Embed Size (px)
DESCRIPTION
Heart Failure. Basics.
Citation preview

PHAY2003: Biological Systems and Therapeutics 2
Heart Failure - Summary
Dr Rebecca Lever
Definitions of Heart Failure
Heart failure can be defined as ‘A clinical syndrome that can result from any structural or functional
cardiac disorder that impairs the ability of the ventricle to fill with or eject blood’ (AHA/ACC HF
Guidelines 2001) or, alternatively, ‘An abnormality of cardiac structure or function leading to failure of
the heart to deliver oxygen at a rate commensurate with the requirements of the metabolizing
tissues, despite normal filling pressures (or only at the expense of increased filling pressures)’. (ESC HF
Guidelines 2008).
Taken together, these definitions capture very well the most important points about heart failure, that
any cardiovascular disorder may ultimately lead to ventricular failure, that the failing heart may initially
compensate in order to retain adequate perfusion of organs and tissues and that ultimately the problem
is a failure of the heart to generate a cardiac output sufficient to support a normal level of function.
This latter point is illustrated very well by the increasing level of disability that occurs as heart failure
progresses; the New York Heart Association (NYHA) classification system being commonly used to
‘define’ levels of disease, although it can be seen that clear overlap between classes exists (e.g. II to III or
III to IV), as the descriptions are somewhat subjective.
NYHA Classification
(Adapted from McMurray et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012. European Heart Journal 2012; 33: 1787-1847).
‘Asymptomatic’
‘Mild’
‘Moderate’
‘Severe’

Signs and Symptoms of Heart Failure
The typical signs and symptoms of heart failure can broadly be listed as attributable to left or right
ventricular failure. However, it should be noted that whilst the right ventricle can fail in isolation, as a
result of chronic disease of the lungs and/or pulmonary circulation, right ventricular failure in the vast
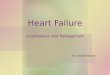
majority of cases is as a result of left ventricular failure. These signs and symptoms, with their origins,
are outlined in the diagram on the next page.
Left ventricular failure leads to fatigue and breathlessness, particularly upon exertion, due to
insufficient perfusion and hence oxygenation of skeletal muscles as the pumping efficiency of the
ventricle declines. Orthopnoea (difficulty in breathing when lying flat) and paroxysmal nocturnal
dyspnoea, whereby the patient wakes suddenly, gasping for air, occur due to the presence of
pulmonary oedema, again as a result of left ventricular failure. When the left ventricle fails as a pump,
it is unable to process its preload effectively, i.e. pump blood that enters during a cardiac cycle into the
systemic arterial system. This leads to an increase in pressure in the left side of the heart that is
transmitted back into the pulmonary veins that feed into the left atrium, and hence the pulmonary
circulation in general. This leads to leakage of fluid out of pulmonary capillaries into the airspaces and
surrounding tissues of the lung, which reduces the efficiency of gas exchange and increases the work of
breathing. The effects are worsened when the patient lies flat because the redistribution of fluid due to
gravity increases the central venous pressure which further increases the preload that the failing heart
cannot process. It is common for patients with poorly managed heart failure to sleep propped up by
pillows to avoid this effect. Signs of left ventricular failure, which tend not to be apparent until function
is significantly impaired, may include cardiac murmurs due to valve dysfunction (e.g. mitral
regurgitation, whereby some blood is ejected back through the mitral valve to the left atrium during
ventricular systole, as a result of pressure overload in the ventricle), or chaotic movement of blood
during ventricular filling (a third heart sound, sometimes called a gallop rhythm). An echocardiogram
may reveal an increased ventricular mass (hypertrophy, initially a compensatory mechanism) or in the
later stages ventricular dilatation due to chronic pressure overload. The heart rate may be increased in
an attempt to increase cardiac output (discussed later). Pulmonary crepitations (known as rales) may be
heard on auscultation of the lungs (listening through a stethoscope), as a result of pulmonary oedema
(fluid-filled alveoli snapping open when breathing in), and pulmonary oedema may also be seen on a
chest X-ray.
Ongoing increased pressure in the pulmonary circulation increases the afterload of the right ventricle
and will eventually lead to its failure (just as the left ventricle may fail as a result of chronic, unmanaged,
systemic hypertension). The right ventricle is particularly susceptible to damage in this way because it is
not used to pumping into a high pressure system (normal mean pulmonary arterial pressure is in the
order of 15 mmHg). Failure of the right ventricle to process its preload will lead to increased pressure
that will transmit back into the vena cava and the systemic venous circulation in general. Signs will arise
that are secondary to venous congestion and include increased jugular venous pressure (JVP), which
may present as a visible distension of the jugular vein in the neck of the patient, hepatomegaly (increase
in the size of the liver), hepatojugular reflux (pressing over the liver causes a prolonged distension of
the jugular vein, due to redistribution of venous overload) and peripheral oedema. The

