Embed Size (px)
DESCRIPTION
HEMATOLOGY EXAM
Citation preview
HEMA 2UEANEMIA OF BONE MARROW FAILURE & SYSTEMIC DISORDER – CH 10CASE STUDY 1A 22-year-old white woman was admitted to the hospital because of severe menstrual bleeding. She had numerous petechiae and some purpura. The patient was a religious missionary who had recently returned from a 2-year assignment in Haiti. Six months ago, she developed a severe respiratory infection. She was treated by a local Haitian physician at that time but was not hospitalized because of the lack of medical facilities on the island. She had refused to return home for further treatment at that time. Initially, she received a cephalosporin-type antibiotic but later received chloramphenicol because her symptoms persisted. At the time of admission, she showed no evidence of a respiratory disorder. However, she had recently discontinued the chloramphenicol that she had taken continuously for 5 months. On admission, the following tests were ordered: CBC, platelet count, cold agglutinin antibody screen, urinalysis, and chest radiograph.
Laboratory Data■Hemoglobin 5.5 g/Dl Hct 18%RBC 1.85 × 1012/L MCV 97.2 fLMCH 29.7 pg MCHC 31 g/dLHer WBC count was 2.1 × 109/L. On the peripheral blood smear, the RBCs had a normochromic, normocytic appearance. Platelets were severely diminished on the blood film. Her platelet count was 6.5 × 109/L. The result of the screening test for cold agglutinins was negative. Urinalysis results were normal. Thirty-six hours after admission the patient died of a massive cerebral hemorrhage. Tests performed on specimens obtained at autopsy revealed that the patient’s bone marrow showed an almost total absence of hematopoiesis. A blood culture was positive for the Gram-negative rod Proteus vulgaris.QUESTIONS1. What is the most likely cause of this patient’s pancytopenia?2. How do certain drugs affect the body’s cellular elements?3. What caused the patient’s death?DISCUSSION1. This patient’s reduced erythrocytes, leukocytes, and thrombocytes (pancytopenia) had probably been induced by the drug chloramphenicol. Certain drugs depress bone marrow activity at a critical dosage level. Chloramphenicol is most notorious for its depression of hematopoiesis. The patient’s prolonged use of this drug with its known high tissue toxicity index undoubtedly produced this bone marrow failure.2. Various types of antibiotics function in different ways in the human body. Penicillin, for example, inhibits the cell wall synthesis of peptidoglycans, which constitute the major cell wall chemical in Gram-positive microorganisms. Many antibiotics interfere with protein synthesis. In the case of chloramphenicol, the specifi c in vivo action is unclear. However, in vitro studies have demonstrated demonstrated that chloramphenicol inhibits protein synthesis and mitochondrial synthetic activity.3. This patient died of bacteremia (septicemia) caused by the Gram-negative microorganism P. vulgaris. Because the patient’s body defenses had been severely compromised because of the effects of chloramphenicol, she was unable to effectively ward off a massive bacterial infection.DIAGNOSIS: Drug-induced Aplastic Anemia
CASE STUDY 2A 6-year-old African boy who had recently immigrated to the United States from Liberia was taken to the emergency department because of a high fever. Physical examination showed bilateral syndactyly and contractures of the fi ngers. His temperature was 100°F. A CBC was ordered.
LABORATORY DATARBC 2.1 × 1012/L Hematocrit 18%Hemoglobin 6.0 g/Dl WBC 1.31 × 109/LPlatelets 45 × 109/LQUESTIONS1. What do the laboratory results suggest?2. Is the boy’s physical appearance suggestive of a hematologic abnormality?3. What is the cause of Fanconi anemia?4. What innovative treatments are available to patients with Fanconi anemia?DISCUSSION1. Decreased red blood cells, white blood cells, and platelets are indicative of a defi ciency of all bone marrow elements. This condition is called pancytopenia.2. Yes. The developmental defects of thumb and radius are suggestive of Fanconi anemia. The childhood onset of pancytopenic anemia further supports the diagnosis. 3. Fanconi anemia is a rare autosomal recessive genetic disorder. Fanconi anemia is one of the well-known chromosome instability syndromes. Hypersensitivity to alkylating or DNA cross-linking agents (e.g., mitomycinC) is used as a standard laboratory assay to confi rm the diagnosis.4. Most patients with Fanconi anemia have a short life expectancy. Recently, a child with Fanconi anemia made news by being the recipient of an umbilical cord blood stem cell transplant from her genetically screened and selected newborn brother.
DIAGNOSIS: Fanconi Anemia
REVIEW QUESTIONS1. Acquired aplastic anemia may be caused byA. benzene or benzene derivativesB. ionizing radiation and vitamin B12C. purine or pyrimidine analoguesD. all of the above
2. The sudden appearance of aplastic anemia or pure red cell aplasia is often caused byA. a hemolytic processB. an immune processC. acute leukemiasD. chronic leukemias
3. Aplastic anemia can occur years before a diagnosis of _____ is made.A. paroxysmal nocturnal hemoglobinuria
B. myelodysplasiaC. acute myelogenous leukemiaD. all of the above
4. If a patient with aplastic anemia is referred to as exhibiting pancytopenia, which cell lines are affected?A. ErythrocytesB. LeukocytesC. ThrombocytesD. All of the above
Questions 5 to 8: Match the following. (Use an answer only once)5. _____ Fanconi anemia6. _____ Familial aplastic anemia7. _____ Pure red cell anemia8. _____ Diamond-Blackfan syndrome
A. A subset of Fanconi anemiaB. A rare congenital form of red cell aplasiaC. Is characterized by selective failure of red blood cell productionD. The best-described congenital form of aplastic Anemia
9. Hematopoietic cell targets in aplastic anemia are affected byA. activated cytotoxic T lymphocytesB. activation of the Fas receptorC. direct cell–cell interactions between lymphocytes and target cellsD. all of the above
10. Fanconi anemia is associated with abnormal genes located on chromosomes __q___, __q___.A. 9, 20B. 5, 22C. 9, 12D. 8, 23
ANSWER1. D 2. B 3. D 4. D 5. D 6. A7. C 8. B 9. D 10. A
ANEMIA OF ABNORMAL NUCLEAR DEVELOPMENT – CH 11CASE STUDYA 50-year-old white woman had seen her physician and reported having no energy and feeling tired all the time. She also reported experiencing mild pain in the abdominal region. The physician ordered a routine CBC.
