Embed Size (px)
Citation preview
Hematologic Problems Including Bleeding, Clotting, Venous Thromboembolic Disease and
Newer Anticoagulant Drugs
Thomas W. Wakefield MDStanley Professor
Section of Vascular SurgeryDirector Samuel and Jean Frankel Cardiovascular Center
University of Michigan
Andrea T. Obi MDAssistant Professor, Vascular Surgery
University of [email protected]
Disclosures
None
Arterial versus Venous thrombosisCommon “truths”
Arterial thrombi are white
Venous thrombi are red
“venous and arterial thrombosis are two different diseases with regards to pathophysiology, epidemiology and treatment strategies”
Harrison’s Principles of Internal Medicine 17th ed. New York: McGraw-Hill; 2008.
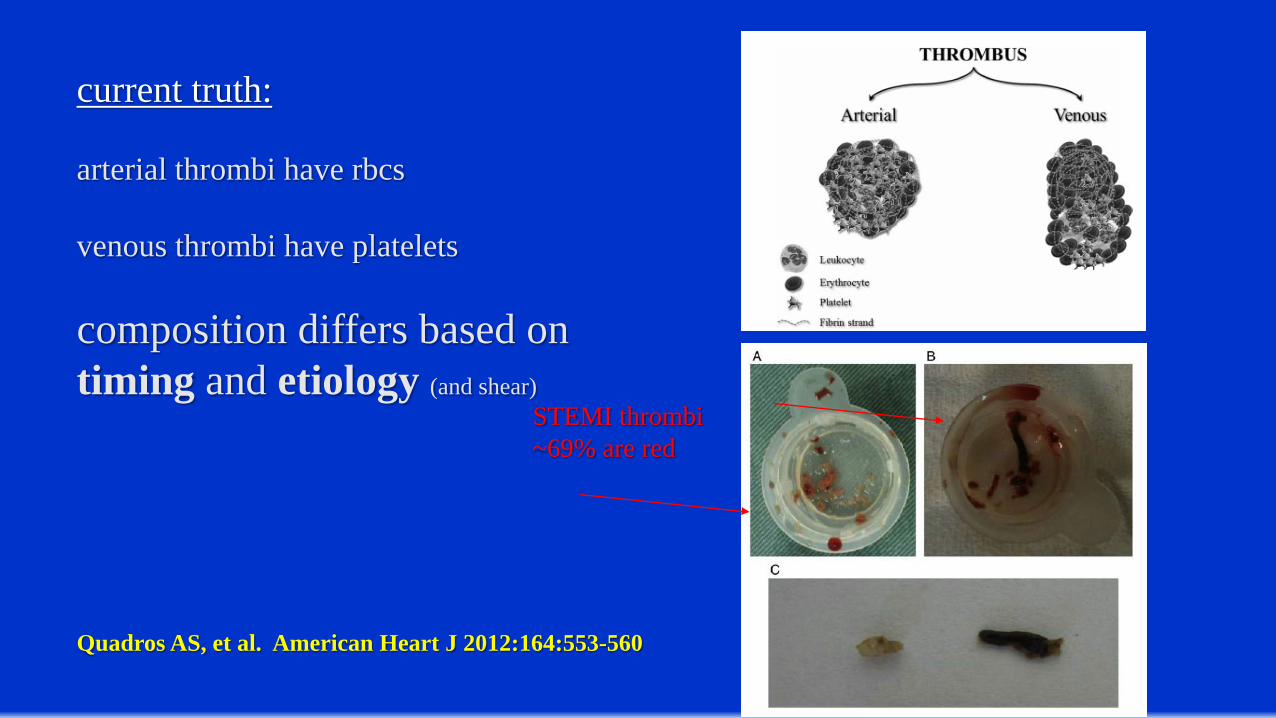
STEMI thrombi~69% are red
current truth:
arterial thrombi have rbcs
venous thrombi have platelets
composition differs based on timing and etiology (and shear)
Quadros AS, et al. American Heart J 2012:164:553-560
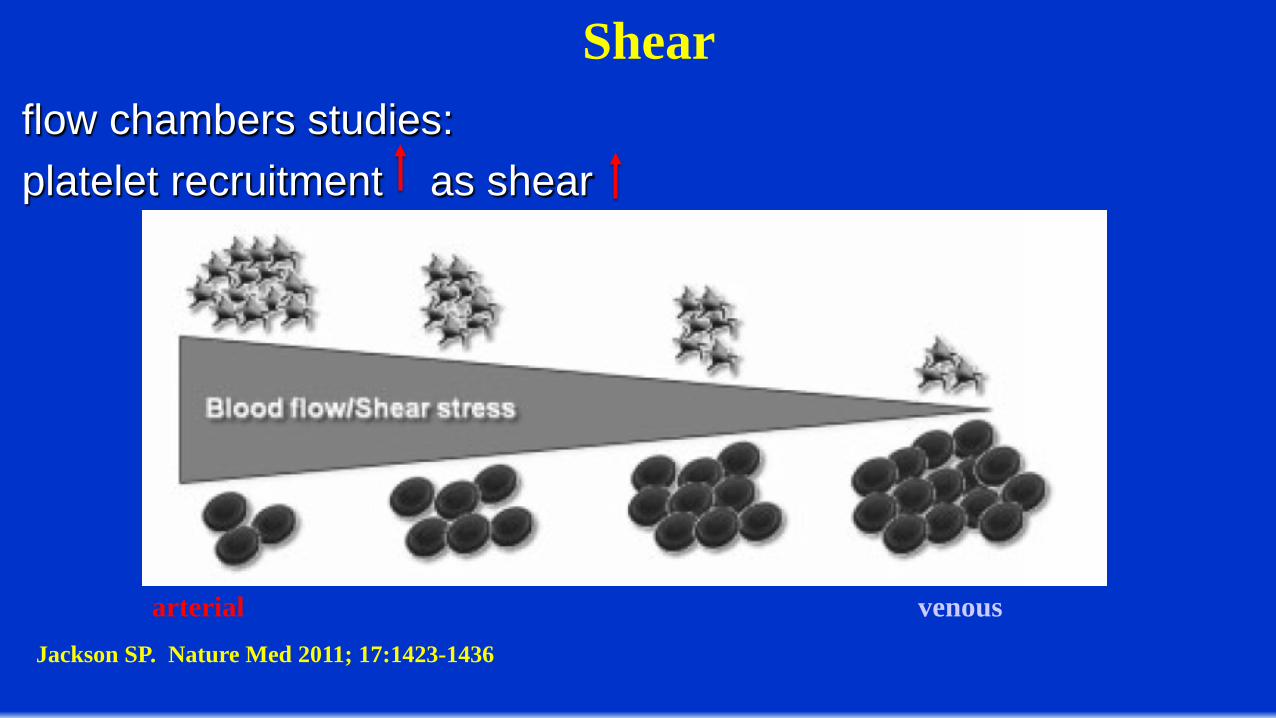
flow chambers studies:platelet recruitment as shear
Jackson SP. Nature Med 2011; 17:1423-1436
arterial venous
Shear
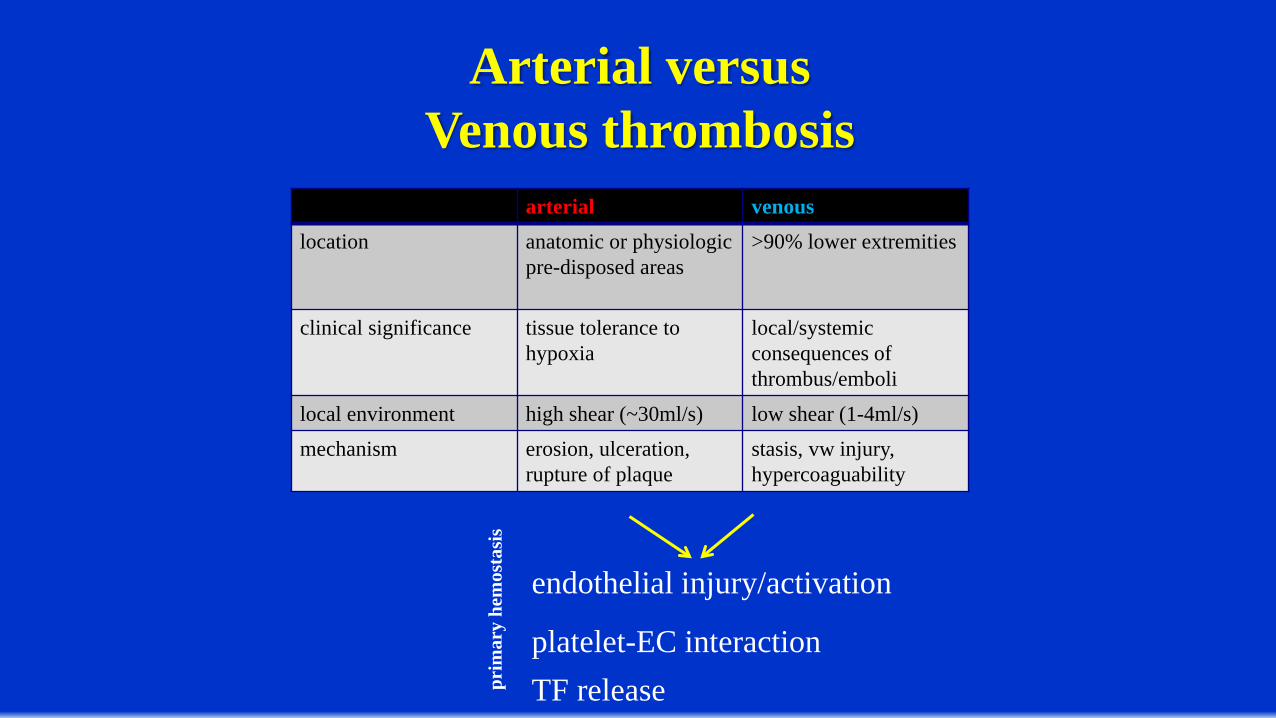
arterial venouslocation anatomic or physiologic
pre-disposed areas>90% lower extremities
clinical significance tissue tolerance to hypoxia
local/systemicconsequences of thrombus/emboli
local environment high shear (~30ml/s) low shear (1-4ml/s)mechanism erosion, ulceration,
rupture of plaquestasis, vw injury, hypercoaguability
endothelial injury/activation
platelet-EC interactionTF releasepr
imar
y he
mos
tasi
s
Arterial versus Venous thrombosis
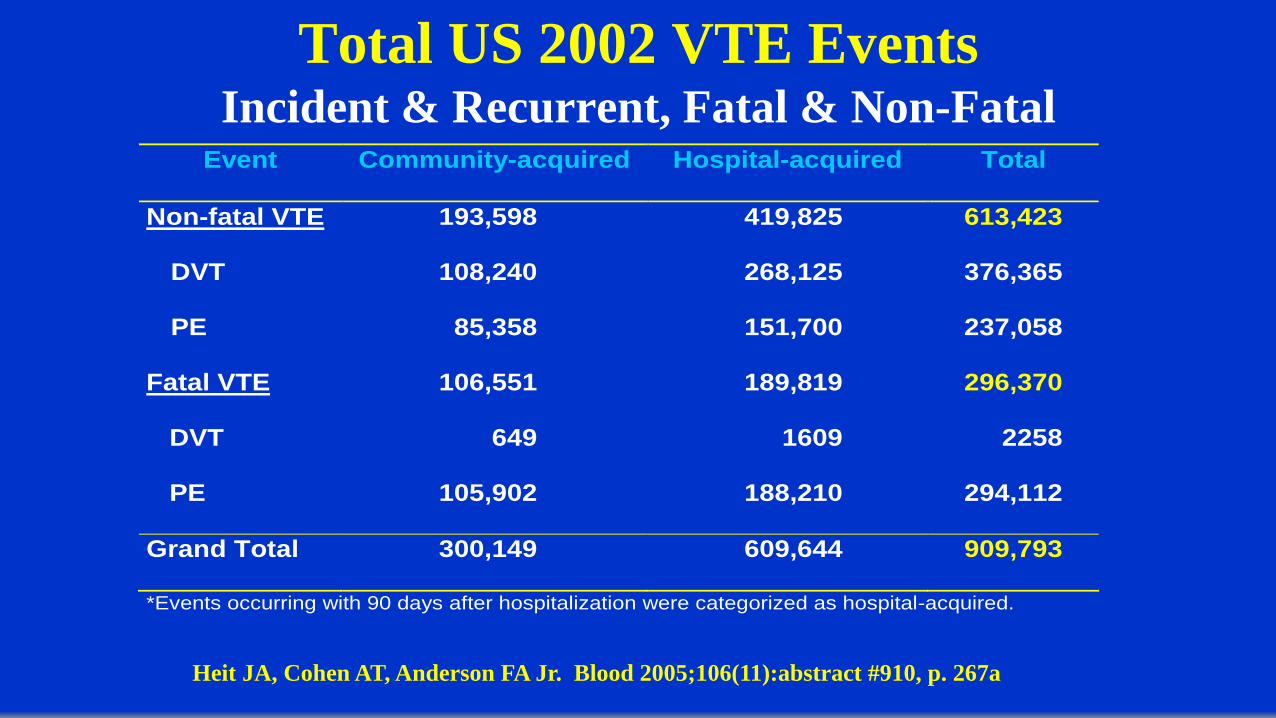
Total US 2002 VTE EventsIncident & Recurrent, Fatal & Non-Fatal
Event Community-acquired Hospital-acquired Total
Non-fatal VTE
DVT
PE
193,598
108,240
85,358
419,825
268,125
151,700
613,423
376,365
237,058
Fatal VTE
DVT
PE
106,551
649
105,902
189,819
1609
188,210
296,370
2258
294,112
Grand Total 300,149 609,644 909,793
*Events occurring with 90 days after hospitalization were categorized as hospital-acquired.
Heit JA, Cohen AT, Anderson FA Jr. Blood 2005;106(11):abstract #910, p. 267a
VTE represents a commonly encountered post-operativecomplication for the vascular surgeon.
VTE rate is 9.4%–13.2% following lower extremity amputationBandeira FC et al, Intl Angiol 2008; 27:489-493; Struijk-Mulder MC et al, JTH 2010; 8:2680-268
VTE rate is 2.4% in patients undergoing open aortic surgery; increases with each risk factor (to a maximum of 8% with ≥4 risk factors): operative time ≥ 5 hours, chronic
steroid use, preoperative dyspnea, body mass index (BMI) ≥ 30, post-operative pneumonia, post-operative mechanical ventilation >48 hours or return to operating room within 30 days
Scarborough JE et al, J Am Coll Surg 2012; 214:620-626
Among all types of outpatient surgery, superficial venous procedures carry the highest risk for VTE (adjusted ORs 13.2 and 15.6)
Pannucci CJ et al, Ann Surg 2012; 255:1093-1099
Delay in chemoprophylaxis following open lower bypass or aortic surgery increases the risk of VTE (OR 2.38)
Sutzko D et al, J Vasc Surg 2018; 67:262-271
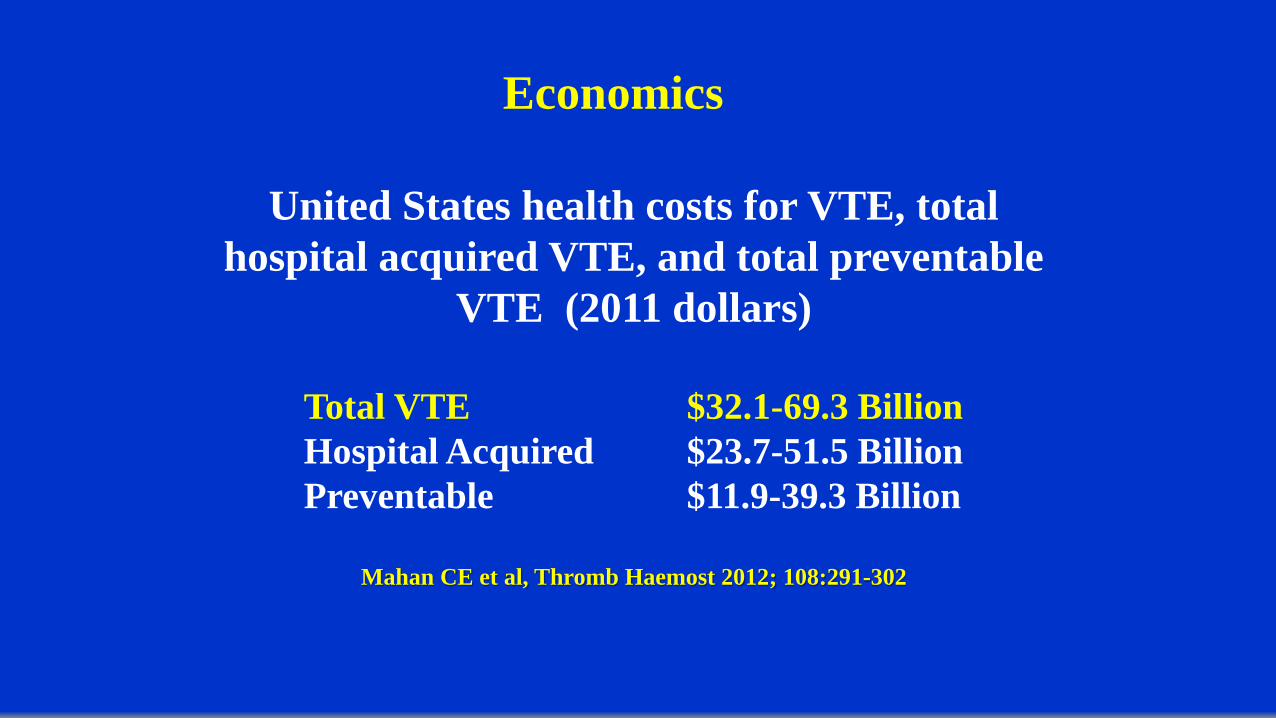
United States health costs for VTE, total hospital acquired VTE, and total preventable
VTE (2011 dollars)
Total VTE $32.1-69.3 BillionHospital Acquired $23.7-51.5 BillionPreventable $11.9-39.3 Billion
Mahan CE et al, Thromb Haemost 2012; 108:291-302
Economics
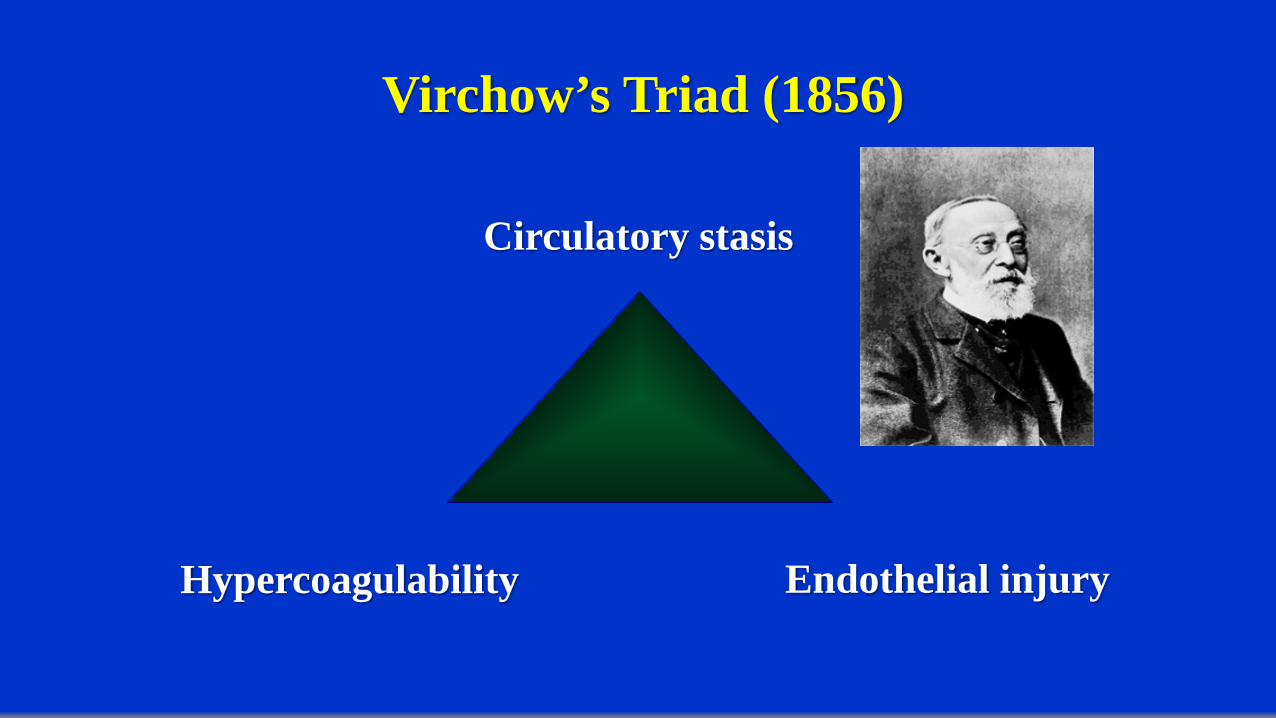
Virchow’s Triad (1856)
Circulatory stasis
Endothelial injuryHypercoagulability
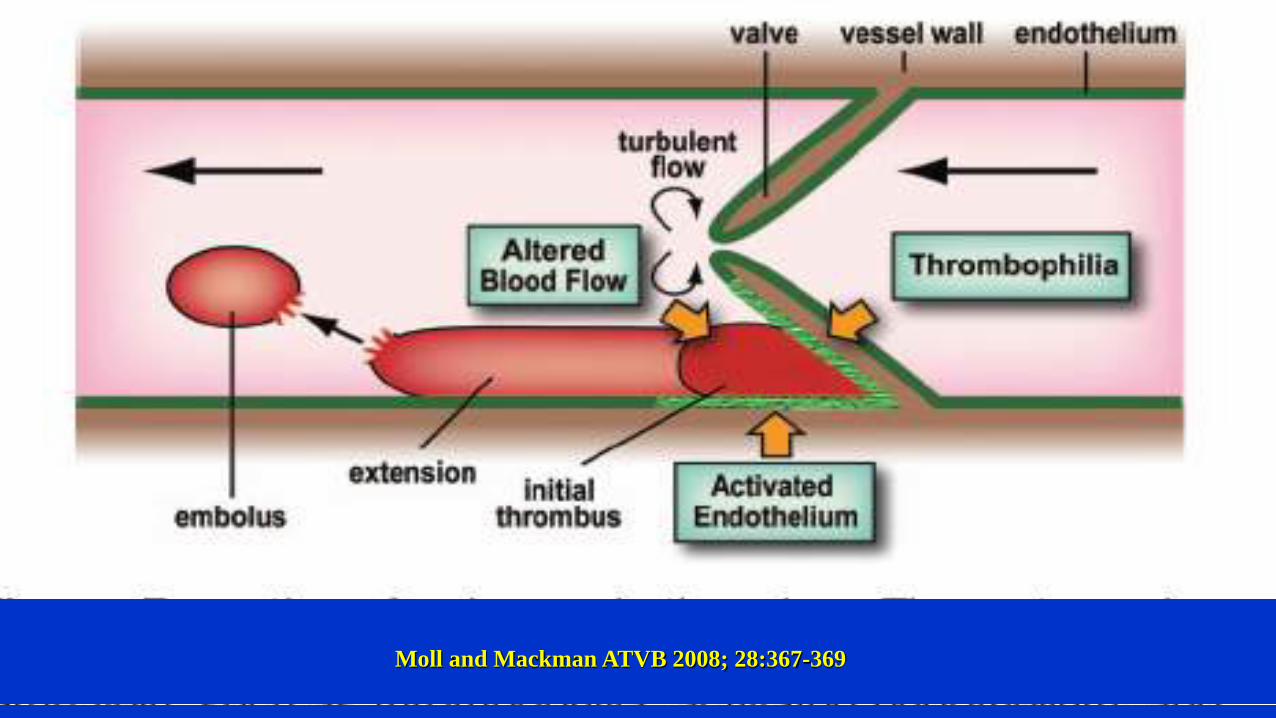
Moll and Mackman ATVB 2008; 28:367-369
