Embed Size (px)
Citation preview

Laboratory 3: Heart Anatomy and Blood Vessels Introduction: In this lab we will use a variety of materials to study the structures that support the blood and its circulation through our body. We will examine the anatomy of the heart using a heart model, preserved sheep hearts and a fresh heart from a pig (same size and shape as a human heart). Remember that you are really looking at the same short list of structures in different organisms, the structures of the heart are amazingly similar in all mammals. The second part of the lab will have you identify some of the major histological structures of arteries and veins. The last part of the lab will have you identify the major arteries and veins on the torso model and the female human cadaver.
In order for blood to properly and effectively circulate throughout your body, two things are required: 1) Your heart must pump blood through the blood vessels, and it must do this at the correct volume and correct pressures to meet the needs of the other organs and tissues of your body; and 2) Those blood vessels must distribute that blood to each tissue or organ at the correct volume and pressure, then return it to the heart. All mammals have closed circulatory systems. That is, the blood is completely contained within blood vessels as it flows through the various organs of the body. This blood is under relatively high pressure in arteries, allowing it to flow against gravity and against the resistance which the vessels normally provide as it passes to lower pressure veins before returning to the atria of the heart. The greater that pressure gradient is the greater the potential flow and the movement of blood (which carries oxygen and removes cardbon dioxide) is called perfusion. Since all other tissues, organs, and systems depend on that perfusion to deliver the materials they need and remove waste products they do not need, the circulatory system is one of the most vital systems in the body. Contraction of the heart, called systole, increases the pressure of the blood and provides the propulsive force which moves blood through the blood vessels to perfuse places which have lower pressure. Relaxation of the heart, called diastole, allows its chambers to refill with blood for the next systole and it has a series of one-way valves which ensure that blood flow occurs in only one direction. Each systole followed by a diastole is called a cardiac cycle.
LEARNING OBJECTIVES: Upon completion of this lab exercise, students will be able to: - Describe the position, gross anatomy, and histology of the heart. - Identify the great vessels and their functions in carrying blood into and out of the heart. - Describe the pathway of blood as is moves through the heart, and the roles of its valves. - Describe the coronary circulation which supplies the capillaries of the myocardium. - Describe the histology of blood vessels - Identify many major blood vessels of the human body
PART I: HEART MODELS
Orient yourself to the anterior surface of the heart model by looking for a prominent diagonal groove (e.g., looks like a gun-sight) that is filled with fat and coronary blood vessels. This groove is named the anterior interventricular sulcus. The less prominent posterior interventricular sulcus can be observed on the posterior (back side that faces the vertebrae) aspect of the heart. Next, locate the right and left sides of the heart, but remember to use the heart's frame of
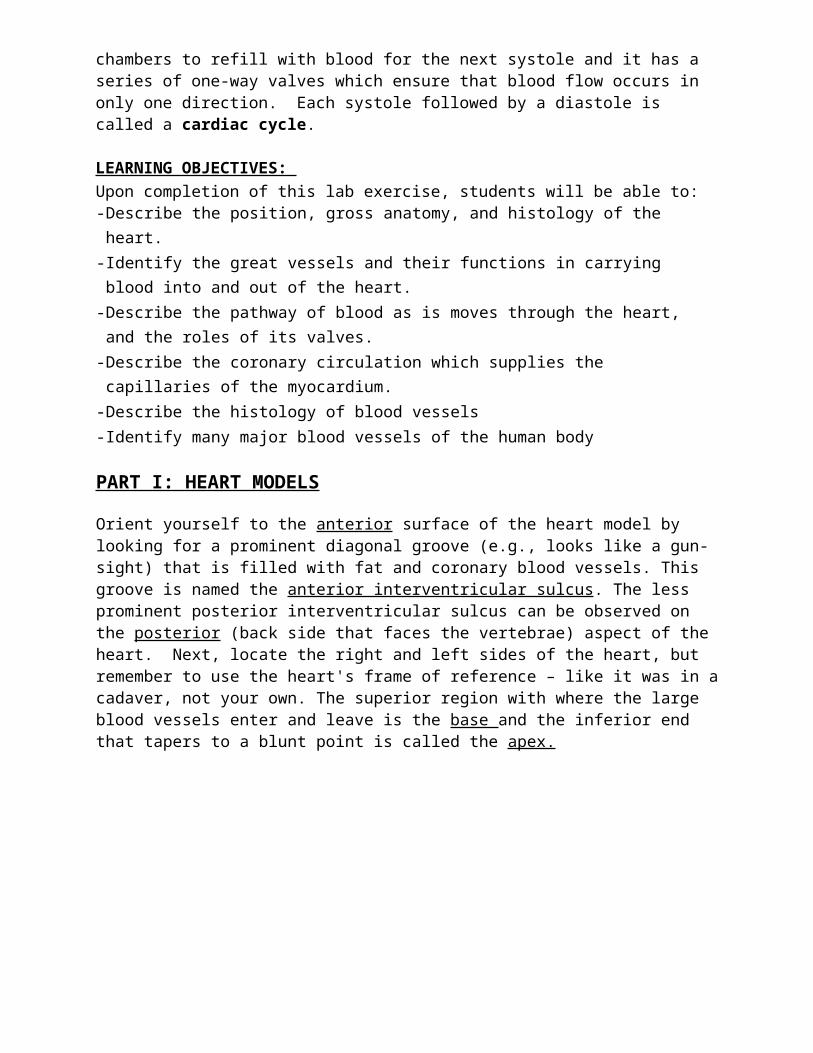
reference – like it was in a cadaver, not your own. The superior region with where the large blood vessels enter and leave is the base and the inferior end that tapers to a blunt point is called the apex.
