Embed Size (px)
Citation preview

Healthy Urban Development Unit
Health and Urban Planning Toolkit


1
Contents
Summary for PCT Chief Executives 02Summary for Directors of Planning and Development 03Introduction 04The purpose of the Toolkit 04The suggested approach 05
Phase 1: Background to engagement 07
The case for engagement 09Population growth 09Policy and legislation drivers 09The role of PCTs 11The role of Local Planning Authorities 12Complementary health and urban planning interests 12Barriers will need to be overcome first! 13What are the outcomes for my organisation? 13
Aligning the PCT and Local Planning Authority 15Strategy 15Systems 16Structure 16Culture 17
Phase 2: Defining the relationship 19
Initiating the engagement process 21Mapping organisational structures 21
Diagnosis 23The Alignment Checklist 24
Defining local issues and priorities 29Health issues and priorities 29Local Planning Authority issues and priorities 30
Setting up an engagement agreement 33
Phase 3: Making engagement work 35
Health and the Local Development Framework 37The strategic framework 37Delivery mechanisms 37Aligning planning and health strategies and processes 38Preparing the Local Development Framework 41Conclusion 48
Integrating health in development control 51The relationship between development control,
health and the PCT 51Planning application process 51Aligning the PCT with the planning application process 54Dealing with Environmental Impact Assessment and
Health Impact Assessment 56Planning obligations and section 106 agreements 56
Building capacity to make better engagement a reality 60Building PCT capacity 60Within the Local Planning Authority 64Summary 64
Summing up 65
Glossary of agencies, health and planning terms and useful links 67
Acknowledgements 75
Background on HUDU 75
Appendices (contained in a separate document)
Appendix 1: Understanding your Primary Care Trust and Local Planning Authority
Appendix 2: Engagement agreement templateAppendix 3: Environmental Impact Assessment
and Health Impact AssessmentAppendix 4: Planning application response templateAppendix 5: Example PCT planning application
response process Appendix 6: Draft job description and work
programme for a town planner employed by a PCT

2
Summary: Influencing planning for health – a message for PCT Chief Executives
The KEY steps that we recommend based on good practice and on actionresearch are set out here – can you say you are up to scratch?
1. Make contact with your Borough Planning department at the highest level
2. Identify staff whose job it will be to talk to the Borough planners
3. Audit current arrangements jointly and agree a simple protocol formanaging communications on planning and health
4. Make sure that you are a consultee in the process for producing the LocalDevelopment Framework and get to know the timetable
5. Make sure your public health report assesses the impacts of the widerdeterminants of health and plots the patterns of ill health and inequalities
6. Make sure your LDP and estates Plan or SSDP contains an assessment of current health services and buildings and plots their location andcatchments
7. Understand the future pattern of growth in the Borough and the likelypopulation changes
8. Work with the Borough to agree key policies to promote health and to plothow the supply of health services matches the projected demand over thenext 15 years
9. Agree arrangements and responsibilities for monitoring planningapplications that have implications for health
10. Agree with the Borough how s106 agreements will contribute to theprovision of new health facilities
11. Put in place sound financial procedures for making use of s106 financial contributions
12. Predict what amount to expect each year from s 106 contributions andensure that it’s reflected in the financial plan and reported on regularly atBoard level.
13. Meet with the Borough now and again to check how things are going
HUDU is there to support you in this process. This toolkit tells you how.
‘the level ofpartnership...between planningand health is stillunderdeveloped...’

3
Summary: Integrating health into planning – a message for Directors of Planning and Development
The KEY steps that we recommend based on good practice and on actionresearch are set out here – can you say you are up to scratch?
1. Make contact with your PCT at the highest level
2. Identify staff whose job it will be to talk to the health sector
3. Audit current arrangements jointly and agree a simple protocol for managing communications on planning and health
4. Make sure that the PCT (as well as the SHA) is a consultee in the process for producing the Local Development Framework and make sure they knowthe timetable
5. Make sure your Core Strategy assesses the impacts of the wider determinantsof health and plots the patterns of ill health and inequalities
6. Insist on an up to date assessment of current health services and buildings and plots their location and catchments
7. Explain the future pattern of growth in the Borough and the likely population changes to the PCT
8. Work with the PCT to agree key policies to promote health and prepare aspatial plan to show how the supply of health services matches the projecteddemand over the next 15 years
9. Agree arrangements and responsibilities for monitoring planning applicationsthat have implications for health
10. Agree with the PCT how s106 agreements will contribute to the provision ofnew health facilities and insert them into relevant LDDs
11. Put in place sound financial procedures for making use of s106 financial contributions
12. Meet with the PCT now and again to check how things are going
HUDU is there to support you in this process. This toolkit tells you how.
‘Performancemanagement of bothPCTs and Boroughswill increasingly lookfor evidence ofpartnership workingto improve health...’

Introduction
4
The purpose of the Toolkit
This Toolkit has been prepared to assist PCTs and Local Planning Authorities to improvejoint working to enable health to be addressed through the planning system. To do this,the Toolkit:
• sets out the case for more effective engagement between PCTs and Local PlanningAuthorities;
• provides PCTs and Local Planning Authorities a means of identifying weaknesses intheir existing relationship;
• provides a framework for collaboration between PCTs and Local Planning Authorities;• provides information on the planning system and health;• provides tools to support an ongoing working relationship; and• provides a step by step guide to improving engagement.
For PCTS, this toolkit aims to strengthen thecommon understanding of the ways in whichthe wider determinants of health can beenhanced through effective planning policesand the ways in which planning for healthservices and plans for the physical developmentof Boroughs can be integrated.
For Borough Planners, this toolkit aims tostrengthen the common understanding of theways in which the wider determinants of healthcan be enhanced through effective spatialplanning polices. It highlights the ways in whichplanning for health services and plans for thephysical development of Boroughs can beintegrated and the very real benefits that can be achieved.
Partnership working is becoming ever moreimportant in the area of health and localgovernment. Many PCTs and Boroughs alreadyhave joint appointments and partnershipworking under section 31. All PCTs andBoroughs contribute to the Local StrategicPartnership. The drive to partnership workingwill become even stronger as the statutory dutyunder the Local Government White Papercomes into force. Performance management ofboth PCTs and Boroughs will increasingly lookfor evidence of partnership working to improvehealth and reduce inequalities.
The links between the environment and healthare well known but the level of partnership orcollaborative working between planning andhealth is still underdeveloped in some places.

The suggested approach
5
Phase 1: Background to engagement
Phase 2: Defining the relationship
Phase 3: Making engagement work
Phases
It is suggested that a PCT and Local Planning Authority follow a systematic approach to buildingthe relationship needed to engage and making it work. An ad hoc approach runs the risk ofmissing important steps.
The steps involved are set out below.
The Steps
1. Identify why engagement between the PCT and Local Planning Authority is a necessity.
2. Understanding the principles of organisational collaboration between the PCT and LocalPlanning Authority.
3. Identify key communication links between the PCT and Local Planning Authority.
4. Use the Alignment Checklist to diagnose the relationship between the PCT and LocalPlanning Authority.
5. Identify the local issues and priorities that the PCT and Local Planning Authority willneed to address.
6. Prepare a simple engagement agreement between the PCT and Local Planning Authorityto set out expectations.
7. Ensure the Local Development Framework and health strategies are mutually aligned.
8. Ensure the Development Control process delivers health outcomes and involves the PCT.
9. Build the capacity of the PCT and Local Planning Authority staff to engage.

6BedZED, London Borough of Sutton

7
The first phase concentrates on understanding the merits of engagement and making the decisionsnecessary to initiate the engagement process involved in Phase 2, and involves the two stepsillustrated below.
Phase 1: Background to engagement
Key messages of this section
• Significant population growth and change will put pressure on PCTs and LocalPlanning Authorities and make it difficult for them to achieve their aimsindependently.
• PCTs can help address the wider determinants of health to improve health and tackleinequalities, and improve the delivery of health services through the planning system.
• Local Planning Authorities must engage with PCTs to achieve sustainabledevelopment and meet statutory obligations.
• The benefits of engagement will outweigh the costs.
• PCTs and Local Planning Authorities will need to align their strategies, systems andstructures to enable engagement.
• A supportive organisational culture will need to underpin engagement.
• Planning obligations (also known as section 106 agreements, or simply as s106) offer a significant contribution to the cost of providing health services and the PCT budget.
Phase 1: Background to engagement
Phase Steps
1. Identify why engagement between the PCT and Local Planning Authority is a necessity.
2. Understanding the principles of organisational collaboration between the PCT and LocalPlanning Authority.

Health and Urban Planning Toolkit Phase 1: Background to engagement
8

Step 1 Understand why engagement between a PCT and Local Planning Authority is a necessity.
Health and Urban Planning Toolkit Phase 1: Background to engagement
9
Population growth
The population of London is projected to growby 895,0001 people by 2021, generated bysignificant development.
There is a risk that the development driving thisgrowth and change will not facilitate improvedcommunity health and well-being andperpetuate health inequalities. This growth willalso increase demand for health services acrossLondon. Demographic profiles of populationsacross London will also change and affect thenature of the demand. This will have significantimplications for the delivery of health services.PCTs will need to tackle these issues throughthe planning system, which manages thegrowth.
Local Planning Authorities need to integratehealth issues into their Local DevelopmentFrameworks so that health outcomes can bedelivered to achieve sustainable development,but will be unable to do so if the growthplanned does not take health into account.
Policy and legislation drivers
Health and urban planning sectors areincreasingly driven towards shared andoverlapping agendas, resulting in the need toengage and collaborate. A number of nationalpolicy and legislation drivers have influencedthis.
Health
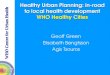
The ‘fully engaged scenario’ proposed by DerekWanless in his report Securing our FutureHealth: Taking a Long Term View (April 2004)requires the NHS to improve health and well-being to tackle a range of health problems suchas obesity to reduce the burden on the healthservice. Achieving the fully engagedscenario would release £31 billion by 2022.To achieve this, the NHS and partners mustaddress the wider determinants of health,which are a range of factors that influence themental and physical health of an individual,including the parts that make up the builtenvironment, as illustrated in Figure 1.1.
Genera
l socio-economic, cultural and environmental conditions
Living and workingconditions
Workenvironment
EducationWater and sanitation
Agriculture and food production
Health-care
services
Unemployment
Social and community networks
Individual lifestyle factors
Age, sex and hereditary factors
Source: Dahlgren (1995)
Figure 1.1 – The wider determinants of health
1. Based on GLA population projection 8.1 from 2006(7.572 million people) to 2021 (8.467 million people)

Health and Urban Planning Toolkit Phase 1: Background to engagement
10
Choosing Health: making healthy choices easier(November 2004) highlights action to tackleinequalities that involves helping people to lead healthier lifestyles. Addressing the widerdeterminants of health underpins this. Itrecognises that joint working with partners likeLocal Planning Authorities is required as mostdeterminants lie outside of the control of the NHS.
Our Health Our Care Our Say (January 2006)emphasised the need to address the widerdeterminants of health and realign theemphasis of health care from hospitals to morecommunity based settings such as GPs. Thisapproach demands more attention to thequality of the built environment and the way itis planned and where health services arelocated. It went on further to specify that PCTswill need to work with Local PlanningAuthorities to address the impacts of newhousing on health services through the planningsystem. It states:
‘New housing developments have an impact onprimary care and community services forexample, immediate increases in demand for GPservices. The Government will explore ways inwhich local planning authorities and localproviders of health services can work togetherbetter, to ensure that the impacts of newdevelopments on existing services are properlyaddressed through the planning system. TheNHS locally is encouraged to work closely withplanning authorities’.
Planning
The spatial planning system introduced by thePlanning and Compulsory Purchase Act 2004broadened the scope of urban planningsignificantly to better enable it to createsustainable communities. This was done byrequiring the Development Plan, which for eachLondon Borough or Local Planning Authority inLondon consists of the London Plan and theirLocal Development Framework, to look beyondtraditional land use considerations and take intoaccount all factors like health that make up asustainable community.
The content of a Local Development Frameworkis set out in Planning Policy Statement 12: LocalDevelopment Frameworks (2004). It should actas the spatial expression of the local CommunityStrategy, and contain ‘an integrated set ofpolicies based on a clear understanding of theeconomic, social and environmental needs ofthe area and any constraints on meeting thoseneeds’, underpinned by a ‘comprehensive andcredible evidence base’. To ensure this, LocalPlanning Authorities should ‘take account of theprinciples and characteristics of other relevantstrategies and programmes’ when preparing it,including ‘strategies for education, health, socialinclusion, waste, biodiversity, recycling andenvironmental protection’, and ‘should consultclosely with the bodies responsible for thosestrategies to ensure effective integration whilstaddressing short, medium and long termpriorities’. It is also subject to stringent tests ofsustainability and soundness to ensure it meetsthese requirements. This means that the LocalDevelopment Framework needs to addressaspirations for health set out in the localCommunity Strategy that have spatialimplications and that Local Planning Authoritiesneed to work with PCTs to source the healthevidence base and take their strategies andprogrammes into account.
Development Plans are subject to StrategicEnvironmental Assessment/SustainabilityAppraisal. The guidance makes it clear thathealth must be thoroughly considered as part ofthe Appraisal. Therefore, the Local PlanningAuthority needs to understand and takeaccount of health if it is to satisfy the Appraisaland produce a sound Development Plan.
Circular 5/2005 (ODPM – July 2005) providesclear justification for planning obligations (alsoknown as section 106 agreements, or simply as
Barking Riverside

s106) to be sought to address the impacts ofdevelopment on health services. It supports‘pump-priming’ revenue contributions wherethere is a ‘time lag between the provision of thenew facility and its inclusion in public sectorfunding streams’. It emphasises meaningfulinvolvement of those with an interest, and an‘integrated approach to the need forinfrastructure created by a number ofdevelopments’. It encourages the use offormulae as part of negotiation. Soundevidence will be required to justify a planningcontribution. This means that Local PlanningAuthorities will need to take impacts on healthservices into account when negotiatingplanning contributions, and will need to involvePCTs in a meaningful way when doing this.
The role of PCTs
PCTs are the statutory authorities responsible forimproving health and well-being and meetinghealth care needs in their area. The three mainfunctions of a PCT are:
• Engaging with its local population to improvehealth and well-being
• Commissioning a comprehensive andequitable range of high quality, responsiveand efficient health services, within allocatedresources, across all service sectors
Health and Urban Planning Toolkit Phase 1: Background to engagement
2. DoH 2006
• Directly providing high quality responsive andefficient health services where this gives best-value2
More detail on the role and structure of PCTs isincluded in Appendix 1.
To help improve health and well-being andachieve other PCT targets, the widerdeterminants of health must be taken intoaccount when shaping the built environment.New development must provide for a quality oflife that facilitates healthier lifestyles andmitigates local and wider impacts on health. To meet increased demand for health servicesdriven by population growth, and minimiseimpacts on the ability to provide services to theexisting population, new development mayneed to make provision for health facilities, orprovide financial support to help fund services.To secure this, the PCT will need to influencethe planning system which manages growthand shapes the built environment.
To make progress PCTs must reach out beyondtraditional clinical concerns, as it already does inother matters, and take spatial implications ofhealth into account. Engaging with the LocalPlanning Authority is a vital aspect of thisapproach but in the past many PCTs have failedto engage consistently and effectively.
11
The Pavilion, Stonebridge Estate

Health and Urban Planning Toolkit Phase 1: Background to engagement
12
The role of Local Planning Authorities
Local Planning Authorities are statutoryauthorities responsible for preparing the LocalDevelopment Framework, for developmentcontrol in their area, and for managing theparticipation of stakeholders including PCTswhere required. They are also responsible forreflecting the vision set out in the localCommunity Strategy in the Local DevelopmentFramework and for achieving sustainabledevelopment. All London Boroughs are theLocal Planning Authority for their area. Teamsare normally set up for each of the planningfunctions – for example ‘Planning Policy’ will beresponsible for preparing the LocalDevelopment Framework and ‘DevelopmentControl’ will be responsible for managing theplanning application process. Appendix 1provides more detail on the role and structureof Local Planning Authorities.
Good quality health and health services are afundamental prerequisite of a sustainablecommunity. Local Planning Authorities need toengage with PCTs to fulfil their participationobligations, to develop their evidence base andto produce truly sound spatial developmentframeworks that are based on realistic androbust delivery expectations.
Complementary health and urban planning interests
PCT’s and Local Planning Authority’s interestsare thus complementary, and are best pursuedthrough joint working because:
• the PCT cannot influence the planning systemwithout the full support of the Local PlanningAuthority
• the Local Planning Authority is unable to takehealth and health services into account unlessthe PCT has the capacity and is committed toengage
To do this, PCTs and Local Planning Authoritiesmust be able to understand and relate to eachother and to work together in an integratedway at strategic, delivery and organisationallevels.
To prepare the Local Development Framework,the Local Planning Authority relies on the PCTto help gather evidence. The PCT must also beable to inform development control and provideinput on planning applications and follow anagreed approach to planning obligations. Timelyinput is essential, putting an emphasis on PCTsto be proactive rather than reactive toproposals.
Queens Market, Newham

