Embed Size (px)
Citation preview
Cynthia Perettie | Global Hematology Franchise Head
David Traub | Lifecycle Leader anti-CD20 Franchise
Pharmaceuticals Division
Roche Pharma Day 2015
Hematology franchise overview
DLBCL FL CLL
AML/MDS MM Hemophilia
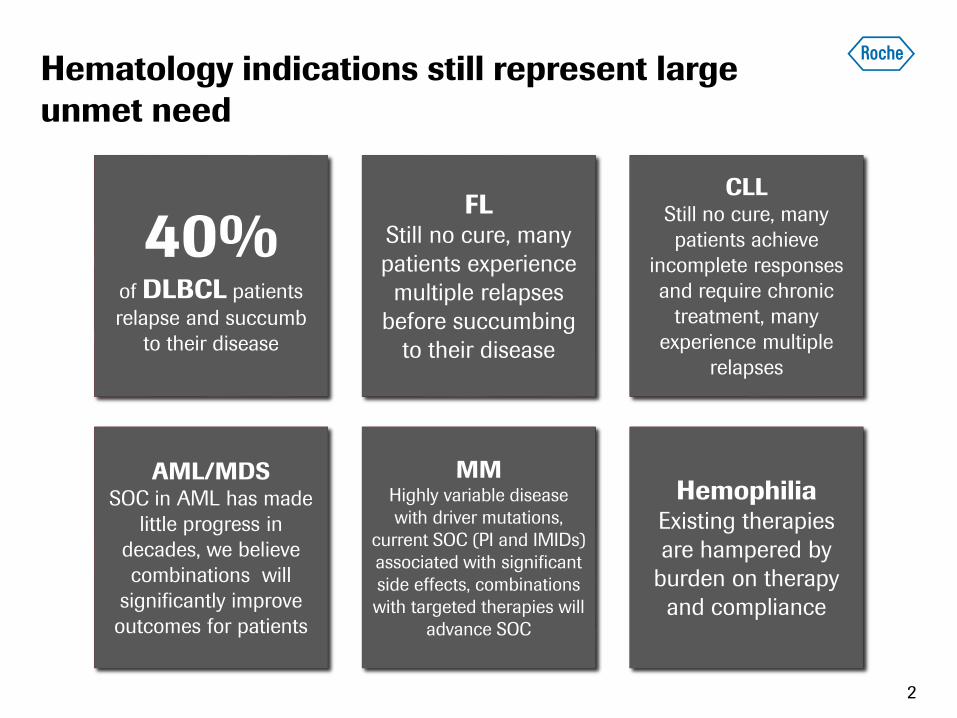
40% of DLBCL patients
relapse and succumb
to their disease
FL Still no cure, many
patients experience
multiple relapses
before succumbing
to their disease
CLL
Still no cure, many
patients achieve
incomplete responses
and require chronic
treatment, many
experience multiple
relapses
AML/MDS
SOC in AML has made
little progress in
decades, we believe
combinations will
significantly improve
outcomes for patients
MM
Highly variable disease
with driver mutations,
current SOC (PI and IMIDs)
associated with significant
side effects, combinations
with targeted therapies will
advance SOC
Hemophilia Existing therapies
are hampered by
burden on therapy
and compliance
Hematology indications still represent large
unmet need
2
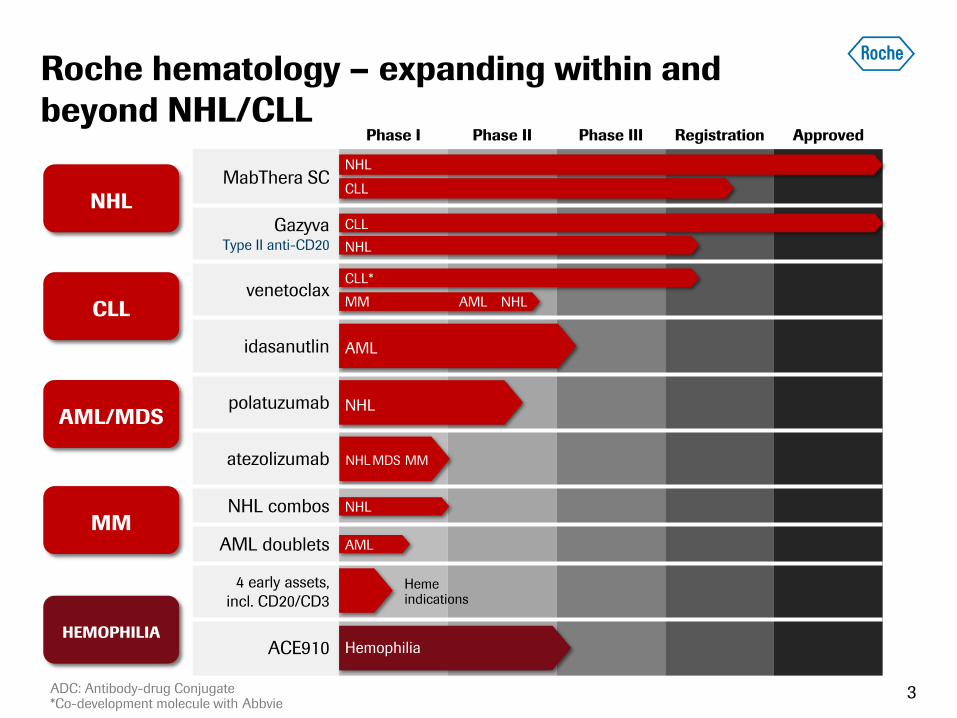
Phase I Phase II Phase III Registration Approved
MabThera SC
Gazyva Type II anti-CD20
venetoclax
idasanutlin
polatuzumab
atezolizumab
NHL combos
AML doublets
4 early assets,
incl. CD20/CD3
ACE910
Roche hematology – expanding within and
beyond NHL/CLL
ADC: Antibody-drug Conjugate *Co-development molecule with Abbvie
CLL*
NHL MM
NHL MDS MM
NHL
AML
Hemophilia
Heme indications
3
NHL
CLL
CLL
NHL
AML
NHL NHL
CLL
AML/MDS
MM
HEMOPHILIA
CLL
AML/MDS
MM
HEMOPHILIA
AML
NHL
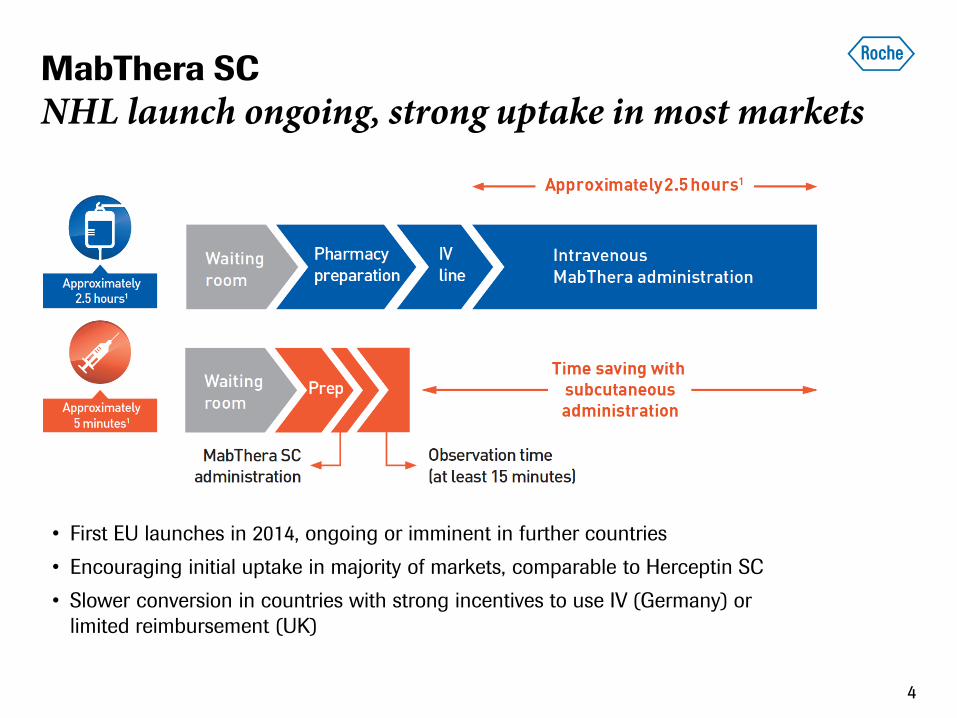
MabThera SC
NHL launch ongoing, strong uptake in most markets
4
• First EU launches in 2014, ongoing or imminent in further countries
• Encouraging initial uptake in majority of markets, comparable to Herceptin SC
• Slower conversion in countries with strong incentives to use IV (Germany) or
limited reimbursement (UK)
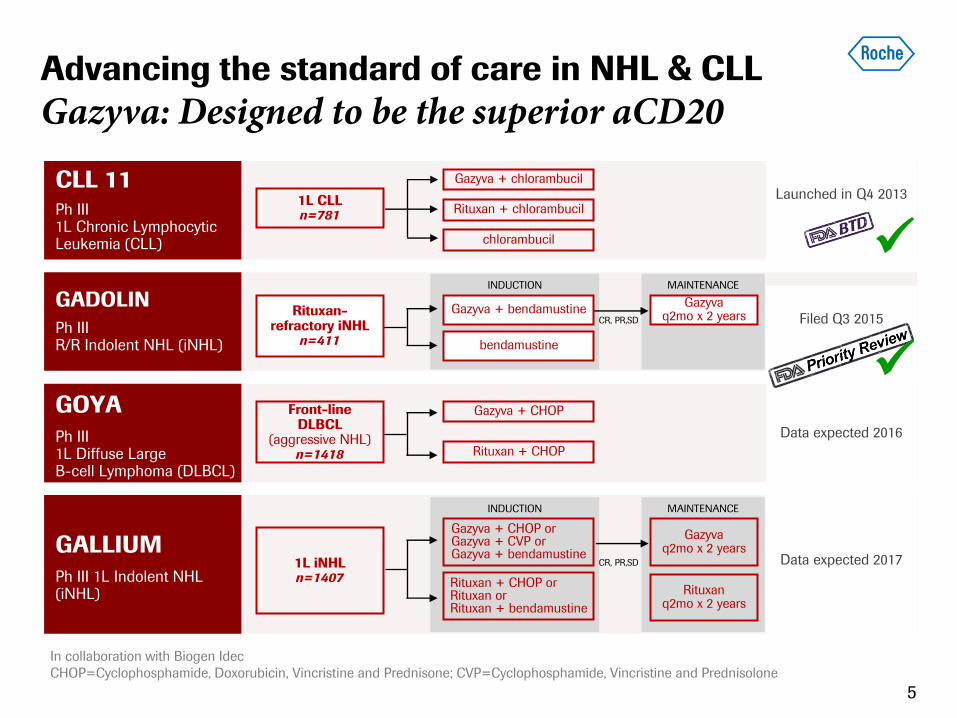
Advancing the standard of care in NHL & CLL
Gazyva: Designed to be the superior aCD20
5
In collaboration with Biogen Idec
CHOP=Cyclophosphamide, Doxorubicin, Vincristine and Prednisone; CVP=Cyclophosphamide, Vincristine and Prednisolone
CLL 11 Ph III 1L Chronic Lymphocytic Leukemia (CLL)
Launched in Q4 2013
Gazyva + chlorambucil
Rituxan + chlorambucil
chlorambucil
GOYA Ph III 1L Diffuse Large B-cell Lymphoma (DLBCL)
Data expected 2016
Gazyva + CHOP
Rituxan + CHOP
GADOLIN
Ph III R/R Indolent NHL (iNHL)
Filed Q3 2015
INDUCTION
bendamustine
MAINTENANCE
Gazyva q2mo x 2 years
Gazyva + bendamustine CR, PR,SD
GALLIUM Ph III 1L Indolent NHL (iNHL)
Data expected 2017
INDUCTION
Rituxan + CHOP or Rituxan or Rituxan + bendamustine
MAINTENANCE
Gazyva q2mo x 2 years
Gazyva + CHOP or Gazyva + CVP or Gazyva + bendamustine
CR, PR,SD
Rituxan q2mo x 2 years
1L CLL n=781
Front-line DLBCL
(aggressive NHL) n=1418
Rituxan-refractory iNHL
n=411
1L iNHL n=1407
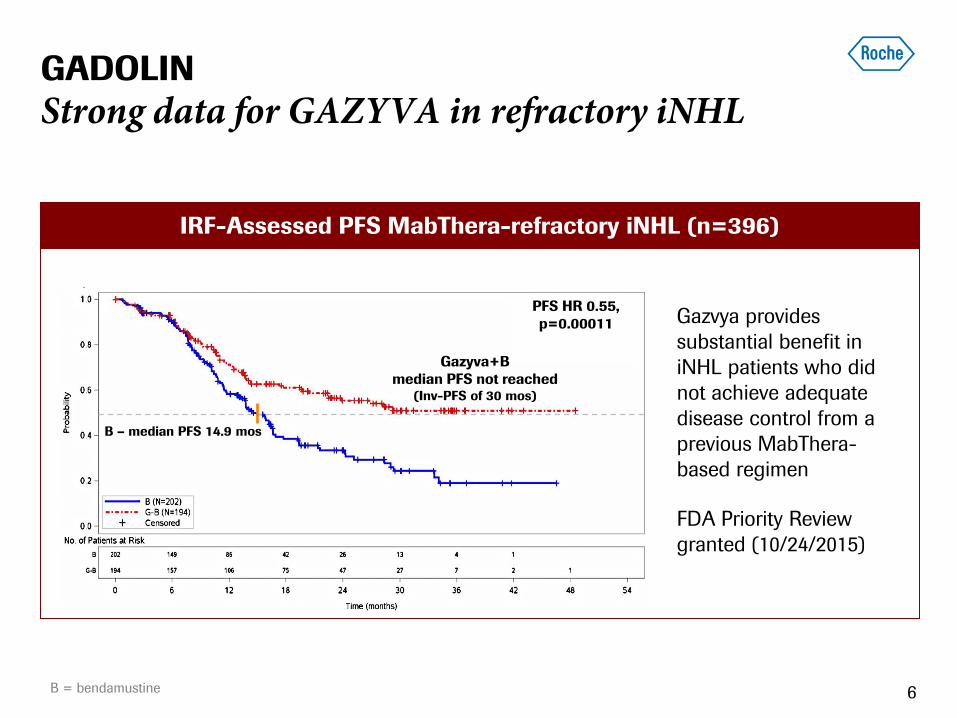
IRF-Assessed PFS MabThera-refractory iNHL (n=396)
B – median PFS 14.9 mos
PFS HR 0.55,
p=0.00011
Gazyva+B
median PFS not reached (Inv-PFS of 30 mos)
GADOLIN
Strong data for GAZYVA in refractory iNHL
6
Gazvya provides
