Embed Size (px)
Citation preview

Basic Principle of Haemodialysis & dialysis machine
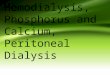
Hemodialysis Machine
Dialysis Process
Concerning the blood, dialysis performs 2 different functions that are normally done by healthy kidneys:
1. Removing excess fluid. 2. Removing waste like urea, and excess electrolytes (chemicals) like potassium,
magnesium, sodium, etc.
The dialysis is performed inside the dialyzer, which is a plastic cylinder, in which the blood enters from the top (the red header), flows through thousands of extremely thin hollow fibers and leaves from the bottom.At the same time the dialysate enters from the bottom (the blue header), flows around and in between the fibers, and leaves from the top.The fibers are semi permeable membranes, that is, smaller molecules in the blood stream can pass through them into the dialysate and bigger molecules as well as blood cells cannot.
Author :Tamer Wagih 1/18

Basic Principle of Haemodialysis & dialysis machine
The dialysate is a water-based solution and its purpose is to absorb from the blood all that should be removed and nothing else.Wastes and electrolytes move from the blood into the dialysate because their concentration in the blood is higher.This process is called diffusion.The dialysate flow ensures that fresh dialysate is present at all times so that the dialysate doesn't become saturated and the process never ends.Fluid is removed from the blood in the same way the kidneys do it - by blood pressure.This process is called Ultra Filtration (UF) and is similar to Reverse Osmosis (RO). In UF, the membrane pore size is larger, allowing some bigger molecules to pass through the pores with the water.The rate at which fluid is removed from the blood is called UFR (UF Rate).There is higher pressure in the blood passing through the dialyzer and lower pressure in the dialysate. This pressure difference is called TMP (Trans Membrane Pressure). The higher the TMP the higher the UFR.As you can see, the dialyzer is doing the job of dialysis. The rest of the machine takes care of supplying the blood and the dialysate to the dialyzer, controls the flow and the pressures, and provides visual indication and alarm when something goes wrong.
Blood flow
The blood pump takes and returns the blood from the patient via the arterial and venous needles.The blood is confined to the disposable plastic tubing and doesn't come in contact with any part of the machine.The blood pump is the distinct feature on all dialysis machines. The pumping is done by squeezing the plastic tube inside the pump using a pair of spring loaded rollers. The suction is done by the elasticity of the tube, which expands after released from the rollers and sucks the blood from the arterial needle.The blood coming from the pump flows to the dialyzer and the blood that leaves the dialyzer returns to the patient through the venous needle.The pump speed, and the resulting blood flow rate, is adjustable from zero to about 600 cc/min.While pump speed is controlled, blood flow rate is displayed. These two usually go hand in hand, but not always.
Author :Tamer Wagih 2/18

Basic Principle of Haemodialysis & dialysis machine
The machine controls the pump speed, so this is the only information that it knows for sure.The blood flow rate is calculated based on the pump RPM (revolution per minute), and the diameter of the tube, entered by a screwdriver driven selector in the pump. The calculated blood flow is displayed.The control doesn't check the real blood flow. It displays blood flow even if the pump turns without the plastic tube installed.The real blood flow may differ from the display because of:
Internal reverse leak; the rollers never squeeze the tube completely so not all the blood is pushed forward, a little goes backward.
High arterial and/or venous pressure reduces the ability of the pump to suck or to deliver.
Any speed above some low value reduces gradually the blood flow. It has been found that with a display of 600 cc/min the actual blood flow was 500 or less.
In addition to the inherent features of the pump, a human error that may reduce blood flow is the way the plastic tube is installed in the pump.If the plastic tube inside the pump is too tight it cannot expand to its full volume, so the suction is reduced and the pump delivers less blood flow than the display indicates. In this case the tube forms a triangle that doesn't make full contact with the inside outline of the pump, in contrast to the desired semi-circle shape.In many newer machines the total BVP (blood volume processed) is also displayed. Remember that this number is calculated form the pump speed and depends upon internal calibration.Along the blood lines there are two pressure chambers that are used for gauging the blood pressure without touching the blood. There is a short tube from each chamber that should be connected to the machine's pressure input via a small filter. The filter prevents contamination of the machine with blood if the chamber overflows, however, once blood gets into the filter it is blocked and should be replaced.Both pressures are displayed on the machine in prominent locations. They can't be missed.They are measured in mmHg (mm Mercury), the same units that are used when measuring blood pressure with a cuff.Each pressure display has a preset for max/min values, which if reached stop the pump and start the alarm.The first display is the arterial pressure, which in most machines measures the negative pressure of the suction.In very few centers the arterial pressure is measured after the pump and it shows the positive pressure where the blood enters the dialyzer.The second gauge measures the venous pressure where the blood is returned to the patient.
Author :Tamer Wagih 3/18

