Embed Size (px)
Citation preview

J Periodontol • May 2004
631
Hemorrhaging Associated With Endosseous ImplantPlacement in the Anterior Mandible: A Reviewof the LiteratureChristos D.R. Kalpidis* and Reza M. Setayesh†
The placement of endosseous dental implants is largely consid-ered a safe surgical procedure. However, upper airway obstructionsecondary to severe bleeding in the floor of the mouth has beenoccasionally reported as a rare but potentially fatal complicationof implant surgery. This review presents critical hemorrhagicepisodes, related to dental implantation in the anterior segmentsof the mandible, published to date. Massive internal bleeding inthe highly vascularized region of the floor of the mouth is theresult of an arterial trauma induced by instrumentation, usuallythrough a perforation of the lingual cortical plate. Depending onthe clinical situation, hemorrhage may commence immediatelyor with some delay after the vascular insult. The progressivelyexpanding lingual, sublingual, submandibular, and submentalhematomas have the tendency of displacing the tongue and floorof the mouth to obstruct the airway. Because the course of air-way deterioration to complete occlusion may be rapid, ensuringa patent airway is of highest priority. Even though upper airwayobstruction is potentially life-threatening, a secure airway wassuccessfully established in all patients without fatal consequences.In most cases, resolution of hemorrhage required a surgical inter-vention for ligation of the bleeding vessels and hematoma evac-uation. To reduce the probability of such a grave complication,preventive and precautionary measures to be taken before, dur-ing, and after implant placement in the anterior mandible arepresented. Issues related to the level of surgical experience, fineregional arterial anatomy, radiographic and clinical evaluationof the osseous morphology, angulation and length of implants,and timing of hemorrhage onset are discussed. In addition, airwayand bleeding management strategies are provided. J Periodontol2004;75:631-645.
KEY WORDSAirway obstruction/prevention and control; dental implantation/adverse effects; dental implantation/complications; dentalimplants/adverse effects; dental implants/complications;emergency care; foramen/anatomy; mouth floor/blood supply;oral hemorrhage/prevention and control.
* Currently, private practice, Thessaloniki, Greece; previously, Department ofPeriodontology and Oral Biology, Boston University, Goldman School of DentalMedicine, Boston, MA.
† Department of Periodontology and Oral Biology, Boston University, Goldman Schoolof Dental Medicine.
After the introduction of the osseoin-tegration concept in dentistry,1,2
endosseous implants have assumeda major role in oral rehabilitation offeringthe option of implant-supported fixed andremovable prosthetic reconstructions. Themultitude of root form implant systems,the elaboration of innovative technologies,the dramatic increase in the number ofpractitioners placing implants, and theexponential rate of implant placement havespectacularly revolutionized everyday clin-ical dentistry.
Implant surgery is largely regarded asa safe and minimally invasive procedurewhen meticulously planned and carefullyperformed. However, implant placement,as any other surgical procedure, is notfree of inherent risks, some of which arenovel and unusual to the dental commu-nity. Management of challenging caseshas resulted in the development of newstrategies, which however inadvertentlyincreased the incidence of side problems.The biologic complications may be local-ized and characterized by low morbidityor may be more generalized and associ-ated with higher morbidity and, extremelyrarely, mortality.
Mechanical compression and/or directinjury during drilling or implant place-ment may disturb the nerve microcircu-lation, cause edema and create a localhematoma, or lead to neural degenerativeprocesses. Neurosensory disorders of theinferior alveolar, mental, and incisivenerves have been reported during place-
Review
3097.qxd 5/10/04 2:15 PM Page 631

632
Hemorrhaging and Implant Placement: A Review Volume 75 • Number 5
ment of implants in the atrophic mandible. Usually, theresulting anesthesia, paresthesia, or even dysesthesiaare temporary in nature but certain long-lasting neuro-pathies that may be considered permanent have alsobeen described.3,4 Transposition of the inferior alveolarneurovascular bundle that was developed to avoid nerveinjury has been associated too with altered neurosen-sory function5 and even iatrogenic fracture.6
Traumatic or spontaneous fractures have beenencountered in severely atrophic implanted mandibles.The fractures may occur post-surgically through implantsites, or at positions of removed non-osseointegratedimplants.7,8 Bone around implants during the osseoin-tegration process is considered more susceptible tofractures than bone around already integrated implants.8,9
Stress concentration in bone of decreased density ordeficient mineralization was also considered as an etio-logic factor.9 When primary immobilization of themandible is achieved, following the principles of fracturemanagement, implants situated on fracture lines usuallyosseointegrate.7-9
Microbial contamination during implant placement,bacterial transmission from adjacent teeth, and localinfection throughout the period from placement to func-tion, may result in an ailing or failing implant and pos-sibly to implant loss.10,11 Peri-implantitis is a site-specificbacterial infection usually restricted to the involvedimplant(s). However, more generalized severe infectionsincluding the life-threatening descending necrotizingmediastinitis have also been related to oral implanta-tion.12 Endosseous implants may provide a route forbacterial spreading into the maxillary sinuses. Cases ofmaxillary sinusitis have been reported after customaryimplant surgery13 or consequent gradual implant dis-placement into the sinus.13,14 Incidents of recurrentsinusitis, accidental implant dislodgement into the sinusduring second stage surgery, and formation of oro-antralfistulas have been described as potential complicationsof implant placement following maxillary sinus augmen-tation.15,16 In addition, perforations of the sinus mem-brane in implant dentistry may also be associated withdevelopment of sinusitis.17
Some fatal incidents related to oral implants have beenreported, although such incidents are extremely rare.18
Placement of implants has claimed so far three lives ofotherwise healthy individuals, including a 16-year-oldteenager, and was nearly deadly in three additionalcases.19,20 The serious medical complications along withthe fatalities were apparently attributed to massive venousair embolism induced during surgery by air-driven hand-pieces. Such fatal events would have been avoided ifproper rotary instruments were used according to themanufacturer’s guidelines.18
Finally, several cases of severe hemorrhage in thefloor of the mouth (FOM) with subsequent life-threatening upper airway obstruction (UAO) have been
recorded in association with implant placement in boththe anterior (Table 1)21-31 and posterior32 portions ofthe mandible. Dangerous and even fatal UAO, sec-ondary to extensive sublingual/lingual bleeding, mayalso result from vascular malignant invasion or necro-sis following radiotherapy,33 maxillofacial or lingualtrauma,34-36 and chronic anticoagulant treatment.37-39
In addition, obstruction of the oropharyngeal airwayand hematoma in the FOM have been reported as pos-sible complications of oral and maxillofacial proce-dures, including the orthognathic horizontal mandibularosteotomies,40 mandibular dermal graft vestibuloplas-ties,41,42 periodontal surgical procedures,43 biopsies ofsalivary glands or mucosal lesions,43,44 and surgicalremoval of ranulas or lipomas from the FOM.39,45
Excessive bleeding and respiratory embarrassment mayalso be rarely encountered as a result of everyday clin-ical dental procedures including local lingual anesthe-sia,45 use of sharp rotating instruments,45,46 and routineor surgical tooth extraction.43,45,47,48 A 1994 casereport demonstrated that formation of an extensivepostextraction hematoma and subsequent airwayobstruction may indeed be fatal.49
The present report reviews articles focusing on severehemorrhagic episodes related to oral implantology in theanterior mandible published through May 2003. Anelectronic search of the literature was conducted usingthe following key words: bleeding, h(a)emorrhage,h(a)ematoma, implant*, and complication* in thetitle and abstract fields (the * provides a search for allterms beginning with this word, e.g., implantation, com-plications). Bibliographic lists of published articles werealso scrutinized in an attempt to retrieve additional per-tinent papers. To the best of our knowledge, all relatedcase reports written in English or other languages wereincorporated in this review. One case report that dis-cussed a similar dangerous hemorrhage was excludedbecause it was related to implantation in the posteriormandible.32 Extracted data included age and gender ofthe patients, details regarding implantation and pros-thetic treatment plans, onset of bleeding, clinical signsand symptoms, etiology and management of hemor-rhage, presence and management of airway occlusion,and duration of hospitalization.
The purpose of the present paper was to: 1) reviewall available published case reports recording massivebleeding incidents following implant positioning inthe anterior segments of the mandible; 2) bring to theattention of the clinical community this extremely rarebut serious and potentially fatal complication; 3) pre-sent a brief but concise regional arterial anatomy anda description of the important anatomical structuresrelated to this life-threatening complication; and 4) pro-vide guidelines for avoiding severe bleeding events andfor immediate management should such an emergentsituation develop during or after surgical implantation.
3097.qxd 5/10/04 2:15 PM Page 632