■ Laboratory DataHemoglobin 6.2 g/Dl Hct 22%RBC 1.7 × 1012/L WBC 4.0 × 109/LMCV 129.4 fL MCH 36.5 pgMCHC 28 g/dLThe peripheral blood smear demonstrated abnormalities of erythrocytes and leukocytes. On receipt of the laboratory data, the physician ordered the following additional tests: vitamin B12 and folate assays, reticulocyte count, serum iron and TIBC, serum bilirubin, and serum LDH. A fecal examination for occult blood was additionally ordered. The results of the tests were as follows:
Vitamin B12: 121 pmol/L (decreased) Serum folate level: normalReticulocyte count: 0.4% Serum iron and TIBC: normalSerum bilirubin: 1.8 mg/dL (slightly increased)Serum LDH: >3,000 units (signifi cantly increased)The test result for occult blood was negative.
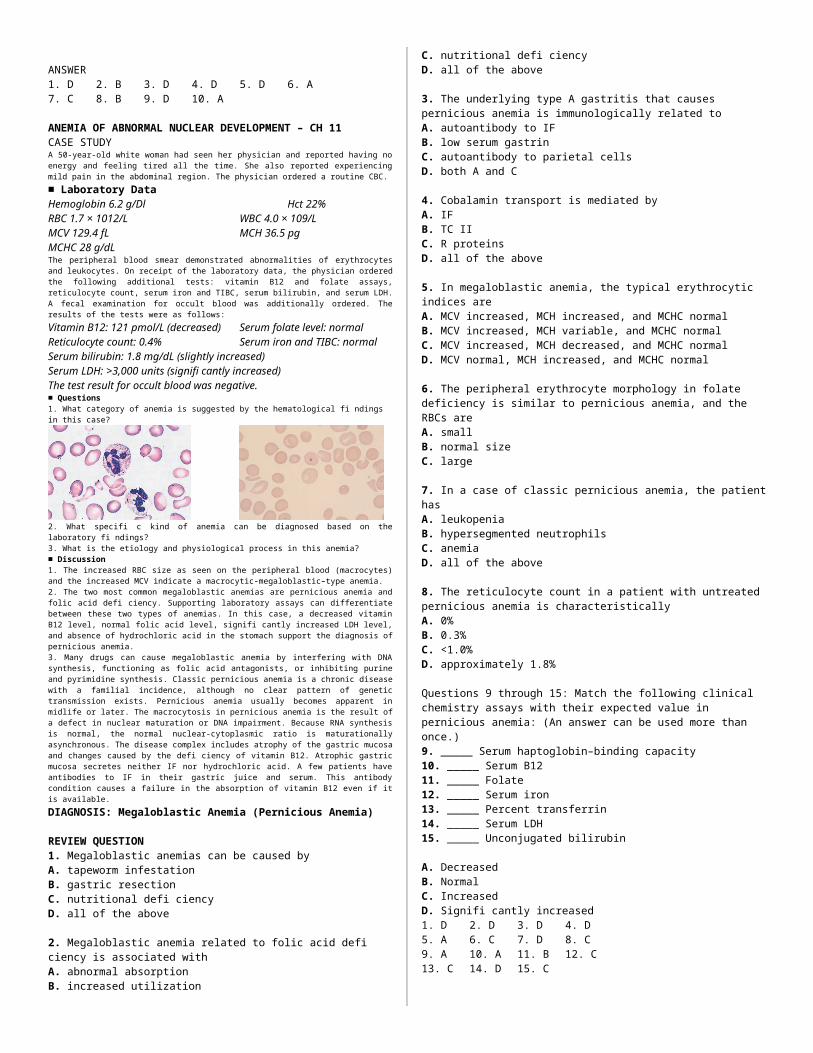
■ Questions1. What category of anemia is suggested by the hematological fi ndings in this case?
2. What specifi c kind of anemia can be diagnosed based on the laboratory fi ndings?3. What is the etiology and physiological process in this anemia?
■ Discussion1. The increased RBC size as seen on the peripheral blood (macrocytes) and the increased MCV indicate a macrocytic-megaloblastic–type anemia. 2. The two most common megaloblastic anemias are pernicious anemia and folic acid defi ciency. Supporting laboratory assays can differentiate between these two types of anemias. In this case, a decreased vitamin B12 level, normal folic acid level, signifi cantly increased LDH level, and absence of hydrochloric acid in the stomach support the diagnosis of pernicious anemia.3. Many drugs can cause megaloblastic anemia by interfering with DNA synthesis, functioning as folic acid antagonists, or inhibiting purine and pyrimidine synthesis. Classic pernicious anemia is a chronic disease
with a familial incidence, although no clear pattern of genetic transmission exists. Pernicious anemia usually becomes apparent in midlife or later. The macrocytosis in pernicious anemia is the result of a defect in nuclear maturation or DNA impairment. Because RNA synthesis is normal, the normal nuclear-cytoplasmic ratio is maturationally asynchronous. The disease complex includes atrophy of the gastric mucosa and changes caused by the defi ciency of vitamin B12. Atrophic gastric mucosa secretes neither IF nor hydrochloric acid. A few patients have antibodies to IF in their gastric juice and serum. This antibody condition causes a failure in the absorption of vitamin B12 even if it is available.