Now that you know front (i.e., anterior) and back (i.e., posterior) as well as right and left, orient yourself to the heart's internal chambers by way of the external auricles. The right and left auricles are the pink flaps on either side of the upper part of the heart. The auricles got their name, which means "little ear", because they are small ear-shaped appendages of the two upper chambers of the heart, the right and left atria. Remember: the auricles are atrial appendages. Locate the spacious right and left atria (chambers) by opening up the heart model. Inferior to these chambers find the right and left ventricles. The four heart chambers can now be used to locate the valves and great vessels attached to the chambers.
The vessels attached to the right atrium are the large, blue (this color is associated with deoxygenated blood) superior and inferior vena cava. These vessels receive blood from all over the body and deliver it to the right atrium. Find the internal openings of the vena cava on the walls of the right atrium.
Blood from the right atrium (deoxygenated) is pushed by the contraction of the atrium and by the vacuum (negative pressure) from the expansion of the ventricles through a large valve named the right atrio-ventricular valve (i.e., tricuspid), into the right ventricle. (The term tricuspid is being phased out and so you should try and learn the structure by the anatomically correct name.) Blood from the right ventricle must then do a big U-turn to exit from the anterior superior part of the right ventricle. Look on the front piece of the model to find the anterior half of the ventricle. In the anterior, superior part of that chamber, find the point of exit of blood through a three-parted valve named the pulmonary semilunar valve. This valve occurs at the junction between the right ventricle and the pulmonary trunk. The pulmonary trunk is so named because it has not yet split into a right and left half. Locate both parts of the blue pulmonary trunk, reassemble the model, and trace the pulmonary trunk to the point where it splits into the pulmonary arteries. Each pulmonary artery carries blood to one of the lungs where it becomes oxygenated.
Oxygenated blood (bright red in coloration) returns from the lungs to the left atrium through the pulmonary veins. Reopen the heart model. On the inside of the left atrium, find four black-

painted circles representing the openings of the four pulmonary veins. Locate the four red pulmonary vein stubs externally. Two are found on each side of the model corresponding to the right and left sides of the body.
Next, find the left atrio-ventricular valve (i.e., bicuspid) below the left atrium. (Like the tricuspid name, the bicuspid name is being phased out and you should try and learn the structure by the anatomically correct term.) Blood passes through it into the left ventricle. Blood in this chamber must again make a big U-turn to pass through the aortic semilunar valve into the red, curved aorta. Find the aortic semilunar valve and aorta on the back piece of the heart. Blood from the aorta is distributed to all parts of the body through numerous branch arteries.
Note: On the model the color of the vessel indicates whether the blood it contains is oxygenated (red) or deoxygenated (blue), not strictly speaking if it is a vein or an artery.
VALVE PARTS :
The heart models show some features of the heart valves as well. The aortic semilunar valve and pulmonary semilunar valve show three semilunar valve flaps which meet snugly in the middle when closed.
The two atrio-ventricular valves have a more complicated structure. The main closure of the opening between the atrium and ventricle is achieved by the atrio-ventricular valve flaps. There are three main valve flaps (or cusps) on the right side of the heart and two main valve flaps on the left side of the heart and these structures gave rise to the obsolete names tricuspid and bicuspid respectively. The edges of the valve flaps are supported by numerous connective tissue cords called chordae tendinae (tendinous cords). Conical mounds of heart muscle (i.e., papillary muscle) serve as anchors for the chordae tendinae to the ventricle walls. Several of these papillary muscles (finger-like muscles) show up well on this model.
LAYERS:
Three layers make up the wall of the heart. From outside to inside they are named the epicardium, myocardium and endocardium. Start with the appearance of these three layers on the detachable piece of the big heart model. You should then be able to find the layers elsewhere on the model.