633
J Periodontol • May 2004 Kalpidis, Setayesh
ANATOMIC CONSIDERATIONS RELATED TOSUBLINGUAL HEMORRHAGEFine Arterial Anatomy of the Floor of the MouthIt is widely accepted that the sublingual artery, a majorbranch of the lingual artery, is the main nutrient vesselto the FOM. Yet, the importance of the submental arteryin supplying blood to sublingual anatomical structureshas also been established.50-52 Mechanical injury to oneor more branches of the local arterial plexus may poten-tially lead to dangerous hemorrhage. Detailed knowl-edge of the regional fine arterial anatomy is, therefore,imperative for the implant surgeon (Fig. 1).
The lingual artery is typically the third consecutive, andthe second anterior branch of the external carotid arteryarising at the level of the hyoid bone. The vessel coursesanteriorly, disappears at the posterior border of the hyo-glossus muscle and continues anterosuperiorly, deepto the hyoglossus muscle, to enter the substance of thetongue.50,51,53 The lingual artery supplies the body andapex of the tongue through the terminating deep lingualartery and dorsal lingual branches, respectively.
At the anterior border of the hyoglossus muscle, thelingual artery gives rise to the sublingual artery. Thisimportant vessel courses forward in the FOM, near themedial and superior surface of the mylohyoid muscle,medially to the sublingual gland, and inferomedially tothe sub-mandibular duct and the lingual nerve.50,51,54
The sublingual artery with a mean diameter of ap-proximately 2 mm52 supplies the anatomical structuresof the FOM including the sublingual gland, the mylohy-oid, geniohyoid, and genioglossus muscles, the mucousmembranes of the FOM, and the lingual gingiva.50,51,54
In addition, the sublingual artery releases several alveo-lar branches for complementary blood supply to the lin-gual anterior cortical plate of the mandible.45,51,52
Superior, inferior, and large middle subdivisions of thesublingual alveolar branches have been identified inhuman specimens.55 Krenkel et al. described an ascend-ing branch that was further divided to a medial and a lat-eral arteriole, while a descending branch was divided toan inferior and a superior arteriole.45 All smaller branchesenter the cortical plate through various accessory lin-gual foramina. A thorough description of the routes of thesublingual alveolar branches has been recently reportedand three main ramifying patterns have been identified.52
The most common configuration was present in 44% ofthe specimens and corresponded to the pattern presentedby Krenkel et al.45 Another pattern (12%) included cra-nial, middle, and caudal branches while the least wide-spread (9%) incorporated a medial and a lateral alveolarbranch.52
The facial artery is normally the fourth consecutive, andthe third anterior, branch of the external carotid artery,unless it originates together with the lingual artery by acommon linguofacial trunk. The artery arises usually
below the posterior belly of the digastric muscle, entersthe submandibular triangle, turns laterally at the superiorborder of the submandibular gland, and courses anteroin-feriorly to the lower border of the mandible.50,54 The facialartery crosses the mandibular border near the anteriorborder of the masseter muscle, turns again, and followsa tortuous course anterosuperiorly to supply portions ofthe face.50,54
The submental artery, with an average diameter of2 mm,56 is one of the most important cervicalbranches of the facial artery. The submental arteryarises from the parent vessel prior to crossing themandibular border and courses interiorly along theinferior surface of the mylohyoid muscle together withthe mylohyoid nerve. The vessel supplies the lymphnodes of the submandibular triangle, the anterior bellyof the digastric muscle, and the mylohyoid mus-cle.50,51,56
Important Arterial Anastomoses and ReportedVariationsThe inferior alveolar arteries reach the symphysis of themandible by the terminating incisive arteries. In addition,complementary blood supply to the lingual inter-canineregion of the mandible is derived from the alveolarbranches of the sublingual arteries.45,52,55,57 Underneaththe mucous membrane in the anterior part of the FOM,the sublingual artery anastomoses with its fellow of theopposite site and penetrates the cortical plate through theaccessory anterior lingual mandibular foramina to anas-tomose with the central alveolar vessels (Fig. 1).45,55,58,59
The entrance of these alveolar arteries to the mandibleestablishes the anastomosis between the lingual and theinferior alveolar arteries. In conclusion, the central andparasymphyseal lingual mandibular regions are irrigatedby a very rich blood supply plexus.45,52,55,57
The blood supply to the mandible is primarily cen-trifugal in younger individuals. Eventual loss of teeth andarteriosclerotic changes of the inferior alveolar artery inolder people set the ground for a gradual shift from thecentral to a centripetal blood circulation.60 This new cir-culatory pattern is increasingly dependent on the exter-nal blood supply provided by the periosteal, muscular,and other soft tissues related to the mandible.55,60,61 Thus,the external vascular supply to the lingual aspect of theanterior mandible becomes very important, especially insurgical procedures involving extensive reflection of lin-gual mucoperiosteal flaps.
The mylohyoid muscles unite in the midline and sep-arate the sublingual and submandibular/mental spacesforming a diaphragm that supports the tongue and formsthe floor of the mouth. The sublingual and submentalarteries follow roughly parallel pathways as they run for-ward along the surface of the mylohyoid muscle (Fig.1).50,54 The sublingual artery is located on the superiorand medial plane of the muscle, while the submental
3097.qxd 5/10/04 2:15 PM Page 633

634
Hemorrhaging and Implant Placement: A Review Volume 75 • Number 5
artery runs on its inferior and lat-eral aspect. The sublingual andsubmental arteries normallyanastomose through their mus-cular mylohyoid branches (Fig.1). The mylohyoid muscle mayactually be considered as anextensive anastomosing fieldbetween the two vessels.50,51,54
These widespread anasto-moses were considered as thefoundation for an anatomic vari-ation in the vascular supply tothe area: the partial replace-ment or even actual substitutionof one artery by the other via alarge branch penetrating themylohyoid muscle to the otherside (Fig. 1).50,54 Bavitz et al.conducted a relevant cadavericstudy and reported that in 53%of the cases, the sublingualartery was either small,unimportant, or absent.51 Asizeable perforator from thesubmental artery was presentto supply the structures of theFOM in 60% of the dissections.The vessel perforating the mylo-hyoid muscle was, in the major-ity of the cases, half the caliberof the feeder artery and wastherefore regarded as its termi-nating branch.
In another pertinent study, theincidence of a missing sublingualartery (29%) and the frequencyof a large submental perforator(2.1 mm diameter) to the sublin-gual region (41%) were signifi-cantly lower.52 A sublingualartery without a complementarysubmental branch was isolated in59% of the dissections.52 In bothstudies,51,52 a variation with alarge perforating submentalbranch in addition to the sublin-gual artery of a normal size wasreported. None of the studies wasable, however, to identify a sub-lingual vessel penetrating themylohyoid muscle into the sub-mandibular region. Despite thereported different incidence rates,these observations revealed thesignificance of the submental
Table 1.
Case Reports of Life-Threatening Hemorrhage Associated With Implant Surgery in the Anterior Mandibular Region
Gender/ Details of ImplantHemorrhage†
Reference Age Placement* Onset Reason
Krenkel & Holzner21 F/59 1 IMP in PEM After 4 hours PRF (O)1986 (#22)
Mason et al.22 1990 F/54 5 IMP in CEM After nearly PRF (S)for FP (#27: 4-5 hours18 mm)
Laboda23 1990 M/67 2 IMP in SuturingCEM for OD (#22)
ten Bruggenkate et al.24 F/58 3 IMP in CEM After 6 hours1993 for OD
(#22 or #27)F/42 4 IMP in CEM for IOP PRF (O)
OD (#28)
Ratschew et al.25 F/80 4 IMP in CEM IOP PRF (O)1994 (#27: 15 mm)
Mordenfeld et al.26 F/69 5 IMP in CEM for Implantation PRF (S)1997 FP (#27: 15 mm)
Darriba & M/72 4 IMP in CEM Implantation DSMMendonça-Caridad27
1997
Panula & Oikarinen28 M/42 2 IMP in PEM After 30 TLP1999 minutes
Givol et al.29 2000 F/63 Immediate IMP Suturing PRF (R)in PEM (#22:18 mm)
Niamtu30 2001 F/64 2 IMP in IOP PRF (O)CEM (#22)
Boyes-Varley & M/50 Single IMP After 30 PRF (R,S)Lownie31 2002 (#23: 15 mm) minutes
* IMP: implant; CEM: completely edentulous mandible; PEM: partially edentulous mandible; FP: fixed prosthesis; OD: overdenture. The implant sites related to massive bleeding are presented within parentheses,followed by the implant length/osteotomy depth in mm, when provided.
† IOP: implant osteotomy preparation; DSM: detrimental surgical manipulations; TLP: tear of the lingual periosteum; PRF: perforation of the lingual plate which was felt through the osteotomy (O), detected surgically (S), or revealed radiographically (R).
‡ FOM: floor of the mouth; HEM: hematoma.§ NST: nasotracheal; USC: unsuccessful.� INT: intraoral approach; EXT: extraoral approach.
3097.qxd 5/10/04 2:15 PM Page 634

