Embed Size (px)
Citation preview

Healthcare Reform and Changing Fiscal and Management Structures and What About PennsylvaniaDale Jarvis

2
Movie: Turning Oranges into Orange Juice

Key Fiscal and Management Structure Issues• New $ and Consumers from
Expansion & Parity
• Changes in Payor Mix
3
New Behavioral Health Consumers and Funding
Uninsured to
Insured
Insured Covered by
MH/SU Parity
Current “Payor” Categories
UninsuredMedicaid and
Medi-MediMedicare Private Insured
New “Payor” Categories
Unin-sured
MedicarePublic Option?Dual Eligible
Plans (Medi-Medi)
MedicaidState
ExchangePrivate Insured
Federal Incubators for
Reforms
StateManaged
• Provider-Level Changes
Reconfiguration to Support Person-Centered Healthcare Homes
Federally Qualified Behavioral Health Centers (FQBHCs)
New Payment Structures and Reimbursement Models
• So What About Pennsylvania

Coverage Expansion and Parity
• 31 to 36 million additional insured
• $16 - $25 billion new BH funding for this group
• To address needs of the 5.2 million indigent, uninsured in need of MH
• Parity and need to “bend curve” will result in increased demand for those already insured
Page 4

Coverage Expansion and Parity• Two layers of funding: Mild & Moderate and Serious & Severe (SMI/SED)• Meeting ½ of the demand for specialty care will require 33,000 FTEs
5
25% 50% 75% 100%Est Hours per Case 26.60 26.60 26.60 26.60 Estimated Hours of Svc 18,868,910 37,737,819 56,606,729 75,475,638 Hours per FTE @ 55% of 2,080 1,144 1,144 1,144 1,144 FTE Gap 16,494 32,988 49,481 65,975
Added Number to Serve to Close Gap by

Changes in Payor Mix• Important changes will be unfolding in the payor
landscape that will impact how states, health plans and providers operate
6
Current “Payor” Categories
UninsuredMedicaid and
Medi-MediMedicare Private Insured
New “Payor” Categories
Unin-sured
MedicarePublic Option?Dual Eligible
Plans (Medi-Medi)
MedicaidState
ExchangePrivate Insured
Federal Incubators for
Reforms
StateManaged

Provider Level Changes• There are three changes unfolding that will impact the
behavioral health service delivery system
7
Reconfiguration to Support Person-Centered Healthcare Homes
Federally Qualified Behavioral Health Centers (FQBHCs)
New Payment Structures and Reimbursement Models

Person-Centered Healthcare Homes• Community Behavioral Healthcare Organizations need to engage with
Medical/Healthcare Homes in one or more of three ways and there is not a “fourth door” for CBHOs
8
Fully Integrated Healthcare Home
Person-Centered Healthcare Home Options
Primary Care Case Rate for:- Screening/Registry Tracking
- Care Mgmt/BH Clinicians- Psychiatric Consultations
- Non-BH Prevent/Mgmt Work
Healthcare Funding
Streams for Primary Care
Services
Behavioral Health
Funding Streams for
Mental Health & Substance Use Services
Focused PartnershipHealthcare Home
Primary Care Case Rate with:- Screening/Registry Tracking
- Care Mgmt/BH Clinicians- Psychiatric Consultations
- Non-BH Prevent/Mgmt Work
Healthcare Funding
Streams for Primary Care
Services
Behavioral Health
Funding Streams for
Mental Health & Substance Use Services
CBHO with Linkage to Multiple Medical Homes
Behavioral Health Case Rate for Svcs
in CBHO
Healthcare Funding
Streams for Primary Care
Services
Behavioral Health
Funding Streams for
Mental Health & Substance Use Services
Food MartCBHO
Primary Care Case Rate for
Svcs in Medical Clinic
Food MartCBHO

9

Federally Qualified Behavioral Health Centers

Federally Qualified Behavioral Health Centers• 2007 Revenues by payor for the 1,067 Federally
Qualified Health Centers that have Section 330 Grants• Note that revenue from the 330 Grants and Indigent
Care programs are not available to CBHOs• FQHCs also have higher Medicaid and Medicare
revenue due to favorable Federal legislation
11
2007 Revenue RatiosGrant Revenue
Section 330 FQHC Grants $1,683,908,963 18.5%Other Federal Grants $200,676,524 2.2%State/Local Grants/Contracts $886,402,060 9.8%Foundations/Private Grants/Contracts $378,384,064 4.2%
Total Grant Revenue $3,149,371,611 34.6%
Patient Service RevenueMedicaid $3,320,438,823 36.5%Medicare $548,357,016 6.0%Other Public $238,597,215 2.6%Third Party Insurance $666,521,498 7.3%Patient Self-Pay $597,170,297 6.6%
Total Patient Service Revenue $5,371,084,849 59.1%
Revenue from Indigent Care Programs $335,084,637 3.7%Other Revenue $234,496,445 2.6%Total Revenue $9,090,037,542 100.0%
Number of Grantees 1,067Average Revenue per Grantee $8,519,248

