Embed Size (px)
Citation preview

Kidney International, Vol. 39 (1991), pp. 1020—1026
Hemodialysis with cuprophane membrane modulatesinterleukin-2 receptor expression
PHILIPPE ZA0uI, WAYNE GREEN, and RAYMOND M. HAKIM
Division of Nephrology, Department of Medicine, Vanderbilt University Medical Center, and Histocompatibility Laboratory, VeteransAdministration Medical Center, Nashville, Tennessee, USA
Hemodialysis with cuprophane membrane modulates interleukin-2receptor expression. Chronic dialysis patients have several indices ofimmune deficiency. We examined the hypothesis that the biocompati-bility of dialysis membranes may influence the ability of lymphocytes toexpress interleukin-2 (IL-2) receptors on their surface, a key event incellular immune response. We investigated the potential role of thedialysis membrane in eight chronic hemodialysis patients. The studydesign was a cross-over study using cuprophane and polyrnethyl-methacrylate (PMMA) membranes. Chronic dialysis with new Cu-prophane membrane leads to an increase in baseline expression of thetwo subunits of IL-2 receptors, IL2Ra (p55, CD25) and IL-2R/3 (p7°), inperipheral blood mononuclear cell (PBMC). However, Phytohemagglu-tinin (PHA) stimulation of PBMC harvested after two weeks of dialysiswith cuprophane membrane showed a markedly decreased expressionof high affinity 1L-2 receptors. These findings are reversed whenpatients were dialyzed with a PMMA membrane which is also associ-ated with minimal complement activation. The increased expression ofIL-2 receptor subunits are reproduced in vitro by direct contact ofPBMC with cuprophane membrane and by the addition of the anaphy-latoxin C5a. This study confirms the participation of lymphocytes in thecomplex blood-membrane interactions that occurs during dialysis; theresults may be relevant to observations of immune deficiency in dialysispatients.
Cuprophane hemodialysis membranes have been shown toactivate several pathways of the inflammatory response, as wellas cellular elements such as neutrophils, monocytes and plate-lets [1—4]. These inflammatory responses are less evident withnon-cellulosic membranes such as the polymethylmethacrylate(PMMA) or polyacrylonitrile (PAN) membrane [3].
Lymphocytes have been assumed to be passive bystanders inthis complex blood-membrane interaction, although minorchanges in lymphocyte count and subsets have been demon-strated [1, 5, 6]. Recently however, specific markers of lym-phocyte activation such as increased numbers of T-lymphocytebearing interleukin-2 receptors (TAC antigen) and increasedsoluble interleukin-2 receptor levels have been demonstrated indialysis patients [7, 81.
IL-2 receptors (IL-2R) are complex and made up of at leasttwo subunits: a and /3 [9]. The IL-2Ra subunit (also known asTAC antigen, p55 or CD25) is expressed de novo; its expression
Received for publication June 26, 1990and in revised form December 21, 1990Accepted for publication December 22, 1990
© 1991 by the International Society of Nephrology
is an index of lymphocyte activation and the extent of activationis expressed as the percent of circulating IL-2Ra positive cells[10]. The /3-subunit (IL-2R/3) also known as p70 subunit isexpressed constitutively on resting T-cells and is regulatedseparately [11]. However, increased expression of IL-2R13 isalso considered a hallmark of lymphocyte activation [11, 12].These subunits have low affinity for IL-2, but their associationresults in a smaller number of receptor complexes, IL-2R, withhigh affinity for IL-2 (Kd — 10 pM) [13]. Several studies haveindicated that this high affinity receptor is uniquely involved inthe rapid binding and internalization of IL-2 and mediates mostof its biological activities [13—16]. Defects in the ability ofT-lymphocytes to express high-affinity IL-2 receptors are asso-ciated with impaired lymphocyte responses in a number ofdiseases [17—21].
Because of the importance of high-affinity IL-2 receptorexpression in immune responses, we hypothesized that defectsin cellular immunity seen in hemodialysis patients may berelated to defects in the ability of lymphocytes harvested fromthese patients to express high-affinity IL-2 receptors. We there-fore studied the potential role of the dialysis membrane on theexpression of these receptors in eight chronic hemodialysispatients in a short term, prospective cross-over design usingeither cuprophane or PMMA membranes for two weeks each.In parallel, we also measured the precent of lymphocytes whichexpress the subunits of IL-2 receptors, IL-2Ra and IL-2R/3, asindices of lymphocyte activation. The results indicate a proba-ble role for dialysis membrane in the ability of lymphocytes toexpress high-affinity IL-2 receptors and its subunits; thesefindings may be relevant to observations of cellular immunedeficiency in dialysis patients.
Methods
Patients
Eight hemodialysis patients, on chronic hemodialysis for 4424 months were selected for participation in this study. All
patients were previously dialyzed with reused cuprophanemembrane involving the use of formaldehyde in the reuseprocess. This reuse procedure significantly attenuates the com-plement activating ability of cuprophane membranes [3]. Onaverage, the number of reuses for each dialyzer was 12; thus,prior to their participation in the protocol, these patients wereexposed to a new cuprophane membrane once every month.The mean age of the patients was 69 years (range 51 to 76).
