Embed Size (px)
Citation preview

Heart 1996;76:50-55
Neuroendocrine response to standing and mildexercise in patients with untreated severe
congestive heart failure and chronic constrictivepericardit'is
Roberto Ferrari, Inder S Anand, Claudio Ceconi, Federica De Giuli,Philip A Poole-Wilson, Peter Harris
AbstractObjectives-Plasma hormones at rest inpatients with untreated severe congestivecardiac failure are similar to those occur-ring during heavy exercise in healthy peo-ple. This study examines the hypothesisthat the neuroendocrine effects of exer-cise are modified in untreated congestivecardiac failure.Design-The effect of lying, standing,upright exercise, and recovery on severalplasma hormones was measured inhealthy controls and 2 groups of patientswith severe untreated heart failure. Thelevel of exercise was the same in allgroups and low enough to be within thecapacity ofpatients with severe failure.Patients-There were 12 healthy controls,9 patients with untreated severe conges-tive cardiac failure caused by myocardialdisease, and 12 patients with untreatedconstrictive pericarditis.Setting-A tertiary referral centre inNorth India.Results-Heart rate, noradrenaline, reninactivity, aldosterone, cortisol, growthhormone and atrial natriuretic peptide(ANP) were higher in the 2 groups ofpatients than in the healthy controls dur-ing both rest and exercise (P < 0 01 forboth comparisons). In general, the effectsof this mild degree of exercise were nogreater than those of standing. Theincrease in heart rate during exercise wasgreater in the group with constrictivepericarditis than in the controls (P =0.04) and (non-significantly) in congestiveheart failure. Apart from these differ-ences the pattern of responses to standingand exercise was similar in the threegroups.Conclusions-While there was evidence ofa broad neuroendocrine activation inpatients with congestive cardiac failure,the only abnormal increase during exer-cise (of marginal significance) was foundfor renin activity in those with myocardialdisease. In patients with untreated con-gestive failure, a substantially normalendocrine response to exercise was super-imposed on abnormal resting concentra-tions.
(Heart 1996;76:50-55)
Keywords: congestive heart failure, neuroendocrineresponse, constrictive pericarditis, exercise.
The severity of congestive cardiac failure isusually graded according to the symptomsreported by the patients and to the amount ofphysical activity that is associated with dysp-noea and fatigue. Thus exercise testing hasassumed a position of importance in the objec-tive assessment of such patients. In overtuntreated congestive cardiac failure or chronicconstrictive pericarditis there is an activationof the neuroendocrine system at rest.1 2 Theneurohumoral response to exercise in healthypeople is in many ways similar to that in con-gestive cardiac failure3-5 and it would not besurprising if the response to exercise weremore intense in cardiac patients. This thesishas not, however, been proved; partly becauseof the rarity with which patients with severecongestive cardiac failure are referred to hospi-tal without previous treatment, and partlybecause of the difficulty in matching theresponse to exercise in healthy people with thevery limited capacity for exercise of cardiacpatients.
Francis et al found that, compared withhealthy people, patients with moderatedegrees of congestive cardiac failure had anabnormally large increase in plasma noradren-aline during exercise for an equivalent increasein oxygen uptake.6 Kirlin et al7 on the otherhand, did not find an abnormally largeincrease in plasma noradrenaline duringequivalent levels of exercise in patients withmoderately severe cardiac failure. Exercisenormally increases plasma renin activity,4 butit is not certain whether this response isincreased in congestive cardiac failure. In astudy of untreated patients with mild conges-tive cardiac failure, Bayliss et al found thatplasma renin activity increased significantlyduring exercise but remained within normallimits.8 Plasma concentrations of several otherhormones are increased during exercise,including vasopressin, aldosterone, andgrowth hormone,4 but we do not knowwhether this response is modified in conges-tive heart failure.We measured plasma adrenaline, noradrena-
line, renin activity, aldosterone, vasopressin,cortisol, growth hormone, prolactin, and atrialnatriuretic peptide (ANP). We used the samelevel of gentle exercise to compare responsesin healthy controls with those in patients with
Cattedra diCardiologia,Universita di Brescia,Brescia, ItalyR FerrariC CeconiF De GiuliDivision ofCardiovascularMedicine, UniversityofMinnesota MedicalSchool, VeteransAdministrationMedical Center,Minneapolis,Minnesota, USAI S AnandNational Heart & LungInstitute, LondonP A Poole-WilsonP HarrisCorrespondence to:Dr I S Anand, Professor ofMedicine, University ofMinnesota Medical School,VA Medical Center 111 C,One Veterans Drive,Minneapolis MN 55417,USA.Accepted for publication22 November 1995
50
on Septem
ber 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.76.1.50 on 1 July 1996. Dow
nloaded from

Neuroendocrine response to standing and mild exercise in patients with untreated severe congestive heartfailure and chronic constrictive pericarditis 51
severe congestive cardiac failure that had neverbeen treated.We did not investigate the effectof maximal exercise but instead we studied alevel of exercise that was likely to be within thelimited range of these very ill patients.9 In thisway, we compared a group of healthy controlswith a group of untreated patients withoedema caused by severe myocardial diseaseand a group of untreated patients with oedemacaused by chronic constrictive pericarditis.
