Embed Size (px)
Citation preview
Hepatitis B and Pregnancy
Tram T. Tran MD Medical Director, Liver Transplant
Director, Hepatology Cedars Sinai Medical Center
Associate Professor of Medicine, Geffen UCLA School of Medicine Los Angeles, CA
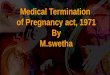
New HBV Infections by Year: United States (1966-2006)
01234567891011121314
Inci
denc
e (p
er 1
00,0
00)
66 68 70 72 74 76 78 80 82 84 86 88 90 92 94 96 98 00 02 04 06 Year
Wasley A, et al. MMWR Surveill Summ. 2008;57:1-24.
Infant Immunization Recommended
Vaccine Licensed
HBsAg Screening of Pregnant Women Recommended
OSHA Rule Enacted
Adolescent Immunization Recommended
0
0.2
0.4
0.6
0.8
1
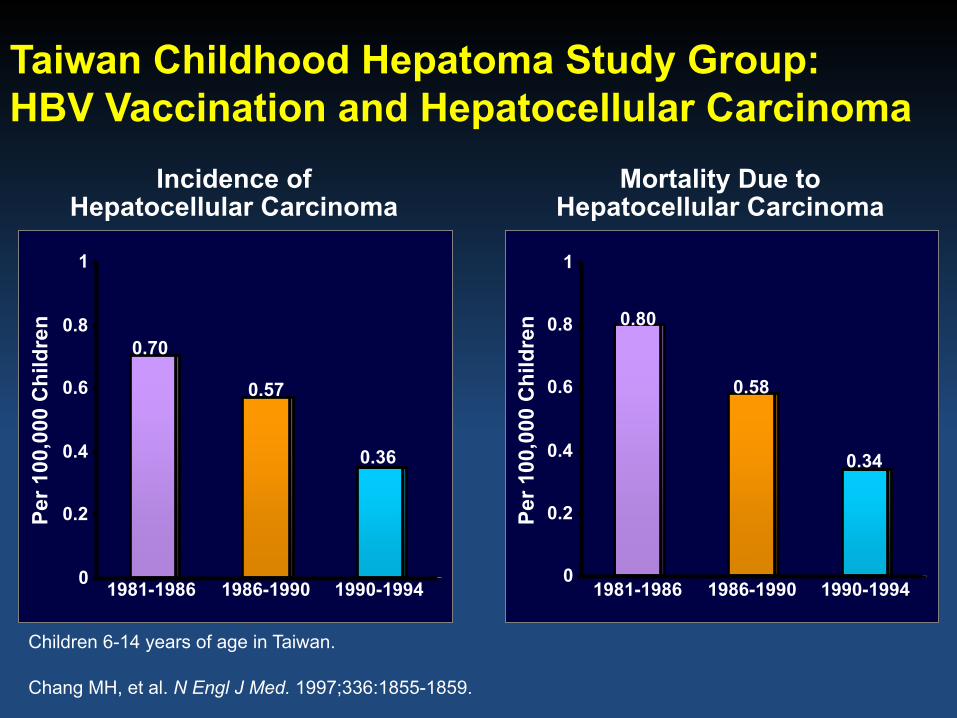
Taiwan Childhood Hepatoma Study Group: HBV Vaccination and Hepatocellular Carcinoma
Per 1
00,0
00 C
hild
ren
0.70
0.57
0.36
Chang MH, et al. N Engl J Med. 1997;336:1855-1859.
Incidence of Hepatocellular Carcinoma
1986-1990 1981-1986 1990-1994
Children 6-14 years of age in Taiwan.
