Embed Size (px)
Citation preview

5Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
REVIEW ARTICLE
Heart Rate Variability as a Measure ofDisease State in Irritable
Bowel Syndrome
Hyo-Jung Park*, RN, PhD
Full-time Lecturer, Division of Nursing Science, College of Health Science, Ewha Womans University, Seoul, Korea
Heart rate variability (HRV) is a noninvasive measure of sympathovagal balance in the autonomic nervoussystem (ANS). This review will: (a) consider HRV measurement in irritable bowel syndrome (IBS); (b) dis-cuss the applicability of HRV measurement in IBS by addressing strengths and limitations; and (c) proposefuture directions in this field of gastrointestinal research and clinical practice. As a strength, analyzing HRVcomponents is a useful method and appears most suitable for detection of changes in ANS sympathovagalbalance in both stress and non-stress conditions with good validity and reliability. Also, it is an appropriatemeasure for ANS in studies with large populations, in both laboratory and clinical settings, and for longi-tudinal studies because of its noninvasive assets. With regard to limitations of measuring HRV, these arepoor standardization, additional human editing, not considering medication or other confounding factors,inconsistent results in gastrointestinal vagal tone study, and different time periods. [Asian Nursing Research2008;2(1):5–16]
Key Words autonomic nervous system, heart rate variability, irritable bowel syndrome
*Correspondence to: Hyo-Jung Park, RN, PhD, Full-time Lecturer, Division of Nursing Science, College ofHealth Science, Ewha Womans University, 11-1 Daehyun-Dong, Seodaemoon-Ku, Seoul 120-750, Korea.E-mail: [email protected]
INTRODUCTION
Heart rate variability (HRV) may provide a new andmore powerful approach for evaluating the auto-nomic nervous system (ANS) in patients with irrita-ble bowel syndrome (IBS). IBS is a common chronicfunctional gastrointestinal (GI) disorder character-ized by chronic intermittent symptoms includingabdominal discomfort/pain, diarrhea, constipation,and bloating. More than 80% of IBS patients com-plain of stress-induced exacerbation of GI symptoms(Levy, Cain, Jarrett, & Heitkemper, 1997;Whitehead,
Crowell, Robinson, Heller, & Schuster, 1992). Sev-eral studies have demonstrated an increased visceralsensitivity and gut dysmotility caused by variousstimuli such as mental stress and meals (Clemens,Samsom, Van Berge Henegouwen, & Smout, 2003;Elsenbruch & Orr, 2001; Gupta, Sheffield, & Verne,2002; Hausken et al., 1993; Mayer, 2000; Mertz,Naliboff, Munakata, Niazi, & Mayer, 1995; Naliboffet al., 1997; Verne, Robinson, & Price, 2001). Thepathophysiology of IBS remains poorly understood.Hence many investigators try to seek the pathogenesisof IBS in patients using several tests. Dysfunction of
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 5

the ANS may be important for the development ofabnormalities of GI motility and visceral perception.The first study dates back to 1928, when Bockus,Bank, and Wilkinson suggested IBS symptoms wereassociated with an imbalance of ANS function. Morerecently, there are a growing number of studies usingHRV to assess the function of the ANS in patientswith IBS.
Thus, the objectives of this review are to: (a)consider the relationship between IBS and HRVmeasurement; (b) discuss the applicability of HRVmeasurement in IBS by addressing strengths and limi-tations; and (c) propose future directions in this fieldof GI research and clinical practice. This paper pro-vides a review of current knowledge of the usefulnessof measurement of HRV in IBS.
HRVHRV is a noninvasive, indirect method of measuringbalance/imbalance of the parasympathetic nervoussystem (PSNS) and sympathetic nervous system(SNS). Originally it was assessed manually from cal-culations of the mean R-R interval and its standarddeviation measured on short-term (2–5 minutes)electrocardiograms (ECG). Recently, the availabilityof increased computing power, innovative micropro-cessor technology, and the remarkable technologicaldevelopments in recording have enabled the analysisof 24-hour long-term records (Task Force of the Euro-pean Society of Cardiology and the North AmericanSociety of Pacing and Electrophysiology, 1996).
Analysis of HRV can be divided into time domainanalysis and frequency domain analysis.Time domainanalysis, known as nonspectral or statistical analysis,is a general measure of ANS balance. Time domainanalysis of HRV is correlated with total variance ofthe heart signal and PSNS (Hayano et al., 1991;Kleiger, Stein, Bosner, & Rottman, 1992; Task Forceof the European Society of Cardiology and the NorthAmerican Society of Pacing and Electrophysiology,1996). The SD 24-hr is the simple standard devia-tion of the set of R-R intervals in a 24-hour period.SD-5-min is the mean of the standard deviations ofnormal R-R intervals for all 5-minute blocks in afull 24-hour ECG recording. The root mean square
successive difference (RMSSD) is the squared dif-ference between two adjacent normal R-R intervalscomputed over the entire 24-hour period. The RR50is the total number of occurrences in a 24-hour pe-riod in which the difference between two successiveR-R intervals exceeds 50 milliseconds. The %RR50(pNN50) is the percentage of the absolute differencebetween adjacent normal R-R intervals that are greaterthan 50 milliseconds computed over the entire 24hours (Kleiger et al.;Task Force of the European Soci-ety of Cardiology and the North American Societyof Pacing and Electrophysiology).
Frequency domain analysis of HRV, known aspower spectral analysis, contains two major spectralcomponents: the high frequency (HF) component(0.15–0.40 Hz) and the low frequency (LF) compo-nent (0.03–0.15Hz or 0.04–0.15Hz or 0.05–0.15Hzdepending on the research) (Akselrod et al., 1981).Normal frequency range has not yet been firmlyestablished. Some studies used medium-frequencypower (MF) (0.07–0.15Hz) (Heitkemper et al., 1998;Karling et al., 1998; McCraty,Atkinson,Tiller, Rein, &Watkins, 1995). Total power is the energy in theheart period power spectrum up to 0.40 Hz. Fre-quency domain analysis of HRV has been used as asensitive index of ANS activities because it can helpdistinguish SNS from PSNS regulation of the sino-atrial node. Dominance by the SNS leads to the fight/flight reaction and PSNS dominance tends to have a rest/digest effect.The HF component has been con-sidered the respiratory sinus arrhythmia (RSA) andis mediated solely by the PSNS, whereas the LF com-ponent corresponds to blood pressure oscillationsand is jointly modified by the PSNS and the SNS.Therefore, HF is considered a pure measure of PSNSactivity and LF is less clear and considered a mixedANS marker. HF is highly correlated with the timedomain variables of RMSSD and %RR50; these threecomponents provide an estimate of PSNS activity(Delaney & Brodie, 2000; Kleiger, Miller, Bigger, &Moss, 1987; Ori, Monir, Weiss, Sayhouni, & Singer,1992). In addition, the LF/HF ratio is a useful param-eter that reflects the balance of ANS activities.The LF/HF ratio was significantly greater in healthy subjects(Achten & Jeukendrup, 2003).
H.J. Park
6 Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 6

7
The polar software system consists of very lowfrequency (VLF) power from 0.0033 Hz to 0.04 Hz,LF power from 0.04 Hz to 0.15 Hz, and HF powerfrom 0.15 Hz to 0.40 Hz. VLF indicates SNS activ-ity. The ultra low frequency (ULF) at 0–0.0033 Hzmay represent humoral and thermoregulatory factors.However, as very slow rhythms are assessed only overlong periods, this component is not always analyzed(Pagani et al., 1986).The physiological mechanisms ofthe ULF and VLF band widths can be modulated byrenin-angiotensin system and/or temperature regula-tion (Akselrod et al., 1981).