DIAGNOSIS: Megaloblastic Anemia (Pernicious Anemia)
REVIEW QUESTION1. Megaloblastic anemias can be caused byA. tapeworm infestationB. gastric resectionC. nutritional defi ciencyD. all of the above
2. Megaloblastic anemia related to folic acid defi ciency is associated withA. abnormal absorptionB. increased utilizationC. nutritional defi ciencyD. all of the above
3. The underlying type A gastritis that causes pernicious anemia is immunologically related toA. autoantibody to IFB. low serum gastrinC. autoantibody to parietal cellsD. both A and C
4. Cobalamin transport is mediated byA. IFB. TC IIC. R proteinsD. all of the above
5. In megaloblastic anemia, the typical erythrocytic indices areA. MCV increased, MCH increased, and MCHC normalB. MCV increased, MCH variable, and MCHC normalC. MCV increased, MCH decreased, and MCHC normalD. MCV normal, MCH increased, and MCHC normal
6. The peripheral erythrocyte morphology in folate deficiency is similar to pernicious anemia, and the RBCs areA. smallB. normal sizeC. large
7. In a case of classic pernicious anemia, the patient hasA. leukopeniaB. hypersegmented neutrophilsC. anemiaD. all of the above
8. The reticulocyte count in a patient with untreated pernicious anemia is characteristicallyA. 0%B. 0.3%C. <1.0%D. approximately 1.8%
Questions 9 through 15: Match the following clinical chemistry assays with their expected value in pernicious anemia: (An answer can be used more than once.)9. _____ Serum haptoglobin–binding capacity10. _____ Serum B1211. _____ Folate12. _____ Serum iron13. _____ Percent transferrin14. _____ Serum LDH15. _____ Unconjugated bilirubin
A. DecreasedB. NormalC. IncreasedD. Signifi cantly increased
1. D 2. D 3. D 4. D5. A 6. C 7. D 8. C9. A 10. A 11. B 12. C13. C 14. D 15. C
ANEMIA OF ABNORMAL IRON METABOLISM N HEME SYNTHESIS – CH 12CASE 10.1A 10-month-old Central American child was referred to the laboratory for testing after being seen by a pediatrician. The phlebotomist noted that the child was very pale and listless. The following tests were ordered: complete blood count (CBC), platelet count, reticulocyte count, total serum bilirubin, total serum iron and TIBC, and a stool examination for occult blood, ova, and parasites. The results were as follows:
■ Laboratory DataHemoglobin 5.6 g/Dl Hct 24%RBC 3.5 ´ 1012/L WBC 10.5 ´ 109/LMCV 68.6 fL MCH 16 pgMCHC 23 g/dLThe peripheral blood smear revealed signifi cant anisocytosis, microcytosis, hypochromia, and poikilocytosis. A normal distribution of platelets was present. Additional laboratory fi ndings:
Platelet count 200 ´ 109/L Reticulocyte count 0.5%Total serum bilirubin 0.9 mg/dL Serum iron 40 mg/dLTIBC 465 mg/dL Percent saturation of transferrin 8.6%A stool examination was negative for occult blood, ova, and parasites.
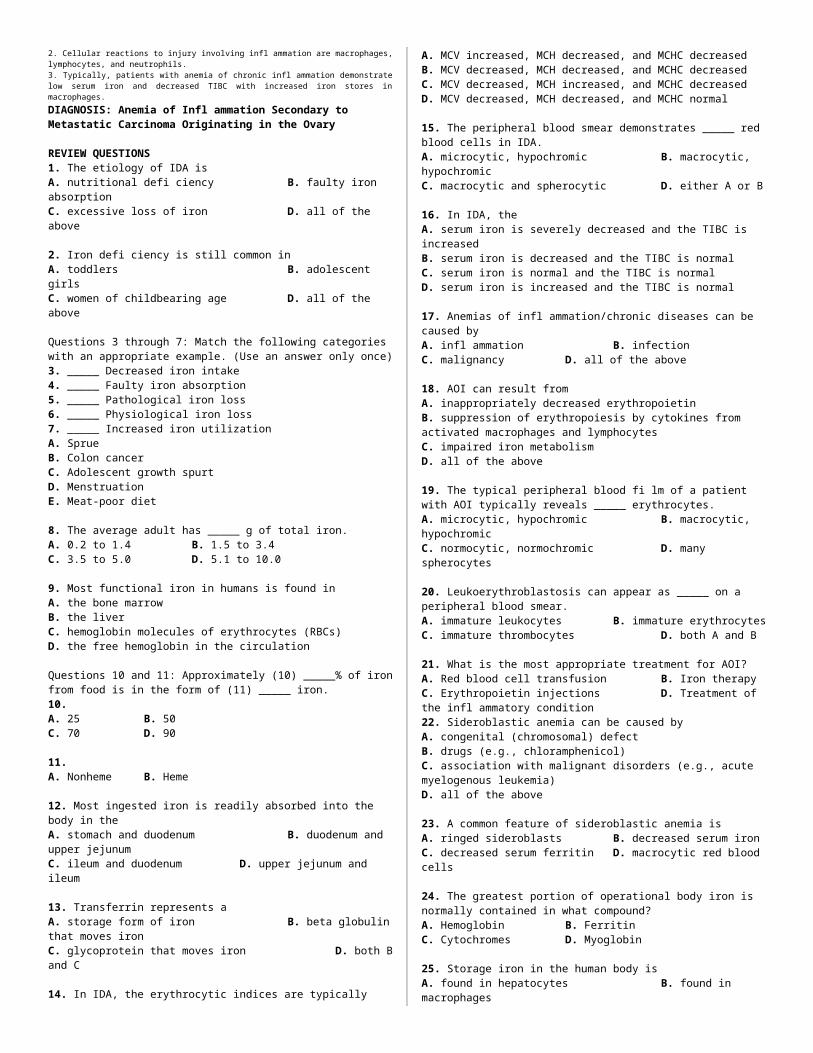
■ Questions1. What category of anemia is suggested by the morphology of the RBCs on the peripheral blood smear?2. What laboratory assays would be of additional value in establishing the diagnosis?3. What is the most probable cause of the patient’s anemia?