All parts of the inside of the heart, including the heart wall, papillary muscles, chordae tendinae and valve flaps, are covered by a thin layer named the endocardium (simple squamous epithelial tissues). Blood inside the heart chambers is actually in contact only with the endocardium. The mission of the endocardium is to prevent inappropriate adhesion of platelets to its surface, this would result in a blood clot (thrombosis). This endothelial layer is continuous throughout the vasculature.
The myocardium of the ventricles is represented on the big heart model by a dark red color – indicative of the color of muscle. On the anterior surface of the heart a square segment (i.e., window) of the myocardium has been removed to show that the myocardium consists of several layers and that the muscle fibers in the different layers run at angles to one another. This provides different planes for contraction. Only the myocardium contains cardiac muscle tissue. (The walls of the atria also have a myocardial layer, but it is not clearly shown on this model.)
The epicardium covers the outer surface of the entire heart and the anterior surface of this piece. It is shown as a rather thin, yellow layer which has been partly cut away. The yellow color
represents adipose tissue which commonly builds up in the epicardium. Another name for the epicardium is the visceral pericardium. This is the connective tissue sac that encloses the heart.
SEPTA (Walls) BETWEEN THE ATRIA AND VENTRICLES
The word septum means "wall" (as in nasal septum) (plural=septa). There are several septa in the heart, the interventricular septum and the interatrial septum. The interventricular septum is, as the name implies, a wall that lies between the two ventricles. To locate it, put a finger in the left ventricle and a thumb in the right ventricle. When you squeeze together, you will be pinching the thick interventricular septum. The other septum, the interatrial septum, occupies a position between the atria. On this model, the aorta occupies the front part of the interatrial septum. Use the thumb and finger method to locate the posterior part of this septum.
A less distinct septa also exists between the right and left atria. During your existence as a fetus, there was a hole in your heart at this location called a Foramen Ovale. Sometimes you can see a small divit (place where the septum is very thin) on the surface of the interatrial septum where this structure used to be (try to find it on the fresh pig heart). In about 80% of the population this hole is sealed. The other 20% of the population is said to have a patent foramen ovale (PFO). Often we do not discover this “hole” until relatively late in life because the heart is very adaptable when you are young, but sometimes can’t keep up with the increased work load as you get older. When you were born a flap of tissue quickly sealed this hole (assuming your heart is healthy), fixing the hole as an adult requires surgery via catheter-based closure, however in many cases the individual would simply be treated with anticoagulants like warfarin (Coumadin) or clopidrogrel (plavix) to prevent the formation of a thromosis within this structure.
CORONARY ARTERIES
The Left Coronary artery (typically larger) and the Right coronary artery (typically smaller) exit the aorta immediately behind the left semilunar valves.
The Right Coronary Artery (RCA) supplies the right ventricle and atrium and crosses the right atrioventricular sulcus and usually becomes the posterior interventricular artery supplying the posterior aspects of the ventricles.
The Left Coronary Artery (LCA) is a short segment that quickly splits into two parts: the anterior interventricular artery and the circumflex branch of the left coronary artery. The Anterior
Interventricular Artery (often called the Left Anterior Descending or LAD) is easy to find in the sulcus along the anterior surface of the heart. The circumflex branch of the left coronary artery delivers blood to the lateral aspects of the left ventricle and is located in a left atrioventricular groove between the atria and ventricles and protected by the epicardial fat that covers it. It is usually the left coronary artery and its branches that create problems with respect to heart attacks because the left side of the ventricle (that they supply) has to generally do more work and needs more perfusion (oxygen) than the right.
The left coronary artery is also often times called the “Widow Maker” by clinicians (in the 21st century perhaps this should be called the ‘single partnerless person maker’). This short vessel supplies blood to both the CIRCUMLFEX AND LAD, and a clot here means the entire anterior aspect of the left ventricle is not delivered with oxygen. As a result the left ventricular tissue dies and pumping into the aorta stops (massive heart attack) and the individual dies. The left anterior descending artery is often where arterial stents (they look like small wire springs) are placed to “open up” a clogged coronary artery because there are a large number of bifurcations where atherosclerotic plaques can accumulate.
The coronary arteries that supply the myocardium with oxygenated blood run along the surface of the epicardium. Smaller arterioles deliver this blood into the myocardium where the capillaries permit gas exchange and delivery of oxygen to the mitochondria of the myocytes. The deoxygenated blood enters veins that travel to the surface of the epicardium. A small amount of deoxygenated venous blood can also drain directly into the chambers of the atria and ventrivles (thespian veins). It is important to remember that blood flow into, out of, or through the myocardial tissue primarily occurs during diastole (heart rest), this is why a high heart rate is especially hard on a weak heart, you just plain don’t supply oxygen if the heart tissue spends too much time in contraction.