Basic Principle of Haemodialysis & dialysis machine
In addition, an air detector is attached to the venous chamber. Air in the blood is very dangerous, therefore even a small amount of air or foam stops the machine and starts the alarm.At the exit from the venous chamber there is a valve that closes the line whenever the pump stops, to prevent uncontrolled blood flow in or out of the venous needle.
Dialysate Bath
The dialysate bath is a water-based solution. The term "Dialysate bath" is historical - in the early machines there was a 30-50 gallon bath where the dialysate for the whole treatment was pre-prepared.With all contemporary machines, the dialysate concentrate is fed into the machine, water is fed from a water tank and a marvelous pump mixes them to the desired concentration.Today, the term "Dialysate bath" means the kind of dialysate prescribed by your neph.Why do we need the concentrate and don't use pure water instead?Because the electrolytes in the blood shouldn't be removed completely. Too low level of sodium, potassium, calcium, phosphorus, magnesium, and other electrolytes, is as dangerous as high level. The dialysate contains these electrolytes in appropriate concentrations that prevent removing too much of them from the blood.Two of these electrolytes can be set as needed in the dialysate bath.
Calcium (Ca) can be 3.5, 2.5, 2 mEq/L, depending upon the patient's calcium. (US units; Ca 3.5 mEq/L equal 1.75 mmol/L).Some patients use lower calcium bath so they can take more calcium-based phosphate-binders.Also when the PTH is high the calcium level in the blood is elevated and low calcium bath is used.
Potassium (K) can be 4, 3, 2, 1 mmol/L, or zero (free-K). (US units, used internationally).4 is for patients that make a significant amount of urine and should not clear any potassium from their system.3 is for patients that make some urine, 2 is for patients w/o any kidney function, 1 is used occasionally for patients with high potassium when needed. Free-K is rarely used and only in extreme cases of high potassium (like after surgery), and should be used only for an hour or so at he beginning of the treatment (to avoid removing too much potassium).
Note that the low limit for potassium in the blood is 3.5.Beware! A patient that comes with K=5.5 and uses 2K bath may leave with K=3.5, but a patient that comes with K=4 with same 2K bath may end up in the ER or worse...
Author :Tamer Wagih 4/18

