Embed Size (px)
Citation preview

7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 1/8
Treating the Elderly Patient with Acute Myelogenous
Leukemia
Selina M. Luger 1
1Hematologic Malignancies and Stem Cell Transplant Program, Hematology-Oncology Division, University of
Pennsylvania Medical Center, Philadelphia, PA
Decisions regarding the optimal treatment of acute myelogenous leukemia in the elderly patient requires the
consideration of multiple factors. Population-based studies have demonstrated that, for all age groups, aggressive
therapy results in improved survival and quality of life when compared with palliative care. The optimal induction and
postremission regimen for older patients has yet to be determined. Furthermore, not all patients are candidates for
such therapy. Consideration of patient and disease-related factors can help to determine the appropriateness of
intensive therapy in a given patient. For those patients for whom aggressive induction therapy does not seem to be in
their best interest, novel agents are being investigated that will hopefully address the issues of induction death and
early relapse associated with these patient populations.
How Is Acute Myeloid Leukemia in the Elderly
Different?Acute myeloid leukemia (AML) presents at all ages, but is mainly a
disease of the elderly, with a median age of 69 years in the white US
population.1 In the Swedish Acute Leukemia Registry, 68% of
patients diagnosed with AML since 1973 were over age 60 years;
between 1997 and 2005, 75% was aged 60 years or more.2
Prognosis worsens every decade beginning at age 30 to 40.1,3 A
report by the German Acute Myeloid Leukemia Cooperative Group
looked at patients 16 to 85 years of age enrolled in two consecutive
trials in 1992 and 1999 with no upper age limit who had AML. 4 In a
multivariate analysis of prognostic factors, age Ն 60 years was a
statistically significant poor prognostic factor for complete remis-
sion (CR), overall survival (OS), remission duration, and relapse-free survival (RFS). Population-based studies have reported 3- and
5-year survival rates of only 9% to 10% and 3% to 8%, respectively,
in patients over age 60, compared with 5-year survival rates of up to
50% for younger patients.2,5,6 Poorer outcome has traditionally been
considered to be the result of less intensive therapy in this
population, concurrent comorbidities, a higher likelihood of under-
lying hematopoietic disorders, and biologically poor risk disease.
Moreover, because of the perception that older adults are less likely
to do well with standard therapy, clinicians are less likely to treat
these patients aggressively or refer them to centers that do so. As
such, lower levels of aggressive treatment may compound underly-
ing prognostic differences associated with patient factors and
disease biology.
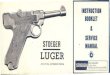
In a retrospective analysis of 968 adults with AML in five
Southwest Oncology Group (SWOG) trials to understand the nature
of how AML changes with age, differences were noted in perfor-
mance status (PS), presenting white blood cell (WBC) count,
percentage marrow blasts, expression of multidrug resistance (MDR),
and karyotype.7 (Table 1). When compared with disease in patients
younger than age 56, those age Ն 56 are are more likely to have
unfavorable cytogenetics and less likely to have favorable cytogenet-
ics. Differences in disease biology are also apparent. For example,
in an analysis of oncogenic pathway dysresgulation in 425 patients
with AML, there is a statistically significant difference in the
expression of E2F and PI3 (phosphoinositide 3) kinase activation,
but a higher probability of RAS, TNF (tumor necrosis factor), Src,
and EPI (extrinsic pathway inhibitor) pathway activation.8 In
younger patients, a similar profile is of poor prognostic significance
and portends for decreased sensitivity to anthracycline.
What Is the Standard Therapy for the Older Patient
With AML?The combination of an anthracycline and cytarabine (3ϩ7), with or
without other agents, is considered the standard induction regimen
for patients under age 60, followed by consolidation therapy that
often uses high-dose cytarabine.9–11 As noted previously, the use of
the standard 3ϩ7 regimen in elderly patients does not yield results
similar to those seen in younger patients. Recent studies have,
therefore, focused on dose intensification of anthracyclines and/or
postremission therapy (Table 2).
In a recently published cooperative group study, Lowenberg et al 12
reports the results of a comparison of induction therapy with
daunorubicin (DNR) at a dose of 45 mg/m2 or 90 mg/m2 in 813
patients over age 60 with previously untreated AML. Although CR
rates were improved in the group that received the higher dose of
DNR (64% vs 54%, Pϭ .002), there was no significant difference in
the two induction groups with respect to OS and event-free survival
(EFS). Thirty-day mortality was 11% to 12% in both groups.
Two-year probabilities of relapse after CR and death during CR for
the standard versus intensified DNR groups were 61% versus 54%
for relapse and 10% versus 16% for death. Exploratory post-hoc
analysis of patients aged 60 to 65 (n ϭ 299), however, demonstrated
a difference in the two dose groups with respect to CR (51% vs
73%), 2-year EFS (14% vs 29%, Pϭ .002), and 2-year OS (23% vs
38%, P Ͻ .001). In the subgroup with core binding factor
abnormalities (n ϭ 33), escalated dose was associated with in-
creased CR and decreased risk of disease progression or death (CR,
74% vs 93%; disease-free survival [DFS], 31% vs 62%).
Although the study by Lowenberg et al12 would suggest that
intensification of DNR leads to superior CR rates with no difference
in toxicity, the use of high-dose DNR by the French Cooperative
CHALLENGES IN ACUTE MYELOID LEUKEMIA
62 American Society of Hematology

7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 2/8
Group in ALFA (Acute Leukemia French Association)-9801 did not
demonstrate similar results.13 In their study, DNR at 80 mg/m2 /day
was compared with standard or high-dose idarubicin (IDA) during
induction therapy of patients ages 50 to 70. Neither high-dose DNR
nor high-dose IDA demonstrated any clinically relevant superiority
over standard dose IDA in this population of patients. Multivariate
analysis revealed age Ͼ 60 orϽ 60 to be of prognostic significance
for OS, but not for CR or EFS. WBCs and cytogenetics significantly
influenced EFS and OS in multivariate analysis. Although the
superiority of higher dose anthracycline as induction is not clearly
established by these trials, they do demonstrate that there is no
increased toxicity with these regimens. In addition, dose-reduced
anthracycline led to inferior CR rates in the Lowenberg study, and
survival was not as good in certain subgroups of patients. As such,
although there is no clear evidence that dose intensification is
needed, there does not seem to be any reason to attenuate doses of
anthracycline in patients over age 60. Doses of DNR at 60 mg/m2 or
IDA at 12 mg/ 2 for 3 days together with cytarabine would be
appropriate to use.
