Embed Size (px)
Citation preview
Page 1
HEE Workforce Planning 2014/15 – Call for Evidence
To submit your evidence please complete this form. Please make your submissions relevant to the
categories provided in the boxes provided. We have categorised the known drivers of demand and
supply under the following headings, and believe this to be a comprehensive description of the variable
involved.
You can provide extracts of reports into the free text boxes below, or submit a whole report with this
form by clicking on the email at the bottom of this form. Please mark clearly in the email which of the
below categories the report/evidence relates to, including any relevant page numbers. Where an
extract is provided, please reference the source.
Please use Part 3 to submit any information/evidence that does not fit the below categories. You can
also leave any comments/observations in the free text box.
Before completing the form below please submit your contact details here:
Name: Dr Di Gilson
Job title: Medical Director Education and Training, Faculty of Clinical Oncology
Organisation: The Royal College of Radiologists (RCR) (submission 2 of 2)
Specialty: Clinical Oncology (submission 2)
Contact email: [email protected]
Contact number: 020 7405 1282
Form submission:
Once completed please submit the form via email to [email protected] making sure all supporting documents are also attached to the email.
Please make the subject of the email: HEE Workforce Planning 2014/15 Call for Evidence-[Insert your organisation’s name]
Data Protection and Freedom of Information
The information you send us may be made available to wider partners, referred to in future published
workforce returns or other reports and may be stored on our internal evidence database.
Any information contained in your response may be subject to publication or disclosure if requested
under the Freedom of Information Act 2000. By providing personal information for this review it is
understood that you consent to its disclosure and publication. If this is not the case, you should limit
any personal information provided or remove it completely.
If you want the information in your response to be kept within HEE’s executive processes, you
should make this clear in your submission, although we cannot guarantee to be able to do this.
Page 2
PART 1 – Future Service and Workforce Models
1.1 Drivers of Future Service Demand
Needs identified by patients and the public
Activity and epidemiology
Quality. Innovation, prevention and productivity
Funding
Other
1.2 Future Service Models
1.3 Future Workforce Models
Associated knowledge and skills – and assessments of the supply and demand
position*
Associated values and behaviours – and assessments as above*
Workforce structure, team structure, skill mix, new roles.
Workforce performance and productivity
*nb – this may include views on the efficacy and quality of education processes in equipping
staff with these skills, knowledge, values and behaviours.
Page 3
PART 1 – RCR Clinical Oncology Response
1.1 Drivers of Future Service Demand
The RCR considers the main drivers of future service demand to be:
Demographics
More than one in three people in the UK will develop some form of cancer during their lifetime. More
than a third of cancers are diagnosed in people aged 75 and over. Estimates for 2009 were that
around one in 13 of the UK resident population were aged 75 and over (4.8 million residents) while
projected growth suggests that about one in nine will be in this age group by 2031 (8.3 million)
(CRUK/ONS).
With the increasing longevity of the population, the incidence of cancer will increase as will the
number of cancer survivors. Older patients tend to have more co-morbidities increasing the input
required from clinical oncologists to support them through treatment for their cancers. Cancer
survivors also require input from clinical oncologists if their disease relapses and or they develop late
complications of their treatment.
Radiotherapy is often the safest treatment option for patients with multiple co-morbidities and the
increase in cancer in the elderly population is expected to produce a disproportionate increase in
radiotherapy workload.
Earlier diagnosis of cancer
Initiatives to facilitate earlier diagnosis of cancer will increase the number of patients presenting with
localised disease. Radiotherapy is an effective local treatment and the smaller a tumour the greater
are the chances of obtaining local control with radiotherapy, potentially avoiding the need for surgery.
Culture
There is increasing awareness of treatment options for patients accompanied by heightened patient
and public expectations. This will be particularly important for patients with cancer. With ever
increasing treatment options, the workforce will need the skills and time to explain these options to
patients and facilitate patients’ decision making.