Ph
ysic
al s
ign
s:ju
gula
r (v
eno
us)
dis
ten
tio
nd
epen
den
t (p
itti
ng)
oe
de
ma
accu
mu
lati
on
of
abd
om
inal
flu
id (
asci
tes)
hep
ato
meg
aly
hep
ato
jugu
lar
refl
ux
Ph
ysic
al s
ign
s:(n
ot
pro
min
ent
un
til l
ater
sta
ges)
enla
rgem
ent
of
the
hea
rtm
itra
l reg
urg
itat
ion
pu
lmo
nar
y o
ed
em
a
Ch
ron
ic lu
ng
dis
eas
ele
adin
g to
incr
ease
dp
ulm
on
ary
resi
stan
ce
Biv
entr
icu
lar
(co
nge
stiv
e)h
eart
fai
lure
Sym
pto
ms:
fati
gue
exer
tio
nal
dys
pn
oe
ao
rth
op
no
ea
no
ctu
rnal
dys
pn
oea
Sym
pto
ms:
fati
gue
bre
ath
less
nes
ssw
olle
n a
nkl
es
Isch
aem
icC
hro
nic
hea
rtsy
stem
icd
ise
ase
hyp
erte
nsi
on
Left
ven
tric
ula
rfa
ilure
Oth
erC
VS
pat
ho
logy
Rig
ht
ven
tric
ula
rfa
ilure
incr
ease
dp
ulm
on
ary
resi
stan
ce
Ori
gin
s o
f th
e K
ey S
ign
s a
nd
Sym
pto
ms
of
Hea
rt F
ail
ure

latter will commonly present as dependent, or ‘pitting’ oedema (if it is pressed with e.g. a finger, an
indentation will be apparent after the pressure is removed) of the ankles and wrists in a patient who is
mobile, or the sacral area in a patient who is bed-bound. Ascites (accumulation of fluid in the peritoneal
cavity, leading to the appearance of abdominal distension) can also sometimes occur.
Biventricular heart failure, i.e. failure of the right ventricle secondary to failure of the left ventricle, is
commonly known as congestive heart failure – it is due to congestion of the normal movement of blood
through the cardiovascular system.
Heart failure is sometimes referred to as being systolic or diastolic in nature. Broadly speaking, these
definitions are used to indicate whether the main problem is with emptying (systolic) or filling (diastolic)
of the ventricle but have been replaced with more precise definitions that reference the ejection
fraction. The ejection fraction is simply the stroke volume divided by the end diastolic volume and
gives an indication of the ability of the ventricle to work as a pump, i.e. to eject the blood that enters
during diastole. In a healthy individual at rest, the ejection fraction is around 70%. However, in ‘systolic
failure’ this would be below 35% and correlates inversely with prognosis. This type of heart failure is
now referred to as heart failure with reduced ejection fraction (HFrEF). Conversely, ‘diastolic failure’ is
now referred to as heart failure with preserved ejection fraction (HFpEF), whereby the ejection fraction
would be greater than 35-55% (precise figure varies) and is often associated with left ventricular wall
thickening (hypertrophy). In practice, most patients with HFpEF can be demonstrated to have at least
mild systolic dysfunction as well and treatment approaches are the same.
Pathophysiology
Over time, a number of physical changes occur within the failing myocardium, many of which are
initially protective or compensatory mechanisms in response to the increases in pressure and/or cardiac
workload, but which are ultimately detrimental. Structural changes to cardiac myocytes include
hypertrophy, changes in energy utilisation, alterations in the relationship between action potential and
contraction, and ultimately cell death. However, structural changes also involve the blood vessels and
interstitium of the heart, which also contribute to the loss of function of the myocardium as an effective
pump.
However, a key feature in the progression of heart failure, which is also the major target of
pharmacological therapy, is activation of the renin-angiotensin-aldosterone system (RAAS) and
sympathetic nervous system, collectively referred to as neurohormonal activation. As the heart fails,
renal perfusion will be compromised as a result of the declining cardiac output and the RAAS will be
activated as though the blood volume had dropped. Hence, sodium and water will be retained and
peripheral resistance will increase, which only worsen the situation by increasing both preload and
afterload. Peripheral vascular resistance will further increase and heart rate will tend to increase as a
result of increased sympathetic activity; the limited cardiac output is ‘allocated’ in favour of e.g. the
central nervous system by a reduction in the perfusion of less vital organs such as the skin and skeletal
muscle, leading to symptoms of fatigue and exercise intolerance. However, this also worsens the
situation as ventricular workload increases as a result of enhanced 1 receptor stimulation by