mp
mp
mp
mp
mp
mpP-selectin
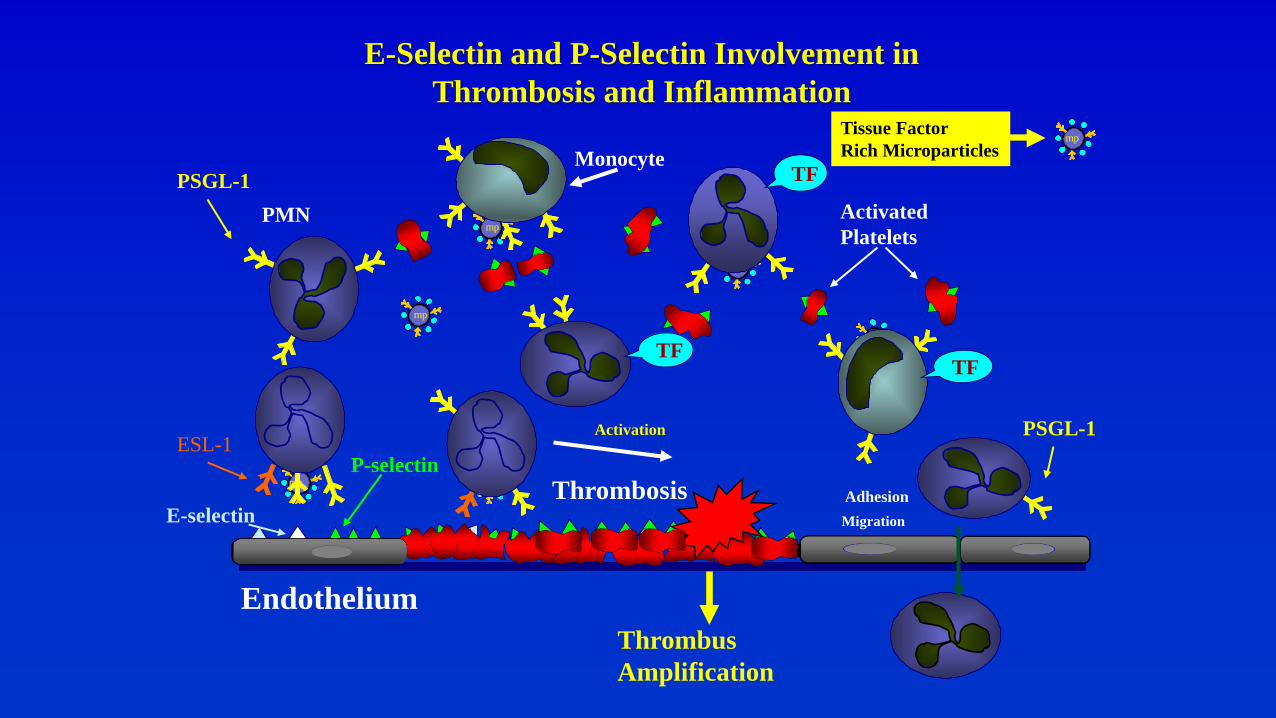
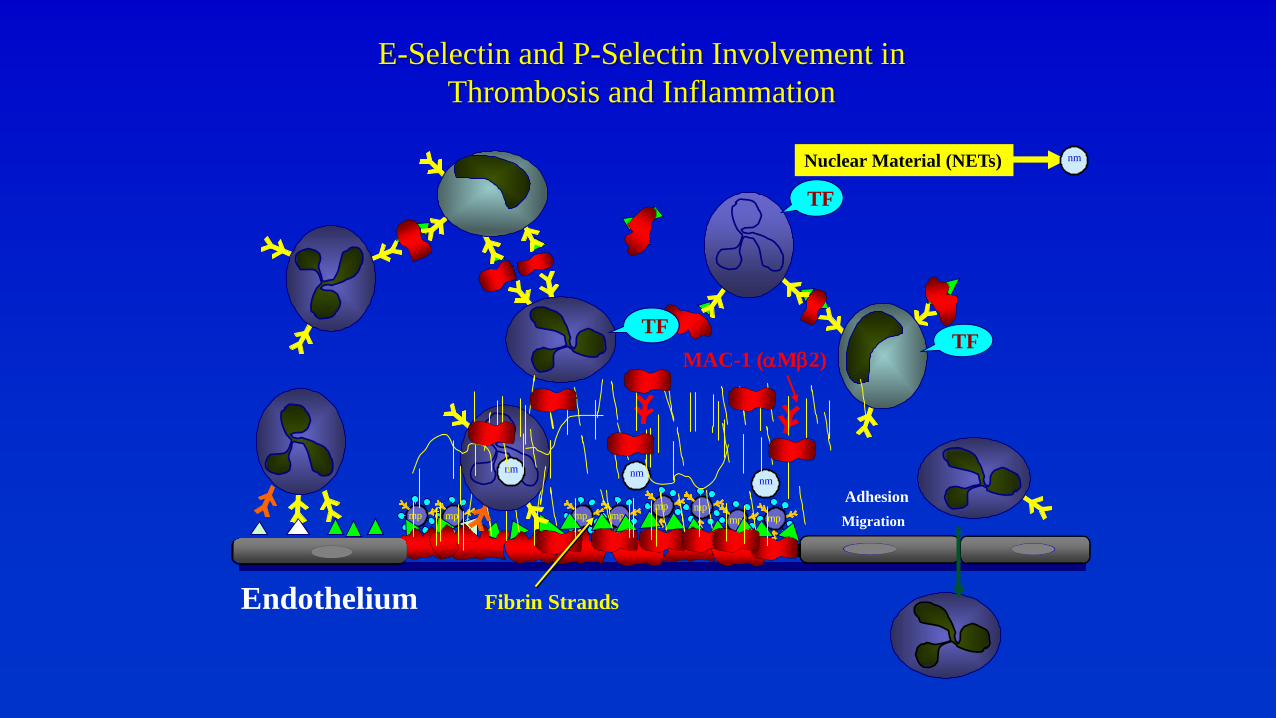
E-Selectin and P-Selectin Involvement in Thrombosis and Inflammation
Activation
MigrationAdhesion
Endothelium
Thrombosis
PMN
Monocyte
ActivatedPlatelets
TF
Tissue FactorRich Microparticles
TFTF
PSGL-1
PSGL-1
ESL-1
Thrombus Amplification
mp
E-selectin
mpmp
mp mp mp mpmp
mp
E-Selectin and P-Selectin Involvement in Thrombosis and Inflammation
MigrationAdhesion
Endothelium
TF
Nuclear Material (NETs)
TFTF
nm
Fibrin Strands
nmnm
nm
MAC-1 (αMβ2)
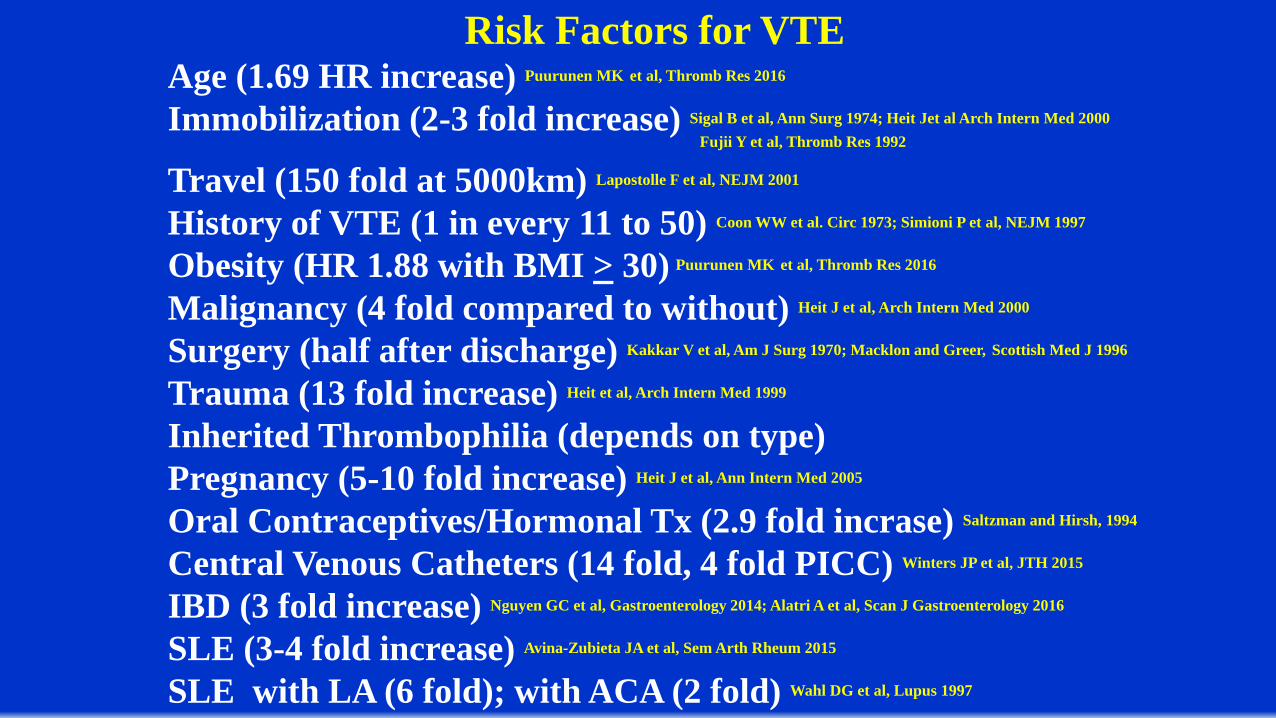
Risk Factors for VTEAge (1.69 HR increase) Puurunen MK et al, Thromb Res 2016
Immobilization (2-3 fold increase) Sigal B et al, Ann Surg 1974; Heit Jet al Arch Intern Med 2000Fujii Y et al, Thromb Res 1992
Travel (150 fold at 5000km) Lapostolle F et al, NEJM 2001
History of VTE (1 in every 11 to 50) Coon WW et al. Circ 1973; Simioni P et al, NEJM 1997
Obesity (HR 1.88 with BMI > 30) Puurunen MK et al, Thromb Res 2016
Malignancy (4 fold compared to without) Heit J et al, Arch Intern Med 2000
Surgery (half after discharge) Kakkar V et al, Am J Surg 1970; Macklon and Greer, Scottish Med J 1996
Trauma (13 fold increase) Heit et al, Arch Intern Med 1999
Inherited Thrombophilia (depends on type) Pregnancy (5-10 fold increase) Heit J et al, Ann Intern Med 2005
Oral Contraceptives/Hormonal Tx (2.9 fold incrase) Saltzman and Hirsh, 1994
Central Venous Catheters (14 fold, 4 fold PICC) Winters JP et al, JTH 2015
IBD (3 fold increase) Nguyen GC et al, Gastroenterology 2014; Alatri A et al, Scan J Gastroenterology 2016
SLE (3-4 fold increase) Avina-Zubieta JA et al, Sem Arth Rheum 2015
SLE with LA (6 fold); with ACA (2 fold) Wahl DG et al, Lupus 1997
Schulman S, Best Pract Res Clin Hem 2012; 25:361-377
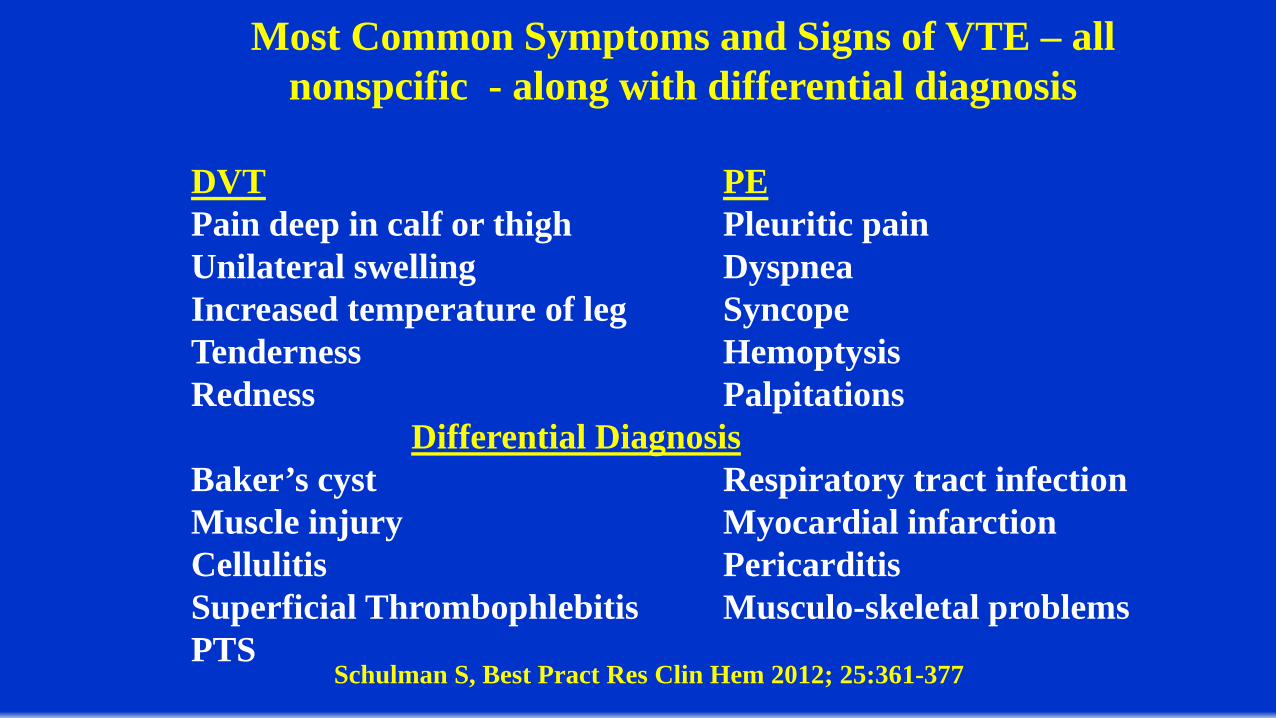
Most Common Symptoms and Signs of VTE – all nonspcific - along with differential diagnosis
DVT PEPain deep in calf or thigh Pleuritic painUnilateral swelling DyspneaIncreased temperature of leg SyncopeTenderness HemoptysisRedness Palpitations
Differential DiagnosisBaker’s cyst Respiratory tract infectionMuscle injury Myocardial infarctionCellulitis PericarditisSuperficial Thrombophlebitis Musculo-skeletal problemsPTS
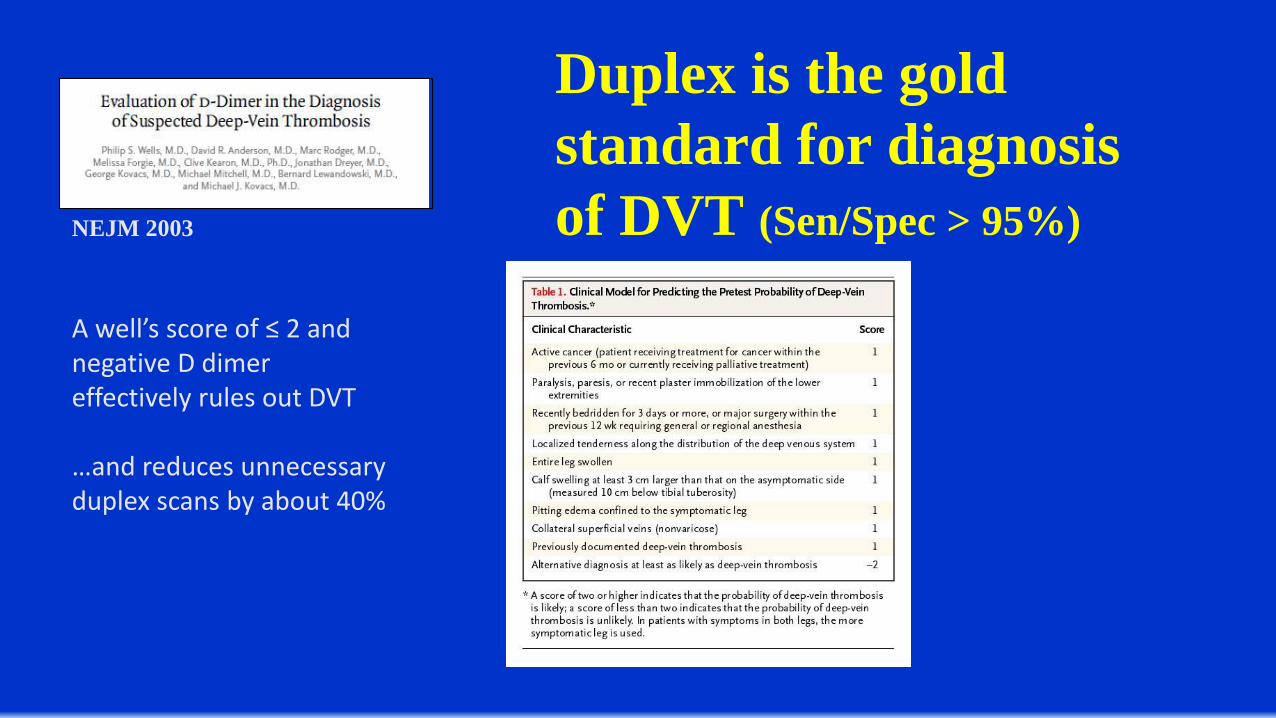
NEJM 2003
A well’s score of ≤ 2 and negative D dimer effectively rules out DVT
…and reduces unnecessary duplex scans by about 40%
Duplex is the gold standard for diagnosis of DVT (Sen/Spec > 95%)
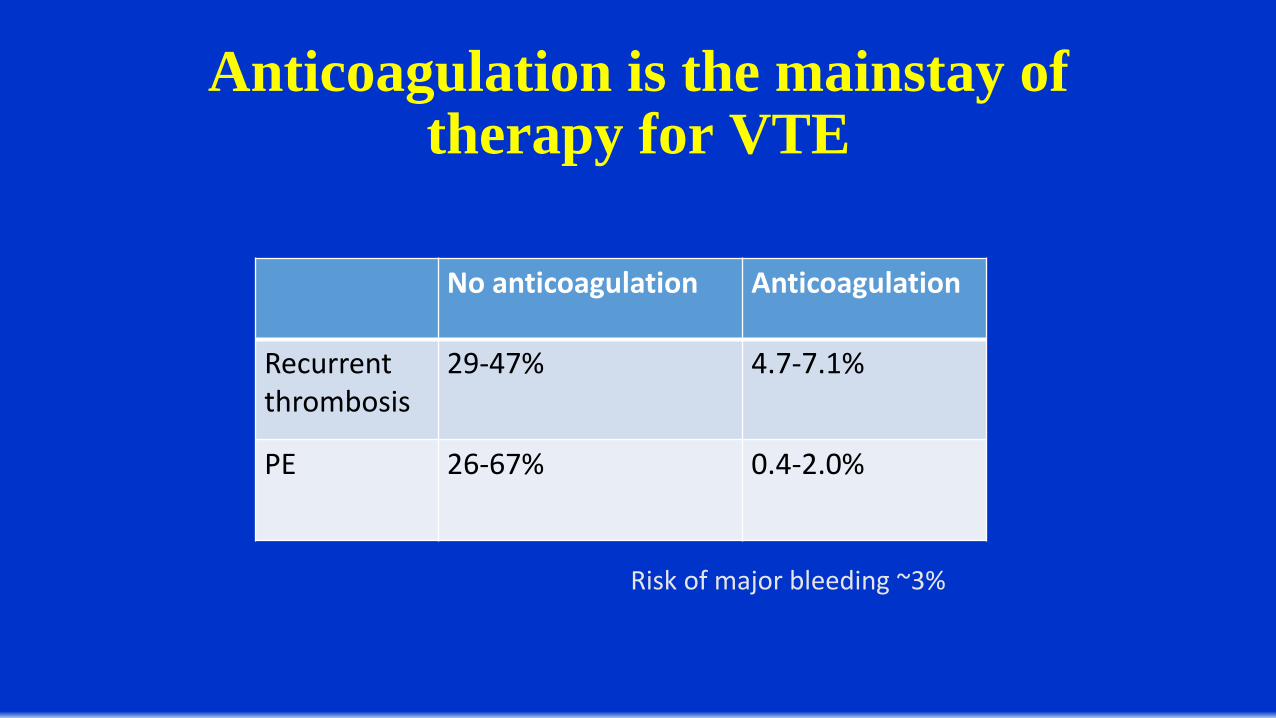
Anticoagulation is the mainstay of therapy for VTE
No anticoagulation Anticoagulation
Recurrent thrombosis
29-47% 4.7-7.1%
PE 26-67% 0.4-2.0%
Risk of major bleeding ~3%

Initial Treatment
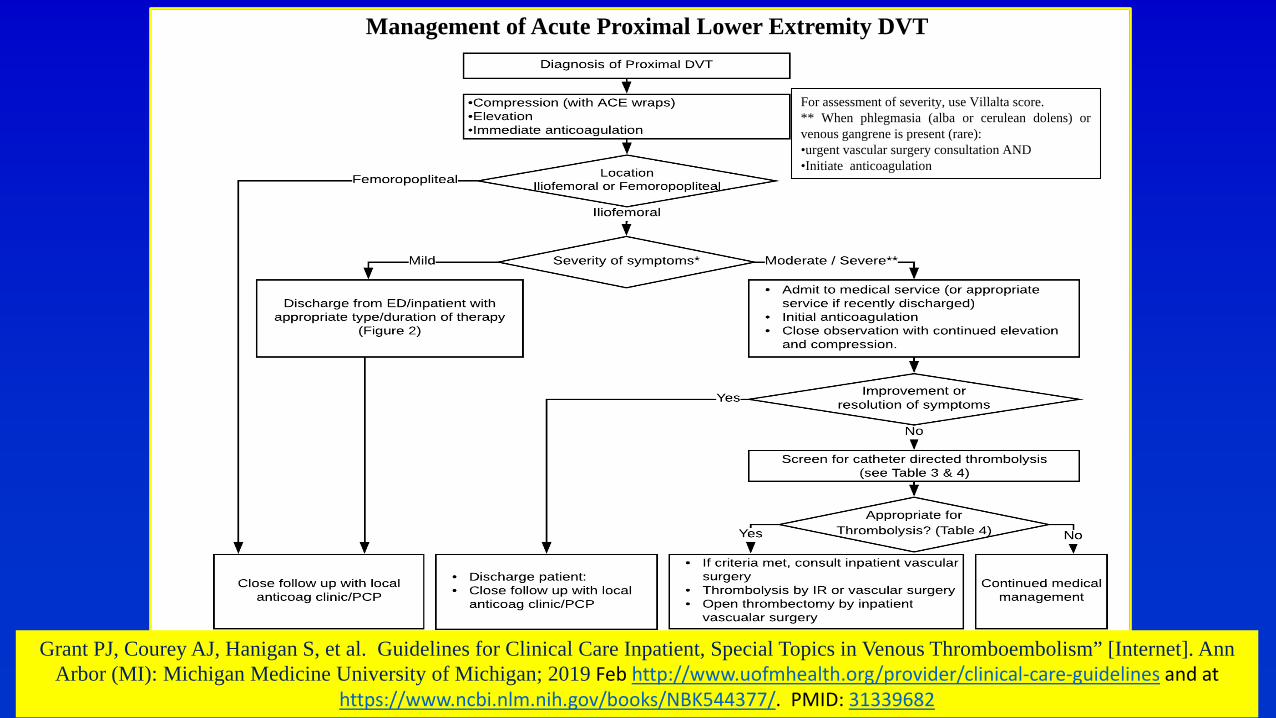
Management of Acute Proximal Lower Extremity DVT
For assessment of severity, use Villalta score.** When phlegmasia (alba or cerulean dolens) orvenous gangrene is present (rare):•urgent vascular surgery consultation AND•Initiate anticoagulation
Grant PJ, Courey AJ, Hanigan S, et al. Guidelines for Clinical Care Inpatient, Special Topics in Venous Thromboembolism” [Internet]. Ann Arbor (MI): Michigan Medicine University of Michigan; 2019 Feb http://www.uofmhealth.org/provider/clinical-care-guidelines and at
https://www.ncbi.nlm.nih.gov/books/NBK544377/. PMID: 31339682
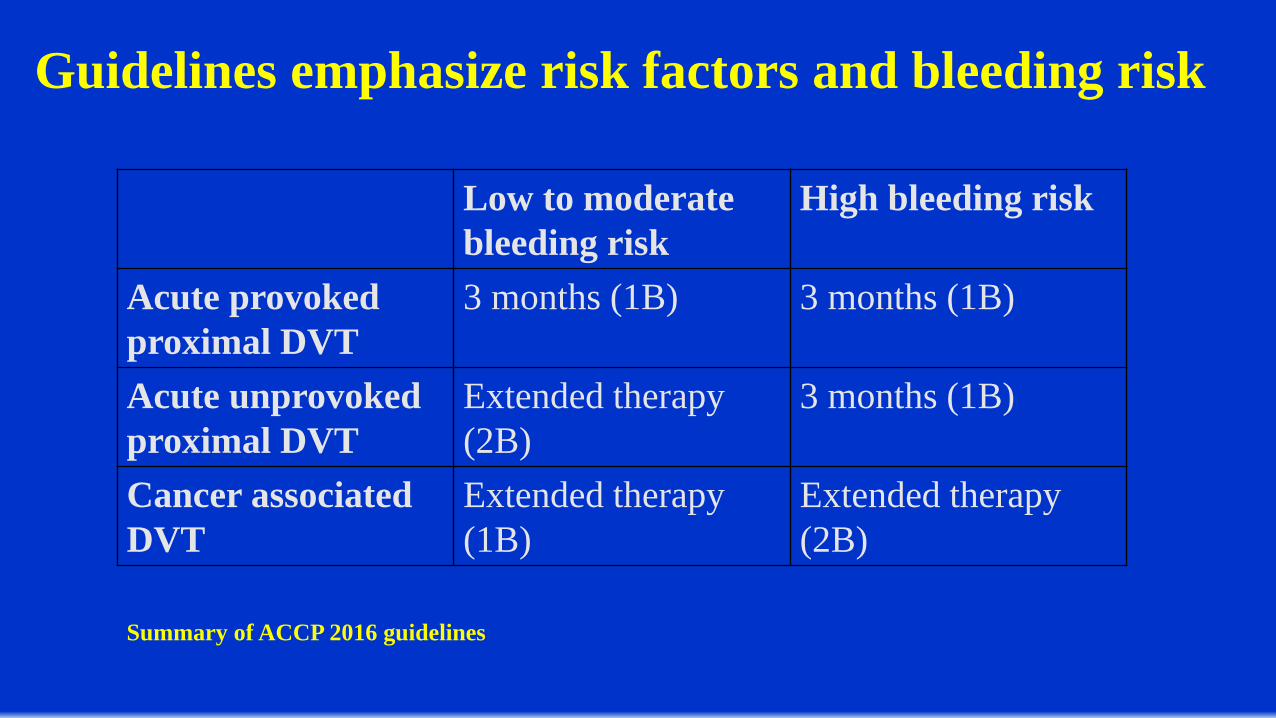
Guidelines emphasize risk factors and bleeding risk
Low to moderate bleeding risk
High bleeding risk
Acute provokedproximal DVT
3 months (1B) 3 months (1B)
Acute unprovoked proximal DVT
Extended therapy (2B)
