Embed Size (px)
Citation preview

British HeartJournal, I975, 37, I36-I49.
Delay and block of cardiac impulse caused byenhanced phase-4 depolarization in the His-Purkinjesystem
Andres Kretz,' Hector 0. Da Ruos,' and Jose R. Leguizamon Palumbo-From the Department of Cardiology, Hospital Argerich, Buenos Aires;and the Coronary Care Unit, Hospital de Vicente Lopez, Buenos Aires, Argentina
The underlying mechanism of bradycardia-dependent bundle-branch and paroxysmal atrioventricular blockappears to be enhancement ofphase-4 depolarization in a branch or in a natural or acquired monofascicularpathway.
Clinical records of these forms of impaired conduction occurring in the bundle-branches, with eitherlonger or shorter cardiac cycle lengths, are presented and analysed. These also include the combination ofMobitz type I atrioventricular block with variable degrees of bundle-branch block, as a representative ex-ample ofnarrow ventricular escape beatsfiring in the zone where prominent diastolic depolarization is present.
Spontaneous depolarization during phase-4 is theelectrophysiological mechanism which enables theautomatic cells to be effective or latent pacemakers(West, I955a, b). Occasionally, under certain patho-logical conditions, the ventricular specialized con-duction system may exhibit prominent diastolic de-polarization (Weidmann, I955; Singer, Lazzara,and HofEman, I967; Wennemark and Ruesta, I97I),the mechanism underlying bradycardia-dependentbundle-branch block (Massumi, I968; Elizari etal., I968; Sarachek, I970; Schamroth and Lewis,I971; El-Sherif, I972; Rosenbaum et al., I973b;Barold and Schamroth, I973). The development ofatrioventricular block due to enhanced phase-4depolarization (Singer et al., I967) occurs either inthe His bundle, or in a branch or division of theconducting system when the remaining routes areblocked.
Association of enhanced automaticity and im-paired conductivity owing to the development ofgeneralized diastolic depolarization in the higherparts of the main intraventricular conduction fas-cicles, may be clinically exemplified by narrowventricular ectopic beats located in the zone showingconduction delays.This paper presents electrocardiograms of pat-
Received I May I974.1 Present address: Department of Experimental Medicine,Instituto de Investigaciones Medicas, Facultad de Medicina,Universidad de Buenos Aires, Buenos Aires, Argentina.
ients with bradycardia-dependent block, which canbe explained in terms of phase-4 depolarization, anddiscussions on the concepts related to this electro-physiological mechanism based upon the corres-ponding records.
Subjects and methodsThe group consisted of i I patients, of whom 6 hadbradycardia-dependent bundle-branch block (Table i),and 5 had bradycardia-dependent paroxysmal atrio-ventricular block (Table 2). The main clinical andelectrocardiographic features are summarized in theseTables. All electrocardiograms were recorded with aSanbom Model 296 direct writing electrocardiograph ata paper speed of 25 mm/second. Vectorcardiograms inthe three-plane projections were recorded in the supineposition by the Frank system, with a Hewlett-Packard1520-A machine, using the fourth intercostal space.
Bipolar recordings of the bundle of His were obtainedas previously described (Scherlag et al., I969), with a 4Fbipolar pacing catheter. Each bipolar lead was con-nected to the AC inputs of a multichannel oscilloscopicphotographic recorder, with filter frequency set at 40and 200 cycles/sec. Records were taken at I00 mm/sec.
All analysed beats were of sinoatrial origin. RR inter-vals were measured to determine the ranges of normaland aberrant intraventricular conduction in the brady-cardia-dependent bundle-branch block. The samemeasurements were performed with the RP intervals inbradycardia-dependent paroxysmal atrioventricularblock. In several cases, slowing of the heart rate wasachieved by carotid sinus pressure.
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

Delay and block of cardiac impulse caused by enhanced phase-4 depolarization 137
TABLE i Bradycardia-dependent bundle-branch block
Case Age Sex Diagnosis Intraventricular Conduction ranges in bundleNo. (yr) conduction aberrancy Phase-3 Normal Phase 4-
block conduction block
I 47 M Coronary heart disease Left bundle-branch block 0-84-I-40 I-22-2-42 2-02-5-802 45 M Aortic disease Left bundle-branch block 0.75-118 vI6-I-303 6i F Coronary heart disease Left bundle-branch block o-62-o-80 0-70-1-42 I-34-3-564 64 M Coronary heart disease Right bundle-branch block 0-54-I-20 I-I8-2-04 I-84-4-o85 58 M Coronary heart disease Left bundle-branch block 0-52-o-84 0.74-I.28 I-20-8-026 53 M Coronary heart disease Right bundle-branch block 0-58-o-64 o-84-i-24
The conduction ranges in bundle are expressed throughout as RR intervals in seconds.
TABLE 2 Bradycardia-dependent atrioventricular block
Case Age Sex Intraventricular Diagnosis Intervals (ms) A V conduction rangesNo. aberrancy AH HV PR
Early AV cond. TardyAV block AV blockzone zone
I 29 M Right bundle-branchblock+ leftposterior hemi-block Cardiomyopathy 0-24 o-I6-0-44 0-36-I-30 I-22-I-96
2 78 M Right bundle-branchblock+ leftanterior Idiopathic chronichemiblock AV block iIo 8o O-I9 0-20-0 50 0.54-I08 I-II-2-88
3 64 F Right bundle-branchblock+ left Coronary heartposterior hemiblock disease Ioo 80 o-i8 0-24-0-34 0-32-0-64 0-56-I-I4
4 80 M Right bundle-branchblock+ left Idiopathic chronicanterior hemiblock AV block - 022 0-23-0-34 0-32-0-58 0-56-i-04
5 65 M Left bundle-branch Coronary heartblock disease - 022 o-I8-o-33 0-30-0-76 0-72-I *09
Atrioventricular conduction ranges are expressed throughout as RP intervals in seconds.