In the National Cancer Research Institute (NCRI) AML 14 trial,
randomizations were conducted of anthracycline dose and cytara-
bine dose in induction, the use of an MDR modulator (PSC 833) in
induction, and a number of postremission courses. 14 No benefit was
seen to any of the interventions tested. The PSC 833 arm was closed
prematurely because of an increased early death rate because of
infection. A randomized trial by the Eastern Cooperative Oncology
Group (ECOG) similarly showed no benefit to the addition of the
MDR modulator zosuquidar to induction therapy with DNR 45
mg/m2 and cytarabine.15 The question of whether the short infusion
time of zosuquidar in this study inadequately blocked the polyglyco-
protein pump has been raised by a subsequent study. 16 A review of
sequential SWOG studies that differed by the addition of cyclospo-
rine to DNR and cytarabine demonstrated that CR rates were the
same with and without cyclosporine (38% vs 44%), with a median
OS of 6 months versus 7 months and an RFS of 14 months versus 8
months.17 The lack of benefit of these agents suggests that they are
either not effective at inhibiting MDR or that MDR inhibition, even
if effective, cannot overcome the drug resistance.
Clofarabine, an agent that was initially approved for use with
patients with acute lymphoblastic leukemia, has recently been
studied in patients with relapsed and refractory AML, as well as
untreated elderly patients with AML.18-20 Results of phase II trials
are encouraging. The upcoming phase III ECOG trial for elderly
patients with AML will randomize patients to induction therapy
with DNR and cytarabine versus single-agent clofarabine.
Once CR has been obtained, there is no standard postremission
strategy in these patients. No prospective randomized study has ever
established the benefit of postremission therapy in older adults;
however, all large studies of AML have included postremission
therapy, presumably because of the concern that patients are all
destined to relapse without postremission therapy. Cycles of
high-dose cytarabine, which is felt to be of benefit in younger
patients, has not been demonstrated to be of benefit in this age group
and is thought to be too toxic.21 Single cycles of high-dose
cytarabine have, however, been well tolerated in cooperative group
studies.13,22 Recent studies of gemtuzumab, as well as studies of
interleukin-2 as postremission therapy, have not demonstrated any
benefit.23,24 In the EORTC-GIMEMA (European Organization for
Research and Treatment of Cancer-Gruppo Italiano Malattie eMatologiche dell’Adulto) AML 13 trial, in which postremission
therapy was randomized between two cycles of intensive intrave-
nous therapy versus oral therapy, no difference in DFS was
demonstrable between the two groups.25,26 The median DFS was 9
months for the noninfusional therapy versus 10.4 months for the
intravenous regimen and 3-year DFS 13 versus 21% ( P ϭ .15).
Although no OS benefit was seen, the only patients who enjoyed
prolonged DFS had received postremission chemotherapy. This
study also offered autologous hematopoetic stem cell transplant
(HSCT) as a postremission therapy, and no benefit was demon-
strated to HSCT.23 Of the 61 patients with AML in CR in this study
who underwent stem cell harvest after first consolidation, 33 of 61
patients had HSCT with a median 3-year OS of 39% and a DFS of
28% for the 33 patients who underwent HSCT and a DFS of 21% forthe 61 patients who underwent stem cell harvest.
Although randomized trials have not been done to unequivocally
establish the need for consolidation therapy, randomized trials have
Table 1. Patientand disease characteristics at presentation of AML, by
age
<56 years 56-65 66-75 >75 year
PS 0 (%) 35 29 27 18
PS<2 (%) 84 75 73 68
PS >2 (%) 2 10 7 14
FavorableKaryotype (%)
16 5 5 4
IntermediateKaryotype (%)
45 55 55 44
Unfavorable
Karyotype (%)
33 38 39 50
MDR+ (%) 33 62 61 57
MDR indicates multidrug resistance. Adapted fromAppelbaum et al.7
Table 2. Intensive regimens for elderly AML
Study
Age (range)
Number
Induction and postremission treatment
regimens and randomizations
CR
ED
Survival
HOVON12,23
67(60-83)
N=813
INDUCTION
Ara-C 200 + DNR (45 vs 90)
Followed by
Ara-C 1000 mg/ m2 x 6 days
POSTREMISSION
Allogeneic HSCT or
GO x 3 cycles or No further treatment
CR
54% vs 64%
ED
12% vs 11%
2 yr DFS 30%
ALFA-980113
60 (50-70)
N=478
INDUCTION
DNR 80 x3d vs. IDA 12 x 3d vs 4d + Ara-C
+/- followed by
MTZ + Ara-C
POSTREMISSION
Ara-C 1 g/ m2 q 12 h x 4 d + induction
anthracycline x 2d +/- IL-2
CR
70% vs 83% vs 78%
ED
8% vs 3% vs 6%
OS 17 mo.
2 yr EFS 23.5%
2 yr OS 38%
AML14 14
67(44-88)
N=1273
INDUCTION
DAT x 2 courses +/- PSC-833
(Ara-C 100 vs 200 mg/m2/day)
POSTREMISSION
MTZ + Ara-C
+/- followed by ICE
54% CR
18% ED
5 yr DFS 13%
ALFA 9803 28
72(65-85)
N=429
INDUCTION
DNR45 or IDA 9 x 4 d + Ara-C
+/- followed by
MTZ + Ara-C
POSTREMISSION
Ara-C 60 mg/ m2 q 12 h x 5 day + anthracycline x
1 d, monthly x 6mo vs
Ara-C 200 mg/ m2 x 7d + anthracycline x 4 d
57% CR
10% ED
OS 12 mo
2 yr OS 27%
4 yr OS 12%
AML HD98-B 29
65(61-78)
N=329
INDUCTION
IDA 12 + Ara-C x 2 cycles +/- ATRA
POSTREMISSION
Ara-C + MTZ + IE(IV) vs oral IE (po)
q mo x 12 mo
46% CR
OS 22.3 mo(IEiv) vs 14.3
mo (IEpo)
4 yr OS 24%
AML-1326
67(61-80)
n=757
INDUCTION
MICE x 1-2 cycles
+/- GCSF
POSTREMISSION
mini-ICE (IV) vs Infusional mini-ICE
x 2 cycles vs 1 cycle +HSCT
57% CR
DFS 1 yr
3 yr DFS 21%
3 yr OS 32%
HOVON indicates Stichting Hemato-Oncologie voor Volwassenen Nederland; ED,
early death; Ara-C, cytarabine; GO, gemtuzumab ozogamicin; MTZ, mitoxantrone;
IL-2, interleukin-2; DAT, daunorubicin, cytarabine, 6-thioguanine; ATRA, tretinoin;
ICE, idarubicin, cytarabine, etoposide; IE, idarubicin, etoposide; MICE, mitox-
antrone, etoposide, cytarabine.