Federally Qualified Behavioral Health Centers
• A parallel structure for CBHOs, Federally Qualified Behavioral Healthcare Centers (FQBHC), based on the FQHC accountability and payment structures
• 10 benefits and the 8 responsibilities come with FQHC status
12

Federally Qualified Behavioral Health Centers• The Community Behavioral Healthcare Organization(CBHO) system will need
to adapt to this new model of service delivery and a high level of expectations from the general healthcare system
• Federally Qualified Behavioral Healthcare Centers (FQBHCs) will become the core of the new specialty system, supplemented by specialized, less comprehensive mental health and substance use provider organizations
13
Organizing the Specialty BH System
MH Provider
Smaller, Specialized MH and SU Providers Supplementing the Service Needs of the Population
SU Provider
MH Provider
SU Provider
MH Provider
SU Provider
MH Provider
SU Provider
FQBHCs: Comprehensive, Quality
CBHOs as Person Centered Healthcare
Homes via Integration or Partnership Model

Federally Qualified Behavioral Health Centers
• FQBHC status will create a single set of national standards that can serve as a blueprint for the types of services and infrastructure that need to be in place to better support the full healthcare needs of persons with serious mental health and substance use disorders
• In addition, the FQBHC designation creates a single, common platform of common assumptions, approaches, and expectations for FQHCs and FQBHCs to partner in providing person-centered healthcare homes
• The ability to achieve FQBHC designation and the accompanying financial benefits are necessary components for Community Behavioral Healthcare Organizations to be able to adapt to the changes that will occur in the general healthcare system
14

New Payment Structures & Reimbursement Models• Funding methods for CBHOs are also going to need to change to
address the imbalances in the current system, reverse existing incentives, and come into alignment with how the rest of healthcare will be funded
15
• Per Service• Per Diem
Fee for Service
• Capitation• Grant-Type
Fixed Fee
• Prevention, Early Intervention• "Back-Porch" ServicesCase Rate
• Fee for Service• Settlement to Cover ShortfallsPPS
• Share in Savings of reduced Total Health ExpendituresBonus
(Note: PPS = Prospective Payment System)
The New FQBHC Payment Model (mirroring the Medical Home model)

New Payment Structures & Reimbursement Models
• Funding is just starting to open up for embedding primary medical care into CBHOs, which is a critical component of meeting the needs of adults serious mental illness
16
Clinical Design for Adults with Low to Moderate and Youth with Low to
High BH Risk and Complexity
Primary Care Clinic with Behavioral
Health Clinicians
embedded, providing
assessment, PCP
consultation, care
management and direct
service
Partnership/Linkage with
Specialty CBHO for persons who need their care stepped up to
address increased risk and complexity with ability to step back to Primary Care
Clinical Design for Adults with Moderate to High BH Risk and
Complexity
Community Behavioral Healthcare Organization with an embedded
Primary Care Medical Clinic with ability to address the full range of
primary healthcare needs of persons with moderate to high
behavioral health risk and complexity
Food Mart
CBHOFood MartCBHO

So, What about Pennsylvania?
17

Page 18
Movie: Ice Fishing, Don’t Be Swallowed by Change

Overview of Pennsylvania’s Safety Net Population• Of the 12.6 million Pennsylvania residents, 2.2 million fall into the Safety Net
because they are indigent and uninsured or have Medicaid coverage (source: Kaiser Family Foundation State Health Facts)
19
Medicaid Youth, 737,856
Medicaid Adult/Elder,
749,138
Indigent/ Uninsured
Youth, 158,879
Indigent/ Uninsured
Adult/Elder, 616,003
Pennsylvania Safety Net Population (2007) 2.2 Million

How does PA MH Funding compare with other states?• Pennsylvania is the most successful state in supporting funding for mental
health services (note: this includes some SU $ but is missing some children’s $)
SMHA-Controlled Mental Health Revenue by StateFiscal Year 2006
State
Total State Mental Health
Revenue
Target # of Persons to Serve/Year
Revenue per Target
Client RankPennsylvania $3,332,904,698 544,949 $6,116 1 Maine $464,300,000 76,362 $6,080 2 District of Columbia $229,400,000 38,093 $6,022 3 Alaska $183,200,000 33,512 $5,467 4 New Hampshire $166,100,000 38,394 $4,326 5 Maryland $810,000,000 233,097 $3,475 6 New Jersey $1,241,600,000 365,082 $3,401 7 Minnesota $721,100,000 213,635 $3,375 8 Vermont $122,500,000 36,426 $3,363 9 New York $3,982,300,000 1,287,434 $3,093 10 Top 10 Average $4,472
20

