Embed Size (px)
Citation preview

Heart Outcomes Prevention Evaluation Study
A large, simple, randomized trial of Ramipril and vitamin E in patients at high risk for cardiovascular events
A lasting legacy : The view 25 years later

SOLVD Combined Trials
Lonn et al, Circulation 1994

Summary of Design
Aim: Effect of Ramipril (up to 10mg/d) or Vit E (400 IU/d) vs its placebo on CV death, MI or stroke (primary)
Design: Randomized double blind, 2x2 factorial,Wide entry criteria, large, simple trial
Size: 9541 patients followed for 4 to 6 years:- High power to detect RRR of 12% overall; - 15% to 25% in key subgroups and individual components of primary and secondary outcome (Revasc, CHF, UA, diabetes complications)
Organization: 267 hospitals from 19 countries in North & South America and Europe, Coordinated by the CCC at McMaster University, Hamilton, Canada

Monitoring Boundaries Over Time
Ramipril versus Placebo
1.51
2.322.75
4.54.31
4.76
-1
0
1
2
3
4
5
Z
↑
Oct
. 95
Aug.
96
Nov
. 97
Nov
. 98
Mar
. 99
Jan.
94
Nov
. 99
Ben
efit

Primary Adjudicated Events –Ramipril vs Placebo 1/2
Ramipril(%)
Plac(%)
RR 95% CI pNo. Rand. 4645 46521°Outcome
MI,Stroke,CVDth 14.1 17.7 0.78 0.70-0.86 0.000002CV Death* 6.1 8.1 0.75 0.64-0.87 0.0002MI* 9.9 12.2 0.80 0.71-0.91 0.0005Stroke* 3.4 4.9 0.69 0.56-0.84 0.0003
Non-CV Death 4.3 4.1 1.03 0.84-1.25 0.78Mortality 10.4 12.2 0.84 0.75-0.95 0.0058
*not mutually exclusive

0
0.05
0.1
0.15
0.2
0 500 1000 1500
Days of Follow-up
Kap
lan-
Mei
er R
ates Ramipril Placebo
Primary Outcome -Ramipril vs Placebo
RR=0.78 (0.70-0.86) P=0.000002

Primary Outcome -Vitamin E vs Placebo
RR=1.05 (0.95-1.16) P=0.35
0
0.05
0.1
0.15
0.2
0 500 1000 1500Days of Follow-up
Kap
lan-
Mei
er R
ates
Vitamin E. Placebo

All CHF - Ramipril vs Placebo
RR=0.77 (0.68-0.87) P=0.00004
0
0.03
0.06
0.09
0.12
0 500 1000 1500
RamiprilPlacebo
Days of Follow-up
Kapl
an-M
eier
Rat
es

Cerebrovascular Events - Ramipril vs Placebo
Ramipril Placebo RR PRandomized 4645 4652Stroke 3.4 4.9 0.69 (0.56-0.84) 0.0003
Non-Fatal 3.0 3.9 0.76 (0.61-0.95) 0.015Fatal 0.4 1.0 0.39 (0.22-0.67) 0.0005
TIA 4.1 4.9 0.82 (0.68-0.99) 0.046Any Above 6.8 8.7 0.77 (0.66-0.89) 0.0004

Ramipril Plac(%) (%) RR 95% CI p
No. Rand. 1808 17701°Outcome
MI,Stroke,CVDth 15.4 19.8 0.76 0.65-0.89 0.0006CV Death* 6.2 9.6 0.63 0.50-0.80 0.0002MI* 10.2 12.8 0.78 0.65-0.95 0.014Stroke* 4.3 6.1 0.68 0.51-0.91 0.0096
Non-CV Death 4.7 4.4 1.05 0.77-1.43 0. 75Mortality 10.8 14.0 0.76 0.63-0.92 0.0047
Diabetics: Adjudicated Events -Ramipril 1/2
*Not mutually exclusive

Diabetes: Survival curves on primary outcome
RR=0.76 (0.65-0.89) P=0.0006
0
0.05
0.1
0.15
0.2
0.25
0 500 1000 1500Days of Follow-up
Kapl
an-M
eier
Rat
es Ramipril Placebo

Other Diabetes Related Events in Follow Up: Ramipril vs Placebo
RandomizedDiabetic Comp.
Overt Nephrop./Renal DialysisLaser Therapy
NewMicroalbuminuria(of Non-MA)New Diabetes(of Non-DM)
5.3
OverallRamipril Placebo RR
4645 46526.2 7.4 0.84*3.0 4.0 0.75*
3.7 4.0 0.9220.6 23.1 0.90*
3.7 0.68**
DiabeticsRamipril Placebo RR
1808 177014.8 17.5 0.83*6.6 8.5 0.76*
9.4 10.5 0.8833.8 37.7 0.91
- - -
*p<0.05, **p<0.01, ***p<0.001