Hematology 2010 63

7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 3/8
evaluated duration and types of postremission therapy. The AML 11
trial demonstrated that there was no benefit when four cycles, rather
than 1 cycle, of moderate intensity postremission therapy were given.27
In the ALFA 9803 trial comparing a cycle of intensive consolidation
versus 6 months of lower dose therapy, prolonged consolidation was
associated with improved OS (56% vs 37%) and DFS (28% vs 17%).28
Repeated courses of low-intensity chemotherapy were also associated
with shorter hospitalization and fewer transfusions. Age, AML type,
and cytogenetics were associated with longer DFS. In the AML HD98
study, in which patients who achieved a CR and after one intensiveconsolidation were randomized to either a second intensive consolida-
tion with IDA/etoposide or mild oral maintenance with the same drugs,
there was a lower relapse rate and superior survival in the group that
received the more intensive therapy (median survival 22.3 vs 14.3
months).29 In addition to supporting the use of high-dose consolidation,
this study suggests that more than one cycle of consolidation was
superior when this regimen was used. Like other studies in the elderly,
only 29% of the initial patient cohort was randomized after first
consolidation. Moreover, only 2 of 96 randomized patients had
high-risk cytogenetics, highlighting the selection bias in many of these
trials. One of the other major issues for studies of postconsoldation is
that many patients do not receive their assigned therapy, making the
trials difficult to interpret. Until there is a randomized trial demonstrat-
ing that there is no benefit to postremission therapy, I feel that it should
be offered to those patients who achieve a CR and are able to tolerate it.
Recent analyses have further tried to elucidate the prognostic
importance of cytogenetics and molecular prognostic factors in
elderly patients. As in younger patients, core binding factor
abnormalities have a more favorable prognosis. In a retrospective
French study of 147 patients who received at least one dose of
induction chemotherapy, 60 had t(8;21) and 87 had inversion (16).
There was an 88% CR rate and a 10% 8-week early death rate. 30
With a median follow-up of 48 months, the 5-year probability of OS
and leukemia-free survival (LFS) was 31% and 27%, respectively.
On multivariate analysis, high WBC count, poor PS, and del(9q)
were of negative impact, and trisomy 22 and intensive consolida-
tion—when compared with maintenance therapy—were of positive
impact. Despite a CR rate of 88%, median LFS was only 18 months.
In the t(8;21) group, the difference in survival following intensive
consolidation was statistically significant when compared with
maintenance (not yet reached vs 10 months). In a recent analysis of
the impact of NPM1 (nucleophosmin) mutation in elderly patients
in 148 patients Ն 60 years of age, with de novo cytogenetically
normal AML enrolled onto CALGB (Cancer and Leukemia Group
B) 9720 and 10201, those patients with NPM1 mutations have a
higher CR (84 vs 48) and longer 3-year DFS (DFS 23 vs 10) and OS
(35 vs 8). In multivariate analysis, this was particularly true in
patientsՆ 70 years of age (CR 87% vs 39%, DFS 30% vs 7%, and
OS 49% vs 5%). Several investigators have suggested that, in
determining therapy for older patients with AML, it would be
appropriate to wait for results of cytogenetic and perhaps molecular
studies before discussing therapeutic options.31
Overall, these studies demonstrate that results of intensive therapy
in elderly patients remain poor. Although CR rates of 40% to 80%
can be achieved, in highly selected populations, long-term survival
is poor. Even in patients with favorable cytogenetics who have 80%
CR rates, relapse rates are high. As such, novel strategies are
needed. With the use of reduced-intensity conditioning regimens,
allogeneic transplantation has become a valid option. Recent reports
have suggested that age, at least up to 70, does not impact outcome
of reduced-intensity transplant and that reduced intensity transplan-
tation may yield better outcomes than chemotherapy in patients
aged 60 to 70. Retrospective registry studies have demonstrated that
age does not appear to be a factor in transplant outcome. In a
retrospective analysis of 629 reduced-intensity allogeneic trans-
plants reported to the French transplant registry, outcomes (OS,
transplant-related mortality, and acute graft-versus-host disease
[GVHD]) in patients over age 65 were comparable with those for
patients who were between ages 60 and 65.32 Two-year OS was 48%
vs 47% for the two age groups. Similarly, data from the Center for
International Blood and Marrow Transplant Research (CIBMTR)on 1080 patients undergoing reduced-intensity conditioning trans-
plant for AML or myelodysplastic syndrome (MDS) demonstrated
no difference in nonrelapse mortality, grade 2 to 4 GVHD, chronic
GVHD, or relapse, when patients ages 60 to 64 or over age 65 were
compared with patients aged 40 to 59.33 Although 2-year survival
rates were lower in patients over age 60, 2-year survival rates were
greater than 30% in all age groups, and multivariate analysis
revealed no significant impact of age on DFS or OS. In a prospective
study of the feasibility of transplant in patients over age 50 at M.D.
Anderson who entered CR, outcome for those patients who
underwent an allogeneic transplant with reduced-intensity condition-
ing had a superior RFS and OS when compared with those who
received postremission chemotherapy.34 A retrospective analysis of
over 1,000 elderly patients with AML in first CR who underwentHSCT or chemotherapy demonstrated improved OS and DFS in the
HSCT group.35 Further prospective studies are needed.
Who Should Not Receive Intensive Therapy?Selection criteria commonly used for inclusion into clinical studies
have a major impact on reported outcome. Furthermore, the
interpretation of clinical trials must be done with caution, in that not
only are eligibility criteria different, but also investigator choice and
patient preference clearly influence patient inclusion. In an analysis
by the Swedish of 9729 patients diagnosed with AML in Sweden
since 1973, the proportion of older patients who were considered
eligible for intensive remission induction therapy decreased from
92% in those aged 60 to 64 years to 80%, 67%, 45%, 23%, and 4%
in those aged 65 to 69, 70 to 74, 75 to 79, 80 to 84, and 85ϩ years,
respectively.2 Importantly, this report found that early death rates
were improved with intensive treatment, compared with palliation
alone. This was seen in all age groups and all PS levels. For
example, within patients age 76 to 89, with a PS of Ͼ 2, those who
received intensive treatment had a 36% early death rate, compared
with 52% for those who received palliation alone. The assessment
of eligibility for intensive therapy is, however, quite subjective, and
the reason that certain patients within the cohort received intensive
therapy whereas others did not is not available in this report. An
analysis was done within the six Swedish health care regions among
patients age 70 to 79 years.2,36 Percentage of patients who were
deemed candidates for intensive therapy differed by region, prob-
ably because of physician and patient preferences, because baseline
characteristics of the patients seem no different. In those regions in
which only 40% of patients were felt to be eligible for intensive
therapy, there was a 16% early death rate with intensive treatment,
compared with 27% with palliation only. The early death rate was
similar in those regions wherein 75% of patients were felt to be
eligible for intensive treatment. When comparing regions where
only 40% versus 75% were treated intensively, CR rates with
intensive treatment were 41% and 49%, respectively, and CR rates
for the entire group in the region was 19% versus 37%. Given the
lower proportion of patients who received intensive therapy in those
regions, the 2-year OS was decreased at 24% versus 50% and 5-year
OS was 1% versus 13%. Furthermore, although PS is more
64 American Society of Hematology

7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 4/8
predictive for early death rate than age, long-term survival may be
achieved in patients with initial poor PS. Based on their report, they
state that standard intensive treatment decreased early death rates in
most patients up to age 80.