635
J Periodontol • May 2004 Kalpidis, Setayesh
artery as either an importantsupplementary or a principalsource of blood supply to theFOM (Fig. 1). However, theauthors also posed the dilemmaof whether the facial or the lin-gual artery should be ligated firstin case an extraoral approachwere required to control hemor-rhage in the sublingual region.50-
52,54
Accessory Anterior LingualMandibular ForaminaNumerous reports have de-scribed several accessoryforamina on both the buccal andlingual surfaces of the man-dible.45,58,59,62-65 The term“accessory” refers to foraminaother than the two major open-ings of the mandibular canalhousing the inferior alveolarneurovascular bundle.64 Sinceheavy hemorrhage and forma-tion of hematomas in the FOMmay ensue from perforations ofthe lingual cortical plate duringimplant site preparation, identi-fication of the lingual foraminain the anterior region of themandible may reduce the like-lihood of these life-threateningincidents.
The reported variability in dis-tribution, incidence, size, andcontents of the accessory lingualforamina has caused consider-able confusion. The most con-sistent of these foramina is the“median, central, midline, ormiddle” lingual foramen (Fig. 2).Located in the midline, at orsomewhat superiorly to thegenial tubercles, the median lin-gual foramen has been detectedwith a frequency ranging be-tween 85% and 99% in dry man-dibles and specimens.45,58,59,63,64
The mean reported diameter ofthe foramen is 0.54 mm63 andits distance to the inferior alveo-lar border averages 10 to 13.7mm.59,63 The associated canalextends deeply into the man-dible, on a buccolingual axis.58,59
Table 1. (continued)
Case Reports of Life-Threatening Hemorrhage Associated With Implant Surgery in the Anterior Mandibular Region
Clinical Signs Airway Hematoma Hospitalizationand Symptoms‡ Management§ Management� (days)
Elevation of the FOM Intubation Implant removal 6Sublingual HEM Evacuation
Elevation of the FOM NST intubation Compression 5Sublingual, lingual, submental, Evacuation (INT)
and submandibular HEM Ligation (INT)Respiratory distress
Elevation of the FOM Intubation Compression 6Submental HEM Evacuation (EXT)Elevation of the tongue Ligation (EXT)
Submandibular HEM NST intubation Hemostatic agents 8Elevation of the tongue Evacuation (INT)Respiratory distressElevation of the FOM Observation Compression 1Lingual HEM Evacuation (INT)
Elevation of the FOM Intubation Conservative 11Sublingual, lingual HEM (compression)Respiratory distress
Elevation of the FOM NST intubation Evacuation (EXT) 4Submental and Ligation (EXT)
submandibular HEMElevation of the
tongue, lingual HEM
Elevation of the FOM USC intubation Evacuation (INT) 14Intraoral bleeding and lingual HEM Tracheostomy Ligation (INT)Complete airway obstruction
Elevation of the FOM Intubation Compression 7Sublingual and lingual HEM Surgical exploration Serious breathing problems (INT)
Elevation of the FOM USC intubation Mucosal incisions 11Sublingual and submandibular HEM Tracheostomy Ligation (INT)Massive lingual HEMRespiratory distress
Elevation of the FOM USC intubation Conservative 6Submental and lingual HEM Laryngeal mask (hemostatic agents) Acute respiratory distress Tracheostomy (compression)
Elevation of the FOM Tracheostomy Surgical exploration (INT) 7Submental and sublingual HEM Evacuation (INT)Acute respiratory distress
3097.qxd 5/10/04 2:15 PM Page 635

636
Hemorrhaging and Implant Placement: A Review Volume 75 • Number 5
Contrary to earlier reports describ-ing a neurovascular bundle,64 morerecent investigations identified asingle nutrient vessel entering themedian lingual foramen.58,59 Fur-ther histologic examinationrevealed a plexus of small perivas-cular veins and occasionally somefine vasomotor neural fibers sur-rounding a single branch of thesublingual artery,58 but no nerveswere detected.58,59
The topographic orientation anddescription of the remainingaccessory lingual mandibularforamina is even more difficult topinpoint with certainty.45,59,63-65
Midline “interspinal,” “supraspinal,”and “subspinal” lingual foraminacontaining small branches of thesublingual artery have beendescribed, according to their ver-tical orientation in relation to thegenial tubercles (Fig. 2).45 Asmaller “inferior midline foramen”was identified below the genialtubercles (frequency 76%)63 whilethe presence of two or three mid-
line lingual foramina has also been detected radi-ographically in the symphyseal area.59
“Lateral lingual foramina” situated posteriorly to thegenial tubercles with a mean distance of 6 mm fromthe inferior mandibular border have been describedrecently (Fig. 2).59 Accessory foramina with a reportedincidence of 63% to 69% were also detected in thebicuspid region, near the inferior mandibular bor-der.63-65 In addition, smaller foramina related to slen-der ramifications of the sublingual arteries have beenfound near the crest of the alveolar ridge (Fig. 2).45,58
The “interalveolar medial foramen” (81% to 83% inci-dence) was located between the central and lateralincisors and the “interalveolar lateral foramen” betweenthe lateral incisors and canines (6% to 14% inci-dence).45 In conclusion, several of the arteries asso-ciated with accessory lingual mandibular foramina areof sufficient size to be implicated in severe hemor-rhaging episodes during implant placement in themandibular anterior region.
Osseous Morphologic Characteristics of the Anterior MandibleAfter tooth extraction, the basal osseous structure remainsfairly stable, whereas the alveolar bone undergoes aninevitable life-long resorptive process in most individu-als.66,67 Residual ridge reduction is considered the endresult of complex interactions between numerous func-
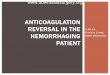
Figure 2.The median lingual foramen (black arrow) is located in the midline,at or somewhat superior to the genial tubercles (open arrows). Otheraccessory lingual mandibular foramina (black arrow heads) have beendescribed: 1) in the midline, above or below the genial tubercles; 2)posteriorly to the genial tubercles, near the inferior mandibular border;and 3) between the central incisors and canines, near the crest of thealveolar ridge. Several of the arteries associated with these accessoryforamina are of sufficient size to be implicated in severe hemorrhagingduring implant placement in the mandibular anterior region.
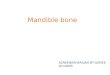
Figure 1.Schematic representation of the arterial anatomy in the floor of the mouth.The mandible is depictedin midsagittal cross-section.The sublingual and submental arteries are the main nutrient vesselsof the region.They follow almost parallel pathways along the surface of the mylohyoid muscle,which is the physical boundary between the sublingual and submandibular/submental regions.Thesublingual artery runs along the superior plane of the muscle while the submental artery courseson its inferior aspect. Important arterial anastomoses are formed between: (A) the sublingual andsubmental arteries, through their muscular mylohyoid branches, and (B) the sublingual and incisivearteries, through multiple accessory lingual foramina (O).The intimate proximity of the anastomosingvascular plexus to the lingual cortical plate may justify extensive bleeding even from minimalosseous perforations during implant placement.
3097.qxd 5/10/04 2:15 PM Page 636