The PCT relies on the support of the LocalPlanning Authority to ensure the LocalDevelopment Framework addresses health andhealth services, underpins planningcontributions and supports delivery of healthoutcomes. The Local Planning Authority alsoneeds to ensure PCT input on developmentproposals is taken into account, and requestsfor planning obligations are supported.
To meet these expectations, PCTs will need todevelop an open and outward looking approachand the means to do the work required. PCTsshould see this as a matter of good governanceand a way of helping to meet their Fitness forPurpose criteria. Local Planning Authorities willneed to be more prepared to integrate healthoutcomes in their approach to strategydevelopment and service delivery. A key prioritytask for both will be to define this commonagenda in a locally relevant way.
Barriers will need to be overcome first!
There are a range of barriers that makeengagement and collaboration difficult:
• There may not be any history of engagementbetween the PCT and Local PlanningAuthority
• A lack of mutual understanding andawareness of structure and function betweenPCTs and Local Planning Authorities
• Staff in both organisations are often not surewho they should talk to
• PCTs and Local Planning Authorities aresubject to different timescales makingstrategic planning difficult
• PCTs may not have the capacity to engage orthe strategies that set out information theplanning system requires
• The focus of PCTs may be on financial andclinical objectives
• Local Planning Authorities may not yet seehealth as an objective in the LocalDevelopment Framework
These barriers, if they exist, will be identified inthe Alignment Checklist in Step 4.
What are the outcomes for myorganisation?
For PCTs, joint working will help to influencethe wider determinants of health, and henceachieve the aims of improving health and well-being and meeting health care need in theirarea. In the short term, PCTs should receivefinancial contributions through section 106agreements to help deliver health services. Overthe longer term, the cost of delivering healthservices should reduce as a healthier communitywill have less need for them.
For Local Planning Authorities, engagementwill fulfil key statutory obligations linked toimproving the condition of the community,participatory inclusion of local stakeholders,sustainability (as well as obligations of theBorough generally) and preparing a soundDevelopment Plan.
Health will once again be an embedded part ofthe planning system, enhancing the ability todeliver sustainable development. PCTs and LocalPlanning Authorities will be better able tomonitor health outcomes, gather a more robustevidence base, and be more responsive inaddressing local health issues. This will make amajor contribution to achieving the localCommunity Strategy.
The cost of engagement may not be as high asimagined. Engagement, as proposed in thisToolkit, will come at a limited cost to PCTs as itshould reduce the long term burden of ill healthand secure additional funding. It will help theLocal Planning Authority to streamline theirprocesses and improve delivery. Table 1.1summarises the benefits over time.
Health and Urban Planning Toolkit Phase 1: Background to engagement
13
Kaleidoscope, Lewisham Centre forChildren and Young People

14
Health and Urban Planning Toolkit Phase 1: Background to engagement
Table 1.1 – The benefits of engagement for PCTs and Local Planning Authorities over time.
PCT
Short Term
• Financial contribution to new facilities and services
• Reduced risk of wasted investment• Meeting Fitness for Purpose and
Annual Health Check tests• Faster planning permission for new
facilities• Staff development
Local Planning Authority
Short Term
• Stronger link to local CommunityStrategy through PCT
• Stronger evidence base for LocalDevelopment Framework
• More efficient and effectiveconsultation process
• Faster planning decision process• Contribution to the Sustainability
Appraisal / Strategic EnvironmentalAssessment process
• Staff development
Medium Term
• Reconfiguration process supported• More cost effective service delivery• Stronger community acceptance of
change• Efficient redevelopment/re-use of NHS
estate• Improved medium term planning
Medium Term
• Soundness test of Local DevelopmentFramework supported
• Contribution to meeting Well-beingpower
• Stronger links with Local StrategicPartnership
• Implementation of Local DevelopmentFramework supported
• Delivery targets met• Partnership working strengthened
Long Term
• Reduction in health inequalities• Improved community health and well-
being• Increased levels of physical activity• Modernised accessible health services• Robust long term planning process
Long Term
• Progress towards more sustainablecommunities
• Meeting planning targets• Effective delivery of the Local
Development Framework
WHAT TO DO NEXT…
Examine whether your PCT or Local Planning Authority are missing out on the benefits of engagement,as discussed above. The following are indicators of failure:
For PCTs:
New development is not facilitating healthierlifestyles or supporting PCT health improvementprogrammes and initiativesMore progress can be made on tackling healthinequalitiesFinancial support has not been secured throughplanning obligations to help make the delivery ofhealth services more affordable
For Local Planning Authorities:
Health input is not readily forthcomingIt is difficult to take health and health services intoaccount and meet planning delivery targetsThere is a risk to the soundness of the LocalDevelopment FrameworkIt is uncertain whether health services can meetincreased demand from population growth
Step 2 provides further information on what must be put in place to facilitate engagement.

15
Health and Urban Planning Toolkit Phase 1: Background to engagement
Step 2 Understanding the principles of organisational collaboration between the PCT and Local Planning Authority.
Culture CultureStrategy
Organisation Organisation
Systems Systems
Strategy
Structure Structure
PCT Local Planning Authority
Enga
gem
ent
Agr
eem
ent
To be able to pursue their interests PCTs andLocal Planning Authorities need to be able towork together at strategic, delivery andorganisational levels. Given the mutual supportrequired to do this, key areas of each
organisation must be aligned in acomplementary way. Figure 2.1 illustrates wherealignment between a PCT and Local PlanningAuthority must occur, and is explained below.
Figure 2.1 – Alignment between a PCT and Local Planning Authority
Strategy
Strategic alignment should be considered apriority by PCTs and Local Planning Authoritiesgiven the central role of strategies in guidingtheir actions. To help a PCT and Local PlanningAuthority achieve strategic alignment, the PCTneeds to have strategies that set out how thewider determinants of health and healthservices should be addressed through theplanning system. It may be possible for PCTs toupdate existing strategies like their StrategicService Development Plans or Annual PublicHealth Reports to do this, or develop newstrategies that include spatial and planningimplications as part of their scope. Either way,they will need to contain an adequate evidencebase, reflect a timeframe agreed with the LocalPlanning Authority, and feature a spatialframework that can be integrated with the
Local Development Framework. Those strategiesmust reflect the overarching local CommunityStrategy and then be embedded in the LocalDevelopment Framework. With thisarrangement in place, health outcomes can bedelivered through development control and theplanning application process.
To further joint working, the PCT and LocalPlanning Authority (and other relevant partners)could pursue a joint strategy that addresses thespatial implications of health and providinghealth services. The joint strategy may bedesigned to address wider initiatives as well asthe planning system.
The Alignment Checklist in Step 4 will help teststrategic alignment between the PCT and LocalPlanning Authority and Step 7 provides moredetail on achieving strategic alignment.

16
Health and Urban Planning Toolkit Phase 1: Background to engagement
Systems
PCTs and Local Planning Authorities must alignsystems to enable timely and effectivecommunication between staff. Given most PCTsare unprepared for joint working it is likely theywill need to develop internal systems forhandling planning matters. Local PlanningAuthorities will need to ensure thatengagement is embedded in their existingsystems and is responsive to PCT input, and thatinput is facilitated appropriately. This includescascading input vertically and horizontallywithin the Local Planning Authority i.e. withinand between corporate directorates. Outcomessuch as improved health and behaviouralchange should also be monitored and recorded.Importantly, expectations and how therespective systems should tie in together shouldbe set out in a simple agreement, as identifiedin Figure 2.1.
The Alignment Checklist will help test systemsalignment between the PCT and Local PlanningAuthority, Step 6 sets out how to prepare anengagement agreement and Steps 7, 8 and 9provide more detail on aligning systems.
Structure
PCTs and Local Planning Authorities must securethe commitment of staff at the highest level.Governing boards of PCTs will have a role toplay in setting a clear priority for thiscollaboration and monitoring process. Thepolitical dimension is also important given therole of elected members, especially in decisionmaking, and there may be a need to involvethem in some way.
Having the right staff in place to do theengagement work and ensure communication isoccurring at the correct levels will be essential.An organisational mapping exercise, explainedfurther in Step 3 will help.
PCTs will need to identify someone at a seniorlevel to provide leadership on an ongoing basis.A cross-directorate team that draws in theexpertise of staff from across the organisationwill need ideally to be set up and coordinatedby someone with an understanding of theplanning system. PCTs will find that staff arealready doing many of the tasks set out in theToolkit, but may be ill coordinated – drawingthem together to work as a team will improvetheir effectiveness. Local Planning Authoritieswill need to allocate responsibility forengagement tasks and provide training whererequired.
Craven Park Health Centre, Stonebridge Estate

The Alignment Checklist in Step 4 will help teststructural alignment between the PCT and LocalPlanning Authority and Step 9 provides moredetail on achieving structural alignment.
Culture
Organisational culture may present a barrier toeffective engagement despite the best ofintentions and good ‘theoretical’ alignment,particularly where PCTs and Local PlanningAuthorities do not have a history ofengagement. The culture of both organisations
Health and Urban Planning Toolkit Phase 1: Background to engagement
17
needs to be outward looking, inclusive and toembrace joint working. This kind of ethosshould ideally be driven from the top of theorganisation and be supported by businessplans, targets, indicators and personaldevelopment plans.
Local Planning Authorities may wish to seekpolitical support for the approaches that are setout in this Toolkit to ensure the process andoutcomes of engagement can be delivered.
WHAT TO DO NEXT…
Consider what working differently to facilitate engagement may involve:
For the PCT:
Could spatial implications of health be taken intoaccount when reviewing strategies such as theStrategic Service Development Plan or preparingthe Annual Public Health Report or ChoosingHealth implementation plan?Are there any forums already set up where thehealth implications of development could bediscussed?Could staff already involved in dealing with healthservice capacity issues help to inform the planningsystem, for example, where a developmentproposal may lead to population growth andincreased registrations with local GPs as a result?Are staff, for instance in public health or estates,already dealing with planning applications orhealth infrastructure proposals but in an illcoordinated way?
A preliminary meeting between the PCT and Local Planning Authority is a good way to begin discussion on engagementbut a corporate decision is needed to deliver effective joint working. The organisational mapping exercise in Step 3 will helpidentify who from the PCT and Local Planning Authority should attend initial meetings.
For the Local Planning Authority:
Have any staff been given the responsibility forliaising with the local PCT?Do staff have the skills to assess the healthimplications of a development proposal?Are planning applications being referred to thePCT during consultation?

18Greenwich Millennium Village

Phase 2: Defining the relationship
Phase 2: Defining the relationship
Phase
The second phase is about the PCT and Local Planning Authority identifying their interests and working out how they will work together to address them, and involves the four stepsillustrated below.
Steps
3. Identify key communication links between the PCT and Local Planning Authority.
4. Use the Alignment Checklist to test the relationship between the PCT and Local Planning Authority.
5. Identify the local issues and priorities that the PCT and Local Planning Authority will need to address.
6. Prepare a simple engagement agreement between the PCT and Local Planning Authority to set out expectations.
19
Key messages of this section
• PCTs and Local Planning Authorities will need to work together to identifyweaknesses in their alignment and agree how to address them. The AlignmentChecklist included provides a structured way to do this.
• A simple agreement will help manage engagement.

Health and Urban Planning Toolkit Phase 2: Defining the relationship
20

21
Health and Urban Planning Toolkit Phase 2: Defining the relationship
Step 3 Identify key communication links between the PCT and Local Planning Authority.
Once a PCT or Local Planning Authority hasagreed to engage either can make the firstapproach to initiate discussions. It is suggestedthat a preliminary meeting be held to discussengagement, and should be attended by staffat the highest level to show credibility andcommitment. An organisational mappingexercise, as discussed below, will help identifywho should be involved in the meeting. Theagenda for the meeting might include thefollowing items:
• By hand, complete the Alignment Checklist in Step 4
• Identify local issues that impinge health andplanning e.g. housing proposals, regenerationareas, rapid development and policies andstrategies, and priorities to address them, asdiscussed in Step 5
• Provide a record of major development in therecent past
• Discuss instances where health has factored in the planning process and any success or failure
• Compare structures and processes (refer tothe organisational mapping exercise below)
• Agree objectives, including a deadline for thepreparation of the engagement agreementdiscussed in Step 6
Appendix 1 provides a description of a PCT andLocal Planning Authority to help you with theorganisational mapping exercise and theAlignment Checklist in Step 4.
Mapping organisational structures
Figure 3.1 provides an example of anorganisational mapping exercise, which can beundertaken as follows:
1. Map out the structure of the Local PlanningAuthority, including the relevant urbanplanning functions and key contacts. Alsomap out the structure of the PCT, includingany roles and key contacts that may beassociated with the planning system. Keycontacts for both organisations shouldinclude high level staff at director or chiefofficer level.
2. Place the maps side by side and mark in anyexisting links, as illustrated in Figure 3.1.Represent the quality of those links wherepossible.
3. Identify where new links are likely to beneeded and where existing links should bestrengthened.
4. The relationship to the Local StrategicPartnership should also be taken into accountgiven its ‘overarching’ strategic role.
5. The map should then be used to identifywho may need to be involved in futurediscussions between the PCT and LocalPlanning Authority.

Health and Urban Planning Toolkit Phase 2: Defining the relationship
22
Figure 3.1 – An example of an organisational mapping exercise
WHAT TO DO NEXT…
Once the exercise has been completed, bringtogether those identified from the PCT and theLocal Planning Authority for the preliminarymeeting.
Key tasks for the meeting include completing theAlignment Checklist included in Step 4, identifyingkey issues and priorities as discussed in Step 5, andpreparing the engagement agreement discussed inStep 6.
At a later stage, when engagement responsibilitieshave been agreed, update the map if necessary anddistribute it to those involved. Appended a copy tothe engagement agreement discussed in Step 6,and update it when necessary.
Local Strategic Partnership
PCT Board
PCT Local Planning Authority
Chief Executive Chief Executive
Council and Committees
Finance Public HealthPrimary Care Estates Directorate e.g. Environment
Public Health Specialist Planning Policy
Development Control
Urban Regeneration
Estates Manager
Weak existing link that needs improvement
Strong existing link
New link required
Directorate e.g. Transport

Once staff from the PCT and Local PlanningAuthority are together they need to assesswhether or to what extent their relationshipmeets the alignment model set out in Step 2.The Alignment Checklist included here has beendeveloped to help do this, and can be used to
23
identify weaknesses in alignment and informthe way forward to address them. It will alsohelp familiarise staff with the otherorganisation, before moving on to identify localissues and priorities discussed in Step 5.
Health and Urban Planning Toolkit Phase 2: Defining the relationship
Step 4 Use the Alignment Checklist to test the relationship between a PCT and Local Planning Authority.
Kaleidoscope, Lewisham Centre for Children and Young People

24
• Use the checklist to test the relationship ofthe PCT and Local Planning Authority and topinpoint where action will be required toimprove alignment.
• Start by answering the questions in the lefthand column. Questions answered with a‘no’ identify a weakness. The right handcolumn provides advice or direction onwhere to go in the Toolkit to addressweaknesses.
The Alignment Checklist
• If you wish, the checklist allows you to scoreyour assessment. The questions areweighted depending on their priority toalignment, so the higher the score thebetter your level of engagement. Guidanceon how to interpret you score is included atthe end of the checklist.
PCT/ LPA
PCT
PCT
PCT
PCT
PCT
Both
LPA
LPA
LPA
Yes/No orDon’t know
Points
3
3
3
3
3
3
3
3
3
If no, the followingaction is required.
Refer to Step 7.
Refer to Step 7.
Refer to Step 7.
Refer to Step 7.
Refer to Step 7.
Refer to Step 7.
Refer to Step 7.
Refer to Step 7.
Refer to Step 7.
1
2
3
4
5
6
7
8
9
Strategy
Is this done at the moment?
Does the PCT have strategies that set out its vision and plans ofaction to address the wider determinants of health and healthservices?
Has the PCT ensured that its vision reflects the local CommunityStrategy?
Is the health strategy based on up to date evidence, a clearbaseline and analysis of the pattern and intensity of ill-healthrelated to social, environmental and economic conditions?
Is the strategy expressed in a spatial form which reflectsprojected changes in the characteristics and geographicalpattern of population change and identifies the patterns ofhealth conditions?
Is the health services strategy expressed in a spatial form thatidentifies the distribution of existing capacity of facilities andservices, and location of proposed new investments?
Do the PCT and Local Planning Authority have any jointstrategies for health improvement or service delivery?
Does the Local Development Framework reflect the healthaspirations set out in the local Community Strategy and containan adequate evidence base?
Does the Local Development Framework contain policies that setout how new development should facilitate healthimprovement?
Has the Local Development Framework process so far taken intoaccount the strategies and programmes of the PCT?