The MRC (Medical Research Council) AML 11 trial allowed for the
use of cytogenetic data to identify prognostic groups in older adults
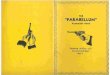
who were treated with intensive therapy on study.37 More recently,
investigators have become interested in developing tools to allow us
to discriminate between patients who are likely to benefit from
intensive chemotherapy versus those who should be candidates for
less aggressive therapy (Table 3).
Patients are now being considered “unfit for intensive therapy” and
more appropriate for alternative or investigational therapy if there is
either a high risk of early mortality or a poor chance of long-term
DFS. In a retrospective analysis by Wheatley of the patients in the
AML 11 trial, five risk factors were identified in AML patients that
were weighted according to the values of their multivariate coeffi-
cients and used to define three subgroup risk classifications that
were then able to be validated in the more recent MRC AML 14
trial.38 Cytogenetic group, age, WBC count, PS, and de novo vs
secondary AML were all found to be highly significant. Good,
standard, and poor risk groups had a 1-year survival of 53%, 43%,
and 16%, respectively (P Ͻ .0001). In a retrospective analysis by
Kantarjian et al39 of 998 patients aged 60 or older who received
intensive therapy at M.D. Anderson Cancer Center, a multivariate
analysis was performed to calculate a prognostic score. They
identified prognostic risk factors: age (Ն 75 years), unfavorable
cytogenetics, poor PS (Ͼ 2), Ն 12-month history of antecedent
hematologic disorder (AHD), lactate dehydrogenase (LDH) Ͼ 600,
elevated creatinine, and treatment outside a laminar flow room.
Three risk subgroups were defined based on the number of poor
prognostic factors. Those with none of the adverse risk factors have
an expected CR rate of Ͼ 60%, induction mortality of 10%, and
1-year survival over 50%. A poor risk group with more than or equal
to three poor prognostic risk factors had CR, induction mortality,
and 1-year survival rates of Ͻ 20%, Ͼ 50%, and Ͻ 10%, whereas
those in an intermediate risk group had rates of 50%, 30%, and 30%,
respectively. Several reports have focused on the impact of comor-
bidities on decision making in AML. A refined Hematopoetic Cell
Transplantation Comorbidity Index (HCTCI) has been found to be
useful in identifying patients who are not candidates for intensive
therapy.40 Malfuson et al41 analyzed 416 patients treated on the
ALFA 9803 multicenter trial to identify independent prognostic
factors that would impact on OS. Based on their analysis, theypropose that, in those patients with unfavorable cytogenetics and the
presence of two poor prognostic factors (age Ն 75 years, PS Ն 2,
and WBC count Ն 50 ϫ 109 /L), the OS is only 19% at 12 months,
and these patients should, therefore, not be considered for standard
chemotherapy.
In a recent analysis of the AML 96 trial of 909 patients with a
median age of 67, univariate and multivariate analyses identified
karyotype, NPM1 mutation status, WBC count, and LDH of
independent prognostic significance for OS, DFS, and relapse.42
Although favorable and poor cytogenetic risk groups had markedly
different OS, those patients with intermediate risk karyotype could
be subdivided based on CD34 expression, along with the abovemen-
tioned factors identified on multivariate analysis, allowing for thedesignation of four groups: (1) favorable cytogenetics, (2) interme-
diate cytogenetic with favorable features, (3) intermediate cytogenet-
ics with adverse risk features, and (4) poor risk cytogenetics, with
3-year OS of 39.5%, 30%, 10.6%, and 3.3%, respectively. These
scoring systems can be used to identify patients who are likely to
respond to standard therapy, as well as those who are not likely to
benefit and should therefore be considered for alternate or investiga-
tional therapy.
What Treatment Options Are Available for Patients
Who Are Not Candidates for Intensive Induction
Therapy?For those patients who are not considered to be candidates for
intensive induction therapy, one would hope to identify agents and
regimens that are more effective and less toxic to address the
concerns regarding early induction death, inadequate response rate,
and high risk of relapse. The NCRI AML 14 study was designed to
allow for randomization of patients between intensive and noninten-
sive therapy, but only eight patients agreed to randomization. 14,43 As
such, data available on novel agents comes from a variety of pilot
and phase II studies with differing eligibility criteria. When
evaluating the outcomes, it is important to also look at the
characteristics of patients who were ultimately enrolled. Table 4
reviews available data from some of these studies.
As part of the NCRI AML 14 study, 212 patients who were deemed
unfit for intensive treatment options by the local investigator were
randomized to receive supportive care alone with hydroxyurea or
cytarabine 20 mg twice daily by subcutaneous injection for 10 days
every 4 to 6 weeks.43 Outcome was improved for the low-dose (LD)
cytarabine arm when compared with supportive care with hydroxyu-
rea alone. CR was 18% versus 1%, and median survival was 575
days for those who achieved CR, compared with 66 days in
nonresponders. DFS for responders was 8 months. Survival benefit
was seen in all age groups, even those over age 75. As none of the
patients with adverse cytogenetics achieved a CR, no survival
benefit was, however, seen in that group. The early death rate was
39% at 8 weeks. Although no criteria were used to define unfit
patients, 78% were over age 70, 27% had secondary AML, 30% had
Table 3. Prognostic scoring in elderly AML
Prognostic Factors CR Rate (%) Early Death
Rate (%)
Overall Survival
Grimwade37
MRC
AML11trial
Cytogenetics
Good.:63
Standard: 53-63Poor:26
5yr (%)
Good:34
Standard :10-15
Poor : 2
Kantarjian39
MDACC
Age>=75
Karotype
ECOG PS>2
AHD >12 mo No laminar flow
Good.: >60
Standard: 50Poor: <20
Good 10
Standard:30
Poor: >50
1 yr. (%)
Good. :>50
Standard: 30
Poor: <10
LDH
Creatinine
Malfuson 41
ALFA
9803, n=418
Cytogenetics
Age>=75
PS>=2
WBC>=50X109/l
1yr (%)
Poor:19
Others: 58
Giles40
MDACCHematopoietic celltransplantation
comorbidity index
(HCTCI)
Good:64Standard:43
Poor:42
Good:3
Standard:11Poor:29
Good:45 wks
Standard:31wksPoor:19 wks
Wheatley 38
AML14
Cytogenetics
Age
WbcPS
De novovs
secondary AML
1/3 year OS(%)
Good: 60/29
Standard: 48/27Poor:30/9
Rollig42
AML 96CD34Wbc
Age
LDH NPM1
Cytogenetics
3 yrOS(%)
Good: 30-40Standard:10.6
Poor: 3.3
MDACCindicatesM.D. Anderson CancerCenter.