637
J Periodontol • May 2004 Kalpidis, Setayesh
tional, anatomic, inflammatory, and systemic factors.68
Besides the significant inter- and intra-individual variabil-ity observed during osseous remodeling, the alveolarprocesses are resorbed in a fairly predictable fashion.Bone loss in the anterior mandible is primarily horizon-tal from the labial side (Fig. 3). This resorptive pattern,66
in combination with the protruding mental tubercles,results frequently in a lingually angulated trajectory of theanterior mandibular region (Fig. 3). Implant placementwith favorable prosthetic angulation may induce lingualperforations in the inclined atrophic edentulous mandibleand severe hemorrhage. In addition, the reduced heightof the residual alveolar ridge may generate lingual fen-estrations far closer to the inferior mandibular border andprovide access to muscular and vascular structureslocated deeper in the FOM.
The sublingual fossa is a fairly distinct osseous depres-sion on the lingual aspect of the anterior alveolar ridge,superiorly to the mylohyoid muscle, in the region extend-ing between the lateral incisor and first premolar.45,54
Part of the sublingual gland, which rests on the mylohy-oid muscle, is located in the sublingual fossa. In fact, itwas suggested that this osseous concavity is formed dur-ing development, under compressive forces generatedby the growing glandular tissue.45 The sublingual fossavaries greatly in anatomy, from being barely discernableto severely pronounced. Instrumentation for the place-ment of an implant in the region of extremely concavesublingual fossae may cause perforations of the lingualcortical plate.52 Tomographic scans provide a detailed
view of the lingual osseous architecture and along withproper flap elevation may help to avoid dangerous hem-orrhage in presence of extreme sublingual undercuts.52,59
CLINICAL CASE REPORTSLife-threatening bleeding in the FOM following implantplacement was first described by Krenkel and Holznerin 1986.21 To date, 11 references have appeared inthe dental literature describing a total of 12 patientswith severe hemorrhage and potentially life-threateningUAO during or after implant surgery in the anteriormandible (Table 1).21-31 The mean age of the patients(8 females and 4 males) was 60 years (range: 42 to80 years). Several implant systems have been utilizedand the implants were placed according to the manu-facturer’s surgical protocol. While in most cases theimplantation was performed under local anesthesia,general anesthesia,22 and intravenous23,30 or oral seda-tion26 were occasionally employed.
A total of 34 endosseous implants were placed inseven completely and three partially edentulousmandibles, even though the dentate status of patientswas not always reported (Table 1). Implantation of asingle abutment in an otherwise fully dentate mandiblewas also recorded.31 One publication was related to theplacement of an immediate implant in an extraction siteaugmented with autogenous bone graft and a collagenmembrane.29 Although sites liable for massive bleed-ing and associated length of implants or depth ofimplant osteotomy preparations (IOP) were not alwaysprovided in the original publications, the majority ofhemorrhaging episodes was related to the mandibularcanine site and ≥15 mm implant length or IOP depth(Table 1).21-26,29-31
The restorative treatment plans included fixedmulti-unit prostheses,22,26 single restorations,31 implant-supported partial dentures,29 and overdentures.23,24
One implant was removed in an attempt to drain thelingual hematoma through the IOP,21 and on one occa-sion, the intended placement of two implants wasdeferred to facilitate control of the critical hemorrhage.30
Successful osseointegration of the remaining implantspermitted the completion of the prosthetic reconstruc-tions according to the initial treatment plans.
The formation of extensive hematomas into the softtissues of the FOM in relation to implant surgery was inthe majority of the cases a consequence of arterialtrauma during IOP or implant placement (Fig. 4). Onseveral occasions, the vascular insult was confirmedduring subsequent surgical exploration of thearea.22,23,26,27,29 Small pieces of soft tissue at the tip ofthe rotating instruments or at the IOP during drilling weresometimes suggestive of a vascular and/or periostealinsult.22,24 The arterial wound was usually induced byinstrumentation through a perforation of the lingual cor-tical plate (Table 1, Fig. 4). The rich anastomosing vas-
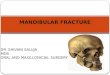
Figure 3.Reduction of the alveolar ridge between the mental foramina is mainlyhorizontal from the labial aspect.This pattern of resorption, combinedwith the projecting mental tubercles, often results in a lingually inclinedanterior mandible. Injudicious implant placement in the area mayinduce perforations of the lingual cortical plate and provoke seriousbleeding. Furthermore, with gradual vertical bone loss, deeply locatedmuscles and blood vessels become progressively more superficial,increasing the likelihood of trauma to these anatomic structures.
3097.qxd 5/10/04 2:15 PM Page 637

638
Hemorrhaging and Implant Placement: A Review Volume 75 • Number 5
hematoma resulted in inability toswallow,24,31 difficulty to articu-late,28,31 and a firm pressing of thetongue against the palate.24,26,30 3)Formation of extensive sublin-gual,21,22,25,28,29,31 submandibu-lar,22,24,26,29 or submental dissectinghematomas.22,23,26,30,31 4) Profuseor pulsating intraoral bleeding.22,27
Persisting internal hemorrhageinto the tongue musculature andthe distensible sublingual soft tis-sues resulted in progressive en-largement of the hematomas. Inthis clinical scenario, the increas-ing mechanical pressure to thepharyngeal lumen posed a poten-tially serious threat for a partial orcomplete UAO (Fig. 4). An inter-vention was typically undertakenwhen either a respiratory distresswas already established22,24,25,27-31
or was considered as immi-nent,23,26 because of the usuallyabrupt nature of UAO. While onecase was successfully managed
with careful airway observation,24 the oropharyngealairway was secured in most patients conservatively withnaso- or oro-tracheal intubation.21-26,28 However, theexpanding severe hematoma, secondary to continuousbleeding, rendered endotracheal intubation impossiblein three cases.27,29,30 Airway control was successfullyaccomplished in the remaining patients surgically, withemergency tracheostomy procedures (Table 1),27,29-31
while cricothyroidotomies were not performed in anyof the reviewed reports. Fortunately, even though theUAO is potentially life-threatening, all cases were han-dled adequately without any fatal consequences.
When the airway was secured, attention was directedtowards controlling the hemorrhage. While severe bleed-ing was conservatively handled in a few patients,25,30
most cases necessitated a surgical exploratory proce-dure for hematoma evacuation and isolation of the trau-matized vessels (Table 1). Efforts to evacuate thehematoma through incisions in the oral mucosa29 orthrough the IOP after implant removal21 yielded noresults. Successful drainage of the excessive hematomaswas performed either with an intraoral22,24,27,31 or anextraoral approach.23,26 Tamponage and digital com-pression were adequate to control bleeding in twopatients.25,30 Utilization of hemostatic agents was occa-sionally adopted to cease bleeding in the FOM24 andIOPs.30 Finally, definite management of the arterialbleeding in several instances required actual ligation ofthe offended vessels. While in one patient attempts toligate the retracted bleeding artery were unsuccessful,24
cular plexus in the anterior region of the mandible andthe intimate proximity of the blood vessels to the lin-gual periosteum and adjacent osseous wall52 may jus-tify profuse bleeding even from a minimal osseousperforation.24,29 The cortical fenestration was detectedsurgically,22,26,31 revealed radiographically,29,31 or feltthrough the IOP.21,24,25,30 New IOPs, angled in relationto the former osteotomies, were occasionally preparedin order to avoid suspected perforations.22,24,25 Thesevere bleeding in one report probably originated froma tear in the lingual periosteum during flap elevation orsubsequent flap handling (Fig. 4).28,69 Finally, the pro-fuse hemorrhage in another case was apparently attrib-uted to extensive detrimental surgical manipulations intothe deep muscular layers of the FOM and direct multi-ple arterial damage (Table 1, Fig. 4).27,70
The onset of perilous hemorrhage in the majority ofthe reports was noticed at some point during the sur-gical intervention.23-27,29,30 In two cases, the vascularinsult was evident shortly after placement,28,31 while inthree patients the latent time was considerably longer,ranging from 4 to 6 hours (Table 1).21,22,24 Whether theonset of hemorrhage was “early, immediate, intraopera-tive” or “late, delayed, postoperative,” profuse bleed-ing and extravasation of blood into the adjacent softtissues resulted in a clinical appearance characterizedby several signs and symptoms: 1) A typical swellingand elevation of the FOM.21-31 2) Distension,22,24-30
elevation,22-24,26-28 and even protrusion of the tonguefrom the mouth.30 In some instances, the lingual
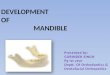
Figure 4.Schematic illustration of the events leading to progressive respiratory distress related to dentalimplantation in the anterior mandible. Severe bleeding and formation of massive hematomas in the floor of the mouth are the result of an arterial trauma.The vascular wound may occur afterdetrimental surgical manipulations or tearing of the lingual periosteum, but in most cases it is attributed to perforations of the lingual cortical plate. Mechanical pressure exerted by theexpanding hematomas displace the tongue and floor of the mouth superiorly and posteriorly,posing a potentially serious threat for obstruction of the upper airway.
3097.qxd 5/10/04 2:15 PM Page 638