Health and Urban Planning Toolkit Phase 2: Defining the relationship
25
PCT/ LPA
PCT
PCT
PCT
PCT
PCT
Both
PCT
Both
Both
Both
LPA
PCT
Yes/No orDon’t know
Points
3
3
3
2
2
3
2
3
2
2
2
1
If no, the followingaction is required.
Refer to Step 7.
Refer to Steps 7 and 9.
Refer to Step 7.
Refer to Step 8.
Physical urban regenerationproposals can require significantinput from a PCT over a longperiod of time. The PCT mustensure it can maintain timely,adequate and effective input.Refer to Step 5 for moreinformation.
Refer to Step 6.
Refer to Step 7.
Refer to Step 7.
Refer to Steps 6 and 9.
The PCT and Local PlanningAuthority should set up regularmeetings, or use existingmeetings if possible, to do this.This should further assist withintegration of services in a localarea. Refer to Step 8 for moreinformation.
Refer to Step 8.
Refer to Steps 5 and 7.
10
11
12
13
14
15
16
17
Systems
Is this done at the moment?
Does the PCT have the following work streams or processes thatsupport engagement?
10.1 Prepare and update the strategies described above;
10.2 Monitor the Local Development Scheme anddevelopment proposals to identify when input isrequired;
10.3 Provide input to local Community Strategies and LocalDevelopment Framework preparation to ensure healthand health services are taken into account;
10.4 Provide informal and formal input to developmentproposals at pre-application and application stages toensure health and health services are taken into account;
10.5 Contribute to long-term physical urban regenerationproposals, such as estate renewals, town centreregeneration and large scale transport infrastructureprovision to ensure health and health services are takeninto account?
Have the PCT and Local Planning Authority agreed on how theywill engage and collaborate?
Does the PCT have the ability to prepare mapping to illustratethe spatial implications of health and health services?
Is key local information or data, such as proposed developmentgrowth areas, population projections or local health issues,exchanged and / or agreed regularly between the PCT and LocalPlanning Authority to assist with strategic planning?
Is information cascaded effectively within each organisation sothat relevant staff are aware of health and urban planningmatters?
Is there a forum where the PCT, Local Planning Authority and other relevant partners such as Education and SocialServices can discuss shared interests?
Are there opportunities for the PCT to discuss the delivery ofhealth services and planning obligations?
Does the PCT coordinate input on urban planning matters forother local NHS Trusts?

Health and Urban Planning Toolkit Phase 2: Defining the relationship
26
PCT/ LPA
Both
Both
PCT
PCT
PCT
Both
PCT
Both
PCT
PCT
PCT
Yes/No orDon’t know
Points
2
1
2
3
3
2
1
3
3
3
2
If no, the followingaction is required.
Where facilities are requiredLIFT should be involved at theearliest stage and highlighted as a potential developmentpartner. Refer to Step 7 to findout what can be done toinvolve LIFT.
Refer to Step 5.
A robust records system should be established. Refer to Step 8.
To work out the scale ofcontributions, estimate theamount of development thatwill be occurring in theBorough and use the HUDUs106 Model to produce afinancial estimate. This estimatecan then be compared againstthe ability for the PCT to meetrequirements with its ownresources.
Refer to Step 8.
Refer to Steps 7 and 8.
Refer to Steps 7 and 8.
Refer to Step 3.
Refer to Step 9.
Refer to Step 9.
Refer to Step 9.
18
19
20
21
22
23
24
25
26
Systems continued
Is this done at the moment?
Is LIFT regularly involved in discussion with the Local PlanningAuthority on planning issues?
Is the PCT involved in area based partnership groups with healthand urban planning implications to help it stay in touch withlocalised initiatives?
Does the PCT have a sound way of storing records on proposalsit has dealt with?
Has the Director of Finance identified and PCT Board consideredthe scale of financial contributions that might be securedthrough the planning system, and if so, has it set targets tosecure them?
Does the PCT have a system for allocating finance securedthrough planning obligations, and for monitoring and reportingtheir delivery to the Local Planning Authority?
Does the PCT and Local Planning Authority use tools, like WatchOut for Health and the HUDU s106 Model to assess plans anddevelopment proposals?
Does the PCT engage with wider partners including the Mayorof London, GLA, LDA and GOL on major development orregeneration proposals?
Structure
Have organisational structures been mapped to see whereengagement needs to occur?
Has the PCT identified the following roles?
26.1 High level ‘champion’ for engagement.
26.2 Urban Planning Lead.
26.3 Urban Planning Coordinator.

Health and Urban Planning Toolkit Phase 2: Defining the relationship
27
PCT/ LPA
PCT
PCT
PCT
PCT
PCT
PCT
LPA
LPA
Both
Yes/No orDon’t know
Points
2
2
2
2
2
2
2
2
1
If no, the followingaction is required.
Note: Existing PCT staff shouldbe able to do these tasks,however it may be necessary toprovide additional training.
Refer to Steps 8 and 9.
Refer to Steps 8 and 9.
Refer to Steps 8 and 9.
Refer to Steps 8 and 9.
Refer to Steps 8 and 9.
Refer to Step 9.
Refer to Step 9.
Refer to Step 9.
Refer to Step 9.
27
28
29
30
31
Structure continued
Is this done at the moment?
Are the following tasks carried out as part of somebody’s job atthe PCT?
27.1 Assessment of plans and development proposals toidentify any wider health implications.
27.2 Assessment of plans and development proposals toidentify whether they will increase the need for healthcare.
27.3 Assess whether any new health services and facilities ormodifications to existing ones are required in response toa plan or development proposal, to meet any increasethe need for health care or accord with health careservice models.
27.4 Apply the HUDU s106 Model.
27.5 Monitor planning obligations and report on their deliveryto the PCT and Local Planning Authority.
Do staff with a range of skills and knowledge from across thePCT (as described above) work together in a coordinated way toengage and collaborate with the Local Planning Authority?
Does the Local Planning Authority have allocated leads forhealth and engagement with the PCT, who can help itunderstand planning proposals?
Does the Local Planning Authority have a good understandingof the health implications of urban planning?
Are there any jointly appointed ‘health and urban planning’staff?
How did you score?
The maximum score is 97.
A High Score – 54 points or better
If you have achieved a high score, your PCT probably has agood level of alignment, but there may still be some gaps thatneed to be addressed. Please get in touch with HUDU – we’rekeen to know what you’ve done, and to help address anyoutstanding gaps.
A Lower Score – 53 points or less
If you have achieved a low score there may be fundamentalweaknesses in alignment and the PCT and Local PlanningAuthority are missing out on significant benefits ofengagement. Urgent action will be required to address theweaknesses if benefits are to be secured. HUDU is availableto help your PCT and Local Planning Authority addressthese issues.

Health and Urban Planning Toolkit Phase 2: Defining the relationship
28
WHAT TO DO NEXT…
Use the advice in the right hand column of theAlignment Checklist to find advice or direction onwhere to go in the Toolkit to develop a plan ofaction to address any weaknesses. Concentrationshould be given first to the weaknesses with thehighest priority.
We suggest that you carry out the scoring on a periodicbasis in order to assess how engagement is going.
Identify local issues and priorities to help direct actions,as discussed in Step 5.
Kaleidoscope, Lewisham Centre for Children and Young People

Developing a mutual understanding of keyissues and priorities will help the PCT and LocalPlanning Authority gain maximum benefit fromthe engagement process.
The PCT will need to set out the local healthissues that need to be tackled through theplanning system. The Local Planning Authoritywill need to give an idea of the input requiredfrom the PCT on various matters over the short,medium and long term. This will help the PCTand Local Planning Authority to programmework appropriately.
At the end of this process, the PCT and LocalPlanning Authority should be clear about:• their key issues and priorities;• the avenues in which they should be pursued;• key projects that that need to be worked on
together;• other stakeholders that need to be involved;
and• an action plan.
Health issues and priorities
Wider determinants of health
A starting point will be the PCTs work on publichealth in the Borough – the Annual PublicHealth Report would act as a useful guide. Thiscould be supported for instance by using therange of data provided by the London HealthObservatory. The outcome should be a cleardescription of the trends and key healthindicators. This analysis of health conditionscould be set in the context of population,environmental and transport data analysed andprovided by the Local Planning Authority. In thisway the relationships between the community,environmental conditions in the widest senseand health outcomes can be mapped andwhere possible pathways identified.
29
Key issues and priorities may be:
• Population characteristics and projectedchanges such as growing proportions ofelderly, ethnic groups or young people
• Relative mortality rates between the Boroughand other places and within the Borough
• High relative incidence of certain diseases andpublic health conditions e.g. coronary heartdisease, obesity, metal health problems andthe pattern across the Borough
• Patterns of road casualties by age and class• Incidence of air pollution• Poor access to quality fresh food• Poor public transport accessibility• Poor access to open space and play space
All of these factors are relevant in devisingpolicies that will improve health conditions andreduce inequalities in health by addressing thewider determinants of health.
Health services
5A description of the state of the local healthestate is important, together with capacityissues and any service model implications.
Key issues and priorities may be:
• Facilities not suitable to upgrade or expand• Areas where accessibility to or availability of
health services is inadequate• The extent and location of population growth
and change from new development thatcould come forward in the short, medium andlong term
• Hot spots where the health service is at orclose to capacity and immediate action isrequired
• Locations where new facilities may berequired given the service model
• Funding implications of providing healthservices
• Need to involve other NHS trusts• Proposals where immediate support from
planning contributions is required• Closure or relocation of hospitals
Health and Urban Planning Toolkit Phase 2: Defining the relationship
Step 5 Identify the local issues and priorities that a PCT and Local Planning Authority will need to address.

Health and Urban Planning Toolkit Phase 2: Defining the relationship
30
These factors will help identify where pressuresfrom development will be felt and the extent towhich the health services needs to besupported, and also signpost the Local PlanningAuthority to other health stakeholders like NHShospital or mental health trusts where required.It will be helpful to support this with mapsshowing potential development sites and thehealth estate for example, preferably preparedusing GIS compatible with the Local PlanningAuthority. If known, unit number, type,projected population number and anticipateddemographic profile of new development wouldalso be helpful to identify potential healthissues.
Local Planning Authority issues andpriorities
Local Development Framework
The Local Planning Authority will be keen toproduce a sound Local Development Frameworkthat delivers the local Community Strategy, andwill rely on input from the PCT to achieve this.
Key issues and priorities may be:
• Define the health aspirations of the localCommunity Strategy in spatial terms
• Scope out the health evidence base for theLocal Development Framework
• Formulate policies that are properly directedat health and health services
• Define targets and indicators for health• Ensure new development has the social
infrastructure, including health services,needed
• The use of tools or formulae to assess healthimpacts
• Meeting deadlines for the production of theLocal Development Framework
The Local Planning Authority will need inputfrom the PCT as early as possible in line withthe emphasis on ‘front loading’ of the LocalDevelopment Framework preparation process toensure health is properly reflected and to help itmeet production deadlines. Agreeing the natureand timing of PCT input will be critical to thishappening.
Development control
The Local Planning Authority may need to sourcea range of information from the PCT throughoutthe planning application process. Much of thisinput may involve providing further detail onhealth matters identified in the LocalDevelopment Framework.
Key issues and priorities may be:
• Guidance on intervention measures toimprove health
• The use of tools or formulae to assess healthimpacts
• Whether new development will impact onhealth services
• Where planning obligations need to bedirected to address impacts
• The scale of planning obligations required toaddress impacts on health services
• Meeting deadlines for determining planningapplications
Regeneration proposals
The Local Planning Authority may not alwayslead on urban regeneration, however it will stillplay a key part in many aspects of the process.Given the scale of many physical regenerationproposals, the extended process, thecharacteristics of the communities ofteninvolved and the potential health implications,the PCT will be relied on to provide input on arange of matters throughout the process.
Key issues and priorities may be:
• Gather detailed evidence base to undertake ahealth needs assessment
• Identify an appropriate health service modelgiven the layout of the proposal and itsrelationship to other local health services
• Contribute to planning guidance likeSupplementary Planning Documents thatinform the regeneration proposal
• Participate in master planning, especiallywhere interventions are required to addresslocal health issues or support initiatives orprogrammes

It will be important to include the PCT as partof the project management team or steeringgroup, and is given a good idea of the likelynature and timing of its input so it can plan itsinvolvement. There may also be opportunitiesfor PCTs to be involved in groups orpartnerships set up for different areas in theBorough, which often have a regenerationfocus.
31
• Resolve operational matters like transitionalarrangements for health services duringdemolition or occupant relocation
• Discuss planning obligations to help addressany impacts on health services or delivermodern facilities
• Discuss co-location or integration with otherpublic service providers
Health and Urban Planning Toolkit Phase 2: Defining the relationship
WHAT TO DO NEXT…
Prepare a list of key issues and priorities and identifythe involvement required, including:
- objectives;- action points;-deadline for the preparation of an engagementagreement; and
- the key contacts involved.
At the end of this process, the PCT and LocalPlanning Authority should be ready come to anagreement on how to work together, as set out inStep 6.
Greenwich Millennium Village

32Regeneration of Stonebridge Estate

33
Step 6
Health and Urban Planning Toolkit Phase 2: Defining the relationship
Prepare a simple engagement agreement between the PCT and Local Planning Authorityto set out expectations.
• identify any key objectives to be achievedthrough the agreement;
• state the principles that underpin theagreement;
• specify the issues and priorities and areas ofwork such as the categories of planningapplications that the agreement is intended tocover;
• set out the responsibilities of the LocalPlanning Authority and any specific actions itneeds to undertake during the term of theagreement, as well as any key contacts;
• set out the responsibilities of the PCT and anyspecific actions it needs to undertake duringthe term of the agreement, as well as any keycontact details;
• identify how and when the agreement will bemonitored so it remains up to date; and
• be signed by high level representatives fromthe PCT and Local Planning Authority.
An engagement agreement template is includedin Appendix 2.
Once the PCT and Local Planning Authorityhave discussed what needs to be done to worktogether and identified the key issues andpriorities that need to be pursued throughengagement a simple formal agreement willhelp to set out how joint working will occur.The agreement should:
• set out the objectives and priorities ofengagement and collaboration;
• make clear obligations and expectations; and• provide commitment to joint working, and
underpin work to achieve alignment.
Without an agreement there is a high risk thatjoint working will fail due to conflictingpriorities or poor commitment, and a lot of timewill be wasted. The principle of entering into anengagement agreement is something thatshould be agreed at Director or Chief Officerlevel.
In terms of structure, the engagementagreement should:• state its purpose;• provide a brief background on why the
engagement agreement is needed;
WHAT TO DO NEXT…
Once signed, the agreement must be cascadedthroughout the PCT and Local Planning Authorityand responsibilities allocated as required, and keptalive and relevant to actual practice, so it is importantto monitor how it is working. A meeting should beheld once or twice a year to review the effectivenessof the agreement. This may also be used as anopportunity to review priorities for the period ahead.
Steps 7, 8 and 9 provide guidance on how the PCTand Local Planning Authority should work togetherto address the Local Development Framework, theplanning application process and build internalcapacity to do this work.