Hematology 2010 65
7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 5/8
PS Ն 2, 27% had heart disease, 49% had other comorbidities, and
59% had a poor risk score by the Wheatley Risk Index. 38 Based on
this study, LD cytarabine became the standard of care for the
treatment of patients felt to be unfit for intensive chemotherapy,
although one could argue that it should not be given to those with
poor risk cytogenetics.
The DNA methyltransferase inhibitors have been the subject of several
recent studies. In a multicenter phase II study of 55 patients over age 60
with untreated AML, decitabine was administered for 5 days monthly
until disease progression.44 With a median of three cycles, the overall
response rate was 24%, median survival was 7.7 months, and 30-day
mortality was 7%. Responses were seen in all cytogenetic risk groups,
as well as in those patients with prior MDS. An alternate schedule of
decitabine was reported by Blum et al.45,46 Patients received an initial
one totwo courses of 10days of decitabine, followed bya course over 3
to 5 days every 4 weeks for 1 year. Of the 53 patients with a median age
of 74, 36% had secondary AML, and 34% had a complex karyotype.
Eighteen patients had a HCTCI score of Ն 3. There was a 64%
response rate after a median of three cycles of therapy. CR occurred in
all subsets, regardless of age, karyotype, presenting WBC, and prior
AHD. One-year survival of poor risk patients was 30% (compared with
10% in patients with a similar Wheatley risk score in the AML 11
trial38).
In a study of azacitidine in AML with 20% to 30% blasts, patients
who were deemed unfit for standard induction chemotherapy were
randomized against either supportive care or LD cytarabine.47 OS
survival was superior in the azacitidine arm. There was a statisti-
cally significant difference seen in OS for patients with poor risk
cytogenetics in favor of azacitidine, compared with conventional
care regimens (12.3 vs 5.3 months, respectively, with 2-year OS of
38% vs 0%).
Gemtuzumab ozogamicin (GO) has been the subject of a recent
study by the EORTC and GIMEMA leukemia groups (AML 19).48
In this randomized multicenter study, 84 patients were randomized
to receive one of two schedules of GO at attenuated doses or best
supportive care. The proportion of patients either achieving a
response or maintaining stable disease was greater in patients who
receive GO at a dose of 6 mg/m2 on day 1 and 3 mg/m2 on day 8,
when compared with a schedule of GO 3 mg/m 2 on days 1, 3, and 5
(63% vs 38%, respectively). Results of the comparison with patients
who were randomized to standard care are not yet available, and a
phase III trial is ongoing.
Clofarabine has been studied as an agent in elderly patients withAML. In a phase II study of the agent in 112 patients over age 60
with untreated AML with at least one unfavorable baseline prognos-
tic factor, there was a 46% response rate.49 The median age of the
patients was 71. Twenty-two percent of patients had a baseline PS of
2, 47% had a prior hematologic disorder (AHD) or secondary AML,
55% had an unfavorable karyotype, and 62% were Ն age 70.
Overall response rate (ORR) was 395 for patients Ն 70, 32% for PS
2, 51% for patients with AHD, 54% for intermediate karyotype and
42% for unfavorable karyotype, and 38% for patients with three risk
factors. Median DFS was 37 weeks, and median OS was 41 weeks
for all patients, 59 weeks for patients with CR/complete remission
with incomplete platelet recovery (CRp), and 72 weeks for patients
with CR. Early death rate (within 60 days) was 16%.
In two consecutive European studies of 106 untreated older patients
with AML who were considered unfit for chemotherapy, partici-
pants were given four to six 5-day courses of clofarabine. 18,50 In the
UWCM (University of Wales College of Medicine)-001 study,
patients who were either over age 70 (68%) or over age 60, with a
PS of 2 or cardiac comorbidity, were treated with clofarabine for 5
days every 28 days for 2 to 4 courses. In the BIOV-121 study,
patients were treated for 5 days every 4 to 6 weeks for up to six
courses. All patients were age Ն 65 and deemed unfit for chemo-
therapy. Overall, 36% of patients had a PS Ն 2, 30% had adverse
risk cytogenetics, 46% had Wheatley poor risk disease, and 65%
were age Ն 70. The ORR was 48%, and the median OS was 19
weeks for all and 45 weeks for those who attained a CR/complete
remission with incomplete blood count recovery (CRi). Responses
were seen in patients with adverse cytogenetics (44% ORR),
patients with secondary AML (31%), and patients age Ն 70 (49%).
The death rate within 30 days was 18%.
A novel agent, laromustine (VNP40101M), a sulfonylhydrazine alky-
lating agent, has been studied in 85 patients with poor risk AML ageՆ
60 years.51 Patients received one to two cycles of laromustine at a dose
of 600 mg/m2, followed by one cycle of cytarabine. Seventy-eight
percent of patients were age Ն 70, 47% had an adverse karytype, 41%
had a PS of 2, 77% had pulmonary disease, 73% had cardiac disease,
and 3% had hepatic disease. All patients with unfavorable karyotype or
ECOG PS had at least one other risk factor at the time of enrollment.
Seventy-five percent of patients had Ն 3 risk factors. The ORR was
32% and was similar in patients over age 70 (32%), with a PS of 2
(32%), with baseline pulmonary or cardiac dysfunction (27%–34%).
There was a 14% 30-day mortality. OS was 3.2 months (12.4 months
for those with CR/CRp), and 1-year survival was 21% (52% for those
with CR/CRp).
These phase II studies are encouraging, in that responses are seen in
all poor risk categories, and early death rates are acceptable.