1020

Zaoui et a!: IL-2 receptor modulation by cuprophane membrane 1021
None of the patients had any clinical evidence for an activeinflammatory disease process, malignancy and none were dia-betic or had IgA nephropathy as the etiology of their chronicrenal failure. None of the patients were on steroid or immuno-suppressive therapy and none were on aluminum-chelationtherapy with desferrioxamine (which is known to inhibit trans-ferrin and IL-2 receptors expression) [22].
During the period of the study, there was no statistical changein the weekly drawn BUN, hematocrit, differential cell countsor albumin. None of the patients had any evidence of intercur-rent viral infections, and all were tested to be free fromHepatitis or HIV infections. Informed consent, approved by theVanderbilt University Medical Center and the Nashville VAHospital IRB was signed by all participants.
MethodsStudy design. The design of the study was a cross over
design. During the first phase of the study all patients weredialyzed for six consecutive times (3 times a week) with a newcuprophane hollow fiber membrane (Gambro, GF- 120) (phaseI). After two weeks, the patients were switched to two weeks ofPMMA (TORAY, B2-1.2H) membrane (phase II) and then werereturned to an additional period of new cuprophane membranesfor another period of two weeks (phase III). All other parame-ters were maintained constant.
Mononuclear cells were harvested from blood drawn pre- andpost-dialysis at the first and sixth (that is, beginning and end ofthe two week period) dialysis with each type of membrane.Control samples, obtained from 18 uremic, non-diabetic andnon-dialyzed patients with serum creatinine greater than 5.0mg/dl (uremic controls) and from 12 normal volunteers (normalcontrols) without known medical problems, were assessed inparallel.
Peripheral blood mononuclear cell (PBMNC) culture. Thirtycc of blood were mixed with equal amounts of Hank's balancedsalt solution (HBSS; Gibco, Grand Island, New York, USA)and carefully layered over Histopaque (Sigma Chemical Co.,St. Louis, Missouri, USA) media allowing gradient densitycentrifugation. The mononuclear cell layer was collected andwashed twice with HBSS and then resuspended in RPMI 1640supplemented with 2 mrvi L-glutamine (Gibco), 100 U/mI peni-cillin U, 10 sg/ml Streptomycin (Sigma) and 10% de-comple-mented, sterile-filtered certified fetal calf serum (FCS; (Gibco).
PBMNC (5 x l0 cells/ml) were placed in 24 well plates(NUNC) and incubated for four days at 37°C in a 5% CO2saturated humidity incubator (Forma Scientific). Viability byTrypan blue dye exclusion was >99% at the beginning of theculture and >90% at the end of the four-day culture period. Partof the cultures were activated with 1% vol/vol Phytohemagglu-tinin (PHA-M, Gibco) in parallel, to investigate the ability ofthese cells to express high affinity IL-2R [161.
Cytofluorometric studies. I) IL-2Ra (p55) expression. Cellpellets (2 x 106 cells) were harvested on the fourth day ofculture and incubated in 500 d phosphate-buffered saline (PBS)with 2% FCS, 0.1% sodium azide (modified PBS) with 5 dfluorescein conjugated anti-IL-2Ra antibody (Becton-Dickin-son) for 30 minutes at 4°C in the dark. Cells were then washedtwice with 2 ml of the modified PBS and kept in 500 pi of thissolution at 4°C until cytometric analysis, generally less than twohours after staining.
Green fluorescence analysis was performed on a flow cytom-eter EPICS 753 with Argon Laser. Fluorescence was standard-ized each day by fluorescent microbeads and voltage, andamplification and compensation was kept identical for all pro-cedures. The percentage of IL-2Rcl positive cells and the meanlog fluorescence channel (log units) of positive cells wereanalyzed on 5,000 lymphocytes gated by size and granularityand recorded on a Coulter computer using Immuno" (Diagnos-tics) software. Background autofluorescence with unstainedcells from the same experiments and non-specific staining ofcells with irrelevant mouse IgG-FITC were digitally subtracted.
2) IL-2Rf3 (p70) expression. Two times 106 cells were simi-larly incubated with 1 jig anti-IL-2R13 antibody (mouse hybrid-oma IgG2, supplied by H. Helderman) and revealed with 5 dfluorescien isothionate conjugated (FITC) goat antimouseF(ab)'2 fragment (Becton Dickinson). Cytofluorometric analysisfor IL-2R/3 expression was performed using procedures similarto those described for IL-2Ra expression. IL-2Rf3 expressionwas measured only during phase III when the antibody becameavailable to the authors.