Because the initiation of exercise is oftenaccompanied by a change in posture, we alsoseparately studied the effects of rising from arecumbent to an upright position.
Patients and methodsPATIENTSThe studies were carried out on 12 healthycontrols, nine patients with severe untreatedcongestive cardiac failure, and 12 patients withuntreated constrictive pericarditis. Written,informed consent was obtained from thepatients and the volunteers. The experimentalprotocol was approved by the hospital ethicscommittee. All studies were carried out at thePostgraduate Institute of Medical Educationand Research, Chandigarh, India. Hormoneconcentrations were measured in Brescia,Italy. The haemodynamic, body fluid com-partment, and plasma hormone data on someof these patients at rest has been reported else-where.1 2
HEALTHY CONTROLSThe mean (SEM) age of the healthy controlswas 32 (9-2) years. They were all men. Nonewas in a state of athletic training. Extracellularvolume was 227 (13) ml/kg and total bodyexchangeable sodium 45 (1 9) mmol/kg.
MYOCARDIAL DISEASEThe cause of congestive cardiac failure wasischaemic heart disease in two patients andidiopathic dilated cardiomyopathy in sevenpatients. The diagnosis was established by car-diac catheterisation. There were four men andfive women, aged 43 (5-1) years. The meanduration of the symptoms was 8 (0 5) months.All were short of breath (mean New YorkHeart Association class 3X5 (0-3)). All hadoedema of the ankles, raised jugular venouspressure, and enlargement of the liver. Signsof ascites were present in five patients. Themean cardiothoracic ratio was 66 (0 6). Themean right atrial pressure was 13 (1 9) mmHg and the pulmonary wedge pressure was 28(2 3) mm Hg. The cardiac index was 1-7 (0 2)1/min/m2. The left ventricular ejection fractionwas 30 5 (1X1)%. Extracellular volume was296 (28) ml/kg and total body exchangeablesodium 60 (4-2) mmol/kg. None of thepatients had ever received any form of treat-ment for cardiac failure.
CONSTRICTIVE PERICARDITISThe probable cause of constrictive pericarditiswas tuberculosis, but this was confirmed bybacteriology in only eight patients. The meanage of this group of patients was 29 (3.4) years
and the mean duration of the symptoms was8'3 (1-3) months. There were ten males andtwo females. All were short of breath (meanNew York Heart Association class 2-9 (02)).All had oedema of the ankles, increased jugularvenous pressure, hepatic enlargement and,with the exception of one patient, ascites. Themean cardiothoracic ratio was 0 50 (0 02).The mean right atrial pressure was 20 (1 7)mm Hg and the pulmonary wedge pressure 23(14) mm Hg. The cardiac index was 1 9 (02)1/min/m2. The mean left ventricular ejectionfraction measured by ventriculography was69-6 (0 9)%. Extracellular volume was 414(19) ml/kg and total body exchangeablesodium 72 (3 1) nmol/kg. It is our normalpractice to withhold cardiac medication frompatients with constrictive pericarditis whilethey await cardiac surgery.2 Therefore, none ofthe patients included in the present study hadreceived any treatment for their heart diseasefor at least a month. The diagnosis of constric-tive pericarditis was confirmed in all patientsat surgery.
