-
EMHJ Vol.17 No.10 2011
EasternMediterraneanHealthJournalLaRevuedeSantdelaMditerraneorientale
784
Review
Health care system in Saudi Arabia: an overviewM. Almalki,1,2 G.
Fitzgerald 2 and M. Clark 2
ABSTRACT The government of Saudi Arabia has given high priority
to the development of health care services at all levels: primary,
secondary and tertiary. As a consequence, the health of the Saudi
population has greatly improved in recent decades. However, a
number of issues pose challenges to the health care system, such a
shortage of Saudi health professionals, the health ministrys
multiple roles, limited financial resources, changing patterns of
disease, high demand resulting from free services, an absence of a
national crisis management policy, poor accessibility to some
health care facilities, lack of a national health information
system, and the underutilization of the potential of electronic
health strategies. This paper reviews the historical development
and current structure of the health care system in Saudi Arabia
with particular emphasis on the public health sector and the
opportunities and challenges confronting the Saudi health care
system.
1College of Health Sciences, University of Jazan, Jazan, Saudi
Arabia (Correspondence to M. Almalki:
[email protected]).2Faculty of Health, School of Public
Health, Queensland University of Technology, Brisbane,
Australia.
Received: 28/12/08; accepted: 05/01/10
:
: : . . .
.
Aperu du systme de sant en Arabie saoudite
RSUM Le gouvernement dArabie saoudite a accord une priorit leve
au dveloppement des services de soins de sant tous les niveaux :
primaire, secondaire et tertiaire. En consquence, la sant de la
population saoudienne sest grandement amliore au cours des dernires
dcennies. Toutefois, le systme de sant est confront de multiples
dfis tels que la pnurie de professionnels de sant saoudiens, les
rles multiples du ministre de la Sant, des ressources financires
limites, lvolution des tableaux de morbidit, la forte demande gnre
par la gratuit des services, labsence de politique nationale de
gestion des crises, laccs mdiocre certains tablissements de soins,
labsence de systme national dinformation sanitaire et la
sous-utilisation du potentiel des stratgies de cybersant. Le prsent
article passe en revue lhistoire du systme de sant saoudien et sa
structure actuelle et met laccent sur le secteur de la sant
publique, les opportunits qui soffrent ce systme et les obstacles
auxquels il est confront.
-
785
Introduction
Health care services in SaudiArabiahavebeengivenahighpriorityby
thegovernment.During thepast fewdec-ades, health andhealth
serviceshaveimprovedgreatly in
termsofquantityandquality.Gallagherhas stated that:Although many
nations have seensizablegrowth in
theirhealthcaresys-tems,probablynoothernation(otherthanSaudiArabia]of
largegeographicexpanseandpopulationhas,incompa-rabletime,achievedsomuchonabroadnationalscale,witharelativelyhighlevelofcaremadeavailabletovirtuallyallseg-mentsofthepopulation(p.182).[1]
AccordingtotheWorldHealthOr-ganization(WHO)[2],theSaudihealthcare
system is ranked26thamong190of theworldshealth systems. It
comesbeforemanyother internationalhealthcare systems such asCanada
(ranked30),Australia(32),NewZealand(41),andothersystemsintheregionsuchastheUnitedArabEmirates(27),Qatar(44)
andKuwait (45).Despite
theseachievements,theSaudihealthcaresys-temfacesmanychallengeswhichrequirenewstrategiesandpoliciesbytheSaudiMinistryofHealth(MOH)aswell
aseffectivecooperationwithothersectors.
This review outlines the
historicaldevelopmentandcurrentstructureoftheSaudihealthcaresystem.Aparticularem-phasishasbeengiventothepublichealthsector
that is operated by
theMOH,includingthekeyopportunitiesandchal-lenges it faces. In
addition, this
reviewhighlightsdemographicchangesandtheeconomiccontextofSaudiArabiainrela-tiontotheSaudihealthcaresystem.
Demographic and economic patterns of Saudi Arabia
Thelastofficialcensus
in2010placedthepopulationofSaudiArabiaat27.1million, comparedwith
22.6million
in 2004 [3].The annual
populationgrowthratefor2004to2010was3.2%perannum[3],andthetotalfertilityratewas3.04
[4].Saudi citizens comprisearound68.9%of the
totalpopulation;50.2%aremalesand49.8%females[3];67.1%of
thepopulationareunder theageof 30 years and about 37.2%
areunder15years;thepopulationovertheageof60yearsisestimatedat5.2%[5].According
toUnitedNationprojec-tions,itisestimatedthatthepopulationofSaudiArabiawill
reach39.8millionby2025and54.7millionby2050[6].This is
anaturaloutcomeof thehighbirth
rate(23.7per1000population),increased life expectancy (72.5
yearsformen,74.7yearsforwomen)[4]anddecliningmortality rateamong
infantsandchildren[1].Theunder5yearsofagemortalityratefell250per1000livebirths
in1960[7] to20.0per1000 in2009 [4].Apart from
advancementsinhealthcareandsocialservices, theseimproved statistics
canmostlybe at-tributed to
thecompulsorychildhoodvaccinationprogramme
implementedbythegovernmentsince1980[7].Thisunprecedented growth
will increasethedemand for essential services andfacilities
includinghealth care,whileat the same time creating
economicopportunities.
SaudiArabiaisoneoftherichestandfastestgrowingcountriesintheMiddleEast.