Randomized trials are needed. Although randomized trials of
intensive versus nonintensive therapy have not been successful, the
ongoing AML 16 trial was designed to randomize patients who are
considered not fit for intensive treatment to LD cytarabine versus
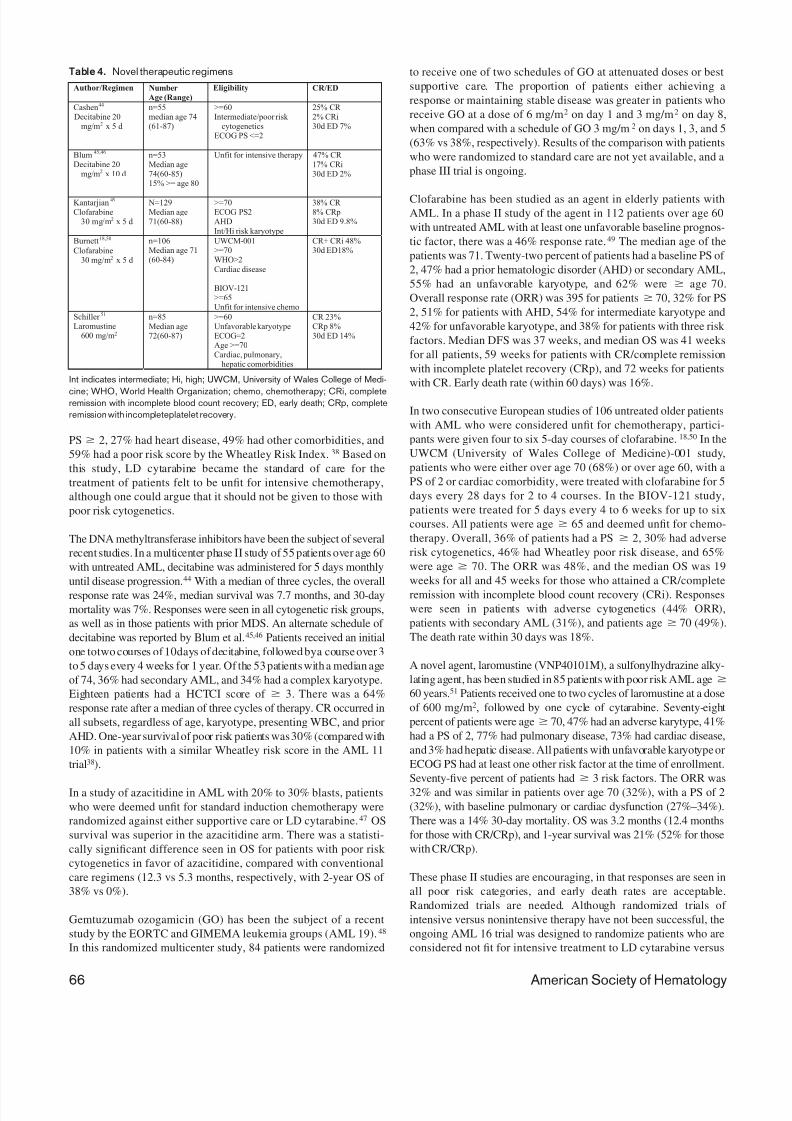
Table 4. Novel therapeutic regimens
Author/Regimen Number
Age (Range)
Eligibility CR/ED
Cashen44
Decitabine 20mg/m2 x 5 d
n=55median age 74(61-87)
>=60Intermediate/poor risk
cytogeneticsECOG PS <=2
25% CR 2% CRi30d ED 7%
Blum45,46
Decitabine 20mg/m2 x 10 d
n=53Median age74(60-85)15% >= age 80
Unfit for intensive therapy 47% CR 17% CRi30d ED 2%
Kantarjian49
Clofarabine30 mg/m2 x 5 d
N=129Median age71(60-88)
>=70ECOG PS2AHD
Int/Hi risk karyotype
38% CR 8% CRp30d ED 9.8%
Burnett18,50
Clofarabine30 mg/m2 x 5 d
n=106Median age 71(60-84)
UWCM-001>=70WHO>2
Cardiac disease
BIOV-121>=65Unfit for intensive chemo
CR+ CRi 48%30d ED18%
Schiller 51
Laromustine600 mg/m2
n=85
Median age72(60-87)
>=60Unfavorable karyotypeECOG=2Age >=70Cardiac, pulmonary,
hepatic comorbidities
CR 23%CRp 8%30d ED 14%
Int indicates intermediate; Hi, high; UWCM, University of Wales College of Medi-
cine; WHO, World Health Organization; chemo, chemotherapy; CRi, completeremission with incomplete blood count recovery; ED, early death; CRp, complete
remission with incompleteplatelet recovery.
66 American Society of Hematology

7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 6/8
LD cytarabine with GO, LD cytarabine with arsenic trioxide or
tipifarnib, or LD clofarabine.52 The arsenic arm has been closed
because of ineffectiveness with CR/CRi of 29%, compared with
24% and a 12-month OS of 27%, compared with 41%. The other
arms continue to accrue patients.
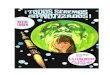
Approach to the Elderly Patient With AMLAML is a disease of the elderly, with the majority of patients over age
60. As our population ages, that percentage will only increase.
Unfortunately, the standard regimens that are successful in treating
younger patients will AML are not as beneficial in the majority of older
patients with the disease. Figure 1 outlines my approach to the elderly
patient with AML. Understanding of the disease biology, as well as the
prognostic factors associated with the host, allows us to betterdetermine which patients are likely to benefit from standard therapy
and which require alternative approaches. Objective scoring systems
are being developed that allow us to define patients unfit for intensive
chemotherapy on the basis of increased risk of induction death, low
response rate, and/or low long-term DFS. Optimal induction and
postremission therapy for patients appropriate for intensive therapy
have yet to be defined, again, because results are not satisfactory with
our current regimens, even in those patients who do not have definable
poor prognostic factors. When compared with young patients with
similar disease-related features, outcomes are inferior. For patients who
are not candidates for intensive therapy because of comorbid condi-
tions, low-intensity therapies appear to be superior to palliative care
alone. Whenever possible, patients should be enrolled in clinical trials
that will allow us to address these issues.
DisclosuresConflict-of-interest disclosure: The author declares no competing
financial interests.
Off-label drug use: Use of gemtuzumab ozogamicin, clofarabine,
and decitabine.
CorrespondenceSelina M. Luger, MD, Professor of Medicine, and Director,
Leukemia Program, Hospital of the University of Pennsylvania,
Perelman Center for Advanced Medicine, 3400 Civic Center Blvd.,
Philadelphia, PA 19104; Phone: (215) 614-1847; Fax: (215) 615-
5888; e-mail: [email protected]
References1. Surveillance Epidemiology and End Results (SEER) Program.
Limited use-data (1973–2004). National Cancer Institute D,
Surveillance Research Program, Cancer Statistics Branch.
SEER Web site. http:// www.seer.cancer.gov. Accessed April
2007.
2. Juliusson G, Antunovic P, Derolf A, et al. Age and acute
myeloid leukemia: real world data on decision to treat and
outcomes from the Swedish Acute Leukemia Registry. Blood .
2009;113:4179– 4187.
3. Pulte D, Gondos A, Brenner H, Pulte D, Gondos A, Brenner H.
Improvements in survival of adults diagnosed with acute
myeloblastic leukemia in the early 21st century. Haemato-
logica. 2008;93:594– 600.
4. Buchner T, Berdel WE, Haferlach C, et al. Age-related risk
profile and chemotherapy dose response in acute myeloid
leukemia: a study by the German Acute Myeloid Leukemia
Cooperative Group. J Clin Oncol. 2009;27:61–69.