When you have cardiac bypass surgery, the cardiologist removes a section of vein from somewhere in your body (often the saphaneous vein in the leg, unless you have varicose veins and have had the saphenous stripped out) and splices the new vessel into and across where the old coronary artery was clogged shut. As a result, oxygenated blood flow is restored to the tissues distal (downstream) to the occlusion and the heart can do more work again.
ELECTRICAL CONDUCTION SYSTEM OF THE HEART (Only on big red heart models)
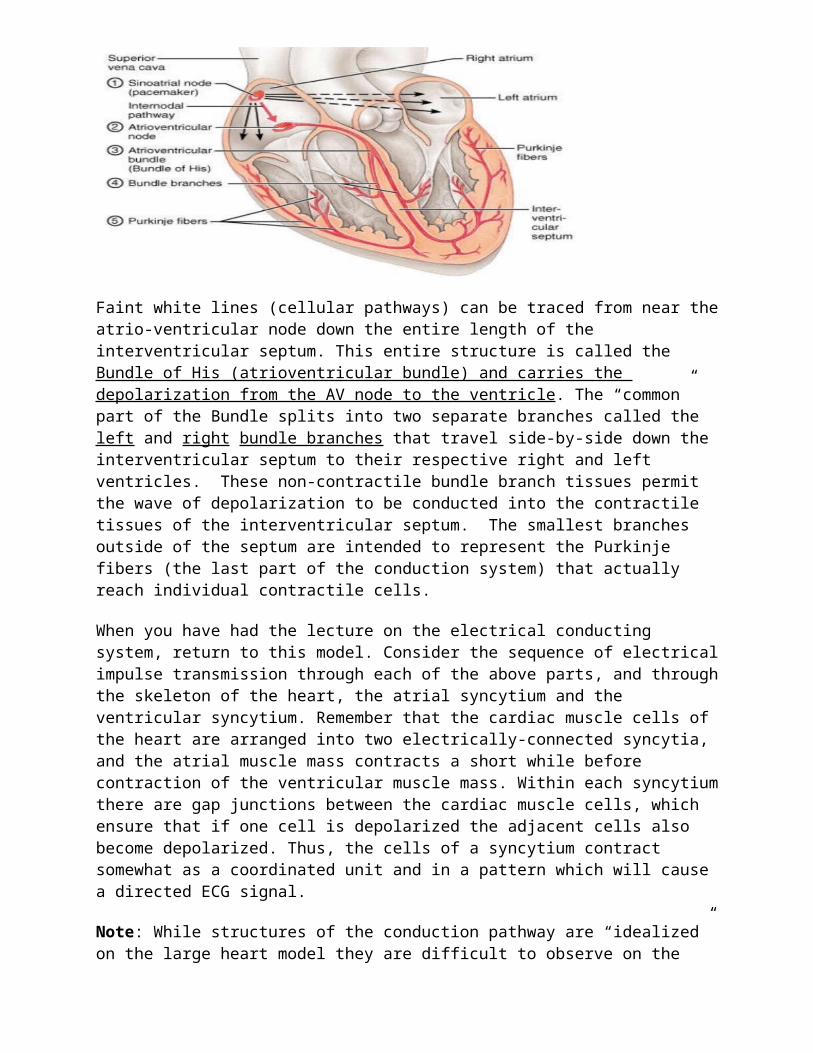
Depolarization and contraction of myocardial tissues occurs along a finely controlled pathway. The electrical conducting system of the heart is a lecture topic that students often find difficult to understand. Try to get a 3-dimensional idea of its structure by studying the big, red heart model (the only model which shows it).The starting point for depolarization that stimulates the heart to contract is the sino-atrial node, commonly called the pacemaker of the heart. This is a patch of cells specialized in generating action potentials. Find this structure, represented in green, at the junction between the superior vena cava and right atrium. The wave of depolarization moves across the atria and simultaneously travels into a second important patch of cells of the conducting system called the atrio-ventricular node, also represented in green. Find this structure on the medial surface of the right atrium.

Faint white lines (cellular pathways) can be traced from near the atrio-ventricular node down the entire length of the interventricular septum. This entire structure is called the Bundle of His (atrioventricular bundle) and carries the depolarization from the AV node to the ventricle. The “common” part of the Bundle splits into two separate branches called the left and right bundle branches that travel side-by-side down the interventricular septum to their respective right and left ventricles. These non-contractile bundle branch tissues permit the wave of depolarization to be conducted into the contractile tissues of the interventricular septum. The smallest branches outside of the septum are intended to represent the Purkinje fibers (the last part of the conduction system) that actually reach individual contractile cells.