PROTOCOLSHaemodynamics, fluid compartments, and renalfunctionThese measurements were made on allpatients on the second or third day afteradmission. The techniques have beendescribed previously.' 2
ExerciseThe exercise test was carried out at 1600 h toavoid diurnal variation. Volunteers andpatients had taken a normal breakfast and alight lunch between 1200 and 1300 h. Each ofthem rested in bed quietly for 30 minutesbefore the test. An indwelling venous cannulawas inserted in one arm and a sphygmo-manometer cuff applied to the other.
Blood samples of 5 ml were drawn on fiveoccasions. The first sample was taken after thepatient had been supine for 30 minutes. Thesecond sample was taken 6 minutes later,while the patient was still supine. The averageof these two samples were taken as the basallying value. The third sample was drawn afterthe patient had been standing for 10 minutes.The subject then exercised for 6 minutes on atreadmill with a gradient of 00. For the first 3minutes the treadmill was run at 1 mph(1 -6 km/h). After 3 minutes, the speed of thetreadmill was increased to 1-5 mph, but thegradient was kept at 00. The fourth samplewas taken at the end of 6 minutes of exercise,while the patient was still standing.The patient was then asked to lie down and
the last sample was obtained after a further 20minutes. The pulse and blood pressure weremonitored after each blood sample was taken.The volunteers had no difficulty in complet-
ing the exercise test. The patients found it dif-ficult but, with encouragement, all of themwere able to complete the protocol. The oxy-gen consumption, measured using this proto-col in a normal group and in two groups ofpatients with different degrees of cardiac fail-ure, was 9 ml/min/kg for the first stage of the
on Septem
ber 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.76.1.50 on 1 July 1996. Dow
nloaded from

Ferrari, Anand, Ceconi, De Giuli, Poole-Wilson, Harris
exercise test and 12 ml/min/kg for the secondstage.9 Patients with severe cardiac failurewould not be expected to achieve an oxygenconsumption of more than 14 ml/min/kg. Thelevel of exercise undertaken by our patientswas, therefore, near their maximum.
Plasma hormonesWe measured renin activity and the concentra-tions of noradrenaline, adrenaline, aldos-terone, vasopressin, cortisol, growth hormone,prolactin, and atrial natriuretic peptide in theplasma by methods described elsewhere.'I 101Noradrenaline and adrenaline were measuredby high-performance liquid chromatographywith electrochemical detection. All the otherhormones were measured by radioimmunoas-say with standard commercial kits. Theradioimmunoassay for atrial natriureticpeptide (ANP) followed extraction with a Sep-Pack C 1 8-column. 125I-synthetic alpha-h-ANP(Eiken, Immunochemical, Tokyo, Japan) andrabbit anti-alpha-h-ANP antibody (Eiken)
Effects ofstanding and exercise in healthy controls and patients with oedema fromuntreated myocardial disease or constrictive pericarditis
Controls Myocardial disease Constictive pericarditis
Mean (SEM) n Mean (SEM) n Mean (SEM) n
Heart rate (beats/min):***RestStandingExerciseRecovery
Systolic arterial pressure(mm Hg):***
RestStandingExerciseRecovery
Adrenaline (pg/ml):RestStandingExerciseRecovery
Noradrenaline (pg/ml):***RestStandingExerciseRecovery
Renin activity (ng/mlh):***RestStandingExerciseRecovery
Aldosterone (pg/ml):*RestStandingExerciseRecovery
Vasopressin (pg/ml)*RestStandingExerciseRecovery
Cortisol (ng/ml):***RestStandingExerciseRecovery
Growth hormone (ng/ml):**RestStandingExerciseRecovery
Prolactin (ng/ml):RestStandingExerciseRecovery
Atrial natriuretic peptide(pg/ml):***
RestStandingExerciseRecovery
74 (1-8)84 (2 7)94 (2 9)79 (2 6)