Radioreceptor assay of high affinity IL-2 receptor. BrieflyPHA-induced blasts were counted and incubated for one hourat 37°C in fresh RPM! 1640 to remove endogenous IL-2 thenresuspended with V25 IL-2 (Dupont NEN, Wilmington, Dela-ware, USA) in triplicates of 2 x 106 cells in 100 d RPMI 1640supplemented with 10% FCS in 1.5 ml Eppendorf silanized(SIGMACOTE) microtest tubes. The method used has beendetailed elsewhere [161. Serial dilutions of 1125 IL-2 wereassayed in this culture to determine the saturation (plateau) ofspecific high affinity binding. This was observed at a concen-tration of IL-2 between 10 and 50 p (data not shown). Furtherstudies were carried out using 50 M of IL-2. The specificradioactivity of the probe (1.7 x 10 dpm/pM) was used toconvert maximal levels of bound radioactivity to number ofbinding sites per cell, assuming one receptor per bound mole-cule of IL-2. Control experiments with unstimulated cells or100-fold excess cold IL-2 confirmed only minor nonspecificbinding (<10% maximal binding of the I'25-IL-2).
Direct effects of dialysis membranes. To investigate thedirect effects of the dialysis membrane, independent of comple-ment products or cytokines, we prepared small volume dialyz-ers, made of the same hollow fiber membranes as used clini-cally, but with a fiber bundle volume of approximately 1.5 to 2.0ml. Such "minidialyzers" were manufactured from cu-prophane, PMMA and PAN (polyacrylonitrile) fibers. Theseminidialyzers were sterilized before each use with high pressuresteam.
Role of monocytes. To ascertain the role of monocytes in thein vitro experiments described above, PBMNC from the samenormal controls were further purified by passage through nylonwool columns and panning to yield mostly T-cells. Purity of theyield was confirmed by an increase in the CD3 staining of 74.8
3.2% and a loss of monocyte markers (CD 14 staining lessthan 0.6% and CD35 less than 1.2%). These purified T-cellswere then incubated in the minidialyzers for four hours andcultured as described previously at 37°C in 5% CO2 for fourdays.
Endotoxin contamination. Supernatants of cultures from invitro dialyzer incubation and from the cross over study weretested by a quantitative LAL assay (LAL, QCL 1000, Whit-

1022 Zaoui et a!: JL-2 receptor modulation by cuprophane membrane
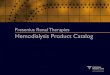
Fig. 1. Percent of PBMC expressing IL-2Ra (p55) subunit duringchronic dialysis with new cuprophane membrane (phase I). Symbolsare: (U) pre-dialysis, () post-dialysis, (•) uremic and normal controls.After two weeks, the percent of IL-2Ra positive cells was significantlyhigher, both pre- and post-dialysis. **p < 0.005 compared to firstdialysis and controls.
taker Bioproducts Inc., Maryland, USA) and were alwaysbelow 2.5 E.U/ml.
Statistical analysisComparisons between the different phases of the cross over
study was by the use of multivariate analysis (ANOVA) usingBMDP software package. Statistical significance between dia-lyzer phases were analyzed using t-test for paired data, whereascomparison with control groups was done using non-pairedt-test, after testing for normality.
Results
Spontaneous IL-2Rcs expression during dialysisPrior to beginning the experimental period with new cu-
prophane membranes, the percent IL-2Ra (p55) positive cells inour study population was 2.6 0.3%, which was not signifi-cantly different from uremic non-dialyzed or normal controls(2.7 0.6%; Fig. 1).
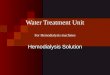
Following the first dialysis with new cuprophane membrane,there was an increase in the number of IL-2Ra positive cellsfrom 2.6 0.3% to 3.8 0.5% (P = NS). However, whensampled at the sixth dialysis, the number of IL-2Rs positivecells had increased to 7.5 2.7% pre-dialysis, and 9.9 1.6%post-dialysis, both significantly greater (P < 0.005) than con-trols or values at the beginning of the first phase (Fig. I). Duringthe first dialysis with the PMMA membrane, the percent ofIL-2Ra positive cells remained significantly high, (10.7 2.5%,pre-dialysis and 9.4 2.6% post-dialysis). However, prior tothe last (6th) dialysis on PMMA membrane, the number ofIL-2Ra positive cells had returned to baseline value, 3.8 0.8%(Fig. 2). When the same patients were again dialyzed with newcuprophane membranes (phase III) results similar to phase Iwere obtained. Thus, the percent of cells expressing IL-2Raincreased from 2.9 0.6% before the first dialysis with cu-prophane membrane to 8.4 1.6% after the sixth dialysis withthis membrane (P < 0.05 compared to baseline) (Fig. 2).
Density of IL-2Ra expression per cell was assessed by themean log fluorescence channel (log units) of IL-2Ra positivecells. The mean log fluorescence channel (MLFC) was also
increased by the chronic use of new cuprophane from 36.32.7 log units at the beginning of the study to 52.3 1.2 log unitsafter the sixth new cuprophane dialysis during phase I (Table 1).The MLFC decreased during dialysis with the PMMA mem-brane (phase II) but increased again during phase III whencuprophane membrane was again used for a further two weekperiod (Table 1). Thus, chronic dialysis with new cuprophanemembranes leads to an increase in the percent of IL-2Rapositive cells and these cells express higher density of IL-2Rcson their surfaces. These effects are reversible with the use ofnon-cellulosic membranes such as PMMA.