The logarithms (e.g. ln%RR50, lnRMSSD, lnHF,lnLF) or logit transformation (e.g., logit50) are some-times chosen because the individual median valuesare not distributed normally, but fit a normal log orlogit distribution.The logarithms or logit transforma-tion are easy to calculate and are highly correlated withthe spectral estimate of cardiac vagal tone. In addition,the logarithm or logit transformation are useful fora small sample and for subjects with a very low levelof HRV (Burr, Motzer, Chen, Cowan, & Heitkemper,2003; Moser et al., 1998). Hence, indicators of ANSimbalance are LF/HF, SD-5-min/RMSSD, and sqLF/HF. These three higher values represent greaterSNS and lower PSNS activity. Indicators of generalANS activity are SD-5-min and lnLF. Indicators ofPSNS activity are HF, RMSSD, and %RR50 (Jarrettet al., 2003; Kleiger et al., 1987).
Effects of confounding variables on HRVThere are several possible different confounding vari-ables that affect HRV, such as gender, age, body posi-tion (supine/standing), breathing frequency, bodymass index (BMI), systolic blood pressure, physicaland mental stress, pain, hormonal fluctuation, familyhistory, genetic, medication, and life-style factors suchas eating, smoking, alcohol, coffee consumption, andhabitual physical activity (Parati & Di Rienzo, 2003).
Age and gender, in particular, have been found toinfluence PSNS tone.There is a significant tendencyfor decreased HRV with increasing age (Cowan,Pike, & Burr, 1994).This is reflective of a reduction inthe absolute values of PSNS and SNS activity (Aubert,Seps, & Beckers, 2003). In general, healthy women
have a lower HRV than do healthy men due to thereduced variance in sympathetic activity (reduced LFand LF/HF) in females (Cowan et al.; Jensen-Urstadet al., 1997;Thayer, Smith, Rossy, Sollers, & Friedman,1998). Also, the luteal phase of the menstrual cyclewas associated with a greater increase in LF and a greater decrease in HF, resulting in a higher LF/HFratio. This suggests SNS activities in young collegewomen (mean age: 19.2 years) are predominant inthe luteal phase as compared with the follicular phaseduring the menstrual cycle despite using a small num-ber of subjects (N = 20) (Sato, Miyake, Akatsu, &Kumashiro, 1995).
HRV decreases significantly with increasing BMIdue to depressed sympathetic modulation of the heartassociated with excessive body weight (Karason,Molgaard, Wikstrand, & Sjostrom, 1999).
Exercise training studies have shown to have asignificantly positive effect on HRV (Aubert et al.,2003). Also, biofeedback and relaxation tasks havebeen found to be beneficial (Cowan, Kogan, Burr,Hendershot, & Buchanan, 1990).
With regard to medication, treatment with tri-cyclic antidepressants (TCAs) reduces HRV (Agelink,Boz, Ullrich, & Andrich, 2002; Khaykin et al., 1998).Treatment with selective serotonin reuptake inhib-itors (SSRIs) normalizes HRV (Tucker et al., 1997;Yeragani & Rao, 2003). The effects of beta-blockersincrease HRV, as reflected by augmented vagal activityunder stress (Sandrone et al., 1994).
FINDINGS
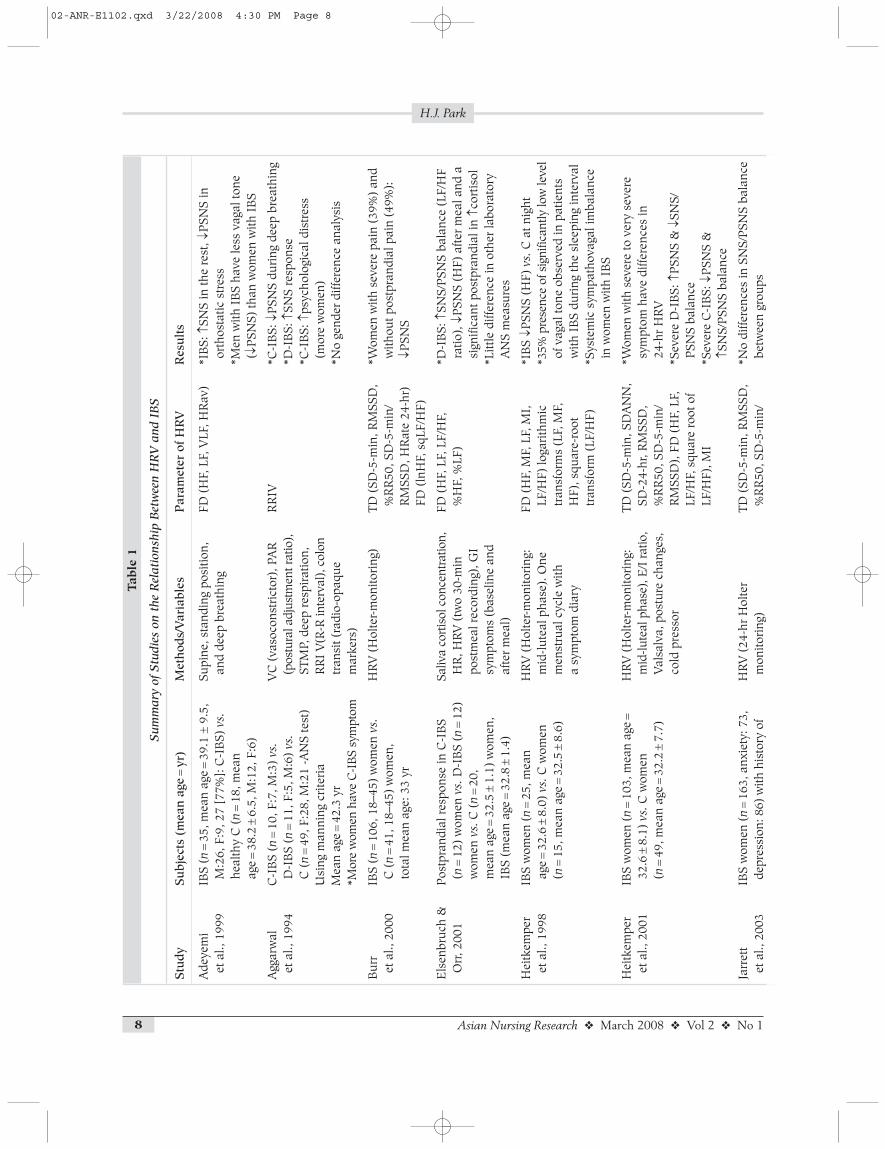
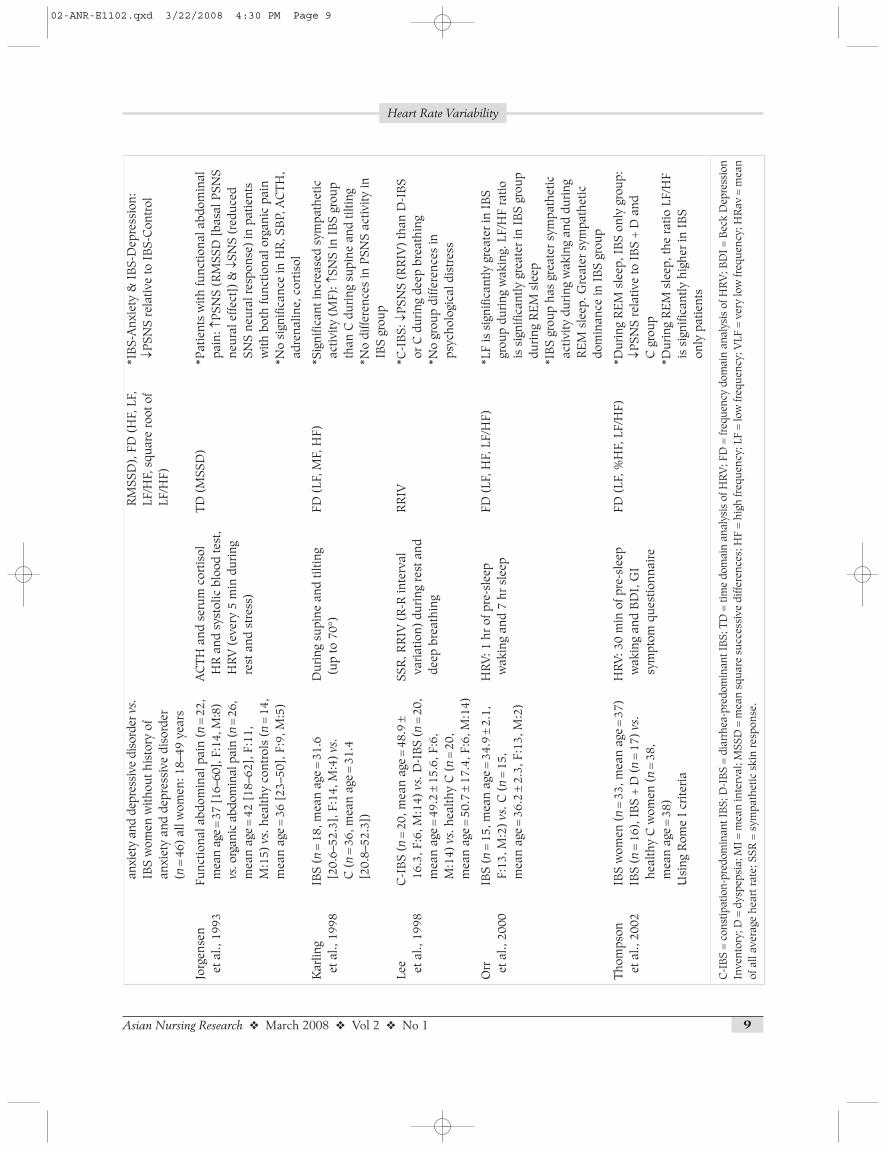