Basic Principle of Haemodialysis & dialysis machine
Tell the staff if you took Kayexalate or had a severe diarrhea the day before your treatment. Better safe than sorry. Your bath is prescribed by your neph. How can you tell whether the right bath is used for you?In many centers there is a central distribution system for the concentrates and different lines are used for the various concentrates, so ask your tech which line is the one you need.In some other centers there are 2 jugs at the machine - one for acid (or acetate) and one for bicarb (bicarbonate). The acid jug should be marked with the potassium and calcium values.
Dialysate flow
The dialysate pump, in addition to mixing the concentrate with water, moves the dialysate through the dialyzer.This pump has adjustable flow rate. For regular dialysis at blood flow up to 250 cc/min the dialysate flow should be 500 cc/min. For more efficient dialysis, called high flux, the blood flow is 400-500 cc/min and the dialysate flow is 800 cc/min.In addition to the controlling the flow, this multi-function pump controls the pressure of the dialysate as to achieve the desired TMP and hence the desired UFR.
Conductivity
The dialysate concentration is expressed in terms of electrical conductivity of the prepared dialysate and displayed constantly.The conductivity is expressed in mS/cm (milli-Siemens/centimeter). The conductivity of pure water is zero and that of the dialysate depends on the amount of sodium in it. While there are many electrolytes in the dialysate, sodium is the major componenet. Different amount of potassium or calcium hardly make any noticeable change.The base conductivity is set by the maintenance tech and should be about 13.8 mS/cm. This is about 138 mmol/L of sodium, like in our blood. For some this is too low and step sodium modeling (see below) can be used to raise it to 14.0-14.2.Remember that the actual conductivity depends upon the calibration of the machine. That's the reason why you may feel different on different machines.Also the concentrate has its own deviations between different production batches.If there is not enough concentrate the conductivity goes down and the machine beeps.Sometimes there are visible bubbles in the lines, which make the conductivity behaves erratically.Note that low bicarb is unsafe but hardly changes the conductivity. To
Author :Tamer Wagih 5/18

Basic Principle of Haemodialysis & dialysis machine
protect yourself, once in a while watch the conductivity and check for bubbles.
Sodium Modeling
Excess fluid in the body is accumulated in the blood and in the tissues. The UF removes fluid from the blood and that causes the fluid from the tissues to flow into the blood. Electrolytes are also removed with the fluid.When too much fluid is removed in a short period of time, too much sodium is removed from the tissues and that causes cramps and low blood pressure, usually during the last half of the dialysis.To compensate for the sodium loss, sodium modeling is used.When set, it increases slightly (up to 7%) the amount of concentrate in the dialysate and therefore there is more sodium, which is indicated by higher conductivity.The sodium attracts water so it helps to extract excess fluid from the tissues without removing sodium from them and therefore avoiding cramps. Later the sodium is dialyzed.What about the potassium and calcium? They too go higher, however, a few percent increase in sodium is a big diference but increasing the potassium from 2 to 2.14 is insignificant.The sodium modeling setting includes:
Amount, usually up to 7% above normal, or sodium of 148 mmol/L (up from 138).With setting of 148 the conductivity is about 14.8-15.
Time to stop. One of 3 programs:
1. Step. A constant dose of sodium is given during the first 30 to 60 minutes of treatment.
2. Linear. Begins the sodium on high and linearly reduces it along the dialysis to zero.
3. Exponential. Similar to Linear but with exponential slope (less sodium is given).
The need for sodium is higher when the patient gains more fluid weight, which means that it should be set according to actual fluid gain.Trouble is, sodium modeling should be prescribed be your nephrologist, but not all doctors are updated with all the tricky features of every machine.
UF Profiling
Author :Tamer Wagih 6/18

Basic Principle of Haemodialysis & dialysis machine
UF profiling makes it possible to remove more fluid with less risk of cramps and low blood pressure.In contrast to constant UFR, the rate at which fluid is removed from the blood is reduced as the amount of fluid coming from the tissues is reduced, thus avoiding patient's blood pressure drop.Another way to look at it is that no one cramps in the first hour, so why not remove more fluid then?UF profiling works best with sodium modeling.The Fresenius 2008H has 8 built-in UFR profiles. 4 are preset and 4 can be programmed.The built-in functions in the Fresenius let you increase the UFR by up to 50% at the first hour and reduce the last hour by the same amount. The preset programs include various combinations of reduced UFR and/or intermittent low UF. The only way to tell which one is best for you is to try, but usually one program is used for all patients (if used at all).
UF Only
To be able to remove a lot of excess fluid without cramps the dialysate pump can be turned off for the last (or extra) 30 to 60 minutes while the UFR is set to 2000 cc/hour (or as much as needed).It is called UF Only or Strictly UF.These terms signify that there is no diffusion, just UF. Waste and electrolytes are removed with the fluid by convection without changing the concentration in the body and hence without cramps.Note that sodium modeling is disabled because there is no dialysate flow.
Blood Leak
Blood may leak inside the dialyzer because of ruptured fibers. This may happen even with a new dialyzer.There could be a minor leak, which is invisible, or a major leak in which blood can be seen in the dialyzer.In both cases the machine stops and sets the alarm. To resume dialysis the dialyzer should be replaced.The techs have a rule of thumb - if the leak cannot be seen the blood in the dialyzer can be return to the patient and if it can be seen the blood should be discarded.I personally would be afraid to get the blood back because of possible flow of dialysate into the blood.In any case some blood can be returned safely - this is the blood in the
Author :Tamer Wagih 7/18