0
0.2
0.4
0.6
0.8
1
Per 1
00,0
00 C
hild
ren 0.80
0.58
0.34
Mortality Due to Hepatocellular Carcinoma
1986-1990 1981-1986 1990-1994
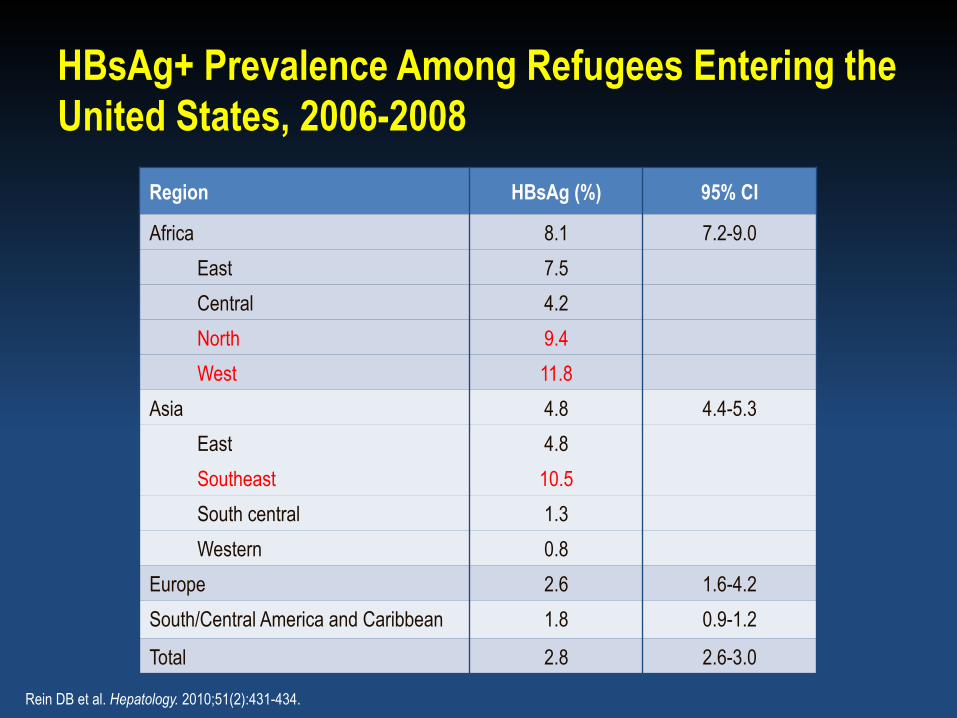
HBsAg+ Prevalence Among Refugees Entering the United States, 2006-2008
Region HBsAg (%) 95% CI
Africa 8.1 7.2-9.0 East 7.5 Central 4.2 North 9.4 West 11.8
Asia 4.8 4.4-5.3 East 4.8 Southeast 10.5 South central 1.3 Western 0.8
Europe 2.6 1.6-4.2 South/Central America and Caribbean 1.8 0.9-1.2
Total 2.8 2.6-3.0
Rein DB et al. Hepatology. 2010;51(2):431-434.
Treatment During Pregnancy: Two SEPARATE Issues
• Treatment for the woman’s benefit – Why treat NOW?
• Woman’s health à advanced disease • Already on therapy à concern for flare • Concern for progression
• Prevention of transmission to infant – No clear AASLD guidelines on treatment – Risk/benefit of treatment in third trimester
AASLD, American Association for the Study of Liver Diseases.
Two Separate Issues in Women of Childbearing Age
• Maternal health • Perinatal transmission
Treatment for Woman’s Benefit
• Scenario One: She has cirrhosis – Unlikely to conceive: incidence of pregnancy in cirrhosis
—1 in 5950 – High rates of spontaneous abortion, premature birth,
and perinatal death – GI bleeding most common complication – Would likely benefit from treatment – Benefit of therapy likely outweighs risks
GI, gastrointestinal. Aggarwal N et al. Aust N Z J Obstet Gynaecol. 1999;39(4):503-506.

Treatment for Woman’s Benefit
• Scenario Two: She has already been on therapy • What is risk of flare if you take her off?