■ Discussion1. The demonstration of hypochromic, microcytic erythrocytes in a peripheral blood fi lm suggests IDA.2. The RBC indices reveal both a decreased MCV and MCH. These fi ndings support the RBC morphology observations of microcytosis and hypochromia. Several follow-up laboratory assays were valuable in establishing the etiology of this patient’s anemia. These tests were the serum iron, TIBC, and percent saturation. A decreased serum iron and percent saturation were present, along with an increased TIBC. The serum bilirubin and reticulocyte count were normal. No evidence of bleeding or parasitic infections was detected.3. The most probable cause of this patient’s anemia is iron defi ciency. The laboratory fi ndings demonstrate an iron defi cit with no evidence of either hemolysis or blood loss. Small children are among the most frequent victims of inadequate dietary iron. The newborn begins life with 350 to 500 mg of iron. A daily intake of 1 mg/ kg (2.2 lb) of body weight is needed during infancy to keep pace with growth. Some iron-poor foods, such as milk, never become useful sources for the absorption of iron. Children in underdeveloped countries frequently suffer from a combination of poor diet and parasitic infections. IDA is a frequent by-product of a diet consisting largely of milk and unsupplemented by fortifi ed food products during the early years of development.
DIAGNOSIS: Iron Defi ciency Anemia
CASE 10.2A 75-year-old woman started feeling a bit weak. The patient reported limited red meat intake. A cholecystectomy was performed at age 60 and some bowel was removed. The patient has occasional diarrhea but considers this a minor inconvenience. The patient has experienced some bilateral loss of sensation in the feet and a tingling that was getting worse and more frequent over the past few months. She takes overthe- counter medications and her husband’s pills for indigestion. The patient complained of arthritis; she has been taking nonsteroidal anti-infl ammatory drugs for 5 years, and she has started low-dose methotrexate for arthritis fl are-ups. The physician is certain that she is anemic and requests a CBC and differential, iron, TIBC, and % Sat/ferritin. No malignancies or GI bleeding is noted. Blood loss from the GI tract has been ruled out. Profound atrophic gastritis with patches of infl ammation is noted, as is H. pylori at stomach biopsy study.
■ Laboratory DataHemoglobin 10 g/dL (reference value, 12 g/dL)Hematocrit 33% (reference value, 36% to 45%)MCV 83 fL (reference value, 81 to 98 fL)RDW 17.5 % (reference value, 11.5% to 14.5%)Iron 25 mg/dL (reference value, 50 to 170 dL)TIBC 250 mg/dL (reference value, 250 to 450 mg/dL)% Sat 10% (reference value, 15% to 50%)Ferritin 45 mg/L (reference value, 12 to 120 mg/L)Serum folate 4 ng/mL (reference value, 3 to 16 ng/mL)RBC folate 100 ng/mL (reference value, 130 to 628 ng/mL)Vitamin B12 100 pg/mL (reference value, 200 to 900 pg/mL)
■ Questions1. Is ferritin a reliable laboratory indicator of iron stores?
■ Discussion1. Ferritin is an iron-storage molecule. The amount in serum refl ects iron storage: every 1 mg/L indicates (very roughly) 10 mg of body stores. Concern about the use of this indicator in the elderly arises because a range of infl ammatory diseases increase ferritin; therefore, its concentration no longer refl ects iron stores. Ferritin acts as an acute-phase reactant. In this case, the increased ferritin was caused by the infl ammation of rheumatoid arthritis, illustrating the diagnostic pitfall of placing too much faith in ferritin. Atrophic gastritis is common in the elderly and is almost certainly caused, to some extent, by H. pylori.
■ Follow-upThe patient was given the usual course of intramuscular vitamin B12 and oral folate, 1 mg/day. The following were the laboratory results at her 3-month follow-up:

Hemoglobin 11 g/dL MCV 75 fLTIBC 500 mg/dL RDW 15Ferritin 8 mg/L Iron 35 mg/dL % Sat 7%Bone marrow ordered for refractory anemia
■ Diagnostic ProblemsThis case presented some challenging diagnostic problems. The patient had an extremely elevated red blood cell distribution width index (RDW), which suggested a mixed red cell population. A mixed vitamin B12/iron defi ciency is well recognized in the literature but seldom considered in practice. Note the normal MCV that became microcytic when the vitamin B12 defi ciency was corrected. A microbiological component to nutritional defi ciency, H. pylori, is very common in the elderly and, ulcers or no ulcers, requires consideration. Biopsy is not necessary for reasonably reliable identifi cation of affected persons; serologic tests are available. However, after the gastric damage has been done, nutritional support may be necessary. Nonresponse to a particular form of oral iron supplement could involve gastric pH, bowel loss or disease, malabsorption secondary to vitamin B12 defi ciency, or other components of her diet which reduce iron absorption.
DIAGNOSIS: Iron Defi ciency and Vitamin B12
Defi ciency AnemiaCASE 10.3A 35-year-old woman with type I diabetes was admitted to the hospital with severe anemia, vomiting, and fever. She had not felt well for the past several months. She had lost more than 25 lb without dieting. Physical examination revealed a pale and slightly obese female with a distended abdomen. She was the mother of two young children, ages 3 and 5. Her menstrual periods were regular. A CBC, blood glucose, urinalysis, and pregnancy test were ordered.
■ Laboratory DataHemoglobin 11.40 g/dL RBC 4.06 ´ 1012/LHematocrit 35.5% MCV 87 fLMCH 28.1 MCHC 32 g/dLRDW 16% WBC 22.1 ´ 109/LHer peripheral blood smear showed abnormal erythrocyte morphology, anisocytosis, poikilocytosis, and some teardrop (dacryocytes) cells. Her serum blood glucose was elevated. Her urinalysis was normal, except for an elevated blood glucose. The result of her pregnancy test was negative. A follow-up ultrasound of the abdomen revealed a 20-cm extrauterine mass. Subsequent surgical excision of the mass revealed a malignant epithelial tumor of the left ovary with metastases to the pelvic lymph nodes, opposite ovary, and right lung.
■ Questions1. Does this patient have AOI?2. Which hematopoietic cells are involved in an infl ammatory response?3. What are the characteristic iron and iron storage results in anemia of chronic infl ammation?