113 (2-9)109 (3 7)125 (3-8)112 (3 0)
93 (20 4)107 (20 8)115 (25-6)99 (29 5)
272 (41 9)403 (49.8)462 (44 3)361 (47 8)
0-5 (0-1)0 9 (0.2)0-8 (0-1)0 7 (0 1)
52 (9 1)59 (10-7)86 (16-9)79 (10 4)
7-3 (1-3)9.3 (3*4)6-6 (1-8)6-3 (1-6)
68 (8 7)74 (10-6)85 (14-1)75 (12-3)
2-7 (2-1)3-4 (2 7)3-2 (1-6)3-4 (1-3)
7-4 (1-1)8-4 (1-1)8-6 (1-2)7-4 (0 9)
12 99 (5-2)12 107 (5-0)12 127 (4-8)12 105 (3 6)
12 123 (6 0)12 118(70)12 135 (7.9)12 124 (6-4)
12 108 (18-0)12 135 (225)12 95 (13-5)12 92 (16-2)
12 824 (89)12 1073 (174)12 1125 (126)12 864 (125)
12 1-3(05)12 1-6(07)12 2-2 (07)12 1-8(07)
12 112 (31-6)12 144 (36-1)12 231 (64 5)12 211 (68.5)
12 10-6 (2.8)12 15-2 (6-0)12 10-6 (2-1)12 90 (24)
12 110 (10-5)12 127 (13-5)12 131 (11-0)12 127 (12-4)
12 8-1 (3-0)12 13-3 (3-5)12 14-2 (5-0)12 11-3(4-3)
12 8-0 (1-5)12 7-9 (1-4)12 8-0 (1-3)12 7-7 (1-3)
24 (6) 12 247 (55)31 (9) 12 254 (48)25 (6) 12 226 (25)21 (4) 12 231 (43)
9 99 (3-1)9 102 (3.7)9 121 (3-3)9 99 (28)
9 107 (35)9 103 (3 3)9 117 (35)9 108 (3 2)
9 81 (15-5)9 101 (24 3)9 102 (20 7)9 132 (583)
9999
9999
9999
7777
9999
9999
9999
940 (172)1164 (181)1245 (231)1081 (208)
4-3 (1-3)4-8 (1-7)6-0 (1-8)5-1 (1-7)
176 (47 9)185 (55-7)185 (59-9)202 (63 7)
8-0 (1-7)6-6 (0 9)6-4 (0-6)6-6 (0-8)
95 (5 4)102 (7 7)102 (5-8)91 (6 0)
10-5 (4-1)10-6 (3.6)12-8 (3 8)11-4 (3.9)
8-2 (1-5)8-1 (1-6)7-8 (1-5)7-7 (1 4)
9 108 (20)9 100 (20)9 95 (16)9 85 (16)
12121212
12121212
11111110
12121212
12121211
11111111
11111111
12121212
11111111
12121212
12121212
were used, according to a previously describedmethod. 12
STATISTICAL ANALYSISFor each measurement, the analysis wasdesigned to answer the following questions: Isthere a difference in the baseline measurementbetween groups? Has the standing-exerciseprotocol had a significant overall effect, asmeasured in all three groups together? Arethere specific differences in the effects of thestanding-exercise protocol between groups?
In each part of the study, a preliminaryanalysis of variance was made for each mea-surement. First, the significance of the differ-ences in the general level of each measurementbetween study groups was established.Second, the significance of the differencesbetween the four conditions of the standing-exercise protocol (lying, standing, exercise,and recovery) was established by combiningthe results from the three different groups.Third, the significance of any alteration in theresponse of a measurement to the standing-exercise protocol between the groups ofpatients was explored. The analysis underesti-mated the significance of the differences ineach measurement between the four condi-tions of the standing exercise protocol,because it was not able to take into accountthe sequential nature of the changes.
Paired t tests were used subsequently to testthe significance of increases in measurementsbetween lying and standing and betweenstanding and exercise. Unpaired t tests wereused to test for differences between the groups(controls, myocardial disease, and constrictivepericarditis).
Data are presented as mean ( SEM).
ResultsGENERAL DIFFERENCES BETWEEN GROUPSDURING THE STANDING EXERCISE PROTOCOL(TABLE, FIG)
Preliminary analyses ofvariance showed sig-nificant differences (P < 0 01) in the baselinevalue of each measurement between the threegroups except for adrenaline and prolactin.The heart rate and plasma noradrenaline,renin activity, aldosterone, cortisol, growthhormone, and ANP were all increased in thetwo groups of patients.
Significant overall differences were alsofound between rest, standing, exercise, andrecovery with respect to heart rate, arterialpressure, and noradrenaline (P < 0 01 for eachcomparison).The response to standing and exercise did
not differ significantly between the threegroups.