It is theworlds
largestproducerandexporterofoil,whichconstitutesthemajorportionofthecountrysrevenues[8,9].Inrecentdecades,however,SaudiArabiahasdiversifieditseconomy,andtodayproducesandexportsavarietyofindustrialgoodsallovertheworld.Thesoundeconomyandwell-establishedindustrybaseaffectstheSaudicommu-nitybyincreasingtheirincome,leadingtoapercapitaincomeofUS$24726in2008[10]comparedwithUS$22935in
2007, US$ 14724 in 2006,
US$13639in2005[11,12]andUS$8140in2000[13].Basedon2010
informa-tion,SaudiArabia is rankedat
ahighlevelintheHumanDevelopmentIndex
(0.75),whichgives thecountrya rankof 55outof 194 countries
[10].Theimprovement in thenational incomeisexpected to
impactpositivelyon itsvarious services including
thehealthcareservices.
Brief overview of health services development
Health services inSaudiArabiahaveincreased and improved
significantlyduring recentdecades [14].Thefirstpublic
healthdepartmentwas estab-lishedinMeccain1925basedonaroyaldecree
fromKingAbdulaziz[15].Thisdepartmentwas responsible for
spon-soringandmonitoring
freehealthcareforthepopulationandpilgrimsthroughestablishinganumberofhospitalsanddispensaries.Whileitwasanimportantfirst
step inprovidingcurativehealthservices, thenational
incomewasnotsufficient to achievemajor advancesinhealth care,
themajorityofpeoplecontinued to depend on
traditionalmedicineandtheincidenceofepidemicdiseases remained high
among thepopulationandpilgrims[15].Thenextcrucialadvancewas
theestablishmentof theMOH in1950under anotherroyaldecree
[15].Twentyyears later,the 5-year development plans
wereintroducedby thegovernment to im-proveall sectorsof thenation,
includ-ing theSaudihealthcare system[16].Since then, substantial
improvementsinhealth carehavebeen achieved inSaudiArabia.
Current structure of health services
Currently theMOHis
themajorgov-ernmentproviderandfinancerofhealthcare services in
SaudiArabia,with atotal of 244hospitals
(33277beds)and2037primaryhealthcare(PHC)
-
EMHJ Vol.17 No.10 2011
EasternMediterraneanHealthJournalLaRevuedeSantdelaMditerraneorientale
786
centres [4].These services
comprise60%ofthetotalhealthservicesinSaudiArabia[4].Theothergovernmentbod-ies
include
referralhospitals(e.g.KingFaisalSpecialistHospitalandResearchCentre),
security forcesmedical serv-ices,army forcesmedical
services,Na-tionalGuardhealthaffairs,MinistryofHigherEducationhospitals
(teachinghospitals),ARAMCOhospitals,RoyalCommission for Jubail and
Yanbuhealth services,
schoolhealthunitsoftheMinistryofEducationandtheRedCrescentSociety.Withtheexceptionofreferralhospitals,RedCrescentSocietyandtheteachinghospitals,eachoftheseagenciesprovidesservices
toadefinedpopulation,usuallyemployeesandtheirdependants.Additionally,
all of themprovidehealth services toall residentsduring crises and
emergencies [16].
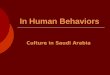
Jointly, thegovernmentbodiesoper-ate39hospitalswitha
capacityof10822beds [4].Theprivate sector alsocontributes to the
delivery of healthcare services, especially in cities
andlargetowns,withatotalof125hospitals(11833beds)and2218dispensariesandclinics(Figure1)[4].
The advancement in health serv-ices, combinedwithother factors
suchasimprovedandmoreaccessiblepubliceducation, increasedhealth
awarenessamong the community andbetter
lifeconditions,havecontributed to thesig-nificant improvements
inhealth
indica-torsmentionedearlier.Ithasbeennoted,however,thatdespitethemultiplicityofhealthserviceprovidersthereisnocoor-dinationorclearcommunicationchan-nels
among them, resulting in awasteof resources andduplicationof
effort
[17].For example, there are consider-ableopportunities to
takeadvantageofequipment, laboratories, training
aidsandwell-trainedpersonnel fromdiffer-ent countries.However, as a
result ofpoorcoordination, thebenefitof
theseopportunitiesislimitedwithineachsec-tor. Inorder toovercome
this and toprovidethepopulationwithup-to-date,equitable,
affordable, organized andcomprehensivehealthcare, a
royalde-creein2002ledtotheestablishmentoftheCouncilofHealthServices,headedby
theMinsterofHealthand
includingrepresentativesofothergovernmentandprivate health sectors
[18].AlthoughtheaimoftheCouncilwastodevelopapolicy
forcoordinationand
integrationamongallhealthcareservicesauthoritiesinSaudiArabia[19],significantprogresshasyettobeachievedinthisarea[20].
Figure 1 Current structure of the health care sectors in Saudi
Arabia (MOH = Ministry of Health) . Source of data: [4]
Employees &
their families
+
Emergencies
Armed forces medical services
Health services in the R oyal
Commission for Jubail & Yanbua
Red Crescent
Security forces medical services
National guard health affairs
% of hospital services provide by various health care sectors
in
Saudi Arabia
59.5%
21.2%
19.3%
MOH Other Govt. Private
Emergencies
Referral hospitals
Teaching hospitals
School health units
ARAMCO health services
Saudi health care system
Govt. sector (free) Private sector (fee)
MOH (public)
Other agencies
All levels of health care
All levels of health care
All levels of health care
-
787
Public health care system (Ministry of Health)
InaccordancewiththeSaudiconstitu-tion, thegovernmentprovidesall
citi-zensandexpatriatesworkingwithinthepublic sectorwith full and
freeaccesstoallpublichealthcareservices[7,21].GovernmentexpenditureontheMOHincreased
from2.8% in1970 [18] to6% in2005and6.2% in2009(Table1)
[4].According toWHOthe totalexpenditure on public health
during2009was5%ofgrossdomesticprod-uct [22].TheMOHis responsible
formanaging, planning and formulatinghealthpolicies and
supervisinghealthprogrammes, as well as
monitoringhealthservicesintheprivatesector[23].It isalsoresponsible
foradvisingothergovernment agencies and theprivatesectoronways
toachieve thegovern-mentshealthobjectives[16].