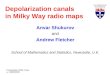
Case reportsIntermittent rate-dependent bundle-branchblockCase I Electrocardiographic and vectorcardiographicstudy (Fig. iA), performed during first admission tohospital of a 49-year-old patient with a two-year historyof angina pectoris, indicated spontaneous intermittentleft bundle-branch block and anteroseptal ischaemia. Along tracing (Fig. 2), performed a week later duringwhich vagal manoeuvres were carried out (Comeau,Hamilton, and White, 1938; Dressler, I959), showed leftbundle-branch block at the shortest and longest dias-tolic intervals; at an intermediate range the intraven-tricular conduction was normal. Three conductionranges were observed: the first, with RR intervals be-tween o084 and I'40 sec and left bundle-branch blockaberrancy; the second, between l22 and 242 sec withnormal intraventricular conduction; and the third, in
which paradoxically the left bundle-branch block re-appeared between 2'02 and 5 8o sec. In the graph (Fig.iB) obtained from the above-mentioned study, repre-senting 954 beats of sinoatrial origin, the three con-duction areas previously described are delimited: a)phase-3 left bundle-branch block (beats arriving at theleft bundle-branch during its absolute or relative refrac-tory period (Katz and Pick, 1956)); b) normal intra-ventricular conduction; and c) phase-4 left bundle-branch block (impulses reaching fibres of the left bundle-branch with reduced levels of membrane potentialcaused by spontaneous diastolic depolarization).
Sinus impulses with left bundle-branch block aber-rancy, which overlap with the beats corresponding toboth ends of the normal conduction zone, should benoted (Rosenbaum et al., 1973a; Garcia and Rosen-baum, 1972).Two months later when the patient was readmitted
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

138 Kretz, Da Ruos, and Leguizamon Palumbo
because of increased symptoms, left bundle-branchblock was registered which was not modified by changesin cardiac frequency. This electrocardiographic patternremained unchanged in follow-up examinations per-formed during the next year and a half.
This case typifies a bradycardia-dependent leftbundle-branch block which has the following out-standing features: i) intraventricular aberrancy occurring
/1-11. . ;c;
a;.0
001 HA.I
.~~~~.
a
...- - . ... .......
*S..
. * .S
., &
... .
F ...
simultaneously with pronounced prolongation of thecardiac cycle length; and 2) transitory stage of thephenomenon of bradycardia-dependent left bundle-branch block.
Case 2 A 45-year-old patient with aortic valve disease,cardiac failure, and syncopal attacks: basic tracing (Fig. 3)shows a sinus rhythm with first degree atrioventricular
A
Phase 3 m=|4mI
NC "
Phase 4LBBB
60111 11111
e.. I eel I
1O 1-4 1-8 2-2 2*6R-R1=1 ,=10, *:o0
30 3.4 38 42 46 5-0 5-4 58
B
FIG. I Panel A: Electrocardiogram and vectorcardiogram with intermittent left bundle-branchblock. In each lead the first beat is without, and the second with, left bundle-branch block.Inverted T waves in leads Vi to V4 are observed in the normal conducted beats. Panel B: Graphicrepresentation of 954 conducted beats with normal intraventricular conduction, and left bundle-branch block aberrancy according to their corresponding RR intervals. Time intervals are
depicted in hundredths of seconds. NC, normal conduction; phase-3 LBBB, phase-3 leftbundle-branch block; phase-4 LBBB, phase-4 left bundle-branch block; RR, RR intervals.
'll'1
a .9 . .. 9 I 9 1- 9 I .- I- 1- I . 9 I 9 I 9 I . 9 9 --r---T-l"
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

Delay and block of cardiac impulse caused by enhanced phase-4 depolarization 139
.... ... . ....,: 11
.....E.. ........::g:l::|:- alz
::'....'.... ... .... .: ....... .... ......:::1::::1::1::::1 :1':
L... ... ,.. _....... .... _ U.AlwXo llm :1:::::::::::; :; ::1:: :: :::l::1::1::1::1:::::::6::::
}_PH-4LBBW0R-R
134 208
FIG. 2 A to E, discontinuous record of lead I. Tracings of conducted sinus beats presentingnormal and aberrant QRS complexes with left bundle-branch block pattern according to pre-vious cycle length. The distribution of the mentioned beats are schematically represented at thebottom of this figure. See text for further explanation. NC, normal conduction; PH-3 LBBB,phase-3 left bundle-branch block; PH-4 LBBB, phase-4 left bundle-branch block; RR, RRintervals.
block (PR 0-28 sec) left ventricular hypertrophy, andincomplete left bundle-branch block. An electrocardio-gram performed two days later (Fig. 4) shows, in stripsA, B, and C, conducted beats preceded by identical Pwaves with constant PR intervals and different degreesof left bundle-branch block starting from an RR intervalof i i6 sec. The variability of conduction disturbance isdirectly related to the previous diastolic pause; greaterdegrees of left bundle-branch block aberrancy are pre-ceded by longer RR intervals.
In strip D an increase in the sinus frequency estab-lishes a 2:I atrioventricular block and the conductedbeats also present variable degrees of left bundle-branchblock.A new record obtained three days later (Fig. 5A)
showed different degrees of bradycardia-dependent leftbundle-branch block and the appearance of narrow ven-tricular escape beats with pure incomplete right bundle-branch block pattern starting from an RR interval of
I-30 sec. In addition, atrioventricular dissociation with asimilar ectopic rhythm firing at a rate of about 5o/minwas recorded during the same study (Fig. 5C). Twomonths later, while the patient was receiving digitalis(Fig. 6, strip A), prolongation of first degree atrio-ventricular block up tO 0-32 sec was noticed. In strip B,an increment of the sinus frequency causes a seconddegree atrioventricular block with a 3: 2 and 4: 3 Luciani-Wenckebach ratio. The fluctuations in diastolic pausesoriginated by the dropped P waves determine the appear-ance of variable degrees of left bundle-branch block in thebeats, which reinitiate the cycle maintaining a constantPR interval of 0-32 sec. In strip C a further increase inthe sinus frequency establishes a 2:i atrioventricularblock with similar characteristics to the one observed inFig. 4, strip D. During this study a vectorcardiogramwas performed simultaneously, registering beats ofsinoatrial origin with progressive left bundle-branchblock aberrancy.