Analysis of MH Unserved in PennsylvaniaIn a FY2007 NCCBH Mental Health Gap Analysis, Pennsylvania:
– Ranked #2 in Medicaid Gap (low # = low gap)
– Ranked #50 in Indigent/Uninsured Gap (out of 51)
(based on Kaiser Population data, national prevalence estimates, and Pennsylvania data submitted to SAMHSA on number served)
Question: Where are the uninsured counts? In the County Allocations?
21
Pennsylvania Gap Analysis FY2007
MedicaidIndigent/
Uninsured TotalMild Need 148,617 80,109 228,726SMI/ SED Need 201,794 114,429 316,223Total Need 350,411 194,538 544,949
Mild Served 132,493 2,097 134,590SMI/ SED Served 161,884 2,563 164,447Total Served 294,377 4,660 299,037
Mild Gap 16,124 78,012 94,136SMI/ SED Gap 39,910 111,866 151,776Total Gap 56,034 189,878 245,912
Mild Gap % 11% 97% 41%SMI/ SED Gap % 20% 98% 48%Total Gap % 16% 98% 45%
U.S. Median Gap 60% 65%

Pennsylvania Needs a Comprehensive Integration Plan
PA stakeholders need to develop a Blueprints document that describes how we got her, where we need to go (clinical, structural, and financial designs) and a comprehensive demand, capacity, revenue and expense model
22

Pennsylvania Needs a Comprehensive Integration Plan
23

Stop Whining and Do Something
1. Complete aPopulation-Based
Planning Project (Howmany people, how
much service?)
2. Identify the ServiceDelivery &
Infrastructure Gaps
3. Project the Cost ofMeeting the Need(Service, Admin,
Infrastructure)
4. Redesign theService Delivery
System to Align withthe Clinical Design
5. Redesign theRegulatory System toAlign with the Clinical
Design
6. Redesign theFinancing System toAlign with the Clinical
Design
7. Develop a RealisticProposal for Closingthe Gaps based onMoney, Political &
Workforce Realities
8. Begin the Changeprocess as progress
is being made onturning support intoLegislative Action
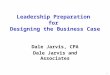
This diagram lists eight steps in a process for transforming the public behavioral health system at the region, state and federal level.
This diagram lists eight steps in a process for transforming the public behavioral health system at the region, state and federal level.

Demand-Capacity, Revenue-Expense Planning
C onsum ersS ervice M ix
U nits o f S erv ice
S ervice S ta ffP roductiv ity H ours
A va ilab le H ours
D irect S ta ff C ostsO ther D irect
O verheadR isk R eserve
E nro lleesC onsum ers
S ervice U n itsC ap ita tion /C ase/
FFS R ates
D em and C apacity R evenue E xpense

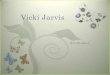
How Many People…North Central Washington RSNPrevalence Analysis
Adams Grant Okanogan Total
A. Total PopulationChild & Adolescent (0 through 17) 5,469 24,053 10,444 39,966 Adults (18 through 59) 8,762 41,845 21,337 71,944 Older Adults (60 and Over) 2,452 12,402 7,820 22,674 Total Population 16,683 78,300 39,601 134,584 Ratios 12% 58% 29%
B. Child/SED Prevalence Estimate DetailChildren At or Below 250% of Poverty 2,599 11,429 4,963 18,991
Estimated Prevalence Rate 9.0% 9.0% 9.0%
Est. SED Prevalence needing Public MH 234 1,029 447 1,709
C. Adult/Older Adult SMI Prevalence Estimate DetailPEMINS SMI Estimate < 200% Poverty 226 1,095 589 1,910SMI in Residential (@ 90% occupancy) 30 144 77 251Jails, Prisons 11 54 29 94Homeless 15 74 40 129Hospitals 5 23 12 40# Needing Public MH 287 1,390 747 2,424
D. SED/SMI Prevalence Estimate TotalsYouth and Adults Needing Public MH 521 2,419 1,194 4,133 Ratios 13% 59% 29% 100%
Mental Health prevalence for a 3-County Region in rural Washington State.