Innovation
For clinical oncology, advanced radiotherapy techniques, such as Intensity Modulated
Radiotherapy (IMRT) offer patients the possibility of improved chances of cure whilst minimising the
side effects of treatment, thus improving the duration and quality of life. Stereotactic body
radiotherapy (SBRT) offers the possibility of increasing the effective dose of radiotherapy delivered to
a tumour with a smaller number of radiotherapy treatments (fractions) resulting in an increased
chance of tumour control and less inconvenience for the patient. The effectiveness of IMRT and
SBRT is entirely dependant on Image Guided Radiotherapy (IGRT) to ensure that treatment is
accurately delivered. IMRT, SBRT and IGRT require greater clinical oncologist input in terms of
increased time to plan and verify radiotherapy.
Page 4
The increase in systemic anti-cancer therapy options for patients means that treatment is available
to more patients and that more lines of treatment are offered to the individual patient.
Molecular radiotherapy options are also likely to increase.
Advances in personalised medicine mean that treatments will be used more selectively for patients
who are most likely to benefit from a specific therapeutic intervention. This will increase the workload
for clinical oncologists in ensuring that individual patients have access to the appropriate treatment.
This should however improve patients’ quality of life and bring economic benefits (see below).
Technological progress
Technological developments in genomics will make the possibility of delivering personalised
medicine a reality. The clinical oncology workforce will need to be at the forefront of implementation of
personalised medicine for patients with cancer (see above).
Increasing clinical trials work
Innovations and technological progress will require evaluation in clinical trials. Recruiting patients into
clinical trials requires extra clinician input and time to ensure that patients are able to make informed
choices about trial entry and that all of the requisite trial data is collected during and after completion
of treatment.
Economics
The use of personalised medicine should improve the cost effectiveness of cancer therapy as
patients will receive the treatment most likely to produce a treatment response. This will reduce the
use of ineffective treatments with benefits in terms of patients’ quality of life and reducing the overall
cost of treatment to the NHS.
Earlier diagnosis of cancer improves the chances of cure of cancer and therefore improves the cost
effectiveness of cancer therapies. As stated above, this is likely to increase the number of patients
being managed with radiotherapy.
Optimum use of radiotherapy is essential, as this is more cost effective than systemic therapies.
Radiotherapy contributes to the cure of 40% of cancer patients, whereas systemic therapy contributes
to the cure of 11% of cancer patients. Radiotherapy alone cures 16% of patients with cancer.
Radiotherapy accounted for 5% of the national spend on cancer treatments in England in 2012.
(https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213151/Radiotherapy-
Services-in-England-2012.pdf)
Page 5
1.2 Future Service Models
The key points are highlighted below:
Clinical oncologists are pivotal in delivering non-surgical oncological care. They are able to
manage patients throughout their non-surgical cancer treatment. They are ideally placed to cost-
effectively manage the integration of systemic therapy and radiotherapy in patients’ care.
Clinical oncologists will need to work more closely with primary care physicians. This will be
necessary to ensure that patients’ co-morbidities are managed appropriately during treatment and
that the acute and late side effects of their treatment and psycho-social needs are addressed.
Increasing therapeutic options will necessitate greater tumour site specialisation for clinical
oncologists to ensure that clinicians have the knowledge and skills to deliver optimum treatment to
individual patients.
With increasing treatment options, research is essential to evaluate treatments. The increased
number of trials being recruited to in itself increases the workload for clinical oncologists, as
patients being recruited into a trial have longer discussions about treatment options and often
more ongoing clinic visits than the normal “standard of care”.