TheMOH supervises 20 regionaldirectorates-generalofhealthaffairs
invariouspartsof
thecountry[18].Eachregionalhealthdirectoratehasanumberofhospitalsandhealthsectorsandeveryhealth
sector supervises a number ofPHCcentres.The roleof
these20di-rectorates includes implementing
thepolicies,plansandprogrammesof
theMOH;managingandsupportingMOHhealthservices;supervisingandorganiz-ingprivatesectorservices;coordinatingwithother
government agencies;
andcoordinatingwithotherrelevantbodies[23].Figure2 illustrates
theorganiza-tional structureand the
relationshipofdepartmentswithintheSaudihealthcaresystem from
thecommunity
toMOHlevel.Healthfriendsisaselectivecom-mitteeconsistingofusefulandinfluentialcommunitymembers,
including repre-sentatives fromPHCcentres,whoareknowledgeable about
common
socialnormsandthepotentialofthecommu-nity.TheessentialroleofthiscommitteeistoliaisebetweenPHCcentresandthecommunitiestheyserve[24,25].
Levels of health care
servicesTheMOHprovideshealthservicesat3levels:primary, secondaryand
tertiary[4].PHCcentres
supplyprimarycareservices,bothpreventiveandcurative,referring cases
that requiremore ad-vanced care to public hospitals (thesecondary
level of care),while casesthatneedmorecomplex
levelsofcarearetransferredtocentralorspecializedhospitals (the
tertiary level of healthcare).
Transition to PHC
servicesUntilthe1980s,inlinewiththeexpecta-tionsofpopulation,health
services inSaudiArabiawere
largelycurative,em-phasizingtheprovisionoftreatmentforexistinghealthproblems
[18,23].Thecurative caremodel, however, canbecostly
tohealthproviders,whenmanydiseasescanbepreventedorminimizedthroughdevelopingapreventivestrat-egy.AvarietyofpreventivemeasureswererunbytheMOHthroughformerhealth
offices and to some
extentthroughmaternalandchildhealthcarecentres.Anumberofdisease
controlactivitieswere performedby verticalprogrammes,e.g.malaria,
tuberculosisandleishmaniasiscontrol[18,23].
In accordancewith theAlma-Atadeclarationat
theWHOGeneralAs-sembly in1978[26], theSaudiMOHdecided to activate
and develop thepreventive health services by adopt-ing the PHC
approach as one of itskeyhealthstrategies.Consequently,
in1980,aministerialdecreewasissuedto
establishPHCcentres.Thefirststepwastoestablishsuitablepremises
through-out the country.Existing facilities lo-cated
inadjacentareaswere
integratedintosingleunits.Theseincludedformerhealthoffices,maternalandchildhealthcentres
and dispensaries.Thehealthposts in small and
ruraldistrictswereupgradedtoPHCcentres[18,23].Thehealthcentresaimedto
focusonthe8elementsofthePHCapproach:educat-ing
thepopulationconcerningprevail-inghealthproblemsandthemethodsofpreventingandcontrollingthem;provi-sionof
adequate supplyof
safewaterandbasicsanitation;promotionoffoodsupplyandpropernutrition;provisionof
comprehensivematernal andchildhealthcare;
immunizationofchildrenagainstmajorcommunicablediseases;preventionandcontrolof
locally en-demicdiseases;appropriate treatmentofcommondiseasesand
injuries; andprovisionofessentialdrugs[24,25].
Focusingon aPHC strategy andapplying a logical referral
systemhashelped to reduce thenumberofvisitstooutpatientclinics
[23].About82%ofclientvisitstoMOHfacilitiesduring2009weretoPHCcentrescomprisingmorethan54millionPHCclients[4].Thecreationof
individual and familyhealthrecordsinsideeachPHCcentrehas
reducedduplicationof
consulta-tions.Theuseoftheessentialdrugslistanddocumentationofprescriptions
inpatienthealthfileshasnotonlyreducedthecostsofmedications,butalso
im-provedprescribingpractices.
Table 1 Budget appropriations for the Ministry of Health (MOH)
in Saudi Arabia in relation to the government budget, 200509
Year Government budget (SRa) MOH budget (SR) %b
2005 280 000 000 16 870 750 6.0
2006 335 000 000 19 683 700 5.9
2007 380 000 000 22 808 200 6.0
2008 450 000 000 25 220 200 5.6
2009 475 000 000 29 518 700 6.2
Source: [4]. aUS$ 1 = 3.75 SR; bAs a % of the total government
budget. SR = Saudi riyals
-
EMHJ Vol.17 No.10 2011
EasternMediterraneanHealthJournalLaRevuedeSantdelaMditerraneorientale
788
Inrecentyears, theMOHhascon-tinued todevelop
thenumberofPHCcentres(Figure3)andhasinitiatedfur-therprojectsaimedatdevelopinghealthcare
ingeneralandPHCs inparticular.Forexample, theprojectof
theCusto-dianoftheTwoHolyMosquesaimstoestablish2000advancedPHCcentres,andtodeveloptheexistingonesintermsofbuildings,workforceandservices.
Health services in the pilgrimage (hajj)
seasonSaudiArabiahasauniquepositionintheIslamicworld,asitembracesthe2holi-estcitiesof
Islam,MeccaandMedina.About2millionpilgrims fromallovertheworld
perform thehajj
annually.Duringthe2009season,therewere2.3millionpilgrims,69.8%ofwhomcamefromforeigncountries[4].Hostingsuchaneventannually
isamajorchallengethat requiresaplannedandorganizedeffort
acrossnumerous agencies
anddepartmentstoensureadequateessen-tialservices,suchashousing,transport,safetyandhealthcare[21].