639
J Periodontol • May 2004 Kalpidis, Setayesh
for the remaining cases, the procedure was effect-ively executed extraorally,23,26 or intraorally,22,27,29
despite the severe distortion of the regional anatomy.The duration of hospitalization ranged from 1 to 11days, depending on the severity of each case. Allpatients recovered uneventfully and were dischargedfree of symptoms.
DISCUSSIONDuring implant placement, transection or laceration ofan arterial branch located in direct contact with the lin-gual periosteum resulted in voluminous discharge ofblood into the FOM and the tongue. Hemorrhage fromlacerations is considered more copious compared toblood loss from transections, because the borders of thearterial wound tend to open up while the transected ves-sel usually constricts.21,44,71 The extravasated blood infil-trates easily the muscular and other soft tissues of theFOM without considerable resistance,45 forming mas-sive hematomas which are rigid upon palpation.30,34,39,43
The muscular anatomy and arrangement of fascialplanes largely determine the course of internal bleeding,similarly to the spreading of an orofacial infection.43,46
Because expanding is restricted by the mandible andsuperficial layers of the deep cervical fascia, sublingualand submandibular hematomas are extending superi-orly and posteriorly, thus displac-ing the tongue and FOM to obstructthe airway (Fig. 4).39,46 The esca-lating symptomatology of massivebleeding and progressive respira-tory distress strongly resemble theclinical development of Ludwig’sangina.31,38,46 Associated in thepast with high mortality rates, thisrapidly progressive odontogenicinfection is also manifested by tenseedema of the FOM, elevation andposterior displacement of thetongue, and severely compromisedairway.72
Formation of extensive hema-tomas into the soft tissues of theFOM may commence either im-mediately23-27,29,30 or with somedelay after the vascular in-sult.21,22,24,28,31,44-47 Sufficient re-flective constriction and retractionof a transected artery along withthe vasoconstricting effect of theepinephrine, contained in theanesthetic solution, may help ini-tially the organization of a bloodclot and bleeding cessation.Delayed, postoperative onset ofhemorrhage may be linked to the
compensatory vasodilation of the offended vessel dueto the gradual absorption of epinephrine, loss of the ini-tial thrombus, and resumptive bleeding.21,22,24,41-44,47
Airway ControlIn case a vascular trauma occurs during implant place-ment, surgeons should be prepared for the control ofa severely compromised oropharyngeal airway. Thetime course leading to UAO is unpredictable and earlyclinical features of airway deterioration may be verysubtle.36 An impending airway loss is manifested byseveral cardinal clinical signs and symptoms includingtachypnea, dyspnea, employment of accessory mus-cles of respiration, stridor, stertor, cyanosis, decreasedphonation, hoarseness, inability to swallow, and drool-ing. However, these clinical signs may be absent untilthe establishment of a significant airway occlusion, dic-tating the necessity of an immediate intervention.36
Although, it is broadly accepted that ensuring apatent airway is of higher priority than other thera-peutic procedures,26,29,31,42-44,48 there is controversyabout monitoring, decision making, and appropriatemanagement of UAO. The airway control optionsinclude: close observation, orotracheal intubation, blindor fiber-assisted nasotracheal intubation, and tra-cheostomy or cricothyroidotomy (Fig. 5). Manual
Figure 5.Flow diagram of airway management and control of massive hemorrhage in the FOM associatedwith implant placement in the anterior mandibular region. Establishment of a safe airway is ofhighest priority and the appropriate management depends upon the setting, experience, and clinicalcourse of each case. Basic bleeding control measures may be instituted simultaneously or priorto airway control. Once the airway is secured, efforts are directed towards definite resolutionof hemorrhage.
3097.qxd 5/10/04 2:16 PM Page 639

640
Hemorrhaging and Implant Placement: A Review Volume 75 • Number 5
tongue decompression and tactile intubation have alsobeen successfully employed in hemorrhagic swellingof the tongue.39 The decision for the appropriate air-way management depends upon the surgical setting,level of experience, available personnel, size of hema-toma, severity of bleeding, upper airway symptoma-tology, patient’s medical history, and clinical course ofeach case.
Since bleeding in the paralingual closed spaces maybe controlled or even self-limited,42 an expectant man-agement was proposed with careful observation of thehematoma and evidence of airway compromise(Fig. 5).43,47 This approach was effective in one patientafter implant placement,24 but may be hazardous whenbleeding is unmanageable and the compressive effectsof the hematomas are increasing. The course of airwaydeterioration to complete UAO and asphyxiation is ofteninsidious without reliable warning clinical markers of theneed for an artificial airway.36,37 Close airway observa-tion in relation to a progressive hematoma may rendera subsequently required endotracheal intubation very dif-ficult, extremely traumatic, or impossible.38,41,42,47
On the other hand, an immediate conservative orsurgical airway intervention was suggested on preven-tive grounds in anticipation of an expanding hematoma(Fig. 5).46 It should be noted that the mechanical pres-sure from sealed bleeding spaces adjacent to the upperairway may become life-threatening extremelyquickly.38,47 Early, prophylactic artificial airway con-trol prevents the necessity for subsequent emergentcrisis intervention and provides a safe airway for thepatients. In several instances following oral surgery,late unsuccessful attempts for intubation after the estab-lishment of the hematoma resulted in the need for emer-gency tracheostomies.42,44
Similarly, unsuccessful endotracheal intubations afterimplant placement necessitated the establishment of asurgical airway.27,29,30 Even though tracheostomy andcricothyroidotomy are definitive treatments, they areboth surgical procedures that may be associated withhemorrhagic and other complications. A tracheostomyperformed after implantation in one patient required sec-tioning of the thyroid gland and some related vessels.30
Although delayed bleeding is generally considered moredemanding in management, most patients presentingwith an already established respiratory distress after oralimplantation were managed adequately with intuba-tions,21,22,24,28 and only one required a tracheostomyto provide a secure airway.31
Bleeding ControlOnce the airway is controlled, efforts are undertakenfor definitive resolution of hemorrhage.26,29,42 Basicbleeding control measures in some of the reviewedcases have already been instituted simultaneously orprior to airway management (Fig. 5). Hemorrhage was
controlled by gauze tamponage,23-25 application ofhemostatic agents,24,30 cauterization,27 or digital com-pression.22,23,25,28,30 Hemodynamics suggest thathematomas may eventually cease expanding whenthe pressure of the extravasated blood exceeds thevascular pressure of the feeding bleeder.47,48 The grad-ually elevated local extravascular pressure along withthe compression from adjacent soft tissues frequentlylimit the internal intraoral hemorrhage encounteredduring or after various oral surgical procedures.26,28,31
Surgical decompression of the hematoma withdrainage may actually have a reverse effect by low-ering the established pressure and hence promotingfurther bleeding.29,43 The severe anatomic distortionof the area in conjunction with the retraction of theoffended vessel into deeper tissues usually render sur-gical maneuvers in the region very demand-ing.24,29,30,43,51 Some surgeons tend, therefore, todefer surgical exploration of the area for bleeding con-trol. Patients are closely monitored in anticipation ofhemorrhage self-resolution aided by local manage-ment of bleeding (Fig. 5).41-43,47 This approach wasadopted successfully in a few cases following implantsurgery.25,30
When the bleeding after implantation was not restric-tive and the local conservative measures were ineffec-tive, a surgical exploratory procedure eased identificationof the hemorrhagic source and resolution of bleeding(Fig. 5).21-23,26-29,31 Generally, surgical treatment is pre-ferred when the hematoma is large and non-restrictive.Surgical evacuation and ligation of the bleeding arterypermit rapid resolution of the hematoma and timely dis-charge from the hospital. Evacuation of large bloodclots from massive hematomas frequently facilitatedisolation of the damaged vessel that was usuallyretracted posteriorly.22,27 An intraoral approach for liga-tion of bleeding vessels has been performed by somesurgeons.22,27,29 Alternatively, an extraoral approachwas adopted by others due to deformation of the localanatomy.23,26,44 Ligation of the bleeding vessel by eithermethod resulted in an immediate hemorrhage controlafter implant surgery.
If an extraoral approach is dictated for ligation of thefeeder artery, the surgeon may confront a dilemma.50,54
Classic anatomy would impose ligation of the lingualartery in Pirogoff’s triangle to stem uncontrolled sublin-gual bleeding.44,50,54 However, in the light of more recentadvances involving the submental artery in the vascu-larization of the region (Fig. 1), some authors have pro-posed initial extraoral ligation of the facial artery tocontrol bleeding in the FOM.50-52,54 In support of thisapproach, it has been recently demonstrated that hem-orrhage in the FOM can be effectively managed by extra-oral ligation of the facial artery.32 Apparently, until theestablishment of consensus guidelines, the decision forextraoral ligation of the lingual or facial artery to con-
3097.qxd 5/10/04 2:16 PM Page 640