..........!, .... .... .+.,......
.. ..,. .... .... ..._ .... _:_ =..
A.]
B.
C.
D.
E.
.. ....
___ *': .-. ... ... _..__......... .... .... ..._-... .... ... .........
4}:
f1-
PH:...LB N580
1;!:- 1; E 1! 7.7, -.-r.. ... ... ETET f"
iiii :li" r: I'l -,t::P -A.iA
.... ....
........
nn... ... .... N.... .. .... ....
7:- 77' -T .......
....
=T :':
....
':::;:::
.:: i ............. O.......
_...-.-.,....
.... t:i:::: :1
* .. :X::::I:::,.::...::..7 _ .
..
vooe
....
*-t*---1-1 1T**':1::t:1:
CI:::7n.:., ....1.1:
1::1::::1:
Ak .17 71T,
77 '77
17 77'l_
::::
,
1::::..
l'''
1::::a;L
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

1140 Kretz, Da Ruos, and Leguizamon Palumbo
* p~~~~~~~~~~4
% D
F lot
a 40 4a 4D ft
dw ip
dwdop
dppl0 40p.
0*01 0,
HO*QJI
FIG. 3 Electrovectorcardiogram shozoing sinus rhythm, left ventricular hypertrophy, andincomplete left bundle-branch block with first degree atrioventricular block.
1241"Wl 21 I fro104 -104. 1128 IB ,1"Tj :i-1 777TI1
ft
LiI~~~~~~~~~.il.A16ffi ~-' - -.r Z ~ -r
kmjpge!!.-. WOOW-M-F-...I 1, !- 7-1
:: " -:D. :: i:''. I..
fI ~ --
VT I:
FIG. 4 Electrocardiogram (discontinuous strips of standard lead I) showing inA, B, C,and D,variable degrees of left bundle-branch block aberrancy related to previous cycle length. See text
for further explanation.
C,
2 1001A 14~I1 ..1-T.-Ti ,- --T-
I.-4---
---.iw-rONii.l !-;. lr,
A I
I
I A.1'.- . 1-. 7I ;.I .A6 .!,
a 1-
-A
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

Delay and block of cardiac impulse caused by enhanced phase-4 depolarization 141
B.
I _~~~~~~~~~~~~~~o_- I4 LZ-r ; _ :_rl-
*.wo!
a11
_. ......,,....., ,_,. .
'41_;-~ - - -- .... ! ! ; _ ..................... . . . . . . ... < , , C - ! - S ! t ..........................._..!....*.,, ------..._i.;. :ii:::'.:.:.i,::.1.:..;.:.ii
....--- J'.. i'-- A t..'- t'- !-t !f-.t..r;:, -q- 1 . F ,............................................................................................t....... i-124 j 11J 8i --.,--'-'-''0t -- :'- -- '---:---128 --'v ' O t3 11--,-0---l-i,'~~- ~
,_,,,,V,,_ _ .LI .- -', -'i''. ±,' '.'jI-----'......:
~~~-L F_l E2FIG. 5 Panel A: Simultaneous recording of leads I and Vi. Variable degrees of bradycardia-dependent left bundle-branch block developed during induced slowing of the heart rate (carotidsinus pressure). Appearance of narrow ventricular escape beats exhibiting pure incomplete rightbundle-branch block aberrancy, preceded by diastolic intervals exceeding rP28 sec. Panel B:Twelve lead electrocardiogram of narrow ventricular escape beats with pure incomplete rightbundle-branch block pattern. Panel C: Atrioventricular dissociation. Narrow ventricular ectopicrhythm with pure incomplete right bundle-branch block configuration discharging at a rate ofabout 50 beats/min. (RR intervals are indicated in hundredths of seconds.)
This case presents the following outstanding features:i) variable degrees of aberrant intraventricular conduc-tion, taking place conjointly with slight increases in car-diac cycle length; 2) coexistence of Luciani-Wencke-bach phenomenon with variable degrees of bradycardia-dependent left bundle-branch block; 3) differing degreesof phase-4 left bundle-branch block, associated withnarrow ventricular ectopic beats exhibiting pure in-complete right bundle-branch block configuration; 4)inability to obtain phase 3 left bundle-branch block(tachycardia-dependent left bundle-branch block) be-cause of the development of 2: i atrioventricular blockwhen heart rate is increased.
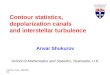
Rate-dependent atrioventricular blockCase I A 27-year-old man with Chagasic cardiomyo-pathy had sinus arrhythmia and advanced atrioventricularblock, requiring a permanent demand type pacemaker.During his stay in hospital paroxysmal episodesof atrioventricular block were observed (Fig. 7), whichaltemated with complete atrioventricular block and i: Iatrioventricular conduction. The electrocardiogram(Fig. 8A) clearly reflects disturbances of the intra-ventricular conduction characterized by a PR interval of0o24 sec and right bundle-branch block, with block in the
posterior inferior division of the left bundle-branch (leftposterior hemiblock). In a long tracing recorded during aseries of syncopal attacks (Fig. 7A), it may be observedthat the first conducted sinus impulse (Ist) is followedby an episode of sinus depression which initiated a periodof ventricular asystole, interrupted by a notched P wave(2nd) representing a blocked atrial beat with an RPinterval of I-34 sec. The following P wave (3rd) is alsoblocked, thus resulting in a diastolic pause which isterminated by a ventricular escape beat. The next sinusimpulse (4th) which follows the escape beat is conductedto the ventricles with an RP interval of o 50 sec, thesucceeding two atrial beats (5th to 6th) also being con-ducted. Then a new episode of sinus depression producesa similar sequence which is repeated in strips A and B.Periods of ventricular asystole varying in duration from2-55 to 8-2o sec, provoked either by spontaneous sinusdepression (strips A and B), or premature artificial stim-ulus (strip C), can be observed all through this figure.To establish the range of propagation and blockage of
atrial impulses in the atrioventricular conductionsystem, I224 beats were analysed (Fig. 8B). Theimmediate post-escape conduction was tabulated inde-pendently and PP and PR intervals were also measured.Atrial post-escape impulses (Fig. 8B above dotted line)
! .: ;. 1, ..,. .;: .; !-TI;.T,-T.: .': I, I 1; f-- I 1-. ..- L. '-.-j - -I ---.