■ Discussion1. This patient has AOI subsequent to a malignancy. In cases of malignancy, it has been shown that anemia may develop when the neoplasm persists for even a few weeks.2. Cellular reactions to injury involving infl ammation are macrophages, lymphocytes, and neutrophils. 3. Typically, patients with anemia of chronic infl ammation demonstrate low serum iron and decreased TIBC with increased iron stores in macrophages.
DIAGNOSIS: Anemia of Infl ammation Secondary to Metastatic Carcinoma Originating in the Ovary
REVIEW QUESTIONS1. The etiology of IDA isA. nutritional defi ciency B. faulty iron absorptionC. excessive loss of iron D. all of the above
2. Iron defi ciency is still common inA. toddlers B. adolescent girlsC. women of childbearing age D. all of the above
Questions 3 through 7: Match the following categories with an appropriate example. (Use an answer only once)3. _____ Decreased iron intake4. _____ Faulty iron absorption5. _____ Pathological iron loss6. _____ Physiological iron loss7. _____ Increased iron utilizationA. SprueB. Colon cancerC. Adolescent growth spurtD. MenstruationE. Meat-poor diet
8. The average adult has _____ g of total iron.A. 0.2 to 1.4 B. 1.5 to 3.4C. 3.5 to 5.0 D. 5.1 to 10.0
9. Most functional iron in humans is found inA. the bone marrowB. the liverC. hemoglobin molecules of erythrocytes (RBCs)D. the free hemoglobin in the circulation
Questions 10 and 11: Approximately (10) _____% of iron from food is in the form of (11) _____ iron.10.A. 25 B. 50C. 70 D. 90
11.A. Nonheme B. Heme
12. Most ingested iron is readily absorbed into the body in theA. stomach and duodenum B. duodenum and upper jejunumC. ileum and duodenum D. upper jejunum and ileum
13. Transferrin represents aA. storage form of iron B. beta globulin that moves ironC. glycoprotein that moves iron D. both B and C
14. In IDA, the erythrocytic indices are typicallyA. MCV increased, MCH decreased, and MCHC decreasedB. MCV decreased, MCH decreased, and MCHC decreasedC. MCV decreased, MCH increased, and MCHC decreasedD. MCV decreased, MCH decreased, and MCHC normal
15. The peripheral blood smear demonstrates _____ red blood cells in IDA.A. microcytic, hypochromic B. macrocytic, hypochromicC. macrocytic and spherocytic D. either A or B
16. In IDA, the A. serum iron is severely decreased and the TIBC is increasedB. serum iron is decreased and the TIBC is normalC. serum iron is normal and the TIBC is normalD. serum iron is increased and the TIBC is normal
17. Anemias of infl ammation/chronic diseases can be caused byA. infl ammation B. infectionC. malignancy D. all of the above
18. AOI can result fromA. inappropriately decreased erythropoietinB. suppression of erythropoiesis by cytokines fromactivated macrophages and lymphocytesC. impaired iron metabolismD. all of the above
19. The typical peripheral blood fi lm of a patient with AOI typically reveals _____ erythrocytes.A. microcytic, hypochromic B. macrocytic, hypochromicC. normocytic, normochromic D. many spherocytes
20. Leukoerythroblastosis can appear as _____ on a peripheral blood smear.A. immature leukocytes B. immature erythrocytesC. immature thrombocytes D. both A and B
21. What is the most appropriate treatment for AOI?A. Red blood cell transfusion B. Iron therapyC. Erythropoietin injections D. Treatment of the infl ammatory condition22. Sideroblastic anemia can be caused byA. congenital (chromosomal) defectB. drugs (e.g., chloramphenicol)C. association with malignant disorders (e.g., acute myelogenous leukemia)D. all of the above
23. A common feature of sideroblastic anemia isA. ringed sideroblasts B. decreased serum ironC. decreased serum ferritin D. macrocytic red blood cells
24. The greatest portion of operational body iron is normally contained in what compound?A. Hemoglobin B. FerritinC. Cytochromes D. Myoglobin
25. Storage iron in the human body is
A. found in hepatocytes B. found in macrophagesC. sequestered as ferritin D. all of the above
26. The most sensitive assay for the diagnosis of hereditary hemochromatosis (HH) isA. serum iron B. serum iron–binding capacityC. transferrin D. transferrin saturation
1. D 2. D 3. E 4. A 5. B6. D 7. C 8. C 9. C 10. D11. A 12. B 13. D 14. B 15. A16. A 17. D 18. D 19. C 20. D21. D 22. D 23. A 24. A 25. D 26. D
HEMOGLOBINOPATHY & THALASSEMIA – CH 13, 14CASE 13.1An 18-year-old black woman was admitted to the hospital for elective surgery. She had a routine preoperative CBC and urinalysis.
■ Laboratory Data Hemoglobin 13.0 g/Dl Hct 40%RBC 4.35 × 1012/L WBC 7.3 × 109/L MCV 92 fL MCH 29.9 pgMCHC 33 g/Dl
The patient’s peripheral blood smear revealed a normochromic, normocytic pattern; however, a moderate number of target cells (codocytes) were noted throughout the smear. A repeat blood smear obtained from fi ngertip bloodagain had a moderate number of codocytes present. The urinalysis revealed no abnormalities. A hematology technician notifi ed the surgeon and anesthetist of the abnormal RBC morphology. On receipt of these results, the anesthetist postponed surgery and ordered a sickle cell preparation, sickle cell screening test, and hemoglobin electrophoresis. The results were Sickle cell preparation positive Hb S screening test positiveHb electrophoresis: Hb A 63%, Hb F 3%, and Hb S 34%
■ Questions1. Why was it important to establish a diagnosis in this patient’s asymptomatic state?2. What kind of disorder does this patient have?3. What is the etiology of this patient’s condition?