substantial benefit in
iNHL patients who did
not achieve adequate
disease control from a
previous MabThera-
based regimen
FDA Priority Review
granted (10/24/2015)
B = bendamustine
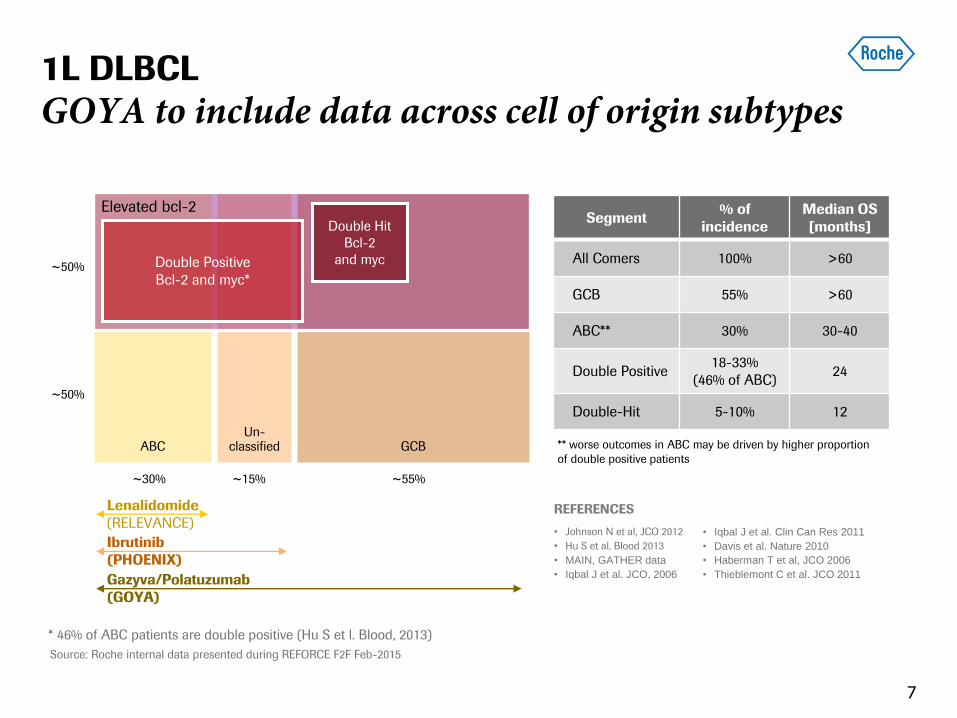
Un-classified ABC GCB
~15% ~55% ~30%
~50%
~50%
Lenalidomide
(RELEVANCE)
Ibrutinib
(PHOENIX)
Gazyva/Polatuzumab
(GOYA)
1L DLBCL
GOYA to include data across cell of origin subtypes
7
Segment % of
incidence
Median OS
[months]
All Comers 100% >60
GCB 55% >60
ABC** 30% 30-40
Double Positive 18-33%
(46% of ABC) 24
Double-Hit 5-10% 12
** worse outcomes in ABC may be driven by higher proportion
of double positive patients
Source: Roche internal data presented during REFORCE F2F Feb-2015
* 46% of ABC patients are double positive (Hu S et l. Blood, 2013)
REFERENCES
• Johnson N et al, JCO 2012
• Hu S et al, Blood 2013
• MAIN, GATHER data
• Iqbal J et al. JCO, 2006
• Iqbal J et al. Clin Can Res 2011
• Davis et al. Nature 2010
• Haberman T et al, JCO 2006
• Thieblemont C et al. JCO 2011
Elevated bcl-2
Double Positive
Bcl-2 and myc*
Double Hit
Bcl-2
and myc
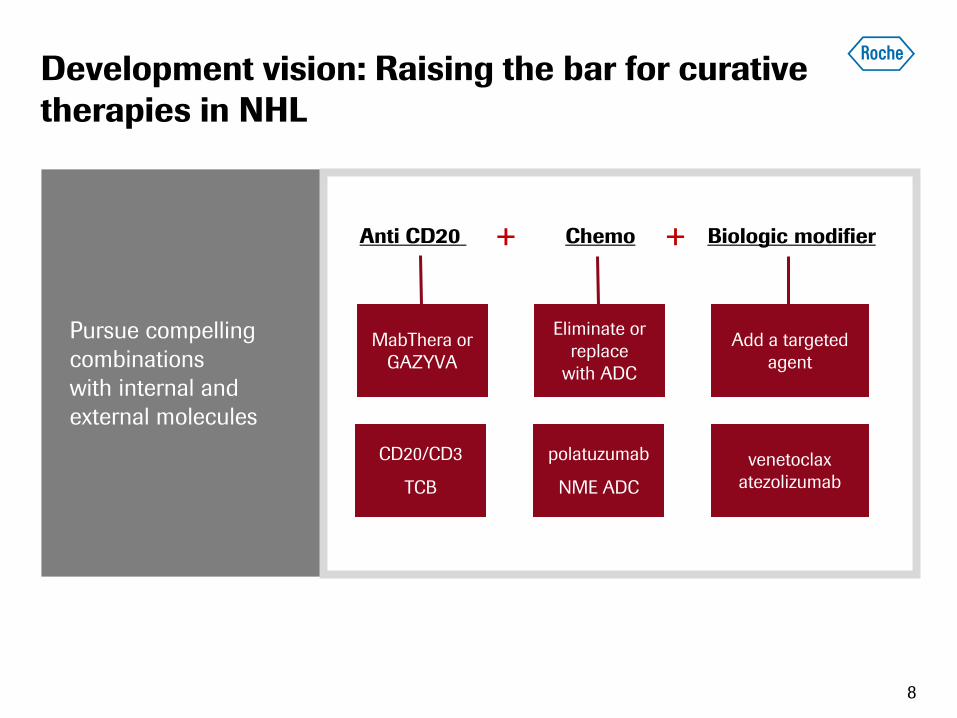
Development vision: Raising the bar for curative
therapies in NHL
Pursue compelling
combinations
with internal and
external molecules
MabThera or
GAZYVA
+ +
polatuzumab
NME ADC
Eliminate or
replace
with ADC
venetoclax
atezolizumab
Add a targeted
agent
Anti CD20 Chemo Biologic modifier
CD20/CD3
TCB
8
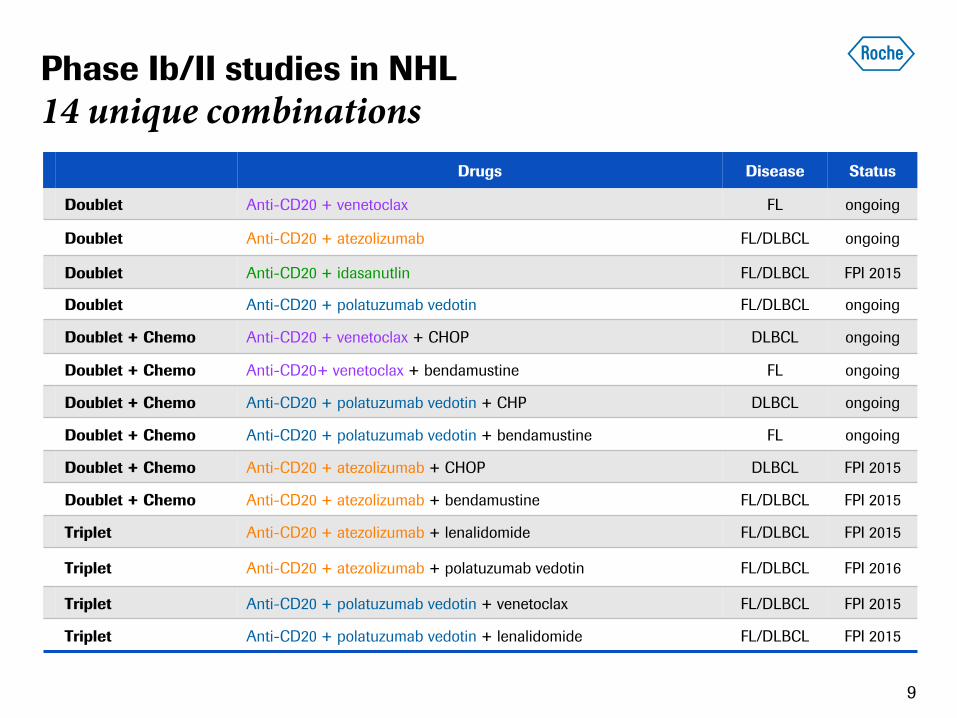
Drugs Disease Status
Doublet Anti-CD20 + venetoclax FL ongoing
Doublet Anti-CD20 + atezolizumab FL/DLBCL ongoing
Doublet Anti-CD20 + idasanutlin FL/DLBCL FPI 2015
Doublet Anti-CD20 + polatuzumab vedotin FL/DLBCL ongoing
Doublet + Chemo Anti-CD20 + venetoclax + CHOP DLBCL ongoing
Doublet + Chemo Anti-CD20+ venetoclax + bendamustine FL ongoing
Doublet + Chemo Anti-CD20 + polatuzumab vedotin + CHP DLBCL ongoing
Doublet + Chemo Anti-CD20 + polatuzumab vedotin + bendamustine FL ongoing
Doublet + Chemo Anti-CD20 + atezolizumab + CHOP DLBCL FPI 2015
Doublet + Chemo Anti-CD20 + atezolizumab + bendamustine FL/DLBCL FPI 2015
Triplet Anti-CD20 + atezolizumab + lenalidomide FL/DLBCL FPI 2015
Triplet Anti-CD20 + atezolizumab + polatuzumab vedotin FL/DLBCL FPI 2016
Triplet Anti-CD20 + polatuzumab vedotin + venetoclax FL/DLBCL FPI 2015
Triplet Anti-CD20 + polatuzumab vedotin + lenalidomide FL/DLBCL FPI 2015
Phase Ib/II studies in NHL
14 unique combinations
9
10
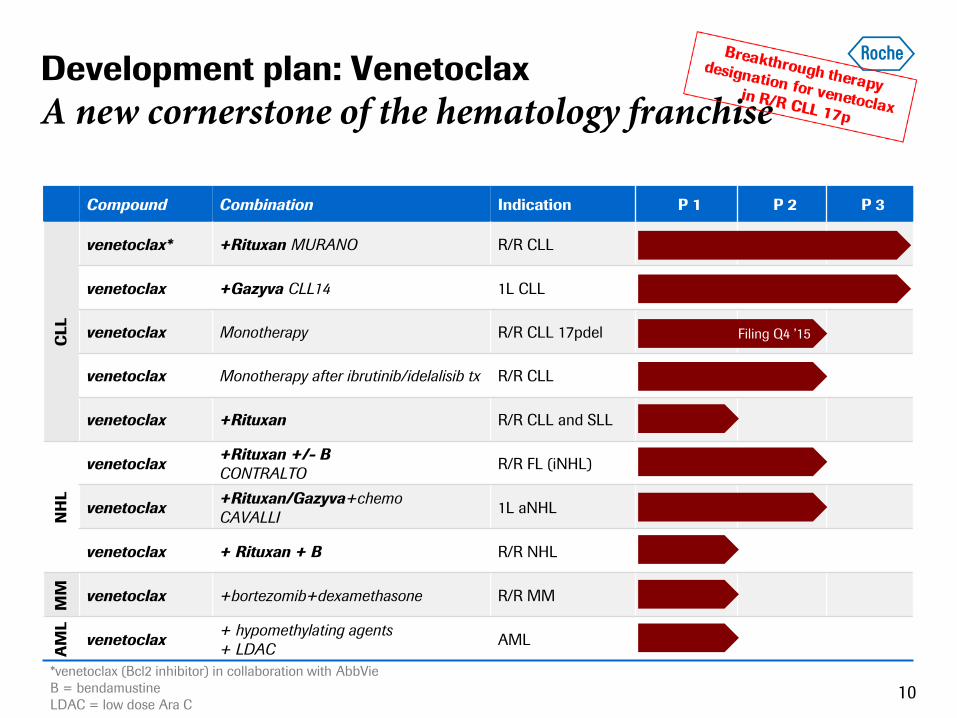
Development plan: Venetoclax
A new cornerstone of the hematology franchise
Compound Combination Indication P 1 P 2 P 3
CLL
venetoclax* +Rituxan MURANO R/R CLL
venetoclax +Gazyva CLL14 1L CLL
venetoclax Monotherapy R/R CLL 17pdel
venetoclax Monotherapy after ibrutinib/idelalisib tx R/R CLL
venetoclax +Rituxan R/R CLL and SLL
NH
L
venetoclax +Rituxan +/- B
CONTRALTO R/R FL (iNHL)
venetoclax +Rituxan/Gazyva+chemo
CAVALLI 1L aNHL
venetoclax + Rituxan + B R/R NHL
MM
venetoclax +bortezomib+dexamethasone R/R MM
AM
L
venetoclax + hypomethylating agents
+ LDAC AML
*venetoclax (Bcl2 inhibitor) in collaboration with AbbVie
B = bendamustine
LDAC = low dose Ara C
Filing Q4 ’15