,= :.1
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

142 Kretz, Da Ruos, and Leguizamon Palumbo
A-1
"0 H H
FIG. 6 Three strips of lead I selected from continuous record. A) Sinoatrial beats with first
degree atrioventricular block. B) Variable degrees of bradycardia-dependent left bundle-branch
block in the first sequence beat of Luciani-Wenckebach period. C) 2:i atrioventricular block with
different degrees of left bundle-branch block aberrancy according to previous diastolic length.Bottom: Vectorcardiogram: horizontal plane. From right to left, different degrees of leftbundle-branch block.
.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~1
.........
FIG. 7 Panels A and B: Short and longer runs of paroxysmal atrioventricular block all
initiated by spontaneous sinus depression. Panel C: Same event induced by artificial prema-
ture atrial impulse (arrow). See text for further explanation.
B.
I,e/$H
-- ---: -.; ----:- .:
-! I.: fi.. ': 1:.-A--
1 .. I.,.: i. ..T:. 'I. .'::: I .:.. ::A
ow H
;- - 1; p- ].:::: :: :. -- -;.:1: .. ::.: .:. .:111111:.:::,:::..:.: ::::-: ::..
.':1- 1----, -1 " - :,,I, I.,
I:. .:. .1. :, .:. ..:9 .... !: -I 1. .;. ;. .: .: :. .: ': .. I :.a: :.. :, Ii :. .;. ,: ,:,, .!I !I ,:. I:. " a .: .: . "
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

Delay and block of cardiac impulse caused by enhanced phase-4 depolarization I43
present an early atrioventricular blocked zone; anotherone of conducted beats; and a third late atrioventricularblocked zone. The rest of the studied beats (Fig. 8Bbelow dotted line) show an atrioventricular conductionzone followed by another one of blocked beats. In thisgroup, early atrioventricular blocked zone is not ob-served, since spontaneous ventricular asystole wasalways initiated by depression of the sinus pacemaker.
'.. ,. ......
.... ...............!, .' :A ..
I A ~ %4
v.s 'vf __ v|i v :*;-a,..i. ......B.
,:...,..'_..:..;_;;; _;. ::.' :::;::. ': :.. '.:,: ,:.'....; .5.'.: !.... '... s~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.Y.,wt.:.! 5 ' ........ ........
.--
.4,
A
A-V Block
A-V Cond
A-V Block
S
Analysing all the beats in the graph corresponding toFig. 8B, the existence of a conduction zone and twoblocked areas can be seen. Blocked atrial impulses over-lapping the beats corresponding to both ends of theatrioventricular conduction zone may be observed.Sinus impulses (below dotted line) which occur after anRP interval longer than I 20 sec or shorter than o-4o sec,are blocked, and those (above dotted line) occurringwith an RP interval between o 4o sec and 130 sec after aventricular escape beat, are conducted. Therefore, onlyatrial impulses which follow a ventricular escape beat oranother supraventricular conducted beat within a lim-ited period are transmitted to the ventricles.This case exemplifies paroxysmal atrioventricular
block; its more remarkable features being: i) episodes ofparoxysmal atrioventricular block originated by changesin atrial frequency; 2) a ventricular escape beat followedby sinus impulse with an adequate time relation to re-initiate the atrioventricular conduction; 3) transitorinessof paroxysmal atrioventricular block periods, altematingwith i: i atrioventricular conduction and completeatrioventricular block.
Case 2 This 78-year-old patient had Adams-Stokesepisodes before his paroxysmal atrioventricular blockwas recognized. These disappeared after the implanta-tion of a pacemaker. Electrocardiogram and vector-cardiogram on admission (Fig. 9) showed right bundle-
H branch block with left anterior hemiblock, and a PRinterval of o I9 sec; it should also be stressed that a pro-longed HV time of 8o msec was recorded.
A-V Cond
AV Block
I.e0o0*[email protected] 00.0.0. 000 I II
0 @011lllll
0-1 0-2 0*3 0-4 0o5 0b 0>7 0:8 0-9 1-o 1-1 1:2 1-3 14 1s5 1.7 1-8 1-9 2-0R-P
1=1 ,= 10,0=lCOB
FIG. 8 Panel A: Electrovectorcardiogram of right bundle-branch block with left posteriorhemiblock and first degree atrioventricular block. Panel B: Graphic representation of RPintervals corresponding to 1224 conducted and non-conducted supraventricular impulses. Post-escape conducted and blocked beats are above the dotted line. Time intervals are depicted inhundredths of seconds. See textfor detailed discussion. Abbreviations, A-V block, atrioventricu-lar block; A-V cond, atrioventricular conduction; RP, RP intervals.
I"000 *.0.....***" I000. II o@001Ill
I..1 Ii
.-A"--.V--
0
r,
I
I0 *" * 1I
lm- .60elillillF=1111,
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

xt4 Kretz, Da Ruos, and Leguizamon Palumbo
Fig. io, corresponding to episodes of paroxysmalatrioventricular block, indicates how the acceleration or
decrease of atrial frequency gives rise to periods of ven-
tricular asystole. Atrioventricular conduction is re-
established when a P wave, occurring after the ven-
tricular escape beat, and maintaining a critical RP inter-
val with the latter, is conducted to the ventricles.