641
J Periodontol • May 2004 Kalpidis, Setayesh
trol sublingual intraoral bleeding should be guided bythe operator’s judgment in each particular case.
In severe hemorrhage, endovascular angiographyas an alternative diagnostic tool can overcome unsuc-cessful attempts to define and isolate the bleedingsource (Fig. 5).33 In addition to the external carotidartery angiography, recent developments in endovas-cular technology allow superselective catheterization ofbleeding feeders.73 Subsequent embolisation andocclusion of the involved arterial branches by the sameendovascular approach may be an attractive thera-peutic modality in emergency management of massiveiatrogenic bleeding after surgical procedures.30,40,44,48
The angiographic diagnostic/therapeutic approach hasbeen successful in the head and neck region,73 but itwas not utilized in any of the reviewed reports.
Preventive MeasuresContemporary dental implant placement has become ahighly specialized field that requires both long-term andongoing training. When performed by experienced oper-ators, the placement of dental implants in the anteriormandibular region should be considered a relatively safesurgical procedure with low complication rates. How-ever, the reviewed reports have clearly demonstratedthat serious bleeding and potentially fatal UAO may turnthis seemingly safe procedure into a difficult situation,even in the hands of skillful surgeons. As more special-ists and other practitioners, who are less trained, engagein placement of implants, the potential for complicationsincreases. To avoid or minimize such hazardous com-plications, oral implant placement should be performedonly by those who are versed in oral surgical proce-dures.24,28,29 Adequate training of the operator was con-sidered a fundamental preventive measure to avoid thislife-threatening complication.22,24,27-29,31,70
Practitioners whose knowledge and understanding ofimplant placement are based on short-term coursesand continuing education classes, rather than accred-ited residency programs where such procedures arean integral and extensive segment of postgraduateeducation, should be very cautious when performingthis surgery. To avoid the life-threatening complica-tion discussed above, these individuals should: 1) refinetheir surgical skills,29 2) strictly follow the appropriatesurgical techniques,70 3) have a good knowledge of theregional arterial anatomy,22,70 and 4) be trained in themanagement of acute airway and other medical emer-gencies,28,31 before placing implants in the inter-foraminal mandibular region. An example of thehazardous consequences when these requirements arenot met occurred during implant placement, when theapparently inexperienced practitioner lacerated thegenioglossus and geniohyoid muscles, transected thedeep lingual and sublingual arteries, and even dam-aged the hypoglossal nerve.27,70 The resultant massive
hematoma and complete UAO were fortunately han-dled efficiently, and the patient’s life was saved.
Implant surgeons should be sufficiently trained in themanagement of medical emergencies and the surgicalsetting should be supplied with the required emergencyequipment including a flexible nasal airway.27-29,31 Inaddition, protocols for management of emergenciessuch as the UAO should be instituted in each practiceand introduced to the auxiliary personnel. Operatorsand assistants could regularly rehearse these protocolsin the surgical setting so that they can promptly han-dle an emergency situation.30,37 In addition, the sur-geon should locate in advance the nearest hospital witha properly trained medical team to promptly managesuch a distressing sequel.
The medical history of the patient is of great impor-tance, especially in relation to cardiovascular diseases.Prophylactic thromboembolic therapy with aspirin, war-farin, heparin, coumarin, or streptokinase affects thecoagulation profile of the patient. Oral anticoagulantspredispose the development of serious bleeding causedby minimal or atypical trauma and can precipitate evenspontaneous formation of massive hematomas.37-39 Inaddition, because thrombolytic agents may contributeto hematoma expansion, timely discontinuation ofanticoagulation is suggested prior to implant place-ment. Dental implantation in these patients should beperformed extremely cautiously and only after consul-tation with the primary physician.
Precautionary Pre-, Intra-, and PostoperativeStrategiesComputed tomography (CT) is recognized as the mostreliable and effective preoperative diagnostic examina-tion in oral implant placement.74 However, it is a rela-tively complex technique with a moderately highexposure to radiation.75 CT scans provide a detailedthree-dimensional reconstruction of the osseous mor-phology. In relation to the complications reviewed inthis paper, the shape of the residual ridge, the lingualaccessory mandibular foramina with related canals, andthe spatial arrangement of the sublingual fossae areclearly depicted in a CT scan.52,59 Conventional, two-dimensional radiography may be occasionally helpful.Indications of the presence of pronounced fossae maybe provided by occlusal radiographs of the anteriormandible.26 In addition, major accessory mandibularforamina may occasionally appear on periapical radi-ographs.21,58 Instrumentation for the placement of animplant in the region of extremely pronounced sublin-gual fossae, accessory nutrient canals (Fig. 2), orseverely inclined atrophic mandibles (Fig. 3), may causeperforations of the lingual cortex, arterial trauma, andbleeding.21,26,31
Alternatively, proper preoperative digital palpationof the lingual mandibular surface may be of assistance
3097.qxd 5/10/04 2:16 PM Page 641

642
Hemorrhaging and Implant Placement: A Review Volume 75 • Number 5
in evaluating the possibility of osseous perforations dur-ing implantation.30 Moreover, surgical lingual probingand adequate elevation of the lingual mucoperiostealflap provide a detailed view of the osseous contour.29-31
Proper lingual flap elevation shields the underlying softtissues, regional sublingual musculature, and superfi-cial vessels when osseous perforations occur duringinstrumentation.24,25,29,30 Extreme caution is advisedthroughout flap elevation and handling because evenminor periosteal tears may also trigger devastatingbleeding in the FOM.28
However, some clinicians are concerned that suchextensive exposure of the atrophic alveolar ridge mayundermine periosteal blood circulation.76 When the lin-gual flap is not sufficiently reflected, digital palpation ofthe lingual mandibular surface is at least recommendedwhile drilling for IOP.30 If during the IOP a resistance isencountered prior to the calculated depth, indicatingdrilling in cortical bone, the surgeon should be alarmedand reevaluate the clinical setting. Several surgeons areproponents of the routine utilization of CT when implantsare placed in the anterior mandible. Others considerstandard CT scanning unnecessary and rely on con-ventional radiographic evaluation supplemented withpreoperative and direct surgical assessment.24 The deci-sion should be largely guided by clinical judgment on anindividual basis but CT may be advisable in demandingcases.30
In view of bleeding complications, the angulation ofthe implants in the anterior mandible should be mainlydetermined on biologic grounds. Problems related toacute inclination of the reduced mandible or pro-nounced sublingual fossae may be dealt with by adjust-ing the angulation of insertion or by placing shorterimplants.26,31 Inconvenient abutment angulation maybe corrected during the prosthetic reconstruction phase.Additionally, when the guidance of an extraction socketis conflicting with proper implant inclination in relationto the mandibular bone, appropriate adjustment of theangulation is required to avoid hemorrhagic complica-tions in immediate implantation.29
Bicortical anchorage in extremely atrophic mandiblesand utilization of longer implants are regarded as desir-able to ensure primary stability during osseointegra-tion.77,78 However, they may both need to be reconsideredin light of the discussed dangerous bleeding episodeswhen performing implant surgery in the anteriormandible.26,31 The advantage of implants as long as18 mm has never been clinically demonstrated,29 whileeven 6 and 8 mm short implants proved to be successfulin the rehabilitation of severely resorbed mandibles.79
Taking into account that life-threatening hematomaswere coupled to placement of ≥15 mm implants in themandible, utilization of <15 mm implants would be advis-able, especially in the canine sites (Table1).
It was noted that delayed onset hemorrhage may
occur after a considerable period following implantsurgery.21,22,24 Therefore, it would be advisable to care-fully monitor patients for a sufficient period after chal-lenging implant surgery in the anterior mandible,especially when perforation of the lingual cortex hasoccurred or was suspected.28,30,31 Under these cir-cumstances, the patient should be informed of the pos-sibility of a bleeding complication in order to cooperatewith the management of an emergency if it occurs.
Crisis Management GuidelinesIn spite of broad preventive measures taken and sys-tematic surgical precautions followed, dangerous hem-orrhaging complications may occur. There is broadagreement that airway management is of prime impor-tance and should be performed early in anticipation ofincreased swelling. However, a concurrent evaluationof the bleeding source and basic management of thehemorrhage is also important (Fig. 5). Both the sur-geon and assisting personnel should be able to followthe rehearsed emergency management protocol. Allinvolved individuals should maintain their composure.24
Panic may be easily imparted to the patient who mustremain calm in order to facilitate management of theemergency.
As soon as the first signs of swelling in the FOMappear, basic bleeding measures should be under-taken. A bimanual compression with one hand press-ing intraorally and the other extraorally has beensuggested. Alternatively, only the thumb can be usedinside the mouth and the index finger can press on theoutside.22,30 Compression should be applied on thesuspected perforation site and significantly more pos-teriorly, to press on a possibly retracted artery. Com-pressive manipulation of the major arterial suppliers tothe FOM has also been proposed. If the injured vesselarises from the facial artery, pressure over the ante-gonial notch may control bleeding. When the tongueis pulled out, the lingual artery is pressed against thehyoid bone, thus reducing hemorrhage from a trau-matized branching vessel.80 Incisions in the mucosa torelieve the hematoma should be avoided because theymay promote further bleeding.29 Removal of an alreadyinserted implant would also be ineffective21 (Fig. 5).At the same time, one assistant should inform the localmedical center about the situation, while the surgeonshould explain calmly to the patient the nature of thecomplication.
The following steps depend largely on the course ofbleeding. A well-sized hematoma may form in as soonas 2 minutes.23,30 In this case, the operator must beprepared to insert a flexible nasal airway (included inthe emergency equipment) during the first signs of dys-pnea.29 The patient should be then immediately trans-ferred to the informed nearby hospital accompaniedby the surgeon. On the other hand, as bleeding in this
3097.qxd 5/10/04 2:16 PM Page 642