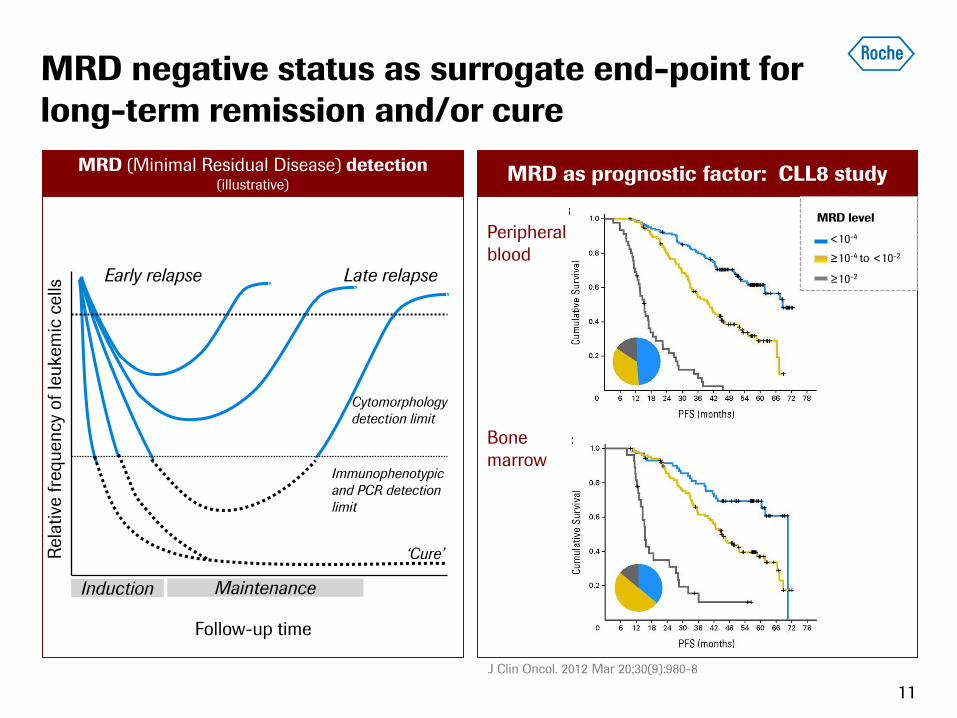
MRD as prognostic factor: CLL8 study MRD (Minimal Residual Disease) detection
(illustrative)
MRD negative status as surrogate end-point for
long-term remission and/or cure
11
Peripheral
blood
Rela
tive
fre
quency
of
leukem
ic c
ells
Follow-up time
Early relapse Late relapse
Induction Maintenance
‘Cure’
Immunophenotypic
and PCR detection
limit
Cytomorphology
detection limit
J Clin Oncol. 2012 Mar 20;30(9):980-8
Bone
marrow
MRD level
<10-4
≥10-4 to <10-2
≥10-2
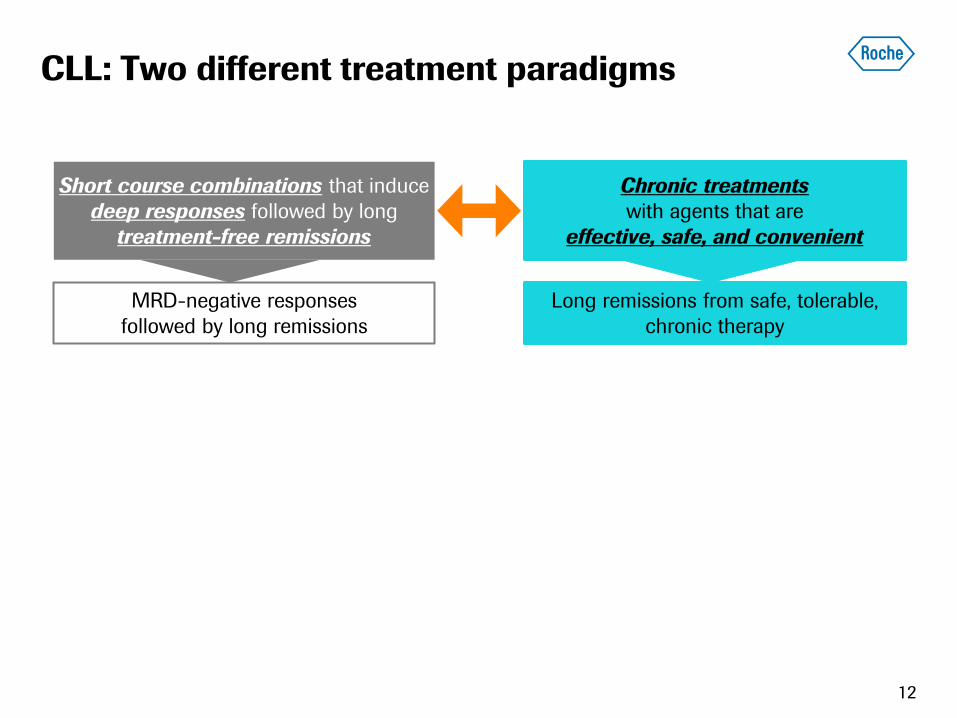
CLL: Two different treatment paradigms
12
Short course combinations that induce
deep responses followed by long
treatment-free remissions
Chronic treatments
with agents that are
effective, safe, and convenient
MRD-negative responses
followed by long remissions
Long remissions from safe, tolerable,
chronic therapy
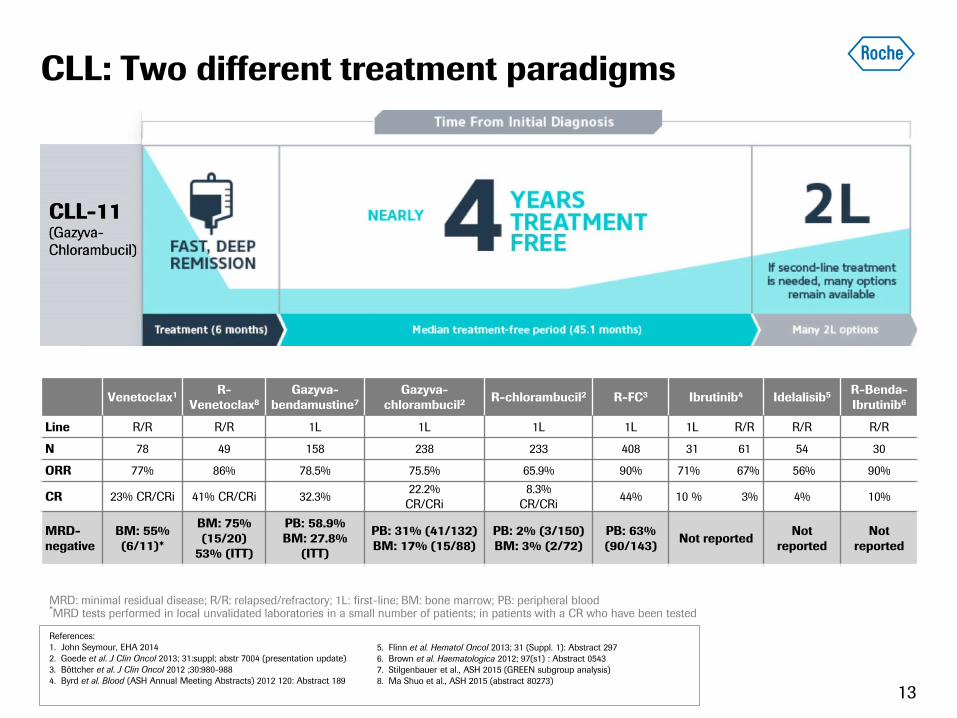
CLL: Two different treatment paradigms
13
Venetoclax1 R-
Venetoclax8
Gazyva-
bendamustine7
Gazyva-
chlorambucil2 R-chlorambucil2 R-FC3 Ibrutinib4 Idelalisib5 R-Benda-
Ibrutinib6
Line R/R R/R 1L 1L 1L 1L 1L R/R R/R R/R
N 78 49 158 238 233 408 31 61 54 30
ORR 77% 86% 78.5% 75.5% 65.9% 90% 71% 67% 56% 90%
CR 23% CR/CRi 41% CR/CRi 32.3% 22.2%
CR/CRi
8.3%
CR/CRi 44% 10 % 3% 4% 10%
MRD-
negative
BM: 55%
(6/11)*
BM: 75%
(15/20)
53% (ITT)
PB: 58.9%
BM: 27.8%
(ITT)
PB: 31% (41/132)
BM: 17% (15/88)
PB: 2% (3/150)
BM: 3% (2/72)
PB: 63%
(90/143) Not reported
Not
reported
Not
reported
MRD: minimal residual disease; R/R: relapsed/refractory; 1L: first-line; BM: bone marrow; PB: peripheral blood *MRD tests performed in local unvalidated laboratories in a small number of patients; in patients with a CR who have been tested
References:
1. John Seymour, EHA 2014
2. Goede et al. J Clin Oncol 2013; 31:suppl; abstr 7004 (presentation update)
3. Böttcher et al. J Clin Oncol 2012 ;30:980-988
4. Byrd et al. Blood (ASH Annual Meeting Abstracts) 2012 120: Abstract 189
5. Flinn et al. Hematol Oncol 2013; 31 (Suppl. 1): Abstract 297
6. Brown et al. Haematologica 2012; 97(s1) : Abstract 0543
7. Stilgenbauer et al., ASH 2015 (GREEN subgroup analysis)
8. Ma Shuo et al., ASH 2015 (abstract 80273)
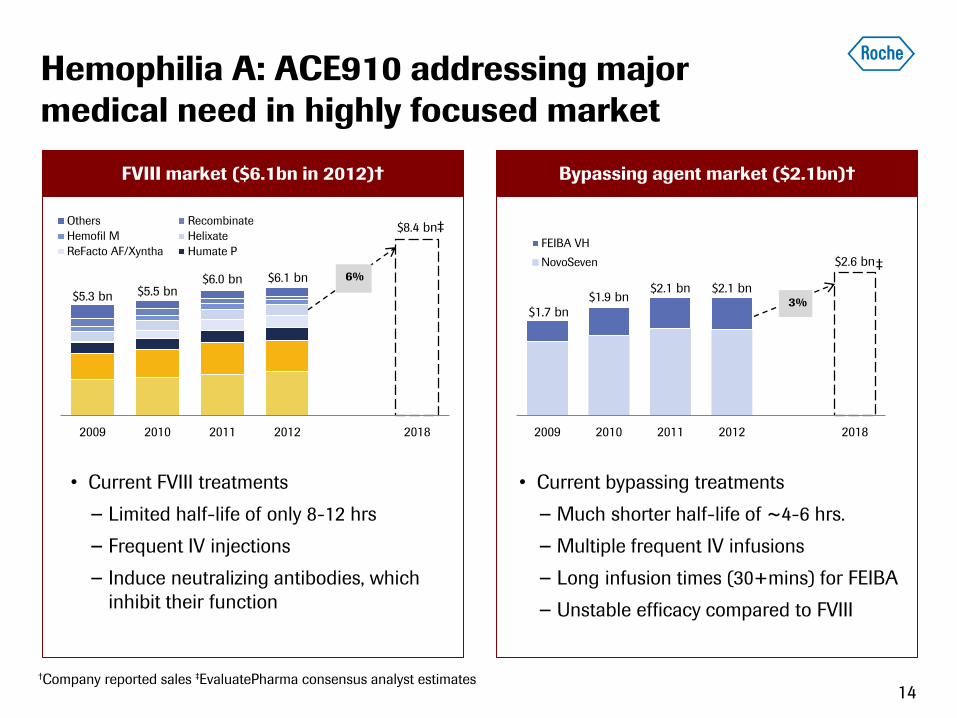
Bypassing agent market ($2.1bn)† FVIII market ($6.1bn in 2012)†
Hemophilia A: ACE910 addressing major
medical need in highly focused market
14 †Company reported sales ‡EvaluatePharma consensus analyst estimates
$5.3 bn $5.5 bn $6.0 bn $6.1 bn
$8.4 bn
2009 2010 2011 2012 2018
Others Recombinate
Hemofil M Helixate
ReFacto AF/Xyntha Humate P
6%
‡
$1.7 bn $1.9 bn
$2.1 bn $2.1 bn
$2.6 bn
2009 2010 2011 2012 2018
FEIBA VH
NovoSeven
3%
‡
• Current FVIII treatments
− Limited half-life of only 8-12 hrs
− Frequent IV injections
− Induce neutralizing antibodies, which
inhibit their function
• Current bypassing treatments
− Much shorter half-life of ~4-6 hrs.
− Multiple frequent IV infusions
− Long infusion times (30+mins) for FEIBA
− Unstable efficacy compared to FVIII
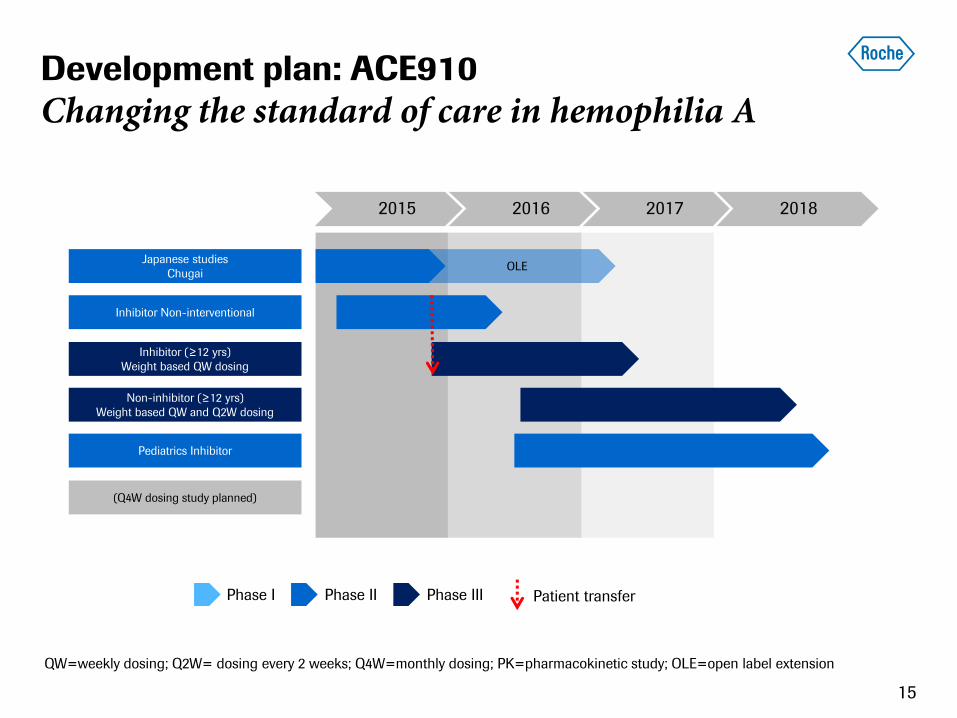
Development plan: ACE910
Changing the standard of care in hemophilia A
15
2015 2016 2017 2018
