticalsServier LaboratoriesShire Pharmaceuticals Solvay HealthcareSSL HealthcareStiefel LaboratoriesTakedaTillotts PharmaUCB PharmaWyeth Consumer HealthcareWyeth Pharmaceuticals
Cork Cara PartnersCentocorCognis (Henkel)CordenDynoEli Lilly & CompanyFMCGE HealthcareGilead SciencesGlaxoSmithKlineJanssen (J&J)NovartisPfizerRecordatiSchering PloughQuest (ICI)Wexport (Leo)
Newbridge Wyeth Medica (AHP)
RathdrumSchering Plough
Arklow Servier
WaterfordArkopharmaGenzymeLawter InternationalNovartis AgribusinessTEVA
DungarvanGlaxoSmithKline
Cashel Ranbaxy
ClonmelClonmel Healthcare (Stada)MSD
KillorglinAstellas PharmaTemmler
Limerick Aughinish Alumnia (Glencore AG)HeraeusInfo Lab (Huber Group)Schwarz PharmaWyeth Nutritional (AHP)
Ennis OlympusRoche
Athlone Athlone PharmaceuticalsElan
Westport Allergan
Sligo Abbott Diagnostics Fort Dodge (AHP)Stiefel Laboratories
Monaghan Norbrook Labs
Bray Takeda
KILLORGLIN
ENNIS
ATHLONE
MONAGHAN16
13 3
4 17
SLIGO
WESTPORT
DUNGARVAN
WATERFORD
CASHEL
ARKLOW
BRAYRATHDRUM
DUBLIN
NEWBRIDGE
5
1 2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
6
710
2
1
11
12
14
15
8
9CLONMEL
CORK
LIMERICK
Design and production: www.slickfish.ieTPG0209

Franklin House140 Pembroke RoadDublin 4Ireland Tel: (353 1) 660 3350 Fax: (353 1) 668 6672 E-mail: [email protected]
www.ipha.iewww.medicines.iewww.feelbetter.ie