Articles were searched from Medline and CINAHLfrom 1990 through November 2007 to identify stud-ies with the key words IBS and HRV. Studies wherethe measurement of HRV was assessed in a singlegroup of subjects before and after a procedure wereexcluded. Table 1 shows the summary of the mea-surement of HRV in IBS studies including samplesize, characteristics of subjects, methods, parametersof HRV, and results.
Most studies were published recently—all but two(Aggarwal et al., 1994; Jorgensen et al., 1993) since
Heart Rate Variability
Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 7
H.J. Park
8 Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
Table
1
Sum
mar
y of
Stu
dies
on
the
Rel
atio
nshi
p B
etw
een
HR
V a
nd I
BS
Stu
dyS
ubj
ects
(m
ean
age
=yr
)M
eth
ods/
Var
iabl
esP
aram
eter
of
HR
VR
esu
lts
Ade
yem
i IB
S (n
=35
, mea
n ag
e=
39.1
±9.
5,
Supi
ne, s
tand
ing
posi
tion,
FD
(H
F, L
F, V
LF, H
Rav
)*I
BS:
↑SN
S in
the
rest
, ↓P
SNS
in
et a
l., 1
999
M:2
6, F
:9, 2
7 [7
7%]:
C-I
BS)
vs.
and
deep
bre
athi
ngor
thos
tatic
str
ess
heal
thy
C (
n=
18, m
ean
*Men
with
IB
S ha
ve le
ss v
agal
tone
ag
e=
38.2
±6.
5, M
:12,
F:6
) (↓
PSN
S) th
an w
omen
with
IB
S
Agg
arw
al
C-I
BS
(n=
10, F
:7, M
:3)
vs.
VC
(va
soco
nstr
icto
r), P
AR
R
RIV
*C-I
BS:
↓P
SNS
duri
ng d
eep
brea
thin
get
al.,
199
4D
-IB
S (n
=11
, F:5
, M:6
) vs
.(p
ostu
ral a
djus
tmen
t rat
io),
*D-I
BS:
↑SN
S re
spon
seC
(n
=49
, F:2
8, M
:21
-AN
S te
st)
STM
P, d
eep
resp
irat
ion,
*C
-IB
S: ↑
psyc
holo
gica
l dis
tres
s U
sing
man
ning
cri
teri
aR
RI
V(R
-R in
terv
al),
col
on(m
ore
wom
en)
Mea
n ag
e=
42.3
yr
tran
sit (
radi
o-op
aque
*N
o ge
nder
diff
eren
ce a
naly
sis
*Mor
e w
omen
hav
e C
-IB
S sy
mpt
omm
arke
rs)
Bur
r IB
S (n
=10
6, 1
8–45
) w
omen
vs.
HR
V (
Hol
ter-
mon
itori
ng)
TD (
SD-5
-min
, RM
SSD
, *W
omen
with
sev
ere
pain
(39
%)
and
et a
l., 2
000
C (
n=
41, 1
8–45
) w
omen
, %
RR
50, S
D-5
-min
/w
ithou
t pos
tpra
ndia
l pai
n (4
9%):
to
tal m
ean
age:
33
yrR
MSS
D, H
Rat
e 24
-hr)
↓PSN
SFD
(ln
HF,
sqL
F/H
F)
Els
enbr
uch
&P
ostp
rand
ial r
espo
nse
in C
-IB
S Sa
liva
cort
isol
con
cent
ratio
n,FD
(H
F, L
F, L
F/H
F,
*D-I
BS:
↑SN
S/P
SNS
bala
nce
(LF/
HF
Orr
, 200
1(n
=12
) w
omen
vs.
D-I
BS
(n=
12)
HR
, HR
V (
two
30-m
in
%H
F, %
LF)
ratio
), ↓
PSN
S (H
F) a
fter
mea
l and
a
wom
en v
s.C
(n
=20
, po
stm
eal r
ecor
ding
), G
I si
gnifi
cant
pos
tpra
ndia
l in
↑cor
tisol
mea
n ag
e=
32.5
±1.
1) w
omen
, sy
mpt
oms
(bas
elin
e an
d *L
ittle
diff
eren
ce in
oth
er la
bora
tory
IB
S (m
ean
age
=32
.8±
1.4)
afte
r m
eal)
AN
S m
easu
res
Hei
tkem
per
IBS
wom
en (
n=
25, m
ean
HR
V (
Hol
ter-
mon
itori
ng:
FD (
HF,
MF,
LF,
MI,
*I
BS
↓PSN
S (H
F) v
s. C
at n
ight
et a
l., 1
998
age
=32
.6±
8.0)
vs.
C w
omen
m
id-l
utea
l pha
se).
One
LF
/HF)
loga
rith
mic
*3
5% p
rese
nce
of s
igni
fican
tly lo
w le
vel
(n=
15, m
ean
age
=32
.5±
8.6)
men
stru
al c
ycle
with
tr
ansf
orm
s (L
F, M
F,
of v
agal
tone
obs
erve
d in
pat
ient
sa
sym
ptom
dia
ryH
F), s
quar
e-ro
ot
with
IB
S du
ring
the
slee
ping
inte
rval
tran
sfor
m (
LF/H
F)*S
yste
mic
sym
path
ovag
al im
bala
nce
in w
omen
with
IB
S
Hei
tkem
per
IBS
wom
en (
n=
103,
mea
n ag
e=
HR
V (
Hol
ter-
mon
itori
ng:
TD (
SD-5
-min
, SD
AN
N,
*Wom
en w
ith s
ever
e to
ver
y se
vere
et
al.,
200
132
.6±
8.1)
vs.