Healthcareservicesinthehajjseasonprovidepreventiveandcurativecareforallpilgrims,irrespectiveoftheirnation-ality.Preventive
care includeshealtheducation programmes,
vaccinationandchemoprophylaxis forallpilgrimsviaquarantine
servicesat
airportsandlandports.Theprovisionofemergencyandcurativeservicestakesplacethroughanetworkofhealthcarefacilities.Forex-ample,in2009,therewere21hospitals,ofwhich7wereseasonal,withatotalof
3408bedsand176bedsforemergencyadmissions.Therewerealso157PHCcentres,ofwhich119wereseasonal.Onaverage,eachPHCcentretreated4734pilgrims.Thetotalworkforce
recruitedtowork in these facilitiesduring2009was17886;an
increaseof5%on
thepreviousyear.Ofthese,69%werephysi-cians,nursesandalliedhealthpersonnel[4].Onaverage,eachphysiciantreatedabout612pilgrims,while
eachnursetreatedabout372.
Figure 2 Organizational structure of the Ministry of Health
(public) health care system in Saudi Arabia. Source: [23]
2037
192519251905
1848
1986
1750
1800
1850
1900
1950
2000
2050
2100
2004 2005 2006 2007 2008 2009
No
. of
PH
C c
en
tre
s
Figure 3 Trends in the number of primary health care (PHC)
centres in the Ministry
of Health in Saudi Arabia, 200409. Source: [4]
-
789
Every year, the Saudi health
careagencies,particularlytheMOH,seektoimprove thehealthcare
services
topil-grims[21].Nevertheless,thefactthatalltheservicesareprovided
freeofchargeforallpilgrims is
creatingconsiderablepressureonthehealthcarebudgetanditmaybenecessarytoseekwaystoprovidebetterservicesata
lowercost.Onesug-gestionistointroduceaseasonalhealthinsuranceforallinternationalpilgrims.
Challenges for health care reform
WhilemanystepshavebeenundertakenbytheMOHtoreformtheSaudihealthcare
system, a number of
challengesremain.Theserelatetothehealthwork-force,financingandexpenditure,chang-ingpatternsofdiseases,
accessibility tohealth care services, introducing
thecooperativehealth insurance
scheme,privatizationofpublichospitals,utiliza-tionofelectronichealth(e-health)strat-egiesandthedevelopmentofanationalsystemforhealthinformation.
Health workforceTheSaudihealth care system is chal-lengedby the
shortageof localhealth
careprofessionals, suchasphysicians,nurses
andpharmacists.Themajorityofhealthpersonnelareexpatriatesandthisleadstoahighrateofturnoverandinstability
in theworkforce [27].Ac-cording to theMOHthe
totalhealthworkforceinSaudiArabia,includingallother sectors, is
about248000;morethanhalfof them(125000)work intheMOH[4].Saudis
constitute38%ofthistotalworkforce.Ofthese,23.1%arephysicians,while32.3%arenurses(Figure4).IntheMOH,Saudisconsti-tuteabout54%ofthehealthworkforce,(physicians22.6%andnurses50.3%).The
ratesofphysicians andnurses
inSaudiArabiaare16and36respectivelyper10000population, lower than
inothercountriessuchasBahrain(30and58per10000),Kuwait(18and37per10000),Japan(12and95per10000),Canada
(19 and 100 per
10000),France(37and81per10000)andtheUnitedStatesofAmerica(27and98per10000)[28].
The ability to formulate and ap-plypractical strategies to
retain andattractmoreSaudis into themedicaland health professions,
particularlynursing, isaclearpriority
foreffectivereformoftheSaudihealthcaresystem.Manyeffortshavebeen
takenby the
government to teach and trainSau-dis forhealthprofessional
jobs.Since 1958 , anumberofmedical,
nursingandhealthschoolshavebeenopenedaround thenation tomeet this
goal[7].Apart fromprivate colleges andinstitutes, therearea
totalof73col-legesformedicine,healthandnursingaswell as4health
institutes inSaudiArabia [4].Efforts to establish suchcollegesare
inaccordancewith train-ingprogrammesthataimtosubstitutethe
largelyexpatriateworkforcewithqualifiedSaudiArabiannationals inall
sectors, includinghealth
[18,29].Thebudgetallocationfortrainingandscholarshipshas
increasedandmanyMOHemployeesareofferedachancetopursue their studies
abroad [18].Thisstrategycould improve
theskillsofcurrentemployees,raisethequalityofhealthcareand,itishoped,decreasetherateofturnoveramonghealthpro-fessionals.However,theseeffortsmaynotbeenoughtosolvethechallenges.TheproportionofSaudiArabianhealthprofessionals
in theMOHworkforceisexpectedtodecreaseinthefutureastheexpansion
inhealthcare facilitiesaround thecountryhas
theeffectofspreadingascareresourceevenmorethinly[17,30].
0
10
20
30
40
50
60
70
80
90
100
MOH Other govt. Private Total
%Physicians
Nurses
Allied health
Figure 4 Distribution of Saudi health personnel in the Ministry
of Health (MOH), other government and private health care
sectors in Saudi Arabia, 2009. Source: [4]
-
EMHJ Vol.17 No.10 2011
EasternMediterraneanHealthJournalLaRevuedeSantdelaMditerraneorientale
790
Morerealisticplansand
long-termstrategiesneedtobeconsolidatedbytheMOHincooperationwithgovernmentandprivatesectors.Agoodexampleofsuchcooperation
is theKingAbdullahinternational scholarshipprogrammewhichwas
establishedby theMinis-try ofHigherEducation. In its stage4,
priorityhasbeengiven tomedicalspecialists includingmedicine,
nurs-ing,pharmacyandotherhealthmajors[31].However,moremedicalcollegesand
trainingprogrammesneed tobeestablishedaround the country.Newlaws
and regulations to develop
andreorganizemedicalhumanresourcesbytheMOHareurgentlyrequired.