Page 6
1.3 Future Workforce Models
Training
In clinical oncology training, trainees complete 2 years of core medical training and 5 years of clinical
oncology training. The first 3 to 3½ years of clinical oncology training cover all tumour sites and
include a course covering the sciences that underpin cancer therapy. This ensures good general
medical and oncology training in all areas on solid tumour oncology. In the final 1½ to 2 years, whilst
consolidating their understanding of cancer treatment and developing their skills in patient
management and leadership, trainees develop advanced competencies in a minimum of 2 tumour
sites. This combination of generalist and specialist training delivers a flexible workforce. This
grounding in general medicine and oncology followed by tumour site specialisation ensures that
clinical oncologists are able to support patients with co-morbidities and acute oncological problems
whilst still delivering tumour site specialist care required to advise on optimal management options for
individual patients.
Working relationships
Cancer care is based on multidisciplinary working both in developing a patient’s treatment plan and
the delivery of care. It is essential that this should continue. Tumour site specialist Multidisciplinary
Team (MDT) meetings underpin and are essential to the delivery of high quality cancer care.
Closer working between medical and clinical oncologists, pharmacists and clinical nurse specialists
and chemotherapy nurses will be required to deliver systemic anti-cancer therapy in the future. To
ensure that this multidisciplinary approach continues to develop, since the end of the National
Chemotherapy Advisory Group, the RCR has established a UK wide Chemotherapy board which has
representation from all of these professional groups. Medical and clinical oncology liaison is also
being facilitated through the RCP/RCR Joint Collegiate Council for Clinical Oncology which continues
to meet regularly.
Likewise a national Radiotherapy Board has been established with the Institute of Physics and
Engineering in Medicine and the Society and College of Radiographers to facilitate the closer working
between the professional groups involved in delivering radiotherapy, including clinical oncologists,
nuclear medicine physicians, medical physicists, dosimetrists and therapeutic radiographers. Part of
the Board’s remit is to develop a strategy and structure for workforce planning and training, and for
professional standards. The closer working relationships between clinical oncologists and nuclear
medicine physicians to optimise the use of molecular radiotherapy are also being facilitated by the
RCP/RCR Intercollegiate Standing Committee for Nuclear Medicine.
We see the continued need to develop aspects of common training to foster understanding of all of
cancer treatment options for individual patients. This will ensure that patients receive the right care at
the right time.
It is also essential that the whole cancer research team, including academics involved in fundamental
biological research, technical radiotherapy development and development of new systemic therapies,
are an integrated part of the cancer therapy team, to ensure that treatment continues to advance and
that we make optimal use of developments in treatment.
Page 7
PART 2 – Forecast of future supply and demand – volumes
If you want to input evidence into the forecasting of future numbers you can report your
perspectives on either;
i) the high level indicators; supply, demand, and any forecast under / over supply, or if
available - Part 2.1
ii) the more granular components of these three components e.g. retirement rates,
output from education relative to attrition – Part 2.2
2.1 Summary forecasts
Forecast Workforce Demand
Forecast Workforce Supply and Turnover
Forecast Under / Over Supply
PART 2.1 – RCR Clinical Oncology Response
Forecast Workforce Demand and Supply
This increased demand on clinical oncologists comes in a number of forms:
The incidence of cancer is expected to increase by 20% over the next 10 years (i.e. 2% per
annum). The majority of this increase will occur in the elderly who often have multiple co-
morbidities.
The aging population will have more co-morbidities and will require more input from the oncology
team to support them through their cancer treatment both in outpatient and acute oncology
settings.
It is estimated the number of cancer survivors is increasing by 3% per year in the UK and there are
currently 2 million cancer survivors in the UK (www.ncin.org.uk/view?rid=70). A proportion of these
patients will develop recurrence of their cancer and require further treatment. Some patients will
have significant delayed long term complications as a result of their treatment. These patients may
be managed by clinical oncologists or require input from clinical oncologists to facilitate onward
referral to other clinicians for appropriate specialist care.
Increase in cancer treatment options makes more lines of therapy available to the individual
patient. Systemic anti-cancer therapy workload is increasing by 8% per annum. Clinical
oncologists deliver 50% of the systemic anti-cancer therapy for adults in England, compared with
33% delivered by medical oncologists and 17% delivered by clinical haematologists (NCIN
Chemotherapy Data Set).