To determine the range of conduction or blockage in
the atrioventricular conduction system, 628 atrial beats
were studied, delimiting: a) a blocking range between
0-20 and o-5o sec: b) an atrioventricular conduction
range from 0-54 to i -o8 sec, and again c) a blocking range
between i.ii and 2-88 sec.
This case presents the following features: i)
paroxysmal atrioventricular block caused by variations
of the atrial frequency; 2) termination of the atrio-
ventricular block episode conditioned by the appearance
of a ventricular escape beat and its timing with the first
~~~~1I~~~~ il Fl
%\
%% I
If
H
A H H
FIG. 9 Electrocardiogram and vectorcardiogram Of right bundle-branch bloch with leftanterior hemibloch and a PR interval of o1i9 sec. Bottom tracing: His bundle electrogram(HBE) recorded simultaneously with lead IL.
-~~~~~~~~~777-.7--7
I.-. P1~~~~~~~~~~~~~~~~~~
FIG. 10 Short runs ofparoxysmal A Vblochkinitiated (VI) by sinus depression and (V2) by a
bloched atrial premature beat.
KIT~~ .-r"'i"'i'vTi_jAV .~~~~~MPt P
m- ,.- ... " I''. 11- ''I ...I.... -1 .!; L 11 L 1- T .. '.I .' ::.I ..i I..t :1 1- 1 :.. ::'' w. .im::.1..11. 111111, -1. r :, i. -..l 1: !. :1 A 1: I
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

Delay and block of cardiac impulse caused by enhanced phase-4 depolarization I45
conducted P wave; 3) intraventricular trifascicularblock, with a normal PR interval and a prolonged HVtime (Narula et al., I971), indicating delayed conductionprobably in the main left bundle or in its posteriordivision; 4) episodes of paroxysmal atrioventricular blockinterposed with I: I atrioventricular conduction andcomplete atrioventricular block.
DiscussionImpulse propagation in incompletely repolarizedfibres of the His-Purkinje system caused by pro-longation of the refractory period, or in fibres whichdevelop phase-4 depolarization, may be affected so
as to result in significant delay or block.Under certain experimental and clinical
pathological conditions: hypoxia and ischaemia(Trautwein and Dudel, I956); increased stretch(Dudel and Trautwein, 1954; Singer et al., I967);and contusion of the intraventricular branchingsystem (Kretz and Da Ruos, 1972), the cardiaccycle length variability constitutes an outstandingfactor in the development of different forms ofimpaired conduction, making evident that bothphase-3 and phase-4 block may be detected, differ-entiated, and their evolution determined by clinical(Massumi, I968) and experimental electrocardio-graphy. Therefore, pronounced decrease in cardiacfrequency may determine paradoxical blockages ofbranches or divisions, owing to the development ofphase-4 depolarization (Case i, Fig. 2). Similarly,delay or interruption in the above-mentionedsystem may also be evidenced by slight prolonga-tion of the cardiac cycle length (Case 2, Fig. 4)which has been attributed by Singer and Ten Eick(I97I) to the probable combination of enhancedphase-4 depolarization and diminished membraneresponsiveness.
Since the ascending slope of spontaneous dias-tolic depolarization is gradual, the appearance ofconducted sinoatrial beats with varying degrees ofbundle-branch block aberrancy developing withincreases in cycle length, may be attributed toatrial impulses reaching the affected fascicle atdifferent levels of diastolic depolarization. Suchelectrocardiographic derangements in the leftbundle-branch (Fig. 4) were clinically recorded. Thereproducibility of such phenomenon in the canineintraventricular bundle-branch system was alsoachieved in our laboratory (Kretz, Da Ruos, andLeguizam6n Palumbo, I974). This finding con-
firms the hypothesis that different degrees of de-cremental conduction obtained with a slow heartrate are produced by the following basic mech-anism: fluctuations in level of transmembranepotential caused by variations of spontaneous
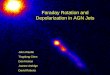
diastolic depolarization in the contusion affectedcells of the corresponding fascicle. In almost all thecases presented in this paper (Table i) clear evi-dence of prolonged recovery associated with spon-taneous diastolic depolarization was recorded (Fig.ii), indicating that such electrophysiological mech-anisms coexist, both at the level of the higher partsof the main intraventricular conduction fascicles andin their peripheral ramifications (Elizari, Lazzari,and Rosenbaum, I973) as well.The development of bradycardia-dependent block
in the branching portion of the intraventricularconduction system, caused by prolongation of thecardiac cycle length caused by a Mobitz type I or IIatrioventricular block, has been pointed out (vonHoesslin, 1923; Scherf and Scharf, 1948; Vesell andLowen, I963; Sherf and James, I969; Sepulveda,Rosselot, and Ahumada, I969; Schamroth andLewis, I971; Friedberg, I97I; Mazzoleni andFletcher, I971; Gallagher et al., I973). Clinicalevidence of this association is shown in Fig. 6,strip B, where Luciani-Wenckebach periods, withvarying degrees of left bundle-branch block aber-rancy in the first sequence beat, are observed(Friedberg, I972). Likewise, the coexistence ofphase-4 block with Mobitz type I form of decre-mental conduction has been reproduced in bothdivisions of the canine left bundle-branch (Kretzand Da Ruos, I972).
Considering that recent electrophysiologicalstudies (Bailey et al., I972; Myerburg, Nilsson, andGelband, 1972) carried out on bundle-branch andPurkinje muscle preparations have indicated thatspontaneous diastolic depolarization occurs withinthe bundle-branches, it can be expected that en-hanced phase-4 depolarization confined to a groupof automatic cells within the main left bundle-branch, might create an ectopic pacemaker (Hoff-man, I966; Drake, Skom, and Singer, I97I).Narrow ventricular ectopic beats arising from suchanatomical origin were recorded in one of ourpatients (Case 2, Fig. 5). This interpretation isbased on Rosenbaum's classification of ventricularextrasystoles (Rosenbaum, I969). Our case accord-ing to QRS pattern and classical criteria (Sodi-Pallares, Bisteni, and Medrano, I964) correspondsto pure incomplete right bundle-branch block con-figuration (Fig. sB), thus suggesting a site of originwithin the main left bundle-branch (Rosenbaumet al., I970b; Puech et al., I97I).