3 months (1B)
Cancer associated DVT
Extended therapy (1B)
Extended therapy (2B)
Summary of ACCP 2016 guidelines
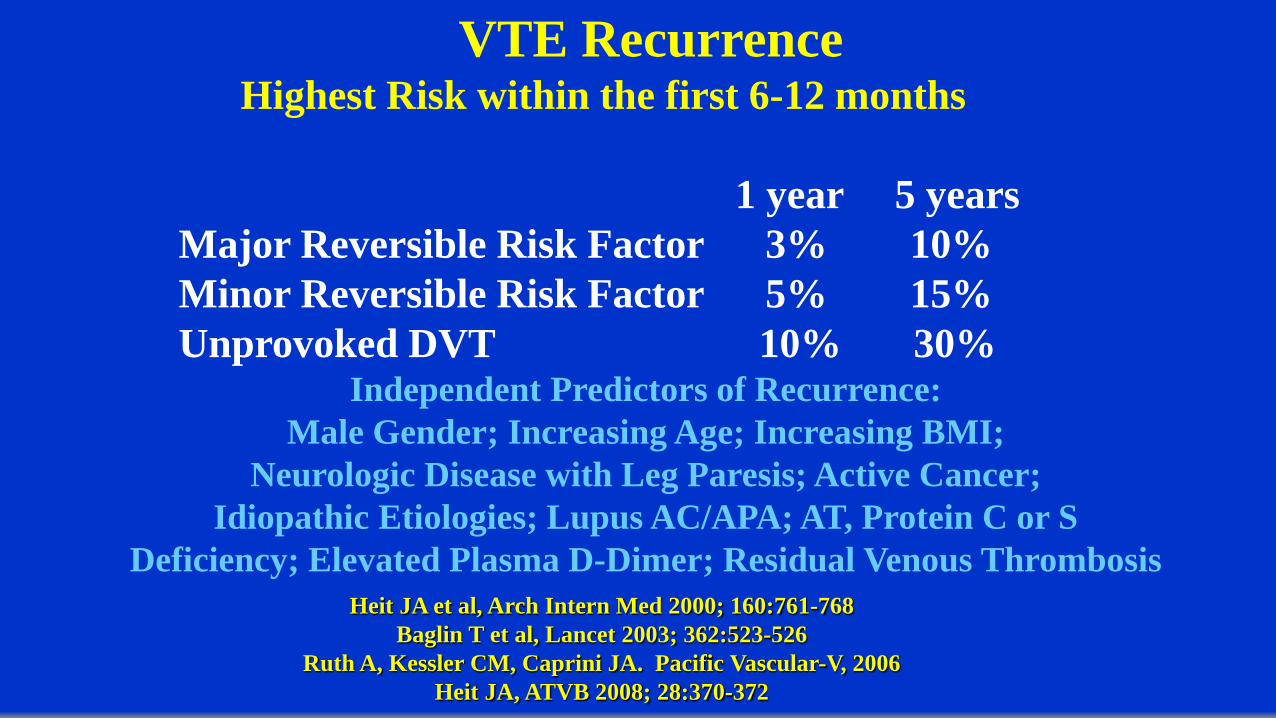
VTE RecurrenceHighest Risk within the first 6-12 months
1 year 5 yearsMajor Reversible Risk Factor 3% 10%Minor Reversible Risk Factor 5% 15%Unprovoked DVT 10% 30%
Independent Predictors of Recurrence:Male Gender; Increasing Age; Increasing BMI;
Neurologic Disease with Leg Paresis; Active Cancer; Idiopathic Etiologies; Lupus AC/APA; AT, Protein C or S
Deficiency; Elevated Plasma D-Dimer; Residual Venous ThrombosisHeit JA et al, Arch Intern Med 2000; 160:761-768
Baglin T et al, Lancet 2003; 362:523-526Ruth A, Kessler CM, Caprini JA. Pacific Vascular-V, 2006
Heit JA, ATVB 2008; 28:370-372
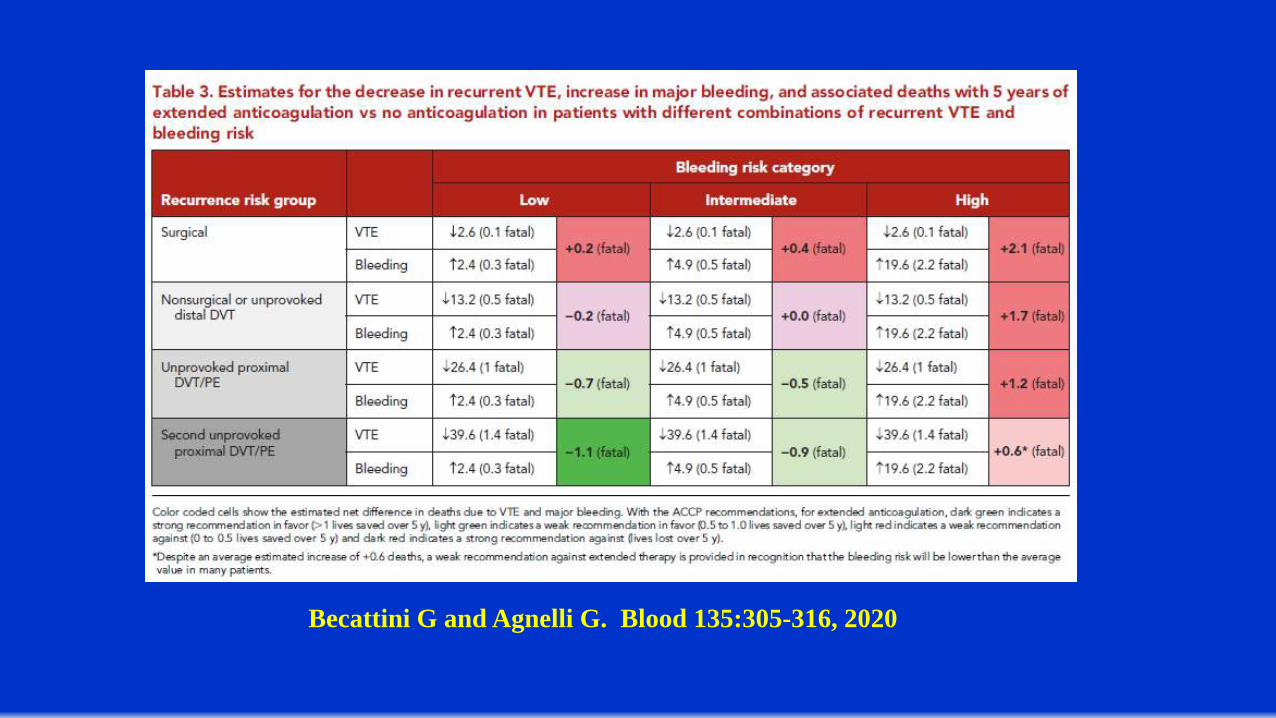
Becattini G and Agnelli G. Blood 135:305-316, 2020
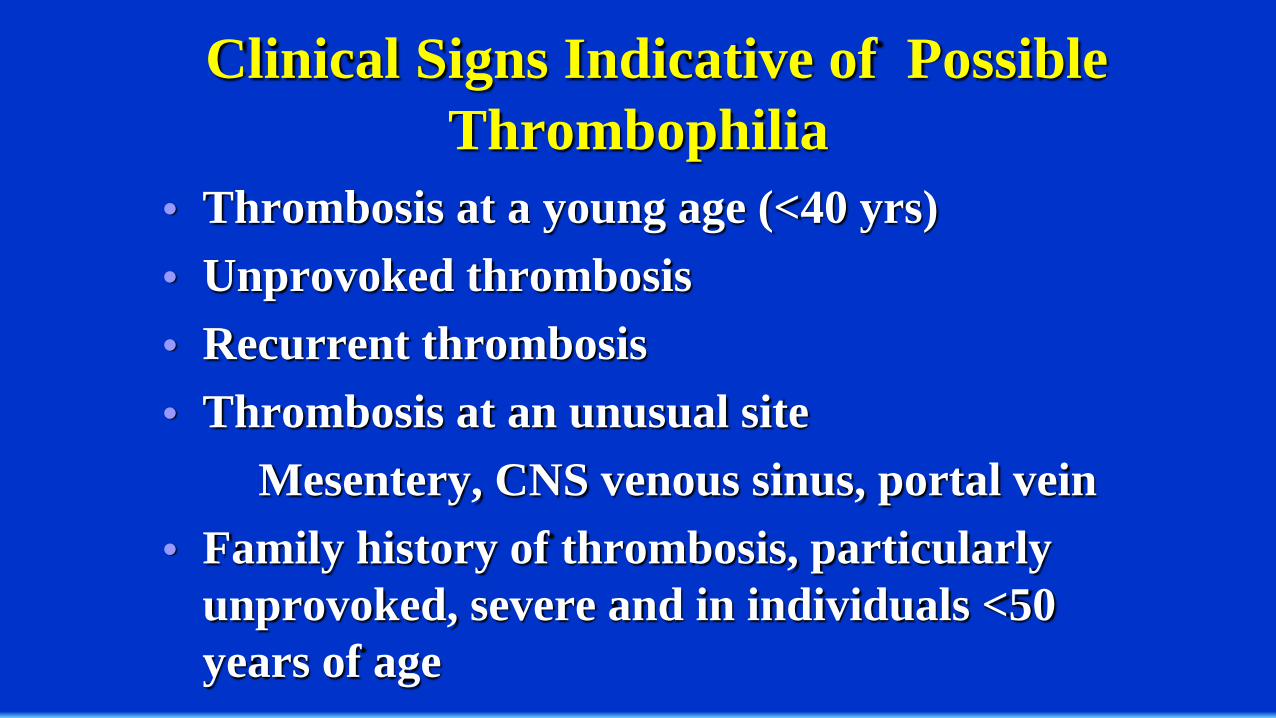
Clinical Signs Indicative of Possible Thrombophilia
• Thrombosis at a young age (<40 yrs)• Unprovoked thrombosis• Recurrent thrombosis• Thrombosis at an unusual site
Mesentery, CNS venous sinus, portal vein• Family history of thrombosis, particularly
unprovoked, severe and in individuals <50 years of age
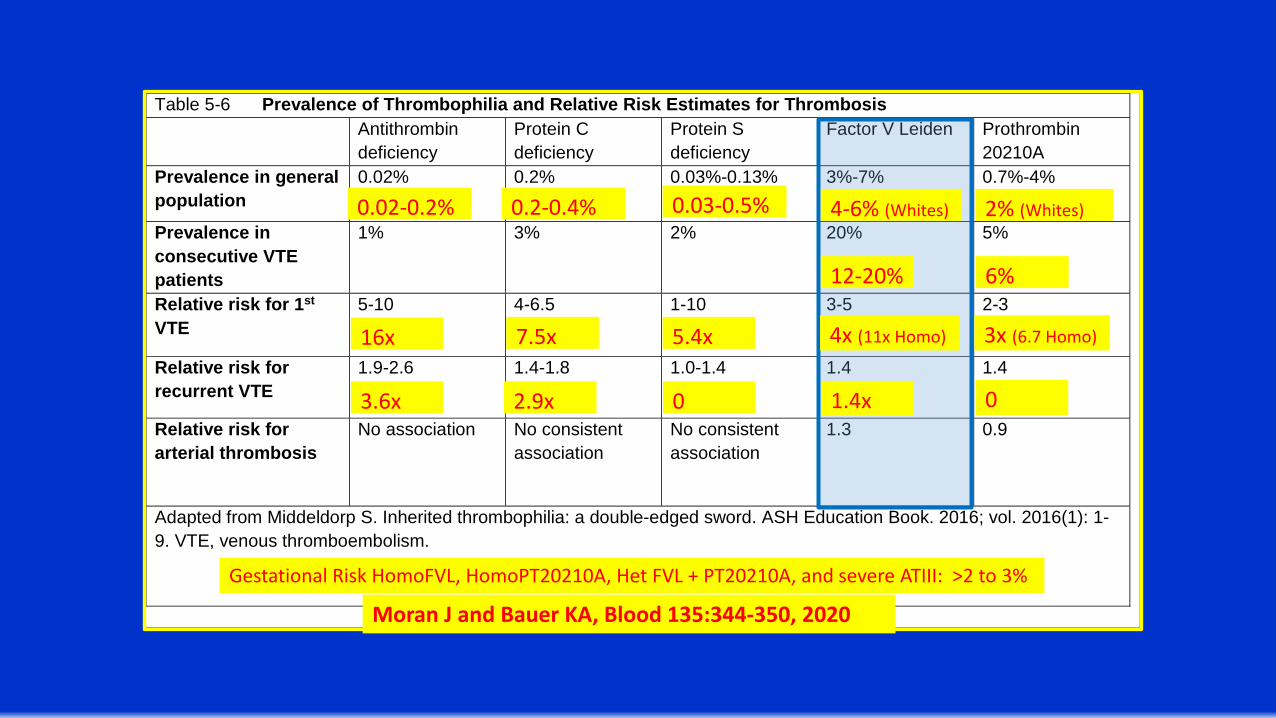
Table 5-6 Prevalence of Thrombophilia and Relative Risk Estimates for Thrombosis Antithrombin
deficiency Protein C deficiency
Protein S deficiency
Factor V Leiden Prothrombin 20210A
Prevalence in general population
0.02% 0.2% 0.03%-0.13% 3%-7% 0.7%-4%
Prevalence in consecutive VTE patients
1% 3% 2% 20% 5%
Relative risk for 1st VTE
5-10 4-6.5 1-10 3-5 2-3
Relative risk for recurrent VTE
1.9-2.6 1.4-1.8 1.0-1.4 1.4 1.4
Relative risk for arterial thrombosis
No association No consistent association
No consistent association
1.3 0.9
Adapted from Middeldorp S. Inherited thrombophilia: a double-edged sword. ASH Education Book. 2016; vol. 2016(1): 1-9. VTE, venous thromboembolism.
16x
0.02-0.2%
7.5x 5.4x
Moran J and Bauer KA, Blood 135:344-350, 2020
4x (11x Homo) 3x (6.7 Homo)
1.4x 0
Gestational Risk HomoFVL, HomoPT20210A, Het FVL + PT20210A, and severe ATIII: >2 to 3%
3.6x 2.9x 0
0.2-0.4% 0.03-0.5% 4-6% (Whites) 2% (Whites)
12-20% 6%
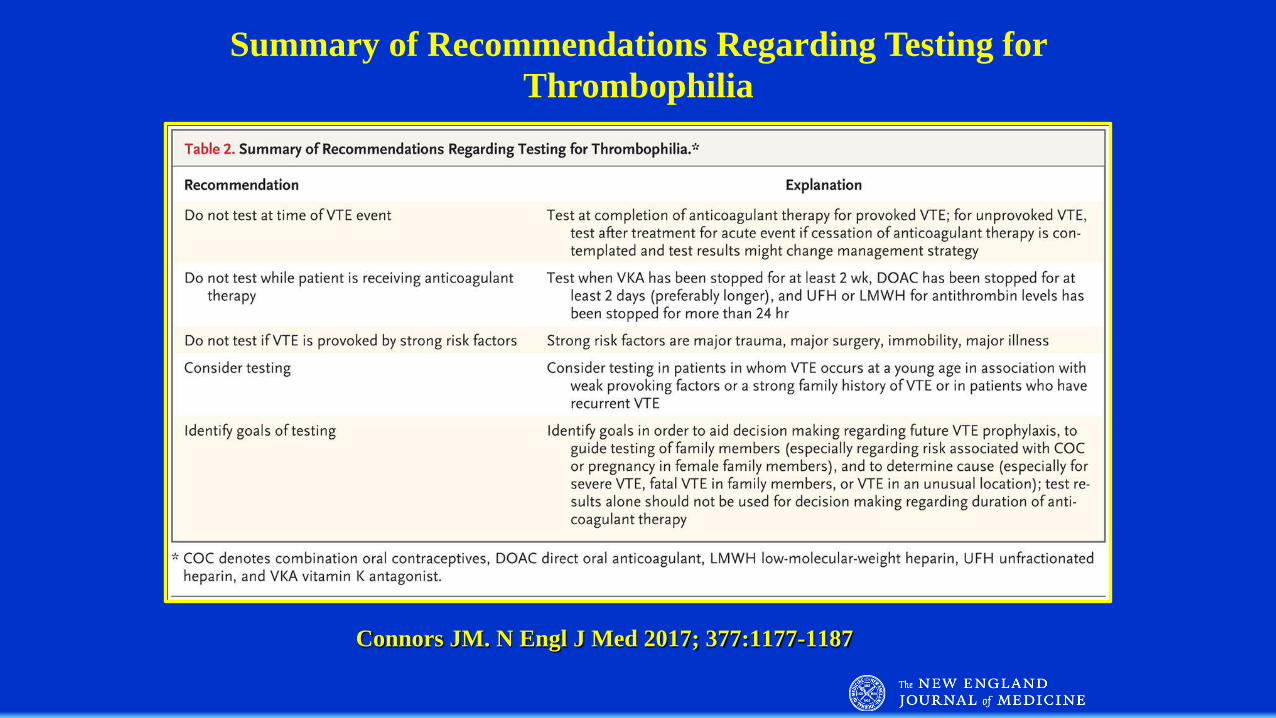
Connors JM. N Engl J Med 2017; 377:1177-1187
Summary of Recommendations Regarding Testing for Thrombophilia
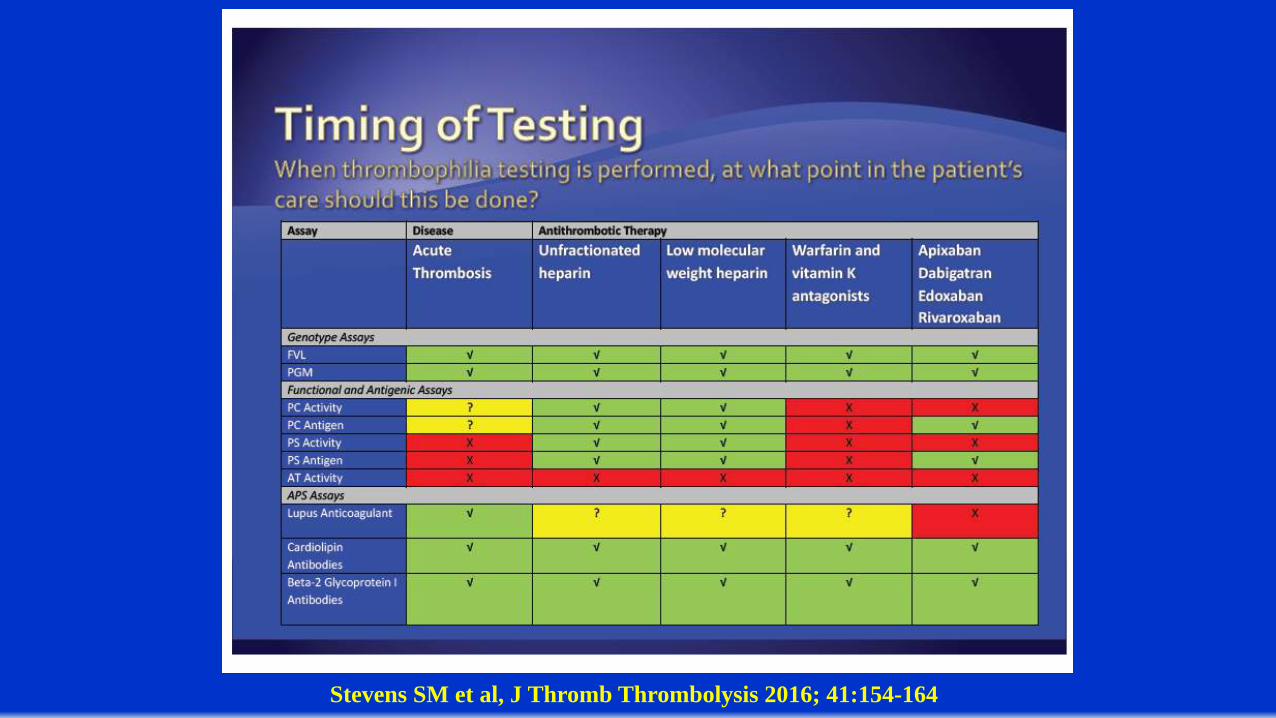
Stevens SM et al, J Thromb Thrombolysis 2016; 41:154-164
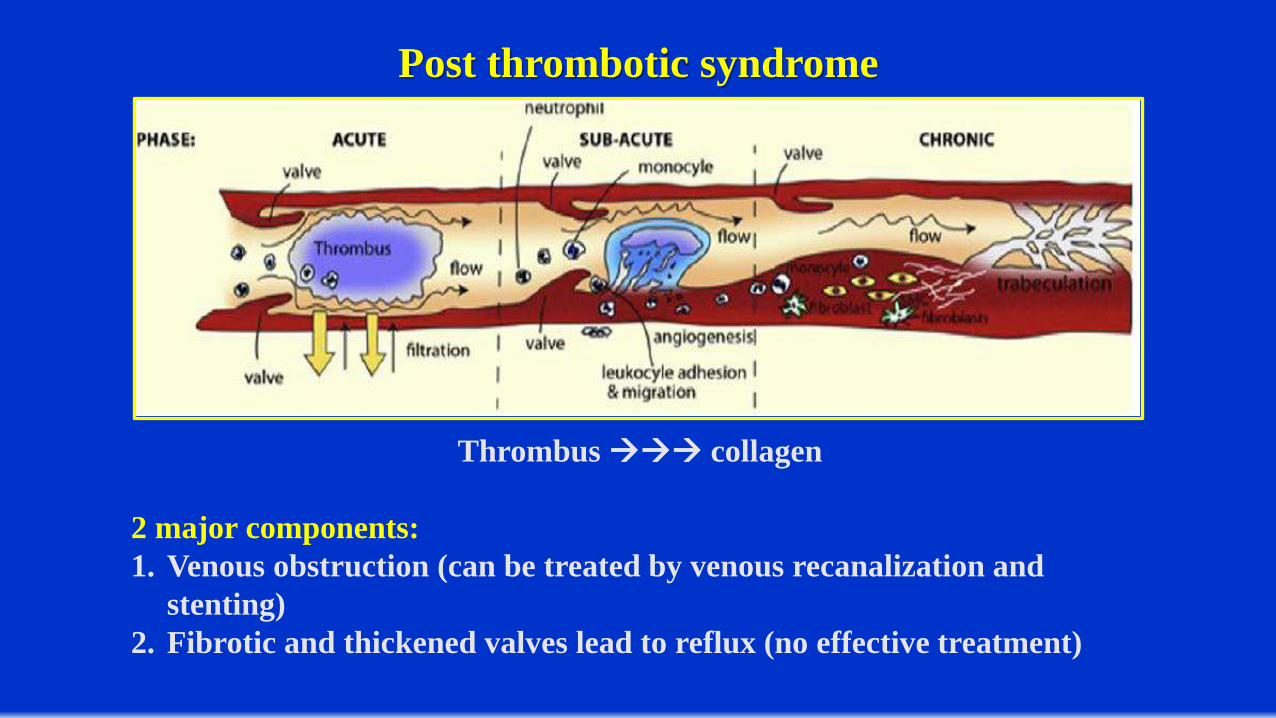
Post thrombotic syndrome
Thrombus collagen
2 major components:1. Venous obstruction (can be treated by venous recanalization and
stenting)2. Fibrotic and thickened valves lead to reflux (no effective treatment)
Ambulation/Stockings
Rate and Severity of Postthrombotic Syndrome after Proximal DVT can be cut by 50% by the use of
Compression StockingsBrandjes DP et al, Lancet 1997; 349:759-762
Prandoni P et al, Ann Int Med 2004; 141:249-256
Walking with Good Compression does not Increase the Risk of PE, while significantly Decreasing the Incidence and
Severity of the Postthrombotic SyndromeSchellong SM et al, Thromb Haemost 1999; 82(Suppl 1):127-129
Aschwanden M et al, Thromb Haemost 2001; 85:42-46Partsch H et al, Sem Vasc Surg 2005; 18:148-152
Kahn SR et al, Lancet 2014; 383:880-888
In patients with acute DVT of the leg, we suggest not using compression stockings routinely to prevent PTS (Grade 2B).
Remarks: This recommendation focuses on prevention of the chronic complication of PTS and not on the treatment of symptoms. For patients with acute or chronic symptoms,a trial of graduated compression stockings is often justified.