When you have had the lecture on the electrical conducting system, return to this model. Consider the sequence of electrical impulse transmission through each of the above parts, and through the skeleton of the heart, the atrial syncytium and the ventricular syncytium. Remember that the cardiac muscle cells of the heart are arranged into two electrically-connected syncytia, and the atrial muscle mass contracts a short while before contraction of the ventricular muscle mass. Within each syncytium there are gap junctions between the cardiac muscle cells, which ensure that if one cell is depolarized the adjacent cells also become depolarized. Thus, the cells of a syncytium contract somewhat as a coordinated unit and in a pattern which will cause a directed ECG signal.
Note: While structures of the conduction pathway are “idealized” on the large heart model they are difficult to observe on the preserved and fresh hearts. The conduction pathway questions on the lab test will be limited to the large plastic heart model.

PART II: PRESERVED SHEEP HEART and FRESH PIG or COW HEART:
Find these same structures on the preserved and fresh hearts. When looking at the fresh heart, try pulling on things and stretching things. See how durable this structure really is! If you over stretch something and it tears, the pig will forgive you. A couple of hearts will be frozen for use on the lab exam later, so do not skip this section thinking there will not be a fresh heart on the lab practical. The material below will help you walk through these structures once again.
Important Tip! Take a metal probe or your finger and move it through the chamber openings. If you put the finger in one opening predict the place where it should reappear. On a test try to be able to identify the structure at the end of the arrow or tip of the pin, but also try to identify the reference structures on either side of what you look at.
Find these external anatomical features: ANTERIOR INTERVENTRICULAR SULCUS - this fat-filled groove passes diagonally across the anterior surface of the heart. It contains branch coronary arteries and veins. Use the anterior interventricular sulcus to locate the anterior surface of the heart. Now you know what is anatomical LEFT and RIGHT on the heart you are looking at! POSTERIOR INTERVENTRICULAR SULCUS - this fat-filled groove is vertical. It occurs on the posterior surface of the heart. CORONARY SULCUS - this groove is usually completely obscured by fat. It circles the heart between the atria and ventricles. Locate the RIGHT AURICLE and LEFT AURICLE - these ear-like flaps are gray in color. They are quite large and distinct on the sheep heart. RIGHT ATRIUM - the large cavity of this chamber of the heart is located posterior and inferior to the right auricle. SUPERIOR VENA CAVA - this vein is a thin-walled vessel which enters the right atrium from above. Locate its opening by probing the superior wall of the right atrium from the inside with your finger. Often both the superior and inferior vena cava will be collapsed. (It is useful to remember that arteries have much thicker walls than veins of the same-sized lumen. Arteries usually retain their shape, while veins often collapse.) INFERIOR VENA CAVA - this vessel is difficult to find on the sheep heart because it adheres closely to the posterior part of the heart. In the sheep heart, it enters the right atrium from the lower medial side. A probe passed through it will make an angle of about 90o with one passed through the superior vena cava. This orientation is quite different from the situation with the human inferior vena cava which is vertical in orientation. With these directions in mind, probe for the opening to this vessel.
Find these Internal Structures: RIGHT ATRIOVENTRICULAR VALVE - this valve lies between the right atrium and right ventricle. The valve consists of valve flaps and chordae tendinae attached to papillary muscles. ATRIO-VENTRICULAR VALVE FLAPS - these thin nearly transparent pieces of tissue meet to close off the opening between the atrium and ventricle to prevent the backflow of blood. CHORDAE TENDINAE - these numerous thin connective tissue cords are attached to the edges of the valve flaps. They prevent valve flap reversal. PAPILLARY MUSCLES - these irregularly shaped mounds of cardiac muscle can be found at various positions on the walls of the ventricle. They serve as passive anchors for the chordae tendinae. They do not act to pull the valve open. PULMONARY TRUNK - the term "trunk" refers to that undivided part of the vessel that splits to form the two main pulmonary arteries. PULMONARY SEMILUNAR VALVE - this valve can be found at the very first part of the pulmonary trunk. It consists of three somewhat shriveled-up, thin valve flaps. Semilunar valves have no chordae tendinae or papillary muscles. From the pulmonary arteries blood flows through branch arteries to the capillaries in the lungs.