Spontaneous IL-2Rf3 expression during dialysis
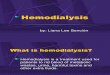
IL-2Rf3 is constitutively expressed on cell surfaces of PBMC;in normal unstimulated controls, 24.9 1.2% of PBMC spon-taneously express IL-2R/3 on their surfaces (Fig. 3). Duringphase III, when new cuprophane membrane was again used, thepercentage of IL-2R13 positive cells increased from 40.8 5.3%of cells at the beginning of phase III to 58.0 2.3% (P < 0.05vs. control) just before the sixth dialysis with new cuprophanemembrane and reached 65.4 2.0% post-dialysis (P < 0.05 vs.pre-dialysis).
The cellular density of IL-2R/3 positive cells, assessed byMLFC of positive cells, was also increased during dialysis withcuprophane membranes (phase III) from 41 2.1 log units priorto the first dialysis to 65 3.1 log units at the end of the sixthdialysis (P < 0.02 from baseline)
PHA -stimulated high-affinity IL-2 receptors (IL-2R)
The number of cells expressing IL-2Ra as well as IL-2R/3were significantly and maximally increased in PHA stimulatedPBMC harvested from patients chronically dialyzed with re-used cuprophane membranes, uremic (non-dialyzed) controlsas well as normal controls. Furthermore, there were no differ-ences in the percent positive cells or the MLFC of these cellsbetween these groups. Thus, the percent of positive cells inthese mitogen stimulated cultures was 82.5 7% for IL-2Raand greater than 92.7 6.5% for IL-2Rf3 subunits. MLFC was
a,
—j—o
5),')
1)o.czo
Ca
15.0
10.0
5.0
0.0
A Phase II (pmma) B Phase III (cupropharie)
Control 1st dialysis 6th dialysis
15.01)
02 .a..-. 10.0•- L)a.,')
z5.0
.E.
0.0
Fig. 2. During dialysis with the PMMA membrane, the % of PBMCexpressing IL-2Ra returns to baseline (A), but is again increased duringthe third phase of the study using cuprophane membrane (B). Symbolsare: (U) pre-dialysis, () post-dialysis. P < 0.05; ** < 0.005compared to first dialysis of phase I.
1st dialysis 6th dialysis 1st dialysis 6th dialysis

Zaoui et a!: IL-2 receptor modulation by cuprophane membrane 1023
Table 1. Mean log fluorescence channel units (MLFC) of IL-2Ra positive cells in unstimulated cultures of PBMC dunng the cross-over study
Phase Icuprophane
Phase IIPMMA
1stDialysis
Phase IIIcuprophane
6thDialysis
1stDialysis
6thDialysis
1stDialysis
6thDialysis
MFLCSEM
36.3/36.32.7/1.5
48.3a/52.3a1.4/1.2
41.4/381.3/0.7
28.2a/28.5a2.5/1.4
27.5/34.33.9/3.6
37.0/43.3a4.9/3.2
For each dialysis, the values (I) represent pre/post-dialysis MLFC.a P < 0.05 vs. first dialysis
A Phase I B Phase II
a)
4500aa)
3500
2500
1500ili 1
Phase Ill
a)csj 80
60
Control 1st dialysis 6th dialysis
Fig. 3 The effect of dialysis with cuprophane membrane (phase III),on IL-2Rf3 expression. Prior to the first new cuprophane dialysis, thepercent of IL-2R/3 positive cells was 40.8 5.3%. During the sixthdialysis with cuprophane membrane, the percent of PBMC with IL-2R/3expression increased from 58.0 2.3% pre-dialysis (La) to 65.4 2.0%post-dialysis (s). < 0.01 compared to uremic controls (U).0.01 compared to pre-dialysis.
71.0 7.8 log units for IL-2Ra and 75.2 2.1 log units forIL-2Rp, respectively.