643
J Periodontol • May 2004 Kalpidis, Setayesh
region is frequently self-limited or manageable, a slowlyforming hematoma may be observed.24 However, it isdeemed appropriate to reserve observation for only themildest, slowly-progressing cases. Palpating the rigidmargins has been a reliable clinical method to deter-mine the boundaries of an expanding hematoma andto evaluate its progression.43 If during the monitoringperiod, dyspneic symptoms are noticed then an air-way maneuver should be performed. The hospital envi-ronment is more appropriate for close observationbecause progression of the hematoma to airway com-promise may happen rapidly. Establishment of a morereliable airway and further handling of bleeding shouldbe promptly undertaken by the appropriate medicalteam (Fig. 5).
When a massive hemorrhage in the FOM developsduring implant surgery and the clinician is not ade-quately trained in the establishment of a patent air-way, the patient should be immediately transferred toa hospital. The same rule applies when implant place-ment is performed in a setting without the requiredemergency equipment. Inexperienced or less trainedpractitioners should be reminded that immediate trans-portation to the nearest hospital might be life-saving.
CONCLUSIONSThe case reports presented in this review illustrate a rarebut life-threatening complication of implant surgery inthe anterior segments of the mandible. In fact, the num-ber of reported cases is extremely low compared tothe thousands of implants placed worldwide. Despite,however, the sporadic nature of publications related tothis unexpected complication, there has been an up-ward but steady trend in reporting such cases duringthe last 16 years. This trend gradually unravels a seri-ous problem that has not been adequately addressedto the clinical community.
Patient demographics and clinical data suggest thatintractable bleeding associated with oral implantationmay be encountered in everyday practice, regardlessof age, type, and system of implants used; number ofimplants placed; and degree of edentulism. Therefore,extensive hematomas and dramatic upper airwaysymptomatology may be potentially confronted in everysingle case of implant placement in the interforaminalarea. The reported data also suggest that insertion of“unnecessary” long implants should be avoided, parti-cularly in the canine region, and especially in theatrophic mandible.
The anterior region of the mandible is customarilypreferred for implant placement because of its favor-able anatomic structure. However, the advice oftengiven during implant courses, to start implant surgerywith “easy” cases such as implantation in this area,should be reconsidered in view of the hazardous hem-orrhagic incidents. In fact, when placing implants in the
anterior mandible, the inexperienced surgeon shouldfollow all the appropriate preventive measures to avoidthe discussed life-endangering complications. Ade-quate training in the management of airway occlusionis mandatory if eventually massive bleeding and res-piratory distress occur, despite all precautions taken.
ACKNOWLEDGMENTThe authors are grateful to Dr. Maria D. Kalpidou,Assumption College, Worcester, Massachusetts, for herthoughtful suggestions and editorial assistance duringthe preparation of this manuscript.
REFERENCES1. Adell R, Hansson BO, Brånemark PI, Breine U. Intra-
osseous anchorage of dental prostheses. II. Review of clini-cal approaches. Scand J Plast Reconstr Surg 1970;4:19-34.
2. Brånemark PI, Hansson BO, Adell R, et al. Osseointe-grated implants in the treatment of the edentulous jaw.Experience from a 10-year period. Scand J Plast ReconstrSurg 1977;11(Suppl. 16):1-132.
3. Bartling R, Freeman K, Kraut RA. The incidence ofaltered sensation of the mental nerve after mandibularimplant placement. J Oral Maxillofac Surg 1999;57:1408-1412.
4. Walton JN. Altered sensation associated with implantsin the anterior mandible: A prospective study. J Pros-thet Dent 2000;83:443-449.
5. Krogh PH, Worthington P, Davis WH, Keller EE. Does therisk of complication make transpositioning the inferioralveolar nerve in conjunction with implant placement a“last resort” surgical procedure? Int J Oral MaxillofacImplants 1994;9:249-254.
6. Kan JY, Lozada JL, Boyne PJ, Goodacre CJ,Rungcharassaeng K. Mandibular fracture after endosseousimplant placement in conjunction with inferior alveolarnerve transposition: A patient treatment report. Int J OralMaxillofac Implants 1997;12:655-659.
7. Tolman DE, Keller EE. Management of mandibular frac-tures in patients with endosseous implants. Int J OralMaxillofac Implants 1991;6:427-436.
8. Raghoebar GM, Stellingsma K, Batenburg RHK, VissinkA. Etiology and management of mandibular fracturesassociated with endosteal implants in the atrophicmandible. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2000;89:553-559.
9. Mason ME, Triplett RG, Van Sickels JE, Parel SM.Mandibular fractures through endosseous cylinderimplants: Report of cases and review. J Oral MaxillofacSurg 1990;48:311-317.
10. Esposito M, Hirsch J-M, Lekholm U, Thomsen P. Biologicalfactors contributing to failures of osseointegrated oralimplants. (II) Etiopathogenesis. Eur J Oral Sci 1998;106:721-764.
11. Mombelli A, Lang NP. The diagnosis and treatment ofperi-implantitis. Periodontol 2000 1998;17:63-76.
12. Li KK, Varvares MA, Meara JG. Descending necrotizingmediastinitis: A complication of dental implant surgery.Head Neck 1996;18:192-196.
13. Ueda M, Kaneda T. Maxillary sinusitis caused by dentalimplants: Report of two cases. J Oral Maxillofac Surg1992;50:285-287.
14. Quiney RE, Brimble E, Hodge M. Maxillary sinusitis fromdental osseointegrated implants. J Laryngol Otol 1990;104:333-334.
3097.qxd 5/10/04 2:16 PM Page 643

644
Hemorrhaging and Implant Placement: A Review Volume 75 • Number 5
15. Regev E, Smith RA, Perott DH, Pogrel MA. Maxillarysinus complications related to endosseous implants. IntJ Oral Maxillofac Implants 1995;10:451-461.
16. Chanavaz M. Maxillary sinus: Anatomy, physiology,surgery, and bone grafting related to implantology–Eleven years of surgical experience (1979-1990). J OralImplantol 1990;16:199-209.
17. Aimetti M, Romagnoli R, Ricci G, Massei G. Maxillary sinuselevation: The effect of macrolacerations and microlac-erations of the sinus membrane as determined byendoscopy. Int J Periodontics Restorative Dent 2001;21:581-589.
18. Girdler NM. Fatal sequel to dental implant surgery. J OralRehabil 1994;21:721-722.
19. Davies JM, Campbell LA. Fatal air embolism during den-tal implant surgery: A report of three cases. Can J Anaesth1990;37:112-121.
20. Dwyer S. Near fatal venous nitrogen/air embolism occur-rence while inserting cylindrical endosseous oral implants.J Periodontol 1992;63:63.
21. Krenkel C, Holzner K. Lingual bone perforation as causalfactor in a threatening hemorrhage of the mouth floor dueto a single tooth implant in the canine region (in German).Quintessenz 1986;37:1003-1008.
22. Mason ME, Triplett RG, Alfonso WF. Life-threateninghemorrhage from placement of a dental implant. J OralMaxillofac Surg 1990;48:201-204.
23. Laboda G. Life-threatening hemorrhage after placementof an endosseous implant: Report of a case. J Am DentAssoc 1990;121:599-600.
24. ten Bruggenkate CM, Krekeler G, Kraaijenhagen HA,Foitzik C, Oosterbeek HS. Hemorrhage of the floor of themouth resulting from lingual perforation during implantplacement: A clinical report. Int J Oral Maxillofac Implants1993;8:329-334.
25. Ratschew C, Czernicky W, Watzek G. Life-threateninghemorrhage during placement of dental implants in themandible. A case report (in German). Dtsch ZahnärztlZ 1994;49:65-67.
26. Mordenfeld A, Andersson L, Bergström B. Hemorrhage inthe floor of the mouth during implant placement in theedentulous mandible: A case report. Int J Oral MaxillofacImplants 1997;12:558-561.
27. Darriba MA, Mendonça-Caridad JJ. Profuse bleedingand life-threatening airway obstruction after placementof mandibular dental implants. J Oral Maxillofac Surg1997;55:1328-1330.
28. Panula K, Oikarinen K. Severe hemorrhage after implantsurgery [letter to the editor]. Oral Surg Oral Med OralPathol Oral Radiol Endod 1999;87:2.
29. Givol N, Chaushu G, Halamish-Shani T, Taicher S.Emergency tracheostomy following life-threatening hem-orrhage in the floor of the mouth during immediate implantplacement in the mandibular canine region. J Periodontol2000;71:1893-1895.
30. Niamtu J III. Near-fatal airway obstruction after routineimplant placement. Oral Surg Oral Med Oral Pathol OralRadiol Endod 2001;92:597-600.
31. Boyes-Varley JG, Lownie JF. Haematoma of the floor of themouth following implant placement. SADJ 2002;57:64-65.
32. Weibrich G, Foitzik C, Kuffner H. Life-threatening oralhemorrhage after implantation into the distal rightmandible (in German). Mund Kiefer Gesichtschir 2002;6:442-445.
33. Zimmerman RA, McLean G, Freiman D, Golestaneh Z,Perez M. The diagnosis and therapeutic role of angio-graphy in lingual arterial bleeding. Radiology 1979;133:
639-643.34. Chase CR, Hebert JC, Farnham JE. Post-traumatic
upper airway obstruction secondary to a lingual arteryhematoma. J Trauma 1987;27:953-954.
35. Saah D, Braverman I, Elidan J, Nageris B. Traumaticmacroglossia. Ann Otol Rhinol Laryngol 1993;102:729-730.
36. Woodmansee VA, Rodriguez A, Mirvis S, Fitzgerald B.Genioglossus hemorrhage after blunt facial trauma. AnnEmerg Med 1992;21:440-444.
37. Rosenbaum L, Thurman P, Krantz SB. Upper airwayobstruction as a complication of oral anticoagulationtherapy. Report of three cases. Arch Intern Med 1979;139:1151-1153.
38. Cohen AF, Warman SP. Upper airway obstruction sec-ondary to warfarin-induced sublingual hematoma. ArchOtolaryngol Head Neck Surg 1989;115:718-720.
39. Piper SN, Maleck WH, Kumle B, Deschner E, Boldt J.Massive postoperative swelling of the tongue: Manualdecompression and tactile intubation as a life-savingmeasure. Resuscitation 2000;43:217-220.
40. Lanigan DT, Hey J, West RA. Hemorrhage followingmandibular osteotomies: A report of 21 cases. J OralMaxillofac Surg 1991;49:713-724.
41. Hull M. Life-threatening swelling after mandibularvestibuloplasty. J Oral Surg 1977;35:511-514.
42. Popowich L, Samit A. Respiratory obstruction followingvestibuloplasty and lowering of the floor of the mouth.J Oral Maxillofac Surg 1983;41:255-257.
43. Goldstein BH. Acute dissecting hematoma: A complica-tion of oral and maxillofacial surgery. J Oral Surg 1981;39:40-43.
44. Burke RH, Masch GL. Lingual artery hemorrhage. OralSurg Oral Med Oral Pathol 1986;62:258-261.
45. Krenkel C, Holzner K, Poisel S. Hematoma of the mouthfloor following oral surgery and its anatomical charac-teristics (in German). Dtsch Z Mund Kiefer Gesichtschir1985;9:448-451.
46. Kattan B, Snyder HS. Lingual artery hematoma result-ing in upper airway obstruction. J Emerg Med 1991;9:421-424.
47. Sakamoto E, Miller R, Stratigos GT, Arthur A. Seriouspostextraction hemorrhage into the submandibular space:Report of a case. J Am Dent Assoc 1975;90:654-658.
48. Moghadam HG, Caminiti MF. Life-threatening hemor-rhage after extraction of third molars: Case report andmanagement protocol. J Can Dent Assoc 2002;68:670-674.
49. Funayama M, Kumagai T, Saito K, Watanabe T. Asphyxialdeath caused by postextraction hematoma. Am J ForensicMed Pathol 1994;15:87-90.
50. DuBrul EL. Sicher’s Oral Anatomy, 7th ed. St. Louis:The C.V. Mosby Co.; 1980:354-357.
51. Bavitz JB, Harn SD, Homze EJ. Arterial supply to thefloor of the mouth and lingual gingiva. Oral Surg Oral MedOral Pathol 1994;77:232-235.
52. Hofschneider U, Tepper G, Gahleitner A, Ulm C. Assess-ment of the blood supply to the mental region for reduc-tion of bleeding complications during implant surgeryin the interforaminal region. Int J Oral Maxillofac Implants1999;14:379-383.
53. Homze EJ, Harn SD, Bavitz BJ. Extraoral ligation of thelingual artery: An anatomic study. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1997;83:321-324.
54. DuBrul EL. Sicher’s Oral Anatomy, 7th ed. St. Louis:The C.V. Mosby Co.; 1980:477-485.
55. Cadenat H, Barthelemy R, Combelles R, Fabie M,
3097.qxd 5/10/04 2:16 PM Page 644