Development of DM: Ramipril vs Placebo
RR=0.68 (0.53-0.87) P=0.002
0
0.02
0.04
0.06
0.08
0.1
200 400 600 800 1000 1200 1400 1600Days of Follow-up
Kapl
an-M
eier
Rat
es
Ramipril Placebo

Mortality Reductions in HOPE vs Prior Trials of Anti-Hypertensive Treatment vs Control
10-15 mmHg↓ in SBP →40%↓Stroke→15%↓MI
Expected fromEpi Studies
Achieved inHOPE
3.3mmHg↓in SBP 13% ↓ Stroke 31% ↓
5% ↓ MI 20% ↓

Risk of Primary / Revasc / All CHF by SBP
Quartiles
≤124
125-139
140-150
151+
Overall
Usual BP
125
134
142
153
Ramipril better Ramipril worseP for trend=0.0060
RR with 95% CIAbs. Risk Reduction
2.1%
4.8%
6.2%
10.4%
5.8%
N
2281
2465
2438
2110

Total benefit of about 2 million events prevented
Annual Global Impact of Ramipril
• approximately 1 to 1.5 million deaths, myocardial infarction, stroke or revascularization procedures will be prevented globally every year
• Plus impact on CHF, diabetic complications and prevention of diabetes, which will prevent an additional 0.5 to 0.6 million such events/year
If 1/4 of eligible patients with vascular disease in developing countries and 1/2 in developed countries are given Ramipril:


Key People who Made HOPE Happen

Sponsors
• Medical Research Council of Canada• Heart & Stroke Foundation of Ontario• Hoechst Marion Roussel• Astra-Zeneca• King Pharmaceuticals• Natural Source Vitamin E Assoc.• NEGMA Pharma
Study independently designed, organized, conducted, analyzed and reported by the Canadian Cardiovascular
Collaboration and HOPE Steering Committee




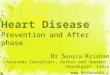
Numbers of New Prescriptions for Angiotensin-Converting-Enzyme (ACE) Inhibitors Filled by Elderly
(aged 65 and over) Ontario Residents
Tu K et al, CMAJ 2003

HOPE publications
• Over 60 papers from HOPE in peer review journals:2 NEJM, 1 Lancet, 2 JAMA, about 12 in Circulation, Eur Heart
J and JACC, etc.
• Collective citations of >20,000
• Raised the profile of Canadian lead RCTs worldwide
• Foundation of the Canadian Cardiovascular Collaboration and CANNECTIN which lead to over 20 large Canadian led global studies in CVD Prevention, Diabetes and ACS (OASIS series of 9 trials)

Citations

Follow Up studies to HOPE
• HOPE 2 : Homocysteine lowering with vitamins ineffective (NEJM 2006).
• HOPE 3: In average risk primary prevention, statins effective, but BP lowering is not (except in those with elevated BP) (NEJM 2016, 374: 2009-20, 2021-31, 2032-43)
• HOPE 4: Combination therapy (2 + BP lowering drugs+ statins) delivered by NPHW reduces projected risk of CVD by 50% (Lancet 2019) in hypertension
• DREAM: Ramipril and rosiglitazone in prevention of DM in those with IGT/IFG (Lancet 2006 and NEJM 2006)
• ONTARGET & TRANSCEND: ACEI and ARB are equivalent and ARB reduces CVD in those who are ACE intolerant (NEJM 2008 and Lancet 2008).

Recognition and Awards for HOPE
Date Award Organization Given By
Description
1999 Top 10 Research Advances in Heart Disease and Stroke
AHA Achievements in basic and clinical research on CVD.
2000 Top 10 Research Advances AHA Stroke reduction
2000 Molecule of the Year MMW Munich Ramipril for HOPE
2000 Top Ten Health Advances Harvard Health Letter “Should you be taking an ACE inhibitor?”
2001 Prix Galien Prix Galien Canada Awarded to Salim Yusuf
2001 President’s Award for Outstanding Service, Team Category
McMaster University Awarded to Jackie Bosch and Janice Pogue
2002 Hot paper in Medicine [NEJM 2000; 342(3): 145-53]
InCites/Sci-Bytes Highest cited original paper in medicine published in the previous 2 years during Nov-Dec 2001.

Supported 20 Scholarships and 2 Chairs
Date Award Organization Description2005 Canada-HOPE Scholarship
ProgramCIHR + Aventis Scholarship program to enable promising
scientists and clinicians from developing countries to be mentored by Canadian researchers.
2001 Population Health Research Chair in Diabetes Research
McMaster U + Aventis Recipient : Hertzel Gerstein
2008 HOPE Chair in Peace and Health
McMaster U + Aventis Research & teaching at the Centre for Peace Studies and Population Health Research Institute on determinants and health impacts of war and health work

HOPE 25 years from the begining
• First trial which established the role of ACE-I in CVD prevention globally
• First trial in DM showing reduction in mortality, MI, stroke and renal dysfunction.
• Adopted by guidelines and influenced practice.• Lead to a series of large Canadian led international
studies.• Built capacity in research thru scholarships and chairs• Changed the culture so that Canadians lead large
independent trials