Basic Principle of Haemodialysis & dialysis machine
arterial line. Saline can push the blood from the arterial chamber and the tubing back to the arterial needle.
Heparin Pump
This pump delivers heparin to the blood tubing. The pump is a regular syringe that is pushed by a controlled motor.On all machines the rate can be adjusted. On newer machines the end time can be programmed too.Usually an initial dose of heparin is given when the treatment begins, then the pump delivers heparin until one hour before the end. Note that not all patients need continuous heparin.In case of a patient after surgery or another kind of bleeding, heparin is used sparingly or not at all.To avoid clotting in the dialyzer it is rinsed with 100 cc saline every hour or so. In spite of that, the blood in the dialyzer may clot, but unless the patient has a very low blood count no treatment is required (of course the heparin dose should be increased when possible).
Temperature
To make it more convenient for the patient, the dialysate temperature can be set to a desired value, so the blood returning to the patient will not be too cold. For most patients a setting of 37 C (98.6 F) is ok.Some staff and patients believe that a higher temperature reduces the blood pressure - I don't think that one-degree can make any significant change to the blood viscosity.However, in many centers all machines are set to the same temperature, and in many cases it is too cold, in addition to the freezing air-condition.
Alarm
Exceptions in the machine operation trigger the alarm.There is a red alarm light and an audible beep.There is a mute button to stop the beeping but if the problem persists the beeping is resumed after a short period of time.There are many reasons for the machine to alarm: the reason is either indicated by a light or a message.Most exceptions, but not all, shut down the pump. Don't be alarmed unless no one shows up in a couple of minutes.If the pump stops there is a risk of clotting inside the dialyzer.
Author :Tamer Wagih 8/18

Basic Principle of Haemodialysis & dialysis machine
Note that some machines stop the clock under alarm conditions and your dialysis will be longer.
Tricks of the Trade
Below is some info that can make the difference between feeling well and feeling crummy.First ask to turn the machine towards you so you will be able to watch it.Make yourself familiar with the various components and displays.Your tech can help you with that. Most techs like to answer patients who show interest.Never touch the machine before you know exactly what is going to happen and how to reverse it if you make a mistake.Find out where the remaining-time is displayed, you'll love this one.When the machine is out of concentrate the dialysate conductivity goes down and the dialysate flow into the dialyzer is bypassed. This triggers the alarm but doesn't stop the pump. Consequently the TMP goes down and this may stop the pump. After a tech replaces the concentrate jug it takes a few minutes to resume the correct conductivity and the staff will be more than happy if you mute the alarm until it becomes ok.Another case is when there is a problem with the water supply and all machines start beeping.Also if the pump stops you can restart it by the start pushbutton, but first be sure that you don't have infiltration...Before you attempt to set your own UF watch the techs doing it and discuss it with them.If you show interest and knowledge the rest will be easy.
The Beginning
Before the patient is connected, the machine should be setup and rinsed.Here are the connection instructions for a tech or a home hemo patient.If you do in-center dialysis, watch the tech as s/he is doing this procedure.
Start the setup by connecting the dialysate lines to the dialyzer.Since the dialysate enters from the blue line you connect the red line first, so when you connect the blue line and dialysate flows in, you are sure that it has a way out.The dialyzer should be mounted with the red header up for a few seconds until the dialysate fills the dialyzer.
Author :Tamer Wagih 9/18