Oxygenated blood flows back to the heart via the pulmonary veins. LEFT AURICLE - this flap serves as a landmark for the location of the left atrium. LEFT ATRIUM - this chamber lies posterior to the left auricle. Determine its full extent by probing. PULMONARY VEINS - these vessels are almost always cut off very short when the sheep's lungs are removed. Often only the holes, where they were attached, remain. Locate the stubs of the pulmonary veins or the openings where they were attached to the posterior surface of the left atrium by gently probing the wall of the atrium from the inside. LEFT ATRIOVENTRICULAR VALVE - this valve, like the right atrioventricular valve in structure, can be found between the left atrium and left ventricle. Locate its valve flaps, chordae tendinae and papillary muscles. LEFT VENTRICLE - note the thick myocardial wall of this chamber. The blood from the left ventricle exits by way of the aorta. The connection between the main chamber of the left ventricle and the aorta is difficult to find. Blood passes through the left atrioventricular valve (i.e., bicuspid valve), U-turns and passes behind the medial valve flap to reach the aorta. AORTA - this large, thick-walled vessel extends upward from the central axis of the heart. It arches off to the left and produces one major branch, the brachiocephalic artery. (The human aorta has three major branches off its arch.) AORTIC SEMILUNAR VALVE - this valve is similar in structure to the pulmonary semilunar valve, consisting of three valve flaps. It occurs at the very base of the aorta. SEMILUNAR VALVE FLAPS - the attachment of these thin structures to the wall of the aorta can be easily observed in the aortic semilunar valve. Their structure has been distorted by the preservative.
CHECKLIST OF PARTS OF THE HEART
Base Apex Anterior/Posterior Left/RightAnterior interventricular sulcus
Tricuspid or right atrio-ventricular valve Atrio-ventricular valve flap Circumflex branch of left
coronary artery
Right auricle Pulmonary semilunar valve Chordae tendinae Anterior interventricular artery
Left auricle Pulmonary trunk Papillary muscles Posterior interventricular artery
Right atrium Pulmonary arteries Epicardium or visceral pericardium Sino-atrial node
Left atrium Pulmonary veins Endocardium Atrio-ventricular node
Right ventricle Bicuspid or left atrio-ventricular valve Myocardium Atrio-ventricular bundle
Bundle of HisLeft ventricle Aortic semilunar valve Interventricular septum Rt/Lt Bundle BranchesSuperior vena cava Aorta Interatrial septum Purkinje Fibers
Inferior vena cava Semilunar valve flap Right and left coronary arteries (origin on aorta)
T.Q. Above Bold on Large Heart Model Only!
If you passed a string through the vena cava to the pulmonary artery, could you name all the structures it crosses?If you passed a string through the pulmonary artery to the aorta, could you name all the structures it passes over?TIP: Whenever you pick up a heart, model or other, look for the anterior sulcus (large gunsight-like groove). This will be the anterior aspect of the heart, so now you know the left and right sides. You can also identify where the great vessels enter and leave, this is called the superior end or the “base” and the inferior end called the apex is its opposite.
PART III: ARTERIES AND VEINS OF THE TORSO MODEL
Find these blood vessels on the human torso model. In several places in this lab you will be asked to find the vessel/structure using a figure or table in the book. These figures and structures may appear on the lab exam if they are listed on the “torso” checklist at the end of this lab. Pay special attention to items in bold and italics, these may also appear on test.
ARTERIES: Remove the heart and lungs from the torso model. Find the pulmonary trunk and the pulmonary arteries. They are painted blue to suggest that they carry deoxygenated blood. Replace the heart and notice how short the pulmonary arteries are. Find their major branches in the lungs. If a thrombosis blocked blood from passing through the pulmonary artery, what would happen to the blood pressure in the pulmonary veins, the lung vasculature and the aorta or vena cava?
Next locate the aorta on the heart. A small part of the ascending aorta is visible. Remove the heart and follow the aortic arch on the model. Note that it arches posteriorly and slightly to the left and then begins to descend. Part of the descending thoracic aorta is visible. Note that it passes behind the trachea. The TV movie star John Ritter died in 2004 when an aortic arch aneurism ruptured causing massive hemorrhaging. What would have happened to his blood pressure, blood volume, and heart rate when this occurred?
The three major branches off the aortic arch proper are visible, although somewhat obscured by the brachiocephalic vein. From right to left, these three branches are the: brachiocephalic trunk (artery), left common carotid artery and left subclavian artery. Trace the brachiocephalic artery upward until it splits into the right common carotid artery and the right subclavian artery (there is no left brachiocephalic artery because the left common carotid and left subclavian branch directly off of the aortic arch) which carries blood to the shoulder and arm. Follow both common carotid arteries up the neck. These vessels are called common because they will give rise to an internal and external branch distally. Look carefully and find the path of the left subclavian artery out toward the left shoulder and arm.
Find the diaphragm that divides the peritoneal and thoracic cavities. Remove the abdominal viscera. Find the descending aorta, inferior to the diaphragm it is called the abdominal aorta. Note three stubs of major branch arteries that project anteriorly from it. The upper one, nearest the diaphragm, is the celiac trunk. This vessel supplies blood to the abdominal viscera. Near the renal artery – the one to the kidney, locate the superior mesenteric artery's base. This vessel supplies blood to the small intestines and some of the large intestine. The lowest unpaired vessel is the inferior mesenteric artery. This supplies blood to the distal end of the large intestine. You should have no trouble finding the paired renal arteries to the kidneys. Remember that these two kidneys receive up to about 25% (12.5% each) of the cardiac output when at rest.