Reorganization and restructuring of the
MOHThepublichealthsectorisoverwhelm-ingly financed, operated,
controlled,supervisedandmanagedbytheMOH[32].Thismodelofmanagementmaynotabletomeetthepopulationshealthcareneeds
into the futureunless
seri-ousandwell-plannedstepsaretakentoseparate thesemultiple
roles.Possiblesolutionsincludegivingmoreauthoritytotheregionaldirectorates,applyingthecooperativehealth
insurance schemeand encouraging
theprivatizationofpublichospitals.
Decentralization of health services and autonomy of
hospitalsTomeet increasing pressure on
theMOH,moreautonomyhasbeengivento theregionaldirectorates in
termsofplanning, recruitmentofprofessionalstaff, formulating
agreements withhealth services providers
(operatingcompanies)andsomelimitedfinancialdiscretion.Ithasbeensuggestedthatthefunctioningoftheregionaldirectoratesisadverselyaffectedbythelackofindi-vidualbudgetsandspendingauthority[16].Expenditure
for themajorityoftheir activitiesmustbe
authorizedbytheMOH,thusaffectingtheautonomyofregionaldirectoratesandhamperingeffectivedecision-making.
In termsofhospitalautonomy, theMOHhas triedanumberof
strategiesforimprovingthemanagementofpublichospitalsduringpastdecades,includingdirectoperationbytheMOH,coopera-tionwithothergovernments
such
theNetherlands,GermanyandThailand,partialoperationbyhealthcarecompa-nies,comprehensiveoperationbyhealthcare
companies and the autonomoushospital system[33].Considering
theadvantagesanddisadvantagesof theseapproaches, theMOHhas
standard-izedanautonomoushospitalsystemfor31publichospitals in
various regions[34].Theautonomoushospitalsystemforpublichospitals
isexpectedtoraisetheefficiencyof theirperformance
inbothmedicalandmanagerialfunctions,achieve financial and
administrativeflexibility through adopting a
directbudgetstrategy,applyqualityinsuranceprogrammes and simplify
the con-tractualprocesswithqualifiedhealthprofessionals[33].
In2009,
theMOHissuednewregulationsforself-operatingpublichospitalstoensureahighlevelofmanagementpracticesandto
improvethequalityof servicesprovided
[35].GivingmoreautonomytohospitalswillhelpthetransitiontofullprivatizationofpublichospitalsinSaudiArabia.Itgivespublichospitalsmoreexperienceinthemanagementof
theirbudgets, healthcarequalityandworkforce.
Health insurance in Saudi
ArabiaFundinghealthcareservicesisacentralchallengefacedbytheMOH[32].Sincethe
total expenditureonpublichealthservices comes from
thegovernmentandtheservicesare free-of-charge, thislead
toconsiderablecostpressureonthegovernment,particularly
inviewoftherapidgrowthinthepopulation,thehighpriceofnew
technologyand thegrowing awareness abouthealth
anddiseaseamongthecommunity[14].Tomeetthegrowingpopulationdemandsforhealthcareand
toensure thequal-ity of services provided, theCouncil
forCooperativeHealth
Insurancewasestablishedbythegovernmentin1999[19].Themain roleof
thisCouncil isto introduce, regulateand superviseahealth
insurancestrategy for theSaudihealthcaremarket.
The implementation of a coop-erative health insurance
schemewasplannedover3stages.Inthefirststage,the cooperativehealth
insurancewasappliedfornon-SaudisandSaudisintheprivatesector,inwhichtheiremployershavetopayforhealthcovercosts.Inthesecond
stage, the cooperative
healthinsuranceistobeappliedforSaudisandnon-Saudisworkinginthegovernmentsector.The
governmentwill pay thecooperativehealth insurancecosts
forthiscategoryofemployee. In thefinalstage, thecooperativehealth
insurancewill be applied toother groups, suchas pilgrims [36].Only
the first stagehas been implemented to
date,withthecooperativehealth insurancebeingimplemented gradually
in a 3-phaseprogrammetoemployeesoftheprivatesector and
theirdependants
[14,37].Thefirstphasecoveredcompanieswith500ormoreemployees,while
thesec-ondphase applied to
employerswithmorethan100workers.ThethirdphaseincludedemployeesofallcompaniesinSaudiArabiaaswellasdomesticwork-ers
[14,37].The government is nowworkingsystematically toapply
there-maining2stagesforemployeesinthegovernment sectorand
forpilgrimsbefore theyprivatize the state-ownedhealthcare
facilities[14].No
informa-tionisavailableyetregardingthecoop-erativehealthinsuranceschemeforthepopulationofSaudiArabiaother
thanemployeesandexpatriates.
While themarket for
cooperativehealthinsuranceinSaudiArabiastartedwithonly1 company
in2004, it cur-rently involves about 25 companies.The
introductionof the scheme is
in-tendedtodecreasethefinancialburdenonSaudiArabiadue to the costs
as-sociatedwithprovidinghealthservicesfree-of-charge. Itwill
alsogivepeople
-
791
moreopportunitytochoosethehealthservicestheyrequire[14].Therealchal-lengeforpolicy-makersinSaudiArabiais
to introduce a comprehensive, fair,and affordable service for
thewholepopulation. Clearly lessons can belearned
fromtheexperiencesofothercountries,includingtheadvantagesanddisadvantagesofdifferentschemes.