ACCP guidelines 2016Compression Stockings
Immediate Application of Stockings
592 adult patients from 10 academic and nonacademic centersProximal DVT
No Compression or Acute Compression within 24 hours of Diagnosis with either multilayer bandaging (62%) or stockings (26%)
Presence of RVO and Recurrent VTEPTS defined as Villalta at least 5 at 24 months
RVO Compression vs. No Compression (46.3% vs. 66.7%, p = .005)PTS Less Prevalent in those without RVO (46% vs. 54%, p = .013)
Recurrent VTE – No Association
Amin EE, Bistervels IM, Meijer K, et al. Blood 132:2298-2304, 2018
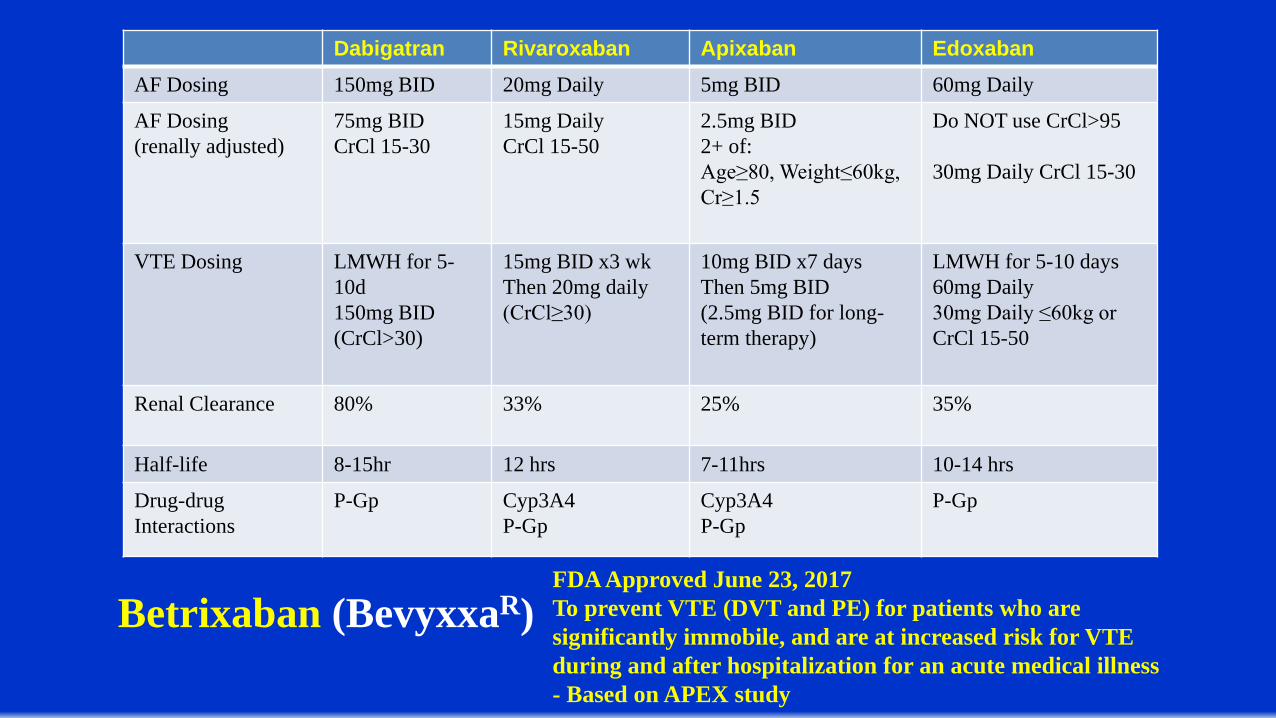
Dabigatran Rivaroxaban Apixaban EdoxabanAF Dosing 150mg BID 20mg Daily 5mg BID 60mg Daily
AF Dosing (renally adjusted)
75mg BIDCrCl 15-30
15mg DailyCrCl 15-50
2.5mg BID2+ of: Age≥80, Weight≤60kg,Cr≥1.5
Do NOT use CrCl>95
30mg Daily CrCl 15-30
VTE Dosing LMWH for 5-10d150mg BID (CrCl>30)
15mg BID x3 wkThen 20mg daily (CrCl≥30)
10mg BID x7 daysThen 5mg BID(2.5mg BID for long-term therapy)
LMWH for 5-10 days60mg Daily30mg Daily ≤60kg or CrCl 15-50
Renal Clearance 80% 33% 25% 35%
Half-life 8-15hr 12 hrs 7-11hrs 10-14 hrs
Drug-drugInteractions
P-Gp Cyp3A4P-Gp
Cyp3A4P-Gp
P-Gp
Betrixaban (BevyxxaR)FDA Approved June 23, 2017To prevent VTE (DVT and PE) for patients who are significantly immobile, and are at increased risk for VTE during and after hospitalization for an acute medical illness - Based on APEX study
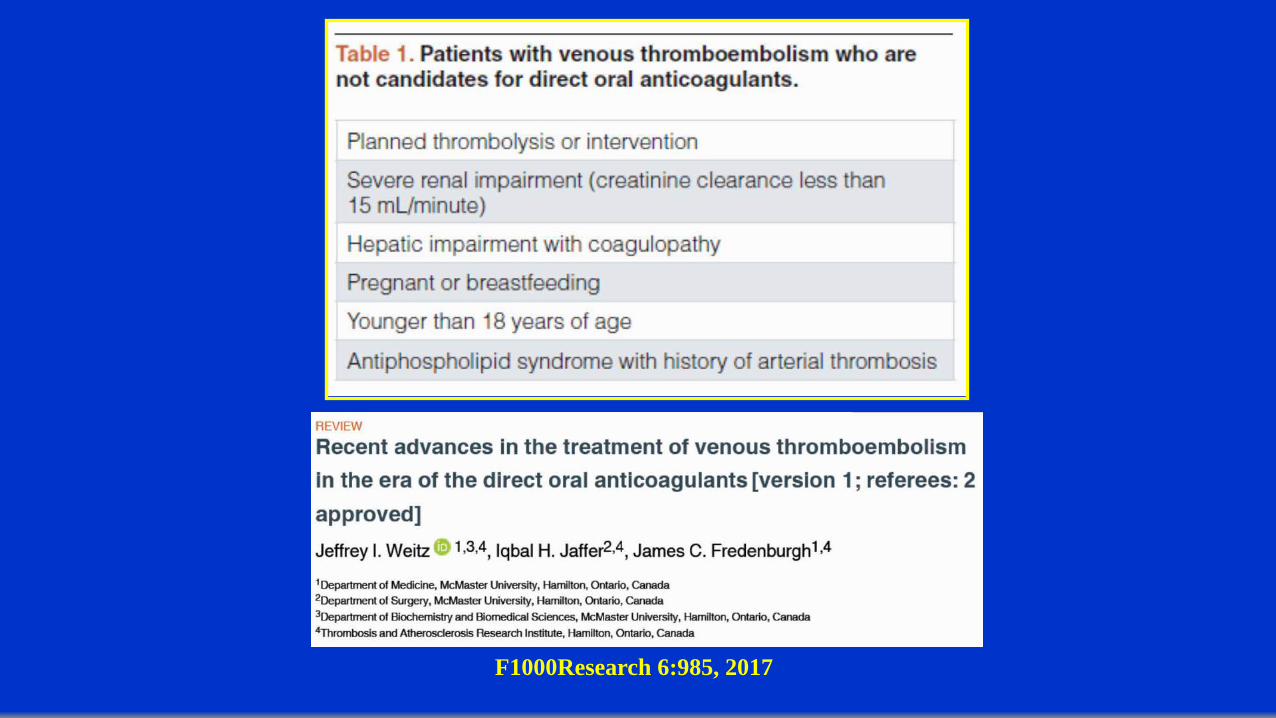
F1000Research 6:985, 2017
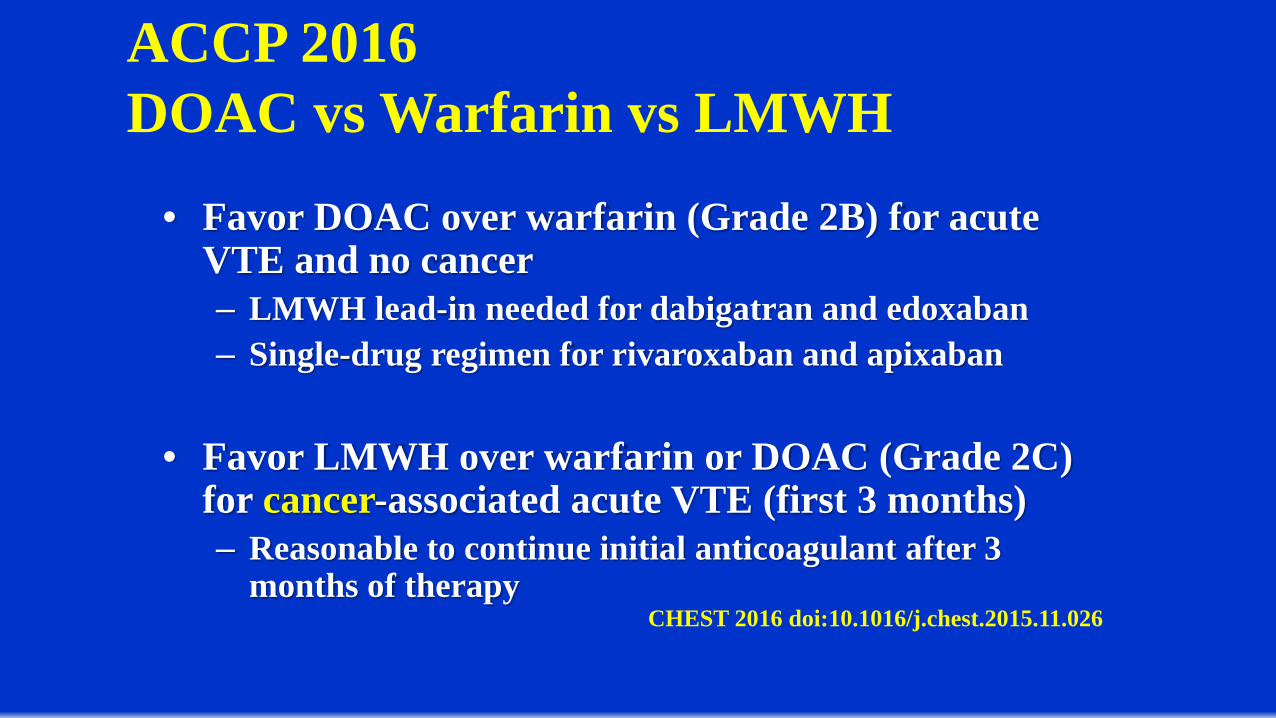
ACCP 2016 DOAC vs Warfarin vs LMWH
• Favor DOAC over warfarin (Grade 2B) for acute VTE and no cancer– LMWH lead-in needed for dabigatran and edoxaban– Single-drug regimen for rivaroxaban and apixaban
• Favor LMWH over warfarin or DOAC (Grade 2C) for cancer-associated acute VTE (first 3 months)– Reasonable to continue initial anticoagulant after 3
months of therapyCHEST 2016 doi:10.1016/j.chest.2015.11.026
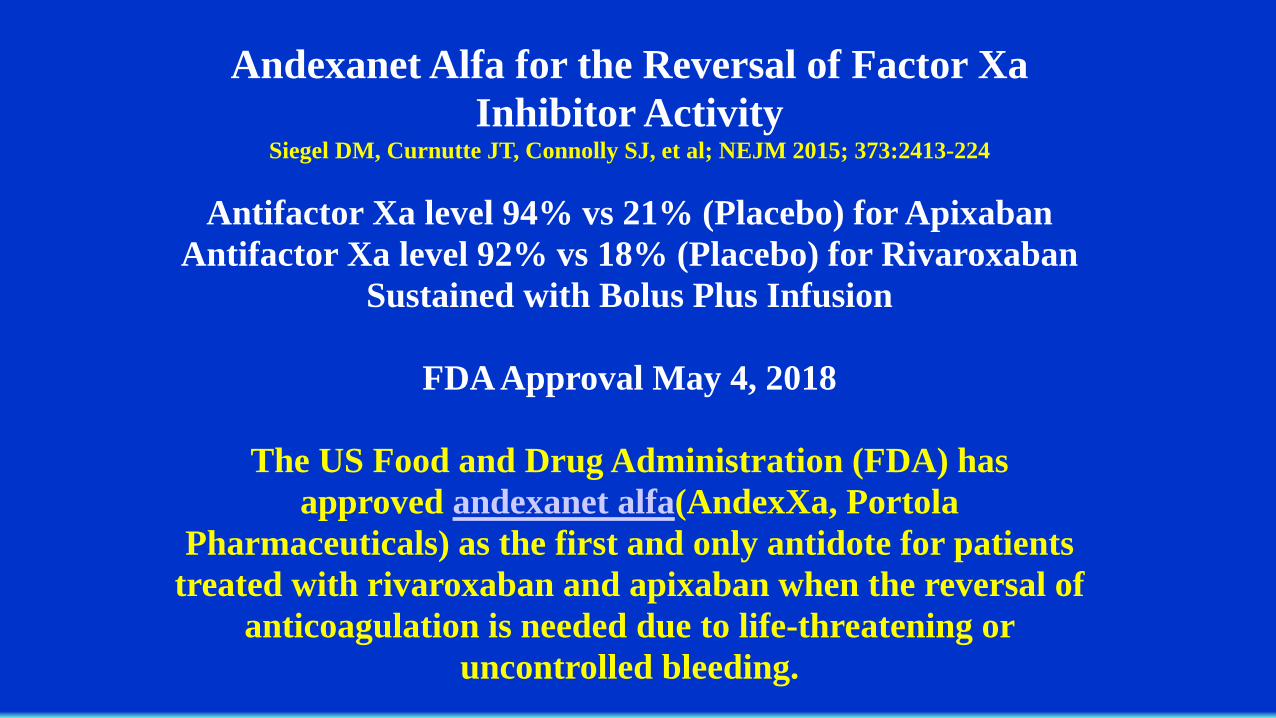
Andexanet Alfa for the Reversal of Factor XaInhibitor Activity
Siegel DM, Curnutte JT, Connolly SJ, et al; NEJM 2015; 373:2413-224
Antifactor Xa level 94% vs 21% (Placebo) for ApixabanAntifactor Xa level 92% vs 18% (Placebo) for Rivaroxaban
Sustained with Bolus Plus Infusion
FDA Approval May 4, 2018
The US Food and Drug Administration (FDA) has approved andexanet alfa(AndexXa, Portola
Pharmaceuticals) as the first and only antidote for patients treated with rivaroxaban and apixaban when the reversal of
anticoagulation is needed due to life-threatening or uncontrolled bleeding.
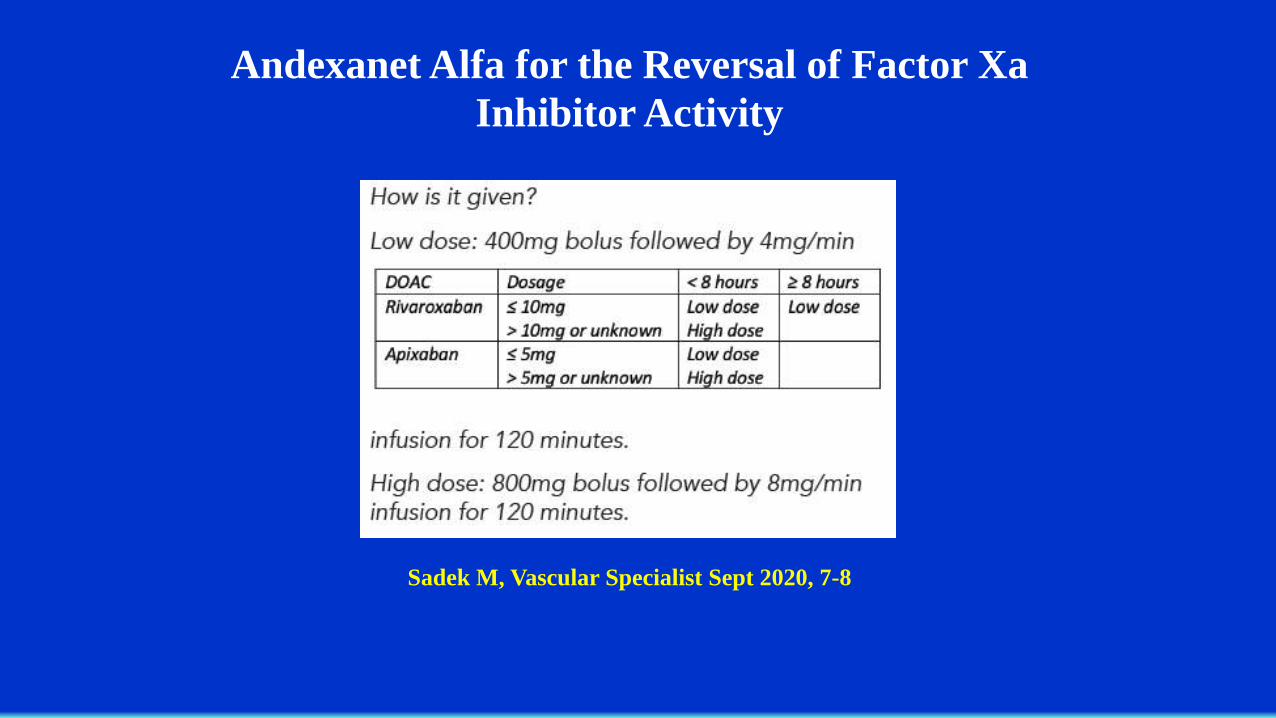
Andexanet Alfa for the Reversal of Factor XaInhibitor Activity
Sadek M, Vascular Specialist Sept 2020, 7-8
Multinational, randomized, investigator-initiated, open-label, noninferiority trial with blinded central outcome adjudication.
Patients with cancer with symptomatic or incidental acute proximal DVT or PE received oral apixaban (10 mg bid for the first 7 days, followed by 5 mg bid) or subcutaneous dalteparin(200 IU/kg qd for the first month, followed by 150 IU/kg qd). The treatments were administered for 6 months.
Recurrent VTE occurred in 32 of 576 patients (5.6%) in the apixaban group and in 46 of 579 patients (7.9%) in the dalteparin group (hazard ratio, 0.63; 95% confidence interval [CI], 0.37 to 1.07; P<0.001 for noninferiority). Major bleeding occurred in 22 patients (3.8%) in the apixabangroup and in 23 patients (4.0%) in the dalteparin group (hazard ratio, 0.82; 95% CI, 0.40 to 1.69; P=0.60).
Oral apixaban was noninferior to subcutaneous dalteparinfor the treatment of cancer-associated venous thromboembolism without an increased risk of major bleeding.
When to Monitor DOACs• Bleeding• Before surgery/procedure with recent DOAC use
(<24hrs, or 48-72hrs if CrCl<30)• Concurrent use of P-gP or CYP3A4-interacting meds• Extremes of body weight• Declining renal function• Potential need for DOAC reversal• Suspected overdose• Assessing compliance (limited by short t1/2)
Baglin T. J Thromb Haemost2013; 11(Suppl 1):122--128
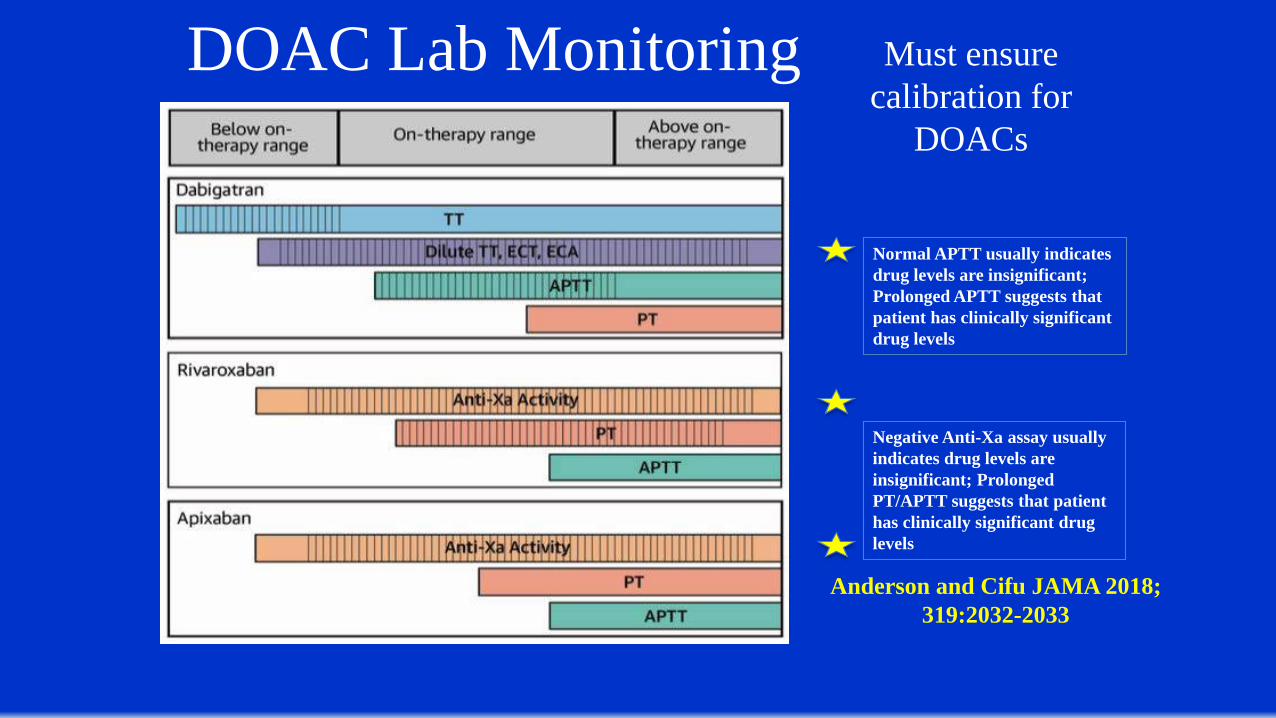
DOAC Lab Monitoring
Anderson and Cifu JAMA 2018; 319:2032-2033
Must ensure calibration for
DOACs
Normal APTT usually indicates drug levels are insignificant; Prolonged APTT suggests that patient has clinically significant drug levels
Negative Anti-Xa assay usually indicates drug levels are insignificant; Prolonged PT/APTT suggests that patient has clinically significant drug levels
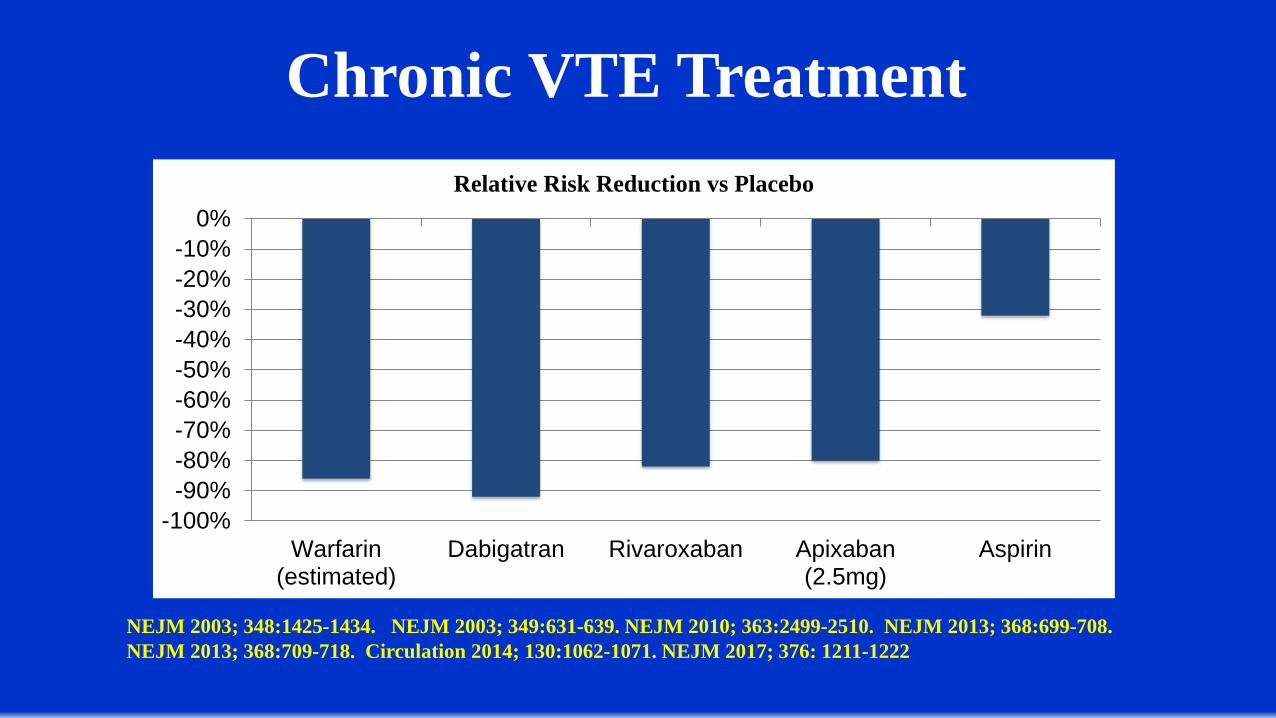
Chronic VTE Treatment
-100%-90%-80%-70%-60%-50%-40%-30%-20%-10%
0%
Warfarin(estimated)
Dabigatran Rivaroxaban Apixaban(2.5mg)
Aspirin
Relative Risk Reduction vs Placebo
NEJM 2003; 348:1425-1434. NEJM 2003; 349:631-639. NEJM 2010; 363:2499-2510. NEJM 2013; 368:699-708. NEJM 2013; 368:709-718. Circulation 2014; 130:1062-1071. NEJM 2017; 376: 1211-1222
ACCP guidelines 2016 Tibial DVT: Treatment
In patients with acute isolated distal DVT of the leg: (i) without severe symptoms or risk factors for extension, we suggest
serial imaging of the deep veins for 2 weeks over anticoagulation (Grade 2C)
(ii) with severe symptoms or risk factors for extension, wesuggest anticoagulation over serial imaging of the deep veins(Grade 2C)
In patients with acute isolated distal DVT of the leg who are managed with anticoagulation, we recommend using the same anticoagulation as for patients with acute proximal DVT (Grade 1B)
Calf Vein DVTThe Compression Alone Versus Anticoagulation for Symptomatic Calf Vein Thrombosis Diagnosed by Ultrasonography (CACTUS) trial was performed to assess the safety of withholding anticoagulantion in patients with isolated symptomatic calf vein DVT at low risk for proximal extension/VTE - no personal VTE history or active malignancy.