EFFECTS OF STANDING (TABLE)Heart rate-Standing caused the heart rate toincrease by 10 beats/min in the healthy people(P = 0 001), by 8 beats/min in the patientswith myocardial disease (P = 0-2), and byonly 3 beats/min in the patients with constric-tive pericarditis (P = 0-3). There were no sig-nificant differences in the increase in heart rate
Probability values from variance analysis, comparing a particular measurement between the threegroups of subjects.*P < 0-01; **P < o-oo1; ***P < 0-0001.
52
on Septem
ber 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.76.1.50 on 1 July 1996. Dow
nloaded from

Neuroendocrine response to standing and mild exercise in patients with untreated severe congestive heart failure and chronic constrictive pericarditis
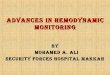
Heart rate (beats/min) 150
100
50
0
300
200
100
0
160 Adrenaline (pg/mi)
120 __
80
40-
0
Vasopressin (pg/mi)24-
18-
12-
6-
0 , , ,,C M PC M
Atrial natriuretic peptide (pg/mi)
C M P
320
240
160
80
0C M P C M P
L Restm Standing- ExerciseC = ControlsM = Myocardial diseaseP = Constrictive pericarditis
Effects of standing and exercise on heart rate, systolic arterial pressure, adrenaline, noradrenaline, plasma renin activity, noradrenaline, aldosterone,cortisol, growth hormone, prolactin and atrial natriuretic peptide in healthy people and patients with severe, untreated congestive cardiac failure frommyocardial disease or constrictive pericarditis.
on standing between the various groups.
Blood pressure Standing was accompaniedby a mean fall in systolic arterial pressure of3-8 mm Hg in the controls, 4-3 mm Hg in thepatients with myocardial disease, and 3-5mm Hg in the patients with constrictive peri-carditis. None of these differences reached sta-tistical significance within a group.
Catecholamines-In all groups the concen-
trations of noradrenaline and adrenaline in theplasma increased after standing. The increasein noradrenaline was 131 pg/ml in controls (P= 0-002), 249 pg/ml in those with myocardialdisease (P = 0 2), and 224 pg/ml in thosewith constrictive pericarditis (P = 0 003).The increase in adrenaline was 14 pg/ml incontrols (P = 0002), 27 pg/ml in myocardialdisease (P = 007), and 20 pg/ml in constric-tive pericarditis (P = 0 2). There was no sig-nificant difference in either noradrenaline or
adrenaline response between the cardiacpatients and the controls.
Renin and aldosterone-A non-significantincrease in plasma renin activity and aldos-terone was seen in each group on standing.There were no significant differences betweenthe groups.
Other hormones Standing produced no sig-nificant changes in the other hormones.
EFFECTS OF EXERCISE (TABLE)In general, the effects of this mild degree ofexercise were no greater than the effects ofrising from the lying to the standing position(figure).
Heart rate-Proceeding from standing toexercise caused a further increase in heart rateof 11 beats/min in the controls (P = 0 0003),20 beats/min in the patients with myocardialdisease (P = 0 003), and 19 beats/min in thepatients with constrictive pericarditis(P < 0 0001). The increase was significantlygreater than normal in constrictive pericarditis(P = 0 009) but did not differ significantlyfrom normal in myocardial disease (P=0 07).
Blood pressure-All groups showed an
increase in systolic arterial pressure duringexercise: 16-3 mm Hg in the controls (P =
0 0001), 16-3 mm Hg in myocardial disease(P = 0-002), and 13-6 mm Hg in constrictivepericarditis (P < 0 0001). There were no
significant differences between the groups.Catecholamines-Plasma noradrenaline rose
during exercise in all three groups, althoughsignificantly so only in the controls. Theincreases were 59 pg/ml in controls (P =
0 01), 52 pg/ml in myocardial disease (P =
0-6), and 81 pg/ml in constrictive pericarditis
C M P
53
on Septem
ber 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.76.1.50 on 1 July 1996. Dow
nloaded from

Ferrari, Anand, Ceconi, De Giuli, Poole-Wilson, Hanis
(P = 0 2). Plasma adrenaline did not changesignificantly during exercise.
Renin activity and aldosterone-Plasma reninactivity did not change during exercise in thecontrols. It rose in the group with myocardialdisease (increase of 0-5 pg/ml/h; P = 0.02)and in the group with constrictive pericarditis(increase of 1-2 pg/ml/h; P = 0 2). Theincrease was significantly greater in thepatients with myocardial disease than in thecontrols (P = 0 04).A non-significant increase in plasma aldos-
terone occurred on exercise in the controlsand the patients with myocardial disease.There was no change in those with constrictivepericarditis. The difference between the twogroups of patients was significant (P = 003).