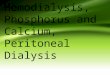
PBMC harvested pre- and post-dialysis at the beginning andend of each of the three phases of the study were then assessedfor their capacity to express high-affinity IL-2R receptors. PHAstimulation induced the expression of high affinity IL-2R inPBMC harvested from dialysis patients during the three exper-imental phases, but the extent of this expression varied depend-ing on sampling time (Fig. 4). Prior to the initiation of the firstcuprophane dialysis (phase I), the number of inducible IL-2Rreceptors per cell was 4152 177 receptors/cell, similar tolevels seen in cells obtained from normal and uremic controls(4174 107 receptors/cell). After the first dialysis with cu-prophane membrane, the maximal PHA inducible number ofIL-2R expressed was only 2451 200 receptors per cell,significantly less than pre-dialysis (P < 0.01). After two weeksof dialysis with the cuprophane membrane, the ability of PHAto induce high affinity receptors remained significantly attenu-ated even in pre-dialysis cultures (mean number of receptors3352 176; P < 0.01). This was further reduced to 2720 267receptors/cell post-dialysis induced by PHA at the last (6th)dialysis with cuprophane membrane. Although the mitogen-induced expression of high affinity IL-2R was still impaired atthe first PMMA dialysis (2768 276 high affinity receptors/cellpre-dialysis), it improved after two weeks of PMMA dialysis(3528 142 receptors/cell). Furthermore, there was no signifi-
ctrl 1st dialysis 6th 1st 6th
Fig. 4. The number of high affinity JL-2R on PHA stimulated PBMCduring 2 weeks of cuprophane (phase I) and PMMA (phase II) mem-brane dialysis. The number of IL-2R decreases post-dialysis ()compared to predialysis (LI) during the initial dialysis and is furtherdecreased pre-dialysis during the sixth dialysis of phase I. The findingsare reversed during phase II but recur during phase III. < 0.01compared to pre-dialysis values of the first cuprophane dialysis (phaseI) and controls (U).
cant difference in PHA induced IL-2R between the pre- andpost-dialysis samples in this phase of the study. The decreaseduring the second period of cuprophane exposure (phase III)was similar to phase I (data not shown). In four patients studiedat the end of a third week of new cuprophane dialysis (phaseIII), the number of high affinity receptors post-dialysis inducedby PHA mitogen remained low (2799 321 receptors/cell) butwas not significantly different from its value at the end of twoweeks. Thus recurrent dialysis with new cuprophane membraneattenuates the ability of lymphocytes to respond to mitogenicstimulation in terms of expression of high affinity IL-2R; thiseffect is reversible by the use of non-cellulosic membranes suchas PMMA.
In vitro incubation of PBMC with dialysis membranes
We incubated PBMC obtained from normal volunteers invarious small volume dialyzers made from different types offibers currently in use (cuprophane, polymethylmethacrylate,polyacrylonitrile) without further stimulation. As can be seen inFigure 5, whereas incubation with synthetic membrane dialyz-ers which do not have the polysaccharide structure of thecuprophane membrane, such as the PMMA or PAN (AN69)membranes resulted in no significant increase in the percent ofcells expressing IL-2Ra, incubation of the same cells with thecuprophane hollow fiber membrane in vitro for four hours priorto culture resulted in a significant increase both in the percent of

1024 Zaoui et a!: IL-2 receptor modulation by cuprophane membrane
0.0Control Cuprophane AN69 PMMA
Fig. 5. In vitro incubation of normal PBMC with hollow fiber dialysismembranes before (U) and after () incubation with C5,. Cuprophanemembrane directly increases the % of PBMC expressing IL-2Ra.Addition of C5a at 50 ng/ml further increases this percentage, but has noappreciable effect on PMMA or PAN non-cellulosic membranes. *D <0.01 compared to control and non-complement activating membranes;**p < 0.05 compared to unstimulated cells incubated with cuprophane.
those cells (4.9 1.1%, P < 0.01) as well as the density ofreceptors as determined by MLFC (from 24.0 5.0 log units to32.0 7.0 log units, P < 0.05). The addition of the anaphyla-toxin C5a to the culture media prior to their incubation with thishollow fiber dialyzer membrane lead to a further increase in thepercent of IL-2Ra positive cells to 8.1 2.5% (P < 0.05);concomitantly the MLFC increased to 39.0 5.0 log units (P <0.05 compared to unstimulated cultures).
IL-2R/3 expression was also affected by incubation with thecuprophane minidialyzer. The percentage of mononuclear cellsexpressing IL-2Rj3 was increased by direct contact with themembrane (from 24.9 1.2% at baseline to 47.3 4.6%) andwas further increased when C5a was added prior to incubation,to 79,5 4.2% (P < 0.01 vs. baseline). Density of receptors asassessed by MLFC of positive cells also increased significantlyfrom 22.0 5.0 to 37.0 8.0 log units after cuprophaneincubation and 49.0 7.0 log units when C, was added to theculture.
Role of monocytes in in vitro experimentsIncubation of the monocyte-free purified T-cell population
with cuprophane membrane alone or following the addition ofC5a resulted in no increase in IL-2Ra or f expression and nochange in the MLFC. Thus monocyte free cultures of PBMC donot respond to C5a or to the polysaccharide structure ofcuprophane.
Discussion
The present cross-over study highlights the participation oflymphocytes in the blood-membrane interactions occurringduring dialysis with cuprophane membrane. Chronic dialysiswith cuprophane membranes, the most widely used dialysismembrane and one which is associated with activation ofseveral pathways of the inflammatory response [1—4], leads toan increase in the expression of IL-2Ra and IL-2R/3 subunits,markers of lymphocyte activation. More importantly, the num-ber of high affinity receptors elicited by PHA is significantlyreduced. These findings are seen following as little as twoweeks of dialysis with new cuprophane membrane, and persist
in the patients for at least an interdialytic period, as seen duringthe cross over period of 72 hours from the sixth dialysis withcuprophane to the first dialysis with PMMA. However, com-parison of the changes of IL-2 receptors at two weeks and atthree weeks of cuprophane membrane exposure suggests thatthese defects are not progressive beyond two weeks.