Basic Principle of Haemodialysis & dialysis machine
Connect the blood lines to the dialyzer. Make sure that the red blood line and the red dialysate line are connected to the dialyzer on the same side.
The rest of the setup should be performed according to the protocol in your unit. When the setup is complete the arterial and venous blood lines are connected
together. The blood tubing and the dialyzer are rinsed by re-circulating saline through
them.At that time the UFR should be set to no less than 300 cc/hour and should be on, and the saline line should be unclamped. Without UFR the dialysate will enter the blood lines and may even go back to the saline bag.With UFR, fluid from the lines plus the re-use agent are flushed down the drain. Usually a full bag of 1000 cc saline is used. In the case of a new dialyzer it is recommended to rinse it with 2 bags because some patients are allergic to small fibers left inside the dialyzerTo remove air from the blood lines and dialyzer, the machine should run for a few minutes with the dialyzer mounted upside down, that is, the red header is down and the blue one is up.In this position the saline flows up, air leaves the dialyzer and is trapped in the venous chamber.
If the dialyzer re-use process is done with formaldehyde or Renalin, a sample of the saline from the blood line should be tested to be free of any residual contamination. Continue with rinsing until the test stays clear.
Before connecting the patient the lines should be free of air. If the saline bag becomes exhausted and air enters the dialyzer it must run again with saline until absolutely no bubbles can be seen.Remember that even if just a small amount of air is left in the blood lines, once they are filled with blood this air becomes foam and causes the air detector to shut the pump down. This may take a tech 5 to 15 minutes to fix; sometimes the patient should be disconnected and the blood must re-circulate for a few minutes.
Once everything is ready the dialyzer should be mounted in the normal way, that is with the red header up.This ensures that no air is trapped in the dialysate side of the dialyzer.
Time for the needles.While doing the needles let the machine continue with the rinse.
Connect syringes to both needles and make sure that the clamps are unclamped.On most needles there are inline clamps. If not you have to use regular clamps.If the patient receives heparin use the syringe on the venous needle for that.
Insert both needles and tape them according to protocol.I hope that you are not going to learn how to do it from my website....Check that you can pump the blood easily in and out, then return the blood to the patient and clamp the needles.
Stop the pump, clamp both arterial and venous lines and clamp the saline line coming from the saline bag.
Author :Tamer Wagih 10/18

Basic Principle of Haemodialysis & dialysis machine
Disconnect the arterial line from the venous line as they were connected for re-circulation. Hang the venous line on a bucket, or drain, make sure that it doesn't touch anything (use the inline clamp as a hanger).
Check once more that all four clamps are clamped (needles and blood lines). Remove the syringe from the arterial needle and connect the red arterial line to the
arterial needle. Unclamp the arterial needle and both blood lines. Turn the pump slowly 100-200 cc/min. Check your unit protocol. The blood flows out of the arterial needle and into the dialyzer. As the blood enters the dialyzer check that there is no visible blood leak at the top
of the dialyzer.If blood is visible stop the pump immediately, replace the dialyzer and start the re-circulation again.
As the blood goes in the saline goes down the drain. Be sure that the levels in both arterial and venous chambers are not too low or too high.
When a slight blood color is seen in the blood line exiting from the venous chamber clamp the venous line and stop the pump.
Connect the blue venous line to the blue venous needle line. Unclamp both clamps on the venous line and needle. Start the pump, increase the speed gradually to the ordered blood flow while
watching the venous needle for signs of infiltration (swelling) and checking both arterial and venous pressures to be in range.
Clear the UF display, set the desired time and goal and start the UF. If ordered start the heparin pump and sodium modeling. Once everything runs smoothly, double check the machine to ensure that nothing
has been overlooked.
Blood Flow Rate (BFR)
There is a misconception concerning BFR and heart overload.The heart is overloaded constantly by the extra blood it has to circulate through the shunt.Pumping the blood during dialysis doesn't add to the overload.For example, if you have 1000 cc/min flow in the shunt and your BFR is 400 cc/min, the blood pump doesn't change the total shunt flow, it just takes 400 cc/min from the arterial needle and returns it through the venous needle. In the area between the two needles the blood flow is 600 cc/min.Of course the BFR cannot be higher than the flow through the shunt. As a rule of thumb, it shouldn't be higher than 50% of the shunt flow.The rate of waste removal increases as the blood flow increases until BFR is about one half of the DFR (Dialysate Flow Rate). Increasing BFR beyond that doesn't help much. Reducing BFR requires more time for adequate dialysis.
Author :Tamer Wagih 11/18