LMWH did not reduce proximal extension or VTE and resulted in increased bleeding complications. It was underpowered for its endpoints, as only 259 patients enrolled and the calculated power required was 572 patients.
Righini M. J Thromb Haemost. 2007;5 Suppl 1:55-9.Righini M, Galanaud JP, Guenneguez H, et al. Lancet Haematol. 2016;3:e556-e562.
Parisi R, Visona A, Camporese G, et al. Int Angiol. 2009;28:68-72.
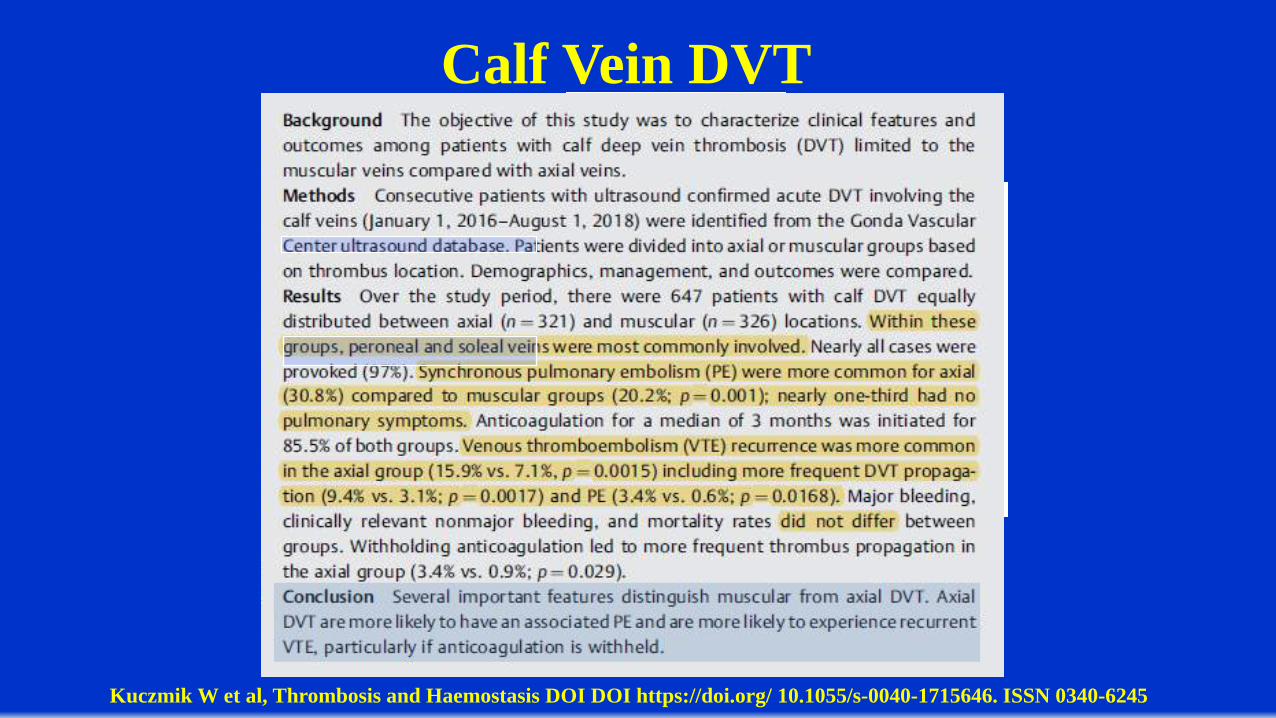
Calf Vein DVT
Kuczmik W et al, Thrombosis and Haemostasis DOI DOI https://doi.org/ 10.1055/s-0040-1715646. ISSN 0340-6245
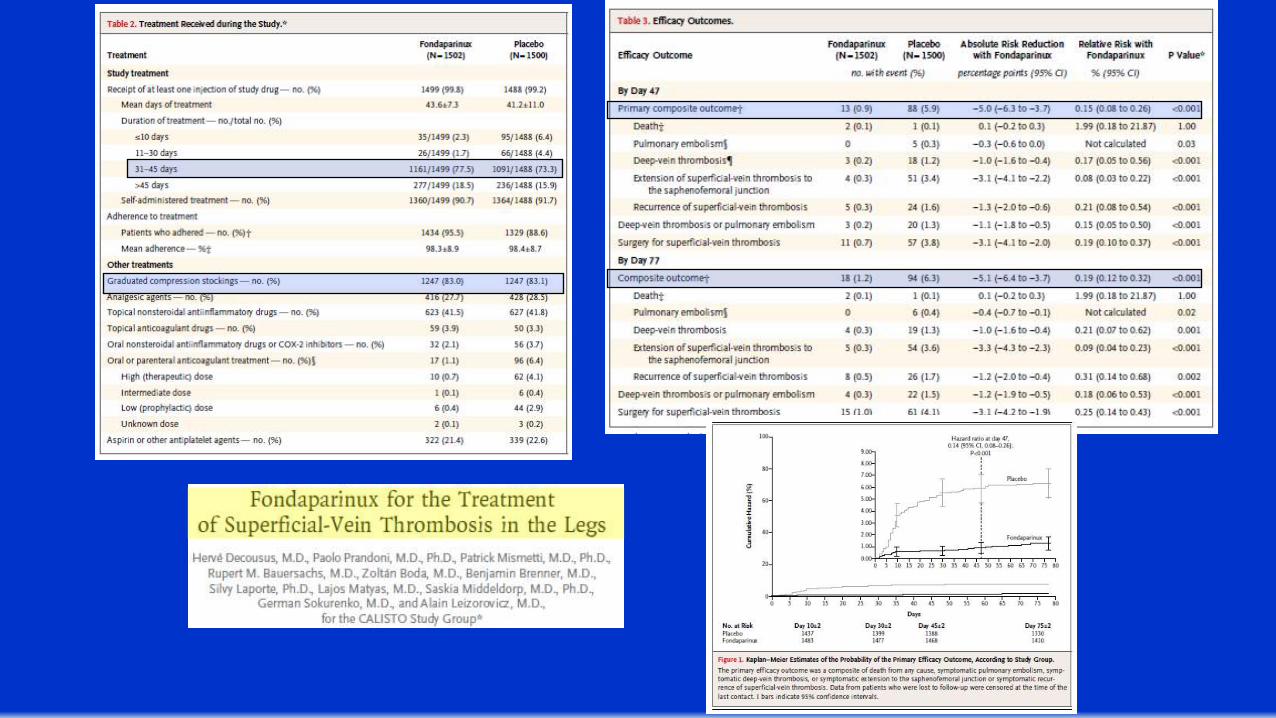
• In those with SVT > 5 cm, use prophylactic dose fondaparinux or LMWH for 45d (2B)
• In those with SVT treated with anticoagulation, suggest fondaparinux (2.5mg) over prophylactic LMWH (2C)
Superficial thrombophlebitis: treatment
Superfical ThrombophlebitisSURPRISE trial, a randomized, open-label trial enrolling 472 patients. A departure from CALISTO which had excluded patients with history of malignancy treated within the last 6 months, the SURPRISE trial was designed to include patients at highest risk for VTE, including those with cancer.
In SURPRISE, patients were included only if they had superficial thrombophlebitis and one of the following risk factors associated with a higher rate of thromboembolic complications: age >65 years, male sex, previous cancer, history of VTE and absence of varicose veins.
When comparing 6-weeks of prophylactic fondaparinux to daily rivaroxaban (10mg qday), rivaroxaban was non-inferior to fondaparinux in the prevention of DVT, PE, and progression or recurrence of SVT.
Rivaroxaban therapy was postulated to be a less expensive and a more patient-friendly.
Decousus H, Prandoni P, Mismetti P, et al. . N Engl J Med. 2010;363:1222-32; Beyer-Westendorf J, Schellong SM, Gerlach H, et al. . Lancet Haematol. 2017;4:e105-e113
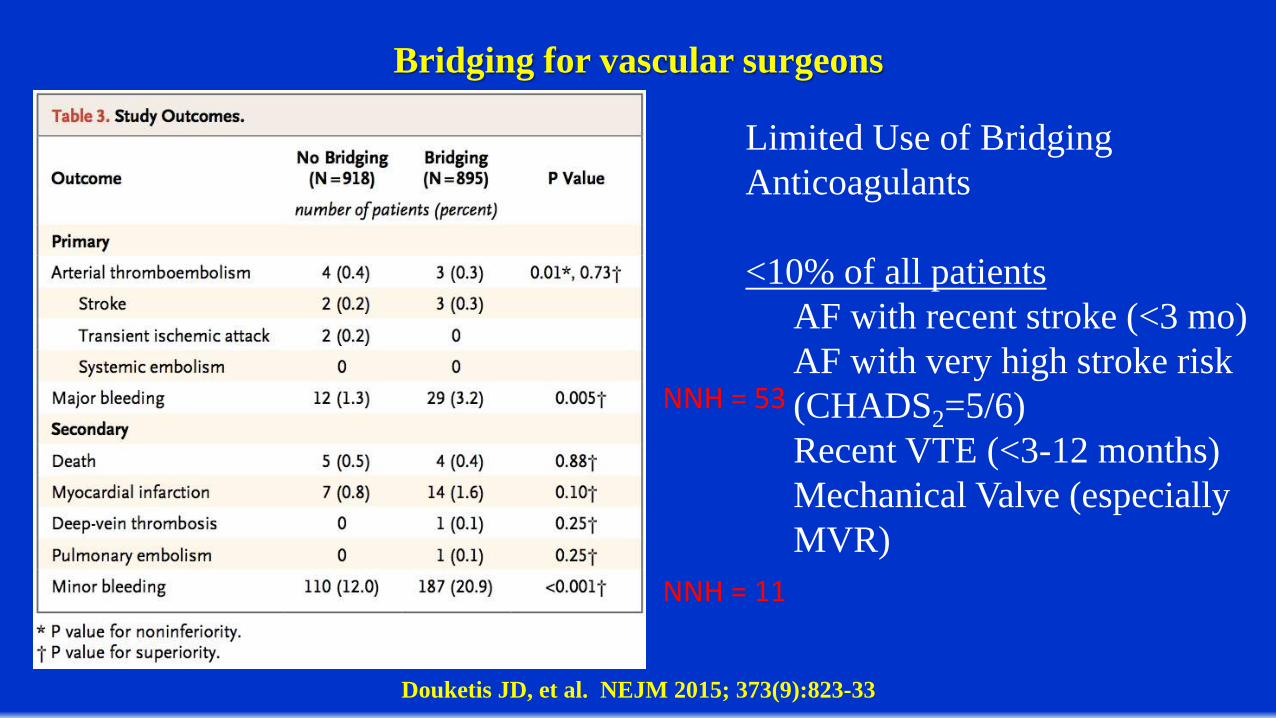
Bridging for vascular surgeons
Douketis JD, et al. NEJM 2015; 373(9):823-33
NNH = 53
NNH = 11
Limited Use of Bridging Anticoagulants
<10% of all patientsAF with recent stroke (<3 mo)AF with very high stroke risk (CHADS2=5/6)Recent VTE (<3-12 months)Mechanical Valve (especially MVR)
Venous Thromboembolism in the Context of Chronic Venous
DiseaseMichael Kemp MD, Andrea Obi MD,
Peter Henke MD, Thomas Wakefield MD
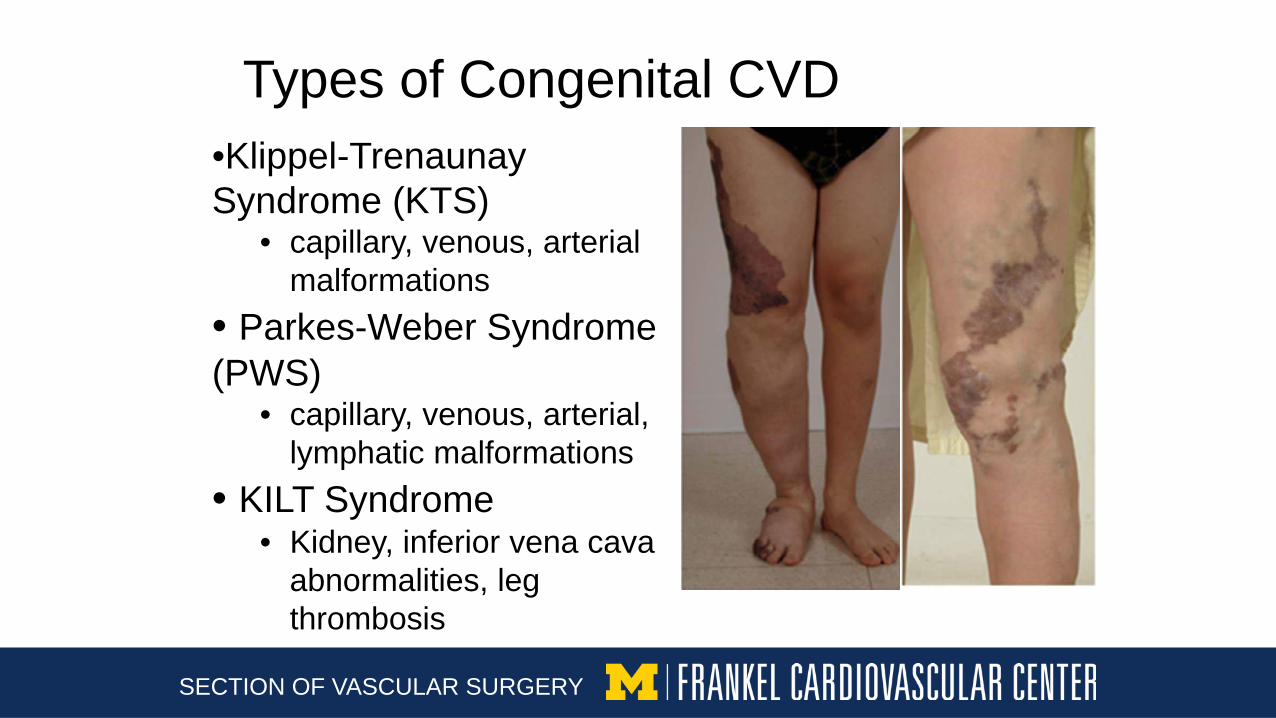
Types of Congenital CVD •Klippel-Trenaunay Syndrome (KTS)
• capillary, venous, arterial malformations
• Parkes-Weber Syndrome (PWS)
• capillary, venous, arterial, lymphatic malformations
• KILT Syndrome• Kidney, inferior vena cava
abnormalities, leg thrombosis
SECTION OF VASCULAR SURGERY
Risk of VTE Congenital CVD • Seems to be increased risk of VTE
• KTS• Few higher level studies
• 8-22% incidence of VTE• ~109 and 106-fold increased risk of DVT/PE• Risk independent of pregnancy status
• PWS• Data primarily limited to case reports involving DVTs
• KILT• Characterized by thromboses (typically deep system)
• Children • If no risk factors…evaluate for congenital
abnormalities/syndromes
SECTION OF VASCULAR SURGERY
Non-congenital CVD• Primary versus secondary often not delineated between • VTE risk in primary CVD
• Few studies• 4.7x increased VTE risk• Estimated 2/3 of DVT patients had
primary CVD• 5% occurrence in a retrospective
observational study • More studies needed
SECTION OF VASCULAR SURGERY
Varicose Veins
• Can be primary or secondary • Increased risk of primary VTE
• HR 5.3 in a retrospective cohort study• Risk decreases with age
• OR 4.2 (age 45) versus OR 0.9 (age 75)• Unclear why
• Increases risk of other high-risk groups• Cancer• Surgical patients
• But may not be predictive of VTE recurrence
SECTION OF VASCULAR SURGERY
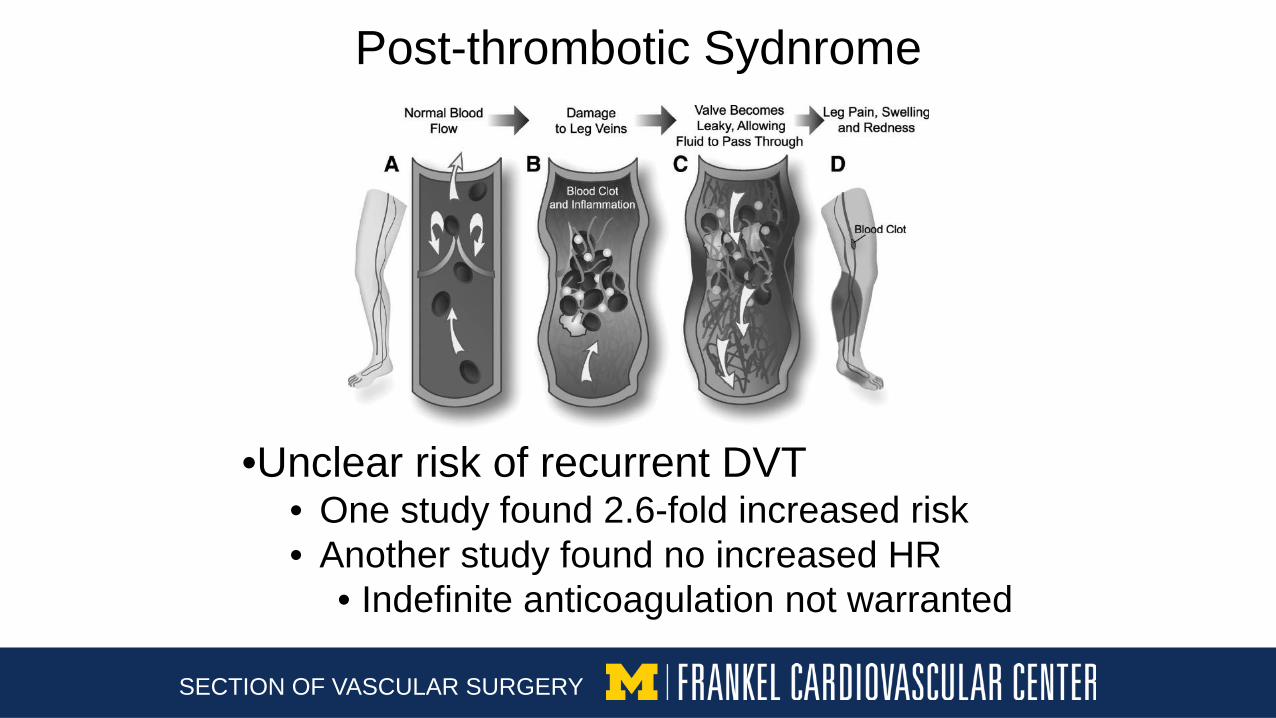
Post-thrombotic Sydnrome
SECTION OF VASCULAR SURGERY
•Unclear risk of recurrent DVT• One study found 2.6-fold increased risk • Another study found no increased HR
• Indefinite anticoagulation not warranted
Post-thrombotic Syndrome
• Residual vein thrombosis (RVT) may be helpful
• Presence at 3 months: ↑ recurrence (HR 2.03)• ↑ risk despite continued/extended
anticoagulation • 10.4% incidence in those with RVT • 1.4% incidence in those without RVT
• Limitations with standardization • Technician dependent • Patient dependent
SECTION OF VASCULAR SURGERY
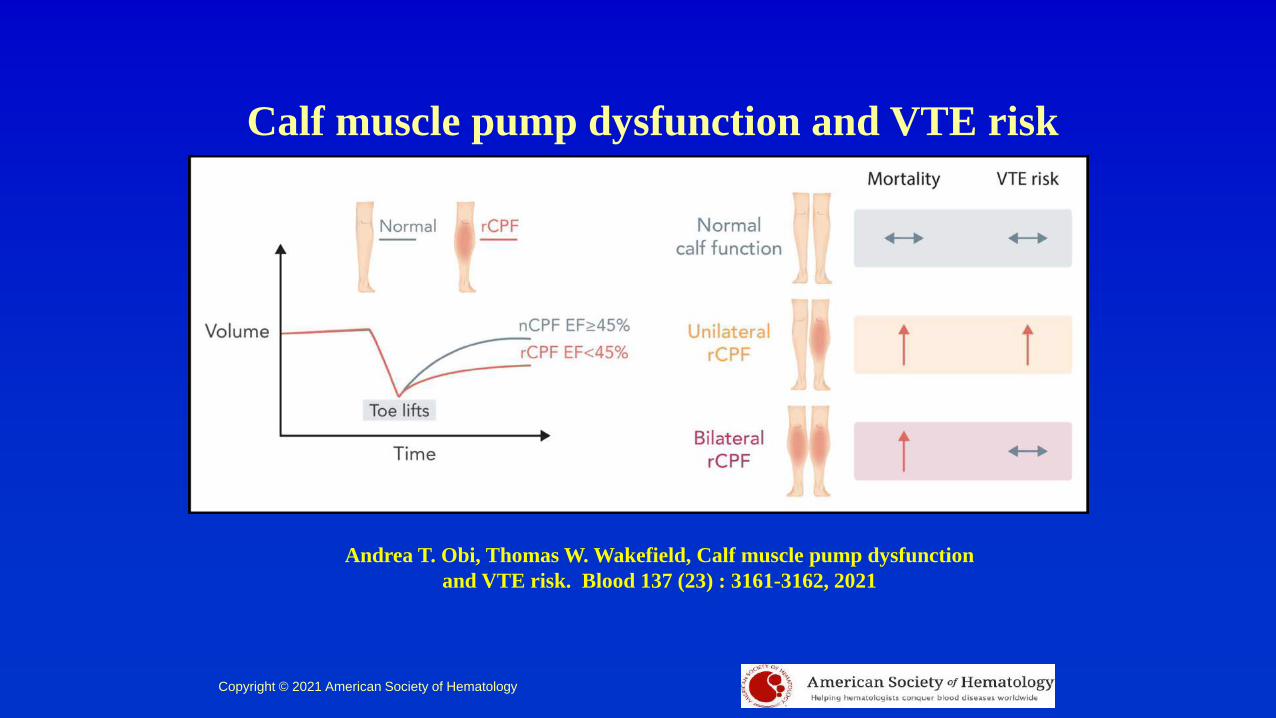
Calf muscle pump dysfunction and VTE risk
Andrea T. Obi, Thomas W. Wakefield, Calf muscle pump dysfunction and VTE risk. Blood 137 (23) : 3161-3162, 2021
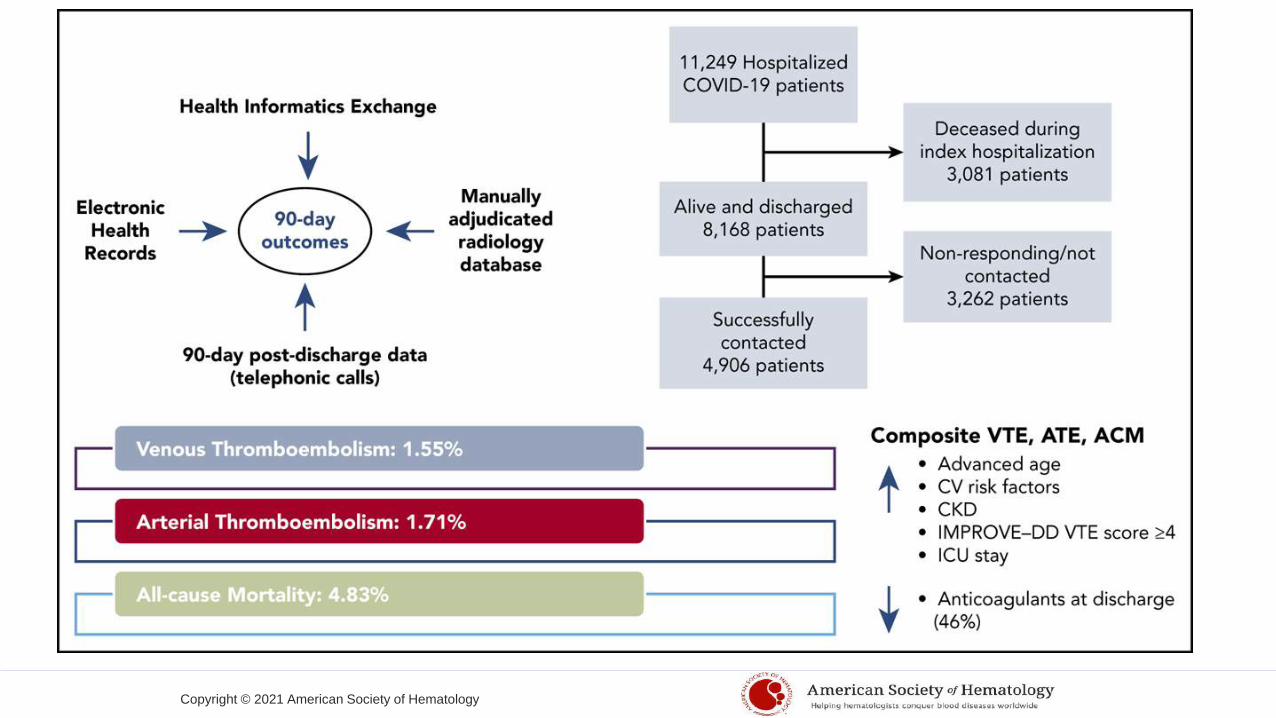
Copyright © 2021 American Society of Hematology
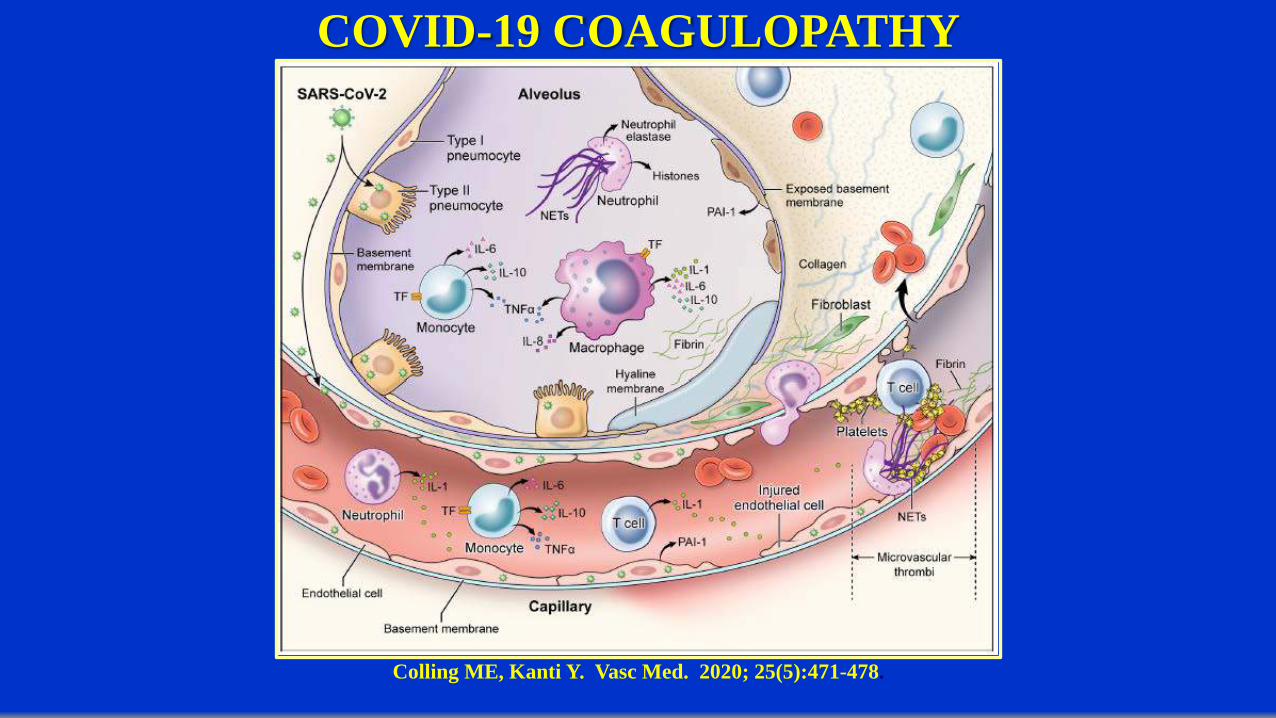
COVID-19 COAGULOPATHY
Colling ME, Kanti Y. Vasc Med. 2020; 25(5):471-478.