How Much Service…Multnomah County: Adult System of Care ProjectionsJan-Dec 2006 - Oregon Health Plan Enrollees
Screening & Triage Only Basic Services
Recovery Mainten-ance
Low Intensity Community
Based Services
Locus Level N/A Locus 0 Locus 1 Locus 2
Locus Score Available to all Clients
< 10 10 to 13 14 to 16
Clients & Case MixCase Mix 7.2% 19.9% 21.4% 8.8%Clients Served 479 1,331 1,433 590
Average Length of Stay and Treatment SlotsALOS 1 3 6 8 Slots 40 333 717 393
Units of ServiceAvg. Units/Case 1 4 10 15 Unit of Measure Std Hr Std Hr Std Hr Std Hr
Completion Rate 70% 70% 70% 70%Paid Units/Case 0.70 2.80 7.00 10.50 Services 335 3,727 10,031 6,195
Category IV: General Outpatient Mental Health Services
The mental health system in Portland Oregon completed a clinical design, identified what services should be available to persons with SMI/SED as well as other Medicaid enrollees needing mental health treatment, and projected demand based on historical use, research, and projected utilization at each level. This slide projects use for non-SMI/SED persons.

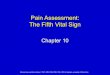
How Much Service…Multnomah County: Adult System of Care ProjectionsJan-Dec 2006 - Oregon Health Plan Enrollees
Category I: ACT
Category II: DBT
Assertive Community Treatment
Dialectical Behavioral
TherapyScreening & Triage Only
Low Intensity Community
Based Services
High Intensity Community
Based Services
Medically Monitored Non-
Residential Services
Locus Level Locus 4 Locus 4 N/A Locus 2 Locus 3 Locus 4
Locus Score20+
generally 3 to 4 on all scale
20+generally 3 to 4 on all scale
Available to all Clients
14 to 16 17 to 19 20+
Clients & Case MixCase Mix 3.0% 0.4% 4.3% 5.6% 16.6% 12.8%Clients Served 200 26 286 373 1,113 855
Average Length of Stay and Treatment Slots (the number of persons who will be served at one time)ALOS 12 12 1 8 11 12 Slots 200 26 24 249 1,020 855
Units of ServiceAvg. Units/Case 100 72 1 15 32 72 Unit of Measure Std Hr Std Hr Std Hr Std Hr Std Hr Std Hr
Completion Rate 95% 95% 70% 70% 70% 70%Paid Units/Case 95.00 68.40 0.70 10.50 22.00 50.40 Services 19,000 1,778 200 3,917 24,486 43,092
Category III: Services for Severely Mentally Ill
This slide projects need for persons with SMI/ SED in Portland Oregon.

Pennsylvania Needs a Comprehensive Integration Plan• Integration Policy Initiative:
Collaboration of California’s public Mental Health and Primary Care community
• Grew out of acknowledgement that BH and PC have not adequately addressed whole health needs of persons with MH/SU conditions
• Addresses integration vision, values, principles, clinical models, implementation issues, and specific recommendations (delivery system, financing, and regulatory)
29

Federal Health Reform Timeline (based on Senate Finance Committee Bill)
Eight key activities begin between 2010 and 2014
Requiring a great deal of implementation effort at the State and Federal levels
30
U.S. Health Reform Legislation TimelineSenate Finance Committee
2010 2011 2012 2013 2014 2015 2016 2017
Implementation Planning Begins
Hi Risk Pools for People with Pre-existing Conditions
State Health Insurance Exchanges Begin
New Payment Methods & Delivery System Redesign Begins
Expand Medicaid to 133% Federal Poverty Level
Optional Mandatory
Employer Tax Credits Begin
Individual/Family Premium Subsidies Begin
Individual Mandates Begin; Penalties Start in 2014
$0 $200 $400 $600 $750

California’s 1115 Waiver Renewal
• Promote Organized Delivery Systems of Care– Enrollment in organized delivery systems for seniors and persons with
disabilities and children and families in rural counties– Children with special health care needs– Dual-eligible beneficiaries– Adults with severe mental illness
• Strengthen and Expand the Health Care Safety Net• Implement Value-Based Purchasing Strategies
– Standardized reporting; risk sharing; pay-for-performance (P4P); healthy rewards and incentives for beneficiaries; and nonpayment for healthcare acquired conditions
• Enhance the Delivery System for the Uninsured to Prepare for National Reform
31

Pennsylvania Behavioral Health Key Issues• What is Pennsylvania’s plan for addressing Medicaid expansion
and development of Health Insurance Exchanges? • What will be Pennsylvania’s stages of Health Plan evolution?• How will Behavioral Health be managed inside the Exchanges – carve-in or
carve-out?• How ready are the state, plans, counties, and providers for wide and rapid
deployment of person-centered healthcare homes?• Is the concept of an Outpatient Behavioral Health System outdated and out of
sync with the delivery system models of the near future?• How many Pennsylvania providers are ready to become FQBHCs?• How does Pennsylvania financially support embedding primary care clinics
inside CBHOs/FQBHCs?• What state regulations need to be re-written to align with needed clinical,
structural and financing changes?• Who will develop Pennsylvania’s comprehensive integration plan and when? • How will attachment to the status quo systems and structures impact the ability
of Pennsylvania to better align with national healthcare reform opportunities?Page 32