There is expected to be a 1% per annum increase in the number of radiotherapy courses
delivered in England (NCIN Radiotherapy Data Set). Courses of radiotherapy delivered are a
better representation of clinical oncologists’ workload than the number of radiotherapy fractions
delivered because each course of radiotherapy is individually planned for the patient. This 1%
increase does not take account of the increasing complexity of radiotherapy (see below).
Page 8
In addition to the 1% per annum increase in courses of radiotherapy, there will be increasing use
of advanced radiotherapy (IMRT, SBRT and IGRT) techniques. These techniques increase the
time required by clinical oncologists (x2-3 per patient) to plan and deliver radiotherapy treatment.
These radiotherapy techniques offer the possibility of increased cure rates for cancer whilst
minimising/reducing the side effects of treatment. This workload to date has been delivered by the
current consultant workforce increasing their working hours often without remuneration or at the
expense of supporting professional activities. There is increasing evidence these advanced
radiotherapy techniques are of benefit to the majority of patients receiving radiotherapy with
curative intent (radical radiotherapy). As the use of these techniques expands, all existing
consultants will need to have time allocated in their job plans to deliver the required radiotherapy
planning and delivery.
The use of advanced radiotherapy techniques to deliver radical (potentially curative) radiotherapy
will continue to increase over the next 5 years. England has lagged behind other developed
countries in introducing these advanced radiotherapy techniques and needs to increase their use if
patients are to receive the best care. A major contributing factor to this delay in introducing
advanced radiotherapy has been consultants not having time to introduce these new techniques.
The current target in England is that 24% of all patients receiving radical radiotherapy should
receive IMRT. The use of advanced radiotherapy techniques (IMRT, SBRT and IGRT) will and
should expand in order to improve tumour control and reduce toxicity. It is anticipated that 80% of
patients receiving radical radiotherapy will be treated with advanced radiotherapy in the future. The
current advanced radiotherapy techniques will continue to evolve and develop and it is essential
for patient care that clinical oncologists have time to implement and use these developments. To
allow for the historical shortfall and required expansion in radiotherapy planning time, it is
estimated that on average consultant clinical oncologists will require at least 0.5 extra PAs per
week for radiotherapy planning to ensure that all appropriate patients have access to these
advanced radiotherapy techniques.
Internationally the role of regular peer review of radiotherapy planning is important in ensuring that
patients receive consistent safe high quality treatment. Ideally all clinical oncologists should take
part in regular radiotherapy planning quality assurance meetings with their peers. To avoid delays
in treatment these meetings need to happen on a weekly basis. At present, the majority of clinical
oncologists are unable to participate in such meetings due to lack of time in their job plans. It is
estimated that on average clinical oncologists require an extra 0.25 PAs per week to deliver
radiotherapy quality assurance.
Twelve per cent of cancer patients currently enter clinical trails (CRUK). Increasing trial availability
increases the time taken to discuss treatment options with patients and also increases follow up
workload over current “standard of care” but is essential to improve outcomes and ensure that
treatment is cost effective.
Page 9
Figures 1 and 2 overleaf illustrate workforce demand and supply. The data and assumptions
underlying this are set out below.
Forecast Workforce/Workload Demand
Our demand forecast is based on:
The estimated increase in courses of systemic therapy of 8% per annum and increase in
radiotherapy courses by 1% per annum. This will result in an estimated increase of 9% per annum
in the workload of clinical oncologists.
A historic deficit in time for radiotherapy planning (0.5 PAs per week) and participation in a regular
radiotherapy planning quality assurance meeting (0.25 PAs per week), totalling 0.75 PAs per week
per consultant. This is will ensure that patients in England receive optimal radiotherapy in line with
internationally accepted standards of care. Workforce requirements have been modelled with and
without additional allowance for this radiotherapy planning time.