Increased IL-2Ra expression, concomitant with decreasedability to express high affinity IL-2R by lymphocytes stimulatedwith mitogens has been shown in a number of disease statesassociated with impaired immune responses [17—21]. Althoughthese findings appear at first glance discrepant, recent studieshave suggested that T-lymphocytes that have undergone a cycleof proliferative response become refractory to further stimula-tion by various mitogens and antigens, and have decreasedIL-2R response upon successive stimulation [23, 24]. Thus ourhypothesis is that the extent of IL-2Ra and p subunits ex-pressed on lymphocytes harvested following chronic dialysiswith cuprophane membrane is an index of their pre-activationand may make them refractory to subsequent mitogenic stimu-lation by limiting their expression of high affinity IL-2R.
The presence of high affinity IL-2R is crucial for T-cellactivation and differentiation since it is a target of the T-cellgrowth factor IL-2 [9, 12, 24, 25]. In association with lowbioavailability of IL-2 in supernatants of stimulated uremicT-cells [7, 26, 27], the present study may shed some light onvarious observations of defective cell-mediated immune re-sponse in hemodialysis patients. These include decreased pro-liferation and low IL-2 production in response to antigenic andmitogenic challenge [7, 27], cutaneous anergy [28, 29], de-creased antibody response to T-helper dependent antigen proc-essing such as influenza [30] and hepatitis B vaccine [31],increased incidence of cell-mediated infections such as myco-bacterium tuberculosis [32, 33] or viral hepatitis B [34].
Several observations made in this and other studies suggestthat the primary defect in the attenuated lymphocyte responsesseen in hemodialysis patients may reside in the monocytes.Meuer and colleagues have suggested that the decreased pro-liferative response of T-lymphocytes in hemodialysis patients isdue to defective monocyte activation and in particular theirinability to support primary T-cell activation in vitro; when theactivation pathway of lymphocyte bypasses monocyte stimula-tion the T lymphocyte response returns to normal [35]. Tsako-los et a! have also shown that the lymphocyte proliferativeresponse is impaired in hemodialysis patients but is correctedby addition of control monocytes [36]. Recent studies onmonocyte activation during dialysis with cuprophane mem-branes [21 as well as our own observations in this study havepointed out that monocyte activation can occur even in theabsence of complement activation, by direct interaction of themonocytes with the polysaccharide structure of the cupróphanemembrane [2, 37].
Thus, our hypothesis is that the immunomodulatory effects ofthe cuprophane membrane are mediated by the chronic stimu-lation of monocytes either by direct contact with the polysac-chande structure of cuprophane or via their C5a receptorsleading to a persistent up-regulation of IL-2Ra and f3subunitson lymphocytes. This chronic stimulation decreases the re-sponse to further antigenic or mitogenic stimuli [23, 24]. This isalso supported by our observation on the reversibility of thesefindings when a non-cellulosic (and non-complement activating)
15.0
12.5
10.0
7.5
5.0
2.5
a:(J_J— U)0) U)aa, •xc,a,,,,
z—.
**

Zaoui et al. IL-2 receptor modulation by cuprophane membrane 1025
dialysis membrane is utilized. This hypothesis needs to beconfirmed by further studies.
While these indices of lymphocyte activation were notpresent when the study was initiated in patients chronicallydialyzed with formaldehyde-reused dialyzers (which have amarkedly attenuated complement activation capacity), it isimportant to point out that chronic dialysis with cuprophanedialyzers reused with bleach (which leads to recurrent comple-ment activation [381 and is prevalent in greater than 30% ofdialysis units) may well result in similar findings.
Finally, although these findings of reduced inducible IL-2receptors are seen as early as two weeks after initiation of newcuprophane dialysis, and persist for up to three weeks, longerterm studies are needed to define the persistence of thesefindings during chronic hemodialysis as well as to define thetime course of the onset of reduced IL-2 receptor expressionpre-dialysis.
In summary, dialysis with cuprophane membranes leads to alow grade stimulation of lymphocytes as expressed by in-creased IL-2Ra and f3 subunits but impairs their expression ofhigh affinity IL-2R, while dialysis with non-cellulosic activatingmembranes reverses many of these abnormalities. While it isdifficult to extrapolate these findings to clinical observations ofimmune deficiency in dialysis patients, the present cross-overstudy highlights the potential deleterious role of cellulosicmembranes on the immune response of chronic hemodialysispatients. A potential pathogenesis of these defects may be in thechronic activation of complement and monocytes by thesemembranes.