■ Discussion1. This patient has sickle cell trait, which, under ordinary conditions, is usually asymptomatic except for the presence of codocytes on a peripheral blood smear. However, the fact that the patient was to undergo elective surgery made it important for the anesthetist to be aware of the patient’s condition to carefully monitor the patient to prevent hypoxia.2. The presence of a great number of true codocytes on a peripheral fi lm is highly suggestive of hemoglobinopathy. Because the codocytes (target cells) persisted on repeated smears, the possibility that the target appearance was an artifact was eliminated. Supplementary laboratory assays provided the differential information needed to establish the diagnosis of sickle cell trait. The profi le of this patient is typical of sickle cell trait. She is a heterozygous Hb A–Hb S. Both the sickle cell preparation, which exposed the cells to reduced oxygen levels, and the Hb S screening test confi rmed the electrophoresis fi ndings of the presence of the abnormal type S hemoglobin. 3. This patient has hemoglobinopathy, which is a genetically inherited trait. In her case, she received only one gene for S-type hemoglobin and was fortunate to have received a normal gene for A-type hemoglobin. Approximately 10% of American blacks possess the sickle cell trait. Identifying its existence in an individual is important for two reasons. Exposure to reduced oxygen levels will cause some of the cells of the individual to sickle, and the genetic consequences to future offspring are an important aspect of prenatal counseling in both men and women who possess the trait.DIAGNOSIS: Sickle Cell Trait
CASE 13.2The 5-year-old son of a Liberian exchange student was hospitalized because of severe diarrhea, abdominal distention, and splenomegaly. The child had been previously diagnosed in Europe as suffering from sickle cell anemia and had experienced several episodes of sickle cell crisis. On admission, the following tests were ordered: CBC, platelet count, bilirubin determination, hemoglobin electrophoresis, Hb S screening test, electrolyte studies, urinalysis, and stool culture.
■ Laboratory DataHemoglobin 5.8 g/dL Hct 19%RBC 2.0 × 1012/L MCV 96 fLMCH 29 pg MCHC 31 g/dLThe total WBC count was 8.7 × 109/L. The peripheral blood smear revealed moderate anisocytosis, macrocytosis,microcytosis, poikilocytosis, polychromatophilia, occasional Howell-Jolly bodies, moderate basophilic stippling, many sickled RBCs (drepanocytes), and 12 (nucleated RBCs) metarubricytes/100 WBCs. The distribution of platelets was normal on the blood smear, and the total platelet count was 0.42 × 1012/L. The patient’s total serum bilirubin was 6.0 mg/dL. Hemoglobin electrophoresis demonstrated Hb S 78% and Hb F 22%. The Hb S screening test result was positive. A routine urinalysis was positive for occult blood, and the stool culture was normal. The patient had severely abnormal electrolytes.
■ Questions1. What is the cause of this patient’s condition?2. What is the clinical course of this disease?3. Explain the presence of the drepanocytes on the peripheral blood fi lm.
■ Discussion1. This patient had been previously diagnosed as having sickle cell anemia. However, the current crisis was undoubtedly precipitated by the dehydration caused by severe diarrhea. Although the exact trigger mechanism is not really known, events such as dehydration, fatigue, and emotional stress can trigger a crisis episode in patients with sickle cell anemia. 2. Sickle cell anemia takes a chronic clinical course. The course of the disease is characterized by hemolytic episodes, severe organ damage, and painful, acute episodes involving both bones and muscles. Painful crises are a feature of this disease. The crises correspond to obstruction of the microcirculation by the sickled cells, followed by ischemia, which produces the associated pain and sometimes consequent necrosis of tissues.3. Congestion in the microcirculation, tissue hypoxia, and the lowering of blood pH are all factors that promote the gelation of Hb S. With this gelation, the sickle cell assumes its characteristic shape. Many of these cells will assume a discoid shape following reoxygenation; however, dense sickle cells are irreversibly sickled. These cells have a distinctive boat shape and will not resume the normal discoid shape after reoxygenation.
DIAGNOSIS: Sickle Cell Anemia
CASE 13.3A 21-year-old white female college student of Greek ethnicity visited her gynecologist in San Francisco. She appeared to be healthy and was 3 months pregnant. She was concerned about her future child because she had been diagnosed as a child as having heterozygous b-thalassemia. However, she had never had any “blood problems” but knew that her disorder had been inherited. The following tests were ordered: CBC, urinalysis, and hemoglobin electrophoresis.
■ Laboratory DataHemoglobin 11.1 g/dL Hct 29%RBC 4.2 × 1012/L Her WBC count was 5.8 × 109/L. The peripheral blood smear revealed the presence of signifi cant microcytosis, 2+ hypochromia, and some codocytes (target cells). MCV 69 fLMCH 26.4 pg MCHC 37 g/dLThe distribution of platelets was normal on the peripheral smear. The hemoglobin electrophoresis revealed a slight increase in the Hb A2 fraction (patient, 3.5%; normal, 2% to 3%) and the F fraction (patient, 2%; normal, <1%). The urinalysis was normal. On receipt of these results the physician referred the patient to a research laboratory for prenatal testing and counseling.
■ Questions1. Explain the asymptomatic state and peripheral blood fi ndings in this patient.2. What kind of advanced prenatal testing can be performed?3. Is there an option for carriers who do not want to risk having a child with thalassemia?