Forecast Workforce Supply
The results of the most recent RCR workforce census in October 2013 showed there were 619
consultant clinical oncologists (headcount) in substantive posts in England (equating to 569 whole
time equivalents (WTEs)).
The median retirement age for consultant clinical oncologists in 2013 was 60. Using this average,
21% of the consultant clinical oncology workforce is expected to retire in the next five years. This
equates to, on average, 26 consultants retiring each year for the next five years.
Taking into account attrition rates (see page 13) and the number of trainees reaching CCT over
the last five years, on average approximately 37 trainees are expected to attain CCT and
subsequently take up a consultant post in England each year for the next five years. This figure
includes an average of one trainee a year taking up a consultant post in England who trained in
one of the devolved nations.
More than 57% of current trainees are female. The participation rate of new consultants is
modelled at 0.95 however the actual level of participation is likely to be lower.
The high number of expected retirements in the next few years, set against static training numbers
and decreasing participation rates, means the workforce shortfall in clinical oncology will not be
overcome without an increase in training numbers.
Page 10
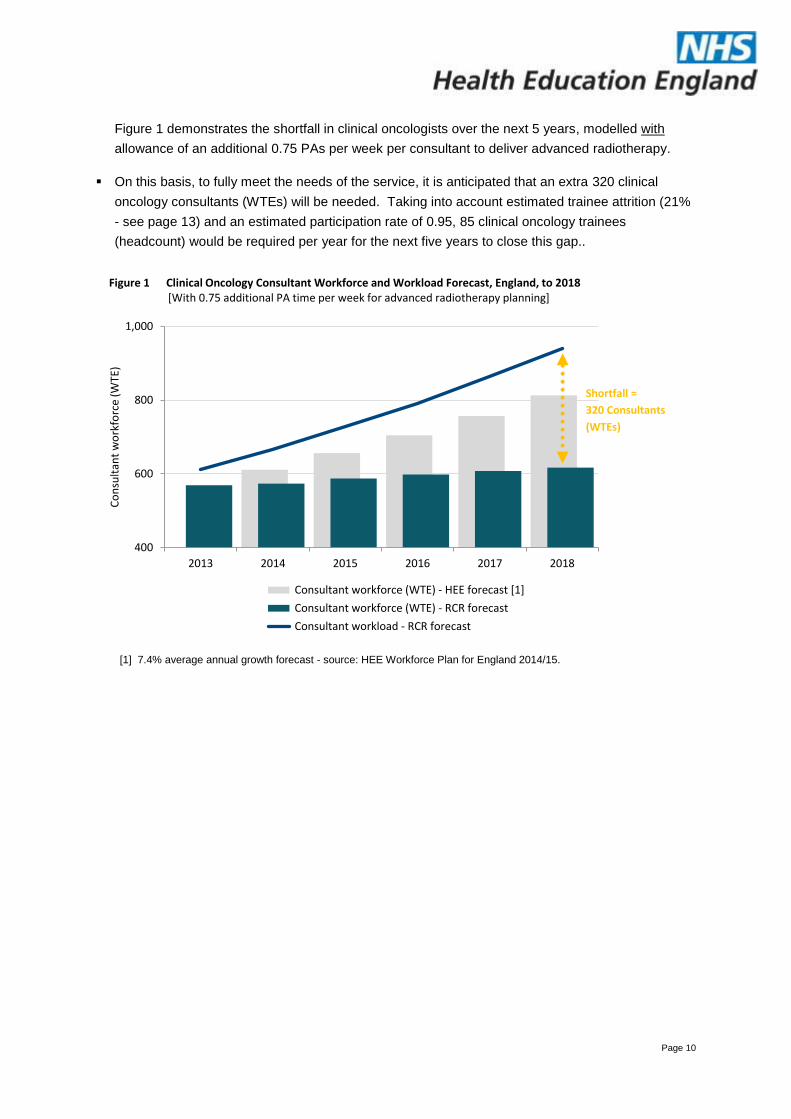
Figure 1 demonstrates the shortfall in clinical oncologists over the next 5 years, modelled with
allowance of an additional 0.75 PAs per week per consultant to deliver advanced radiotherapy.