5. Lerch E, Espeli V, Zucca E, et al. Prognosis of acute myeloid
leukemia in the general population: data from southern Switzer-
land. Tumori. 2009;95:303–310.
6. Alibhai SM, Leach M, Minden MD, et al. Outcomes and quality
of care in acute myeloid leukemia over 40 years. Cancer .2009;115:2903–2911.
7. Appelbaum F, Gundacker H, Head DR, et al. Age and acute
myeloid leukemia. Blood . 2006;107:3481–3485.
8. Rao AV, Valk PJ, Metzeler KH, et al. Age-specific differences
in oncogenic pathway dysregulation and anthracycline sensitiv-
ity in patients with acute myeloid leukemia. J Clin Oncol.
2009;27:5580–5586.
9. Appelbaum FR, Baer MR, Carabasi MH, et al. NCCN practice
guidelines for acute myelogenous leukemia. Oncology. 2000;14:
53–61.
10. Dohner H, Estey EH, Amadori S, et al. Diagnosis and
Non-M3 AML
Age > 80 Age 60-79
Poor PS, comorbidities, unfavorable
karyotype+ poor prognostic factors
Good PS, good /intermediate karyotype
Clinical trial/low intensity therapy
Clinical trial for all patients preferable
Induction therapy with standard dose anthracycine and
cytarabine
Postremission therapy with 1 or 2 cycles of
intermediate or high dose cytarabine containing regimen
Complete Remission
Consideration of RIC transplant
Figure 1. My approach to the patient over age 60 with AML.
Hematology 2010 67

7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 7/8
management of acute myeloid leukemia in adults: recommenda-
tions from an international expert panel, on behalf of the
European LeukemiaNet. Blood . 2010;115:453– 474.
11. Morra E, Barosi G, Bosi A, et al. Clinical management of
primary non-acute promyelocytic leukemia acute myeloid
leukemia: Practice Guidelines by the Italian Society of Hematol-
ogy, the Italian Society of Experimental Hematology, and the
Italian Group for Bone Marrow Transplantation. Haemato-
logica. 2009;94:102–112.
12. Lowenberg B, Ossenkoppele GJ, van Putten W, et al. High-dose daunorubicin in older patients with acute myeloid leuke-
mia. N Engl J Med . 2009;361:1235–1248.
13. Pautas C, Merabet F, Thomas X, et al. Randomized study of
intensified anthracycline doses for induction and recombinant
interleukin-2 for maintenance in patients with acute myeloid
leukemia age 50 to 70 years: results of the ALFA-9801 study.
J Clin Oncol. 2010;28:808– 814.
14. Burnett AK, Milligan D, Goldstone A, et al. The impact of dose
escalation and resistance modulation in older patients with
acute myeloid leukaemia and high risk myelodysplastic syn-
drome: the results of the LRF AML 14 trial. Br J Haematol.
2009;145:318–332.
15. Cripe LD, Uno H, Paietta EM, et al. Zosuquidar, a novel
modulator of P-glycoprotein, does not improve the outcome of
older patients with newly diagnosed acute myeloid leukemia: a
randomized, placebo-controlled, trial of the Eastern Coopera-
tive Oncology Group (ECOG 3999). Blood . 2010 Aug 17.
[Epub ahead of print]
16. Lancet J, Gotlib J, Wetzler M, et al. Phase I/II study of the
P-glycoprotein (Pgp) inhibitor zosuquidar administered by
continuous infusion (CIV) with daunorubicin (DNR) and
cytarabine (ARA-C) as primary therapy in older patients with
Pgp-positive acute myeloid leukemia (AML) [abstract]. Blood .
2007;110.
17. Chauncey TR, Gundacker H, Shadman M, et al. Sequential
phase II Southwest Oncology Group studies (S0112 and S0301)
of daunorubicin and cytarabine by continuous infusion, without
and with ciclosporin, in older patients with previously untreated
acute myeloid leukaemia. Br J Haematol. 2009;148:48 –58.
18. Burnett A, Russell N, Kell J, et al. European development of
clofarabine as treatment for older patients with acute myeloid
leukemia considered unsuitable for intensive chemotherapy
[abstract]. J Clin Oncol. 2010;28.
19. Faderl S, Erba HP, Claxton DF, et al. Clofarabine produces
durable remissions in older patients with AML with unfavor-
able prognostic factors and multiple comorbidities [abstract
4155]. Blood . 2009;114.
20. Faderl S, Ravandi F, Huang X, et al. A randomized study of
clofarabine versus clofarabine plus low-dose cytarabine as
front-line therapy for patients aged 60 years and older with
acute myeloid leukemia and high-risk myelodysplastic syn-
drome. Blood . 2008;112:1638 –1645.
21. Mayer RJ, Davis RB, Schiffer CA, et al. Intensive postremis-
sion chemotherapy in adults with acute myeloid leukemia.
N Engl J Med . 1994;331:896 –903.
22. Rowe JM, Neuberg D, Friedenberg W, et al. A phase 3 study of
three induction regimens and of priming with GM-CSF in older
adults with acute myeloid leukemia. A trial by the Eastern
Cooperataive Oncology Group. Blood . 2004;103:479– 485.
23. Lowenberg B, Beck J, Graux C, et al. Gemtuzumab ozogamicin
as postremission treatment in AML at 60 years of age or more:
results of a multicenter phase 3 study. Blood . 2010;115:2586–
2591.
24. Baer MR, George SL, Caligiuri MA, et al. Low-dose interleu-
kin-2 immunotherapy does not improve outcome of patients
age 60 years and older with acute myeloid leukemia in first
complete remission: Cancer and Leukemia Group B Study
9720. J Clin Oncol. 2008;26:4934– 4939.
25. Jehn U, Suciu S, Thomas X, et al. Non-infusional vs intrave-
nous consolidation chemotherapy in elderly patients with acute
myeloid leukemia: final results of the EORTC-GIMEMA
AML-13 randomized phase III trial. Leukemia. 2006;20:1723–
1730.26. Thomas X, Suciu S, Rio B, et al. Autologous stem cell
transplantation after complete remission and first consolidation
in acute myeloid leukemia patients aged 61–70 years: results of
the prospective EORTC-GIMEMA AML-13 study. Haemato-
logica. 2007;92:389 –396.
27. Goldstone A, Burnett A, Wheatley K, Smith AG, Hutchinson
M, Clark R. Attemps to improve treatment outcomes in acute
myeloid leukemia (AML) in older patients: the results of the
United Kingdon Medical Research Council AML11 trial.
Blood . 2001;98:1302–1311.
28. Gardin C, Turlure P, Fagot T, et al. Postremission treatment of
elderly patients with acute myeloid leukemia in first complete
remission after intensive induction chemotherapy: results of the
multicenter randomized Acute Leukemia French Association
(ALFA) 9803 trial. Blood . 2007;109:5129 –5135.