■ Discussion1. Patients with heterozygous b-thalassemia are frequently asymptomatic. The expression of this disorder can range from an asymptomatic state, as in this patient, to a fairly severe anemia. Her peripheral blood fi lm is typical of the heterozygous patient with microcytosis, hypochromia, and codocytes. This condition can be confused with iron defi ciency anemia until further laboratory studies are conducted, such as serum iron and TIBC and hemoglobin electrophoresis.2. Modern prenatal testing for hematological disease began in 1974. Before that time, chromosomal studies were performed on amniotic fl uid in older women with a high risk of Down syndrome or to determine fetal sex if the patient was at risk for a sex-linked disorder. Methods for obtaining fetal blood in utero were established in 1974, and this led to the development of prenatal diagnosis of any blood disorder that expressed itself in utero. The fi rst disorders to be studied were the hemoglobinopathies, specifi cally thalassemia. Recently, a third technique that uses amniotic fl uid was developed for use with DNA probes. Sampling of fetal blood remains the method of choice for the detection of hematological diseases for which DNA probes are not available. During the midtrimester, blood is aspirated from the placenta. To determine the proportion of fetal blood in the sample, RBC size (MCV) is performed immediately on the specimen. Fetal erythrocytes have an average MCV of 140 fL, compared with adult or maternal RBCs, which have an average MCV of 100 fL. The sample is then labeled with a radioactive substance and incubated to label newly synthesized globin chains. Mutant b-globins are detected with this technique because they separate from normal b-globin on chromatographic analysis. The diagnosis of a- or b- thalassemia can be made based on either the absence of or the substantially reduced amount of globin in the sample. By this method, 25% of the samples lead to a diagnosis of thalassemia in cases in which the fetus is at risk. This frequency is proportional to the expected frequency for autosomal recessive disorders. If amniocentesis studies are done, the fl uid is obtained at 16 to 20 weeks of gestation. The sample must contain enough fetal cells to provide DNA for studies of the globin genes. Earlier studies may now be done using chorionic villi specimens. All these procedures are aimed at the early diagnosis ofhematological diseases of genetic origin. 3. Assisted reproductive therapy is an option for carriers who do not want to risk having a child with thalassemia. A new technique, PGD, used in conjunction with in vitro fertilization, may enable parents with thalassemia or thalassemia trait to give birth to healthy babies. Embryos created in vitro are tested for the thalassemia gene before being implanted into the mother, allowing only healthy embryos to be selected.
DIAGNOSIS: Prenatal Patient with Thalassemia Minor(Heterozygous b-thalassemia)
CASE 13.4A 23-year-old Italian woman is noted to be suffering from mild anemia in a preemployment physical examination. The patient denied any signifi cant illness in the past. She has no history of joint or abdominal pain and she was not sickly as a child. She had been told on several occasions that she has anemia and was given medications containing iron. She has not noted any unusual bleeding. Her menstrual periods are regular at monthly intervals and they last for about 3 days. She has never been pregnant. She has no history of excessive alcohol intake. Physical examination revealed an enlarged spleen. She has no icterus, purpura, or lymphadenopathy. Her liver is not enlarged.
■ Laboratory DataHemoglobin 11.0 g/dL Hematocrit 35%RBC 5.0 × 1012/L WBC 9.5 × 109/LThe peripheral blood smear shows target cells, an occasional sickle-shaped cell, microcytes, and slight hypochromia. The reticulocyte count is 7.2%.
■ Questions1. What is the differential diagnosis?2. What test will aid in the differential diagnosis?3. What is the probable diagnosis?4. How do you account for this patient’s benign course?5. Why does the patient have disease, compared to AS individuals who are asymptomatic?6. What complications might arise in the future?
■ Discussion1. Striking target cells are seen in liver disease and hemoglobinopathies. The fact that hemolysis is present and this patient lacks clinical evidence of liver disease both favor the latter alternative.2. The following will aid in the differential diagnosis: hemoglobin electrophoresis, serum Fe/TIBC to rule out iron defi ciency, liver function tests, and solubility test for the presence of hemoglobin S. This patient’s liver function was normal. The hemoglobin electrophoresis on acrylamide gel was abnormal.3. Sickle b+ thalassemia4. The extent of polymer formation is less in S b+ thalassemia, owing primarily to lower MCHC and less crowding of hemoglobin molecules in the red cell. The ability to synthesize some Hb A also reduces intracellular polymer formation.5. Cells contain much more Hb S and therefore will form more polymer.6. Proliferative retinopathy and avascular necrosis of hip; these complications are particularly common in sickle b+ thalassemia and in SC disease for unclear reasons.
DIAGNOSIS: Sickle b-thalassemia
CASE 13.5A 50-year-old white woman wanted to realize a lifelong dream of trekking in Nepal. One year before her expected date of departure, she began a vigorous exercise program to build up her strength and endurance for this trip. She was in excellent health at the beginning of her training and at her departure from the East Coast of the United States for Katmandu, Nepal. After a few days on the trail, as the group was approaching the base camp at 6,500 ft, the patient began to experience shortness of breath, abdominal pain in her left upper quadrant, and blood in her urine. She was rushed to the nearest emergency station and then transported by air lift to Katmandu. In Katmandu, the patient was examined and found to have a very slightly enlarged spleen with slight tenderness. A CBC and urinalysis were ordered.
■ Laboratory DataRBC 3.82 × 1012/L Hematocrit 29%Hemoglobin 9.5 g/dL WBC 15.1 × 109/LPlatelets 455 × 109/L MCV 74 fLMCH 25 pg MCHC 33 g/dL
■ Leukocyte Differential1% band neutrophils 68% segmented neutrophils 5% eosinophils 1% monocytes 25% lymphocytes The peripheral blood smear revealed 2+ polychromatophilia, 2+ anisocytosis, and 2+ target cells. Urinalysis showed 3+ blood.
■ Questions1. What is the signifi cance of the laboratory fi ndings?2. Do any of the other fi ndings suggest a hemoglobinopathy?3. What other tests would be valuable?4. What precipitated the incident?5. This woman is not of African ancestry. How can she be a sickle cell carrier?
■ Discussion1. The targeted red cells could be caused by an artifact, and a repeat blood smear should be made. However, the presence of polychromatophilia, targeted red blood cells, and a slight anemia are suggestive of hemoglobinopathy. 2. Yes. The presence of an enlarged spleen indicates that a hematological condition might exist. Painless hematuria that is otherwise unexplained can occur in sickle cell trait. 3. A reticulocyte count and hemoglobin electrophoresis were ordered for this patient. In this case, the results revealed an increased reticulocyte count (3.5%), and the hemoglobin electrophoresis revealed the presence of Hb A and Hb S.4. In the United States, the heterozygous state (sickle cell trait [AS]) is usually considered to be a benign condition in about 9% of Americans of African descent. However, at moderately high altitudes (5,400 to 9,600 ft above sea level), sickle cell carriers can express clinical symptoms (e.g., splenic infarction causing abdominal pain). Increased fragility of RBCs seen in sickle cell trait can lead to hematuria. Other conditions that can precipitate a sickle cell crisis in carriers include anesthesia, unpressurized aircraft, congestive heart failure, and lower respiratory tract problems.5. In addition to being found in persons of African ancestry, sickle cell anemia and trait occur in Mediterranean countries (e.g., Sicily), the Arabian peninsula, and India. Isolated cases have been found in other countries.