Pediatrics Inhibitor
Inhibitor Non-interventional
Inhibitor (≥12 yrs)
Weight based QW dosing
(Q4W dosing study planned)
Non-inhibitor (≥12 yrs)
Weight based QW and Q2W dosing
Japanese studies
Chugai OLE
QW=weekly dosing; Q2W= dosing every 2 weeks; Q4W=monthly dosing; PK=pharmacokinetic study; OLE=open label extension
Phase II Phase III Phase I Patient transfer
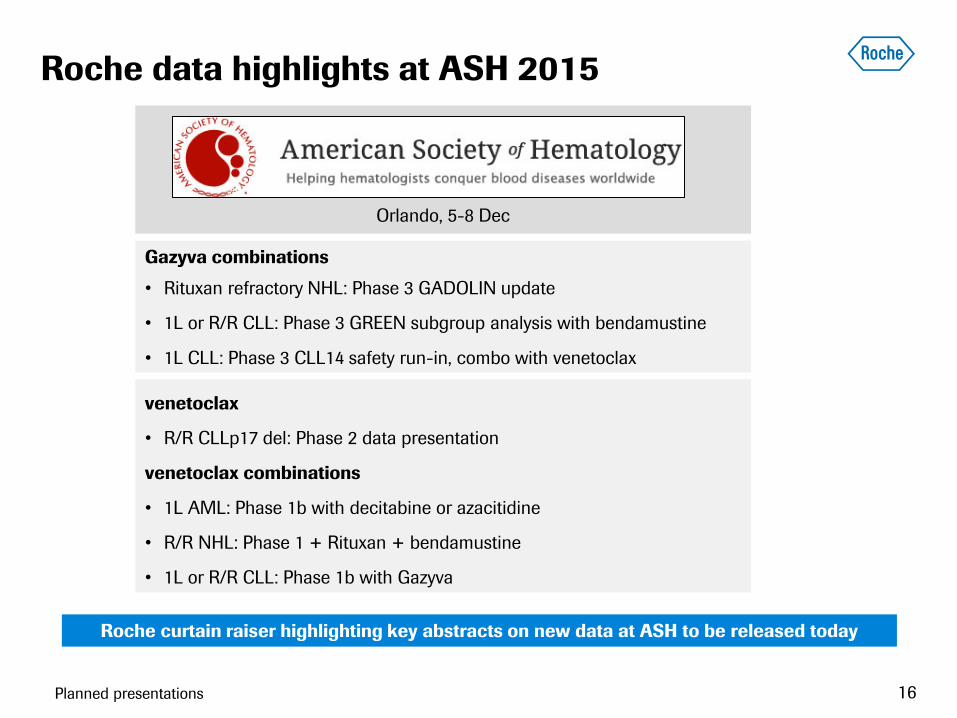
Roche data highlights at ASH 2015
Gazyva combinations
• Rituxan refractory NHL: Phase 3 GADOLIN update
• 1L or R/R CLL: Phase 3 GREEN subgroup analysis with bendamustine
• 1L CLL: Phase 3 CLL14 safety run-in, combo with venetoclax
Abstracts planned/submitted Abstracts planned/submitted Abstracts planned/submitted
Orlando, 5-8 Dec
Planned presentations
venetoclax
• R/R CLLp17 del: Phase 2 data presentation
venetoclax combinations
• 1L AML: Phase 1b with decitabine or azacitidine
• R/R NHL: Phase 1 + Rituxan + bendamustine
• 1L or R/R CLL: Phase 1b with Gazyva
Roche curtain raiser highlighting key abstracts on new data at ASH to be released today
16
Garret Hampton | VP, Oncology Biomarker Development
Pharmaceuticals Division
Roche Pharma Day 2015
Molecular Information
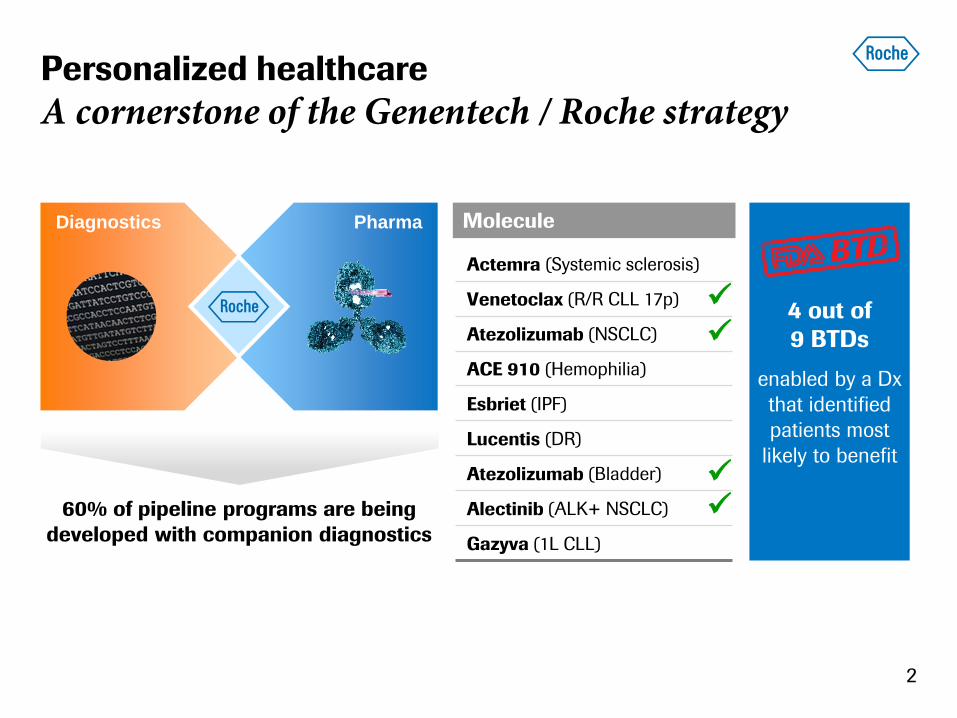
Personalized healthcare
A cornerstone of the Genentech / Roche strategy
2
Diagnostics Pharma
60% of pipeline programs are being
developed with companion diagnostics
4 out of
9 BTDs
enabled by a Dx
that identified
patients most
likely to benefit
Molecule
Actemra (Systemic sclerosis)
Venetoclax (R/R CLL 17p)
Atezolizumab (NSCLC)
ACE 910 (Hemophilia)
Esbriet (IPF)
Lucentis (DR)
Atezolizumab (Bladder)
Alectinib (ALK+ NSCLC)
Gazyva (1L CLL)
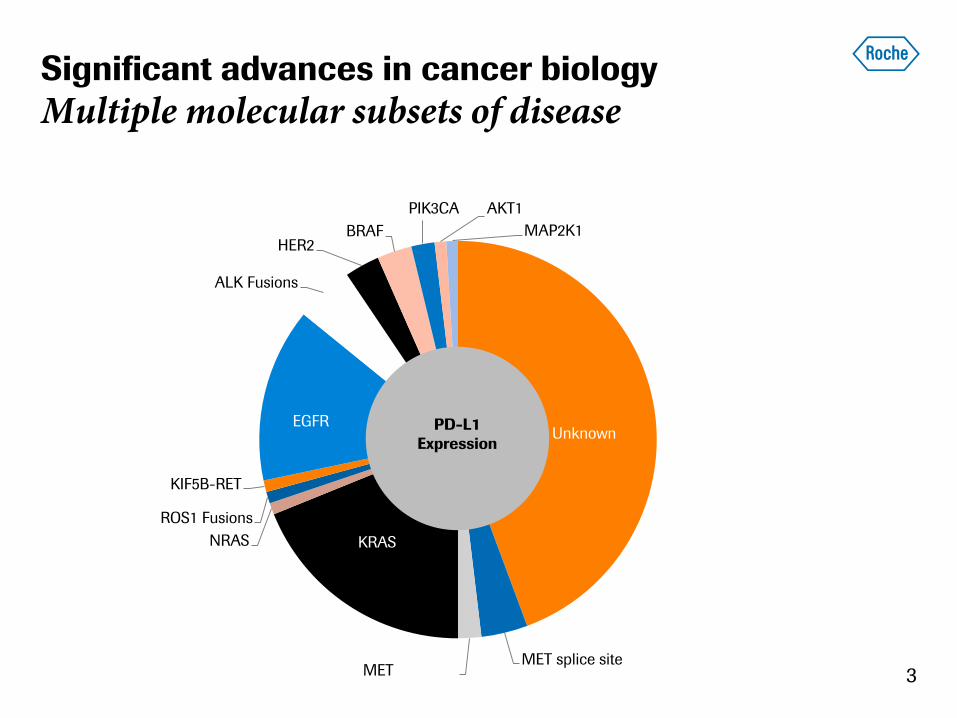
Significant advances in cancer biology
Multiple molecular subsets of disease
Unknown
MET splice site MET
Amplification
KRAS NRAS
ROS1 Fusions
KIF5B-RET
EGFR
ALK Fusions
HER2 BRAF
PIK3CA AKT1
MAP2K1
PD-L1
Expression
3
4
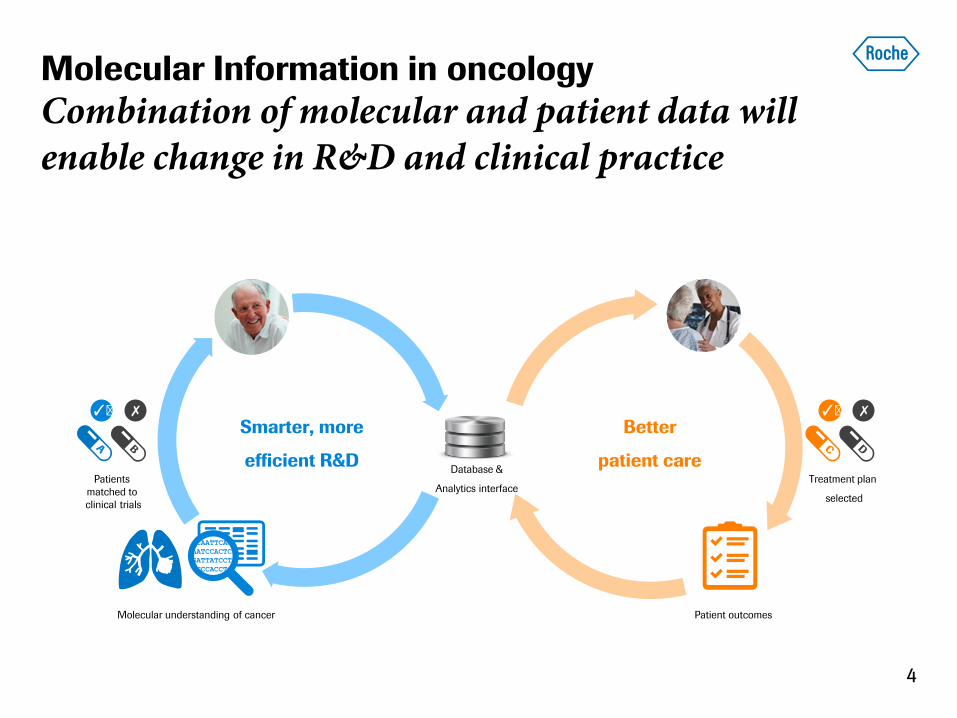
Molecular Information in oncology
Combination of molecular and patient data will enable change in R&D and clinical practice
✓ ︎ ✗ ✓ ︎ ✗
Smarter, more
efficient R&D
Better
patient care Patients
matched to
clinical trials
Treatment plan
selected
Molecular understanding of cancer Patient outcomes
Database &
Analytics interface
Multiple capabilities required
Comprehensive tumor analysis and longitudinal assessment
mRNA-
expression
Cell signatures,
targets
RNA
sequencing
DNA-mutation
& CNVs
Ex: EGFR, BRAF
DNA
sequencing
Protein-
expression
PDL1, other CI
targets
Multiplex
IHC
Comprehensive tumor analysis Continuous monitoring over time
Cell free tumor
DNA
Blood DNA
sequencing
Imaging
Ex: ImmunoPet
Imaging
Ex: EGFR, BRAF
5
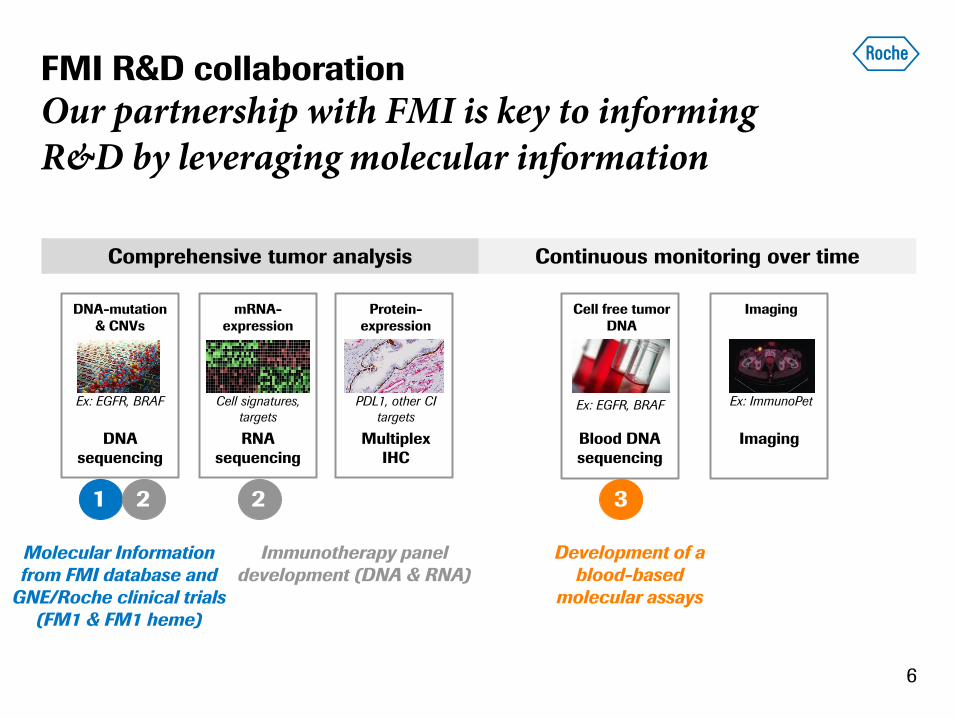
FMI R&D collaboration
Our partnership with FMI is key to informing R&D by leveraging molecular information
6
Molecular Information
from FMI database and
GNE/Roche clinical trials
(FM1 & FM1 heme)
mRNA-
expression
Cell signatures,
targets
RNA
sequencing
DNA-mutation
& CNVs
Ex: EGFR, BRAF
DNA
sequencing
Protein-
expression
PDL1, other CI
targets
Multiplex
IHC