645
J Periodontol • May 2004 Kalpidis, Setayesh
Maneaud M. Importance of mandibular vascularizationin maxillofacial surgery (in French). Rev Stomatol ChirMaxillofac 1972;73:60-65.
56. Martin D, Pascal JF, Baudet J, et al. The submentalisland flap: A new donor site. Anatomy and clinical appli-cations as a free or pedicled flap. Plast Reconstr Surg1993;92:867-873.
57. Ragot B, Poirot G. Anatomic study of the vasculariza-tion of the anterior region of the mandible (in French).Rev Odontostomatol 1983;12:49-54.
58. McDonnel D, Reza Nouri M, Todd ME. The mandibularlingual foramen: A consistent arterial foramen in themiddle of the mandible. J Anat 1994;184:363-369.
59. Tepper G, Hofschneider UB, Gahleitner A, Ulm C. Com-puted tomographic diagnosis and localization of bonecanals in the mandibular interforaminal region for pre-vention of bleeding complications during implantsurgery. Int J Oral Maxillofac Implants 2001;16:68-72.
60. Bradley JC. The clinical significance of age changes inthe vascular supply to the mandible. Int J Oral Surg1981;10(Suppl. 1):71-76.
61. Castelli WA, Nasjleti CE, Díaz-Pérez R. Interruption of thearterial inferior alveolar flow and its effects on mandibu-lar collateral circulation and dental tissues. J Dent Res1975;54:708-715.
62. Porter A, Sweet S. A statistical analysis of the incidenceof nutrient channels and foramina in five hundred peri-apical full-mouth radiodontic examinations. Am J OrthodOral Surg 1942;28:427-442.
63. Shiller WR, Wiswell OB. Lingual foramina of the mandible.Anat Rec 1954;119:387-390.
64. Sutton RN. The practical significance of mandibularaccessory foramina. Aust Dent J 1974;19:167-173.
65. Chapnick L. A foramen on the lingual of the mandible.J Can Dent Assoc 1980;46:444-445.
66. Cawood JI, Howell RA. Reconstructive preprostheticsurgery. I. Anatomical considerations. Int J Oral Maxillo-fac Surg 1991;20:75-82.
67. Tallgren A. The continuing reduction of the residual alve-olar ridges in complete denture wearers: A mixed-longi-tudinal study covering 25 years. J Prosthet Dent 1972;27:120-132.
68. Kingsmill VJ. Post-extraction remodeling of the adultmandible. Crit Rev Oral Biol Med 1999;10:384-404.
69. Worthington P. Severe hemorrhage after implant surgery[letter to the editor]. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1999;88:1.
70. Triplett RG. Profuse bleeding and life-threatening airwayobstruction after placement of mandibular dental imp-lants [discussion]. J Oral Maxillofac Surg 1997;55:1330.
71. Rich NM. Vascular trauma. Surg Clin North Am 1973;53:1367-1392.
72. Moreland LW, Corey J, McKenzie R. Ludwig’s angina:Report of a case and review of the literature. Arch InternMed 1988;148:461-466.
73. Remonda L, Schroth G, Caversaccio M, et al. Endovas-cular treatment of acute and subacute hemorrhage in thehead and neck. Arch Otolaryngol Head Neck Surg 2000;126:1255-1262.
74. Williams MY, Mealey BL, Hallmon WW. The role of com-puterized tomography in dental implantology. Int J OralMaxillofac Implants 1992;7:373-380.
75. Schwarz MS, Rothman SL, Rhodes ML, Chafetz N.Computed tomography: Part I. Preoperative assessmentof the mandible for endosseous implant surgery. Int J OralMaxillofac Implants 1987;2:137-141.
76. Adell R, Lekholm U, Brånemark PI. Surgical procedures.In: Brånemark PI, Zarb GA, Albrektsson T, eds. Tissue-Integrated Prostheses. Osseointegration in Clinical Den-tistry. Chicago: Quintessence Publishing Co., Inc.; 1985:214-216.
77. Ivanoff CJ, Sennerby L, Lekholm U. Influence of mono-and bicortical anchorage on the integration of titaniumimplants. A study in the rabbit tibia. Int J Oral Maxillo-fac Surg 1996;25:229-235.
78. Winkler S, Morris HF, Ochi S. Implant survival to 36months as related to length and diameter. Ann Peri-odontol 2000;5:22-31.
79. ten Bruggenkate CM, Asikainen P, Foitzik C, Krekeler G,Sutter F. Short (6-mm) non-submerged dental implants:Results of a multicenter clinical trial of 1 to 7 years. IntJ Oral Maxillofac Implants 1998;13:791-798.
80. Misch CE. Root form surgery in the edentulous mandible:Stage I implant insertion. In: Misch CE, ed. ContemporaryImplant Dentistry, 2nd ed. St. Louis: The C.V. MosbyCo.; 1999:353-354.
Correspondence: Dr. Christos D.R. Kalpidis, Periodontal HealthCenter, 14 Karolou Diehl St., 546 23 Thessaloniki, Greece.Fax: 30-2310-272-228; e-mail: [email protected].
Accepted for publication September 12, 2003.
3097.qxd 5/10/04 2:16 PM Page 645