C w
omen
m
id-lu
teal
pha
se),
E/I
rat
io,
SD-2
4-hr
, RM
SSD
, sy
mpt
om h
ave
diffe
renc
es in
(n
=49
, mea
n ag
e=
32.2
±7.
7)V
alsa
lva,
pos
ture
cha
nges
, %
RR
50, S
D-5
-min
/24
-hr
HR
Vco
ld p
ress
orR
MSS
D),
FD
(H
F, L
F,
*Sev
ere
D-I
BS:
↑P
SNS
& ↓
SNS/
LF/H
F, s
quar
e ro
ot o
f P
SNS
bala
nce
LF/H
F), M
I*S
ever
e C
-IB
S: ↓
PSN
S &
↑S
NS/
PSN
S ba
lanc
e
Jarr
ett
IBS
wom
en (
n=
163,
anx
iety
: 73,
HR
V (
24-h
r H
olte
r TD
(SD
-5-m
in, R
MSS
D,
*No
diffe
renc
es in
SN
S/P
SNS
bala
nce
et a
l., 2
003
depr
essi
on: 8
6) w
ith h
isto
ry o
fm
onito
ring
)%
RR
50, S
D-5
-min
/be
twee
n gr
oups
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 8
9
Heart Rate Variability
Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
anxi
ety
and
depr
essi
ve d
isor
der v
s.R
MSS
D),
FD
(H
F, L
F,
*IB
S-A
nxie
ty &
IB
S-D
epre
ssio
n:
IBS
wom
en w
ithou
t his
tory
of
LF/H
F, s
quar
e ro
ot o
f ↓P
SNS
rela
tive
to I
BS-
Con
trol
anxi
ety
and
depr
essi
ve d
isor
der
LF/H
F)(n
=46
) al
l wom
en: 1
8–49
yea
rs
Jorg
ense
n Fu
nctio
nal a
bdom
inal
pai
n (n
=22
,A
CTH
and
ser
um c
ortis
olTD
(M
SSD
)*P
atie
nts
with
func
tiona
l abd
omin
al
et a
l., 1
993
mea
n ag
e=
37 [1
6–60
], F:
14, M
:8)
HR
and
sys
tolic
blo
od te
st,
pain
: ↑P
SNS
(RM
SSD
[ba
sal P
SNS
vs.o
rgan
ic a
bdom
inal
pai
n (n
=26
, H
RV
(ev
ery
5 m
in d
urin
g ne
ural
effe
ct])
& ↓
SNS
(red
uced
m
ean
age
=42
[18
–62]
, F:1
1,
rest
and
str
ess)
SNS
neur
al r
espo
nse)
in p
atie
nts
M:1
5) v
s.he
alth
y co
ntro
ls (
n=
14,
with
bot
h fu
nctio
nal o
rgan
ic p
ain
mea
n ag
e=
36 [
23–5
0], F
:9, M
:5)
*No
sign
ifica
nce
in H
R, S
BP,
AC
TH,
adre
nalin
e, c
ortis
ol
Kar
ling
IBS
(n=
18, m
ean
age
=31
.6
Dur
ing
supi
ne a
nd ti
lting
FD
(LF
, MF,
HF)
*Sig
nific
ant i
ncre
ased
sym
path
etic
et
al.,
199
8[2
0.6–
52.3
], F
:14,
M:4
) vs
.(u
p to
70°
)ac
tivity
(M
F): ↑
SNS
in I
BS
grou
p C
(n
=36
, mea
n ag
e=
31.4
th
an C
dur
ing
supi
ne a
nd ti
lting
[20.
8–52
.3])
*No
diffe
renc
es in
PSN
S ac
tivity
in
IBS
grou
p
Lee
C-I
BS
(n=
20, m
ean
age
=48
.9±
SSR
, RR
IV (
R-R
inte
rval
R
RIV
*C-I
BS:
↓P
SNS
(RR
IV)
than
D-I
BS
et
al.,
199
816
.3, F
:6, M
:14)
vs.
D-I
BS
(n=
20,
vari
atio
n) d
urin
g re
st a
nd
or C
dur
ing
deep
bre
athi
ngm
ean
age
=49
.2±
15.6
, F:6
, de
ep b
reat
hing
*No
grou
p di
ffere
nces
in
M:1
4) v
s.he
alth
y C
(n
=20
, ps
ycho
logi
cal d
istr
ess
mea
n ag
e=
50.7
±17
.4, F
:6, M
:14)
Orr
IB
S (n
=15
, mea
n ag
e=
34.9
±2.
1,
HR
V: 1
hr
of p
re-s
leep
FD
(LF
, HF,
LF/
HF)
*LF
is s
igni
fican
tly g
reat
er in
IB
S et
al.,
200
0F:
13, M
:2)
vs.C
(n
=15
, w
akin
g an
d 7
hr s
leep
grou
p du
ring
wak
ing.
LF/
HF
ratio
mea
n ag
e=
36.2
±2.
3, F
:13,
M:2
)is
sig
nific
antly
gre
ater
in I
BS
grou
pdu
ring
RE
M s
leep
*IB
S gr
oup
has
grea
ter
sym
path
etic
ac
tivity
dur
ing
wak
ing
and
duri
ng
RE
M s
leep
. Gre
ater
sym
path
etic
do
min
ance
in I
BS
grou
p
Thom
pson
IB
S w
omen
(n
=33
, mea
n ag
e=
37)
HR
V: 3
0 m
in o
f pre
-sle
epFD
(LF
, %H
F, L
F/H
F)*D
urin
g R
EM
sle
ep, I
BS
only
gro
up:
et a
l., 2
002
IBS
(n=
16),
IB
S +
D (
n=
17)
vs.
wak
ing
and
BD
I, G
I ↓P
SNS
rela
tive
to I
BS
+ D
and
he
alth
y C
wom
en (
n=
38,
sym
ptom
que
stio
nnai
reC
gro
upm
ean
age
=38
)*D
urin
g R
EM
sle
ep, t
he r
atio
LF/
HF
Usi
ng R
ome
I cr
iteri
ais
sig
nific
antly
hig
her
in I
BS
only
pat
ient
s
C-I
BS
=co
nstip
atio
n-pr
edom
inan
t IB
S; D
-IB
S =
diar
rhea
-pre
dom
inan
t IB
S; T
D =
time
dom
ain
anal
ysis
of H
RV
; FD
=fr
eque
ncy
dom
ain
anal
ysis
of H
RV
; BD
I =
Bec
k D
epre
ssio
nIn
vent
ory;
D =
dysp
epsi
a; M
I =
mea
n in
terv
al; M
SSD
=m
ean
squa
re s
ucce
ssiv
e di
ffere
nces
; HF
=hi
gh fr
eque
ncy;
LF
=lo
w fr
eque
ncy;
VLF
=ve
ry lo
w fr
eque
ncy;
HR
av =
mea
nof
all
aver
age
hear
t rat
e; S
SR =
sym
path
etic
ski
n re
spon
se.
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 9

1998. A total of 12 studies were identified using cri-teria of key words IBS and HRV, and publication inEnglish.All studies had healthy controls as comparinggroups. One study included an organic abdominalpain group as a comparing group as well (Jorgensenet al.).