Comprehensive tumor analysis Continuous monitoring over time
Cell free tumor
DNA
Blood DNA
sequencing
Imaging
Ex: ImmunoPet
Imaging
Ex: EGFR, BRAF
1 3
Development of a
blood-based
molecular assays
2
Immunotherapy panel
development (DNA & RNA)
2 2

Clinical trial data
Roche database FMI clinical database
50,000+ patient data in FMI database
1
Roche / FMI database queries
Example: PIK3CA mutations in multiple cancers
7
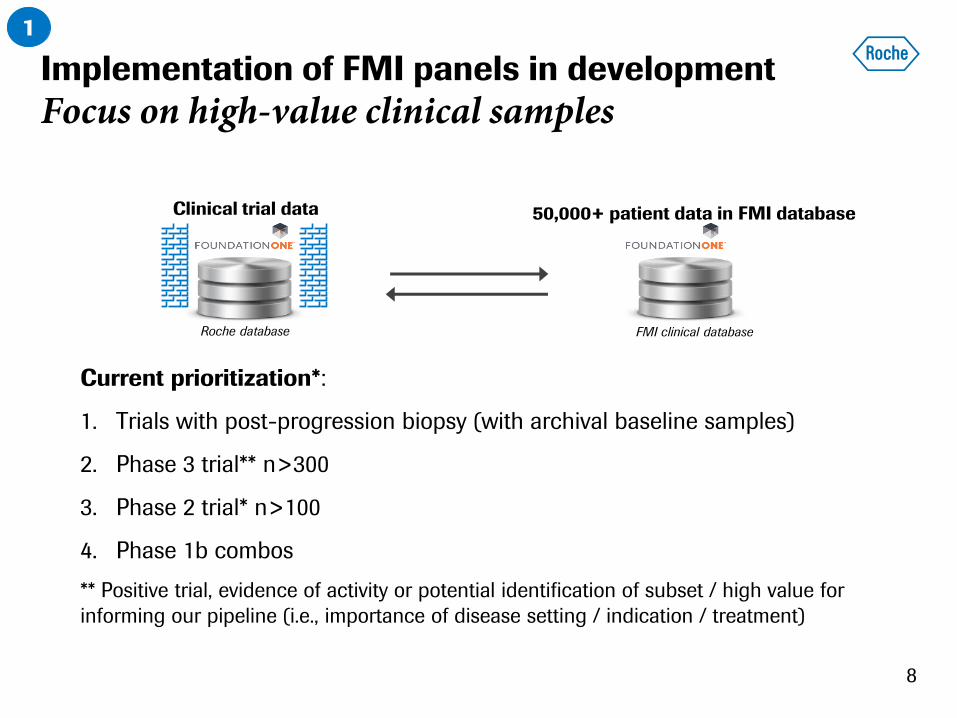
Implementation of FMI panels in development
Focus on high-value clinical samples
Clinical trial data
Roche database FMI clinical database
Current prioritization*:
1. Trials with post-progression biopsy (with archival baseline samples)
2. Phase 3 trial** n>300
3. Phase 2 trial* n>100
4. Phase 1b combos
** Positive trial, evidence of activity or potential identification of subset / high value for
informing our pipeline (i.e., importance of disease setting / indication / treatment)
50,000+ patient data in FMI database
1
8
FMI R&D collaboration
Immunotherapy R&D collaboration
9
2
Immunotherapy panel
development (DNA & RNA)
mRNA-
expression
Cell signatures,
targets
RNA
sequencing
DNA-mutation
& CNVs
Ex: EGFR, BRAF
DNA
sequencing
Protein-
expression
PDL1, other CI
targets
Multiplex
IHC
Comprehensive tumor analysis Continuous monitoring over time
Cell free tumor
DNA
Blood DNA
sequencing
Imaging
Ex: ImmunoPet
Imaging
Ex: EGFR, BRAF
2
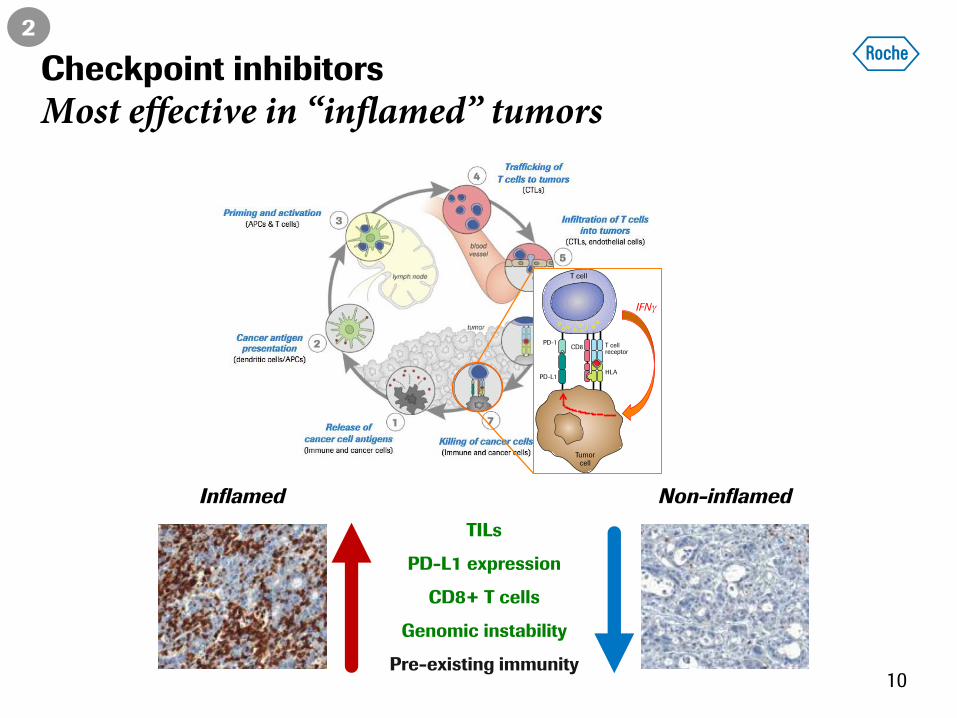
Checkpoint inhibitors
Most effective in “inflamed” tumors
Inflamed Non-inflamed
TILs
PD-L1 expression
CD8+ T cells
Genomic instability
Pre-existing immunity
2
10
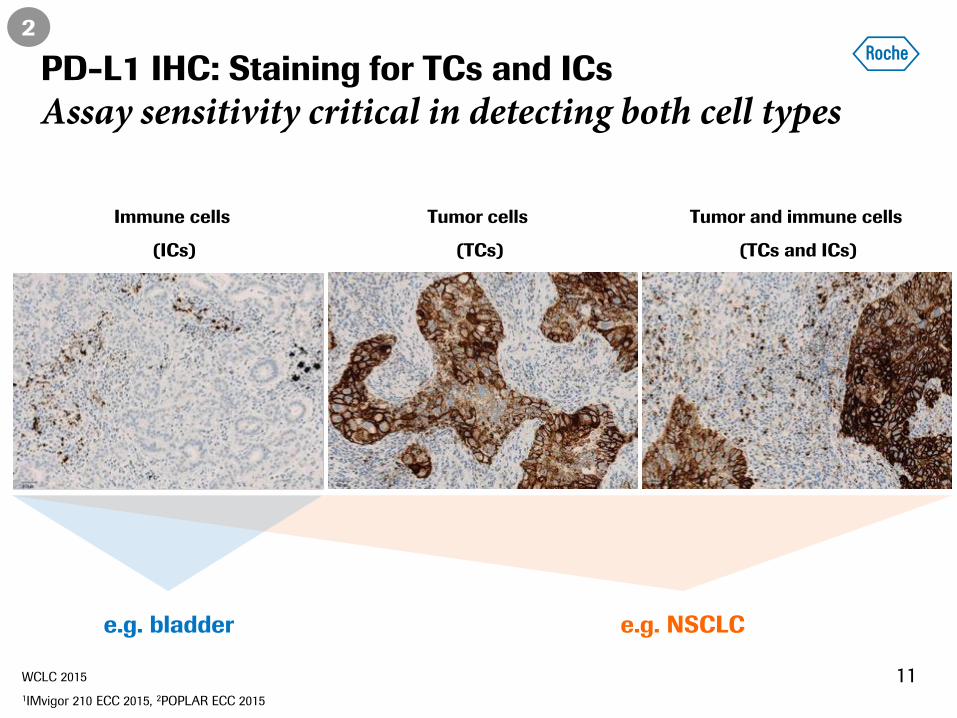
PD-L1 IHC: Staining for TCs and ICs
Assay sensitivity critical in detecting both cell types
11
Tumor cells
(TCs)
Tumor and immune cells
(TCs and ICs)
WCLC 2015
1IMvigor 210 ECC 2015, 2POPLAR ECC 2015
e.g. NSCLC e.g. bladder
Immune cells
(ICs)
2
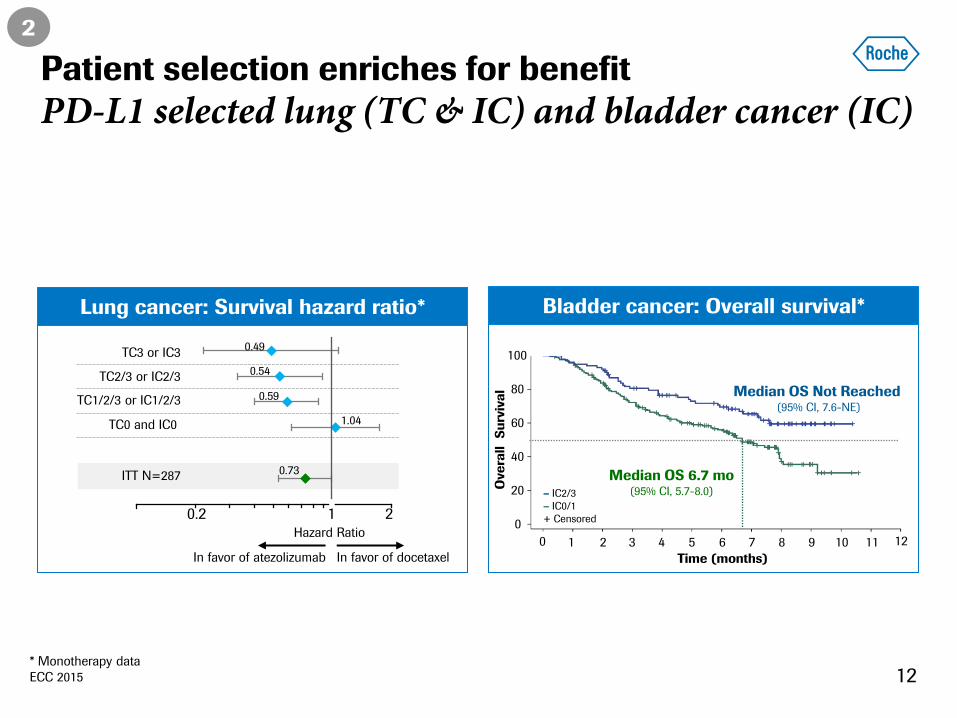
Patient selection enriches for benefit
PD-L1 selected lung (TC & IC) and bladder cancer (IC)
Bladder cancer: Overall survival* Lung cancer: Survival hazard ratio*
* Monotherapy data
ECC 2015
Time (months)
100
80
60
40
20
0
5 6 7 8 9 10 11 1 2 3 4 0
– IC2/3
– IC0/1
+ Censored
12
Ove
rall
Su
rviv
al
Median OS 6.7 mo (95% CI, 5.7-8.0)
Median OS Not Reached (95% CI, 7.6-NE)
0.1 1
In favor of docetaxel
0.73
1.04
0.59
0.54
0.49
Hazard Ratio
In favor of atezolizumab
0.2 1 2
TC3 or IC3
TC2/3 or IC2/3
TC1/2/3 or IC1/2/3
TC0 and IC0
ITT N=287
2
12
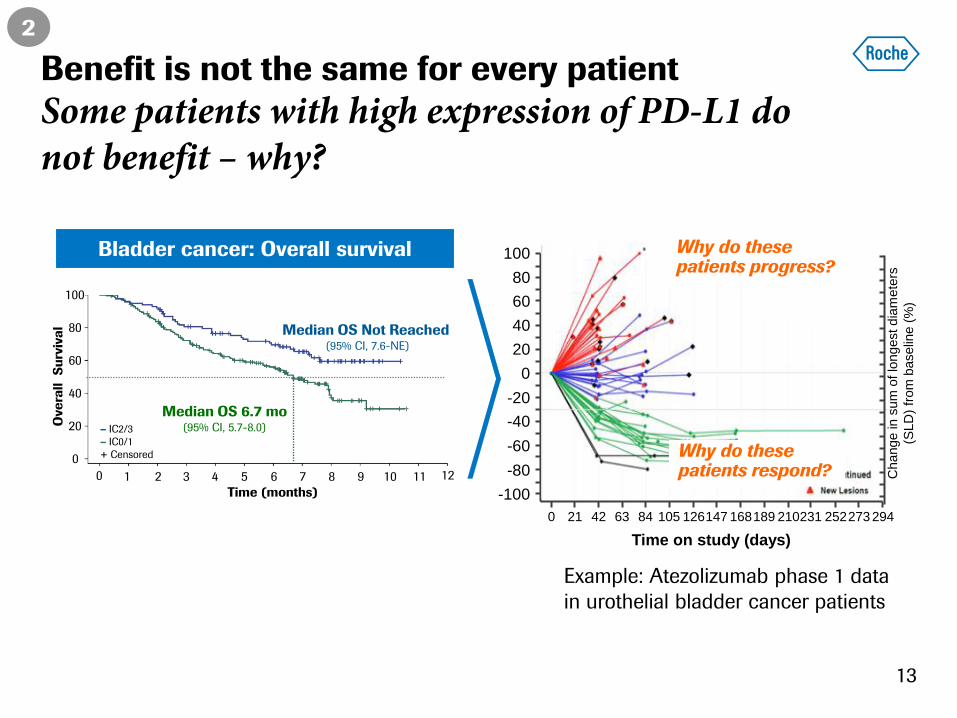
Bladder cancer: Overall survival
Example: Atezolizumab phase 1 data
in urothelial bladder cancer patients
100
80
60
40
20
0
-20
-40
-60
-80
-100
0 21 42 63 84 105 126 147 168 189 210 231 252 273 294
Time on study (days)
Why do these patients progress?
Why do these patients respond? C
hange in s
um
of lo
ngest dia
mete
rs
(SLD
) fr
om
baselin
e (
%)
Time (months)
100
80
60
40
20
0
5 6 7 8 9 10 11 1 2 3 4 0
– IC2/3
– IC0/1
+ Censored
12
Ove
rall
Su
rviv
al
Median OS 6.7 mo (95% CI, 5.7-8.0)
Median OS Not Reached (95% CI, 7.6-NE)
Benefit is not the same for every patient
Some patients with high expression of PD-L1 do not benefit – why?