Acknowledgments
Antibody against IL-2RJ3 receptor was kindly supplied by Dr. H.Helderman and is gratefully acknowledged. This work was supported.by NIH grant #5-R0l-HL-3605. The authors would like to express theirappreciation to the staff and the patients of the Veterans AdministrationMedical Center and of the Dialysis Clinic Inc. facility in Nashville,Tennessee, for their help and participation.
Reprint requests to Raymond M. Hakim, M.D., Ph.D., ClinicalServices, Division of Nephrology, Vanderbilt University, B-2214 Med-ical Center North, Nashville, Tennessee 37232-2373, USA.
References
1. HAKIM RM, L0wRIE EG: Hemodialysis-associated neutropeniaand hypoxemia: The effect of dialyzer membrane materials. Neph-ron 32:32—39, 1982
2. ROCCATELLO D, MAZZUCCO G, Coo R, PiccoL! G, R0LLIN0 C,SCALZO B, GUERRA MG, CAVALLI G, GIAcHIN0 0, AM0RE A,MALAVASI F, SENA LM: Functional changes of monocytes due todialysis membranes. Kidney mt 35:622—631, 1989
3. HAKIM RM, FEARON DT, LAZARUS JM: Biocompatibility of dialy-sis membranes: Effects of chronic complement activation. Kidneymt 26:194—200, 1984
4. HAKIM RM, SCHAFFER A: Hemodialysis associated platelet acti-vation and thrombocytopenia. Am J Med 78:575—580, 1985
5. CHANDY KG, PAHL M, VAZIRI ND, GUPTA S: Acute effects ofdialysis on T lymphocytes in patients with end-stage renal disease.J Clin Lab Immunol 17:119—124, 1985
6. CHIDA Y, SAKURAI S, YOSHIYAMA N: The effect of hemodialysison lymphocyte subsets during dialysis. Clin Nephrol 25:159—163,1986.
7. CHATENOUD L, DUGAS B, BEAURAIN G, TOUAM M, DRUEKE T,VASQUEZ A, GALANAUD P, BACH i-F, DELFRAISSY i-F: Presence
of preactivated T cells in hemodialyzed patients: Their possible rolein altered immunity. Proc NatI Acad Sci USA 83:7457—7461, 1986
8. BEAURAIN G, NARET C, MARCON L, GRATEAU G, DRUEKE T,URENA P, NELSON DL, BACH i-F, CHATENOUD L: In vivo T cellpreactivation in chronic uremic hemodialyzed and non-hemodia-lyzed patients. Kidney mt 366:636—644, 1989
9. TESHIGAWARA K, W0NG HM, KATO K, SMITH KA: Interleukin-2high affinity receptor expression requires two distinct bindingproteins. JExp Med 165:223—238, 1987
10. UCHIMAYA T, BRODER 5, WALDMAN TA: A monoclonal antibody(anti-TAC) reactive with activated and fucntionally mature T cells.I. Production of anti-Tac monoclonal antibody and distribution ofTac (+) cells. Jlmmunol 126:1393—1397, 1981
11. DUKOVITCH M, WANO Y, THYU L, THI B, KATZ P, CULLEN B,KEHR J, GREEN WC: A second human IL-2 binding protein thatmay be a component of high affinity IL-2 receptors. Nature327:518—522, 1987
12. ROBB Ri, GREENE WC: Internalization of interleukin-2 is mediatedby the /3 chain of the high affinity interleukin-2 receptor. J Exp Med165:1201—1206, 1987
13. GREENE WC, BOHALEIM E, SIEKAVITZ M, BALLARD DW, FRANZABR, LOwENTHAL JW: Structure and regulation of the human IL-2receptor. Adv Exp Med Biol 254:55—60, 1989
14. YAGITA H, NAKATA M, AZUMA A, NITTA T, TAKESHITA T,SUGAMURA K, OKUMURA K: Activation of peripheral blood T cellsvia the p75 interleukin 2 receptor. J Exp Med 170:1445—1450, 1989
15. REED JC, Roas Ri, GREENE WC, NOWELL PC: Effect of wheatgerm agglutinin on the interleukin pathway of human T lymphocyteactivation. J Immunol 134:314—323, 1985
16. PETERSEN CM, CHRISTIANSEN BS, KALTOFT K: Binding, uptakeand degradation of human recombinant interleukin-2 (125-ala) inactivated human T- and B-lymphocytes and in monocyte-macro-phages. Tissue Antigens 29:257—272, 1987
17. K0NIsHI K, MOLLER DR, SALTINI C, KIRBY M, CRYSTAL RG:Spontaneous expression of the interleukin 2 receptor gene andpresence of functional interleukin 2 receptors on T lymphocytes inthe blood of individuals with active pulmonary sarcoidosis. J Clin
Invest 82:775—781, 198818. HAYWARD AR, HERBERGER M: Culture and phenotype of activated
T-cells from patients with type I diabetes mellitus. Diabetes 33:319—