Study populationStudies ranged from 30 to 209 total subjects, withan average sample size of 85, and a median samplesize of 60. The number of IBS subjects ranged from12 to 163, with an average sample size of 42, and a median sample size of 22. IBS subjects sometimeswere divided by stool type or severity even though a large sample size was used. Therefore, most studiesutilized a small number of subjects for analysis.
The subgroups of constipation-predominant anddiarrhea-predominant patients with IBS were toosmall to enable comparison (Karling et al., 1998).Many studies failed to clearly describe the numberand characteristics of non-participants. Some stud-ies described only age range or total mean age so itwas difficult to estimate a mean age and a median agein all studies. If selecting studies shown mean age,the mean age of study subjects was 37 years old withthe median age 36 years old. The duration of symp-toms was reported in all studies and was typicallychronic.While all subjects in six studies were women,men participated in six studies in both IBS and con-trol groups, though in smaller numbers than women.However,Adeyemi, Desai,Towsey, and Ghista (1999)used a predominantly male sample of IBS patients(26 men and 9 women) and healthy controls (12 menand 6 women).Average subjects had attained at leasta high school education. Few studies mentioned raceor ethnicity. Most studies used Caucasians.The coun-try was the US in eight studies, United Arab Emiratesin one (Adeyemi et al.), Denmark in one (Jorgensenet al., 1993), Sweden in one (Karling et al.), andTaiwan in one (Lee et al., 1998).
All but two studies (Aggarwal et al., 1994;Jorgensen et al., 1993) used Rome criteria. IBSpatients were referred to gastroenterology clinics orinstitutes of health research in five studies (Adeyemiet al., 1999; Aggarwal et al.; Elsenbruch & Orr, 2001;
Karling et al., 1998; Orr, Elsenbruch, & Harnish, 2000),outpatient clinics in two studies (Jorgensen et al.;Lee et al., 1998), and community care in the otherfive studies.Therefore, several studies mainly recruitedin a restricted geographical area. The selection sub-groups were constipation-predominant IBS versusdiarrhea-predominant IBS, postprandial pain, painseverity, functional versus organic disorders, IBS witha history of depression or anxiety versus IBS withouta history of depression or anxiety, and IBS versusIBS with dyspepsia. Four studies classified sub-groups into predominant bowel habit (Aggarwal et al.; Elsenbruch & Orr; Heitkemper et al., 2001;Lee et al.) and one study divided subgroups into post-prandial pain intensity (Burr, Heitkemper, Jarrett, &Cain, 2000). One study classified subgroups intowomen with a history of anxiety and depressionwho have IBS (Jarrett et al., 2003) and other studiesdivided into IBS versus Control.
Parameters of HRVFour studies used 24-hour Holter monitoring (Burret al., 2000; Heitkemper et al., 1998; Heitkemper et al., 2001; Jarrett et al., 2003) and other studieshave been obtained during a short period of 2–5minutes. The Heitkemper studies used all womensubjects so there is no study using both gender and24-hour Holter monitoring. Selecting between theshort and the long periods of EKG recording dependson the objective of the study. For example, a 24-hourECG recording provides an average value of eachcomponent for the entire recording period. However,there are inconsistent recordings underlying HRVbecause of sleep, exercise, deep breathing, and others(Task Force of the European Society of Cardiologyand the North American Society of Pacing and Elec-trophysiology, 1996). Also, it is important to differ-entiate responses noted under stressful conditionsand data obtained from individuals under restingconditions in short-term recording. If subjects havearrhythmia, ectopic beats, and missing data, long-termrecording is better than short-term recording. Onthe other hand, short-term recording is better thanlong-term recording if subjects do not have ectopicbeats, arrhythmia, or noise effects (Bigger et al., 1992).
H.J. Park
10 Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 10

11
Five studies tested HRV during postural changeor deep breathing or tilting (Adeyemi et al., 1999;Aggarwal et al., 1994; Heitkemper et al., 2001; Karlinget al., 1998; Lee et al., 1998) and two studies testedduring sleep (Orr et al., 2000;Thompson, Elsenbruch,Harnish, & Orr, 2002). The majority of studies usedfemale populations, so it is difficult to find a gender-difference in HRV of IBS. Also, gender-related dif-ferences in HRV have not been studied or analyzedvery well in this area. Comparisons of the vagal tonein males and females based on symptom subgroupsremain to be studied. Most studies used frequencydomain analysis; only one study used time domainanalysis (Jorgensen et al., 1993) and the other twostudies used only RR-interval (Aggarwal et al.; Leeet al.). Frequency domain analysis is a more sophis-ticated method for distinguishing between the dif-ferent components (e.g., PSNS, SNS, SNS/PSNS) inHRV than the time domain method; it would begood to compare the diarrhea-predominant with theconstipation-predominant subgroup of patients withIBS in terms of differences in ANS function.
RESULTS
There were inconsistent results in the studies. It wasdifficult to generalize the conclusions because eachstudy had a small sample size (IBS subgroup sub-jects: 10–86) and used different subgroup categoriesas mentioned before. Twenty-five women with IBShad lower vagal tone compared to 15 healthy controls(Heitkemper et al., 1998). Subjects with constipation-predominant IBS had lower PSNS tone (HF, RRIV)and elevated ANS balance (LF/HF) while those withdiarrhea-predominant IBS had greater PSNS toneand depressed ANS balance (Aggarwal et al., 1994;Heitkemper et al., 2001; Lee et al., 1998). In theHeitkemper study, there was no difference in 24-hourHRV measure between women with IBS (n = 103)compared to controls (n = 49). However, there was adifference in those women who reported severe IBSsymptoms. Therefore, certain subgroups were moreor less suitable for HRV measurement. A similar re-sult was demonstrated in patients in the constipation
group (n=27 out of 35 IBS patients) in deep breathing(Adeyemi et al., 1999). The same result was shownin women in the diarrhea-predominant group (n = 12)after a meal in Elsenbruch and Orr’s study (2001).In this study, there were no significant differencesbetween women with predominant constipation andthe control group related to meals.
Karling et al. (1998) showed significantly increasedSNS activity (MF) in the IBS group (n = 18) whencompared to the control group (n = 36) during thesupine position and tilting (head up to 70°). No dif-ferences in PSNS activity (HF) was found in the IBSgroup (Karling et al.).With regard to symptom sever-ity, HRV measurement was effective in subgroupswho reported severe and very severe symptoms(Heitkemper et al., 2001). In addition, women withsevere pain and without postprandial pain had lowervagal tone (Burr et al., 2000). Both functional andorganic abdominal pain related to reduced SNS re-sponses were shown (Jorgensen et al., 1993). Signifi-cantly greater SNS activity (LF) was shown in IBSpatients (n = 13) during waking and a significantlygreater LF/HF ratio was shown in IBS patients duringREM sleep (Orr et al., 2000). Similarly, higher SNSactivity (elevated LF/HF ratio) during REM sleepwas shown in the IBS only group (n=16) (Thompsonet al., 2002). Regarding anxiety and depression, re-duced vagal tone in women with IBS had been asso-ciated with depression and anxiety (Jarrett et al.,2003); this study provided evidence for the relation-ship between mood state and physiological indicator,which changes visceral motility.