Finally, locate the termination of the aorta in the lower peritoneal cavity where it splits to form the right and left common iliac arteries. The common iliac arteries will branch into the internal and external iliac arteries. On the right side, the smaller internal iliac artery (figure 20.27) can be seen along the pelvic wall near the rectum. This vessel provides blood to numerous other arteries including the gluteal, vaginal uterine and middle rectal. The continuation of the common iliac artery below the internal iliac artery is the larger external iliac artery. This artery is called the femoral artery after it exits the peritoneal cavity, this supplies blood to the leg. Assume your leg was amputated at the knee as a result of fiery car crash (or a horrible Anatomy experiment gone bad). Would you want the paramedic to put strong direct pressure over the superior ramus of the pubic bone OR over the lesser sciatic notch of the ischium (please do not try amputation at home or in lab!). Why would you choose this place for applying the pressure to stop the bleeding?
VEINS
Let us begin with the pulmonary veins. On this model they are painted red indicating that the blood they carry from the lungs to the heart is oxygenated. Find the pulmonary branch veins in the lungs. On the heart, inferior to the pulmonary arteries, two left pulmonary veins and four

right pulmonary vein branches are shown. Usually the branches come together to form two main veins that enter the left atrium on each side.
Next, look at the Torso Model and, find the superior vena cava. Trace it upward until it splits into the right and left brachiocephalic veins. They extend laterally as the two very large internal jugular veins. The external jugular veins are not shown on this model. They would typically drain into the superior vena cava just distal to the internal jugular veins. If a person applies light pressure to the surface of the skin to one side of the neck you can often see blood pool in the external jugular vein, if you palpate the skin you can feel the pooled blood inside the vessel. CAUTION: do this at your own risk and do not try this if you are older than 40 years of age or have circulatory disease! Instead, think about what a tight collar on a button up shirt might do and the appearance you might have with respect to this vein?
Lateral to the base of the internal jugular veins, the continuation of the brachiocephalic vein that carries blood from the arm, is the subclavian vein. Note that this vein is actually "beneath the clavicle", as its name implies. Distal to the clavicle this vein is called the axillary vein. Why?
Return to the heart and locate the stub of the inferior vena cava where it is attached to the right atrium. Find the next segment of it as it passes through the liver. The rest of the inferior vena cava can be located to the right of the aorta on the posterior abdominal wall. Trace it to its termination where it splits to form the common iliac veins. By analogy with the arteries of the same name, find the following veins: renal veins, internal iliac veins, external iliac veins and femoral veins.
Blood vessels tend to vasodilate (open-up) in response to local heat and the body has some special tricks it can use to dissipate heat when too warm, or to conserve body heat when exposed to the cold. When excess heat is present the smooth muscle tends to relax and the vessel will dilate allowing blood to enter them and fill distant capillaries. When smooth muscle gets cold it tends to cause the vascular smooth muscle to constrict making it difficult for blood to enter a vessel. The blood draining the regions below the knee have two veins it can take to return to the external iliac and vena cava. The returning blood can travel deep in the leg next to the femur bone through the femoral vein or it can travel just under the surface of the skin of your inner thigh in the saphenous vein.
When you exercise the blood is warm and causes the smooth muscle on the saphenous vein to relax and dilate, making it easy for blood to travel through it. As a result heat can easily radiate out of the superficial saphenous vein warming adjacent tissue and allowing heat transfer from the surface of the skin to the surrounding air. This safely cools the blood before it enters your body’s core. When you are cold, the smooth muscle of the saphenous vein constricts and blood is diverted to the deeper femoral vein. Blood coming from the femoral vein has not lost as much of its warmth, so it is not too cold when it enters the body cavity next to your internal organs. When the saphenous vein is removed for heart bypass, the person will of course be less able to radiate heat when they exercise because all venous blood must return via the femoral vein.
It is possible to find the hepatic portal vein (and some of its branches) on this model and on Figure 20.38. Look on the detachable piece containing the pancreas. On the posterior surface of this piece, the hepatic portal vein is shown in purple. Its continuation is also depicted on the liver near the common bile duct. The hepatic portal vein carries blood that was deoxygenated by the cells of the intestine and abdominal organs, it carries nutrients from the food you ate and may also carry toxins that entered the blood in the gut. The blood is “cleaned up” in the liver prior to delivery by the hepatic veins into the vena cava and the heart proper. The red vessel traveling to the liver from the celiac artery is the hepatic artery. What was the importance of this portal

system? Why does the liver also need a separate system that brings oxygenated blood via the hepatic artery (a branch of the cephalic artery, near diaphragm)? Would the use of blood containing very little oxygen help an important organ function well?