Basic Principle of Haemodialysis & dialysis machine
BFR setting is directly linked to the arterial and venous pressure as explained next.
Arterial & Venous Pressure
These pressures are the result of the blood forced to flow through the plastic tubing, the dialyzer, and the needles.The venous pressure is positive while the arterial pressure is negative (in most centers).Note: higher negative pressure means a higher magnitude but a lower pressure.Pressure difference as a result of flow depends upon a few factors (in addition to the patient shunt that can affect the pressure because of its size and blood flow):
Blood flow rate.The effect of blood flow is easy to follow - any change in pump speed is immediately reflected on the pressure displays.The higher the flow the higher the pressure.In fact, both pressures represent the blood flow rate more accurately than the pump display.For instance, if there is a kink in the arterial line less blood can flow. In this case the pump display doesn't change, the arterial pressure will be more negative and the venous pressure will be lower.If the limits are set correctly the pump should stop.
Blood viscosity.Blood viscosity is affected by its HCT (percentage of solids in the blood), and slightly by the temperature (because the temperature changes are very small).Here is a piece of info that is not so common:With all other factors equal, the higher the blood count the higher the pressure.
Cross-section of the tubes and needles.The cross section of the tubing is fixed (too bad if it is not). The only variable is the needles.The smaller the needles the higher the pressure.
Needle gauge color code:#14 white--largest#15 blue#16 green#17 orange#18 pink---smallest
What is important about the arterial pressure.When the blood flow rate increases the arterial pressure becomes more negative. If it is too negative the red blood cells may break down.
Author :Tamer Wagih 12/18

Basic Principle of Haemodialysis & dialysis machine
This is called hemolysis.To be on the safe side never let the arterial pressure go below -220 mmHg. If it goes below that the pump speed should be reduced.If your blood count is low and you are on Epo and iron you may notice that the pump speed should be reduced as your blood count goes up. I had this problem with blood flow above 400 cc/min when my Hgb was above 12.Warning:In some centers they don't connect the arterial pressure gauge, to enable running at speeds as high as 600 cc/min without beeping and therefore reducing the dialysis time. This practice is dangerous and against the manufacturers' instructions.In addition to the risk of hemolysis, there are no pressure limits to shut down the pump in case of emergency.It should be noted that running the pump at 600 cc/min doesn't mean that this is the real blood flow, and running faster doesn't make the cleansing better either. The diffusion takes time, and the blood shouldn't rush through the dialyzer.Every dialyzer has a graph that shows the urea clearance per minute vs. blood speed and dialysate speed. The optimum is achieved when blood flow rate is about half of the dialysate flow rate.Reasons to shut down are:
The arterial needle becomes loose or dislodged.The pump sucks air through the needle and generates a typical sound.If the pump doesn't stop, air enters the dialyzer. The patient is still protected from the air by the air detector, but after the needle is fixed, air in the dialyzer generates foam, which is hard to get rid of.
The arterial blood vessel doesn't supply enough blood. This may occur when the patient raises his/her hand, or when the needle is too close to the blood vessel wall. If the machine doesn't stop the blood vessel may be damaged and the patient may feel a sharp pain.This may also occur if the arterial line has kinks.
What is important about the venous pressure.First, the venous pressure gauge must be connected or the UFR won't work.Reasons to shut down are:
Blood flow is obstructed before the chamber, e.g. the dialyzer is clotted.In this case the venous pressure goes down
Blood flow is obstructed after the chamber.This occurs if the venous needle is clotted or not in the vein because of infiltration.Also, there is a filter in the venous chamber to prevent particles and clots from entering the blood stream.This filter may be clogged.
Author :Tamer Wagih 13/18