Privatization of public
hospitalsPrivatizationofpublichospitalshasbeenseenbypolicy-makers
and research-ersasthebestwaytoreformtheSaudihealth care system
[38,39]. Steps toimplementaprivatizationstrategyhavebeen initiated
and related regulationhasbeenpassedbythegovernment.Asa result,
anumberofpublichospitalsarelikelytobesoldorrentedtoprivatefirmsoverthenextfewyears[14].Priva-tizationofhospitalsisexpectedtobringanumberofadvantagestothegovern-mentandtothenation.Itishopedthatprivatizationwill
assist in speedingupdecision-making, reducing thegovern-ments
annual expenditureonhealthcare,producingnewfinancial sourcesfor
theMOH and improving healthcareservices[38].
On the other hand,
privatizationmayaffectthecurrentintegratedsystembetweenhospitals
andPHC facilities[14].Ashospitalsbecomeprivatized,theywill focuson
attractingpatients,even thosewhomaynot
requirehos-pital-levelcare.Moreover,peoplewithhealth covermayprefer
to accessbighospitalsdirectly insteadof viaPHCcentresor
communityhospitals.Ad-ditionally, private hospitalswill
haveincentivestoshiftnon-refundablecostsback to the public PHC
[14]. Suchpracticeswillplacefinancialburdensonthegovernment.
A furtherdrawbackofprivatizationis that the traditional
state/publichos-pitalswillnotbeabletoabsorbenoughof the health
caremarket comparedwith private companies, unless theyupgradeatall
levels(e.g.management,
infrastructure andworkforce)beforestarting toprivatize [14]. In
themovetoprivatization,privatecompaniesarelikely to focus their
activities withincities and largercommunities, leavingpeople in
ruralareasatadisadvantage.Thegovernmentshouldsetregulationsthatprotecttherightsofruralcommu-nities
andprovide themwith fair andequitablehealthcareservices.
Finally,ifthegovernmentdoesnotap-plyadequatecontrolover
thehealthcaremarket,
expenditureonhealthcaremayincreasedramaticallyasa
resultofhigherpricingandprofit-seekingbehaviour[14].
Accessibility to health servicesOptimizing
theaccessibilityofhealthcare services requires equity in
thedistribution of health care facilitiesthroughout thenation and
equityofaccess tohealthprofessionals, includ-ingtransport
toservicesandproviders.Accessibilityisalsoaffectedbythelevelofcooperationbetweenrelatedsectors[23,39].ThecurrentMOHstatisticsindicate
that there
isamaldistributionofhealthcareservicesandhealthprofes-sionals
across geographical areas
[4].Peopleexperiencelongwaitinglistsformanyhealthcareservicesand
facilities[14].Additionally, there is adearthofservices
fordisadvantagedgroupssuchas theelderly, adolescentsandpeoplewith
special needs such as disability,particularly in ruralareas
[39].Finally,manypeopledonothavetheabilitytoaccesshealthcare
facilities,particularlythoselivinginborderandremoteareas.
Inorder to improveaccessibility tohealth care services in all
partsof
thecountry,aholisticstrategyfortheredistri-butionofhealthcareservices,involvingPHCcentres,generalhospitals,centraland
specialisthospitals aswell as
thehealthprofessionals,shouldbeadoptedby
theMOH.TheMOHshouldalsoliaisewithothersectorssuchtransport,waterandpowercompaniesandsocialsecurity
services in order to
developservicesindeprivedareasandtocareforpeoplewiththegreatestneeds.
Patterns of diseasesThechange in disease patterns
fromcommunicable tononcommunicablediseases in Saudi Arabia is
anotherchallenge that needsmore attentionfrom
theMOH[21].Therehasbeenanalarming increase in theprevalenceof
chronicdiseases, such asdiabetes,hypertension, andheartdiseases,
can-cer,geneticblooddisordersandchild-hoodobesity[28,40,41].Treatmentofchronicdiseasesiscostlyandmayevenbe
ineffective [40]. For example, theannual cost for
treatmentofdiabetesmellitus
inSaudiArabiawasestimatedtobe7billionSaudi riyal
(SR)(US$1.87billion) [42].Earlyprevention isthemost effectiveway to
reduce theprevalenceofchronicdiseasesand thecosts anddifficulties
associatedwithtreatment in the
laterstagesofdisease.Anyprojectedreformsinthehealthcaresystemmust
involveplans to addressthischangeinemphasize.
Promotion and prevention programmes for crisesDevelopment and
implementationof practical plans and procedures tomeetnational
crises
inSaudiArabia,suchaswars,earthquakesandfiresandexplosionsatpetroleumfactories,areafurtherimportantneed.Roadtrafficac-cidents,forexample,killedmorethan39000andinjuredabout290000peoplebetween1995and2004[43].Accord-ingtoWHO,roadtrafficaccidentsarenowthehighestcauseofdeath,
injuryanddisabilityinadultmalesaged16to36years inSaudiArabia
[32].Caringforpeople affectedby roadaccidentsconsumes a
significantproportionoftheMOHbudget;forexample,thecostof treating
injuredpeopleduring2002wasestimated
tobeSR652.5million(US$174million) [43].These fundscould be used to
develop the healthsystemand improve services.Plans tomanage
issuesof thiskindneed tobecomprehensive
andwell-coordinatedamongtherelatedsectorsinordertobeachievable.
-
EMHJ Vol.17 No.10 2011
EasternMediterraneanHealthJournalLaRevuedeSantdelaMditerraneorientale
792
References
Gallagher EB. Modernization and health reform in Saudi Ara-1.
bia, Chapter 4. In: Twaddle AC, ed. Health care reform around the
world. London, Auburn House, 2002:181197.
The world health report 2000. Health systems: improving per-2.
formance. Geneva, Word Health Organization, 2000.
Key indicators.3. Central Department of Statistics and
Information, Saudi Arabia [online database]
(http://www.cdsi.gov.sa/english, accessed 27 June 2011).