Other hormones-Exercise had no significanteffect on any of the other hormones.
DiscussionIn this study we useed the same methods tocompare patients with severe untreated car-diac failure with healthy people. Patients withuntreated heart disease were chosen because itwas not clear from earlier reports whethertreatment might itself modify the neuroen-docrine response to exercise. The exercise pro-tocol and load were identical in the healthypeople and the patients, so that a direct com-parison could be made. For such comparabil-ity, a mild degree of exercise had to be chosen.Thus the level of exercise was low relative tothe maximum in the healthy people; but it wasnear maximum in the patients. This meansthat the exercise was more stressful in thepatients, which might have made the neuroen-docrine response more severe. There is littlepublished information on whether the neu-roendocrine response in untreated congestivecardiac failure is different from normal.
All patients had severe congestive cardiacfailure. The cardiac index was reduced, theheart rate was rapid, and pressures in the pul-monary circulation and in the right atriumwere increased. The right atrial pressure wasparticularly high in patients with chronic con-strictive pericarditis. The systemic arterialpressure was normal in both groups ofpatients, which is consistent with the hypothe-sis that the neuroendocrine response leadingto the oedematous syndrome contributes tothe maintenance of blood pressure.'3 14Retention of water and sodium was confirmedby appropriate measurements.
Analysis of variance showed that consider-able differences in the heart rate, arterial pres-sure, and levels of plasma hormones separatedthe two groups of patients from the healthycontrols. The analysis of variance does not takeinto account the sequential nature of the con-ditions of lying, standing, exercise, and recov-ery; but it is clear that the differences we reportwere mainly determined by the initial, basalvalues while the patients were lying down.The standing-exercise protocol had the
same significant overall effects in all threegroups of subjects-with no significant differ-ences between the three groups in the effects
of the protocol on any factor studied. Thus,from the analysis of variance alone, no specificeffect of congestive failure on the response toexercise could be detected.
Separate analyses by t tests of the increasesduring standing did not reveal any specific dif-ference in the response between the cardiacpatients and the healthy people. Levine et alreported a normal response of plasma reninactivity and noradrenaline to tilt in patientswith congestive cardiac failure who had nor-mal resting haemodynamics, but a diminishedresponse in those patients who had abnormalresting haemodynamics. 5 The haemodynamicresponse to tilt was similar in their two groupsof patients. In our patients, the response ofplasma noradrenaline to standing was, if any-thing, greater in the cardiac patients. The actof standing is, however, not entirely compara-ble with passive tilting.The increase in heart rate during exercise
tended to be greater than normal in the twogroups of patients, significantly so in thosewith constrictive pericarditis (t test). The arte-rial pressure rose by about the same amount inall three groups. Francis commented thatpatients with congestive cardiac failure have anincreased heart rate response and a normalarterial pressure response for a given uptake ofoxygen.'6 It is only when the increases areexpressed as a function of the maximal oxygenuptake that the responses of the heart rate andarterial pressure in congestive cardiac failureseem to be less than normal. Plasma reninactivity rose more during exercise in the twogroups of patients, and the increase was signif-icantly greater than normal by t test in myocar-dial disease.
GENERAL CONCLUSIONSThe neurohumoral response in congestive car-diac failure seems to be directed to the preser-vation of arterial pressure. 213141718 Theneurohumoral response to standing and exer-cise is similar to that in congestive cardiac fail-ure5 and is probably also directed to themaintenance of the arterial pressure and,thereby, perfusion of the tissues.We found that during exercise the cardiac
patients had a greater increase than normal inheart rate (significant only for constrictivepericarditis) and in plasma renin activity (sig-nificant only for myocardial disease). Wefound no other significant difference in theresponse to the standing-exercise protocol.
Because any differences were small we con-clude that, except for the responses of heartrate and perhaps ofplasma renin activity duringexercise, the neuroendocrine response tostanding and exercise is not substantially mod-ified by congestive cardiac failure. Essentially,normal responses are superimposed on anabnormal resting state. This conclusion is, ofcourse, valid only for the limited degree ofexercise that can be undertaken by suchpatients who are extremely ill.