34Kaleidoscope, Lewisham Centre for Children and Young People

Phase 3: Making engagement work
Phase
The third phase involves doing the work required to bring about alignment to enable healthoutcomes to be delivered through the planning system, and involves the three steps illustrated below.
Steps
7. Ensure the Local Development Framework and health strategies are mutually aligned.
8. Ensure the Development Control process delivers health outcomes and involves the PCT.
9. Build the capacity of PCT and Local Planning Authority staff to engage.
Key messages of this section
• PCTs will need to ensure that their strategies for health and health services includethe plans and programmes it would want pursued through the planning system.They should be publicly consulted on before informing the Local DevelopmentFramework.
• Local Planning Authorities will need to ensure the Local Development Frameworkreflects the vision for health set out in the local Community Strategy and is based onsound evidence and addresses the wider determinants of health, including healthservices, and health inequalities.
• PCTs should set up internal processes that enable them to contribute to the LocalDevelopment Framework preparation process and new development proposals andrespond in a timely manner.
• PCTs should allocate engagement tasks to existing staff where possible, and changetheir job descriptions to ensure tasks are embedded. A PCT may consider appointinga Town Planner.
• Watch Out for Health is a tool that can be used to assess health implications ofpolicies and development proposals.
• The HUDU s106 Model can be used to help quantify impacts on the local healthservice from new development and estimate the cost of addressing those impacts.
35
Phase 3: Making engagement work

Health and Urban Planning Toolkit Phase 3: Making engagement work
36

The strategic framework
The overarching strategic framework for aBorough is the local Community Strategy. This isthe means by which community visions,objectives and priorities are identified andmonitored. The Local Development Frameworkis expected to be the spatial expression of thelocal Community Strategy. Health will inevitablyfigure in community aspirations and there maywell be health targets attached to theobjectives. The Local Development Framework isdesigned to facilitate the delivery of the plans ofstatutory bodies such as PCTs. PCTs will usuallybe actively involved in the Local StrategicPartnership and it follows that local healthstrategies must be consistent with the localCommunity Strategy.
Health Strategy
PCTs will be producing a range of healthstrategies including the Local Delivery Plan, aStrategic Services Development Plan as well asthe Annual Public Health Report (more detail onthese is provided in Appendix 1). Together thesewill show how the service is expected todevelop and change and in some cases describethe investment programme (through LIFT orotherwise). The PCT will also almost certainlyhave a record of all primary care facilities andmay know something about their condition.Information concerning hospital and mentalhealth trusts plans and facilities may not be soreadily available but should be reflected at least.
Planning Strategy
The context for planning strategy is provided bynational planning policy set out in planningpolicy statements and the spatial developmentstrategy for London, which is the London Plan.The London Plan comprises one part of thestatutory Development Plan. In striving forstrategic alignment at the Borough level thepolicies in the London Plan must be taken intoaccount.
Local Planning Authorities are producing LocalDevelopment Frameworks (described in moredetail below), which comprise the local part ofthe statutory Development Plan. These willrequire a sound evidence base which ought toinclude health conditions and will be subject toappraisal that must assess the likely effects onhealth. The policy framework is expected tohave wide scope encompassing health andother social infrastructure and facilitatingdelivery of a range of service strategies anddelivery plans. Key sites may be identified in theLocal Development Framework.
Delivery mechanisms
Health
Health developments are delivered through avariety of vehicles but LIFT plays a key role inprimary care facilities. Hospital and mentalhealth facilities may be delivered throughdifferent public/private partnerships.Modernisation of the health service will, in verysimple terms, result in more services beingdelivered closer to home, in primary caresettings or directly at home
A PCT’s funding for services is allocated onceresidents have registered with a GP in the area– hence the limited availability for ‘pump-priming’ funding. Funding for capital works alsotends to be a small portion of the overallfunding received. Allocations do attempt to pickup projected increases in population, but arebased on Office of National Statistics projectionswhich are conservative compared to the GLAprojections that take planned housing growthinto account. The allocations are alsodetermined on a three year rolling cycle basis,so there is usually a delay in updated populationprojections being taken into account in theallocation in any case. These factors contributeto a funding gap, particularly for capital works,making it difficult for PCTs to fund developmentof services, especially in areas experiencing rapidpopulation growth.
Health and Urban Planning Toolkit Phase 3: Making engagement work
37
Step 7 Ensure the Local Development Framework and health strategies are mutually aligned.

Health and Urban Planning Toolkit Phase 3: Making engagement work
38
Planning
The Local Development Framework will bedelivered through a multitude of means. Themost important route is through developmentcontrol and the planning application process.Virtually all public and private developmentrequires planning permission. Developmentcontrol is the process by which such proposalsare considered by the Local Planning Authority.In coming to a decision to refuse or to approvesubject to conditions and obligations an LocalPlanning Authority will first and foremost beguided by the Development Plan which sets the
performance criteria or standards fordevelopment and to a large extent determineswhat development gets built and where.
Aligning planning and health strategiesand processes
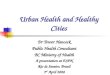
The key task at the core of this Toolkit is toensure that these planning and health strategiesand delivery mechanisms are aligned. Figure 7.1below attempts to illustrate and map thisalignment process. The elements of the diagramand process are described over page.
Local Community Strategy
Local Development
Framework
Planning Obligations
Health Outcomes
Planning Application Process
London Plan
Health and Wellbeing Strategy
Health Services and Facilities Strategy e.g. SSDP
Wider determinants
of health
Common Spatial Framework
Hospital
Proposed
Proposed
DoctorísSurgery
Existing
Healthier Built Environment
Health Facilities and Finance
Figure 7.1 – Aligning Strategies – producing a common spatial framework
For further detail on Common Spatial Framework and the Wider determinants see page 39.

Strategic framework
The elements of the strategic framework are: • The local Community Strategy which sets a
high level vision, aspirations, objectives andtargets
• The health strategy which sets out the way inwhich the service will develop and whatinvestment will be made where and when
• The Local Development Framework whichshows what type and scale of developmentwill be permitted and how it relates to thewhole range of infrastructure includinghealth. It will quantify the number ofdwellings expected to be built over perhaps a15 year period, identify the major transportimprovements, employment developments,town centres and social infrastructure.
There are two key areas where alignment iscritical for health:• Protecting and promoting health and well-
being• The rational planning of health services
Protecting and promoting health – securinghealth outcomes
The health of the community is affected by thewider determinants of health in a verysignificant way. The wider determinants includethe socio-economic and environmental contextin which communities find themselves. If theenvironment is poor and degraded, if jobs areunavailable and if communities are fractured
and individuals isolated, levels of physical andmental ill health will be very high. Spatial plansaddress many if not all of the widerdeterminants of health. It follows that if healthoutcomes are to be optimised the polices in thespatial plans must identify those factors causingor likely to cause ill health and seek to avoiddetrimental impacts and enhance positiveimpacts. It also follows that PCTs have a directand significant interest in ensuring that thosespatial planning polices are soundly based andthat wherever possible they reinforce the healthimprovement policies in their Local DeliveryPlans.
Planning health services and the commonspatial framework
The key to aligning health service planning andthe Local Development Framework is a commonspatial framework. What we mean by this issome kind of geographically based model ormap that enables the spatial and temporalrelationship between the demand for healthservices (i.e. the population and its characteristicand growth and locations) and the supply (thatis the scale, location and quality of healthfacilities) to be matched. This could be preparedusing Geographical Information Systems (GIS).The outcome of this matching process is that:• facilities are provided within the overall model
of care that are in the right place;• are accessible;• are available at the right time when new and
existing communities need them; and
Health and Urban Planning Toolkit Phase 3: Making engagement work
39
The Pavilion, Stonebridge Estate

Health and Urban Planning Toolkit Phase 3: Making engagement work
40
• are of the right quality and modernised toprovide the highest possible services to meetall community needs.
This is a tall order. This process of alignment isdifficult because the situation is fraught withuncertainty and subject to change. Neverthelessit is essential if major risks are to be avoided.Creating communities without health servicesand building health services in inaccessiblelocations has been a common failure in the past.
Ensuring effective delivery
The key aspects of delivery alignment are:• ensuring development contributes to health
and well-being;• ensuring investment plans in the health
service take account of development andpopulation growth; and
• ensuring that planning obligations securefinancial resources for the provision of healthfacilities to meet the needs of newpopulation.
The process of development control seeks toensure that development meets all thestandards set in the Local DevelopmentFramework. The impact of a development onthe wider determinants of health ought to bepositive and adverse health impacts avoided.Failure to secure these qualitative outcomesthrough development control means that thepolicies in the Development Plan, howeverrobust and soundly based, will be frustrated.
PCTs and Local Planning Authorities shouldtherefore develop effective links to enable PCTsto appraise developments that may have healthimplications from the earliest stage. This mayinvolve dealing with Environmental ImpactAssessment or may require a formal HealthImpact Assessment (see page 56 for moredetail). The engagement agreement should setout how this relationship will be handled.
Planning obligations for health services
In many parts of London increases in populationas a result of new housing will have a severeimpact on the ability of the PCT to deliverhealth services of the required standard. This islargely because most facilities are at or beyondcapacity. Planning policy guidance and theLondon Plan make it absolutely clear in thosecircumstances that it would be appropriate toseek planning obligations to meet the needgenerated by the new development (see page56 for more detail). In order for this process tobe efficient, transparent and predictable it iscrucial that the policy framework is clearlyestablished in the Local DevelopmentFramework and in Supplementary PlanningDocuments. Robust procedures and goodcommunications as set out in the engagementagreement will ensure that resources aregenerated for health and that as a result healthservices are expanded to meet the needs of thenew population.
Summary: steps in alignment
• The local Community Strategy sets high levelobjectives for health
• The Local Development Framework isprepared using sound health evidence and haspolicies to promote health and well-being andto secure health services and facilities for newand existing populations
• The PCT prepares its health strategydocuments taking into account the localCommunity Strategy objectives for health andensuring that the spatial implications areclearly identified
• A map or spatial framework is prepared incollaboration with the Local PlanningAuthority to show diagrammatically howgrowth and services will be matched over theplan period
• In considering planning applications the LocalPlanning Authority ensures development has apositive or neutral effect on the widerdeterminants of health
• The Local Planning Authority takes intoaccount the PCTs views on significantdevelopments
• Where local services cannot cope financialresources are secured to improve themthrough section 106 agreements
• The potential flow of finance through section106 agreements is fully integrated into thePCTs investment and delivery plans
Greenwich Millennium school and Health Centre

41
Health and Urban Planning Toolkit Phase 3: Making engagement work
Scheme and Statement of CommunityInvolvement set the context for preparation ofthe Development Plan Documents. A briefdescription of these and other key documentsand their relevance to health and PCTs isincluded below in Table 7.1.
Relevance to health
May identify documents thataddress health or healthimplications.
Secures the involvement of healthagencies and the public enablinginput on health matters.
Should identify how the spatialimplications of health should beaddressed and outcomes delivered.
Should include criteria that canachieve health improvement,reduce inequalities and securehealth services.
May identify sites with publichealth implications for example, orto mark the location of a proposedhealth facility or NHS landholding.
The document can be used to helpaddress health issues or healthservices, particularly areas about toundergo physical regeneration.
Can identify the geographicalrelationship of policies with healthimplications.
Relevance to PCTs
Forewarns PCTs of the need for involvement in preparationprocesses, and should bemonitored.
PCTs can seek to be included. NHSLondon must be included as it is astatutory consultee for the LocalDevelopment Framework.
Should reflect the PCTs strategiesand programmes and addresshealth.
The PCT may propose or helpformulate specific interventionswhich can be reflected in thecriteria.
The PCT may need to address theimplications of a site allocationdepending on the use, or possiblyseek allocations for health facilitiesor landholdings.
The PCT may have a specificinterest in an area relating to healthissues or services.
Policies of interest to the PCT couldbe reflected in the Proposals Map.
Document
Core Strategy
GenericDevelopmentControl Policies
Site SpecificAllocations ofLand
Action Area Plans
Proposals Map
Description
Sets out the documents that willmake up the Local DevelopmentFramework and the timetable fortheir preparation.
Sets out how the Local PlanningAuthority will involve the communityand stakeholders in the LocalDevelopment Frameworkpreparation process and consult onplanning applications.
Sets out the vision, objectives andspatial strategy for the Borough. Itshould reflect the local CommunityStrategy, and the strategies andprogrammes of other stakeholders,and include a monitoring andimplementation framework.
Sets out criteria in accordance withthe Core Strategy against whichplanning applications will beassessed.
Identifies land that is allocated for aspecific use or uses.
Provides a framework for areaswhere significant change orconservation is needed.
Illustrates the geographical extent ofpolicies.
Statement of Community Involvement
Local Development Scheme
Development Plan Documents
Table 7.1 – Components of the Local Development Framework and their relevance to health and PCTs
Preparing the Local DevelopmentFramework
Each of the Local Development Documents thatmake up the Local Development Framework hasa different purpose. The Local Development

42
Steps in preparing the Local DevelopmentFramework Development Plan Documents
Early consultation
Legislation and guidance emphasises ‘frontloading’ of the preparation process, whichmeans that Local Planning Authorities should beseeking input at the earliest stage, even beforeit has started to set out the parameters of theCore Strategy and the Sustainability Appraisal.The PCT will find its input most influential atthis stage as health has a better chance ofbeing a part of the overall fabric of the CoreStrategy and the Sustainability Appraisal. KeyPCT input to be provided at this early stageincludes:
• Description of the PCTs spatial vision forhealth
• Health evidence base for public health andhealth inequalities
• Infrastructure, including statistics or healthestates condition reports
• Health needs assessment to ascertainpotential health service requirements
• Health issues and hotspots• Potential interventions to address health issues• Sustainability criteria for assessing the
document against• Assistance with the formulation of options for
development in the Borough and assessmentof the potential health outcomes of thoseoptions.
Local Planning Authorities are encouraged toinclude a representative from the PCT on anyteam coordinating the Local DevelopmentFramework to ensure health is addressedproperly. Figure 7.2 illustrates the key stepsinvolved in the Local Development Frameworkpreparation process, including detail on keyopportunities for PCT input.
As illustrated in Figure 7.2, the PCT will alsohave formal opportunities at later stages toprovide input, including at the ‘issues andoptions’ and ‘preferred options’ stages, andExamination in Public. It will be important forPCTs to take these opportunities to provideinput, particularly as submissions are not carriedthrough the process and only count for theassociated stage of preparation. This underlinesthe need for PCTs to put in place a system tomonitor and provide input to LocalDevelopment Framework preparation whererequired so opportunities are not missed. It mayalso be possible for the PCT to appear beforethe Inspector if required. This is discussedfurther on pages 46 and 47.
Health and Urban Planning Toolkit Phase 3: Making engagement work
Relevance to health
Matters may have health or healthservices implications.
Indicates whether health targetsand policies are being achieved.This will also assist revision of theLocal Development Frameworkdocuments.
Relevance to PCTs
The matter may be of interest tothe PCT- a Planning ObligationsSupplementary Planning Documentis a common example.
The approach to monitoring shouldbe integrated with the PCT.
Document Description
Provides further detail on mattersalready included in the DevelopmentPlan Documents.
Provides assessment of LocalDevelopment Schemeimplementation and the extent towhich policies in the LocalDevelopment Documents are beingachieved, based on monitoringsystems.
Supplementary Planning Document
Annual Monitoring Report

43
Health and Urban Planning Toolkit Phase 3: Making engagement work
Figure 7.2 – Indicative Local Development Framework Development Plan Document preparation process and PCT engagement
Advise vision and provide health evidence base, issues and potential interventions. Assist with health sustainability appraisal criteria. Assist with formulation of options. (Refer to pages 44 and 45 for more detail).
Review report to ensure it reflects statutory requirements (e.g. the London Plan, local Community Strategy and strategies and programmes of the PCT.) (Refer to pages 46 and 47 for more detail).
Review report to ensure it meets the expectations of the PCT and respond accordingly. (Refer to pages 46 and 47 for more detail).
Make written representations supporting or objecting to the Submission Development Plan Document and sustainability report if required. (Refer to pages 46 and 47 for more detail).
Prepare scoping report for Sustainability Appraisal.
Prepare an initial appraisal of issues and options.
Prepare a final appraisal of issues and options.
Submit amended final sustainability report to Government.
Attend informal pre-examination meeting if requested by the PCT. (Refer to pages 46 and 47 for more detail).
Attend examination if requested by the PCT. (Refer to pages 46 and 47 for more detail).
PCT engagement Sustainability appraisalThe Local Planning Authority’s role
Gather evidence on social, economic and environmental characteristics, including health, of the Borough. Refer to page 44 on scoping the evidence base.
Ongoing engagement and consultation with consultation bodies.
Prepare and publish an Issues and Options report. Refer to page 45 on scoping the policy framework.
Ongoing engagement and consultation with consultation bodies.
Prepare and publish a Preferred Options report.
6 weeks consultation on Preferred Options and Appraisal.
Prepare and submit Submission Development Plan Document.
6 weeks consultation on Submission Development Plan Document and Appraisal.
Pre-examination meeting.
Independent examination of the Submission Development Plan Document before an Inspector.
Inspector issues the ‘binding’ report on the Submission Development Plan Document.
Council modifies the Development Plan Document in accordance with the Inspector’s binding report and adopts it.
Monitoring and review.