2
13
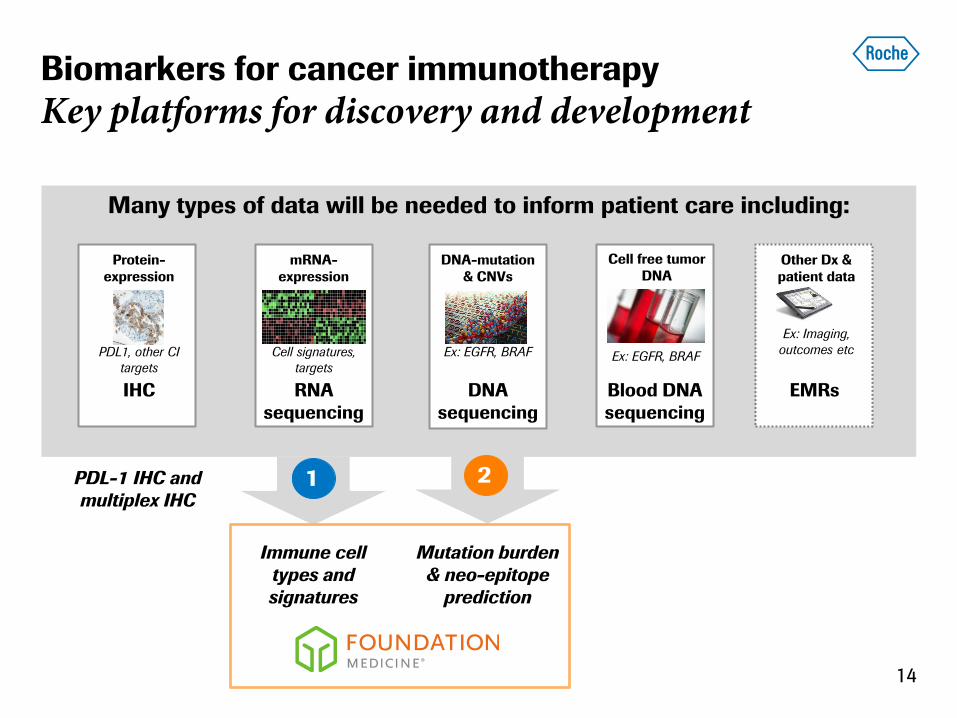
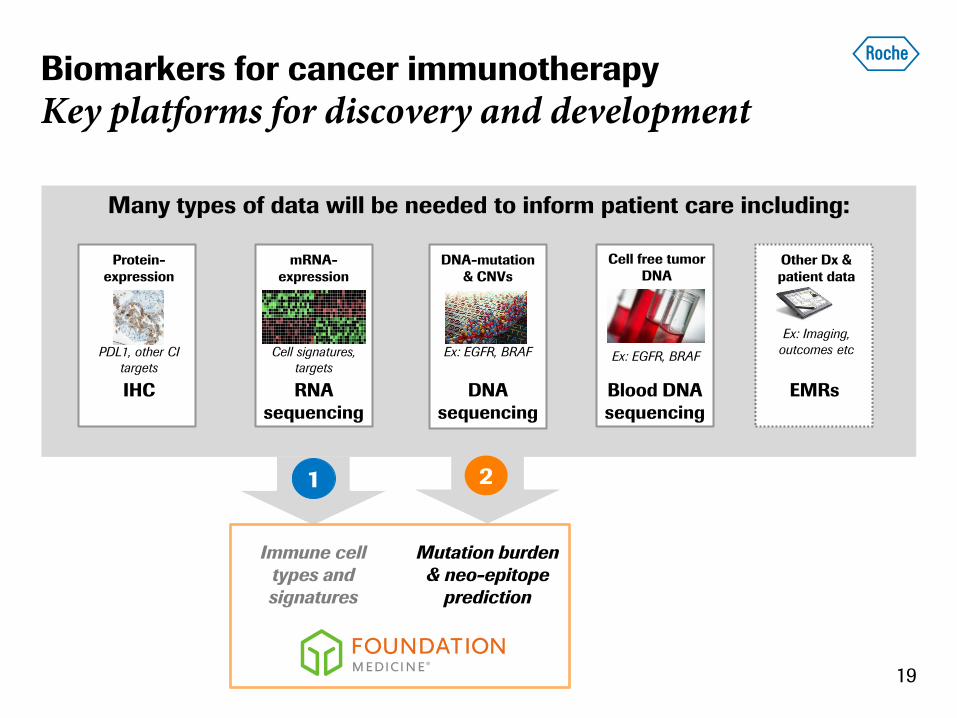
Many types of data will be needed to inform patient care including:
Biomarkers for cancer immunotherapy
Key platforms for discovery and development
mRNA-
expression
Cell signatures,
targets
RNA
sequencing
DNA-mutation
& CNVs
Ex: EGFR, BRAF
DNA
sequencing
Protein-
expression
PDL1, other CI
targets
IHC
Cell free tumor
DNA
Blood DNA
sequencing
Ex: EGFR, BRAF
Other Dx &
patient data
Ex: Imaging,
outcomes etc
EMRs
PDL-1 IHC and
multiplex IHC
Mutation burden
& neo-epitope
prediction
Immune cell
types and
signatures
1 2
14
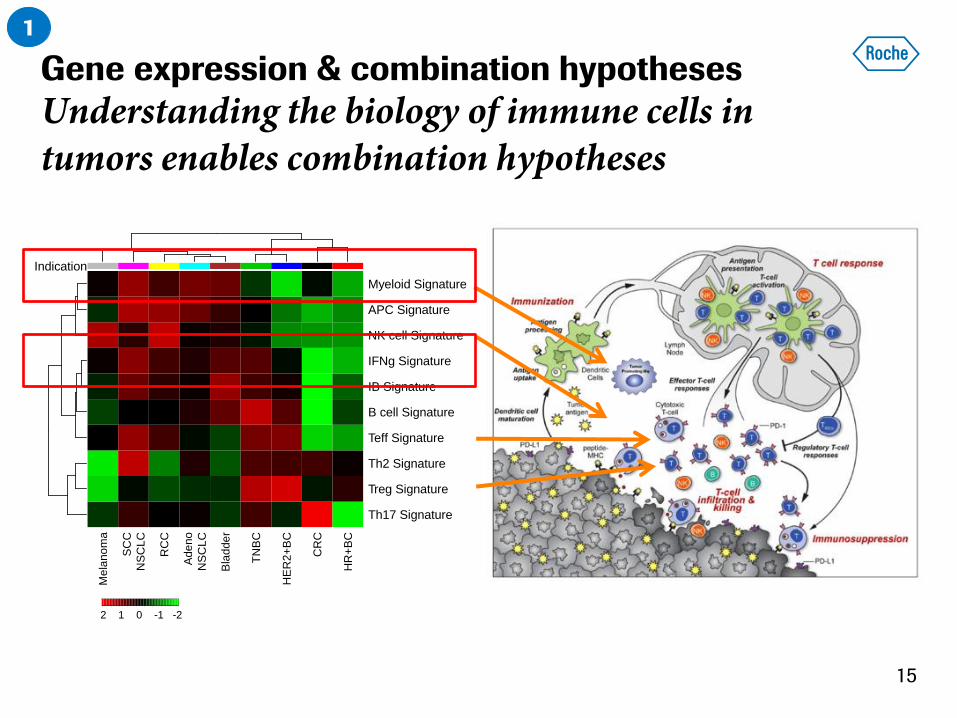
Gene expression & combination hypotheses
Understanding the biology of immune cells in tumors enables combination hypotheses
−2 −1.6 −0.67 0.22 1.1 1.6 2
2 1 0 -1 -2
cbind(1:nc)
Indication
Me
lan
om
a
SC
C
NS
CL
C
RC
C
Ade
no
NS
CL
C
Bla
dde
r
TN
BC
HE
R2
+B
C
CR
C
HR
+B
C
Th17 Signature
Treg Signature
Th2 Signature
Teff Signature
B cell Signature
IB Signature
IFNg Signature
NK cell Signature
APC Signature
Myeloid Signature
1
15
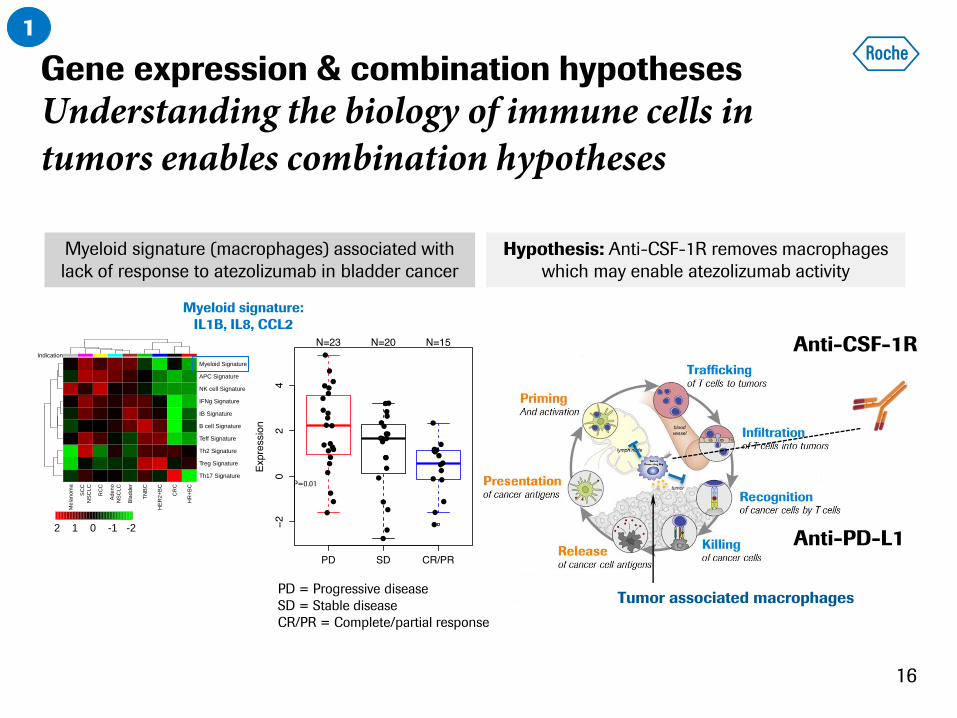
Gene expression & combination hypotheses
Understanding the biology of immune cells in tumors enables combination hypotheses
16
Myeloid signature (macrophages) associated with
lack of response to atezolizumab in bladder cancer
−2 −1.6 −0.67 0.22 1.1 1.6 2
2 1 0 -1 -2
cbind(1:nc)
Indication
Me
lan
om
a
SC
C
NS
CL
C
RC
C
Ade
no
NS
CL
C
Bla
dde
r
TN
BC
HE
R2
+B
C
CR
C
HR
+B
C
Th17 Signature
Treg Signature
Th2 Signature
Teff Signature
B cell Signature
IB Signature
IFNg Signature
NK cell Signature
APC Signature
Myeloid Signature
Anti-CSF-1R
Anti-PD-L1
Tumor associated macrophages
Hypothesis: Anti-CSF-1R removes macrophages
which may enable atezolizumab activity
Myeloid signature:
IL1B, IL8, CCL2
P=0.01
PD = Progressive disease
SD = Stable disease
CR/PR = Complete/partial response
1
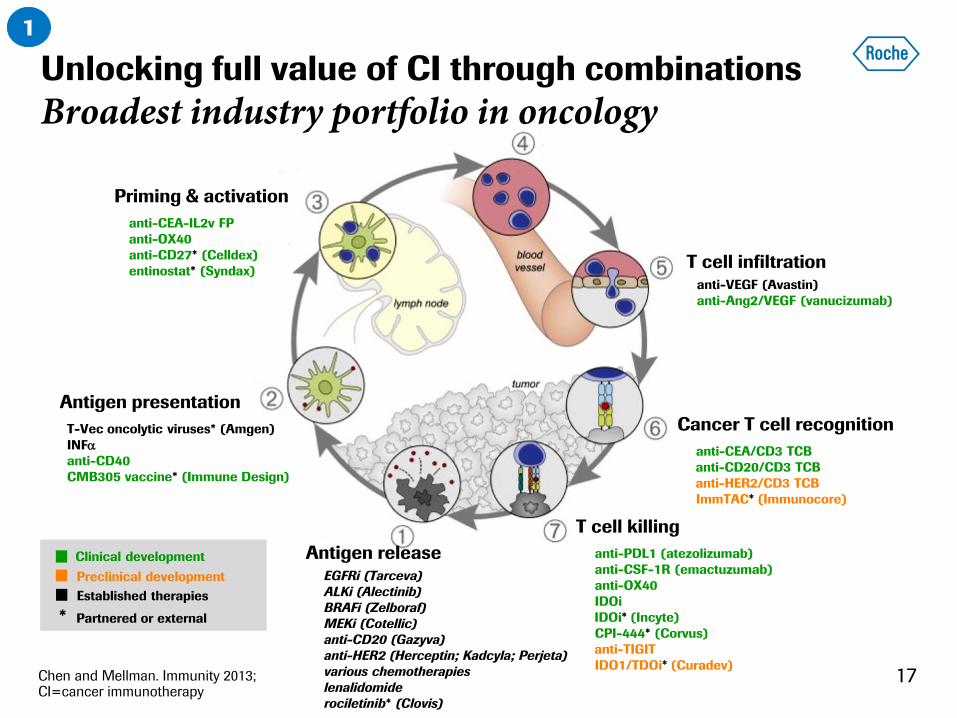
T cell infiltration
Cancer T cell recognition
anti-CEA/CD3 TCB
anti-CD20/CD3 TCB
anti-HER2/CD3 TCB
ImmTAC* (Immunocore)
anti-VEGF (Avastin)
anti-Ang2/VEGF (vanucizumab)
Chen and Mellman. Immunity 2013; CI=cancer immunotherapy
T cell killing
anti-PDL1 (atezolizumab)
anti-CSF-1R (emactuzumab)
anti-OX40
IDOi
IDOi* (Incyte)
CPI-444* (Corvus)
anti-TIGIT
IDO1/TDOi* (Curadev)
EGFRi (Tarceva)
ALKi (Alectinib)
BRAFi (Zelboraf)
MEKi (Cotellic)
anti-CD20 (Gazyva)
anti-HER2 (Herceptin; Kadcyla; Perjeta)
various chemotherapies
lenalidomide
rociletinib* (Clovis)
Antigen presentation
T-Vec oncolytic viruses* (Amgen)
INFa
anti-CD40
CMB305 vaccine* (Immune Design)
Priming & activation
anti-CEA-IL2v FP
anti-OX40
anti-CD27* (Celldex)
entinostat* (Syndax)
Antigen release
17
Unlocking full value of CI through combinations
Broadest industry portfolio in oncology
1
Clinical development Preclinical development
* Partnered or external
Established therapies
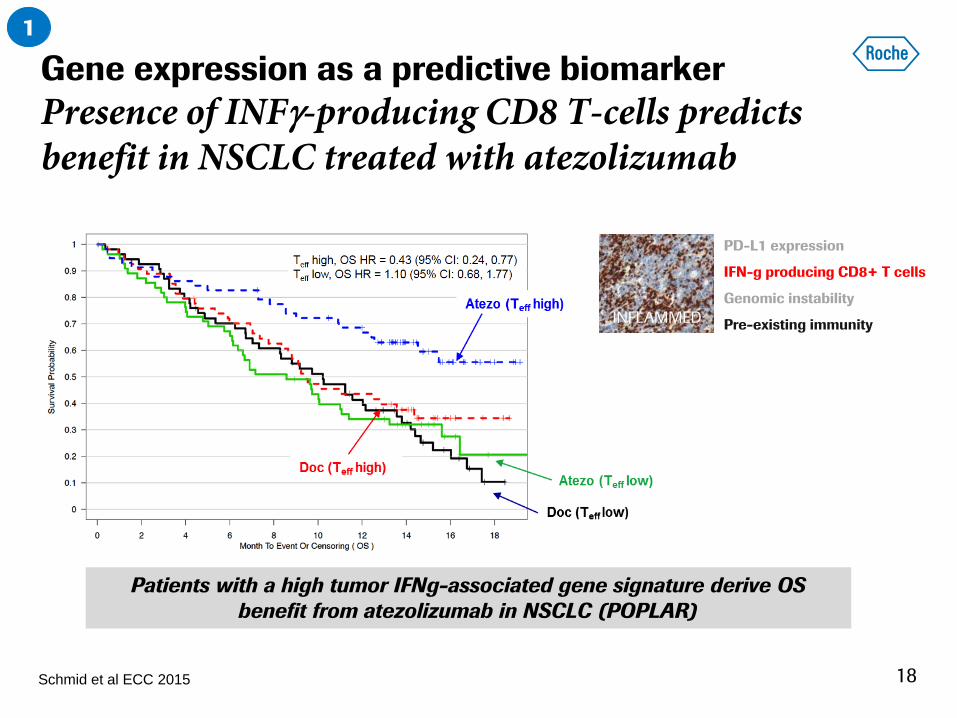
Schmid et al ECC 2015
Patients with a high tumor IFNg-associated gene signature derive OS
benefit from atezolizumab in NSCLC (POPLAR)
PD-L1 expression
IFN-g producing CD8+ T cells
Genomic instability
Pre-existing immunity INFLAMMED
Gene expression as a predictive biomarker
Presence of INFg-producing CD8 T-cells predicts benefit in NSCLC treated with atezolizumab
1
18
Many types of data will be needed to inform patient care including:
Biomarkers for cancer immunotherapy
Key platforms for discovery and development
mRNA-
expression
Cell signatures,
targets
RNA
sequencing
DNA-mutation
& CNVs
Ex: EGFR, BRAF
DNA