Since narrow ventricular ectopic beats do arise atthe ventricular level from the higher parts of themain intraventricular conducting fascicles, it maybe assumed that when diastolic depolarization de-velops in such areas, an association of impaired con-ductivity is most likely; therefore transmission of
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

146 Kretz, Da Ruos, and Leguizamon Palumbo
Al.
D. r-
FIG. II (Case 6). Transient rate-dependent right bundle-branch block during the course of anacute myocardial infarction. Panel A. Twelve-lead electrocardiogram showing diaphragmaticinfarction and Mobitz type I atrioventricular block. Panel B obtained the same day revealsventricular tachycardia. After direct current cardioversion, a transient right bundle-branchblock was recorded (panel C). In panel D (leads I and Vi) recorded 2 minutes later, each longventricular diastolic pause caused by an induced ventricular complex (s) or by a dropped beat isfollowed by an atrial complex with a similar right bundle-branch block configuration (phase-4bloch). Note progressively decreasing degrees of right bundle-branch aberrancy of beats closingcycles of o64 sec or shorter in duration (phase-3 block). Since ischaemic injured Purkinje cellsmay develop generalized diastolic depolarization concomitantly with prolonged phase-3, consis-tent block of the impulse in the right bundle-branch can be explained by assuming the presence oftwo different mechanisms that alternate with each other. Normal intraventricular conductionwas restored 4 minutes later (strip E).
the atrial impulse through such enhanced phase-4areas must be delayed or blocked (Watanabe, I97I).This assumption appears to be strongly supportedby the findings previously reported (Fig. 5A),where sinus beats showing variable degrees ofbradycardia-dependent left bundle-branch blockcoexisted with narrow ventricular ectopic beatswith pure incomplete right bundle-branch block.Variations in the spontaneous firing rate of such
centres of impulse formation can be explained bychanges in levels of diastolic membrane potential inconjunction with variations in the extent of phase-4depolarization and variability of the thresholdpotential (Singer et al., I967) in the cells locatedwithin the boundaries of the main left bundle-branch.The development of phase-4 depolarization in
the monofascicular pathway (His bundle), or in a
-fe v V3 <AL V5
V2 .... :
VR F1; _.: 8,4, 88 .- ,90 .::-:92-'6.2-.116 11' ', ,,t8_........... :, :'
i''. _ ... 120 E. _&; '.'.''.''.;@i,,i,.t*,................................_ _ k _ I . i ,::.:: i. :1 i.,
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

Delay and block of cardiac impulse caused by enhanced phase-4 depolarization 147
branch or division confronted by blockage of theremaining fascicles, will give rise to bradycardia-dependent atrioventricular block (Singer et al.,I967). Disturbance of the atrioventricular conduc-tion assigned to this mechanism has been referredto in recent reports: in monofascicular atrioventricu-lar block (Slama et al., I969), in bifascicular atrio-ventricular block (Coumel et al., I97I), and intrifascicular atrioventricular block, both clinically(Rosenbaum et al., I973c) and experimentally (DaRuos et al., I97I).
All these, because of their clinical features, havebeen included in the paroxysmal atrioventricularblock group (Sachs and Traynor, 1933), and areoutstanding because of the sudden appearance ofatrioventricular block, caused by acceleration or de-crease of atrial frequency. Atrioventricular conduc-tion is resumed after the escape of a subsidiary pace-maker, the latter keeping an adequate timing withthe first atrial impulse which is conducted to theventricles. These peculiarities observed in all ourclinical (Fig. 7 and io) and experimental (Da Ruoset al., I971) cases lead us to assume that this ven-tricular escape beat would have the function of de-polarizing by retrograde conduction the blockedphase-4 fascicle, thus permitting the reinitiation ofanterograde atrioventricular conduction (Rosen-baum et al., 1973c).From the findings in Tables i and 2 it seems that
the bradycardia-dependent bundle-branch andatrioventricular block have common character-istics: a) a premature blocked zone, b) another oneof conduction, and c) a tardy block zone. Thepresence of late blocking evidenced in branches by abradycardia-dependent block of the affected fascicleor a bradycardia-dependent atrioventricular block,when occurring in a normal or acquired mono-fascicular pathway, is significant. It may be in-ferred from the above that the existence of a com-mon mechanism attributable to prominent phase-4depolarization appears to be a plausible explanationfor the late blocking zone in bradycardia-dependentforms of impaired conduction.
In our cases of bradycardia-dependent atrio-ventricular block, supernormality cannot be' in-voked, since a wide range of atrioventricular con-duction has been observed (Table 2) (Lewis andMaster, 1924). In spite of the fact that repetitiveconcealed conduction of atrial impulses may pro-voke prolonged periods of ventricular asystole(Langendorf and Pick, I964; Chung, 197I), thisreport establishes the close relation between theprolongation of the cardiac cycle length and the de-velopment of enhanced phase-4 depolarization asthe underlying mechanism of the bradycardia-dependent paroxysmal atrioventricular block. There-
fore, it is unlikely that, in our cases, ventricularasystole may be attributed to concealed conduction(Moore, Knoebel, and Spear, I971).As chronic trifascicular atrioventricular block is
often preceded by blockage in two or more of thethree fascicles of the bundle-branch system (Rosen-baum et al., I97oa), the most probable site wherebradycardia-dependent paroxysmal atrioventricularblock will develop in patients with right bundle-branch block coexisting with left anterior orposterior hemiblock and a prolonged HV interval(Table 2) seems to be in the main left bundle or inone of its principal subdivisions. This has beenexperimentally proved in the canine heart (DaRuos et al., 1972). Bradycardia-dependent paroxys-mal atrioventricular block as a forerunner of com-plete atrioventricular block was almost invariablyobserved in our clinical cases. Therefore, an under-standing of this type of impaired conduction may beclinically important because of the therapeutic valueof cardiac pacemakers.The advice and encouragement of Dr. F. Batlle, Direc-tor of the Department of Cardiology and Dr. C. A.Bertolasi, Chief of the Coronary Care Unit, HospitalCosme Argerich, are gratefully acknowledged.