On this basis, to fully meet the needs of the service, it is anticipated that an extra 320 clinical
oncology consultants (WTEs) will be needed. Taking into account estimated trainee attrition (21%
- see page 13) and an estimated participation rate of 0.95, 85 clinical oncology trainees
(headcount) would be required per year for the next five years to close this gap..
400
600
800
1,000
2013 2014 2015 2016 2017 2018
Co
nsu
ltan
t w
ork
forc
e (W
TE)
Figure 1 Clinical Oncology Consultant Workforce and Workload Forecast, England, to 2018[With 0.75 additional PA time per week for advanced radiotherapy planning]
Consultant workforce (WTE) - HEE forecast [1]
Consultant workforce (WTE) - RCR forecast
Consultant workload - RCR forecast
[1] 7.4% average annual growth forecast - source: HEE Workforce Plan for England 2014/15.
Shortfall =
320 Consultants
(WTEs)
Page 11
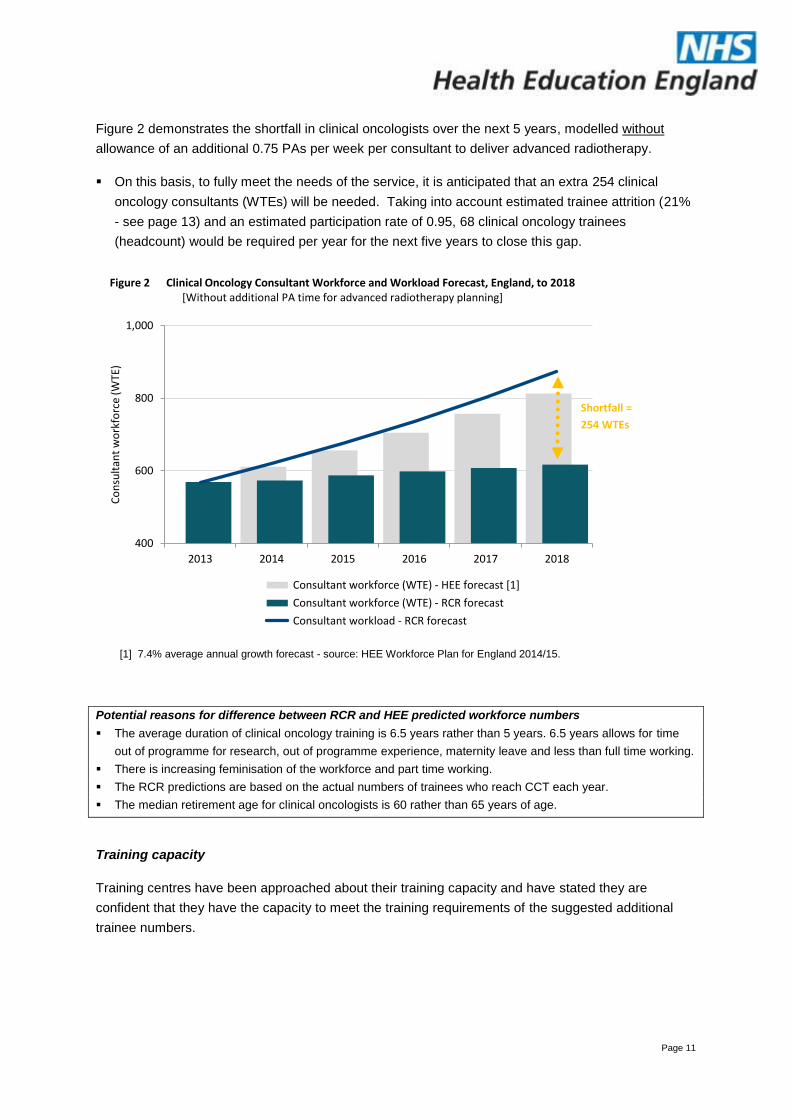
Figure 2 demonstrates the shortfall in clinical oncologists over the next 5 years, modelled without
allowance of an additional 0.75 PAs per week per consultant to deliver advanced radiotherapy.