catecholamines and the increased afterload due to widespread vasoconstriction of small arteries in e.g.
skin and muscle. This vicious cycle continues and the heart becomes progressively less able to
compensate.
Pharmacological Treatment of Heart Failure
The aims of treatment are to 1) increase survival, through reduction of neurohormonal changes and
progression of the disease (remodelling) and 2) improve quality of life by increasing exercise capacity
and reducing symptoms. All patients, unless there are clear contraindications, should be treated with an
ACE inhibitor and a beta blocker licensed for heart failure and the majority will also require treatment
with a diuretic. Additional therapeutic agents may be added, which include digoxin, aldosterone
receptor antagonists, angiotensin receptor antagonists and other agents such as ivabradine,
hydralazine with isosorbide dinitrate and anticoagulants in selected patients.
Diuretics
Diuretics are indicated in all stages of symptomatic heart failure where there are signs of fluid retention
(e.g. peripheral oedema, dyspnoea and/or lung rales associated with pulmonary oedema, jugular venous
distension, hepatomegaly). Diuretics are essential for the control of symptoms secondary to fluid
retention and symptomatic benefits are achieved quickly, within hours or days as opposed to weeks or
months for other therapies used in heart failure. Whilst diuretics themselves have no direct effect on
survival, their appropriate use influences the success of other therapies that do improve survival (e.g.
beta blockers cannot be started if signs of fluid overload are present).
Thiazide diuretics such as bendroflumethiazide act in the proximal portion of the distal convoluted
tubule and inhibit the Na+/Cl- symporter. Less than 10% of filtered sodium is reabsorbed here (i.e. the
vast majority of that originally filtered at the glomerulus has already been reabsorbed), hence these
agents contribute only a moderate degree of diuresis. They also possess some direct vasodilator
activity (probably due to activation of large conductance calcium-activated potassium channels (BKCa) in
vascular smooth muscle). Loop agents such as furosemide are more potent diuretics than thiazides and
lead to secretion of up to 25% of the sodium filtered at the glomerulus. These agents act in the thick
ascending limb of the loop of Henle, where the Na+/K+/2Cl- symporter in the apical membrane is
inhibited. This reduces the accumulation of ions in the medullary interstitium. As the thick ascending
loop is water impermeable, concentration of ions in the interstitium in the absence of water increases
osmotic pressure which drives the reabsorption of water from the collecting duct (under the influence
of vasopressin). Loop diuretics hence reduce this reabsorption, causing diuresis. They have an indirect
vasodilator effect and are particularly useful in reducing the symptoms associated with pulmonary
oedema. Thiazide and loop diuretics both have the potential to cause hypokalaemia and the potassium-
sparing diuretic amiloride is sometimes given alongside drugs such as bendroflumethiazide or
furosemide, if they are used e.g. in the treatment of hypertension, to prevent this. However, patients