COVID-19 COAGULOPATHY (ICU/Non ICU and D-dimer)• Recent registry study has demonstrated that in 1114 patients with an ICU
subset (n170), symptomatic VTE was seen in 27% (despite VTE prophylaxis)
Piazza G, Campia U, Hurwitz S, et al, J Am Coll Cardiol 76(18): 2060-2072, 2020.• Systematic review and meta-analysis of 66 studies (28,173 patients)
demonstrated VTE prevalence of 40.3% (ultrasound screening) and 9.5% (without ultrasound screening).
• VTE prevalence (overall) of 7.9% (non-ICU) and 22.7% (ICU patients)• VTE prevalence (screening) 23% (non-ICU) and 45.6% (ICU patients)
Nopp S, Moik F, Jilma B, Pabinger I, Ay C. Res Pract Thromb Haemost 2020; 4:1178-1191.
• DVT found in 14.7% (ultrasound screening) in 156 non-ICU patients with elevated D-dimer >1000ng/ml
• DVT found in 85.4% (ultrasound screening) of 48 critically ill patients with 75% isolated distal / 10.4% proximal DVT with marked elevations in D-dimerDemelo-Rodriguez P, Cervilla-Munoz E, Ordieres-Ortega L, et al. Thrombo Res 2020; 192:23-26.
Ren B, Yan F, Deng Z, et al. Circulation 2020; 142:181-183.
COVID-19 COAGULOPATHY (At Discharge and Beyond)• Screening for DVT upon admission to an Inpatient rehabilitation facility
DVT 22% (25/113) with 7.1% (8/113) Proximal• Risk factors – male sex, younger age, and having been on ventilatorKirshblum SC, DeLauter G, Eren F, et al. American Journal of Physical Medicine and Rehabilitation 2021; 100:419-423.
Artifoni M, Danic G, Gautier G, et al. J Thromb Thrombolysis https://doi.org/10.1007/s11239-020-02146-z
• Systematic lower limb venous duplex ultrasonographty performed at hospital discharge or earlier if DVT clnically suspected and Chest CT performed if PE suspected.
• DVT 22.5% (16/71) and PE 10% (7/71) despite adequate prophylaxis predicted by Increased D-dimer
• Following 1877 hospital discharges, 9 episodes of hospital associated DVT within 42 days (0.5%) or rate of 4.8/1000 discharges
• Over 2019 following 18,159 discharges, 56 episodes of hospital associated DVT within 42 days (0.7%)
Roberts LN, Whyte MB, Georgiou L, et al. Blood 2020; 136:1347-1350.
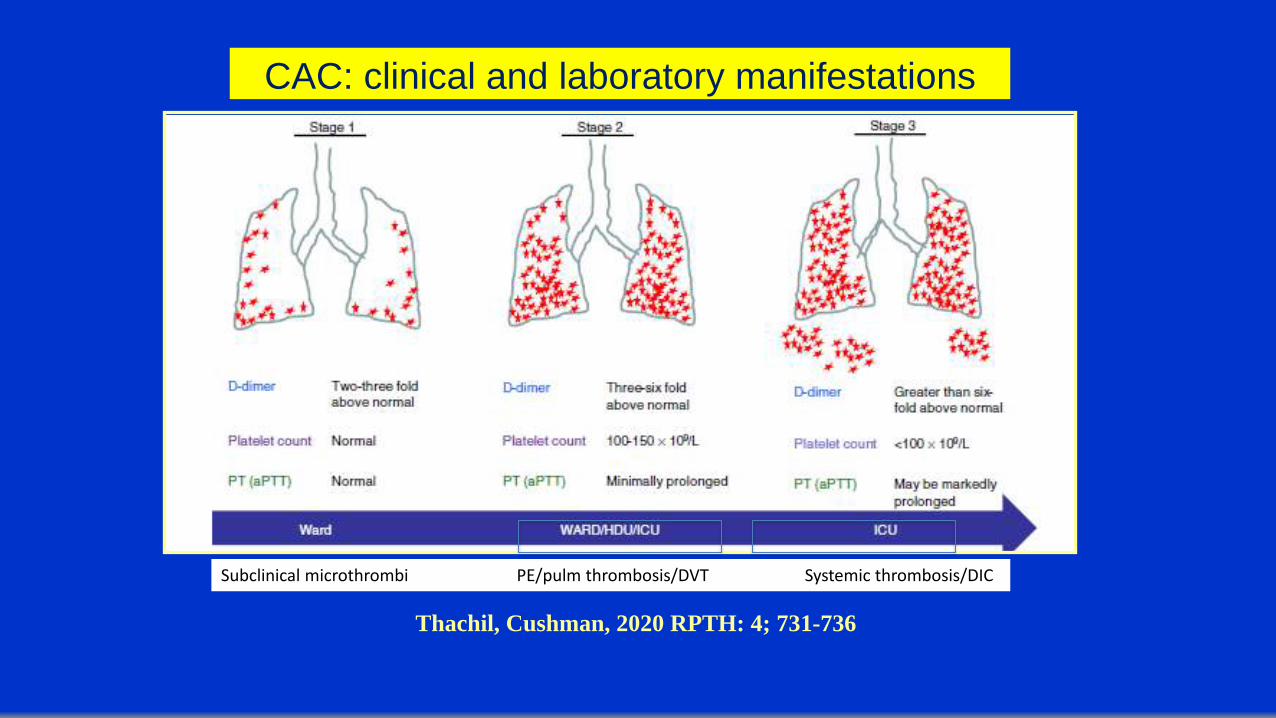
CAC: clinical and laboratory manifestations
Thachil, Cushman, 2020 RPTH: 4; 731-736
Subclinical microthrombi PE/pulm thrombosis/DVT Systemic thrombosis/DIC
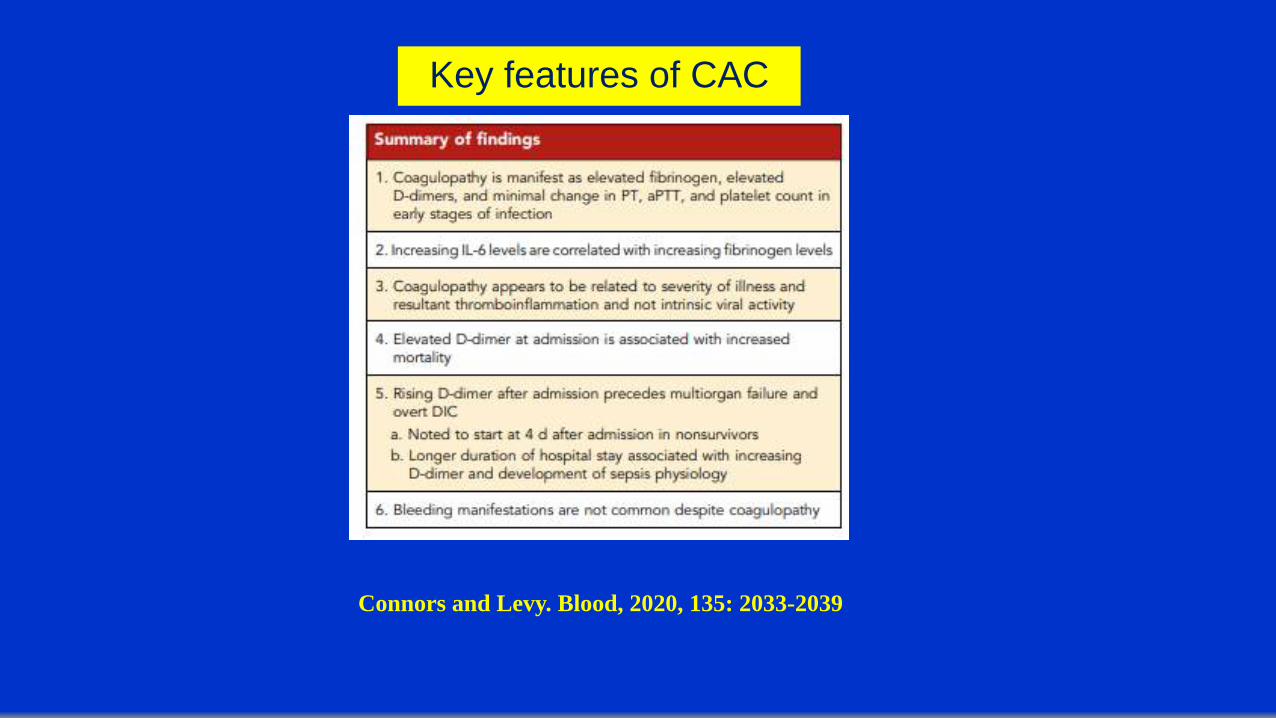
Key features of CAC
Connors and Levy. Blood, 2020, 135: 2033-2039
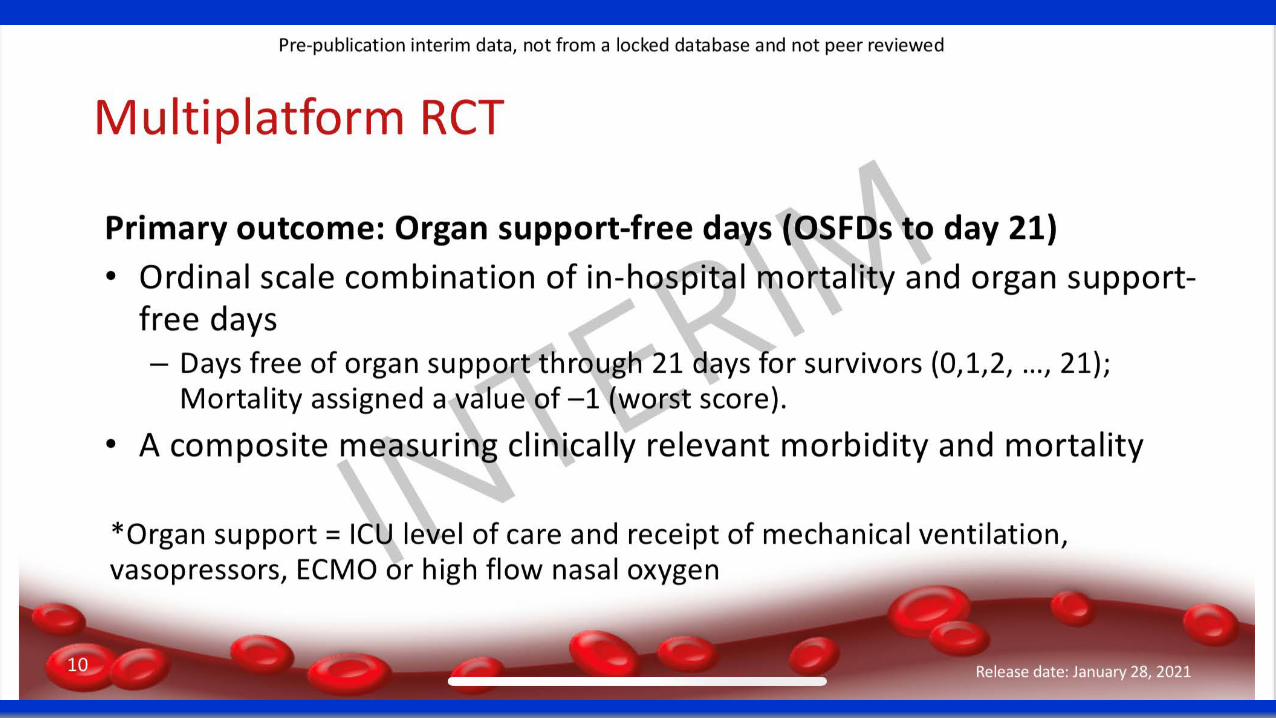

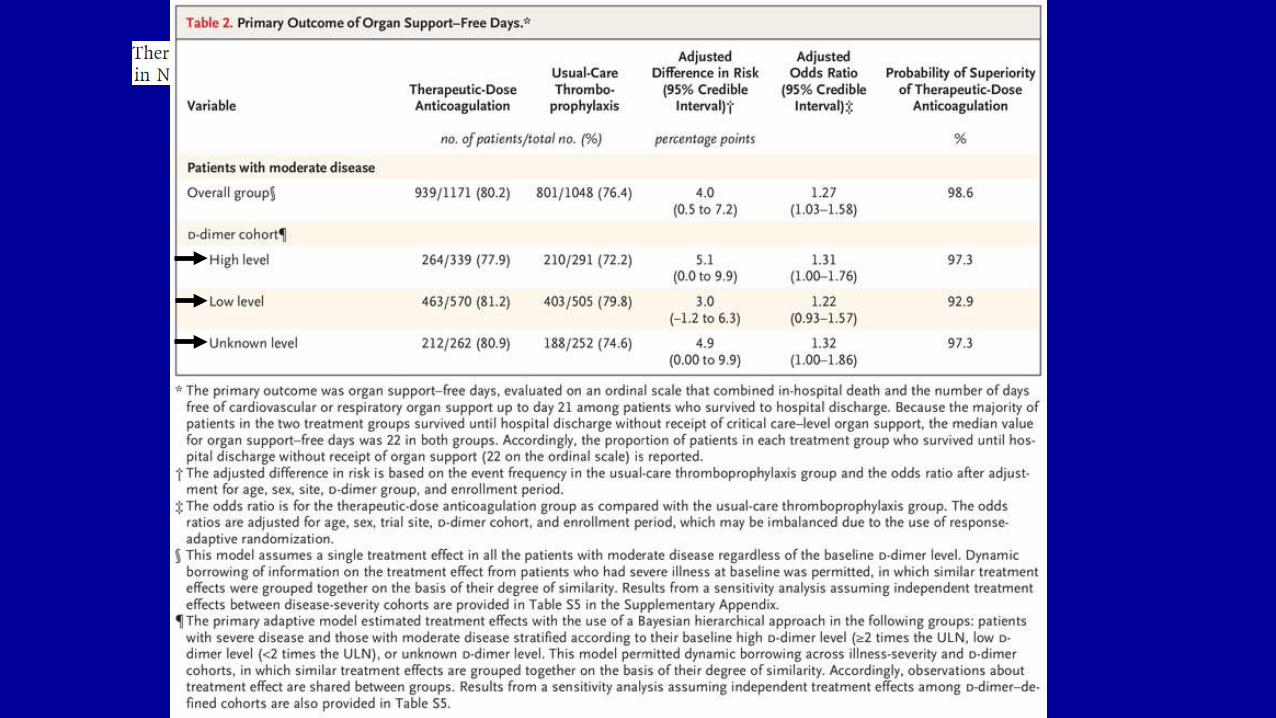
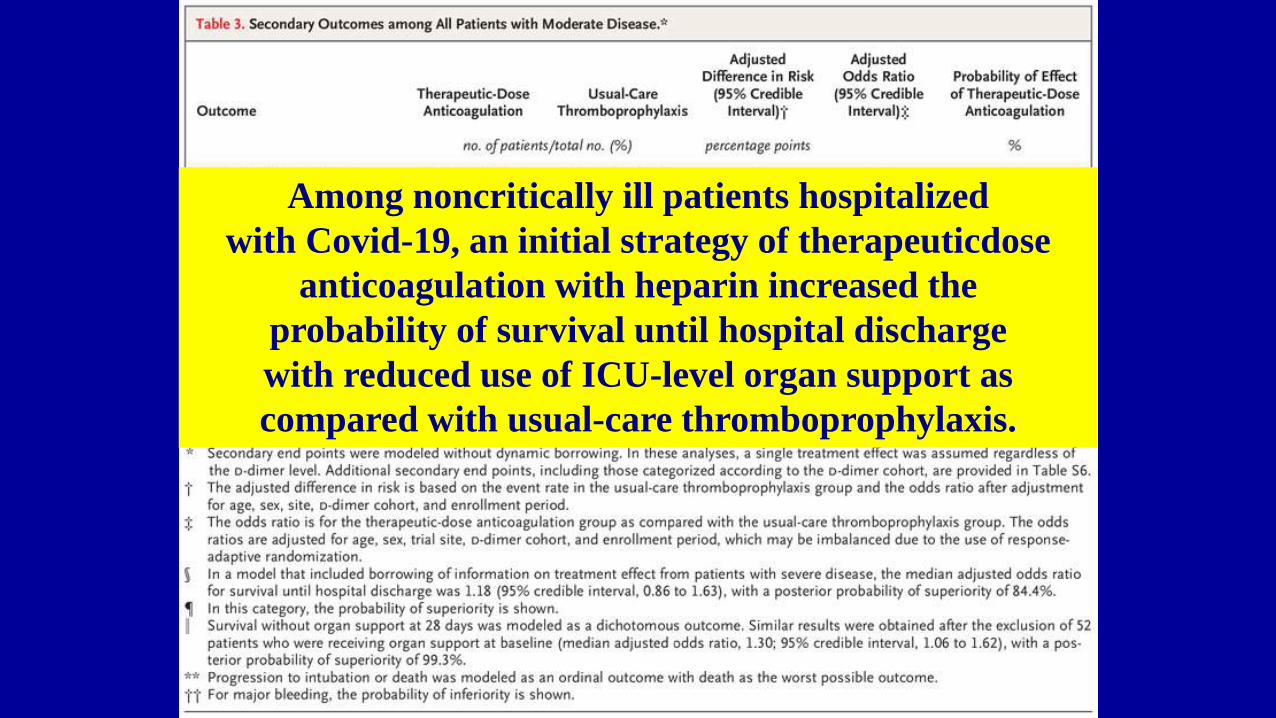
Among noncritically ill patients hospitalizedwith Covid-19, an initial strategy of therapeuticdose
anticoagulation with heparin increased theprobability of survival until hospital dischargewith reduced use of ICU-level organ support ascompared with usual-care thromboprophylaxis.