On this basis, to fully meet the needs of the service, it is anticipated that an extra 254 clinical
oncology consultants (WTEs) will be needed. Taking into account estimated trainee attrition (21%
- see page 13) and an estimated participation rate of 0.95, 68 clinical oncology trainees
(headcount) would be required per year for the next five years to close this gap.
400
600
800
1,000
2013 2014 2015 2016 2017 2018
Co
nsu
ltan
t w
ork
forc
e (W
TE)
Figure 2 Clinical Oncology Consultant Workforce and Workload Forecast, England, to 2018[Without additional PA time for advanced radiotherapy planning]
Consultant workforce (WTE) - HEE forecast [1]
Consultant workforce (WTE) - RCR forecast
Consultant workload - RCR forecast
[1] 7.4% average annual growth forecast - source: HEE Workforce Plan for England 2014/15.
Potential reasons for difference between RCR and HEE predicted workforce numbers
The average duration of clinical oncology training is 6.5 years rather than 5 years. 6.5 years allows for time
out of programme for research, out of programme experience, maternity leave and less than full time working.
There is increasing feminisation of the workforce and part time working.
The RCR predictions are based on the actual numbers of trainees who reach CCT each year.
The median retirement age for clinical oncologists is 60 rather than 65 years of age.
Training capacity
Training centres have been approached about their training capacity and have stated they are
confident that they have the capacity to meet the training requirements of the suggested additional
trainee numbers.
Shortfall =
254 WTEs
Page 12
2.2 Detailed / Component forecasts
Forecast Workforce Demand
Service Demand drivers
Change in use of temporary staff
Addressing historic vacancies
Skill Mix / New Roles
Workforce Productivity
PART 2.2 – RCR Clinical Oncology Response
Service Demand Drivers
See section 1.
Other information
There is no significant use of temporary staff to deliver the work of consultant clinical oncologists.
Clinical oncology has used skill mix to deliver both radiotherapy and systemic therapy and will
continue to develop this where possible. The competencies required by clinicians to plan and
prescribe IMRT, SBRT and to use IGRT are largely acquired during advanced clinical oncology
training in the 18 to 24 months prior to completion of specialist training. These are not roles that
could be devolved to ‘trained doctors’ or other staff.
Data collected through RCR Advisory Appointment Committees (AACs) shows that NHS trusts in
England requested RCR representatives to attend committees to appoint to 38 vacant consultant
posts in England (for the period January – May 2014).
o For the 24 vacant posts where the interview process has now been concluded, a third
of posts were not appointed to due to lack of suitable candidates. (The recruitment for
14 of the 38 posts is still in progress.)
o 31 of the 38 vacant posts are newly created posts (as opposed to replacement).
o The true number of vacant posts is likely to be higher as foundation trusts are not
obliged to follow the AAC process.
Among cancer clinicians, 'burnout' has been found to be more prevalent among clinical oncologists
than among medical oncologists and palliative care specialists. 'Burnout' was related to the stress
of feeling overloaded, high stress and low satisfaction from dealing with patients, and with low
satisfaction from having adequate resources. (http://www.ncbi.nlm.nih.gov/pubmed/7540037)
Page 13
Forecast Supply from HEE commissioned education
Assumed training levels
Under recruitment
Attrition
Employment on completion of training
RCR Clinical Oncology Response
Assumed training levels / Under recruitment
In the last round of nationally coordinated central recruitment all NTNs and LAT posts in England
were filled.