sequencing
Protein-
expression
PDL1, other CI
targets
IHC
Cell free tumor
DNA
Blood DNA
sequencing
Ex: EGFR, BRAF
Other Dx &
patient data
Ex: Imaging,
outcomes etc
EMRs
Mutation burden
& neo-epitope
prediction
Immune cell
types and
signatures
1 2
19
PFS
/ O
S
Time
High
Low
Mutation burden
# o
f m
uta
tio
ns
e.g. Lung tumors
Low
High
1
2
Tumor cell
1
Tumor cell
2
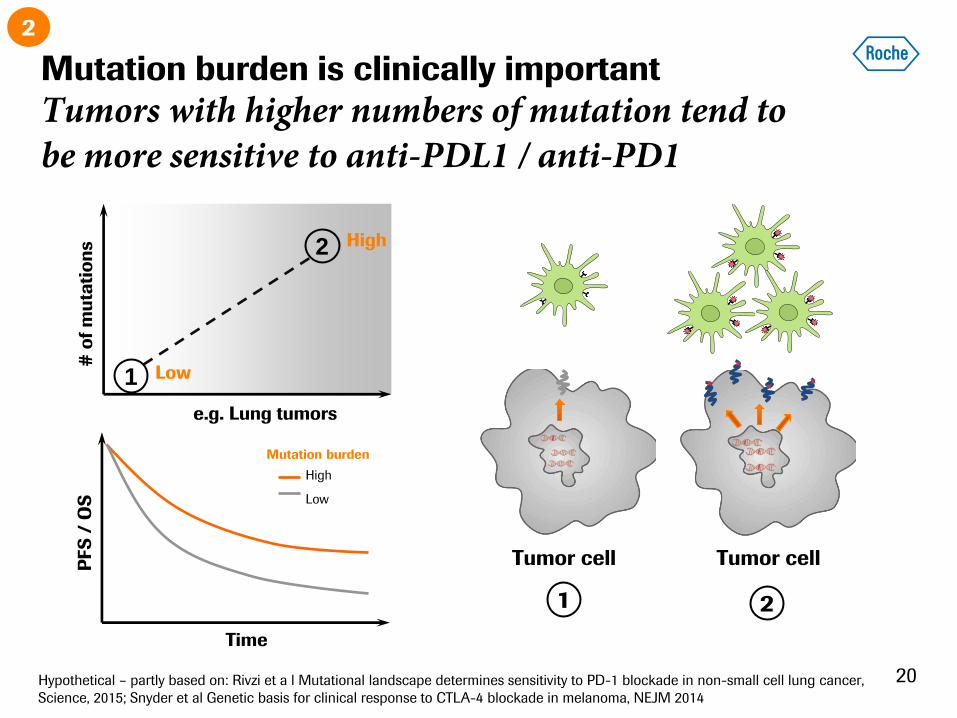
Mutation burden is clinically important
Tumors with higher numbers of mutation tend to be more sensitive to anti-PDL1 / anti-PD1
Hypothetical – partly based on: Rivzi et a l Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer,
Science, 2015; Snyder et al Genetic basis for clinical response to CTLA-4 blockade in melanoma, NEJM 2014
2
20

Conclusions
21
Personalised
healthcare
Molecular
Information
Transformational
time
Diagnostics Pharma
R&D insights
✓ ︎ ✗
Roche Pharma Day 2015
Biosimilar market in context
Fermin Ruiz de Erenchun | Global Head Biologic Strategy Team
Pharmaceuticals Division
2
Biosimilars: Ten years in the making
Regulatory environment
Summary
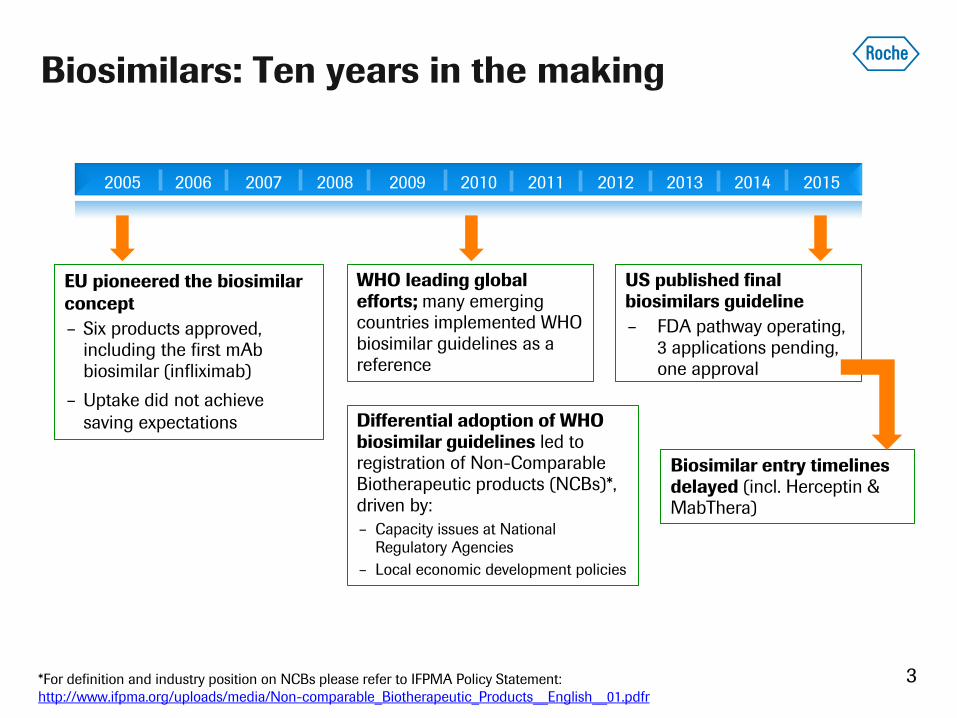
Biosimilars: Ten years in the making
3
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
EU pioneered the biosimilar
concept
– Six products approved, including the first mAb biosimilar (infliximab)
– Uptake did not achieve
saving expectations
WHO leading global efforts; many emerging countries implemented WHO biosimilar guidelines as a reference
US published final biosimilars guideline
– FDA pathway operating, 3 applications pending, one approval
Biosimilar entry timelines delayed (incl. Herceptin & MabThera)
Differential adoption of WHO biosimilar guidelines led to registration of Non-Comparable Biotherapeutic products (NCBs)*, driven by:
– Capacity issues at National
Regulatory Agencies
– Local economic development policies
*For definition and industry position on NCBs please refer to IFPMA Policy Statement:
http://www.ifpma.org/uploads/media/Non-comparable_Biotherapeutic_Products__English__01.pdfr
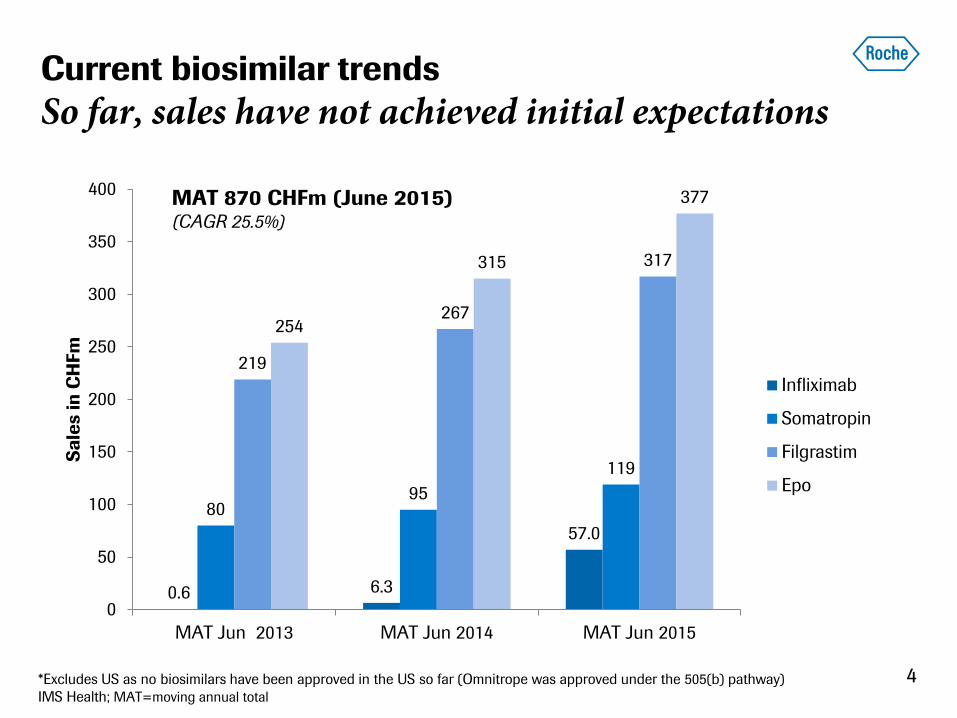
0.6 6.3
57.0
80 95
119
219
267
317
254
315
377
0
50
100
150
200
250
300
350
400
MAT Jun 2013 MAT Jun 2014 MAT Jun 2015
Sa
les in
CH
Fm
Infliximab
Somatropin
Filgrastim
Epo
Current biosimilar trends
So far, sales have not achieved initial expectations
4
MAT 870 CHFm (June 2015) (CAGR 25.5%)
*Excludes US as no biosimilars have been approved in the US so far (Omnitrope was approved under the 505(b) pathway)
IMS Health; MAT=moving annual total
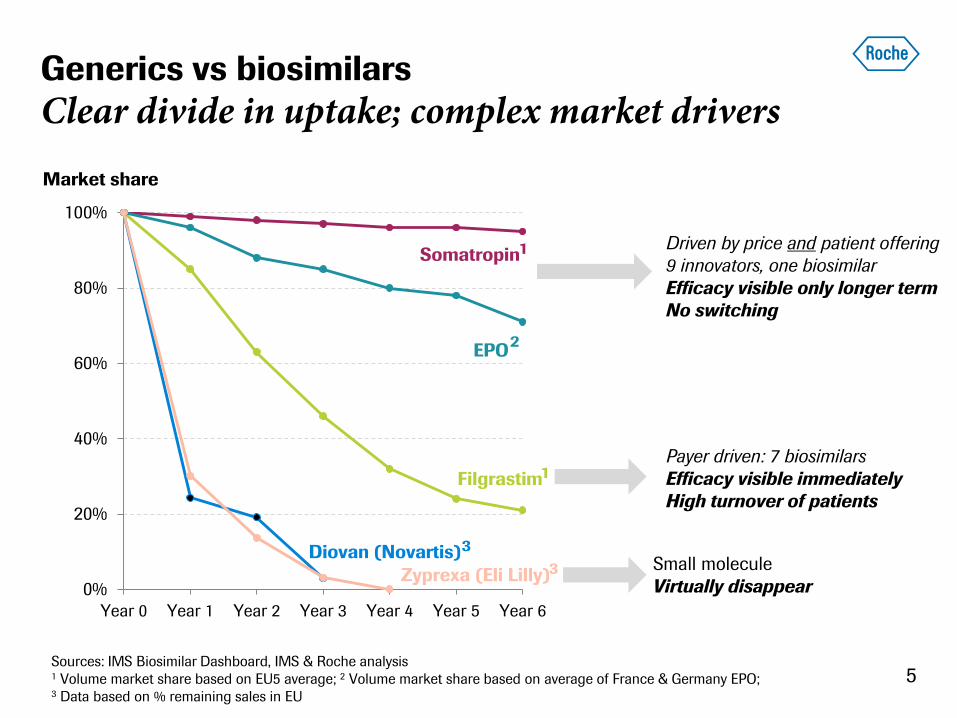
Generics vs biosimilars
Clear divide in uptake; complex market drivers
0%
20%
40%
60%
80%
100%
Year 0 Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
5
Market share
Zyprexa (Eli Lilly)
Diovan (Novartis)
Filgrastim
EPO
Somatropin
Small molecule
Virtually disappear
Payer driven: 7 biosimilars
Efficacy visible immediately
High turnover of patients
Driven by price and patient offering
9 innovators, one biosimilar
Efficacy visible only longer term
No switching
Sources: IMS Biosimilar Dashboard, IMS & Roche analysis 1 Volume market share based on EU5 average; 2 Volume market share based on average of France & Germany EPO; 3 Data based on % remaining sales in EU
1
1
2
3
3
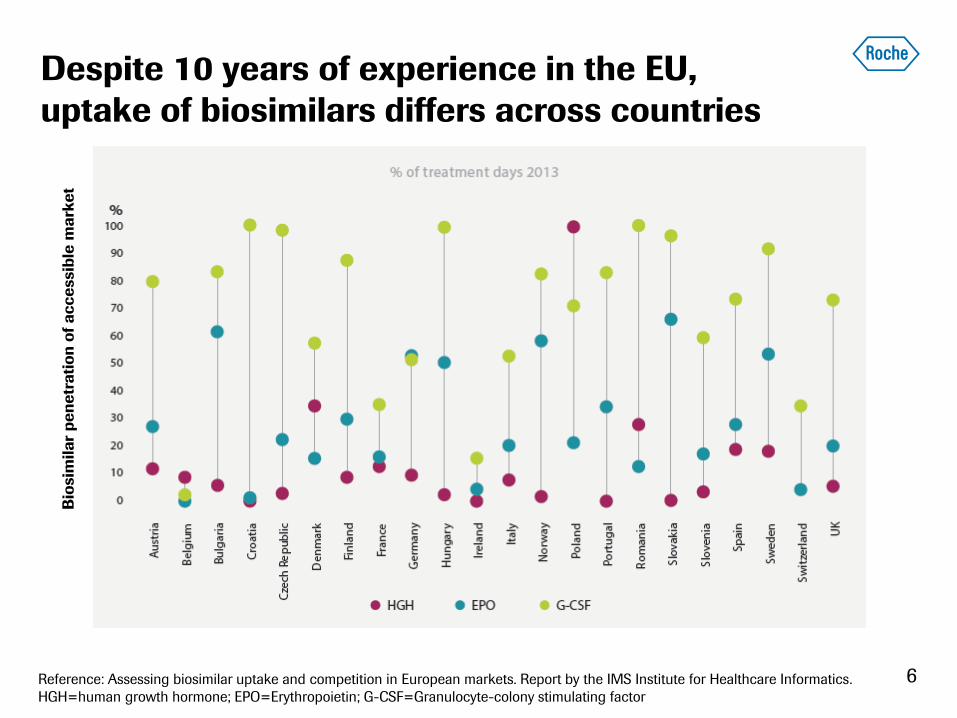
Despite 10 years of experience in the EU,
uptake of biosimilars differs across countries
6
Bio
sim
ila
r p
en
etr
ati
on
of
ac
ce
ssib
le m
ark
et
Reference: Assessing biosimilar uptake and competition in European markets. Report by the IMS Institute for Healthcare Informatics.