PART IV: BLOOD VESSELS OF THE CADAVER:
Be sure to be able to identify the following blood vessels on the human cadaver. Cadaver Arteries: Aortic Arch, Abdominal Aorta, Renal Arteries, Common Iliac Arteries Common Carotid arteries, and Subclavian arteries. Cadaver Veins: Vena Cava (Inferior/Superior), Common Iliac veins, Femoral Veins, and Saphenous veins.
PART V: HISTOLOGY OF ARTERIES AND VEINS:
The histology of the artery and vein on the artery, vein and nerve slide (Slide #3) was examined last semester and it will now be reviewed again. First, relocate the artery and the vein. Recall that the artery has a much thicker wall than the vein. Also note that the wall of the artery contains lots of smooth muscle tissue (thick walled) , while the vein's wall contains less smooth muscle (thin walled). These differences in anatomy illustrate functional differences in the vessels. You can also find cross sections of nerves traveling along with the artery and nerve in a neurovascular bundle. The nerves are solid structures without a lumen. At 400X (40X objective; 10X ocular) you should be able to see cross sections of nerve fibers which have a dot-like axon in the center of a clear myelin sheath.
Each of these vessels has three layers or "coats" called tunics (See Figure 20.2 Saladin). The names of the three layers are, from inside to outside, the tunica intima, tunica media and tunica externa. Let us study the layers of the artery first. The tunica intima of the artery has two distinctive parts. Next to the blood is the layer of simple squamous epithelial tissue we studied previously. The name given to this layer in an artery or elsewhere in the circulatory system is the endothelium. You will have to look very carefully to see the thin flattened cells of the endothelium. (Remember that they are cut in cross section.)
Beneath the endothelium is the internal elastic membrane. This structure is the distinctly solid and rippled layer that literally looks like a rubber band. Both the endothelium and the elastic membrane are parts of the tunica intima. Together they act to provide a smooth, flexible surface over which blood can flow; the elastic properties let vessels expand and return to original size when receiving a pulse of blood.
The second major layer is the tunica media. In all but the largest (elastic) arteries this layer is made up of circularly arranged smooth muscle tissue. When these smooth muscle cells constrict the lumen (inside open diameter) of a blood vessel decreases. This strong layer must also resist the high pressure of the blood in the artery. It also can contract to help control blood pressure and blood flow.
Name a paracrine messenger that can be created by platelets and could cause constriction of the smooth muscle in an artery. What would this do to the delivery of blood and oxygen to a region of the heart supplied by the artery? In a healthy blood vessel, what cells produce prostacyclin? How would prostacyclin reduce the release of paracrine messengers and constriction? If the endothelium was injured, perhaps due to materials in cigarette smoke, what might the blood vessel do?

Surrounding the tunica media, and often blending into the surrounding tissue, is the tunica externa. This outer layer of the artery consists of loose connective tissue that helps hold the artery in position among surrounding organs. Next, we will compare the structure of the artery to that of a vein.. The tunica intima of the vein has an observable lining of endothelium like the artery but the elastic membrane is usually not visible. The thinner tunica media of the vein contains much dense connective tissue, but relatively little smooth muscle tissue. Finally, the tunica externa of the vein is relatively much thicker than the corresponding layer of the artery. It makes up much of the thickness of the wall of the vein. It probably strengthens the wall of the vein as well as holds the vein in place.
CHECKLIST FOR ARTERIES AND VEINS OF THE TORSO MODEL
Arteries Arteries Veins Veins
Pulmonary trunk Pulmonary arteries Pulmonary veins Superior vena cava
Ascending aorta Aortic arch R&L Brachiocephalic veins Internal jugular veins
Descending thoracic aorta Brachiocephalic artery Subclavian vein Inferior vena cava
Left common carotid artery Left subclavian artery Common iliac veins Renal veins
Right common carotid artery Right subclavian artery Internal iliac veins External iliac veins
Abdominal aorta Celiac trunk Femoral veins Greater saphenous vein
Superior mesenteric artery Inferior mesenteric artery Hepatic portal vein
Renal artery Common iliac artery Portal System
Internal iliac artery External iliac artery Diaphragm (is a muscular sheet between thoracic and peritoneal cavities)
Diaphragm is used as a reference point for names of arteries and veins.
Femoral artery
Checklist for Vessel Histology
Artery (thick wall) Vein (thin wall) Nerve endothelium simple squamous epithelial tissue
elastic membrane tunica intima of A&V tunica media of A&V tunica externa of A&V Endothelial cell
Where are thromboxane, prostacyclin and nitric oxide produced?What do they do to smooth muscle cells?