Overall, these studies suggested changes in ANSfunction were shown in patients with IBS and maydiffer among subgroups. For example, the majorityof patients were those with alternating symptomsof diarrhea and constipation, the ANS function ab-normality was obscure. It may be there are differentresults in the alternating IBS symptom subgroup orin those who experience constipation alone. It is stillunclear if ANS function may increase GI symptomsincluding visceral sensitivity and motility alterationor is the result of abdominal pain sensitivity and dis-comfort. Pain and bloating may reflect visceral hyper-sensitivity (Ragnarsson & Bodemar, 1999).They found
Heart Rate Variability
Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 11

there was no relationship between pain/bloating andprone bowel pattern so there might be differentmechanisms in symptoms. There has been no studyregarding the relationship between bloating symp-toms and ANS function so far. The inclusion of agroup of women with bloating symptoms in a futurestudy is both critical and significant for HRV databasedevelopment and understanding of the underlyingmechanisms of IBS in IBS research.
DISCUSSION
StrengthFirstly, HRV and its components were a useful andsimple method and appeared the most suitable fordetection of changes in integrated ANS sympatho-vagal balance in both static and dynamic conditionsin IBS patients. Many studies have shown HRV wasa useful tool to assess the ANS characteristics andresponses in IBS patients because it could help dis-tinguish sympathetic from parasympathetic regulationof the sinoatrial node. Therefore, it could providevaluable information to health care providers andresearchers. The use of this methodology has provento be pathophysiologically and clinically reliable, validand more sensitive in both psychological and physi-ological variables than conventional cardiovasculartests. It may offer a unique insight, including the pos-sibility of predicting disease outcome and assessinga combination of enhanced mental load and otherstressors. It may allow monitoring of the effect oftherapeutic interventions on gut autonomic regula-tion as compared to other ANS measures. For instance,skin temperature was an insensitive measurementof sympathetic cholinergic response. Studies usinglaboratory measures of ANS function have only founddifferences when stool-type subgroups are compared(diarrhea-predominant vs. constipation-predominant)or in IBS patients with severe symptoms (Burr et al.,2000; Heitkemper et al., 2001). Also, heart rate andblood pressure were found to be less sensitive thanHRV between IBS patients and healthy controls inlaboratory testing (Heitkemper et al.; Huikuri et al.,1999; Jorgensen et al., 1993; Karling et al., 1998;
Sato et al., 1995); there is a difference using HRV asan outcome variable even though there are no dif-ferences using heart rate and blood pressure in thesame study. Thus, study of the effects of exposure to stressors may be misleading if only differences inheart rate are examined.
Secondly, HRV is an appropriate measurement instudying large populations, in both laboratory andclinical settings, and in longitudinal studies becauseit is easily and noninvasively performed. Hence sub-jects have less stress and need only minimal subjectcollaboration. In addition, it suggests cost-effectivemeasurements compared to other cardiovasculartests.
Thirdly, the analysis of continuous 24-hour ECGdata recordings allows one to observe variations oc-curring throughout the day and night for circadianpattern detection. It is a comprehensive assessmentnot only of fast, but also of slower and sometimesless regular, heart rate fluctuations. A more sophisti-cated approach to the study of HRV based on spectralmethodology proves to adequately assess the sym-pathovagal balance. In addition, it provides variousnaturalistic activities under a natural environmentrather than a laboratory environment.
LimitationsFirst of all, even though there have been progressivetechnological improvements in Holter processing sys-tems, most studies require additional human edit-ing. HRV is calculated after removal of aberrant beats.Some software packages contain an automatic defaultfiltering procedure and a removal of any aberrant beatsmanual procedure. Also, ambulatory ECG recordinghas difficulty in controlling for activity, posture, andrespiration. In addition, most software and analysismethods are different. Standardization of HRV mea-surement has remained poor even though it has beenTask force presented (Task Force of the EuropeanSociety of Cardiology and the North American Soci-ety of Pacing and Electrophysiology, 1996). There isa need for standardization in methodology to facil-itate the interpretation and comparison of results.More exact methodology is essential to extract theinformation embedded in HRV.
H.J. Park
12 Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 12

13
Secondly, there is the limitation that cardiac vagaltone may not reflect gastrointestinal vagal tone. Eventhough it is a sensitive method for balance (LF/HF)or PSNS activity (HF), it is less sensitive for SNSactivity (LF: mixed marker of SNS and PSNS) inthe GI system (Jarrett et al., 2003; Jorgensen et al.,1993). Heitkemper and coworkers (2001) have shownit is more sensitive to test ANS symptoms in womenwho report severe and very severe symptoms.There-fore, further studies of the relationship between GIand cardiac vagal tone is needed; is there any differ-ent role between GI vagal fiber and cardiac vagalfiber? Also, it would be better practice to combineHRV measures with biochemical measures such asepinephrine and norepinephrine.
Considering limitations of research design in pre-vious studies, there are issues related to subjects orcovariance variables. Several studies have small sam-ple sizes with limited statistical power. Also, severalstudies have a small number of patients across a widerange of ages, mainly recruited in a restricted geo-graphical area (Aggarwal et al., 1994; Elsenbruch &Orr, 2001; Lee et al., 1998; Orr et al., 2000). Thereare limitations in age and gender differences as wellas ovarian hormone status differences in women.As mentioned earlier, the age dependency of vagaltone is quite pronounced (Cowan et al., 1994; Jensen-Urstad et al., 1997; Thayer et al., 1998). Confound-ing variables might be responsible for IBS patients.Smoking is associated with decreased HRV so re-searchers should try to control for smoking status(Hayano et al., 1990). In addition, several studies didnot include different ethnic groups. Most studiesuse Caucasians. Moreover, control groups have notalways been matched for age and sex even thoughboth factors are known to influence ANS function(Cowan et al.; Jensen-Urstad et al.; Thayer et al.).Some studies did not control for the menstrual cycle(Orr et al.). Even though the above review demon-strates medication or other conditions contribute toHRV, medicated and unmedicated patients were notcarefully separated in some of studies; medicatedpatients are not physiologically comparable to unmed-icated patients. Some studies reported washout peri-ods for their drug free patients or included patients
who were still taking medication at the time of thestudy. Also, some studies do not have a well-definedgroup of patients characterized by the presence orabsence of other disease. Every researcher used dif-ferent criteria for recruiting subjects: community or referral clinics. Some studies (Aggarwal et al.)have Manning criteria rather than Rome criteria toensure maximum sensitivity even though Rome IIwas developed more recently than Manning criteria.
Thirdly, there are issues related to the time period.Some studies have only tested once so they need todetermine stability over time. The short term HRVmeasurement has limitations. It may not adequatelyreflect the day-to-night fluctuation in ANS responses.More complicated analysis of HRV using a long periodis necessary.
Fourthly, it was demonstrated hypnosis can pro-duce a decrease in the LF/HF ratio in cardiovasculardisease (Cowan et al., 1994). However, there is nostudy using HRV in measuring the effect of inter-vention on IBS area. In addition, most studies focuson negative emotions in the IBS field. There are nostudies showing that positive emotions can signifi-cantly influence HRV in IBS patients. Also, manyinvestigators have commonly divided subgroups onlyinto categories of pain, predominant stool type orsymptom severity and frequency, and postprandialpain. To date, there has been very little research onthe bloating symptom. In addition, there is no studyon classifying bloating subgroups using HRV mea-surement even though bloating symptoms are knownto be the most troublesome disease symptoms insome studies (Lembo et al., 1999; Talley, Howell, &Poulton, 2001). Furthermore, there is no study usingHRV in classifying constant pain groups or intermit-tent pain groups. Future research is necessary to takethese into consideration.