Based on RCR trainee records for the five year period between 1 January 2009 and 31 December
2013:
On average 46 trainees reach CCT each year in the UK and 36 of these reach CCT in England
and take up a consultant post in England. There has been no significant change in training
numbers in recent years and the number of trainees completing training each year is not expected
to change significantly.
On average one trainee reaching CCT each year in a devolved nation subsequently takes up a
consultant post in England.
Attrition / Employment on completion of training
Based on RCR trainee records for the five year period between 1 January 2009 and 31 December
2013:
On average 7% of trainees in England do not reach CCT, leaving training prior to completion.
On average 14% of trainees who reach CCT in England subsequently take up a post outside
England.
On average, the total attrition rate from the point of starting training to taking up a consultant post
in England is therefore estimated to be 21%.
Page 14
Forecast Supply – Other Supply and Turnover
From other education supply
To/from the devolved administrations
To/from private and LA health and social care employers
To/from the international labour market
To/from other sectors / career breaks and ‘return to practice’
To/from other professions (e.g. to HV or to management)
Increased / decreased participation rates (more or less part time working)
Retirement
RCR Clinical Oncology Response
To/from the devolved administrations
There is no expected significant supply of clinical oncologists from the devolved nations. RCR
trainee records show that an average of one trainee a year joined the consultant workforce in
England from the devolved nations over the past five years.
To/from the international labour market
There are very few successful applications for entry on the specialist register for clinical oncology
via the equivalence route (CESR) each year – one in 2013, none so far in 2014.
It is unlikely that doctors from the EU will be able to fill clinical oncology posts as the majority of
European countries train radiation oncologists whose training does not include managing patients
with systemic anti-cancer therapy.
Increased / decreased participation rates (more or less part time working)
Based on RCR 2013 Clinical Oncology Workforce Census data and RCR trainee records:
46% of the consultant workforce in England is female. This compares with 57% of current trainees.
It is expected that participation rates will fall, as the majority of clinical oncology trainees are
female and part time working is more prevalent in the female workforce than the male.
36% of the female consultant workforce works part time compared with 8% of males.
Retirement
21% of the workforce is aged 55 or older and the median retirement age is 60. On this basis, it is
predicted that 21% of the consultant workforce will retire in the next 5 years.
Page 15
PART 3 – General / Other Evidence not included elsewhere
What is a Clinical Oncologist?
Clinical oncology is the non-surgical management of malignant disease, using both radiotherapy and
systemic therapy (chemotherapy, hormone therapy and biological agents).
Clinical oncologists are specialist physicians who are trained in the care of the full range of malignant
diseases in adults, and in some teenage and young adult, childhood and haematological
malignancies. They are the only specialist group trained in the assessment of patients for
radiotherapy and treatment of patients with radiotherapy. They are the only medical specialists
qualified to prescribe radiotherapy. Clinical oncologists are also trained in the use of systemic
therapies in the management of cancer. The majority of clinical oncologists regularly deliver both
systemic therapy and radiotherapy, either as single or sequential single modality therapies or, in some
indications, concomitantly in combination with radiotherapy (chemoradiotherapy). These patterns vary
to ensure appropriate patterns of care required for different areas of tumour site specialisation. They
also depend upon the availability of overlapping and complementary skills mix in other health care
professionals.
Many clinical oncologists will have undertaken a substantive period of clinical or basic research during
their training and some will have a research degree (MD or PhD). Clinical oncologists are active in
clinical trials, within both systemic therapy and radiotherapy practice. Some clinical oncologists follow
academic careers, more commonly in the development of radiotherapeutic techniques, novel
radiotherapy schedules or in combination with systemic therapies. Some also have academic roles in
drug development or basic cancer biology.























![TFIEY early years workforce review evidence and good practice [2013]](https://img.pdfslide.net/doc/110x75/55be6b7cbb61eb715a8b4736/tfiey-early-years-workforce-review-evidence-and-good-practice-2013.jpg)