Health and Urban Planning Toolkit Phase 3: Making engagement work
44
Sourcing the evidence base
Local Development Frameworks and thestrategies prepared by the PCT to inform it needto identify the baseline of health conditions,health issues affecting the area and healthinequalities. As far as health is concerned, it iscrucial that any planning policies are distinctive,relevant to local circumstances and based onsound evidence. The PCT in its Annual PublicHealth Report and in other analyses is ideallyplaced to collect that evidence. All PCTs willalready be doing this in one form or another.
Health inequalities are key indicators forsustainable communities. The nature ofinequalities and their spatial distribution maywell be relevant to setting planning polices.Some inequalities may reflect the relative stateof health in the Local Planning Authority area asa whole, in relation to London or to thenational average. These too may point toplanning policies. PCTs and Local PlanningAuthorities should collaborate to have acommon approach to identifying, quantifyingand monitoring health and health inequalities.The following list in Table 7.2 suggests somelinks between environment and health.
Symptom or condition
Heart disease
Obesity
Mental illness
Accidents
Respiratory disease
Linked to environmental factor
Availability of space and opportunity for exercise
Availability of space for exercise, safe walking
Lack of green space, isolation
High vehicle speeds, lack of safe walkways
Air pollution
Table 7.2 – Examples of links between environment and health.

45
Health and Urban Planning Toolkit Phase 3: Making engagement work
Table 7.3 – Watch Out for Health Checklist – Key headings for health and the role of planning policy to address them.
Identifying these and other links locally andputting together sound evidence that is spatiallyreferenced using for instance GIS, will provide agood basis for the later stages of detailed policyformulation.
Scoping the policy framework for health inthe Local Development Framework
Watch Out for Health is HUDU’s checklist thatsets out the key influences (the widerdeterminants) on health, which can be used toidentify pathways and interventions andsystematically assess policies (refer to page 47for more information on Watch Out for Health).Using the categories from Watch Out forHealth, the summary table below givesexamples of how planning policies can bedesigned to support healthy communities.
Healthy Community Indicator
Healthy lifestyles
Housing quality
Access to work
Accessibility – ease of movingaround by whatever means
Access to fresh high qualityaffordable food
Crime reduction community safety
Air quality
Social cohesion
Access to services
Resource use and climatechange
Role of planning policy
Making provision for a good standard and range of open space readily accessible, securingsafe paths to access the space and encouraging physical activity wherever possible
Insisting on high environmental standards in new housing; identifying areas of poor housingand planning for improvement and renewal
Making provision for diverse employment opportunities accessible to the community;protecting employment by retaining workplaces and mixed land uses
Ensuring that pedestrians in particular children have safe and direct pathways; that distancesare minimised and barriers to walking and cycling removed; that there is opportunity toprovide safe and reliable public transport close to homes
Make provision for a diversity of food outlets, for markets and for space for local productionof food; protecting key markets and food outlets
Making provision for high quality public realm and spaces and facilities that are supervised bythe community
Identifying and predicting poor air quality; reducing traffic levels and protecting homes fromsources of air pollution; providing green space, water and ventilation and tree planting toimprove air quality
Identifying strong and weak community settings; securing community and socialinfrastructure and avoiding severance by roads and other barriers; ensuring high qualitypublic realm to encourage social interaction
Identifying the spatial relationship between the demand for personal and community servicesand the location, character and density of population; identifying existing and future gapsand making provision for new service delivery locations
Discouraging development that uses no renewable resources; insisting on buildings that useenergy highly efficiently, conserving water resources and encouraging walking and cycling

46
Evaluating the Options
Once the issues and options report has been prepared, a consultation period will offer a formalopportunity for the PCT to scrutinise the document. The PCT may find the following checklistuseful:
Does the report comply with statutory requirements:
Reflects the local Community Strategy;
Reflects the London Plan;
Takes into account the strategies and programmes of the PCT; and
Accompanied by a Strategic Environmental Assessment/SustainabilityAppraisal that addresses health?
Does the Sustainability Appraisal provide an adequate framework for assessinghealth impacts?
Does the Sustainability Appraisal identify ways of enhancing positive healtheffects and are these incorporated into the Core Strategy?
Is the report based on robust evidence, which adequately highlights the healthissues and the scope for health interventions?
Have the spatial implications of those health issues been taken into account anda response to those issues set out in policies?
Does the report set out a policy framework that can influence health inequalitiesand improve health in a realistic way?
Are the options proposed realistic and have they accurately taken into accountthe likely health outcomes?
Are the options sustainable i.e. will the options contribute to healthimprovement and enable adequate provision of health services?
Does the report identify key targets and indicators for health improvement?
Does it provide a spatial framework for investment in health infrastructure thatwill enable successful delivery of the Local Development Framework?
YES NO
Health and Urban Planning Toolkit Phase 3: Making engagement work

whether it believes the document to be sound –whether the document has been preparedproperly, whether it conforms to legislation, theLondon Plan and the local Community Strategy,and whether the policies are coherent,consistent and effective. The PCT can makewritten representations on this if it is unhappyeven at this late stage, and may be expected tocomplete its submission on standard proforma.The PCT will need to provide detail on why thedocument is unsound together with suggestionsas to how the document could be made sound.The Local Planning Authority is expected todraw the representations together forconsideration by the Inspector. Furtherinformation on soundness can be obtained fromthe Borough. The PCT will also be asked tonominate whether it wants to attend theexamination and present its representations inperson.
The Local Planning Authority can be directed bythe Inspector or the Secretary of State to makechanges to the document if required. Thepotential difficulties that may arise frombringing up issues with the SubmissionDevelopment Plan Document at this late stageunderline the importance of ‘front loading’ andinvolving the PCT as early as possible andmaking sure everyone understands theimplications for health.
47
Health and Urban Planning Toolkit Phase 3: Making engagement work
The PCT should monitor its input, particularlywith the engagement agreement in mind, andfound out how input will be taken intoaccount.
Following consultation on the issues andoptions report, the Local Planning Authority willprepare a report that sets out the preferredoption for spatial development in the Borough.The PCT can also use the above points to checkwhether the preferred option will facilitatehealthy outcomes. The PCT will have a formalopportunity to comment on the preferredoption.
Written representations for the SubmissionDevelopment Plan Document
Once the Local Planning Authority is satisfiedthat the preferred option has been identified, itwill prepare a final version known as theSubmission Development Plan Document (forexample, the Core Strategy SubmissionDevelopment Plan Document). This version willbe submitted to the Planning Inspectorate forindependent examination, on behalf of theSecretary of State. At this point, the SubmissionDevelopment Plan Document will undergoanother six week consultation period in whichfurther representations can be made by thecommunity and stakeholders, including the PCT.The focus for the PCT at this stage will be
Using HUDU Tools to scope and evaluate the LocalDevelopment Framework policy framework
Watch Out for Health is HUDU’s checklist for health which contains ten key categoriesthat address the wider determinants of health, ranging from healthy lifestyles and foodaccess to social cohesion and climate change. It provides a structure for scoping out policiesin the Local Development Framework that address health, and for evaluating those policies.Importantly, it will help health and planning practitioners work together to find solutions toaddress local health issues. It also provides links to further information on each of thecategories.
It is based on the WHO publication Healthy Urban Planning (WHO 2000) prepared by HughBarton and Catherine Tsourou. A generic version of Watch Out for Health is downloadablefrom www.healthyurbandevelopment.nhs.uk.
It is currently being developed to provide guidance on effective policies and designprinciples for health improvement. This guidance to be called ‘Delivering HealthierCommunities’ is expected to be published in May 2007.

48
Health and Urban Planning Toolkit Phase 3: Making engagement work
The process
The Local Strategic Partnership
The local Community Strategy
The Local DevelopmentFramework
YES NO
Indicators of success for strategic engagement
Tasks for PCT
PCT chief officer or senior staff actively engaged in the Local StrategicPartnership
PCT public health and clinical staff identify key health issues from public healthand epidemiological analysis
Effective engagement with community and stakeholders to decide on priorities
Realistic but challenging objectives set for health improvement and reduction ininequalities
Objectives aligned with local delivery plan and Strategic Services DevelopmentPlan so that investment follows objectives
Objectives are fed into the Local Area Agreement
Monitoring systems set up and reviews undertaken
PCT is engaged at a senior level and the earliest stage, helping to set the corestrategy and the key objectives
PCT and others bring evidence of health issues quantified and plotted spatiallyand suggest priority interventions
PCT participates in the process by which the community engages in the LocalDevelopment Framework to explain and gain support for health objectives
Realistic objectives (targets and indicators) set in collaboration with the LocalPlanning Authority that have a spatial dimension
An effective set of policies is designed in collaboration with the Local PlanningAuthority
PCT aligns these spatial policies with its Local Delivery Plan and StrategicService Development Plan
Regular monitoring, review and re evaluation in the light of changing healthindicators
Conclusion
The above guidance will enable PCTs to findtheir way through what is a complex process. Itwill help Local Planning Authorities to managetheir approach to the Local DevelopmentFramework in a way that will maximise thepositive health outcomes and ensure healthservices are fully embedded in the
implementation plan, thus reinforcing thesoundness of the Development Plan.
The following checklist can be used to measurethe success of the engagement process as itevolves:

49
Health and Urban Planning Toolkit Phase 3: Making engagement work
Health in a Healthy City; The Annual Report of the Director of PublicHealth 2005 and Brighton and Hove City Health Development Plan –Brighton and Hove City PCT
Health in a Healthy City goes beyond what is normally expected of an AnnualPublic Health Report as it looks at wider determinants of health such aslifestyle, transport, housing, crime, economic development and city planning.The section on city planning highlights the important relationship between thelocal Community Strategy the Local Development Framework and health. Italso cites matters like transport, open space and food access that will need tobe addressed through the Local Development Framework to address healthand lists recommendations to help achieve this. These recommendations arealso supported by a delivery plan which sets out the actions required toimplement them like the education of city planners, and requiring HealthImpact Assessment to be done on all Local Development Framework policydocuments.
Brighton and Hove City and thePCT are part of the WHO HealthyCities Project, and have preparedHealth in a Healthy City as arequirement its membership. TheWHO Healthy Cities Projectembraces the ‘principles of inter-sectoral co-operation, communityinvolvement, equity and politicalsupport in the planning process’,which this Toolkit also supports.Further information and a copy ofHealth in a Healthy City can befound atwww.brightonhovecitypct.nhs.uk.
Best Practice Examples
The way forward may seem difficult however there are already a number of PCTs and LocalPlanning Authorities working together as described above – two best practice examples ofthis are included below.
Bes
t Pr
acti
ce E
xam
ple

Health and Urban Planning Toolkit Phase 3: Making engagement work
50
WHAT TO DO NEXT…
Informing the Local Development Framework will secure the possibly of healthoutcomes through the planning process. However, the PCT and Local PlanningAuthority will still need to work together to ensure those outcomes aremaximised through development control, as identified in Step 8.
Tower Hamlets Primary and Community Care Services Strategy
The Tower Hamlets PCT and the London Borough of Tower Hamletsworked together to produce Improving Health and Well-being in TowerHamlets – A Strategy for Primary and Community Care Services 2006 to2016, a shared vision for primary and community care services.
It links strategic aims and more detailed targets with the investment inprimary and community care services required to help deliver those aims.To arrive at a common spatial framework, the Strategy takes into accounta range of services, the fitness for purpose of the current estate,population growth and likely demand, and opportunities for development.
As well as guidingcorporate activities,the strategy caninform thepreparation of theLocal DevelopmentFramework and theplanning applicationprocess. Thisapproach received acommendation at theLondon PlanningAwards 2006.
Further informationand a copy of theStrategy can be foundat www.thpct.nhs.uk.
Bes
t Pr
acti
ce E
xam
ple

This step identifies how health should beintegrated into development control and theplanning application process to maximise thedelivery of health outcomes. It also sets out away for the PCT to inform the process bysetting up its own systems and aligning themwith the Local Planning Authority.
The relationship between developmentcontrol, health and the PCT
Development control is a generic term used todescribe the function of the Local PlanningAuthority that manages the planningapplication process. A team of planners will beresponsible for a range of tasks linked to theprocess, like liaison with applicants,consultation, assessment and reporting. Staffusually have delegated power from the BoroughCouncil Planning Committee to determine manyproposals, however the Committee will beresponsible for determining most of the largeror more contentious planning applications.
The key purpose of engagement withdevelopment control for the PCT is the deliveryof development on the ground that facilitatesimproved health of the population and includesthe health services necessary to meet theirneeds.
The PCT should be in a position to work withdevelopment control and get involved in theplanning application process at all stages,particularly pre-application stages whendevelopment proposals are being formulated,Environmental and Health Impact Assessmentsundertaken and planning obligations estimated.The Local Planning Authority should positivelyinclude the PCT.
To do this, the PCT will need to set up its ownsystems for informing the planning applicationprocess where required, and align them withthose of the Local Planning Authority. The LocalPlanning Authority will need to ensure policiesof the Local Development Frameworksupporting health are implementedappropriately, and PCT input is taken intoaccount where required.
Planning application process
The planning application process involves threekey phases – the pre-application, applicationand post-application phases, discussed below.Figure 8.1 provides an illustration of thisprocess. There are also potentially a number ofsub-processes that occur concurrently includingEnvironmental Impact Assessment and section106 processes where health can be addressed,also discussed below and illustrated in Figure 8.1.
51
Health and Urban Planning Toolkit Phase 3: Making engagement work
Step 8 Ensure the Development Control process delivers health outcomes and involves the PCT.

Development proposal formulated.
s106 required?If yes…
s106 contribution estimated.
EIA screening.EIA required…
EIA scoping opinion – sought to define issues.
Prepare Environmental Statement.
Baseline Study.
Consultation.
Impact assessment.
Environmental Statement finalised.Proposal finalised.
Environmental Statement also consulted.
Environmental Statement evaluated by LPA.
Developer submits further detail if required.
LPA works out s106 contribution.
Developer completes & submits viability study.
Contribution agreed.
LPA prepares report.
Recommendation to Approve.Recommendation to Refuse.
Application may be withdrawn.
Approval – Delegated or Committee Decision.
Refusal – Delegated or Committee Decision.
Formal s106 agreement completed.
Financial s106 contribution secured.
Physical s106 contribution delivered.
Developer proceeds with proposal.
Planning Application submitted together with Environmental Statement and other supporting documents.
Public and stakeholder consultation for 21 days.
Application assessed by Local Planning Authority.
Developer submits further detail if required.
Developer drops proposal or modifies it.
Planning Application Process
Main processes
Pre-
appl
icat
ion
phas
eA
pplic
atio
n ph
ase
Post
-app
licat
ion
phas
e
Pre-application discussion with Local Planning Authority (LPA).
Decision Challenged – Developer submits appeal to the Planning Inspectorate.
EIA process s106 process
52
Health and Urban Planning Toolkit Phase 3: Making engagement work
Figure 8.1 – Planning application process and concurrent Environmental Impact Assessment (EIA) and section 106 (s106) processes

Planning applications for a range of proposals,such as residential, commercial and industrialmay have health implications. PCTs should beinterested in proposals that involve:• Opportunities for health improvement or
where this is not being facilitated properly, forexample residential proposals that provideinsufficient open space or have poor foodaccess or commercial proposals that do notfacilitate physical activity
• Impacts on public health, for exampleindustrial plants that emit air pollution
• Impact on health services, for example fromresidential proposals in areas where healthservices would struggle to handle additionalpatients
Pre-application phase
The process usually begins with the pre-application discussions between the LocalPlanning Authority and developer, which can becritical to setting the right direction for aproposal. The Local Planning Authority willconfirm whether a proposal will requireEnvironmental Impact Assessment and whetherplanning obligations will be required and forwhat.
Depending on the proposal, the PCT may wantto raise any health issues and suggest how theyshould be addressed, or request that a HealthImpact Assessment be undertaken. The PCTmay also want to contribute to scoping of theEnvironmental or Health Impact Assessmentprocesses for example as part of a steeringgroup or to provide evidence or other expertise.
There is no formal remit for the PCT to beinvolved at this stage, so it will be essential thatthe engagement agreement discussed in Step 6ensures this happens in appropriate cases.Intelligence provided by the Local PlanningAuthority on future development proposals willalso help the PCT anticipate its involvement –which might include proactive approaches todevelopers. Also, it is not uncommon fordevelopers to approach PCTs directly at thisstage in any case. Use of tools such as WatchOut for Health and the HUDU s106 Model canbe suggested at this stage. More informationon these tools is provided on page 55.
Application phase
Once the development proposal (and potentiallythe Environmental Impact Assessment) has beenfinalised, the developer will seek planningpermission for it by lodging a planningapplication with the Local Planning Authority.The planning application will be accompaniedby plans and possibly several other supportingdocuments like an Environmental Statement(the final report of the Environmental ImpactAssessment process) if required. The LocalPlanning Authority will forward the proposal tostakeholders, including the PCT if agreed withthe Borough. The PCT will have 21 days torespond to the proposal. This period will providethe PCT with the opportunity to formallyrespond to the proposal and object if necessary.
The PCT should provide a response in line withthe engagement agreement. Not all applicationswill require a detailed assessment by the PCT –in fact some may only require a simple letter ofsupport. Where a detailed response is required,as a minimum, an assessment of the widerdeterminants of health and suggested planningobligations should be provided to ensure thePCTs interests are addressed. The Local PlanningAuthority will need detail on planningobligations in particular as it will want tofinalise its request to the applicant. Informationon existing health services capacity, thepotential impact and where and when planningobligations will be required will be useful. ThePCT should also be ready to get involved innegotiations if the need arises. Further detail onresponding to consultation, including asuggested process is included below.
Once consulted, the case officer will assess theproposal, taking into account the DevelopmentPlan and any other material considerations, aswell as responses from stakeholders. The LocalPlanning Authority will also be keen to finalisethe requirement for planning obligations andwill probably do so following the consultationperiod. The developer may undertake a study todetermine the viability of the request forplanning obligations. The resulting report by thecase officer will give a recommendation toapprove or refuse. It may need to go toPlanning Committee or may be approved underdelegation. If planning obligations are requiredthe applicant will need to sign the section 106agreement before the approval is issued.
53
Health and Urban Planning Toolkit Phase 3: Making engagement work