29. Schlenk RF, Frohling S, Hartmann F, et al. Intensive consolida-
tion versus oral maintenance therapy in patients 61 years or
older with acute myeloid leukemia in first remission: results of
second randomization of the AML HD98-B treatment trial.
Leukemia. 2006;20:748–750.
30. Prebet T, Boissel N, Reutenauer S, et al. Acute myeloid
leukemia with translocation (8;21) or inversion (16) in elderly
patients treated with conventional chemotherapy: a collabora-
tive study of the French CBF-AML intergroup. J Clin Oncol.
2009;27:4747–4753.
31. Sekeres MA, Elson P, Kalaycio ME, et al. Time from diagnosis
to treatment initiation predicts survival in younger, but not
older, acute myeloid leukemia patients. Blood . 2009;113:28–
36.
32. Chevallier P, Blaise D, Milpied N, et al. Reduced intensity
conditioning (RIC) allogeneic stem cell transplantation for
patients agedϾϭ60 years: a retrospective study of 629 patients
from the Societe Francaise De Greffe De Moelle et de therapie
cellulaire (SFGM-TC). Blood . 2009;114:84– 85.
33. Rollig C, Thiede C, Gramatzki M, et al. A novel prognostic
model in elderly patients with acute myeloid leukemia: results
of 909 patients entered into the prospective AML96 trial.
Blood . 2010;116:971–978.
34. Estey E, de Lima M, Tibes R, et al. Prospective feasibility
analysis of reduced-intensity conditioning (RIC) regimens for
hematopoietic stem cell transplantation (HSCT) in elderly
patients with acute myeloid leukemia (AML) and high-risk
myelodysplastic syndrome (MDS). Blood . 2007;109:1395–
1400.
35. Kurosawa S, Yamaguchi T, Uchida N, et al. Comparison of
allogeneic hematopoietic cell transplantation and chemo-
therapy as post-remission strategy in elderly patients with
non-M3 AML in CR1: retrospective analysis with 1036 patients
[abstract 524]. Blood . 2009;114.
36. Juliusson G, Billstrom R, Gruber A, et al. Attitude towards
remission induction for elderly patients with acute myeloid
leukemia influences survival. Leukemia. 2006;20:42– 47.
37. Grimwade D, Walker H, Harrison G, et al. The predictive value
68 American Society of Hematology

7/30/2019 Hematology 2010 Luger 62 9
http://slidepdf.com/reader/full/hematology-2010-luger-62-9 8/8
of hierarchical cytogenetic classification in older adults with
acute myeloid leukemia (AML): analysis of 1065 patients
entered into the United Kingdom Medical Research Council
AML11 trial. Blood . 2001;98:1312–1320.
38. Wheatley K, Brookes CL, Howman AJ, et al. Prognostic factor
analysis of the survival of elderly patients with AML in the
MRC AML11and LRF AML14 trials. Br J Haematol. 2009;145:
598–605.
39. Kantarjian H, O’Brien S, Cortes J, et al. Results of intensive
chemotherapy in 998 patients age 65 years or older with acutemyeloid leukemia or high-risk myelodysplastic syndrome:
predictive prognostic models for outcome. Cancer . 2006;106:
1090–1098.
40. Giles FJ, Borthakur G, Ravandi F, et al. The haematopoietic
cell transplantation comorbidity index score is predictive of
early death and survival in patients over 60 years of age
receiving induction therapy for acute myeloid leukaemia. Br J
Haematol. 2007;136:624– 627.
41. Malfuson JV, Etienne A, Turlure P, et al. Risk factors and
decision criteria for intensive chemotherapy in older patients
with acute myeloid leukemia. Haematologica. 2008;93:1806–
1813.
42. Rollig C, Aulitzky WE, Bodenstein H, et al. Risk stratification
and prognostic factors in elderly AML patients—updatedresults of 909 patients entered into the prospective AML96 trial
[abstract 329]. Blood . 2009;114.
43. Burnett AK, Milligan D, Prentice AG, et al. A comparison of
low-dose cytarabine and hydroxyurea with or without all-trans
retinoic acid for acute myeloid leukemia and high-risk myelo-
dysplastic syndrome in patients not considered fit for intensive
treatment. Cancer . 2007;109:1114 –1124.
44. Cashen AF, Schiller GJ, O’Donnell MR, et al. Multicenter,
phase II study of decitabine for the first-line treatment of older
patients with acute myeloid leukemia. J Clin Oncol. 2010;28:
556–561.
45. Blum W, Garzon R, Klisovic RB, et al. Clinical response and
miR-29b predictive significance in older AML patients treated
with a 10-day schedule of decitabine. Proc Natl Acad Sci U S A.
2010;107:7473–7478.
46. Blum W, Klisovic R, Liu S, et al. Preliminary results of a phase
II study of low dose decitabine as a single agent in older
patients (age Ͼϭ60) with previously untreated acute myeloid
leukemia (AML) [abstract 2957]. Blood . 2008;112.
47. Fenaux P, Mufti GJ, Hellstrom-Lindberg E, et al. Azacitidine
prolongs overall survival compared with conventional careregimens in elderly patients with low bone marrow blast count
acute myeloid leukemia. J Clin Oncol. 2010;28:562–569.
48. Amadori S, Suciu S, Selleslag D, et al. Randomized trial of two
schedules of low-dose gemtuzumab ozogamicin as induction
monotherapy for newly diagnosed acute myeloid leukaemia in
older patients not considered candidates for intensive chemo-
therapy. (A phase II study of the EORTC and GIMEMEA
leukaemia groups (AML-19).) Br J Haematol. 2010;149:376–
382.
49. Kantarjian HM, Erba HP, Claxton D, et al. Phase II study of
clofarabine monotherapy in previously untreated older adults
with acute myeloid leukemia and unfavorable prognostic
factors. J Clin Oncol. 2010;28:549 –555.
50. Burnett AK, Baccarani M, Johnson P, et al. A phase II study(biov-121) of clofarabine monotherapy first line in patients
aged 65 years or older with acute myeloid leukemia for whom
standard intensive chemotherapy is not considered suitable
[abstract 425]. Blood . 2006;108.
51. Schiller GJ, O’Brien SM, Pigneux A, et al. Single-agent
laromustine, a novel alkylating agent, has significant activity in
older patients with previously untreated poor-risk acute my-
eloid leukemia. J Clin Oncol. 2010;28:815–821.
52. Russell NH, Hills RK, Hunter AE, et al. Low dose ara-C versus
low dose ara-C and arsenic trioxide: the UK NCRI AML16
“pick a winner” comparison [abstract 486]. Blood . 2009;114.
Hematology 2010 69