Health statistical year book.4. Riyadh, Saudi Arabia, Ministry
of Health, 2009.
Statistical year book 455. . Riyadh, Saudi Arabia, Central
Depart-ment of Statistics and Information, 2009.
World population 20026. . New York, United Nations, 2003.
Aldossary A, While A, Barriball L. Health care and nursing in 7.
Saudi Arabia. International Nursing Review, 2008, 55:125128.
Profile research: Kingdom of Saudi Arabia8. . Oil and Gas
Directory Middle East [online factsheet]
(http://www.oilandgasdirectory.com/research/Saudi.pdf, accessed 27
June 2011).
Exports of Saudi Arabia: the main commodities9. . Riyadh, Saudi
Arabia, Ministry of Finance, 2010.
Human10. development report 2010.The real wealth of nations:
Pathways to human development. New York, United Nations, 2010.
Human11. development report 2009. Overcoming barriers: Human
mobility and development. New York, United Nations, 2009.
e-health and national health information systemsThere is
increasingconcernabout
theunderutilizationofelectronichealthsys-tems inSaudiArabia.
Implementationofe-healthandelectronic
informationsystemshasalreadystartedinanumberofhospitalsandorganizations
suchastheKingFaisal specialisthospital
andresearchcentre,nationalguardhealthaf-fairs,medicalservicesofthearmyforcesand
university hospitals [44].Whileuptakeof e-health systems
ismovingslowlyinMOHinstitutions,thereareanumberofinformationsystemsoperat-ing
in the regionaldirectoratesand incentralhospitals.Unfortunately,
theseinformationsystemsarenotconnectedtoeachotherortootherprivateorspe-cializedhealthorganizations[44].
Todevelope-healthservices in thepublic sector,
abudgetofSR4billion(US$1.1billion)wasallocatedby
theMOHtoruna4-yeardevelopmentpro-gramme(200811)[45].Additionally,aseriesofconferencesone-healthhavebeenheldbytheSaudiAssociationforHealth
Information toemphasize theimportanceof e-health in
enhancingthequalityofhealthcaredeliveryandtoexplorethenecessarystrategies,policies,applicationsandinfrastructure[46].
Morecoordinationamongdifferenthealthcareprovidersisneededinordertoenhancetheuseofe-healthstrategiesandtolaunchacomprehensivenationalsystem
forhealth information.Ahigh
levelofcoordinationmustbeachievedwithotherrelatedsectorstoprovidetherequiredinfrastructuresuchas
internetandphoneservices.
New strategy for health care servicesTomeet the challengesof
theSaudihealth care system and to improvethequalityofhealthcare
services, theMOHhas set a national strategy forhealthcare
services.This strategywasapprovedby
theCouncilofMinistersinApril2009.Itfocusesondiversifyingfunding
sources;developing informa-tion systems; developing
thehumanworkforce; activating the
supervisionandmonitoringroleoftheMOHoverhealthservices;encouragingtheprivatesector
to take itsposition inprovidinghealth services; improving
thequalityofpreventive, curative and rehabilita-tive care;
anddistributinghealthcareservicesequallytoallregions.
Thenationalstrategyforhealthcareservices is tobe implementedby
theMOHincooperationwithotherhealthcareprovidersanditwillbesupervisedby
theCouncilofHealthServices.A20-year timeframe for achieving
theobjectivesofthisstrategyhasbeeniden-tified[39].
Conclusion
Asa resultof thecontinuedattentiontoand support from
thegovernment,
Saudi health services have advancedgreatlyover recentyears inall
levelsofhealthservices:primary,secondaryandtertiary. Asa
consequence, thehealthof theSaudipopulationhas
improvedmarkedly.TheMOHhas introducedmanyreforms to its
services,with sub--stantialemphasisonPHC.
Despite these achievements,healthservices,and
inparticularpublicsectorhealthservices,arestillfacingmanychal--lenges.These
include:humanresourcedevelopment;separationoftheMOHsmultiple roles
(financing,
provision,controlandsupervisionofhealthcaredelivery);diversifyingfinancialsources;implementing
the
cooperativehealthinsurance,privatizationofpublichos-pitals,effectivemanagementof
chronicdiseases;developmentofpracticalpoli-ciesfornational
crises;establishmentofanefficientnationalhealthinformationsystemandtheintroductionofe-health.Inordertoaddressthesechallengesandcontinue
to improve the statusof theSaudi health care system, theMOHandother
relatedsectors shouldcoor-dinate their efforts to implement
andensure the successof thenewhealthcarestrategy.
Acknowledgements
Thispaper ispartof thefirst authorsdoctoral research, supported
by thegovernmentofSaudiArabia.
-
793
General statistics12. . Riyadh, Saudi Arabia, Ministry of
Economy and Planning, 2007.
Saudi Arabia. Data13. . The World Bank [online database]
(http://data.worldbank.org/country/saudi-arabia, accessed 15 June
2011).
Walston S, Al-Harbi Y, Al-Omar B. The changing face of
health-14. care in Saudi Arabia. Annals of Saudi Medicine, 2008,
28:243250.
Alharthi F et al. 15. Health over a century. Riyadh, Ministry of
Health and ASBAR Centre for Studies Research and Communication,
1999.
Mufti MHS. 16. Healthcare development strategies in the Kingdom
of Saudi Arabia. New York, Kluwer Academic/Plenum, 2000.
Alhusaini HA. [17. Obstacles to the efficiency and performance
of Saudi nurses at the Ministry of Health, Riyadh Region:
analytical field study]. Riyadh, Saudi Arabia, Ministry of Health,
2006 [in Arabic].
Health system profile. Saudi Arabia18. . World Health
Organization Eastern Mediterranean Regional Health System
Observatory [online database].