ReferencesBailey, J. C., Greenspan, K., Elizari, M. V., Anderson, G. J.
and Fisch, C. (1972). Effects of acetylcholine on auto-maticity and conduction in the proximal portion of theHis-Purkinje specialized conduction system of the dog.Circulation Research, 30, 2IO.
Barold, S. S., and Schamroth, L. (I973). Tachycardia-dependent left bundle branch block associated withbradycardia-dependent variable left bundle branch block:a case report. Circulation, 48, 2I6.
Chung, E. K. (I97i). A reappraisal of concealed atrioventricu-lar conduction. American Heart_Journal, 82, 408.
Comeau, W. J., Hamilton, J. G. M., and White, P. D. (I938).Paroxysmal bundle-branch block associated with heartdisease; a review and an analysis of the literature, with I3new cases and notes upon the influence of the vagus.American Heart Journal, I5, 276.
Coumel, P., Fabiato, A., Waynberger, M., Motte, G., Slama,R., and Bouvrain, Y. (I97i). Bradycardia-dependentatrioventricular block. Journal of Electrocardiology, 4, I68.
Da Ruos, H. O., Kretz, A., Elizari, M. V., Lazzari, J. O., andRosenbaum, M. B. (197I). Bloqueo auriculo-ventricularexperimental relacionado con despolarizaci6n diast6licaespontanea en fase-4 (abstract). Medicina (Buenos Aires),31, 545.
Da Ruos, H. O., Kretz, A., Leguizam6n Palumbo, J. R.,Irigoyen, E. H., Sosa, J. M., and Schnetzer, E. (1972).Bloqueo A-V bradicardico-dependiente. Correlaci6nclinico experimental (abstract). Medicina (Buenos Aires),32, 715.
Drake, F., Skom, J., and Singer, D. H. (I97I). Aberrationoccurring in conjunction with minimal changes in cyclelength. Cited by Singer et al. in American Journal ofCardiology, 28, 38I.
Dressler, W. (1959). Transient bundle branch block occurringduring slowing of the heart beat and following gagging.American Heart_Journal, 58, 760.
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

148 Kretz, Da Ruos, and Leguizamon Palumbo
Dudel, J., and Trautwein, W. (I954). Das Aktionpotentialund Mechanogramm des Herzmuskels unter dem Einflussder Dehnung. Cardiologia, 25, 344.
Elizari, M. V., Lazzari, J. O., and Rosenbaum, M. B. (i973).Phase-3 and phase-4 intermittent left anterior hemiblock.Chest, 62, 673.
Elizari, M. V., Rosenbaum, M. B., Lazzari, J. O., Kretz, A.,Da Ruos, H. O., and Leguizam6n Palumbo, J. R. (i968).Evidencias clinicas de un nuevo mecanismo electrofisio-l6gico en la patologia de la conducci6n. Segundo CongresoNacional de Cardiologia, Rosario, Argentina.
El-Sherif, N. (I972). Tachycardia-dependent versus brady-cardia-dependent intermittent bundle-branch block.British Heart Journal, 34, i67.
Friedberg, H. D. (197I). Mechanism of the Wedenskyphenomena in the left bundle branch. American Journal ofCardiology, 27, 698.
Friedberg, H. D. (1972). Observations on the duration ofWedensky facilitation in the left bundle branch. J'ournal ofElectrocardiology, 5, i85.
Gallagher, J. J., Damato, A. N., Varghese, P. J., Caracta,A. R., Josephson, M. E., and Lau, S. H. (I973). Alterna-tive mechanisms of apparent supemormal atrioventricularconduction. American Journal of Cardiology, 31, 362.
Garcia, H., and Rosenbaum, M. B. (I972). El 'efecto fuelle'en los bloqueos intermitentes de rama. Revista Argentinade Cardiologia, 40, 75.
Hoffman, B. F. (I966). The electrophysiology of the heartmuscle and the genesis of arrhythmias. In Mechanisms andTherapy of Cardiac Arrhythmias, p. 27. Ed. by L. S.Dreifus and W. Likoff. Grune and Stratton, New York.
Katz, L. N., and Pick, A. (1956). Clinical Electrocardiography,Part I. The Arrhythmias. Lea and Febiger, Philadelphia.
Kretz, A., and Da Ruos, H. 0. (I972). Experimental Luciani-Wenckebach phenomenon in the anterior and posteriordivisions of the left bundle branch of the canine heart.American Heart Journal, 84, 5I3.
Kretz, A., Da Ruos, H. O., and Leguizam6n Palumbo, J. R.(1974). Conduction disturbances due to enhanced phase 4depolarization in the bundle branches of the canine heart.To be published.
Langendorf, R., and Pick, A. (I964). Causes and mechanismsof ventricular asystole in advanced A-V block. In SuddenCardiac Death, p. 97. Ed. by B. Surawicz. Grune andStratton, New York.
Lewis, T., and Master, A. M. (I924). Supernormal recoveryphase, illustrated by two clinical cases of heart-block.Heart, II, 371.
Massumi, R. A. (I968). Bradycardia dependent bundlebranch block: a critique and proposed criteria. Circulation,38, io66.
Mazzoleni, A., and Fletcher, E. (I97I). Facilitation of conduc-tion in left bundle of His. British Heart3journal, 33, 970.
Moore, E. N., Knoebel, S. B., and Spear, J. F. (I97I). Con-cealed conduction. American Journal of Cardiology, 28, 406.
Myerburg, R. J., Nilsson, K., and Gelband, H. (I972).Physiology of canine intraventricular conduction and endo-cardial excitation. Circulation Research, 30, 217.