54
The Local Planning Authority must decide theapplication in line with the policies in theDevelopment Plan unless there are otheroverriding considerations. A significant negativeimpact upon health could be enough for aplanning application to be refused. If planningpermission is refused, the development proposalwill not go ahead and any section 106contribution will not be forthcoming. Thedeveloper has a right to appeal against theplanning refusal, a process which is dealt withby the Planning Inspectorate, an independentnon-governmental body, which could overturnthe original decision.
Post-application phase
If the developer wishes to proceed with theapproval, they will fulfil the conditions ofplanning approval including the terms of thesection 106 agreement if required. Financialcontributions will be provided to the LocalPlanning Authority who will forward them to athird party, such as the PCT, if part of theagreement. Any infrastructure to be providedwill be delivered as part of the development. Ifthe developer is unhappy with conditions theymay decide to lodge an appeal.
The PCT must be able to monitor the use of anyfinancial contributions it receives and providefeedback on this to the Local PlanningAuthority. The PCT should be able to do thisthrough its normal accounting procedures. Theterms of this arrangement may be set out in theengagement agreement discussed in Step 6.
Deadlines and timescales
Local Planning Authorities have tight deadlineswhen dealing with a planning application. Forexample, minor applications should bedetermined within 8 weeks, major applicationsshould be determined within 13 weeks, andapplications subject to Environmental ImpactAssessment determined within 16 weeks. Theformal consultation period for planningapplications is usually twenty one days.Adherence to these deadlines has an impact onachieving government targets and future LocalPlanning Authority funding. As a consequencePCTs should get involved as quickly as possiblein the process, should alert the planners at the
earliest possible opportunity if they have anyconcerns or comments, and should respond torequests for further comment quickly. Failure torespond in a timely fashion will limit the healthbenefits of engagement.
Aligning the PCT with the planningapplication process
When a PCT becomes aware of a planningapplication it needs to assess the likely impactof the proposal upon health and health serviceand facilities, and then respond in a way whichmaximises the opportunity to gain the greatesthealth outcome and limits the possible negativeeffects. This assessment should follow thefollowing stages:
• Understand the proposal – what is beingproposed?
• Identify and assess possible impacts uponhealth services and wider public health issues,including evaluating any EnvironmentalStatement (prepared as part of anEnvironmental Impact Assessment) or HealthImpact Assessment (refer to page 56 andAppendix 3 for more detail on EnvironmentalImpact Assessment and Health ImpactAssessment)
• The PCT can assess the planning applicationusing two HUDU tools highlighted below:
• Likely impact on wider public health – WatchOut for Health (refer to page 55)
• Likely impact on health services – HUDU s106Model (refer to page 55)
• Identifying what would need to be changed inorder to minimise negative impacts andmaximise positive ones, including detail onplanning obligations
• Collect views from across the PCT and fromexternal invitees if required
• Prepare a response to the Local PlanningAuthority. The letter template at Appendix 4can help
• Submit the response to the Local PlanningAuthority and continue with ongoingdialogue, including section 106 negotiations
These stages are given in greater detail in anindicative response process (with suggestedinvolvement of PCT staff identified) in Step 9and at Appendix 5.
Health and Urban Planning Toolkit Phase 3: Making engagement work
Queens Market, Newham

Using HUDU Tools to evaluate impacts on health from development proposals
Watch Out for Health, HUDU’s checklist for health introduced in Step 7, can also beused to assess development proposals and scope out health issues in Environmental andHealth Impact Assessment processes. It also can be customised with local information andmethods for dealing with health issues, and support PCT health strategies. For example,health hotspots can be listed and linkages with local food access initiatives can beidentified in the document. This offers a real opportunity for PCTs, particularly if they areable to work with local stakeholders including the Local Planning Authority to ‘localise’ thedocument. In this way, a localised Watch Out for Health could be used by planning staffwhen assessing development proposals.
A generic version of Watch Out for Health is downloadable fromwww.healthyurbandevelopment.nhs.uk.
The HUDU s106 Model is a computer spreadsheet that calculates the health facilitiesrequired by the likely occupants of a housing proposal. It works out the requirements ofthe new population in terms of primary care (GPs only), intermediate care, acute care andmental health care and assesses the likely revenue and capital costs to the local NHS ofproviding it. The HUDU s106 Model seeks to calculate the overall financial burden that islikely to fall on the PCT as a consequence of the proposed development. This informationcan then be used to influence the assessment of a planning application and negotiationson planning obligations for health services. It should be noted that health will only be oneof a number of planning obligations requirements, and it may often be the case that notenough financial scope exists within the development process to fund all of the likelyhealth implications of new developments. Refer to pages 56 to 59 for further informationon planning obligations and section 106 agreements.
The HUDU s106 Model is being used by many London Local Planning Authorities. It hasbeen used to help secure over £10 million for additional health services since its launch inApril 2005.
A generic version of the HUDU s106 Model is available free of charge and downloadablefrom www.healthyurbandevelopment.nhs.uk. Bespoke versions for each PCT and LondonBorough are also available free of charge, and should be requested by emailing HUDU [email protected].
55
Health and Urban Planning Toolkit Phase 3: Making engagement work

56
Dealing with Environmental ImpactAssessment and Health Impact Assessment
Environmental Impact Assessment and HealthImpact Assessment are two processes that canbe undertaken to identify health impacts ofdevelopment. The key aspects of each, andwhere they may be relevant are explainedbelow.
Environmental Impact Assessment
• Environmental Impact Assessment is astatutory requirement imposed on some largecomplex development projects
• The purpose of Environmental ImpactAssessment is to identify and assess thesignificant environmental impacts and ifnecessary suggest alternatives or mitigation toavoid the negative impacts
• Environmental impacts include effects on thepopulation and including health effects
• The scope of an Environmental ImpactAssessment is set out in a scoping report
• The findings of an Environmental ImpactAssessment are set out in the EnvironmentalStatement
• An Environmental Statement must besubmitted with the planning application
• If consulted, PCTs should receive notice of anEnvironmental Statement at the same time asa planning application (but PCTs are notstatutory consultees)
• A limited amount of time (16 weeks) isallowed to consider a proposal which issubject to an Environmental ImpactAssessment
• Any weaknesses or omissions in theEnvironmental Impact Assessment found bythe PCT should be reported to the LocalPlanning Authority at the earliest possibleopportunity
• Unacceptable health impacts are grounds forrefusal
• Mitigation must be viable and realistic andagreed before planning permission is granted.Planning conditions or section 106 can beused to ensure the measures are built in
• PCTs should reassure themselves that themeasures are likely to be adequate andeffective
• PCTs should seek some involvement in themonitoring of mitigation measures affectinghealth
Health and Urban Planning Toolkit Phase 3: Making engagement work
Health Impact Assessment
• Health Impact Assessment is not a statutoryrequirement and needs to be agreed with theLocal Planning Authority at an early stage
• An Health Impact Assessment can be carriedout as part of an Environmental ImpactAssessment
• Any Health Impact Assessment shouldnormally be carried out before the planningapplication is considered
• The scope of Health Impact Assessmentshould identify the baseline, the most likelyhealth pathways and identify the mostsignificant health effects
• Health impacts should be assessed on thebasis of best public health knowledge andpractice and not simply in relation toprevailing standards
• Mitigation measures should be practical andeffective
• Implementation of mitigation should besecured through project design, planningconditions or legal agreement
• The means of monitoring health effects andmitigation measures should be agreed at thetime of permission and the PCT should seekto be involved where appropriate
• Please refer to Appendix 3 for morebackground on Environmental and HealthImpact Assessment.
Planning obligations and section 106agreements
Detailed control of development is normallyexercised through planning conditions whichare imposed when planning permission isgranted to control such things as access, designand landscaping.
However planning legislation also provides forthe Local Planning Authority and the developerto enter voluntarily into a legal agreement torun with the planning permission to controlthings that are not suitable or legally possiblefor planning conditions. These legal agreementssigned under section 106 of one of theplanning acts3 mean that developers andsometimes others with an interest in the landbecome subject to planning obligations. Thewording of section 106 is very wide but thepractice of planning obligations is also regulatedthrough Government guidance which is set outin Circular 05/2005.

Whilst section 106 agreements are essentiallyvoluntary the Local Planning Authority canrequire them as a precondition for grantingplanning permission. It follows that if adeveloper chooses not to enter into anagreement the planning permission will berefused in part because of its impact on localconditions.
The ability of a Local Planning Authority torequire such agreements in a particular casemust be based on a clear policy justification. In principle the planning act and regulationsreferenced above are sufficient but in practicelocal planning policy – the Development Plan(i.e. the London Plan and the LocalDevelopment Framework) must contain clearpolicy guidance on this topic.
The London Plan4 makes it clear that planningobligations should be required wheredevelopment will have an unacceptable impacton services and also in securing affordablehousing. The Mayor has decided that his firstpriorities for section 106 are transport andaffordable housing and that priority should alsobe given to education, childcare, health facilitiesand services and learning and skills (climatechange is proposed to be added in future).
Many Local Planning Authorities have policies intheir local plans or emerging Local DevelopmentFrameworks that reinforce or amplify this policy
57
Health and Urban Planning Toolkit Phase 3: Making engagement work
Planning obligations can require things to bedone on or off the particular site or may requiresums of money to be paid. Their purpose is toremove what otherwise would be barriers toplanning permission being granted.
Planning obligations have been used to addressa range of matters including aspects oftransport provision, affordable housing openspace and health and community facilities (orsocial infrastructure in general). The mainjustification for using them in respect of socialinfrastructure is that the developmentproposed, normally housing but not necessarily,would impose unacceptable burdens on existingcapacity in the locality – of health services oreducation for instance. In such a case aplanning obligation would require the developerto provide or make a payment that wouldenable the local facilities to be expanded orimproved so that they would be capable ofmeeting the needs of the proposed populationwithout causing deterioration in the servicesavailable to the existing community.
The cumulative impact of smaller applicationscan also be taken into account. Where theimpact of one small development is notsufficient to trigger the provision of a newfacility for example, then pooling ofcontributions is acceptable under Circular05/2005. PCTs and Boroughs should agree theapproach to pooling.
3. Town and Country Planning Act 19904. Policy 6A.4 and 6A.5 of the London Plan
Impression ofCrossharbour, theredevelopment ofthe London Arenasite, Isle of Dogs

58
and some have Supplementary PlanningDocuments that sets out in detail how planningobligations will be dealt with.
Summary and key facts for PCTs and Boroughs:
• Planning obligations are a legitimate means ofensuring that new developments do notcompromise the ability of local health servicesto deliver high quality services to both existingand new communities
• It is necessary to show that additionalprovision is made necessary as a result of thedemand created by new development andthat there is insufficient existing capacity andto quantify that required additional provision
• The scale of the additional provision needs tobe related to the actual impact of thedevelopment
• Then pooling of contributions from a numberof smaller developments is acceptable underCircular 05/2005
• It is the developer’s responsibility to pay thefull cost or if appropriate a contribution to thefull cost of the services needed5
• An obligation can require a contribution toboth facilities (buildings and or land) andservices (the revenue cost). A requirement forsupport for revenue may be limited to theperiod up to when mainstream fundingbecomes available6
• The PCT needs to be involved in anynegotiations that may result in a healthobligation
• The terms of a planning obligation should beclear and agreed by all parties prior to consentbeing granted
• The PCT needs to show how the financialcontribution or facility will be used to provideservices for the new population within areasonable period of time
• Clear arrangement should be in place to allowthe financial contribution to be usedappropriately by the PCT
• The HUDU s106 Model provides a systematicand accurate way of calculating healthrequirement (refer to page 55 for more detailon the HUDU s106 Model)
Revenue funding for health via section 106
While the provision of a capital asset (such as abuilding) through section 106 funding is anaccepted principle, the recognition of runningcosts for health is an emerging area of policyand practice, although revenue funding forother services (such as maintenance of open
space) has been accepted as a legitimateplanning obligation for many years. Theargument for including the revenue componentto section 106 agreements related to health isoutlined below.
Where the provision of health facilities isacknowledged to be needed as a result of adevelopment proposal (where there is notcapacity in the local NHS to meet the healthneeds of the new population, for example) thenthe provision of a capital health asset alone(such as a GPs surgery, for example) does not initself meet the planning need. Health servicesmust also be provided to meet the need andservices need to be funded. The HUDU s106Model assesses the likely revenue costs until theNHS funding allocation process takes account ofthe new population (normally 1 to 3 years) andmainstream funding takes over. Paragraph B19of Circular 5/05 states:
‘Where contributions to the initial support(‘pump priming’) of new facilities are necessary,these should reflect the time lag between theprovision of the new facility and its inclusion inpublic sector funding streams, or its ability torecover its own costs in the case of privately-runbus services, for example. Pump primingmaintenance payments should be time-limitedand not be required in perpetuity by planningobligations.’
The inclusion of revenue for health via s106 isfurther justified by London Plan policy 6A.5Planning Obligations, which states:
‘Boroughs should set out a clear framework fornegotiations on planning obligations in UDPshaving regard to central government policy andguidance and local and strategic considerations(see Policy 6A.4) to the effect that:
• it will be a material consideration whether adevelopment makes appropriate provision for,or contribution towards requirements that aremade necessary by and are related to, theproposed development
• negotiations should seek a contributiontowards the full7 cost of all such provisionthat is fairly and reasonably related in scaleand in kind to the proposed development andits impact on the wider area
• boroughs should refer to planningobligations that will be sought in the relevantparts of the UDP (such as transport andhousing policies).’
Health and Urban Planning Toolkit Phase 3: Making engagement work
5. Policy 6A.5 of the London Plan6. Circular 05/20057. Our emphasis

A number of Local Planning AuthoritySupplementary Planning Documents nowspecifically refer to the HUDU s106 Model asthe preferred method of assessing the impact ofdevelopment upon health care needs andinclude revenue for health. A recent examplefrom the London Borough of Merton isdiscussed further below.
Without recognition of the revenue impact ofnew populations the PCT would need toreallocate existing resources to meet the healthneeds of the new population. This is likely tomean that the service to the existing populationwould be constrained by the need to meet thisadditional unfunded demand, until mainstreamfunding was adjusted. This could constitutesignificant damage to interests ofacknowledged importance, and thus can be asignificant reason to refuse planning permission.
Should funding be secured for health through
section 106 the Local Planning Authority willneed to agree what that money will be spenton. The PCT should consider in advance whereany funding should go, bearing in mind thefollowing points:
• The health services provided through s106funding should directly relate to the healthneeds of the new population and should be ingeographical proximity to the facilitatingdevelopment
• Not all elements of health care deemednecessary in the HUDU s106 Model will bedirectly addressed in the section 106agreement in every case. This is partly becauseit would be impractical to secure incrementaland small scale improvements in every case
The health services secured through section 106agreements should integrate with the PCTs ownservice development plans, such as its StrategicService Development Plan.
59
Health and Urban Planning Toolkit Phase 3: Making engagement work
WHAT TO DO NEXT…
Once the PCT has confirmed the steps necessary to provide input to the planningapplication process, it will be important to allocate responsibilities to staff toundertake the tasks, which is discussed further in Step 9.
Bes
t Pr
acti
ce E
xam
ple Merton Planning Obligations Supplementary Planning Document
The London Borough of Merton has adopted a planning obligationsSupplementary Planning Document that sets out a ‘framework for assessingthe requirement, calculating and completing planning obligations fordevelopments’ to help with negotiating planning obligations.
To assess impacts on health services, theBorough adopted the HUDU s106 Modeland intends to apply it ‘on a site by site basisin consultation with the Sutton and MertonPrimary Care Trust’. The SupplementaryPlanning Document also states that where anew health facility is required the Boroughwill pursue both capital and revenuecontributions if required.
A copy of the SPD can be downloaded from the Borough website atwww.merton.gov.uk/living/planning/spg.htm.
SPDSupplementary Planning DocumentLondon Borough of Merton
PlanningObligations
July 2006

