Embed Size (px)
Citation preview

Heart Failure and Sleep Apnea: Heart Failure and Sleep Apnea: Managing Our Patients During Managing Our Patients During
SleepSleep
John L. Tan, MD, PhDHeart Failure Program at the
North Texas Heart Center
Presbyterian Hospital of Dallas

Case Vignette: Initial Presentation
WM is a 71 y/o Caucasian preacher who initially presented with a prolonged episode of chest pain.
He was found to have “tombstone” ST-elevations in the anterior leads.
Taken emergently to cath and had a stent placed in an acutely occluded LAD at its ostium.
Subsequent prolonged CCU stay in cardiogenic shock.
Ultimately improved and discharged after a long stay in the skilled nursing unit.

Case Vignette: Subsequent Care
At home, symptomatically in NYHA Class III-IV heart failure. He had lost significant muscle mass with a BMI of 20.3 kg/m2.
Up-titration of meds (ARB-II B, -B) limited by symptomatic hypotension. QRS of normal duration.
Recurrent hospitalizations due to congestive heart failure, profound fatigue, and hypotension.
Noted to have crescendo-decrescendo sequences of hyperventilation and apnea as well as loud snoring.

Case Vignette: Questions
Does this patient have sleep apnea syndrome?
What is the significance, if any, of his disordered breathing during sleep, especially in the context of his heart failure?
Does this patient warrant further evaluation such as a sleep study?
Is there any value in treating this patient’s disordered breathing during sleep?

Definitions: Sleep Apnea
• Repetitive episodes of decreased or total cessation of respiratory airflow during sleep.
• Leading to fall in oxygen saturation of at least 4% and sleep fragmentation.
• Associated with loud snoring, restless sleep, nocturnal dyspnea, morning headaches, and excessive daytime sleepiness.

Definitions: Sleep Apnea
Obstructive (OSA):
Central (CSA): (Cheyne-Stokes)
Caused by upper airway collapse during inspiration and is accompanied by strenuous breathing efforts.
Characterized by apneas due to diminution or cessation of thoraco-abdominal respiratory movements secondary to dysfunction of central respiratory control mechanisms.

Obstructive and Central Sleep Apnea
Rib cage and abdominal movements are in opposite directions as a result of attempts to breathe against a closed airway.
No respiratory effort is seen during apnea.
Drazen. NEJM. 2002. 346:390.Both disturb normal sleep.

Normal Sleep: Cardiovascular Effects
• NREM sleep , which constitutes ~85% of total sleep time, is a state of cardiovascular relaxation.
• In NREM sleep, metabolic rate, SNS activity, HR, CO, and SVR all decrease.
• There are intermittent surges in SNS activity, HR and BP in REM sleep but average BP and HR remain below waking levels.

OSA: Cardiovascular Effects
Bradley and Floras. Circulation. 2003. 107(12):1671.

CSA: Cardiovascular Effects
Bradley and Floras. Circulation. 2003 107(13):1822.

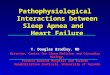
Myocardial InjuryMyocardial Injury Fall in LV performanceFall in LV performance
Activation of RAAS, SNS, ET,Activation of RAAS, SNS, ET,and othersand others
Myocardial toxicityMyocardial toxicity Peripheral vasoconstrictionPeripheral vasoconstrictionHemodynamic alterationsHemodynamic alterations
Remodeling andRemodeling andprogressiveprogressive
worsening ofworsening ofLV functionLV function Heart failureHeart failure
symptomssymptomsMorbidityMorbidity
and mortalityand mortality
ANPANPBNPBNP
-
-
Heart Failure PathophysiologyHeart Failure Pathophysiology

Mechanisms of CV Effects
Quan and Gersh. Circulation. 2004. 109(8):951.