DIAGNOSIS: Sickle Cell Trait
CASE 13.6A 30-year-old pregnant Thai woman was referred to a hematologist because of anemia. The hematologist ordered a hemoglobin, hematocrit, and RBC indices; serum iron; percent saturation; and urinalysis.
■ Laboratory DataHematocrit 27% Hemoglobin 8.1 g/dLMCV 65 fL MCH 20 pg MCHC 30 g/dL
Serum iron and percent saturation were within normal limits. Urinalysis results were also normal. ■ Questions
1. What is the cause of this patient’s low hemoglobin and hematocrit?2. What follow-up laboratory assays should be ordered?3. What confi rmatory laboratory assay should be performed?4. What is the etiology of her hemoglobinopathy?
■ Discussion1. During pregnancy many women suffer from iron defi ciency anemia, which is characterized by a decreased hemoglobin and hematocrit and decreased red blood cell indices. However, this patient was not iron defi cient according toher serum iron and percent saturation values. 2. Because of the patient’s Asian ancestry and the exclusion of iron defi ciency anemia as a diagnosis, a hemoglobin electrophoresis was ordered. The results of the procedure demonstrated an abnormal hemoglobin band whosemigration pattern was suggestive of Hb H.3. Hb H is an unstable hemoglobin. Demonstration of Heinz bodies, inclusions formed by precipitated unstable hemoglobin in red blood cells that are oxidatively denatured and stained with brilliant cresyl blue stain, confi rms the presence of the unstable hemoglobin.
4. The genetic defect responsible for the presence of Hb H is a gene deletion. a-Thalassemias are most frequently caused by deletion mutations that affect globin chain synthesis. Anemia associated with thalassemia is causedby diminished production of functional hemoglobin and increased destruction of red blood cells compromised by intracellular inclusions.
DIAGNOSIS: a-Thalassemia
REVIEW QUESTIONS1. The common denominator in the hemoglobinopathies is that all areA. structural defects in the erythrocyte membraneB. metabolic defects in the erythrocytic physiologyC. inherited or genetic defects related to hemoglobinD. acquired defects related to hemoglobin
2. Hemoglobinopathies can be classifi ed asA. abnormal hemoglobin globulin structureB. a defect of hemoglobin globulin synthesisC. a combination of defects of both structure and synthesisD. all of the above
3. Normal adult hemoglobin contains the following components:Hb A (95% to 98%), Hb A2 (2% to 3%), Hb A1 (3% to 6%), and Hb F (<1%).A. True B. False
4. In the hemoglobinopathies, a trait is described asA. heterozygous and asymptomatic B. heterozygous and symptomaticC. homozygous and asymptomatic D. homozygous and symptomatic
5. In sickle cell anemia the cause isA. a change of a single nucleotide (GAT to GTT)B. the substitution of valine for glutamic acid at the sixth position on the beta chain of the hemoglobin moleculeC. not geneticD. both A and B
6. In sickle cell disease the abnormality is related toA. the rate of synthesis of hemoglobinB. an abnormal molecular structure of hemoglobinC. an acquired defectD. a membrane dysfunction
7. One of the two most common monogenetic diseases of man isA. sickle cell trait B. sickle cell anemiaC. a-thalassemia D. Hb SC disease
8. If a patient with sickle cell anemia is in an acute crisis state, peripheral blood smears may exhibitA. leptocytes B. drepanocytesC. ovalocytes D. stomatocytes
9. What estimated percentage of black Americans are heterozygous for Hb S?A. 4% B. 8%C. 12% D. More than 25%
10. What factors contribute to the sickling of erythrocytes in sickle cell anemia crisis?A. Increase in blood pH and increase in oxygenB. Extremely hot weatherC. Extremely reduced oxygen and increased acidity inthe bloodD. Sickling is spontaneous
11. The most common complaint associated with sickle cell anemia?A. Acute pain B. Organ or tissue failureC. Stroke D. All of the above
12. Thalassemias are characterized by A. abnormal amino acid sequence of the hemoglobin moleculesB. defective iron synthesisC. absence or decrease in synthesis of one or moregloblin subunitsD. skeletal membrane defects
13. Homozygous b-thalassemia patients haveA. no manifestations of anemia B. only mild anemia

C. moderate anemia D. severe transfusion-dependent anemia
14. In a-type thalassemia, with three inactive a genes, which of the following is characteristic?A. Hb A2 B. Hb AC. Hb H D. Hb F and A2
15. What is the primary risk to thalassemia major patients who receive frequent and multiple blood transfusions?A. Iron overload B. Citrate toxicityC. Polycythemia D. Hyperviscosity
16. The peripheral blood smear in silent state patients with a-thalassemia typically appears asA. normochromic, normocytic B. microcytic, hypochromicC. macrocytic, normocytic D. macrocytic, hypochromic
17. The characteristic hemoglobin concentration in a patient’s silent state with heterozygous b-thalassemia isA. Hb A level normal B. Hb A2 increasedC. Hb A2 level decreased D. Hb F level increased
18. Deoxyhemoglobin C hasA. decreased solubility B. increased solubilityC. the ability to form intracellular crystals D. both A and C
19. The incidence of Hb E hemoglobinopathy is highest inA. Southeast Asia B. ChinaC. Vietnam D. Native Americans
20. Most unstable hemoglobinsA. are inherited autosomal dominant disordersB. result from amino acid substitutions or deletionsC. are hemoglobin variantsD. all of the above
1. C 2. D 3. A 4. A 5. D 6. B7. B 8. B 9. B 10. C 11. A 12. C13. D 14. C 15. A 16. A 17. A 18. D19. A 20. D