This work was supported by the Indian Council of MedicalResearch, Italian Research Council (CNR) target Project"Prevention and Control Disease Factor" (87-01485-04 and87-00491-56), and the British Heart Foundation.
54
on Septem
ber 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.76.1.50 on 1 July 1996. Dow
nloaded from

Neuroendocrine response to standing and mild exercise in patients with untreated severe congestive heart failure and chronic constrictive pericarditis 55
1 Anand IS, Ferrari R, Kaira GS, Wahi PL, Poole-Wilson P,et al. Edema of cardiac origin. Studies of body water andsodium, renal function, hemodynamic indexes andplasma hormones in untreated congestive cardiac failure.Circulation 1989;80:299-305.
2 Anand IS, Ferrari R, Kalra GS, Wahi PL, Poole-Wilson P,Harris P. Pathogenesis of edema in constrictive pericardi-tis studies of body water and sodium, renal function,hemodynamics and plasma hormones before and afterpericardictomy. Circulation 1991;83:1880-7.
3 Francis G, Goldsmith S, Levine T, Olivari M, Cohn J. Theneurohumoral axis in congestive heart failure. Ann InternMed 1984;101:370-7.
4 Ferrari R, Ceconi C, Rodella A, De Guili F, Panzali A,Harris P. Temporal relations of the endocrine responseto exercise. Cardioscience 1991;2:131-40.
5 Harris P. Evolution and the cardiac patient. Cardiovasc Res1983;17:313-9.
6 Francis G, Goldsmith S, Ziesche S, Cohn J. Response ofplasma noradrenaline and epinephrine to dynamic exer-cise in patients with congestive heart failure. Am J Cardiol1982;49:1152-6.
7 Kirlin P, Grekin R, Das S, Ballor E, Johnson T, Pitt B.Neurohumoral activation during exercise in congestiveheart failure. Am 7Med 1986;81:623-9.
8 Bayliss J, Norell M, Canepa-Anson R, Sutton G, Poole-Wilson P. Untreated heart failure: clinical and neuroen-docrine effects of introducing diuretics. Br Heart
_ 1987;57:17-22.
9 Lipkin D, Perrins J, Poole-Wilson P. Respiratory gasexchange in the assessment of patients with impairedventricular function. Br Heart J 1984;54:321-328.
10 Ferrari R, Ceconi C, Signorini C, Anand I, Harris P,Albertini A. Sample treatment for long-distance trans-port of plasma for hormone assay. Clin Chem 1989;35:331-2.
11 Ferrari R, Ceconi C, Rodella A, Harris P, Visioli 0.Hormonal response in untreated myocardial infarction.Cardioscience 1990;1:55-60.
12 Poiesi C, Rodella A, Mantero G, Cannela G, Ferrari R,Albertini A. Improved radioimmunoassay of atrial pep-tide in plasma. Clin Chem 1989;35:1431-4.
13 Harris P. Congestive cardiac failure: central role of the arte-rial blood pressure. BrHeartJ 1987;58:190-203.
14 Harris P. Role of arterial pressure in the oedema of heartdisease. Lancet 1988;i:1036-8.
15 Levine T, Francis G, Goldsmith S, Cohn J. The neuro-humoral and hemodynamic response to orthostasis tilt inpatients with congestive heart failure. Circulation 1983;67:1070-5.
16 Francis G. Hemodynamic and neurohumoral responses todynamic exercise: normal subjects versus patients withheart disease. Circulation 1987;76suppl VI: 11-6.
17 Anand IS, Chandrashekhar Y, Ferrari R, Sarma R, GuleriaR, Jindal S, et al. Pathogenesis of congestive state inchronic obstructive pulmonary disease. Studies of bodywater and sodium, renal function, hemodynamics, andplasma hormones during edema and after recovery.Circulation 1992;86: 12-21.
18 Anand IS, Chandrashekhar Y, Ferrari R, Poole-Wilson PA,Harris PC. Pathogenesis of edema in chronic severe ane-mia: studies of body water and sodium, renal function,hemodynamics variables, and plasma hormones. Br Heart7 1993;70:357-62.
on Septem
ber 14, 2020 by guest. Protected by copyright.
http://heart.bmj.com
/H
eart: first published as 10.1136/hrt.76.1.50 on 1 July 1996. Dow
nloaded from