(http://gis.emro.who.int/HealthSystemOb-servatory/Profile/Forms/frmProfileSelectionByCountry.aspx?CountryID=SAP000000000000000000&CountryName=Saudia%20Arabia,
accessed 15 June 2011).
[19. Vision and tasks of the Council of Health Services in Saudi
Arabia]. Council of Health Services [website]
(http://www.chs.gov.sa/COHS/default.aspx, accessed 15 June 2011)
[in Arabic]
Alkhazem M. [Health coordination starts from the Ministry]. 20.
Al Riyadh Daily. 12 April 2009 [in Arabic].
Jannadi B et al. Current structure and future challenges for the
21. healthcare system in Saudi Arabia. Asia Pacific Journal of
Health Management, 2008, 3:4350.
Countries: Saudi Arabia22. . Word Health Organization
[website](http://www.who.int/countries/sau/en/, accessed 15 June,
2011).
Al-Yousuf M, Akerele TM, Al-Mazrou YY. Organization of the 23.
Saudi health system. Eastern Mediterranean Health Journal, 2002,
8:45.
Al Mazrou Y, Al-Shehri S, Rao M. 24. Principles and practice of
primary health care. Riyadh, Saudi Arabia, Ministry of Health,
1990.
Al Mazrou Y, Salem AM. [25. Primary health care guide]. Riyadh,
Saudi Arabia, Ministry of Health, 2004 [in Arabic].
Al-Ahmadi H. Quality of primary health care in Saudi Arabia: 26.
a comprehensive review. International Journal for Quality in Health
Care, 2005, 17:331346.
Saudi Arabia: country cooperation strategy: at a glance27. .
World Health Organization [online factsheet]
(http://www.who.int/countryfocus/cooperation_strategy/ccsbrief_sau_en.pdf,
ac-cessed 15 June 2011).
World health statistics28. . Geneva, Word Health Organization,
2010.
Tumulty G. Professional development of nursing in Saudi Ara-29.
bia. Journal of Nursing Scholarship, 2001, 33:285290.
Alamri AS, Rasheed MF, Alfawzan NM. [30. Reluctance of Sau-di
youth towards the nursing profession and the high rate of
unemployment in Saudi Arabia: causes and effects]. Riyadh, Saudi
Arabia, King Saud University, 2006 [in Arabic].
[31. Program of the Custodian of the Two Holy Mosques for
studying overseas (Phase IV)]. Ministry of Higher Education, Saudi
Arabia [website] (http://kas.mohe.gov.sa/kas4/indexu4.aspx,
ac-cessed 28 June 2011) [in Arabic].
Country cooperation strategy for WHO and Saudi Arabia 200632.
2011. Cairo, World Health Organization Regional Office for the
Eastern Mediterranean, 2007 (EM/ARD/014/E/R).
Al-Ateeq FA. 33. Experience of Saudi Arabia in operation of
public hospitals: the transition from companies operating system to
self-operating system. Paper presented at the Conference on Recent
Trends in the Management of Private and Public Hospitals in the
Arab World, 1214 March 2002. Cairo, Arab Administrative Development
Organisation, 2002.
[34. Achievements of the Ministry of Health]. Ministry of
Health, Saudi Arabia [website]
(http://www.moh.gov.sa/Ministry/MediaCenter/News/Pages/NEWS-2007-9-24-001.aspx,
ac-cessed 28 June 2011) [in Arabic].
Al-Zahrani S. [Requiring employees of self-operating public 35.
hospitals to work for six days per week instead of five].
Al-Madinah Daily, 26 July 2009 [in Arabic].
Alsharif AI. 36. Health system and insurance in Saudi Arabia.
Paper presented at the Board of Healthcare Funders Southern African
Annual Conference, Durban, 3-16 July 2008. Port Elizabeth, South
Africa, Providence Healthcare Risk Mangers, 2008.
Al-Shaikh S. Saudi health care sector: need for more invest-37.
ment. Arab News, 7 August 2006.
Saati A. [Privatisation of public hospitals: future vision and
38. proposed framework]. Al-Egtisadia Daily, 2 December 2003 [in
Arabic].
[New strategy for health services in Saudi Arabia]. 39.
Al-Egtisadia Daily, 9 September 2009 [in Arabic].
Al-Qurashi MM et al. The prevalence of sickle cell disease in
40. Saudi children and adolescents: a community-based survey. Saudi
Medical Journal, 2008, 29:14801483.
Al-Turki YA. Overview of chronic diseases in the Kingdom of 41.
Saudi Arabia. Saudi Medical Journal, 2000, 21:499500.
[42. Allocation of 110 million riyals for establishment of 20
diabetes care centre]. Riyadh, Ministry of Health, 2007
(http://www.moh.gov.sa/Ministry/MediaCenter/News/Pages/NEWS-2007-10-29-001.aspx,
accessed 28 June 2011) [in Arabic].
Assaied RA. [43. Economic impact of traffic accidents]. Riyadh,
Naif Arab University for Security Sciences, 2008 [in Arabic].
Altuwaijri MM. Electronic-health in Saudi Arabia: just around
44. the corner? Saudi Medical Journal, 2008, 29:171178.
Qurban MH, Austria RD. 45. Public perception on e-health
services: implications of preliminary findings of KFMMC for
military hos-pitals in KSA. Paper presented at the European and
Mediter-ranean Conference on Information Systems (EMCIS2008), 2526
May 2008. Dubai, Information Systems Evaluation and Integration
Group, 2008.
Towards national e-health. 46. Saudi e-health conference, 1719
March 2008. Riyadh, Saudi Association for Health Informat-ics, 2008
(http://www.saudiehealth.org/2008/, accessed 28 June 2011).