Basic Principle of Haemodialysis & dialysis machine
The venous needle is dislodged.
Once you know your usual venous pressure be alerted if it changes. Normal pressure shouldn't be above 200 mmHg unless your blood pressure is really high.Most technicians tend to reduce the pump speed when the pressure goes up, and you must be watching.
UF & UFR
In modern dialysis machines either UF or UFR can be set.When UF is set it is called Goal; that's how many grams or cc of fluid to remove. Treatment time should also be entered so the control can calculate the UFR and the TMP. This is the way it is done in most centers.The control is sophisticated enough to recalculate the UFR if the goal is changed during the treatment.Also UF profiling can be selected from a menu.If the goal is set to zero, UFR can be programmed. The UFR should be calculated and can be modified to perform manual UF profiling.Although this sounds very simple, it is not, because in every center the Goal is defined differently.You may think that the goal should be your weight minus your dry-weight. Wrong!In many units the techs have a one-size-fits-all way of setting the machine, for example, all patients should remove no less than 2 kg.Even if dry weight is used, it should be noted that this number is not set in stone.In addition to weight gain or loss, there are cyclical changes of one kg or more, as we eat more or less, do physical activity, or have mood changes.And there are changes due to different clothes, constipation, period, or what have you.Once you "feel" your body you should tell the tech what your goal is for every treatment.Now suppose we determine correctly the amount of fluid to remove.If you plan to drink during the treatment the amount you drink should be added to the goal.But in many centers the techs add 0.5 kg on top of that.Why?They calculate the saline that you receive at the beginning and the end (prime and rinse-back) as 250 cc each.Not true! The total volume of the tubing and dialyzer is about 250-300 cc.
Author :Tamer Wagih 14/18

Basic Principle of Haemodialysis & dialysis machine
The tubing is filled with blood before the venous line is connected, so you may receive about 50 cc of extra saline at the beginning and not 250 cc. The same is true at the end. I never considered these values in determining my UFR.But there is more to this. New patients may still make urine.Patients with PKD may urinate everything they drink and they need dialysis to remove waste only.So if you have no fluid restriction, you need no UF at all. Anything you drink on the machine should be ignored, same as drinking at home. Dry weight is meaningless since your kidneys keep the fluid balance in your body.To record your weight, go to the bathroom before you step on the scale.But that's not the end of the story.The UFR should never be set to zero.Most machines won't let you set it to zero, but that's not the reason.Remember that the ultra filtration is the result of TMP - higher pressure in the blood pushes fluid through the membranes into the dialysate. Zero UFR means zero TMP.When the TMP is too low or zero, dialysate ingredients, as well as water, move from the dialysate into the blood.If the water is not absolutely pure, bacteria can move into the blood as well.This is called Back filtration.This is more important with high flux dialyzers because less TMP is required for fluid removal.With the F80 dialyzer that I used, the lowest UFR that I would set is 300 cc/hour.If you don't need UFR, the amount removed should be compensated by either drinking it or receiving 300 cc saline every hour. If you have high BP, remember that a liter of saline contains 9 grams of salt, (but the liter of fluid removed from you contains salt too).
URR, Kt/V & Treatment Time
URR stands for Urea Reduction Ratio, and it is expressed as a percentage.This is an easy to measure approximation of dialysis efficiency based on a 3-4 hour treatment.If you begin your treatment with pre-Bun of 100 and your post-Bun is 30, then the URR is 70%.URR = 100 * (pre - post) / preURR doesn't take into account the change in weight due to UF, and the generation of urea during the treatment.
Author :Tamer Wagih 15/18