Finally, recent studies raise issues related to ge-netic effects on HRV in the Framingham Heart Study(Singh, Larson, O’Donnell, & Levy, 2001; Singh et al.,2002; Singh et al., 1999). In these studies, using a10 cM genome-wide scan in 725 subjects in 230extended families, including 390 sibling pairs, theyfound evidence of linkage of LF to chromosome 1 at153 cM and VLF to chromosome 15 at 62 cM even
Heart Rate Variability
Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 13

though there are limitations such as predominantlyCaucasian, laboratory evaluation, and intermediateduration recordings (2 hours). Several studies havebeen limited in genetic homogeneity of populations.
Future applicationsA novel approach for studying the abnormality ofANS function in IBS is essential. Further developedapplication of HRV measurements needs to be dis-covered. Also, further study needs to find if the IBSintervention research (both pharmacological and non-pharmacological) is associated with a dose-relateddecrease in HRV using prospective, randomized con-trolled long-term studies. A broader picture of ANSstates in IBS would require HRV with additionalchecking of the sensitivity and specificity and usingmore complicated analysis, other measures of ANSin response to a standardized laboratory stressor test,as well as ambulatory monitor recordings that mea-sure physiological responses to everyday stressors indifferent subgroups of IBS. Larger studies with a vari-ety of individuals assessing the effects of behavioralintervention and examining assessments of HRV andoutcomes are essential to determine the clinical util-ity of intervention. Moreover, gender-related differ-ences in HRV regarding IBS with a larger sample sizeare necessary. To give IBS patients the best qualityof nursing care, nursing should have multi-factorialviews for this health care problem, including physi-ological indicators such as HRV and psychologicaldistress. Nursing may bridge the gap between theory,practice, and research in future IBS study.
REFERENCES
Achten, J., & Jeukendrup,A. E. (2003). Heart rate monitor-ing: applications and limitations. Sports Medicine, 33,517–538.
Adeyemi, E. O., Desai, K. D., Towsey, M., & Ghista, D.(1999). Characterization of autonomic dysfunction inpatients with irritable bowel syndrome by means of heart rate variability studies. American Journal ofGastroenterology, 94, 816–823.
Agelink, M. W., Boz, C., Ullrich, H., & Andrich, J. (2002).Relationship between major depression and heart rate
variability. Clinical consequences and implications forantidepressive treatment. Psychiatry Research, 113,139–149.
Aggarwal,A., Cutts,T. F.,Abell,T. L., Cardoso, S., Familoni,B., Bremer, J., et al. (1994). Predominant symptoms inirritable bowel syndrome correlate with specific auto-nomic nervous system abnormalities. Gastroenterology,106, 945–950.
Akselrod, S., Gordon, D., Ubel, F. A., Shannon, D. C.,Berger, A. C., & Cohen, R. J. (1981). Power spectrumanalysis of heart rate fluctuation:A quantitative probeof beat-to-beat cardiovascular control. Science, 213,220–222.
Aubert, A., Seps, B., & Beckers, F. (2003). Heart rate vari-ability in athletes. Sports Medicine, 33, 889–919.
Bigger, J. T., Jr., Fleiss, J. L., Steinman, R. C., Rolnitzky,L. M., Kleiger, R. E., & Rottman, J. N. (1992). Fre-quency domain measures of heart period variabilityand mortality after myocardial infarction. Circulation,85, 164–171.
Bockus, H. L., Bank, J., & Wilkinson, S. A. (1928). Neuro-genic mucous colitis. The American Journal of the MedicalSciences, 176, 813–829.
Burr, R. L., Heitkemper, M., Jarrett, M., & Cain, K. C.(2000). Comparison of autonomic nervous systemindices based on abdominal pain reports in womenwith irritable bowel syndrome. Biological Research forNursing, 2, 97–106.
Burr, R. L., Motzer, S. A., Chen, W., Cowan, M. J., &Heitkemper, M. M. (2003). Logit50: A nonlinear trans-formation of pNN50 with improved statistical prop-erties. Journal of Electrocardiology, 36, 41–52.
Clemens, C. H., Samsom, M., Van Berge Henegouwen,G. P., & Smout, A. J. (2003). Abnormalities of leftcolonic motility in ambulant nonconstipated patientswith irritable bowel syndrome. Digestive Diseases andSciences, 48, 74–82.
Cowan, M. J., Kogan, H., Burr, R., Hendershot, S., &Buchanan, L. (1990). Power spectral analysis of heartrate variability after biofeedback training. Journal ofElectrocardiology, 23 (Suppl), 85–94.
Cowan, M. J., Pike, K., & Burr, R. L. (1994). Effects ofgender and age on heart rate variability in healthyindividuals and in persons after sudden cardiac arrest.Journal of Electrocardiology, 27 (Suppl), 1–9.
Delaney, J. P., & Brodie, D. A. (2000). Effects of short-term psychological stress on the time and frequencydomains of heart-rate variability. Perceptual and MotorSkills, 91, 515–524.
H.J. Park
14 Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 14

15
Elsenbruch, S., & Orr, W. C. (2001). Diarrhea- and constipation-predominant IBS patients differ in post-prandial autonomic and cortisol responses. AmericanJournal of Gastroenterology, 96, 460–466.
Gupta, V., Sheffield, D., & Verne, G. N. (2002). Evidencefor autonomic dysregulation in the irritable bowel syn-drome. Digestive Diseases and Sciences, 47, 1716–1722.
Hausken, T., Svebak, S., Wilhelmsen, I., Haug, T. T.,Olafsen, K., Pettersson, E., et al. (1993). Low vagaltone and antral dysmotility in patients with functionaldyspepsia. Psychosomatic Medicine, 55, 12–22.
Hayano, J., Sakakibara, Y., Yamada, A., Yamada, M.,Mukai, S., Fujinami,T., et al. (1991).Accuracy of assess-ment of cardiac vagal tone by heart rate variability innormal subjects. American Journal of Cardiology, 67,199–204.
Hayano, J., Yamada, M., Sakakibara, Y., Fujinami, T.,Yokoyama, K., Watanabe, Y., et al. (1990). Short- andlong-term effects of cigarette smoking on heart ratevariability. American Journal of Cardiology, 65, 84–88.
Heitkemper, M., Burr, R. L., Jarrett, M., Hertig, V.,Lustyk, M. K., & Bond, E. F. (1998). Evidence forautonomic nervous system imbalance in women withirritable bowel syndrome. Digestive Diseases and Sciences,43, 2093–2098.
Heitkemper, M., Jarrett, M., Cain, K. C., Burr, R., Levy, R. L.,Feld, A., et al. (2001). Autonomic nervous systemfunction in women with irritable bowel syndrome.Digestive Diseases and Sciences, 46, 1276–1284.
Huikuri, H.V., Makikallio,T.,Airaksinen, K. E., Mitrani, R.,Castellanos,A., & Myerburg, R. J. (1999). Measurementof heart rate variability: A clinical tool or a researchtoy? Journal of the American College of Cardiology, 34,1878–1883.
Jarrett, M. E., Burr, R. L., Cain, K. C., Hertig,V.,Weisman,P., & Heitkemper, M. M. (2003). Anxiety and depres-sion are related to autonomic nervous system functionin women with irritable bowel syndrome. DigestiveDiseases and Sciences, 48, 386–394.
Jensen-Urstad, K., Storck, N., Bouvier, F., Ericson, M.,Lindblad, L. E., & Jensen-Urstad, M. (1997). Heartrate variability in healthy subjects is related to age and gender. Acta Physiologica Scandinavica, 160,235–241.
Jorgensen, L. S., Christiansen, P., Raundahl, U., Ostgaard, S.,Christensen, N. J., Fenger, M., et al. (1993).Autonomicnervous system function in patients with functionalabdominal pain. An experimental study. ScandinavianJournal of Gastroenterology, 28, 63–68.