HGH=human growth hormone; EPO=Erythropoietin; G-CSF=Granulocyte-colony stimulating factor
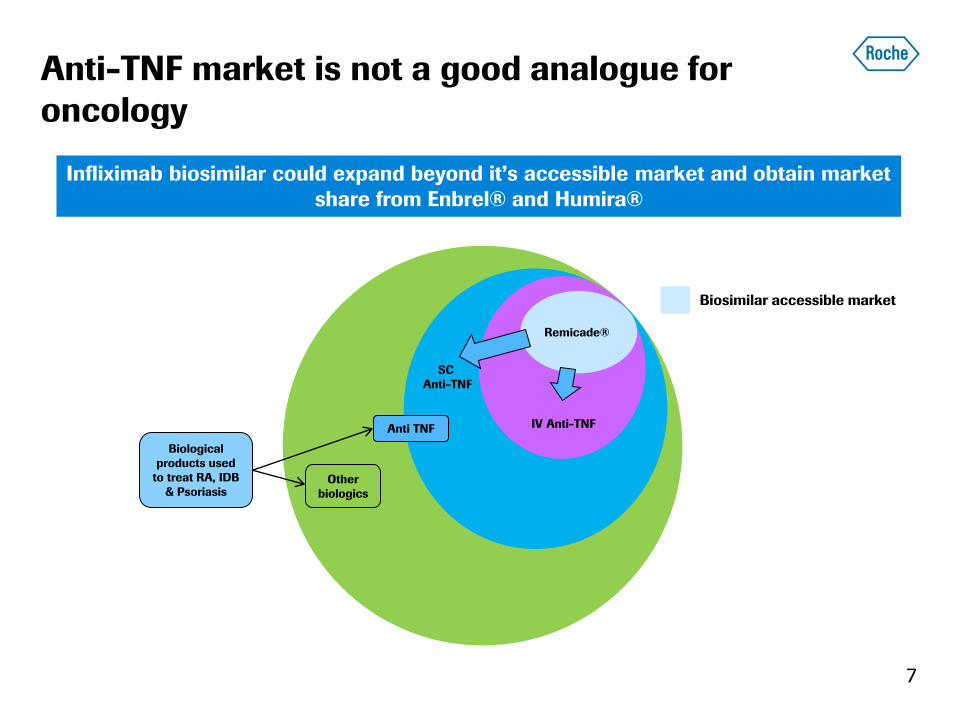
Anti-TNF market is not a good analogue for
oncology
7
Anti TNF
Other
biologics
IV Anti-TNF
SC
Anti-TNF
Biological
products used
to treat RA, IDB
& Psoriasis
Infliximab biosimilar could expand beyond it’s accessible market and obtain market
share from Enbrel® and Humira®
Remicade®
Biosimilar accessible market
Small molecules and biologics
Not all the same
• Small molecule policies allow substituting patients only the price counts
• For biologics, European Medicine Agency (EMA) does not provide
guidance on interchangeability and substitution
• Most countries in Europe have specific policies in place to distinguish
between small molecule and biologic medicines
– Biologics must be prescribed by brand name
– Laws against substitution
– Switching remains a physician’s choice
8
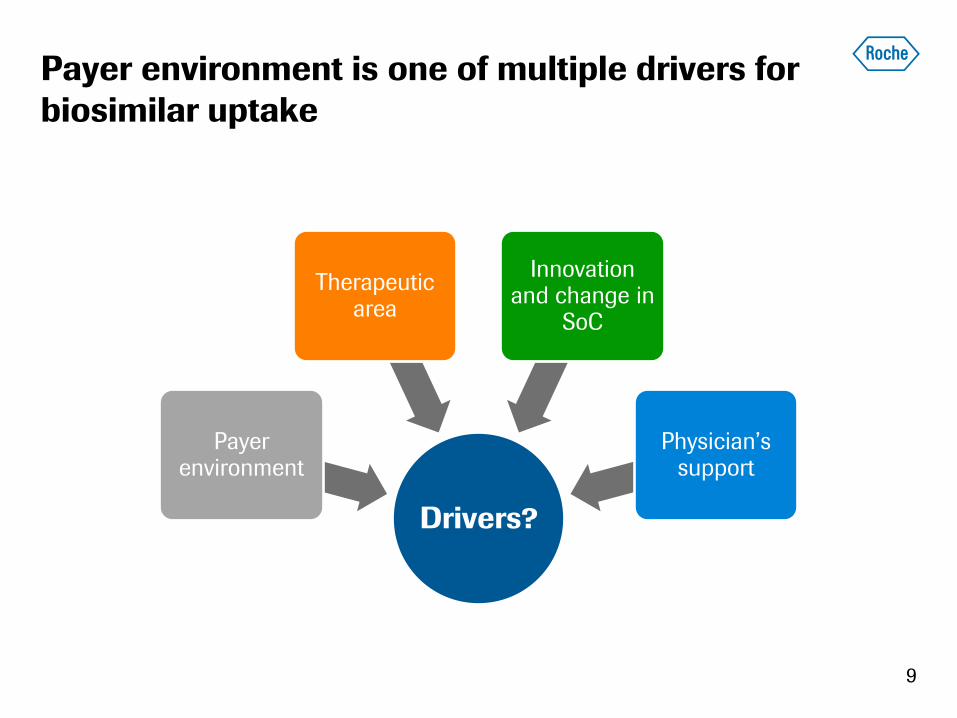
Payer environment is one of multiple drivers for
biosimilar uptake
9
Drivers?
Payer environment
Therapeutic area
Innovation and change in
SoC
Physician’s support
10
Biosimilars: Ten years in the making
Regulatory environment
Summary
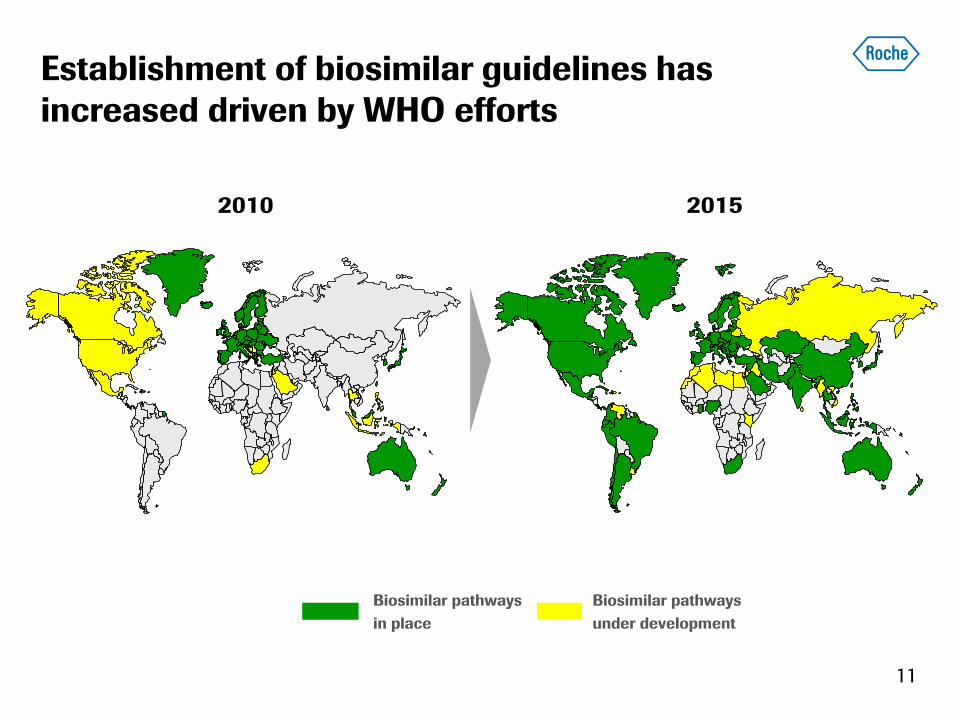
Biosimilar pathways
in place
Biosimilar pathways
under development
2010 2015
Establishment of biosimilar guidelines has
increased driven by WHO efforts
11
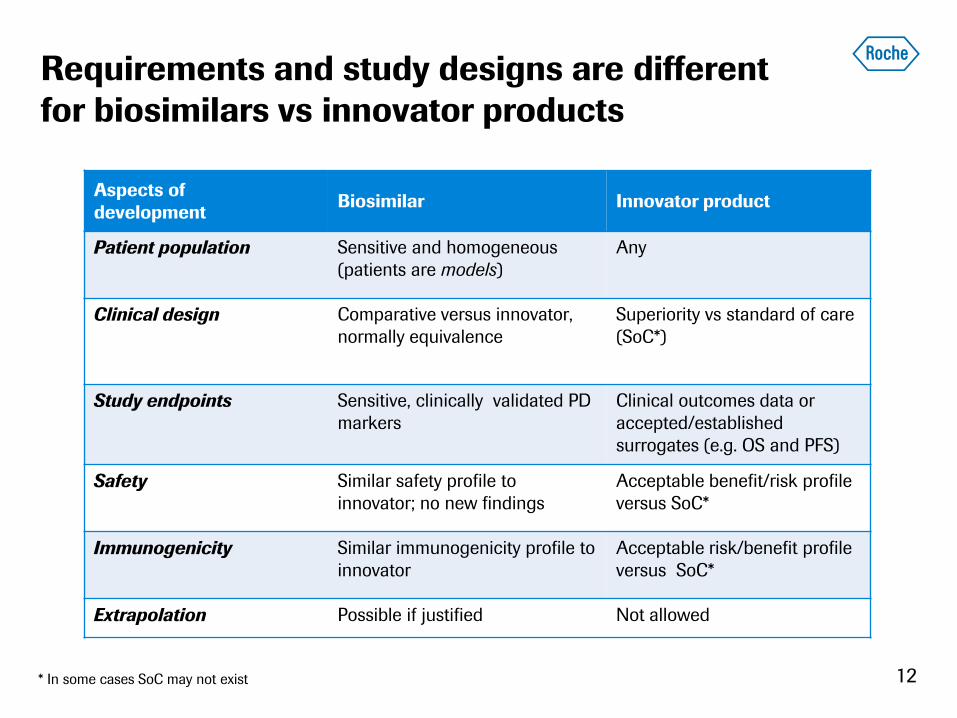
Requirements and study designs are different
for biosimilars vs innovator products
12
Aspects of
development Biosimilar Innovator product
Patient population Sensitive and homogeneous
(patients are models)
Any
Clinical design Comparative versus innovator,
normally equivalence
Superiority vs standard of care
(SoC*)
Study endpoints Sensitive, clinically validated PD
markers
Clinical outcomes data or
accepted/established
surrogates (e.g. OS and PFS)
Safety Similar safety profile to
innovator; no new findings
Acceptable benefit/risk profile
versus SoC*
Immunogenicity Similar immunogenicity profile to
innovator
Acceptable risk/benefit profile
versus SoC*
Extrapolation Possible if justified Not allowed
* In some cases SoC may not exist
How should extrapolation risk be managed?
The regulator’s perspective
13
Analytical
Non-clinical
Clinical
How should extrapolation risk be managed?
The physicians’ perspective
14
Analytical
Non-clinical
Clinical
Analytical
Clinical
Non-clinical
I would like to
see a phase III
trial for each
indication
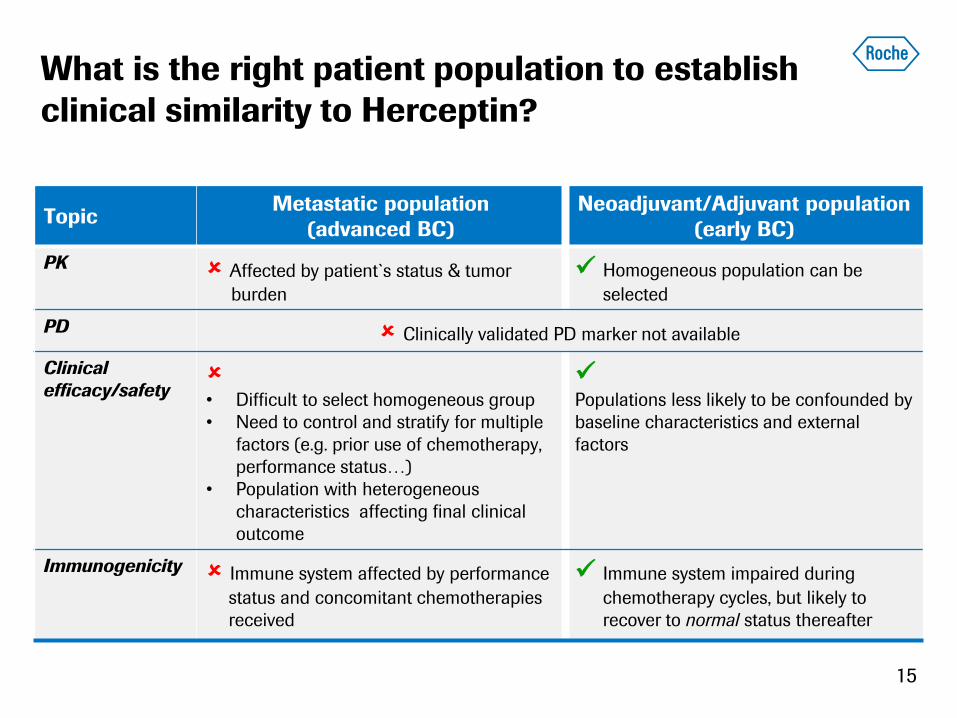
What is the right patient population to establish
clinical similarity to Herceptin?
15
Topic Metastatic population
(advanced BC)
Neoadjuvant/Adjuvant population
(early BC)
PK Affected by patient`s status & tumor
burden
Homogeneous population can be
selected
PD Clinically validated PD marker not available
Clinical
efficacy/safety • Difficult to select homogeneous group
• Need to control and stratify for multiple
factors (e.g. prior use of chemotherapy,
performance status…)
• Population with heterogeneous
characteristics affecting final clinical
outcome
Populations less likely to be confounded by
baseline characteristics and external
factors
Immunogenicity Immune system affected by performance
status and concomitant chemotherapies
received
Immune system impaired during
chemotherapy cycles, but likely to
recover to normal status thereafter
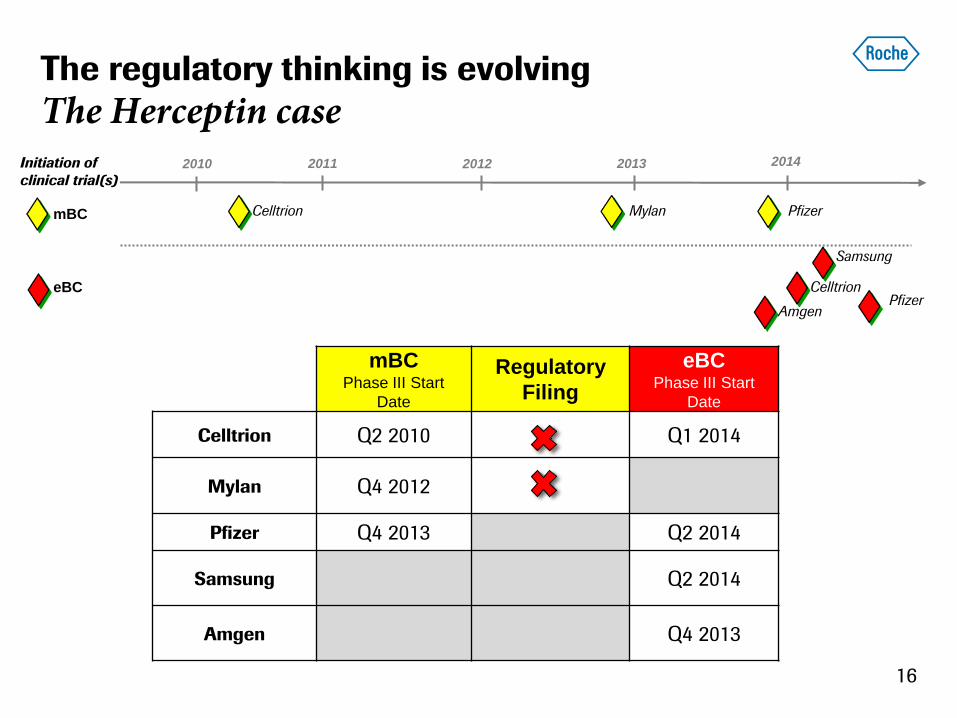
mBC Phase III Start
Date
Regulatory
Filing
eBC Phase III Start
Date
Celltrion Q2 2010 Q1 2014
Mylan Q4 2012
Pfizer Q4 2013 Q2 2014
Samsung Q2 2014
Amgen Q4 2013
Pfizer
Samsung
2011 2012 2013 2014 2010
mBC
eBC
Initiation of
clinical trial(s)
Celltrion Mylan Pfizer
Celltrion
Amgen
The regulatory thinking is evolving
The Herceptin case
16
17
Biosimilars: Ten years in the making
Regulatory environment
Summary
Generics, biosimilars: Not all the same
18
• Small molecules: Policies allow fast penetration of generics
• Biosimilars: Countries in Europe have specific policies in place to distinguish
between small molecule and biologic medicines
– Biologics must be prescribed by brand name, laws against automatic
substitution, switching remains a physician’s choice, EMA - no guidance
on interchangeability
– After 10 years of experience in the EU, uptake of biosimilars differ heavily
across countries
• Regulatory environment: Still evolving with authorities in the process of finally
establishing frameworks; case by case decisions likely












![Lymphoma - ISD Scotland · [DLBCL/Burkitts Lymphoma] MYCDATE Date (DD/MM/CCYY) 10 15 MYC Testing Result [DLBCL/Burkitts Lymphoma] MYCRESULT Integer 2 16 Location of Diagnosis {Cancer}](https://img.pdfslide.net/doc/110x75/5fe202d4c67e945f1a036fa7/lymphoma-isd-scotland-dlbclburkitts-lymphoma-mycdate-date-ddmmccyy-10-15.jpg)