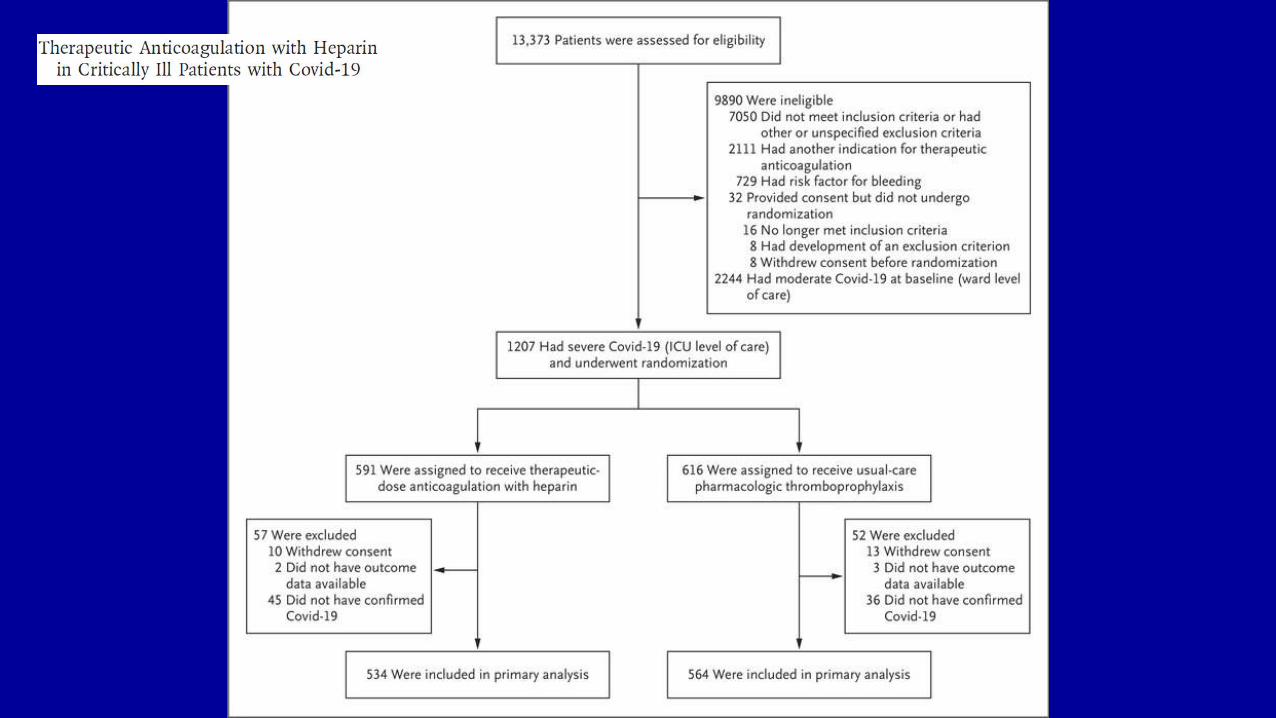
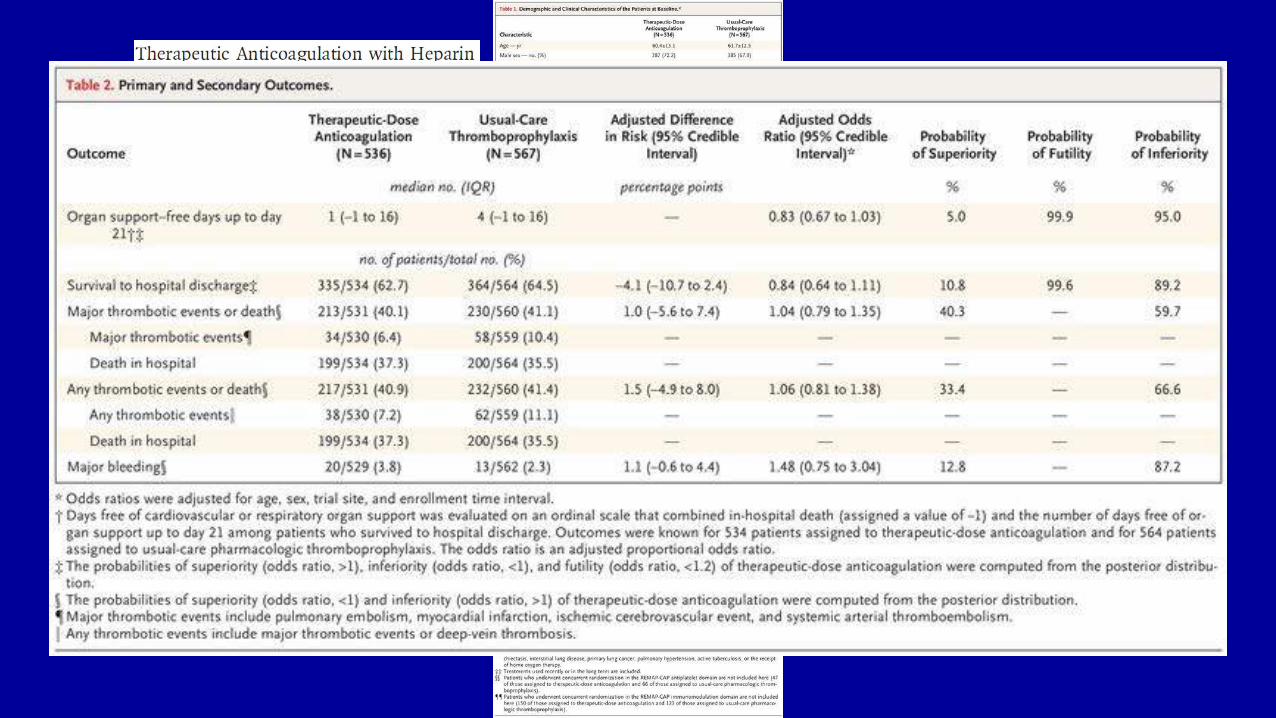
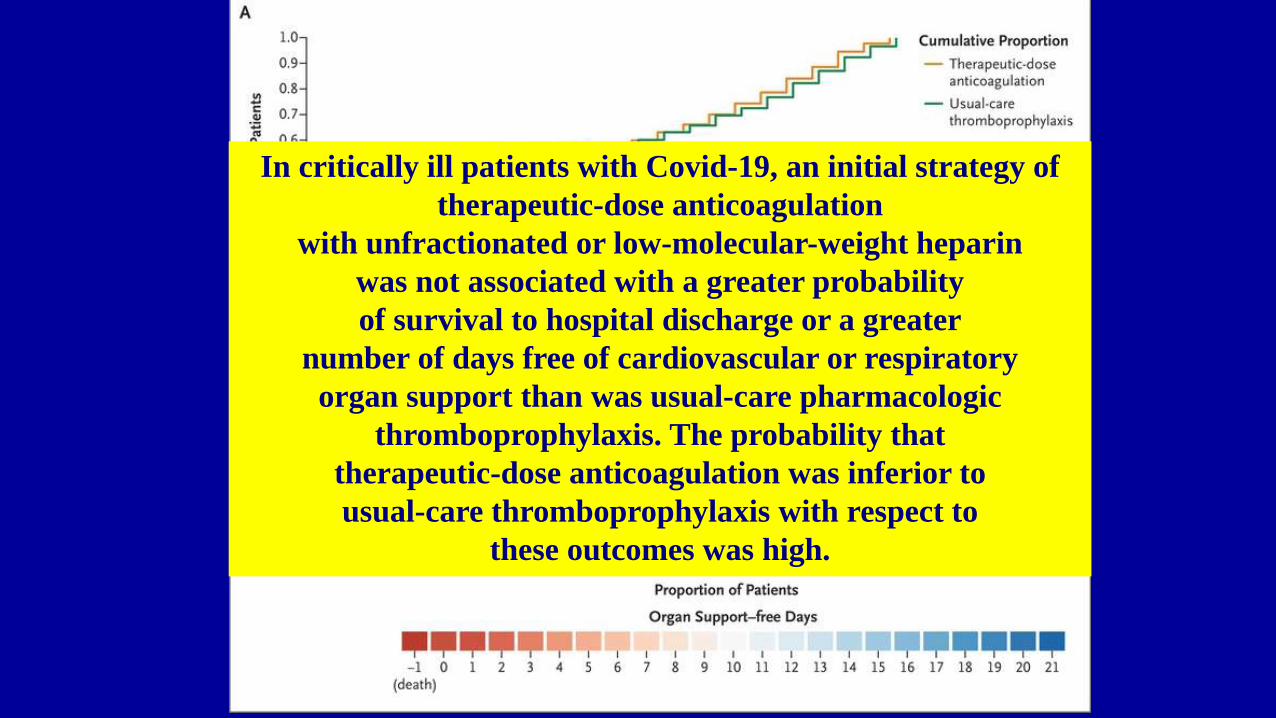
In critically ill patients with Covid-19, an initial strategy of therapeutic-dose anticoagulation
with unfractionated or low-molecular-weight heparinwas not associated with a greater probabilityof survival to hospital discharge or a greater
number of days free of cardiovascular or respiratoryorgan support than was usual-care pharmacologic
thromboprophylaxis. The probability thattherapeutic-dose anticoagulation was inferior tousual-care thromboprophylaxis with respect to
these outcomes was high.
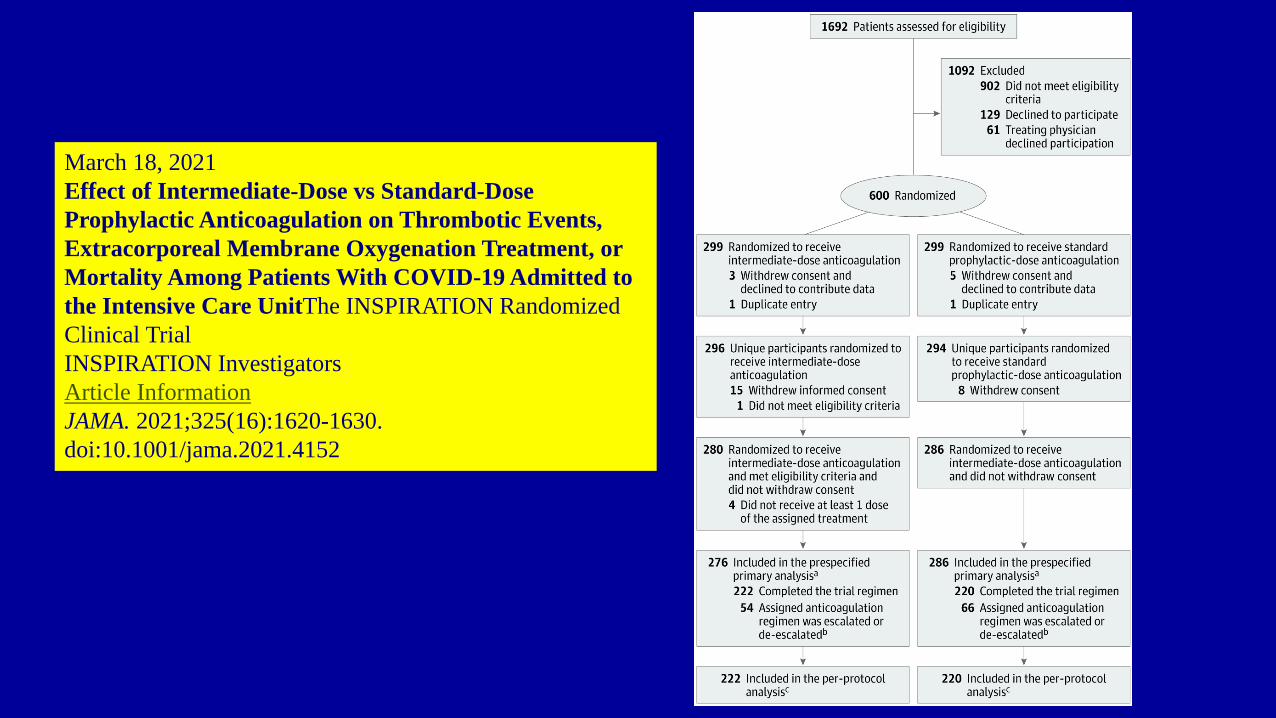
March 18, 2021Effect of Intermediate-Dose vs Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care UnitThe INSPIRATION Randomized Clinical TrialINSPIRATION InvestigatorsArticle InformationJAMA. 2021;325(16):1620-1630. doi:10.1001/jama.2021.4152
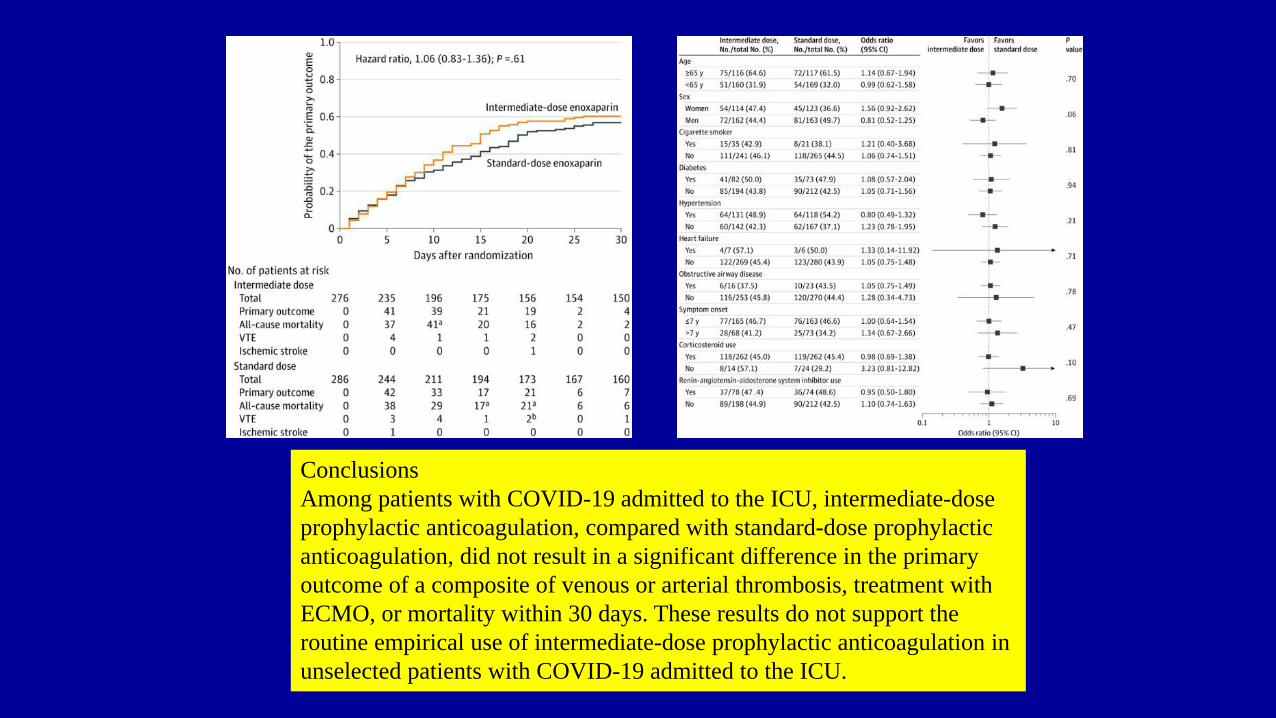
ConclusionsAmong patients with COVID-19 admitted to the ICU, intermediate-dose prophylactic anticoagulation, compared with standard-dose prophylactic anticoagulation, did not result in a significant difference in the primary outcome of a composite of venous or arterial thrombosis, treatment with ECMO, or mortality within 30 days. These results do not support the routine empirical use of intermediate-dose prophylactic anticoagulation in unselected patients with COVID-19 admitted to the ICU.
Anticoagulation in Patients Hospitalized
with COVID-19
Renato D. Lopes, MD, PhDon behalf of the ACTION COALITION
COVID-19 Brazil Investigators
The AntiCoagulaTIon cOroNavirus (ACTION) Trial
www.thelancet.com Published online June 4, 2021 https://doi.org/10.1016/S0140-6736(21)01203-4
Slides provided by Eduardo Ramacciotti
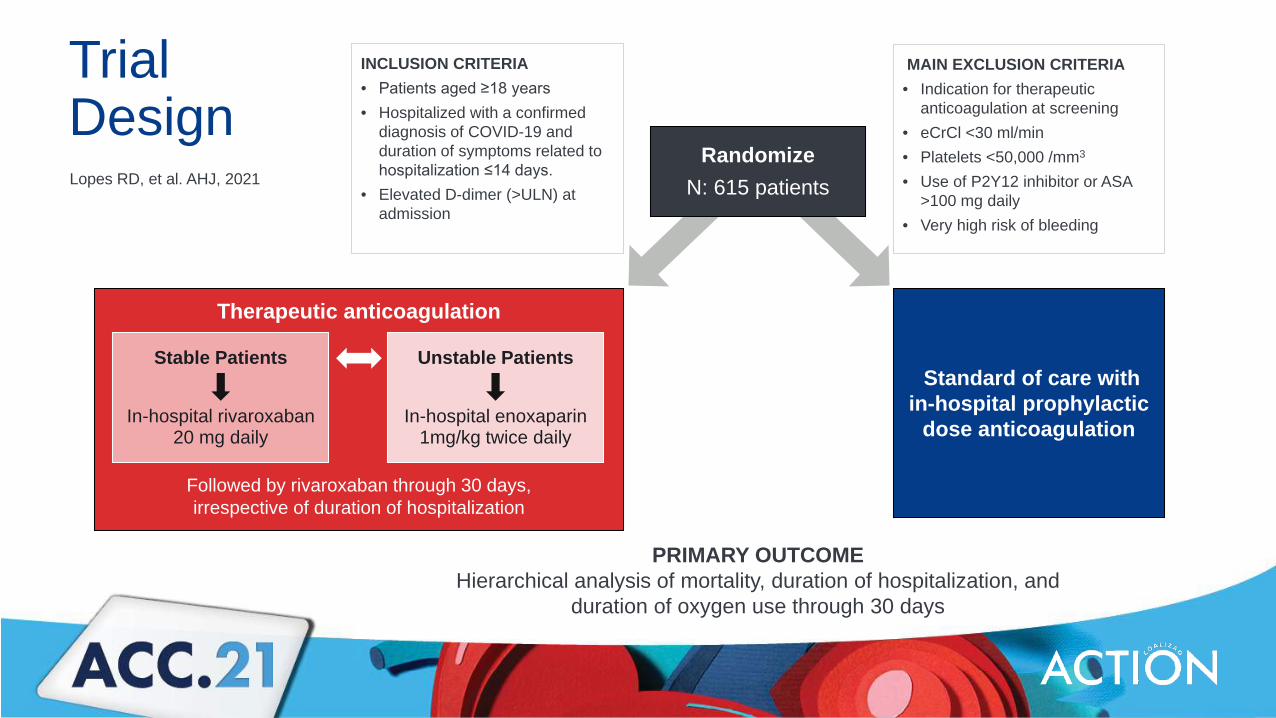
Therapeutic anticoagulation
Followed by rivaroxaban through 30 days, irrespective of duration of hospitalization
TrialDesign
Multicenter, phase IV, randomized clinical trial
PRIMARY OUTCOMEHierarchical analysis of mortality, duration of hospitalization, and
duration of oxygen use through 30 days
Standard of care with in-hospital prophylactic
dose anticoagulation
INCLUSION CRITERIA• Patients aged ≥18 years• Hospitalized with a confirmed
diagnosis of COVID-19 and duration of symptoms related to hospitalization ≤14 days.
• Elevated D-dimer (>ULN) at admission
MAIN EXCLUSION CRITERIA• Indication for therapeutic
anticoagulation at screening• eCrCl <30 ml/min• Platelets <50,000 /mm3
• Use of P2Y12 inhibitor or ASA >100 mg daily
• Very high risk of bleeding
Stable Patients
In-hospital rivaroxaban 20 mg daily
Unstable Patients
In-hospital enoxaparin1mg/kg twice daily
Lopes RD, et al. AHJ, 2021 Randomize
N: 615 patients
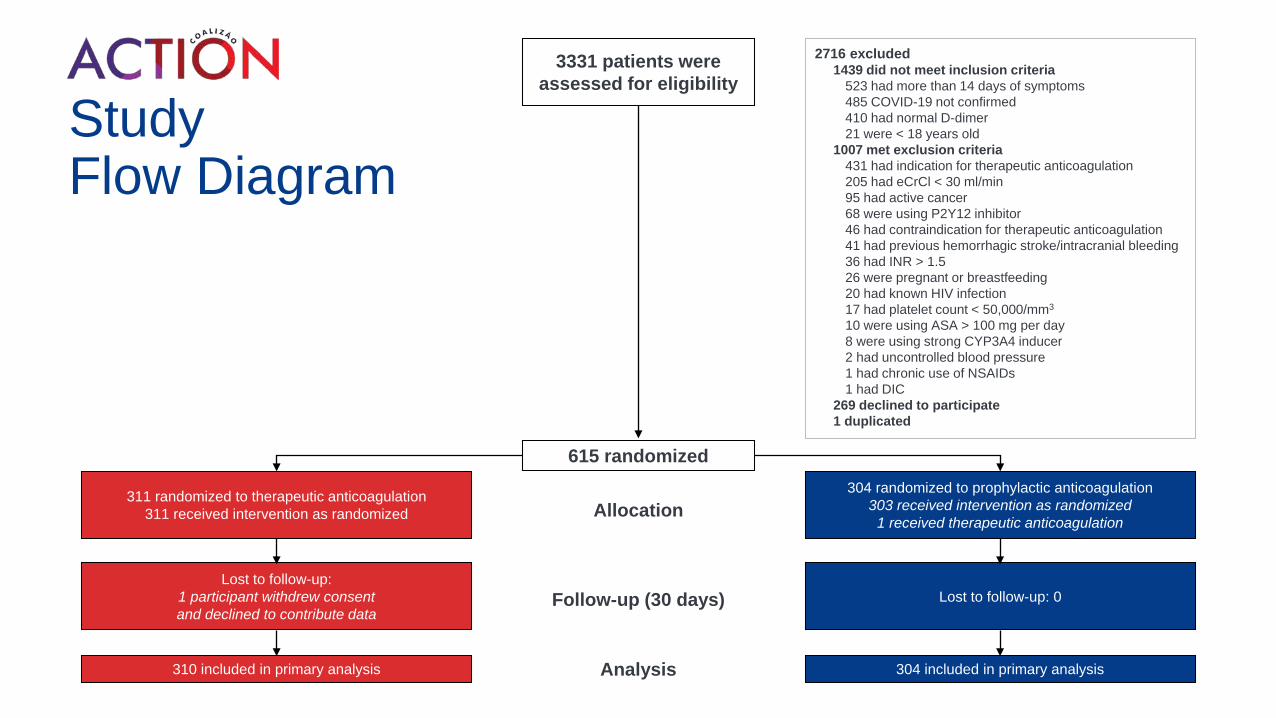
Study Flow Diagram
311 randomized to therapeutic anticoagulation311 received intervention as randomized
304 randomized to prophylactic anticoagulation303 received intervention as randomized
1 received therapeutic anticoagulation
Analysis
3331 patients were assessed for eligibility
615 randomized
Follow-up (30 days)
Allocation
Lost to follow-up:1 participant withdrew consent and declined to contribute data
310 included in primary analysis
Lost to follow-up: 0
304 included in primary analysis
2716 excluded1439 did not meet inclusion criteria
523 had more than 14 days of symptoms485 COVID-19 not confirmed410 had normal D-dimer21 were < 18 years old
1007 met exclusion criteria431 had indication for therapeutic anticoagulation205 had eCrCl < 30 ml/min95 had active cancer68 were using P2Y12 inhibitor46 had contraindication for therapeutic anticoagulation41 had previous hemorrhagic stroke/intracranial bleeding36 had INR > 1.526 were pregnant or breastfeeding20 had known HIV infection17 had platelet count < 50,000/mm3
10 were using ASA > 100 mg per day8 were using strong CYP3A4 inducer2 had uncontrolled blood pressure1 had chronic use of NSAIDs1 had DIC
269 declined to participate1 duplicated
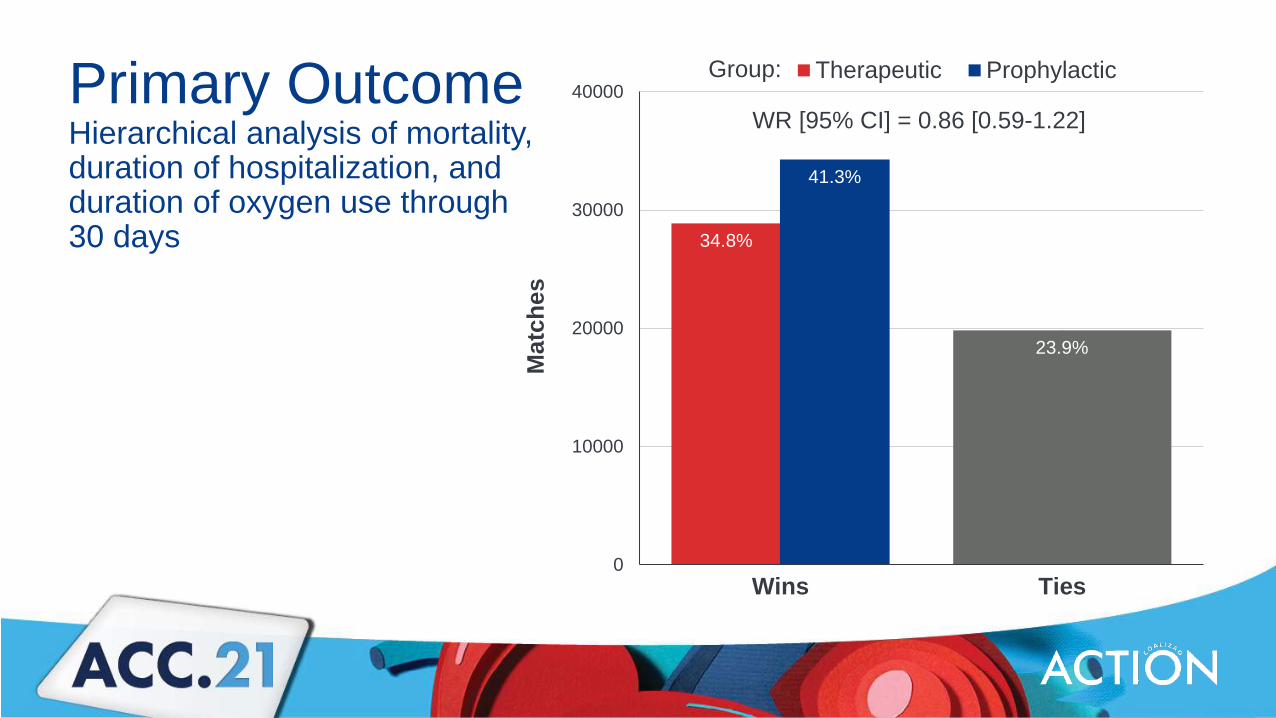
Primary Outcome Hierarchical analysis of mortality, duration of hospitalization, and duration of oxygen use through 30 days 34.8%
41.3%
23.9%
0
10000
20000
30000
40000
Wins Ties
Mat
ches
Group: Therapeutic Prophylactic
WR [95% CI] = 0.86 [0.59-1.22]
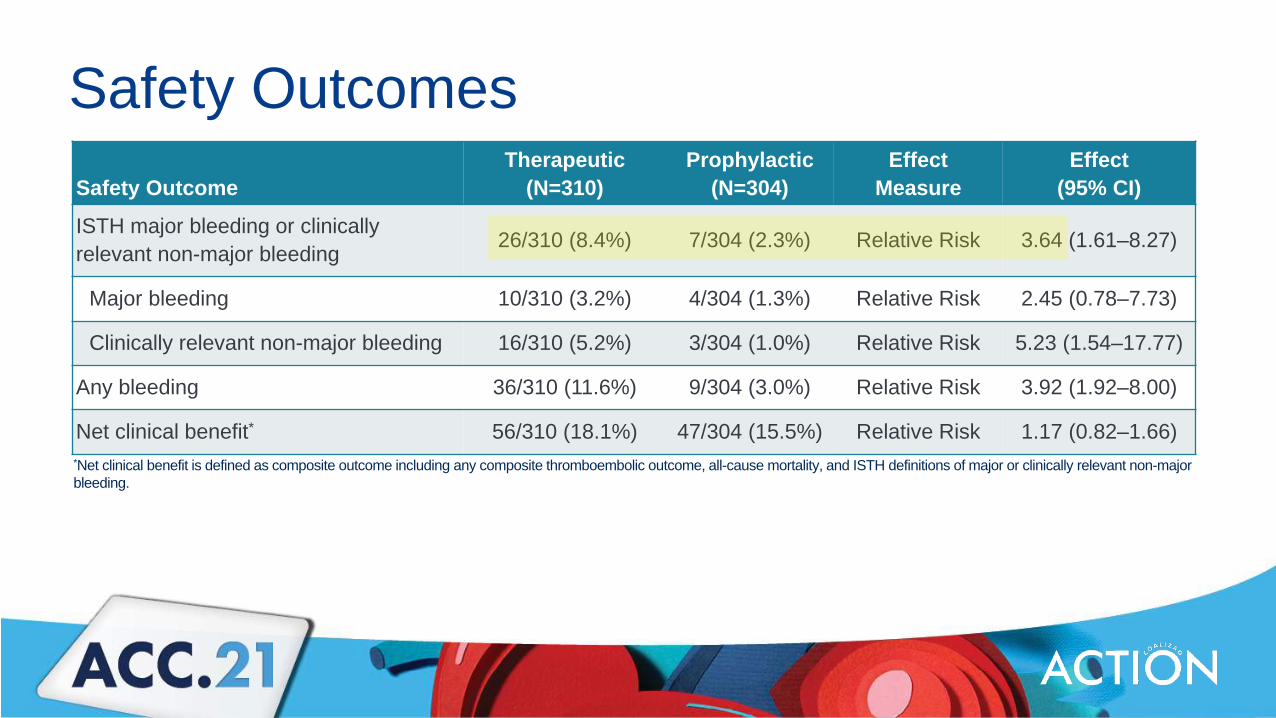
Safety OutcomesSafety Outcome
Therapeutic(N=310)
Prophylactic(N=304)
EffectMeasure
Effect(95% CI)
ISTH major bleeding or clinically relevant non-major bleeding 26/310 (8.4%) 7/304 (2.3%) Relative Risk 3.64 (1.61–8.27)
Major bleeding 10/310 (3.2%) 4/304 (1.3%) Relative Risk 2.45 (0.78–7.73)
Clinically relevant non-major bleeding 16/310 (5.2%) 3/304 (1.0%) Relative Risk 5.23 (1.54–17.77)
Any bleeding 36/310 (11.6%) 9/304 (3.0%) Relative Risk 3.92 (1.92–8.00)
Net clinical benefit* 56/310 (18.1%) 47/304 (15.5%) Relative Risk 1.17 (0.82–1.66)*Net clinical benefit is defined as composite outcome including any composite thromboembolic outcome, all-cause mortality, and ISTH definitions of major or clinically relevant non-major bleeding.