Karason, K., Molgaard, H., Wikstrand, J., & Sjostrom, L.(1999). Heart rate variability in obesity and the effectof weight loss. American Journal of Cardiology, 83,1242–1247.
Karling, P., Nyhlin, H., Wiklund, U., Sjoberg, M., Olofsson,B. O., & Bjerle, P. (1998). Spectral analysis of heart ratevariability in patients with irritable bowel syndrome.Scandinavian Journal of Gastroenterology, 33, 572–576.
Khaykin, Y., Dorian, P., Baker, B., Shapiro, C., Sandor, P.,Mironov, D., et al. (1998). Autonomic correlates ofantidepressant treatment using heart-rate variabilityanalysis. Canadian Journal of Psychiatry, 43, 183–186.
Kleiger, R. E., Miller, J. P., Bigger, J. T., Jr., & Moss, A. J.(1987). Decreased heart rate variability and its asso-ciation with increased mortality after acute myocardialinfarction. American Journal of Cardiology, 59, 256–262.
Kleiger, R. E., Stein, P. K., Bosner, M. S., & Rottman, J. N.(1992). Time domain measurements of heart ratevariability. Cardiology Clinics, 10, 487–498.
Lee, C. T., Chuang, T. Y., Lu, C. L., Chen, C. Y., Chang,F. Y., & Lee, S. D. (1998). Abnormal vagal cholinergicfunction and psychological behaviors in irritable bowelsyndrome patients: A hospital-based Oriental study.Digestive Diseases and Sciences, 43, 1794–1799.
Lembo,T., Naliboff, B., Munakata, J., Fullerton, S., Saba, L.,Tung, S., et al. (1999). Symptoms and visceral percep-tion in patients with pain-predominant irritable bowelsyndrome. American Journal of Gastroenterology, 94,1320–1326.
Levy, R. L., Cain, K. C., Jarrett, M., & Heitkemper, M. M.(1997). The relationship between daily life stress andgastrointestinal symptoms in women with irritablebowel syndrome. Journal of Behavioral Medicine, 20,177–193.
Mayer, E. A. (2000). The neurobiology of stress and gas-trointestinal disease. Gut, 47, 861–869.
McCraty, R., Atkinson, M., Tiller, W. A., Rein, G., &Watkins,A. D. (1995).The effects of emotions on short-term power spectrum analysis of heart rate variability.American Journal Cardiology, 76, 1089–1093.
Mertz, H., Naliboff, B., Munakata, J., Niazi, N., & Mayer,E. A. (1995). Altered rectal perception is a biologicalmarker of patients with irritable bowel syndrome.Gastroenterology, 109, 40–52.
Moser, M., Lehofer, M., Hoehn-Saric, R., McLeod, D. R.,Hildebrandt, G., Steinbrenner, B., et al. (1998). Increasedheart rate in depressed subjects in spite of unchangedautonomic balance? Journal of Affective Disorders, 48,115–124.
Heart Rate Variability
Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 15
Naliboff, B. D., Munakata, J., Fullerton, S., Gracely, R. H.,Kodner, A., Harraf, F., et al. (1997). Evidence for twodistinct perceptual alterations in irritable bowel syn-drome. Gut, 41, 505–512.
Ori, Z., Monir, G., Weiss, J., Sayhouni, X., & Singer, D. H.(1992). Heart rate variability. Frequency domain analy-sis. Cardiology Clinics, 10, 499–537.
Orr, W. C., Elsenbruch, S., & Harnish, M. J. (2000). Auto-nomic regulation of cardiac function during sleep inpatients with irritable bowel syndrome. AmericanJournal of Gastroenterology, 95, 2865–2871.
Pagani, M., Lombardi, F., Guzzetti, S., Rimoldi, O.,Furlan, R., Pizzinelli, P., et al. (1986). Power spectralanalysis of heart rate and arterial pressure variabilitiesas a marker of sympatho-vagal interaction in man andconscious dog. Circulation Research, 59, 178–193.
Parati, G., & Di Rienzo, M. (2003). Determinants of heartrate and heart rate variability. Journal of Hypertension,21, 477–480.
Ragnarsson, G., & Bodemar, G. (1999). Division of theirritable bowel syndrome into subgroups on the basisof daily recorded symptoms in two outpatients’ sam-ples. Scandinavian Journal of Gastroenterology, 34,993–1000.
Sandrone, G., Mortara, A., Torzillo, D., La Rovere, M. T.,Malliani, A., & Lombardi, F. (1994). Effects of betablockers (atenolol or metoprolol) on heart rate vari-ability after acute myocardial infarction. AmericanJournal of Cardiology, 74, 340–345.
Sato, N., Miyake, S., Akatsu, J., & Kumashiro, M. (1995).Power spectral analysis of heart rate variability inhealthy young women during the normal menstrualcycle. Psychosomatic Medicine, 57, 331–335.
Singh, J. P., Larson, M. G., O’Donnell, C. J., & Levy, D.(2001). Genetic factors contribute to the variance infrequency domain measures of heart rate variability.Autonomic Neuroscience, 90, 122–126.
Singh, J. P., Larson, M. G., O’Donnell, C. J., Tsuji, H.,Corey, D., & Levy, D. (2002). Genome scan linkage
results for heart rate variability (the Framingham HeartStudy). American Journal of Cardiology, 90, 1290–1293.
Singh, J. P., Larson, M. G., O’Donnell, C. J., Tsuji, H.,Evans, J. C., & Levy, D. (1999). Heritability of heart ratevariability: The Framingham Heart Study. Circulation,99, 2251–2254.
Talley, N. J., Howell, S., & Poulton, R. (2001). The irri-table bowel syndrome and psychiatric disorders in the community: Is there a link? American Journal ofGastroenterology, 96, 1072–1079.
Task Force of the European Society of Cardiology andthe North American Society of Pacing and Electro-physiology. (1996). Heart rate variability: Standards ofmeasurement, physiological interpretation and clinicaluse. Circulation, 93, 1043–1065.
Thayer, J. F., Smith, M., Rossy, L.A., Sollers, J. J., & Friedman,B. H. (1998). Heart period variability and depressivesymptoms: Gender differences. Biological Psychiatry,44, 304–306.
Thompson, J. J., Elsenbruch, S., Harnish, M. J., & Orr,W. C.(2002). Autonomic functioning during REM sleep dif-ferentiates IBS symptom subgroups. American Journalof Gastroenterology, 97, 3147–3153.
Tucker, P., Adamson, P., Miranda, R., Jr., Scarborough, A.,Williams, D., Groff, J., et al. (1997). Paroxetine increasesheart rate variability in panic disorder. Journal of ClinicalPsychopharmacology, 17, 370–376.
Verne, G. N., Robinson, M. E., & Price, D. D. (2001).Hypersensitivity to visceral and cutaneous pain in theirritable bowel syndrome. Pain, 93, 7–14.
Whitehead, W. E., Crowell, M. D., Robinson, J. C., Heller,B. R., & Schuster, M. M. (1992). Effects of stressfullife events on bowel symptoms: Subjects with irritablebowel syndrome compared with subjects without boweldysfunction. Gut, 33, 825–830.
Yeragani, V. K., & Rao, R. (2003). Effect of nortriptylineand paroxetine on measures of chaos of heart ratetime series in patients with panic disorder. Journal ofPsychosomatic Research, 55, 507–513.
H.J. Park
16 Asian Nursing Research ❖ March 2008 ❖ Vol 2 ❖ No 1
02-ANR-E1102.qxd 3/22/2008 4:30 PM Page 16