Sleep Apnea: CV Associations
• Systemic hypertension
• Pulmonary hypertension
• Myocardial infarction
• Stroke
• Arrhythmias (PVB’s, atrial fibrillation)
• Heart Failure

OSA in Heart Failure
• OSA is an independent risk factor for HF: the presence of OSA confers a 2.4 fold relative increase in the likelihood of having HF, independent of other known risk factors. (Shahar et al. Am J Respir Crit Care Med. 2001. 163:19.)
• OSA is common in HF patients: OSA is detected in 11-37% of HF patients.
(Sin et al. Am J Respir Crit Care Med. 1999. 160:1101.; Javaheri et al. Circulation.
1998. 97:2154.)

CPAP: Treating OSA in HF
Tkacova et al. Circulation. 1998. 98:2269.

CV Effects of CPAP in OSA/HF
Kaneko et al. NEJM. 2003. 348:1233.

Treating OSA: Improved LVEF
Kaneko et al. NEJM. 2003. 348:1233. EF increased from 25+/-3 to 34+/-2.EF 9+/-2 vs 2+/-2

Treating OSA: Decreased LVESD
Kaneko et al. NEJM. 2003. 348:1233.

CSA in Heart Failure
• Unlike OSA, CSA likely arises secondarily to heart failure.
• CSA is common in HF: CSA seen in 33-40% of HF patients but is rarely seen in the general population.
(Sin et al. Am J Respir Crit Care Med. 1999. 160:1101.; Javaheri et al.
Circulation. 1998. 97:2154.)

CSA in Heart Failure
Bradley and Floras. Circulation. 2003 107(13):1822.

Enhanced Sensitivity to Carbon Dioxide in HF Patients with CSA
Javaheri. NEJM. 1999. 341:949.
Hyperventilatory response during sleep may lower carbon dioxide levels to below the apneic threshold

Significance of CSA in HF
• CSA in HF patients is associated with increased mortality: CSA is an independent risk factor for death or cardiac trans-plantation in multivariate analyses. (Lanfranchi et al. Circulation. 1999. 99:1435.; Sin et al. Circulation. 2000.
102:61.)

CSA as Prognostic Indicator in HF
Sin et al. Circulation. 2000. 102:61.

CSA in HF Progression
• Unlike OSA, no negative intrathoracic pressure is generated in CSA: limited impact of increased afterload.
• However, there is neurohormonal activation: HF patients with CSA have norepinephrine levels elevated in proportion to their degree of apnea-related hypoxia. (Naughton et al. Am J Respir Crit Care Med. 1995. 152:473.)

Treating CSA: Improved LVEF
Sin et al. Circulation. 2000. 102:61.

Treating CSA: Improved Survival
Sin et al. Circulation. 2000. 102:61. RR reduction 81%

Case Vignette: Questions
Does this patient have sleep apnea syndrome?
What is the significance, if any, of his disordered breathing during sleep, especially in the context of his heart failure?
Does this patient warrant further evaluation such as a sleep study?
Is there any value in treating this patient’s disordered breathing during sleep?

Case Vignette: Polysomnogram
The patient underwent a sleep study with the following findings:
Sleep efficiency reduced at 78% (Normal >90).Stage 1 sleep increased at 75% of total sleep time.No deep Stages 3/4 sleep.REM sleep reduced at 8.2% of total sleep time.
Total apnea/hypopnea index high at 44.5 per sleep hour.Both obstructive and central sleep apnea were present.Oxygen saturation fell to as low as 78.7%.

Case Vignette: Follow up
The patient was prescribed CPAP.
With this, his fatigue significantly improved.
Symptomatically he is now in NYHA Class II-III though he still has orthostatic hypotension.
He has had no further hospitalizations.
His ejection fraction has yet to be re-evaluated.

HF and Sleep Apnea: Conclusions
• There is growing evidence of the long-term consequences of sleep apnea on CV disease in general and heart failure in particular.
• Given this, our focus on the evaluation and management of chronic heart failure in the awake state may need to be broadened to include the implications of sleep-disordered breathing on the pathophysiology and progression of heart failure.