Narula, 0. S., Scherlag, B. J., Samet, P., and Javier, R. P.(I97I). Atrioventricular block. Localization and classifica-tion by His bundle recordings. American Journal ofMedicine, 50, 146.
Puech, P., Grolleau, R., Latour, H., Dufoix, R., Cabasson, J.,and Robin, J. (197i). Enregistrement de l'activite de labranche gauche du faisceau de His par voie endocavitaire.Archives des Maladies du Coeur et des Vaisseaux, 64, IO.
Rosenbaum, M. B. (I969). Classification of ventricular extra-systoles according to form. Journal of Electrocardiology, 2,289.
Rosenbaum, M. B., Elizari, M. V., Kretz, A., and Taratuto,
A. L. (197oa). Anatomical basis of A-V conduction dis-turbances. Geriatrics, 25, No. II, 132.
Rosenbaum, M. B., Elizari, M. V., Lazzari, J. O., Halpern,M. S., Nau, G. J., and Levi, R. J. (I973a). The physio-logical basis of intermittent bundle branch block. InCardiac Arrhythmias, p. 349. Ed. by L. S. Dreifus andW. Likoff. Grune and Stratton, New York and London.
Rosenbaum, M. B., Elizari, M. V., Lazzari, J. O., Halpern,M. S., Nau, G. J., and Levi, R. J. (I973b). The mechanismof intermittent bundle branch block: relationship to pro-longed recovery, hypopolarization and spontaneousdiastolic depolarization. Chest, 63, 666.
Rosenbaum, M. B., Elizari, M. V., Levi, R. J., and Nau, G. J.(1973c). Paroxysmal atrioventricular block related tohypopolarization and spontaneous diastolic depolarization.Chest, 63, 678.
Rosenbaum, M. B., Halpern, M. S., Nau, G. J., Elizari,M. V., and Lazzari, J. 0. (I97ob). The mechanism ofventricular ectopic beats. In Symposium on CardiacArrhythmias, p. 223. Ed. by E. Sand0e, E. Flensted-Jensen, and K. H. Olesen. AB Astra, SodertalIje, Sweden.
Sachs, A., and Traynor, R. L. (I933). Paroxysmal completeauriculo-ventricular heart-block. American Heart j3ournal,9, 267.
Sarachek, N. S. (1970). Bradycardia-dependent bundlebranch block. American Journal of Cardiology, 25, 727.
Schamroth, L., and Lewis, C. M. (I97I). Normalization of abundle branch block pattern in early beats. journal ofElectrocardiology, 4, 199.
Scherf, D., and Scharf, M. M. (I948). Supernormal phase ofintraventricular conduction. American Heart J3ournal, 36,621.
Scherlag, B. J., Lau, S. H., Helfant, R. H., Berkowitz, W. D.,Stein, E., and Damato, A. N. (I969). Catheter techniquefor recording His bundle activity in man. Circulation, 39,13.
Sherf, L., and James, T. N. (I969). A new electrocardio-graphic concept: synchronized sinoventricular conduc-tion. Diseases of the Chest, 55, I27.
Sepfilveda, G., Rosselot, M. D., and Ahumada, J. (I969).Second degree atrioventricular block with intermittentright plus left anterior branch block. Diseases of the Chest,56, 553.
Singer, D. H., Lazzara, R., and Hoffman, B. F. (I967).Interrelationships between automaticity and conduction inPurkinje fibers. Circulation Research, 2!, 537.
Singer, D. H., and Ten Eick, R. E. (I97I). Aberrancy:electrophysiologic aspects. AmericanJournal of Cardiology,28, 38I.
Slama, R., Coumel, P., Motte, G., Fanjoux, J., Auperrin, A.,and Penther, P. (I969). Etude electrocardiographique del'installation et de la disparition du trouble de conductiondans deux cas de bloc auriculo-ventriculaire paroxystique.Archives des Maladies du Coeur et des Vaisseaux, 62, 101.
Sodi-Pallares, D., Bisteni, A., and Medrano, G. A. (I964).Electrocardiografia y vectocardiagrafia deductivas, Vol. I.La Prensa Medica Mexicana, Mexico, D. F.
Trautwein, W., and Dudel, J. (I956). Aktionpotential undKontraktion des Herzmuskels im Sauerstoffmangel.Pflugers Archivfur die gesante Physiologie des Menschen undder Tiere, 263, 23.
Vesell, H., and Lowen, G. (I963). Bundle branch block oncardiac slowing at a critical slow heart rate. AmericanHeart Journal, 66, 329.
von Hoesslin, H. (I923). Uber einer besonderen Fall vonStorung der Reizleitung und der Reizbarkeit des Herzens.Deutsches Archiv fur Klinische Medizin, x41, 348.
Watanabe, Y. (197I). Reassessment of parasystole. AmericanHeartJournal, 8I, 451.
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from

Delay and block of cardiac impulse caused. by enhanced phase-4 depolarization I49
Weidmann, S. (1955). The effect of the cardiac membranepotential on the rapid availability of the sodium-carryingsystem. J7ournal of Physiology, 127, 2I3.
Wennemark, J. R., and Ruesta, V. J. (197I). Microelectrodestudy of 2:1 conduction block in canine Purkinje fibers.J7ournal of Electrocardiology, 4, 50.
cardiac pacemaker. Journal of Pharmacology and Experi-mental Therapeutics, 115, 283.
West, T. C. (I955b). Auricular cellular potentials: ultramicro-electrode recording of drug effects on nodal and extra-nodal regions (abstract). Federation Proceedings, 14, 393.
Ren1e1Ptq fnr renrints to Dr. Andreq Kretz. Arenaleq woAAWTX,CaUiqUT9leLeA J1T9UrrorLOLmthe*erPiso, B s A, A nJ
West, T. C. (1955a). Ultramicroelectrode recording from the ler Piso, Buenos Aires, Argentina.
on October 2, 2020 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.37.2.136 on 1 February 1975. D
ownloaded from