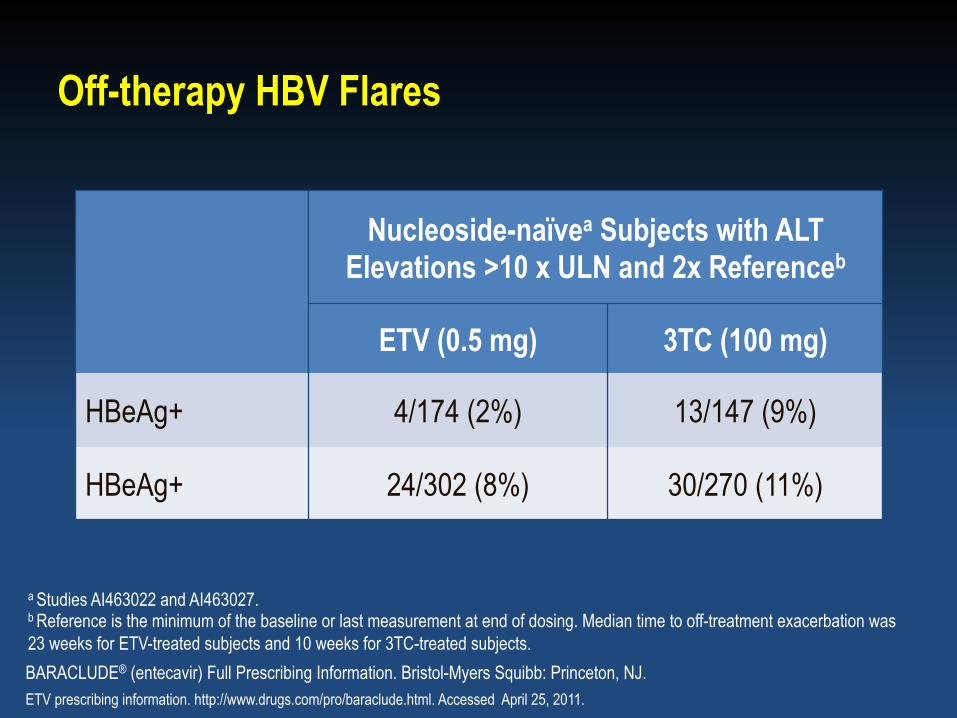
a Studies AI463022 and AI463027. b Reference is the minimum of the baseline or last measurement at end of dosing. Median time to off-treatment exacerbation was 23 weeks for ETV-treated subjects and 10 weeks for 3TC-treated subjects.
Off-therapy HBV Flares
Nucleoside-naïvea Subjects with ALT Elevations >10 x ULN and 2x Referenceb
ETV (0.5 mg) 3TC (100 mg)
HBeAg+ 4/174 (2%) 13/147 (9%)
HBeAg+ 24/302 (8%) 30/270 (11%)
BARACLUDE® (entecavir) Full Prescribing Information. Bristol-Myers Squibb: Princeton, NJ. ETV prescribing information. http://www.drugs.com/pro/baraclude.html. Accessed April 25, 2011.
Treatment for Woman’s Benefit
• Scenario Three: You are concerned about progression of disease – Not likely over a short period of pregnancy

Perinatal Transmission of HBV: an Australian Experience
HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus. Wiseman E et al. Med J Aust. 2009;190:489-492.