being treated for heart failure will almost certainly be receiving at least one other drug that promotes
potassium retention (e.g. ACE inhibitor, angiotensin receptor antagonist, aldosterone receptor
antagonist) so additional measures are not usually required. However, the monitoring of potassium
levels in patients undergoing treatment for heart failure, especially in the initial stages, is sensible.
ACE Inhibitors
ACE inhibitors such as enalapril, lisinopril, ramipril are extremely useful in the management of heart
failure because, like diuretics, they improve symptoms but, unlike diuretics, they also prolong survival
and reduce the rate of progression of the disease. They are indicated in all stages of symptomatic heart
failure, although benefit has also been demonstrated in early, asymptomatic disease. The benefits of
ACE inhibitors in terms of disease progression and survival are at least in part due to their ability to
delay further remodelling of the myocardium and possibly induce a degree of ‘reverse remodelling’, i.e.
repair of changes that have already occurred. ACE inhibitors break the cycle of inappropriate and
detrimental activation of the RAAS, which leads to an improvement in symptoms and an increase in
cardiac output as salt and water retention and vasoconstriction are reduced. Effects on remodelling are
due to inhibition of negative effects of angiotensin II on cardiac myocytes (proliferation, fibrosis,
oxidative stress) and also to indirect inhibition of the negative effects of aldosterone on the heart (see
later). The patient would be started on a low dose of drug which would be increased gradually towards
a maintenance dose. Angiotensin receptor antagonists such as losartan and valsartan may be used as
an alternative in patients who cannot tolerate ACE inhibitors e.g. due to dry cough. An angiotensin
receptor antagonist may also be added on as second line therapy in patients already receiving optimum
therapy with a beta blocker and an ACE inhibitor in whom symptoms are not fully controlled. However,
ACE inhibitors are preferred as first-line agents because their positive effects on survival are better
documented.
Beta Blockers
Beta receptor antagonists should be offered to all patients with left ventricular systolic dysfunction. The
patient must be stable before starting treatment, with no physical evidence of fluid retention. For this
reason, most patients will already be on a diuretic and it is conventional to start and stabilise patients on
an ACE inhibitor first also. The only absolute contraindications for the use of beta blockers in heart
failure are reactive airways disease (i.e. asthma) and atrio-ventricular block. Over the long term, beta
blockers lead to an improvement in symptoms, and also prolong survival, although patients will initially
feel worse due to the negative inotropic effects of the drug. For this reason, a very low dose is used to
begin with which is titrated up towards a target dose, as far as the patient may tolerate the increases.
Beta blockers slow disease progression, reduce further remodelling and, like ACE inhibitors, may to an
extent reverse some of the remodelling that has already occurred. The specific agents that are licensed
in the UK for heart failure are bisoprolol, carvedilol and nebivolol, the latter for use in patients of 70
years or older. The positive effects of beta blockers are due in part to their anti-ischaemic, anti-
hypertensive and anti-arrhythmic properties, which tie in with their uses in other indications, but also

are due to anti-oxidant and anti-proliferative properties that reduce cardiac damage and remodelling.
Furthermore, in heart failure there are detrimental changes to the expression profile of cardiac beta-
adrenoceptors and long-term use of beta blockers can help to correct this.
Digoxin
Digoxin is added to therapy as a second line treatment in patients who remain symptomatic despite
optimum treatment with diuretics, ACE inhibitors and beta blockers. Digoxin is a positive inotrope,
which works by indirectly increasing intracellular [Ca2+] through inhibition of the Na+/K+-ATPase. It
improves symptoms but does not have any effect on survival or disease progression. Digoxin also
promotes a degree of sodium excretion and tends to improve neurohormonal control.
Aldosterone receptor antagonists
Aldosterone receptor antagonists have a significant positive effect on survival. They are added to
therapy as second line treatment in patients who remain symptomatic despite optimum treatment with
diuretics, ACE inhibitors and beta blockers. Spironolactone is the most commonly used example and
eplerenone is a newer and more selective agent that lacks the effects of spironolactone at other
hormone receptors and thus causes fewer side-effects. Aldosterone causes a range of detrimental
effects that promote disease progression in heart failure, including myocardial fibrosis, endothelial cell
dysfunction and baroreceptor dysfunction, which these drugs inhibit. Spironolactone is traditionally
known as a potassium-sparing diuretic. However, it is a very weak diuretic and is not used in this
setting for that specific property, not least because the majority of patients will already be treated with
a stronger loop or thiazide agent. However, the potassium-sparing effects of aldosterone receptor
antagonists should be borne in mind in relation to all other drugs that the patient is taking that might
also affect potassium levels; i.e. diuretics (promote loss), ACE inhibitors (promote retention) and
angiotensin receptor antagonists (promote retention). Importantly, both aldosterone receptor
antagonists and angiotensin receptor antagonists can be used as add-on therapy in patients who are
receiving an ACE inhibitor, but not both at the same time for this reason.