60
To make engagement a reality, the PCT andLocal Planning Authority will need to identifyand allocate responsibilities to staff. This stepsuggests how the PCT may allocateresponsibilities to staff, and how they wouldwork together to operate the systems.Suggestions are also provided for Local PlanningAuthorities to improve their understanding ofhealth.
Building PCT capacity
As identified in the Alignment Checklist in Step4, somebody should take responsibility for thefollowing roles:• High level ‘champion’ for engagement
- Director-level responsibility for the urbanplanning function
• Urban Planning Lead- Day to day management of the urban
planning function• Urban Planning Coordinator
- Coordinate urban planning matters,monitor planning proposals including theLocal Development Framework andplanning applications, liaise with the LocalPlanning Authority, prepare responses toplanning proposals and lead onnegotiation
The following tasks should become part ofsomebody’s job:• Assessment of health needs that arise from
plans or proposals (for example, withreference to the Annual Public Health Reportand more detailed population and healthdata) to inform decisions on the types ofhealth improvement measures or healthservices that may be required by new orchanging populations
• Assessment of plans and developmentproposals (using Watch Out for Health) todetermine whether health outcomes will bemaximised, and to identify interventionmeasures to improve health if required
• Assessment of health services and facilities todetermine whether they are sufficient andidentify where they need to be improved toaddress impacts
• Applying the HUDU s106 Model, to helpquantify health service requirements
• Monitoring and reporting on planningobligations
PCTs will already have staff in variousdepartments with the skills necessary toundertake the majority of the roles and tasks aspart of their current jobs. For example, a publichealth specialist may already be responsible forundertaking health needs assessment, andwould be well placed to look at this in relationto development proposals as well. There mayalready be a person that manages primary careservices who would be well placed to respondto health service capacity issues. In manyinstances, staff will already be doing this orsimilar work as part of their normal jobs. Theysimply need to be joined up in the wayproposed in this Toolkit.
Figure 9.1 illustrates how a PCT might matchexisting staff from various departments withthese roles and tasks. The organisationalmapping exercise described in Step 3 may alsohelp. Figure 9.1 also illustrates how togetherthese staff would form an inter-departmental‘Engagement Team’. The team would be linkedtogether by a coordinator who would do mostof the practical engagement work.
It is unlikely however that a PCT will have staffwith sufficient urban planning knowledge andskills to fulfil the coordinator role. It may needto take on new staff to fulfil this role,particularly if engagement and collaboration islikely to be intensive. Appendix 6 includes ageneric job description for a town planner,which provides further guidance on what therole is likely to entail together with an indicativework programme. It is likely that the PCT willfind appointment of a town planner costeffective as the role should be self-fundinggiven the planning obligations that the PCT willbe able secure.
Health and Urban Planning Toolkit Phase 3: Making engagement work
Step 9 Build the capacity of PCT and Local Planning Authority staff to engage.

This will have workload implications for staffinvolved, which will need to be managed.However, supported by adequate strategydocuments and Local Planning Authority staffwith more robust planning guidance, theadditional workload will be manageable. This front-loaded approach should also helpminimise the growth in workload overall overthe long run as the health of the populationimproves.
Appointing a planning consultant may be anoption for PCTs where discrete, large-scaleprojects are involved, however this may beunviable on an ongoing basis. The consultant isstill likely to require input from existing staff inthe ways identified above.
61
Health and Urban Planning Toolkit Phase 3: Making engagement work
Figure 9.1 – Indicative Structure for Inter-Departmental ‘Engagement Team’
PCT Board
Chief Executive
Director as ë champion’
Health Strategy Public Health Primary Care Estates Finance
Lead and / or Coordinator
Tasks: Prepare and manage responses.
Delegated Staff
Tasks: Assess plans and proposals.
Delegated Staff
Tasks: Health needs assessment.
Delegated Staff
Tasks: Assess health services implications
Delegated Staff
Tasks: Assess health facilities implications.
Delegated Staff
Tasks: Apply HUDU s106 Model and monitoring and reporting s106.
Admin Support
Engagement Team
Fawood Children’s Centre, Stonebridge Estate

62
Figure 9.2 illustrates how these roles and tasks might be linked as part of the planning applicationresponse process suggested in Step 8. Appendix 4 provides more detail on the process.
Figure 9.2 – The Engagement Team responding to consultation on a planning application.
Health and Urban Planning Toolkit Phase 3: Making engagement work
Planning Coordinator receives and screens proposal.
Health needs assessment. Apply HUDU s106 Model.Assess plans & proposals (use Watch Out for Health).
Assess health services implications.
Assess health facilities implications.
Planning Coordinator receives and screens proposal.Planning Coordinator combines comments.
Team Meeting if required
Planning Coordinator prepares response to Local Planning Authority.
Planning Lead signs off response.
Seek further information if required.
Health services implications?If yes…
Wider determinants of health implications? If yes…
Max
imu
m o
f 21
day
s
Local Planning Authority
Application consultation
Local Planning Authority
Response to Local Planning Authority
Discuss related health service implications if
required.

63
Health and Urban Planning Toolkit Phase 3: Making engagement work
Bes
t Pr
acti
ce E
xam
ple Greenwich Health Engagement Project
A town planner wascontracted to work withthe Greenwich TeachingPrimary Care Trust(GTPCT) to help addressa range of pressureslinked to populationgrowth occurring in theLondon ThamesGateway. The project,which was jointly run bythe GTPCT and HUDU,helped realise thepotential of the GTPCTto engage in theplanning system anddemonstrated thebenefits of having atown planner on board.
The town planner was able to use tools like Watch Out for Health andthe HUDU s106 Model to identify health impacts, and draw on the skillsand knowledge of existing staff from across the GTPCT to deviseeffective responses to those impacts. This approach improved thecapacity of the GTPCT to respond to development proposals, identifywhere planning obligations would be needed on the ground and securethose obligations.
The GTPCT has taken on board the recommendations from this project,and intends to develop its ongoing capacity to engage.
Greenwich Millennium Village

64
Within the Local Planning Authority
Local Planning Authorities will already have staffin place to operate and lead on the processesthat make up the planning system. For example,a lead will be allocated to the preparation ofthe Local Development Framework, andplanning applications are allocated to caseofficers. However, staff will need to be madeaware of the expectations set out in theengagement agreement and assignedresponsibilities for engagement wherenecessary.
Managers and team leaders should ensurehealth is taken into account, and that healthaspects are explicitly reported on in appropriatecases. Adding a health component to reporttemplates would help with this, and could beagreed as part of the engagement agreement.Case officers should have the skills to be able toidentify or consider health implications andrespond where required. The use of toolsincluding Watch Out for Health and the HUDUs106 Model could also be agreed with the PCT.Additional training on health issues, localresponses and Health Impact Assessment willneed to be provided to ensure staff have thenecessary skills to do this. The Local PlanningAuthority could work with the PCT to develop astaff training programme. HUDU can providethis service.
Health and Urban Planning Toolkit Phase 3: Making engagement work
Summary
• The PCT will need to allocate key roles andtasks, and potentially modify job descriptionsto ensure engagement work embedded.
• PCTs will already have many of the staffrequired to fulfil these roles and tasks, andmany may be doing the work requiredalready, however they may need to work in amore coordinated and joined up way to bemore effective.
• Local Planning Authorities will already havethe staff in place, but will need to ensure responsibilities are allocated andstaff have the skills to deal with health issues.
• The PCT and Local Planning Authority maywant to work together to develop a staff training programme, which HUDU canassist with.
WHAT TO DO NEXT…
The PCT should identify the staff who will need to work together as part of theEngagement Team, and assign responsibilities. This may involve modifying some jobdescriptions to ensure the tasks are embedded. The feasibility of employing a townplanner to coordinate the PCTs urban planning function should also be considered,taking into account the potential to secure planning obligations.
The PCT and Local Planning Authority should work together to develop a trainingprogramme for staff. HUDU can help with this.

65
this work can be made far more effective inmeeting the key objectives of PCTs and LocalPlanning Authorities. Figure 10.1 provides asummary of many of these interactions wherekey work streams are concerned, as well assome of the outcomes that will makeengagement and collaboration a necessity.
The success of this Toolkit will depend on theextent to which PCTs and Local PlanningAuthorities across London are able to use it as aguide to build and maintain their relationshipson an ongoing basis to achieve shared goals.
The Toolkit will evolve, requiring updates aslegislation and policy change and PCTs andLocal Planning Authorities are subject to newchallenges. HUDU will continue to develop theToolkit – adding components and revising it inresponse to your feedback and to newchallenges.
Summing up
It is clear that there is a link between health andwell-being and the built environment. Inaddition, access to high quality health services isa key factor in reducing health inequalities. PCTsand Local Planning Authorities must thereforeengage and collaborate if they are to shape thebuilt environment to improve health, tackleinequalities, and deliver sustainabledevelopment. Through this, the health servicewill help achieve its goal of a ‘fully engagedscenario’, proposed by Derek Wanless. Theplans of the Local Planning Authority will meettests of soundness and it will have confidencethat it can source the health input it needs fromthe local PCT.
There are many aspects to engagement andcollaboration as described in this Toolkit.However, many of the activities are alreadybeing carried out by PCTs and Local PlanningAuthorities. The Toolkit suggests ways in which

Figure 10.1 – Summary of interactions between PCTs and Local Planning Authorities on key work streams.
• For Local Planning Authorities, reading across the table from each of the key work streams will identifythe interaction required with the PCT, and corresponding planning outcomes.
• For PCTs, reading down the table from each of the key work streams will identify the interaction requiredwith the Local Planning Authority, and corresponding health outcomes.
66
Health and Urban Planning Toolkit Summing up
Hea
lth
Ou
tco
mes
Health interests andcorresponding outcomesthat can be expected
key
Urban planning functions andcorresponding outcomes thatcan be expected
Elements of joint health andurban planning activity
Health Services
• Plan and deliver health servicesto meet growth.
• Secure resources to assist withprovision.
• Share strategy, including aspatial plan, for provision ofhealth services.
• Set out health evidence base.• Identify potential gaps in health
services.• Set out plan for provision of
health services.• Formulate policies that support
planning obligations for healthservices.
• Input at pre-application andapplication stages.
• Input to preparation ofEnvironmental or Health ImpactAssessments.
• Use HUDU s106 Model toassess impacts on healthservices and mitigation.
• Identify how impacts should beaddressed.
• Refer to Local DevelopmentFramework and PCT strategieswhere relevant.
• Make case for planningobligations and pursue.
• Monitor outcomes and planningobligations.
• Identify transition healthservices arrangements.
• New health services required.• Planning obligations for health
services.
• Better delivery and integrationof health services.
• Planning contribution for healthservices makes delivery moreresponsive and affordable forthe NHS.
PCT
Wider Determinants of Health
• Address local health issues,including inequalities.
• Shape built environment tofacilitate health improvement.
• Share strategy for addressingwider determinants of health.
• Set out health evidence base.• Identify health issues at front-
end of preparation process. • Formulate targets and policies
for improving health andtackling inequalities.
• Input at pre-application andapplication stages.
• Input to preparation ofEnvironmental or Health ImpactAssessments.
• Use Watch Out for Health toassess health impacts.
• Refer to Local DevelopmentFramework and PCT strategieswhere relevant.
• Monitor outcomes.
• Input during master planningstages, or preparation ofEnvironmental or Health ImpactAssessments.
• Use Watch Out for Health toassess health impacts.
• Refer to Local DevelopmentFramework and PCT strategieswhere relevant.
• Improved health and well-beingof the community.
• Reduce burden on healthservices.
• Improve awareness andunderstanding of health issuesamongst stakeholders.
Loca
l Pla
nn
ing
Au
tho
rity
Development Plan• Sound evidence base.• Reflects health aspirations
of the local CommunityStrategy.
• Reflects strategies andprogrammes of PCT.
• Sustainability appraisal.
Development Control• Seek input on health
improvement.• Identify impacts and need
for planning obligations.
Urban Regeneration• Seek input on health issues.• Identify impacts and need
for planning obligations.• Tackle existing inequalities.• Ensure health services meet
needs during developmentand long term.
Planning Outcomes
• Robust and credible document.• Statutory obligations of the
Local Planning Authority met.• Improved response to health
implications of development.• Enables Local Planning Authority
to ensure development issustainable.
• Improves quality of developmentproposals.
• Improves assessment times asresponse times to healthimplications should be shorter.
• Achieves sustainabledevelopment.
• Improves quality of urbanregeneration proposals.
• Improves response times tohealth implications.
• Ensures community issustainable.

67
Glossary and Useful Links
Queens Hospital, Romford

68
Health and Urban Planning Toolkit Glossary and Useful Links
Communities and Local Government (CLG)
www.communities.gov.uk
The CLG is the government departmentresponsible for community cohesion andequality, housing, urban regeneration, planningand local government.
Planning Inspectorate (PINS)
www.planning-inspectorate.gov.uk
PINS is the public body responsible forprocessing planning appeals, holding inquiriesinto local development plans and othercasework under planning and environmentallegislation in England and Wales.
Commission for the Built Environment(CABE)
www.cabe.org.uk
CABE is a statutory body that acts as achampion of good design in England. It alsoproduces a range of best practice guidance onhealthy building design.
Environment Agency
www.environment-agency.gov.uk
The principal government body responsible forthe protection of the environment.
Department for Health (DoH)
www.dh.gov.uk
The government department responsible forhealth. It fulfills its responsibility to providehealth services through the NHS.
The Glossary provides general descriptions of a range of agencies and terms relevant to health andurban planning. It is an introductory guide only and should not be used as a source for statutorydefinitions.
Government departments and other agencies
National level Health PlanningCommunities and Local Government (CLG) xPlanning Inspectorate (PINS) xCommission for the Built Environment (CABE) xEnvironment Agency N/ADepartment for Health (DoH) xNational Health Service (NHS) xHealth Protection Agency (HPA) x
Regional levelGovernment Office for London (GOL) xRegional Public Health Group (RPHG) xGreater London Authority (GLA) x xTransport for London (TFL) N/ALondon Development Agency (LDA) x xStrategic Health Authority (SHA) xNHS London Healthy Urban Development Unit (HUDU) x xLondon Health Commission (LHC) xLondon Health Observatory (LHO) x
Local levelLocal Strategic Partnership (LSP) x xLocal Authority (LA) x xLocal Planning Authority (LPA) xPrimary Care Trust (PCT) x

69
National Health Service (NHS)
www.nhs.uk
The NHS is a public body set up in 1948 toprovide health services in England, based onneed rather than the ability to pay for it. It isalso responsible for health and well-beingimprovement. The NHS is funded by thetaxpayer and is responsible to the Departmentof Health. At a regional level it is represented byten Strategic Health Authorities, including NHSLondon. At a local level, the NHS is representedby a range of organisations such as PCTs,hospital trusts, mental health trusts andambulance trusts, with each responsible forvarious elements of the local health service.
Health Protection Agency (HPA)
www.hpa.org.uk
The HPA is a non-departmental public body thatprovides support and advice on public health tothe NHS, local authorities, emergency servicesand other bodies. For example, proposalsinvolving air quality concerns may be referred tothe HPA for technical assessment, and it canalso help with IPPC applications.
Government Office for London (GOL)
www.gos.gov.uk/gol/
GOL is the regional office of the governmentfor London.
Regional Public Health Group – London
www.gol.gov.uk/gol/publichealth/
The Department of Health’s presence in theGovernment Office for London, and works toimprove and protect health, tackle inequalitiesand improve public health expertise.
Greater London Authority (GLA)
www.london.gov.uk
The GLA is the strategic authority for Londonand made up of a directly elected Mayor andAssembly. The Mayor is responsible forpreparing the London Plan, the spatialdevelopment strategy for London, and otherstrategic guidance on a range of topicsincluding health. Transport for London and theLondon Development Agency are also part ofthe ‘GLA family’ as they are the responsibility ofthe Mayor.
Transport for London (TFL)
www.tfl.gov.uk
The agency of the GLA that is responsible forthe majority of the public transport system inLondon.
London Development Agency (LDA)
www.lda.gov.uk
The agency of the GLA that is responsible foreconomic development in London. It is theRegional Development Agency (RDA) forLondon, and holds the health portfolio for allRDAs in England.
Strategic Health Authority (SHA)
www.london.nhs.uk
An SHA is a regional level NHS body responsiblefor the supervision of lower level NHS bodiessuch as PCTs within its area. The three mainfunctions of an SHA are:
• strategic leadership; • organisational and workforce development;
and • ensuring local systems operate effectively and
deliver improved performance.
(DoH 2006)
NHS London is the SHA for London andmanages the performance of 31 PCTs, 35hospital trusts, 9 mental health trusts and theLondon Ambulance Service.
Health and Urban Planning Toolkit Glossary and Useful Links