323, 198419. SCHENA FP, MASTROLITTI G, JIRILLO E, MUNNO 1, PELLEGRINO
N, FRACASSO AR, AVENTAGGIATO L: Increased production ofinterleukin-2 and IL-2 receptor in primary IgA nephropathy. Kid-ney mt 35:875—879, 1989
20. GUPTA 5: Interleukin-2 receptor and transferring receptor expres-sion in T cells and production of interleukin-2 in patients withacquired immune deficiency syndrome (AIDS) and AIDS-relatedcomplex. Clin Immunol Immunopathol 38:93—100, 1986
21. GHIO R, HAUPT E, PIsT0IA V, PERATA A, MINALE P: Impairedin-vitro growth of PHA induced T lymphocyte colonies in hemodi-alyzed renal failure patients. Blut 50:135—140, 1985
22. CAROTENUTO P, PONTESILLI 0, CAMBIER JC, HAYWARD AR:Desferoxamine blocks IL 2 receptor expression on human Tlymphocytes. J Immunol 136:2342—2347, 1986
23. CANTRELL DA, SMITH KA: The transient expression of interleukin2 receptors. Consequences for T cell growth. J Exp Med 158:1895—
1922, 198324. CHURILLA AM, BRACIALE TJ, BRACIALE VL: Regulation of T
lymphocyte proliferation. Interleukin 2-mediated induction ofc-myb gene expression is dependent on T lymphocyte activationstate. JExp Med 170:105—121, 1989
25. WALDMANN TA, T5UD0 M: Interleukin-2 receptors: Biology and
therapeutic potentials. Hosp Pract 22:77—94, 198726. LOWENTHAL JW, CEROTTINI JC, MACDONALD HR: Interleukin
I-dependent induction of both interleukin 2 secretion and interleu-kin 2 receptor expression by thymoma cells. J Immunol 137:1226—
1231, 198627. KuRZ P, KOHLER H, MEUER 5, HUTTEROTH T, BUSCHENFELDE
K-H: Impaired cellular immune responses in chronic renal failure:Evidence for a T-cell defect. Kidney mt 29:1209—1214, 1986
28. GOLDBLUM S, REED WP: Host defenses and immunologic alter-

1026 Zaoui et a!: IL-2 receptor modulation by cuprophane membrane
ations associated with chronic haemodialysis. Ann Intern Med93:597—613, 1980
29. MoRRIsoN AB, MANESS K, TAWES R: Skin homograft survival inchronic renal failure. Arch Pathol 75:139—147, 1963
30. CAPPEL R, VANBEERS D, LIESNARD C, DRATWA M: Impairedhumoral and cell mediated immune responses in dialyzed patientsafter influenza vaccination. Nephron 33:21—25, 1983
31. STEVENS CE, ALTER MD, TAYLOR PE, ZANG E, HARLEY EJ,SZMUNESS W: Hepatitis B vaccine in patients receiving hemodial-ysis. Immunogenicity and efficacy. N Eng! JMed 311 :496—501, 1984
32. ANDREW OT, SCHOENFELD PY, HOPEWELL PC, HUMPHREYS MH:Tuberculosis in patients with end-stage renal disease. Am J Med68:59—65, 1980
33. LUNDIN AP, ADLER AJ, BERLYNE GM: Tuberculosis in patientsundergoing maintenance hemodialysis. Am J Med 67:597—603, 1979
34. CI-JATENOUD L, HEBERLIN A, BEAURAIN G, DESCAMPS-LATSCHAB: Immune deficiency of the uremic patient. Adv Nephrol 19:259—274, 1990
35. MEUER SC, HAUER M, Kuz P, MEYER ZUM BUSCI-1ENFELDE
K-HM, KOHLER H: Selective blockade of the antigen-receptor-mediated pathway of T cell activation in patients with impairedprimary immune responses, J Clin Invest 80:743—749, 1987
36. TSAKOLOS ND, THEOI-IARIDES TC, HENDLER ED, GOFFINET J,DWYER JM, WISLER RL, ASKENASE PW: Immune defects inchronic renal impairment: Evidence for defective regulation oflymphocyte response by macrophages from patients with chronicrenal impairment on haemodialysis. Clin Exp Immunol 63:218—227,1986
37. BETZ M, HAENSCH G, RAUTERBERG E, BOMMER J, RITZ E:Cuprammonium membranes stimulate interleukin- I release andarachidonic acid metabolism in monocytes in the absence ofcomplement. Kidney mt 34:67—73, 1988
38. HOENICH NA, JOHNSTON SRD, BUCKLEY P, HARDEN J, WARDMK, KERR DNS: Hemodialyzer reuse: Impact on function andbiocompatibility. mt JArtif Organs 6:261—266, 1983
39. LANGHOFF E, LADEFOGED J: Cellular immunity in renal failure.Depression of lymphocyte transformation by uraemia and methyl-prednisolone. liii Arch Allergy App! Immun 74:241—245, 1984