Basic Principle of Haemodialysis & dialysis machine
URR can never be 100% because even if you run a very long time your Bun will never reach zero as new urea is constantly generated. The true value of URR is therefore a few percent higher.A more accurate (and more complex) way to express efficiency is Kt/V (pronounced K. t. over V)Kt/V natural logarithm formula:Kt/V = -Ln (R - 0.008 * t) + (4 - 3.5 * R) * UF/WIn which:Ln is the natural logarithm;R is the post-dialysis-Bun / pre-dialysis-Bun;t is the dialysis session length in hours;UF is the ultra filtration volume in liters;W is the patient's post-dialysis weight in kgThe accepted values are:URR > 65%Kt/V > 1.3Kt/V of 1.3 is roughly equivalent to true URR of 72%Note: In PD, URR cannot be measured. Kt/V is calculated based on creatinine clearance, so don't compare.If your numbers are too low you don't get adequate dialysis and your treatment time should be increased.Remember that the true effectiveness of your treatment is not only the removal of urea.The greatest benefit of longer treatment is removal of medium size molecules, like Beta Globulin, and better clearance of phosphorus. The clearance of these molecules is not measured in the monthly labs.Another advantage of longer treatment is that the process is slower and easier on the body.
The End
Time to be disconnected from the machine. The pump stops.This can be done in 2 ways.
1. The arterial line connected to the needle is released.The saline line is released and connected to the free arterial tube.The pump is turned on at 100-200 cc/min and the blood is returned to the patient.When the blood is completely returned the pump is stopped.In many centers the 1.5 cc of blood in the arterial needle is pushed back by saline.When done the patient can be disconnected.
2. The arterial line below the saline connection is clamped.The saline line is open.The pump is turned on at 100-200 cc/min to return the blood in the dialyzer.When the blood is completely returned the pump is stopped and the clamp is released.
Author :Tamer Wagih 16/18

Basic Principle of Haemodialysis & dialysis machine
The blood in the arterial line is returned via the arterial needle.When done the patient can be disconnected.
While the blood is returned the tech may kink the blood lines by hand or by a clamp to release blood cell attached to the tubing.What's my take:The first method is susceptible to contamination, but I have never seen one happen.On the other hand the blood flow is controlled by the machine and goes the same way that it did during the treatment.The second method is also called emergency take-off because it is the fastest way to disconnect.This method leaves the system closed, but returning the blood via the arterial needle may cause infiltration.The worst is when the tech wants to make it short and squeezes the saline bag. In this case the blood flow into the shunt is uncontrolled and may cause damage. I have never seen that one happen either.I prefer this method when I do it myself because I can do it with one hand.If it is done by a tech I always warned them not to squeeze.
Power Failure
What if the power goes off and you are connected?In many centers, and of course in hospitals, there is a backup generator.But what if there isn't?The blood shouldn't stay in the dialyzer for more than a few minutes.In all machines there is a handle for rotating the blood pump by hand. In the Fresenius machine it is built into the pump.Ask your tech where and how this is done on your machine.Before you can start, the venous line coming off the venous chamber should be released from the safety valve (which blocks the flow when the pump is off).Follow the emergency take-off protocol and turn the pump manually when needed.
Fire Alarm
In case of fire it is essential to leave the place as soon as possible.Returning the blood may take a couple of minutes. This is too risky.The fastest way out is to clamp both needles and their connecting tubes (4 clamps), disconnect the lines and run for your life. Don't care about the pump - it will shut down automatically. To be on the safe
Author :Tamer Wagih 17/18

Basic Principle of Haemodialysis & dialysis machine
side, carry a small cutter with you. In case of total confusion clamp the lines and cut them between the clamps.Consult your nurse in charge about their fire alarm protocol and fire drills. (Don't be surprised if they don't have any).
Good luck!
Author :Tamer Wagih 18/18