70
London Health Commission (LHC)
www.londonshealth.gov.uk
The London Health Commission is anindependent, high level, strategic partnershipthat was set up by the Mayor of London whichseeks to improve the well-being of allLondoners and reduce health inequalities.
London Health Observatory (LHO)
www.lho.org.uk
The LHO is one of a network of nine regionalPublic Health Observatories that were set up toimprove collection and availability of healthdata. It is a good source of health data, andguidance on Health Impact Assessment.
Local Strategic Partnership (LSP)
The Local Strategic Partnership is made up ofleaders from the public, private, business,community and voluntary sectors. Its role is toestablish priorities for joint action and developthe long-term strategic framework set out inthe local Community Strategy.
Local Authority (LA) or London Borough
A Local Authority is an administrative unit oflocal government responsible for a range ofmatters such as education, social services,transport and planning. Local Authorities areresponsible for preparing the local CommunityStrategy. All Local Authorities in London arealso referred to as London Boroughs, and arealso the Local Planning Authorities for theirarea.
More information on London Boroughs can befound at www.londoncouncils.gov.uk.
Local Planning Authority (LPA)
The Local Authority that is empowered by lawto exercise planning functions. All LondonBoroughs are also the Local Planning Authorityfor their area. Appendix 1 provides more detail.
More information on London Boroughs can befound at www.londoncouncils.gov.uk.
Primary Care Trust (PCT)
A PCT is an NHS body responsible for meetinghealth care need and improving the health andwell-being at a local level. The three mainfunctions of a PCT are:
• Engaging with its local population to improvehealth and well-being;
• Commissioning a comprehensive andequitable range of high quality, responsiveand efficient health services, within allocatedresources, across all service sectors; and
• Directly providing high quality responsive andefficient health services where this gives best-value.
Most PCTs in London are co-terminus withLondon Boroughs, with the exception of Cityand Hackney PCT (responsible for the City ofLondon Corporation and the London Boroughof Hackney) and Sutton and Merton PCT(responsible for the London Boroughs of Suttonand Merton).
Appendix 1 provides more detail. For links to allPCTs in London please go towww.london.nhs.uk.
Health and Urban Planning Toolkit Glossary and Useful Links

71
Terms
General Terms
Community Strategy
Local Authorities are required to prepare aCommunity Strategy under the LocalGovernment Act 2000. The objective of thelocal Community Strategy is to improve theeconomic, environmental and social wellbeingof local areas and contribute to theachievement of sustainable development. TheLocal Strategic Partnership made up of public,private, voluntary and community organisationsthat operate locally help set the vision andpriorities of the local Community Strategy.
Geographical Information Systems (GIS)
A computer application used to store, view, andanalyze geographical information, especiallymaps.
Sustainable community
Communities, defined by the Government, asplaces ‘where people want to live and work,now and in the future’.
Sustainable developmentA widely used definition drawn up by the WorldCommission on Environment and Developmentin 1987 is ‘Development that meets the needsof the present without compromising the abilityof future generations to meet their own needs’.
Health Terms
Funding allocation
PCT funding allocation is determined bycomparing the cost of care for a PCT’spopulation (based on age, need etc) comparedwith the actual spend of the PCT. NHS fundingis allocated to the PCT at a higher than averagerate where the PCT is below target (andconversely, a lower than average rate where thePCT is above target).
Funding is only allocated once residents haveregistered with a GP in a PCT’s area. Revenueallocations are determined on a three-yearrolling basis with a one-year overlap. As aconsequence there is likely to be period when anew population requires health services withoutsufficient funding being available. Someadditional funding can be available to take
account of some of the impact of increasedpopulation (such as Growth Area Adjustment,or ‘GAA’). In the experience of London PCTshowever the additional support does not coverthe extra cost of the newly created need.
Health
Strictly, health refers to the functional mentaland physical condition of an organism. TheWorld Health Organisation defines health in amore aspirational sense as ‘a state of completephysical, mental and social well-being and notmerely the absence of disease or infirmity’.More recently, it has been modified to includethe ability to lead a ‘socially and economicallyproductive life.’
Health Impact Assessment (HIA)
Health Impact Assessment is a method ofestimating the potential health effects of theimplementation of a plan or developmentproposal, which may or may not be aimed atinfluencing the health of the population.
Health inequalities
Health inequalities are variations in health orhealth determinants between differentpopulation groups, and are the result of acomplex and wide-ranging network ofdeterminants. People who experience materialdisadvantage, poor housing, lower educationalattainment, insecure employment orhomelessness are among those more likely tosuffer poorer health outcomes and an earlierdeath compared with the rest of thepopulation. Refer to the London HealthObservatory website (www.lho.org.uk), or yourlocal PCT website for more information onhealth inequalities in your area.
Health needs assessment (HNA)
Health needs assessment is a systematic methodfor reviewing the health issues facing apopulation, leading to agreed priorities andresource allocation that will improve health andreduce inequalities.
Health services
Services offered by the medical and allied healthprofessions for the prevention, treatment, andmanagement of illness and the preservation ofmental and physical well-being.
Generally, health care is divided into thefollowing categories:
Health and Urban Planning Toolkit Glossary and Useful Links

72
• Primary care is the medical care a patientreceives upon first contact with the healthsystem, and before referral elsewhere in thesystem. Primary care services and facilitiestend to be community based, closer topeople’s homes and mainly relate to generalpractice, community care and allied servicessuch as podiatry. Meeting local need for theseservices is the responsibility of a PCT, whichmay commission services for the communityfrom providers like GPs, or provide them itselfin some instances.
• Intermediate care relates to the services andfacilities provided to those not ill enough togo to hospital, but not well enough tomanage on their own at home and may beprovided to people in a community basedsetting or people’s homes. Meeting local needfor these services is the responsibility of a PCT,which may commission services fromproviders, or provide them itself.
• Secondary services and facilities mainly relateto basic surgical procedures undertakenwithin hospitals and in some casesintermediate centres. Meeting local need forthese services is the responsibility of a PCT,which may commission services fromproviders like NHS hospital trusts.
• Tertiary care services and facilities mainlyrelate to more complicated or specialistsurgical procedures such as organ transplantsundertaken within hospitals. Meeting localneed for these services is the responsibility ofa PCT, which may commission services fromproviders like NHS hospital trusts.
• Mental health care services and facilities relateto a range of means to deal with mentalhealth issues such as schizophrenia. Meetinglocal need for these services is theresponsibility of a PCT, which commissionsservices from providers like NHS mental healthtrusts.
Local Delivery Plan (LDP)
A plan that sets out how a PCT intends toachieve key targets and how annual fundingallocations would to be used to achieve thatdelivery.
Local Improvement Finance Trust (LIFT)
LIFT is a government scheme to involve theprivate sector in financing primary and socialcare and community infrastructure. PCTs andLocal Authorities are usually share holders in the LIFT for the local area.
Model of care
A framework that establishes how particularhealth care should be delivered.
Public health
The effort organised to protect the health andwell-being of a whole community. It is also afunction of the NHS, and PCTs at a local level.
Service model
An approach taken to the delivery of healthservices in response to the model of care.
Strategic Services Development Plan (SSDP)
The Strategic Services Development Plan is aplan that sets out the vision of the local LIFT forimproving health services and facilities.
Well-being
Well-being refers to quality of life and a state ofbeing healthy, happy and prosperous.
Wider determinants of health
A range of factors that can affect an individual’shealth including:
• Their age, sex and lifestyle factors• Individual lifestyle factors• Social and community influences• Living and working conditions• General socio-economic, cultural and
environmental conditions
Planning Terms
Development Control
The function of a Local Planning Authoritymainly involved with managing the planningapplication process, whereby it receives andconsiders the merits of a planning applicationand whether it should be given permissionhaving regard to the Development Plan and allother material considerations.
Development Plan
The Development Plan consists of the RegionalSpatial Strategy (or the spatial developmentstrategy for London – the London Plan) and theLocal Development Framework, prepared underthe Planning & Compulsory Purchase Act of2004.
Health and Urban Planning Toolkit Glossary and Useful Links

73
Development Plan Documents (DPDs)
Development Plan Documents are prepared byLocal Planning Authorities and outline the keydevelopment goals of the Local DevelopmentFramework.
Development Plan Documents form an essentialpart of the Local Development Framework andinclude the Core Strategy, Site-specificAllocations of Land and, where needed, AreaAction Plans. There will also be an adoptedproposals map which illustrates the spatialextent of policies that must be prepared andmaintained to accompany all Development PlanDocuments.
All Development Plan Documents must besubject to rigorous procedures of communityinvolvement, consultation and independentexamination, and adopted after receipt of theinspector’s binding report. Once adopted,development control decisions must be made inaccordance with them unless materialconsiderations indicate otherwise.
Environmental Impact Assessment (EIA)
Environmental Impact Assessment is a statutoryrequirement imposed on some large complexdevelopment projects and is a process used toidentify and assess significant environmentalimpacts of a development proposal and ifnecessary suggest alternatives or mitigation toavoid the negative impacts. The findings of anEnvironmental Impact Assessment are set out inthe Environmental Statement. Applicants forcertain types of development, usually moresignificant schemes, are required to submit anEnvironmental Statement accompanying aplanning application. This evaluates the likelyenvironmental impacts of the development,together with an assessment of how theseverity of the impacts could be reduced.
Local Development Framework (LDF)
The Local Development Framework is a portfolioof Local Development Documents whichcontain the policies and proposals for thedevelopment and use of land and is theresponsibility of the Local Planning Authority toprepare. It describes the sort of developmentthat will be permitted in the area and provides abasis for planning decisions. It is required tolook beyond traditional land use considerationsand take into account all factors like health thatmake up a sustainable community. The Local
Development Framework must also act as aspatial expression of the local CommunityStrategy and is central to its delivery. A LocalDevelopment Framework comprises:
• Development Plan Documents (which formpart of the statutory Development Plan)
• Supplementary Planning Documents
The Local Development Framework alsocomprises:
• the Statement of Community Involvement • the Local Development Scheme • the Annual Monitoring Report; and • any Local Development Orders or Simplified
Planning Zones that may have been added
Local Development Scheme
The Local Development Scheme sets out a LocalPlanning Authority’s timetable for theproduction of Local Development Documentsthat make up the Local DevelopmentFramework. It must be agreed with Governmentand reviewed every year.
London Plan
London Plan is the name given to the Mayor’sspatial development strategy for London, andperforms a function similar to a Regional SpatialStrategy required for other regions of England.It forms, together with the Local DevelopmentFramework or Unitary Development Framework,the statutory Development Plan for eachLondon Borough.
Planning appeal
The process whereby a planning applicant canchallenge an adverse decision, including arefusal of permission. Appeals can also be madeagainst the failure of the planning authority toissue a decision within a given time, againstconditions attached to permission, against theissue of an enforcement notice and againstrefusals of listed building and conservation areaconsent.
In England and Wales, appeals are processed bythe Planning Inspectorate.
(Planning Portal 2006)
Planning Application
An application made to the Local PlanningAuthority seeking full permission for adevelopment proposal, with no matters reservedfor later planning approval.
Health and Urban Planning Toolkit Glossary and Useful Links

74
Planning obligations
Legal agreements between a planning authorityand a developer, or undertakings offeredunilaterally by a developer, that ensure thatcertain extra matters related to a developmentare undertaken. For example, the provision ofhighways. Planning obligations are also knownas section 106 agreements, or simply as s106.
Planning contributions
The benefits or safeguards, often forcommunity benefit, secured by way of aplanning obligation as part of a planningapproval and usually provided at the developer’sexpense. For example, affordable housing,community facilities or mitigation measures.Also known as planning gain.
Spatial development
Changes in the distribution of activities in spaceand the linkages between them in terms of theuse and development of land.
(Planning Portal 2006)
Spatial planning
Spatial planning brings together and integratespolicies for the development and use of landwith other policies and programmes whichinfluence the nature of places and how theyfunction. In this way, it goes beyond traditionalland use planning which primarily focused onspecifying what land should be used for.
This should include policies which can impacton land use by influencing the demands on, orneeds for, development, but which are notcapable of being delivered solely or mainlythrough the granting or refusal of planningpermission and which may be implemented byother means.
Statement of Community Involvement (SCI)
The Statement of Community Involvementforms part of the Local DevelopmentFramework and sets out the processes to beused by the local authority in involvingstakeholders in the preparation, alteration andcontinuing review of all Local DevelopmentDocuments and development control decisions.
Strategic Environmental Assessment (SEA)
Strategic Environmental Assessment wasintroduced by European Directive 2001/42/EC(the SEA Directive) and requires a formal
environmental assessment of certain plans andprogrammes, including the Development Plan,which are likely to have significant effects onthe environment (including health). The SEADirective is transposed into UK law by theEnvironmental Assessment of Plans andProgrammes Regulations 2004.
The environmental assessment involves the:
• preparation of an environmental report• carrying out of consultations• taking into account of the environmental
report and the results of the consultations indecision making
• provision of information when the plan orprogramme is adopted
• showing that the results of the environmentassessment have been taken into account
Strategic Environmental Assessment may beundertaken with Sustainability Appraisal as anintegrated process.
Sustainability Appraisal (SA)
An appraisal of the economic, environmentaland social effects, including health, of a planfrom the outset of the preparation process toallow decisions to be made that accord withsustainable development. SustainabilityAppraisal may be undertaken with StrategicEnvironmental Assessment as an integratedprocess.
Unitary Development Plan (UDP)
An old-style Development Plan prepared byLondon Boroughs, superseded by the newDevelopment Plan system. These plans willcontinue to operate for a time after thecommencement of the new Development Plansystem, by virtue of specific transitionalprovisions.
Urban design
The art of making places. It involves the designof buildings, groups of buildings, spaces andlandscapes, in villages, towns and cities, tocreate successful development.
(Planning Portal 2006)
Urban regeneration
Making an urban area develop or grow strongagain through means such as job creation andphysical renewal.
Health and Urban Planning Toolkit Glossary and Useful Links

Acknowledgements
HUDU would like to thank a number of partners for their involvement leading up to thepreparation of this document, including Matrix RCL who prepared the North and SouthWest London Engagement Strategies and the PCTs and Local Planning Authorities thatcontributed to those projects, and the Greenwich TPCT who worked with us on theGreenwich Health Engagement project. More information on the North and South WestLondon Engagement Strategies and the Greenwich Health Engagement Project can befound at www.healthyurbandevelopment.nhs.uk.
Photo on Page 44 courtesy of Stanhope PlcPhoto on Page 57 courtesy of Ballymore Properties LimitedPhotography by Luke Hayes
Health and Urban Planning Toolkit
75
Background on HUDU
This document has been prepared by Neil Blackshaw, Ryan Victa and Tim Chapman. TheNHS London Healthy Urban Development Unit (HUDU) is a specialist unit with a remit acrossLondon to promote better engagement at all levels between the health sector and theplanning sector. It aims to improve health, reduce health inequalities and secure the timelyprovision of modern health services in new communities in London. It is staffed by townplanners and from its inception to March 2007 is funded by the NHS, the Regional PublicHealth Group for London and the London Development Agency. From April 2007 onwardsthe unit will be funded by London PCTs and the London Development Agency.
HUDU Advice and Support
The team is always ready to provide advice and support to PCTs and Local PlanningAuthorities. This could take the form of presentations to key decision makers or involvedirect support to PCTs. This might include addressing the policy framework in the LocalDevelopment Framework or a major development proposal.
HUDU provides PCTs with alerts when new planning documents, policies or majordevelopments are proposed in their area. The tools HUDU has developed including WatchOut for Health, the HUDU s106 Model, the Social Infrastructure Framework and this Toolkitenable PCTs to formulate an effective and focused response and help Borough planners toscope health matters. In appropriate cases HUDU can offer advice on the application of theHUDU s106 model and assist with negotiations to secure new health facilities.
Find out more
Our website – www.healthyurbandevelopment.nhs.uk – provides further background onHUDU, contains downloadable versions of the above tools and the team’s contact phonenumbers and email addresses. Our generic email address is [email protected].
© February 2007

HUDU is supported by the following organisations
Contact details:
W: www.healthyurbandevelopment.nhs.uk
Des
ign:
Po
siti
ve2