ConclusionIn patients hospitalized with COVID-19 with elevated D-dimer levels, initial in-hospital therapeutic anticoagulation with rivaroxaban 20 mg once daily for stable patients or enoxaparin for unstable patients followed by rivaroxaban through 30 days did not improve clinical outcomes and increased bleeding compared with in-hospital prophylactic anticoagulation.
Copyright © 2021 American Society of Hematology
DRAFT RECOMMENDATION (UPDATED JULY 8, 2021)
The ASH guideline panel suggests not using anticoagulant outpatient
thromboprophylaxis in patients with COVID-19 who are being discharged from the
hospital and who do not have suspected or confirmed VTE or another indication for
anticoagulation (conditional recommendation based on very low certainty in the
evidence about effects).
Remarks: An individualized assessment of the patient’s risk of thrombosis and bleeding and
shared decision-making is important when deciding whether to use post-discharge
thromboprophylaxis. Validated risk assessment models to estimate thrombotic and bleeding
risk in COVID-19 patients following hospital discharge are not available. The panel
acknowledged that post-discharge thromboprophylaxis may be reasonable in patients judged
to be at high thrombotic risk and low bleeding risk.
Design: Prospective, randomized, open-label, controlled, multi-center trial
No anticoagulation
Rivaroxaban (10 mg/day)
Day 35±4
R
Day 75 (phone call)
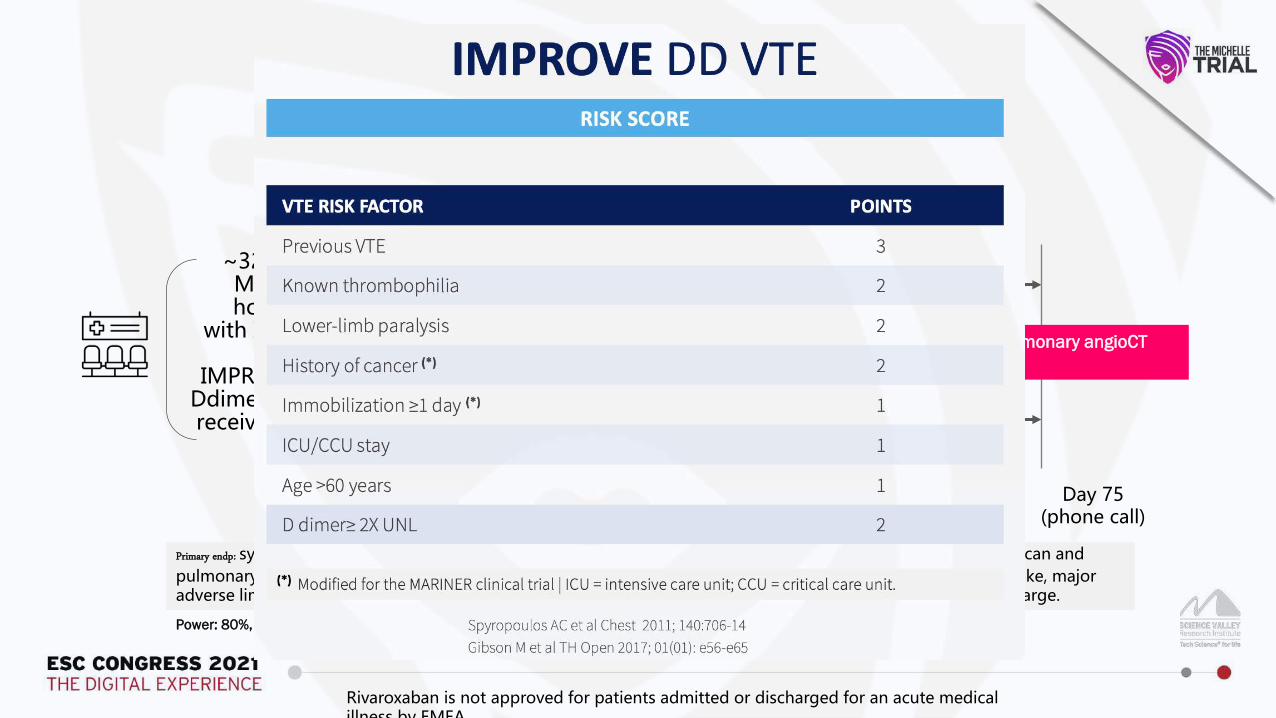
~320 COVID+Medically Ill hospitalized
with IMPROVE ≥4or
IMPROVE 2-3 with Ddimer >500 ng/mL receiving LMWH or
UFH Discharge
Screening
Follow-up
Doppler US + pulmonary angioCTat day 35+4
Primary endp: symptomatic VTE, VTE-related death, VTE detected by mandatory bilateral lower limbs venous duplex scan and pulmonary angioCT on day 35±4 post-hospital discharge and (myocardial infarction [MI], non-hemorrhagic stroke, major adverse limb events [MALE] and cardiovascular [CV] death + all cause death up to day 35±4 post-hospital discharge.
Power: 80%, Two sided alpha 0.05 (Control 15%, Treatment 5%; 67% RRR)
STUDY DESIGN
Rivaroxaban is not approved for patients admitted or discharged for an acute medical illness by EMEA
KEY INCLUSION AND EXCLUSION CRITERIA
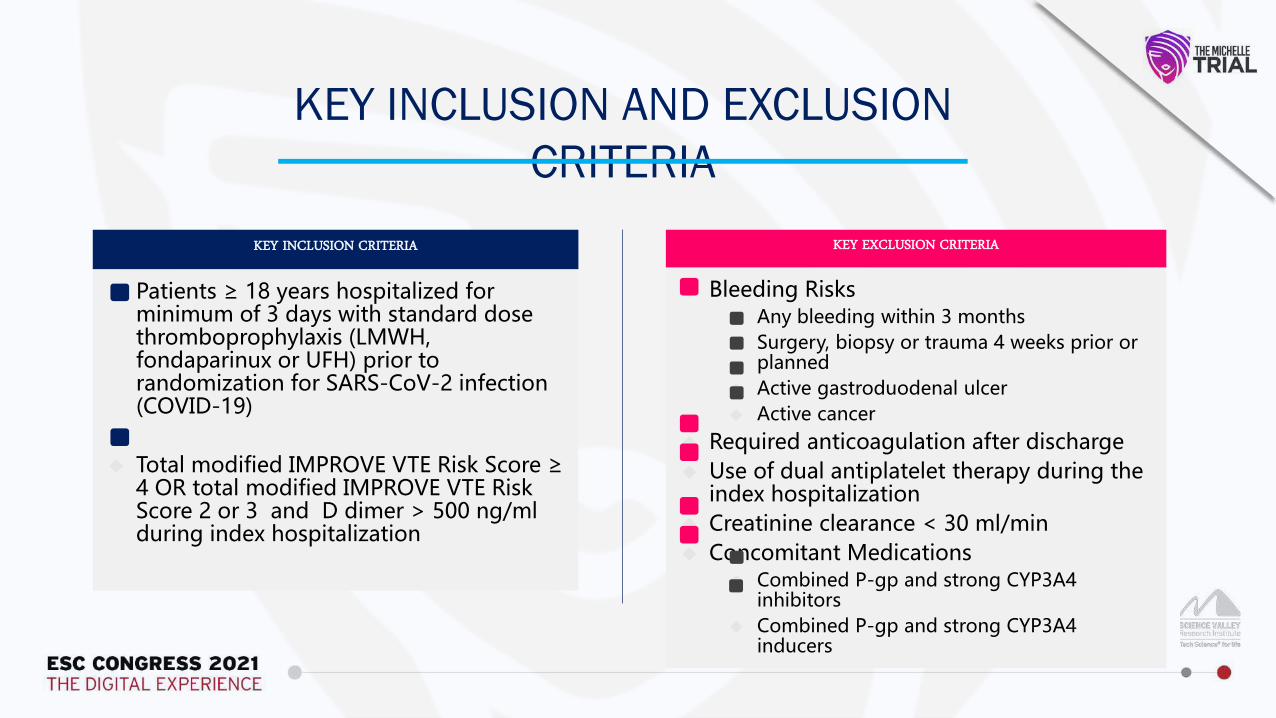
KEY INCLUSION CRITERIA
Patients ≥ 18 years hospitalized for minimum of 3 days with standard dose thromboprophylaxis (LMWH, fondaparinux or UFH) prior to randomization for SARS-CoV-2 infection (COVID-19)
Total modified IMPROVE VTE Risk Score ≥ 4 OR total modified IMPROVE VTE Risk Score 2 or 3 and D dimer > 500 ng/ml during index hospitalization
KEY EXCLUSION CRITERIA
Bleeding Risks Any bleeding within 3 months Surgery, biopsy or trauma 4 weeks prior or
planned Active gastroduodenal ulcer Active cancer
Required anticoagulation after discharge Use of dual antiplatelet therapy during the
index hospitalization Creatinine clearance < 30 ml/min Concomitant Medications
Combined P-gp and strong CYP3A4 inhibitors
Combined P-gp and strong CYP3A4 inducers
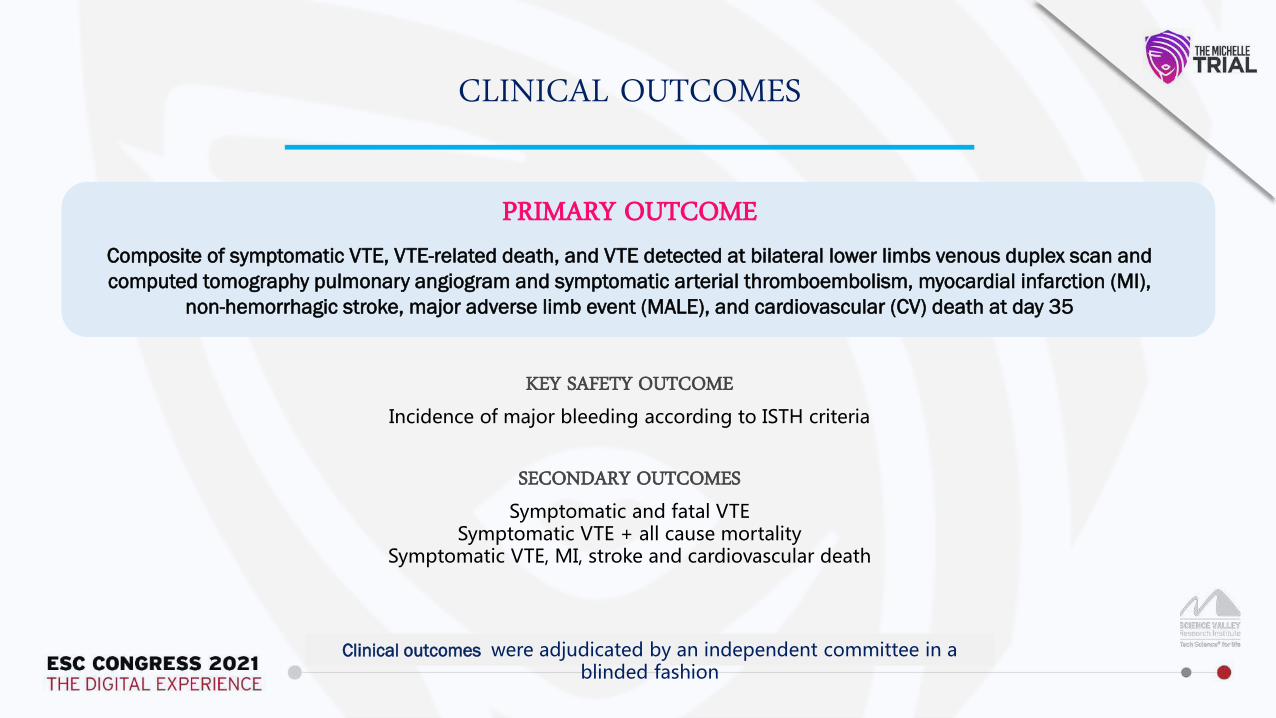
CLINICAL OUTCOMES
PRIMARY OUTCOMEComposite of symptomatic VTE, VTE-related death, and VTE detected at bilateral lower limbs venous duplex scan and computed tomography pulmonary angiogram and symptomatic arterial thromboembolism, myocardial infarction (MI),
non-hemorrhagic stroke, major adverse limb event (MALE), and cardiovascular (CV) death at day 35
Clinical outcomes were adjudicated by an independent committee in a blinded fashion
SECONDARY OUTCOMES
Symptomatic and fatal VTESymptomatic VTE + all cause mortality
Symptomatic VTE, MI, stroke and cardiovascular death
KEY SAFETY OUTCOME
Incidence of major bleeding according to ISTH criteria
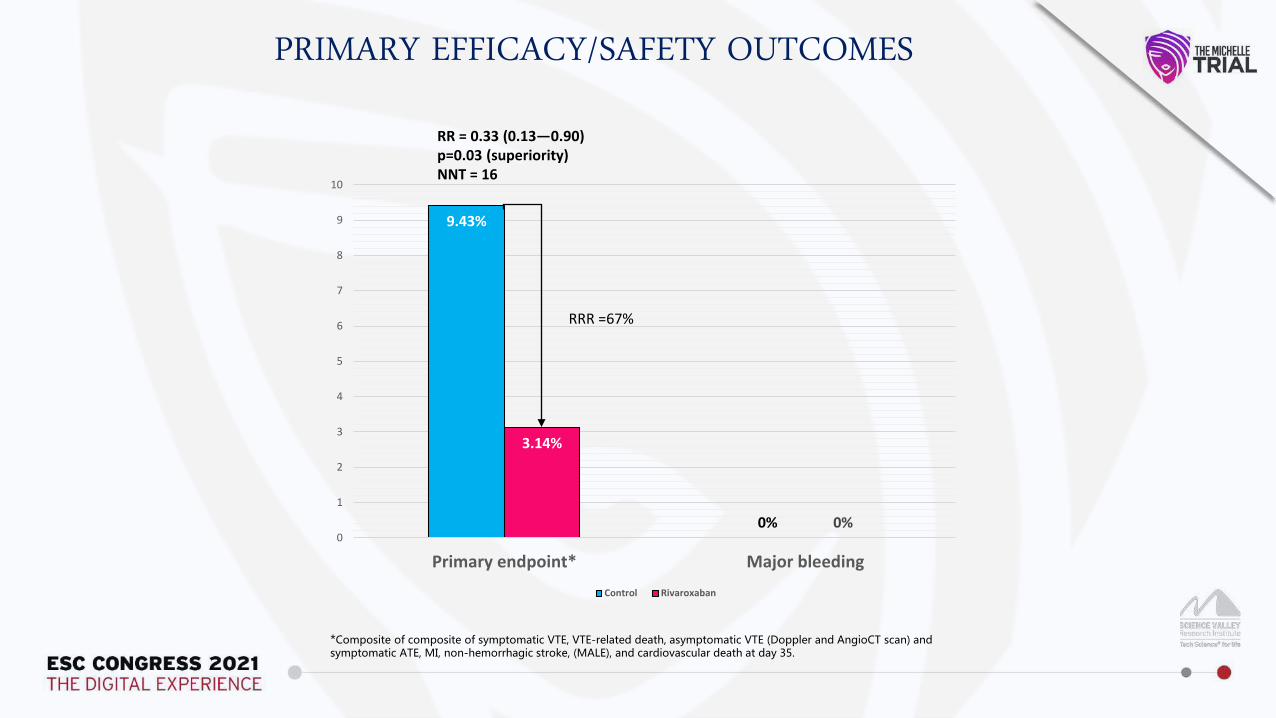
9.43%
0%
3.14%
0%0
1
2
3
4
5
6
7
8
9
10
Primary endpoint* Major bleedingControl Rivaroxaban
PRIMARY EFFICACY/SAFETY OUTCOMES
*Composite of composite of symptomatic VTE, VTE-related death, asymptomatic VTE (Doppler and AngioCT scan) and symptomatic ATE, MI, non-hemorrhagic stroke, (MALE), and cardiovascular death at day 35.
RRR =67%
RR = 0.33 (0.13—0.90)p=0.03 (superiority)NNT = 16
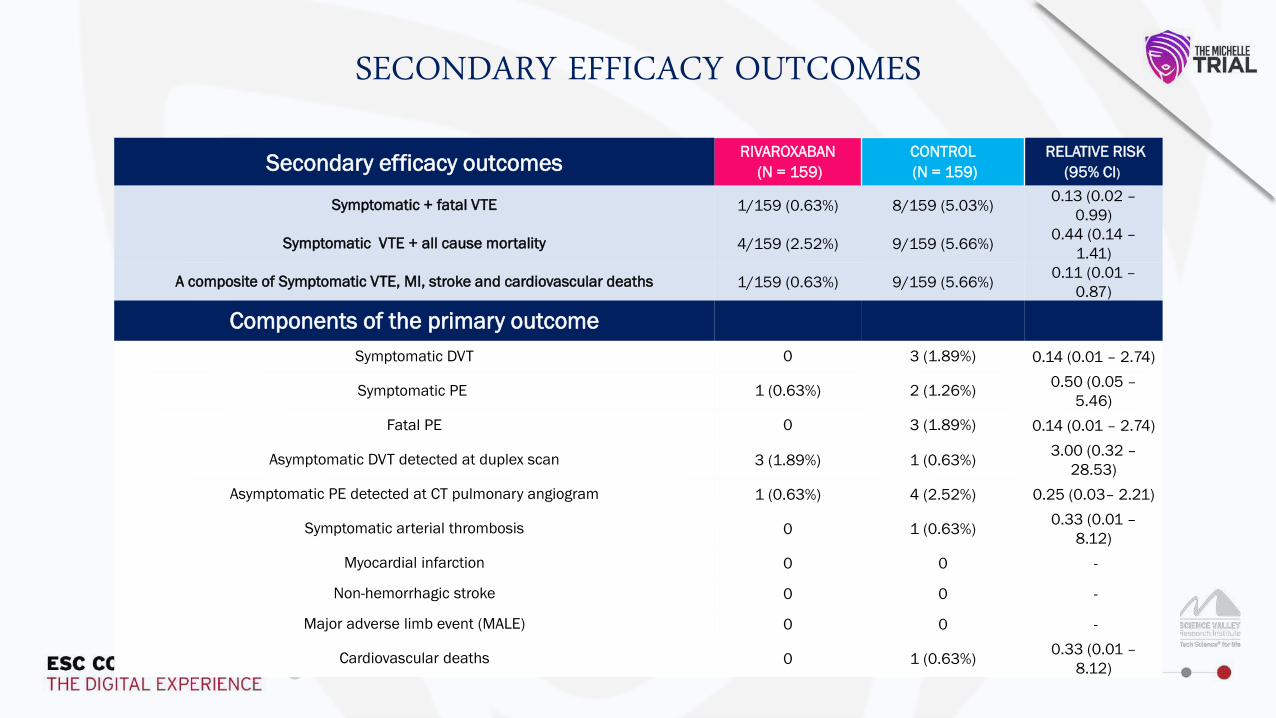
Secondary efficacy outcomes RIVAROXABAN(N = 159)
CONTROL(N = 159)
RELATIVE RISK(95% CI)
Symptomatic + fatal VTE 1/159 (0.63%) 8/159 (5.03%) 0.13 (0.02 –0.99)
Symptomatic VTE + all cause mortality 4/159 (2.52%) 9/159 (5.66%) 0.44 (0.14 –1.41)
A composite of Symptomatic VTE, MI, stroke and cardiovascular deaths 1/159 (0.63%) 9/159 (5.66%) 0.11 (0.01 –0.87)
Components of the primary outcomeSymptomatic DVT 0 3 (1.89%) 0.14 (0.01 – 2.74)
Symptomatic PE 1 (0.63%) 2 (1.26%) 0.50 (0.05 –5.46)
Fatal PE 0 3 (1.89%) 0.14 (0.01 – 2.74)
Asymptomatic DVT detected at duplex scan 3 (1.89%) 1 (0.63%) 3.00 (0.32 –28.53)
Asymptomatic PE detected at CT pulmonary angiogram 1 (0.63%) 4 (2.52%) 0.25 (0.03– 2.21)
Symptomatic arterial thrombosis 0 1 (0.63%) 0.33 (0.01 –8.12)
Myocardial infarction 0 0 -
Non-hemorrhagic stroke 0 0 -
Major adverse limb event (MALE) 0 0 -
Cardiovascular deaths 0 1 (0.63%) 0.33 (0.01 –8.12)
SECONDARY EFFICACY OUTCOMES
CONCLUSION
In patients discharged after hospitalization due to COVID-19 with increased IMPROVE score, thromboprophylaxis with rivaroxaban 10 mg once-daily for 35 days improved clinical outcomes, without increasing bleeding compared with
no out-of-hospital anticoagulation
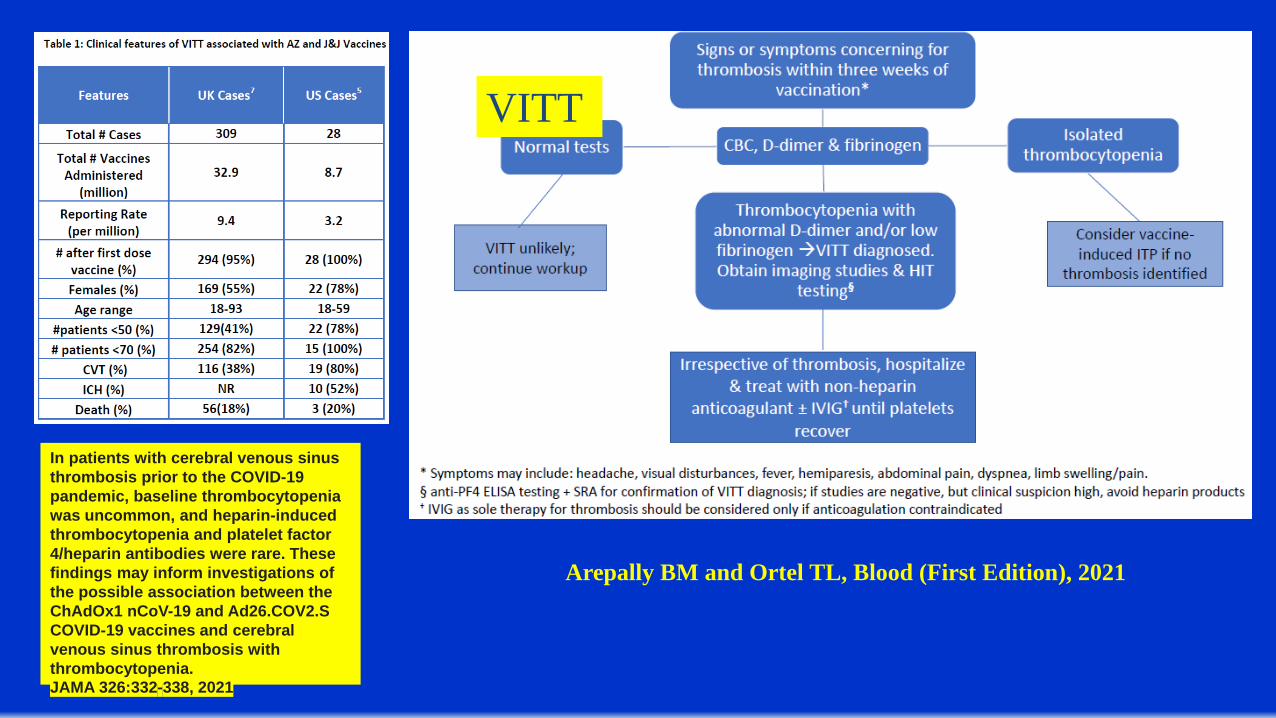
Arepally BM and Ortel TL, Blood (First Edition), 2021
VITT
In patients with cerebral venous sinus thrombosis prior to the COVID-19 pandemic, baseline thrombocytopenia was uncommon, and heparin-induced thrombocytopenia and platelet factor 4/heparin antibodies were rare. These findings may inform investigations of the possible association between the ChAdOx1 nCoV-19 and Ad26.COV2.S COVID-19 vaccines and cerebral venous sinus thrombosis with thrombocytopenia.JAMA 326:332-338, 2021

Thank You