HBV DNA (copies/mL) Low: <105
High: 105 to 108
Very high: >108
HBsAg+ pregnant women
(N = 313)
Women with detectable HBV DNA (n = 213)
Infants tested (N = 138)
HBsAg+ infants (n = 4)
HBeAg (%) Negative (n = 122)
Positive (n = 91)
Low HBV DNA (n = 115) 106 9
High HBV DNA (n = 29) 16 13
Very high HBV DNA (n = 69) 0 69
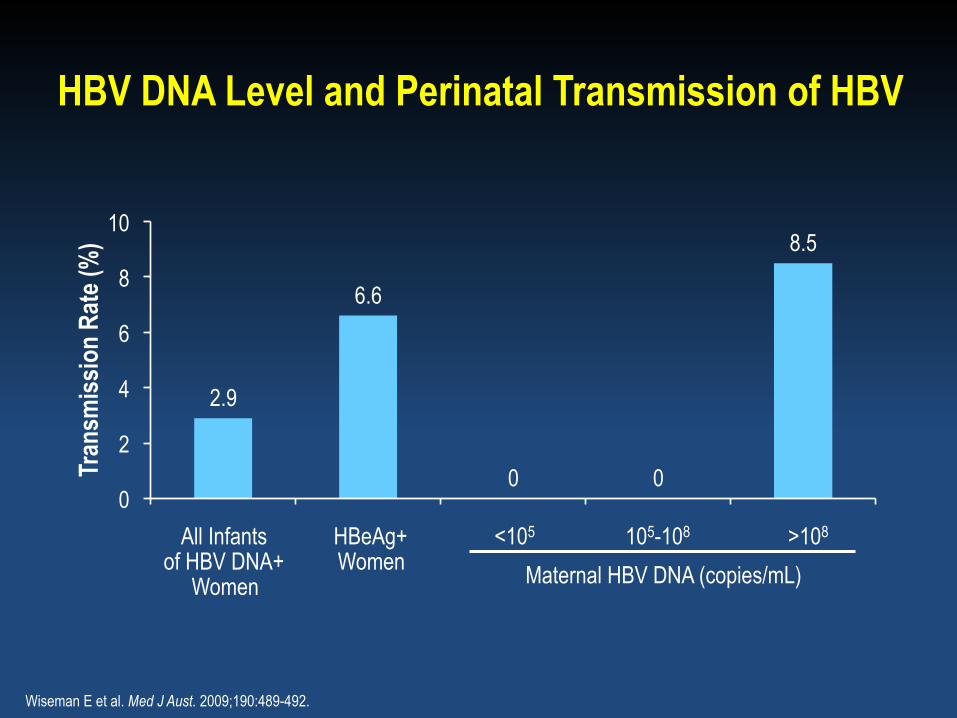
HBV DNA Level and Perinatal Transmission of HBV
>108 All Infants of HBV DNA+
Women
HBeAg+ Women
<105 105-108
Maternal HBV DNA (copies/mL)
Wiseman E et al. Med J Aust. 2009;190:489-492.
2.9
6.6
0 0
8.5
0
2
4
6
8
10
Tran
smiss
ion
Rate
(%)
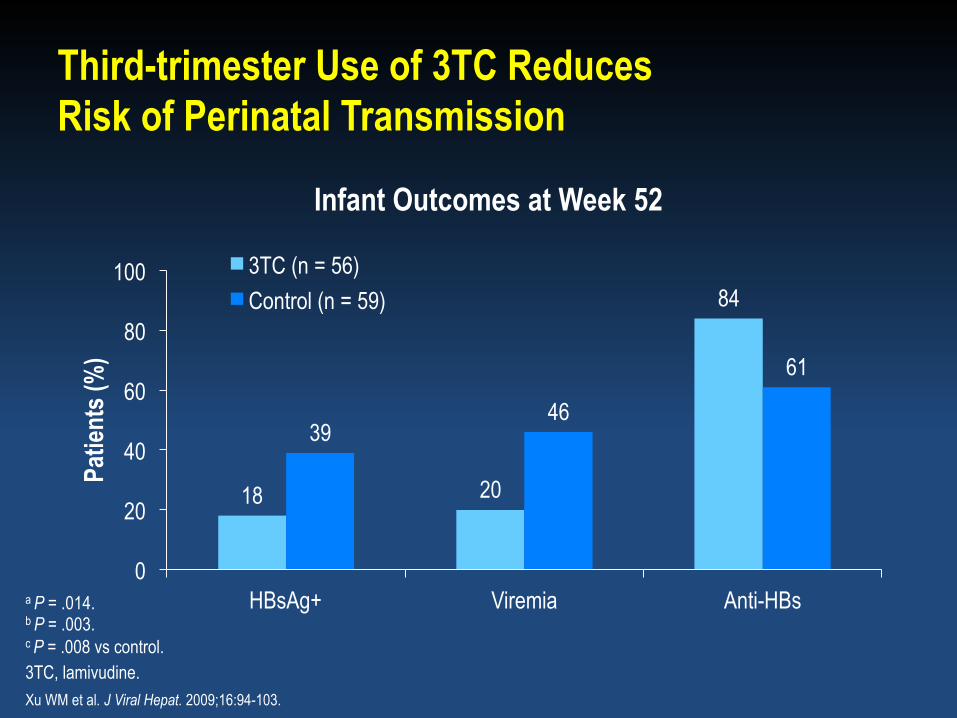
Third-trimester Use of 3TC Reduces Risk of Perinatal Transmission
a P = .014. b P = .003. c P = .008 vs control. 3TC, lamivudine. Xu WM et al. J Viral Hepat. 2009;16:94-103.
18 20
84
39 46
61
0
20
40
60
80
100
HBsAg+ Viremia Anti-HBs
Patie
nts (
%)
Infant Outcomes at Week 52
3TC (n = 56) Control (n = 59)
a b
c
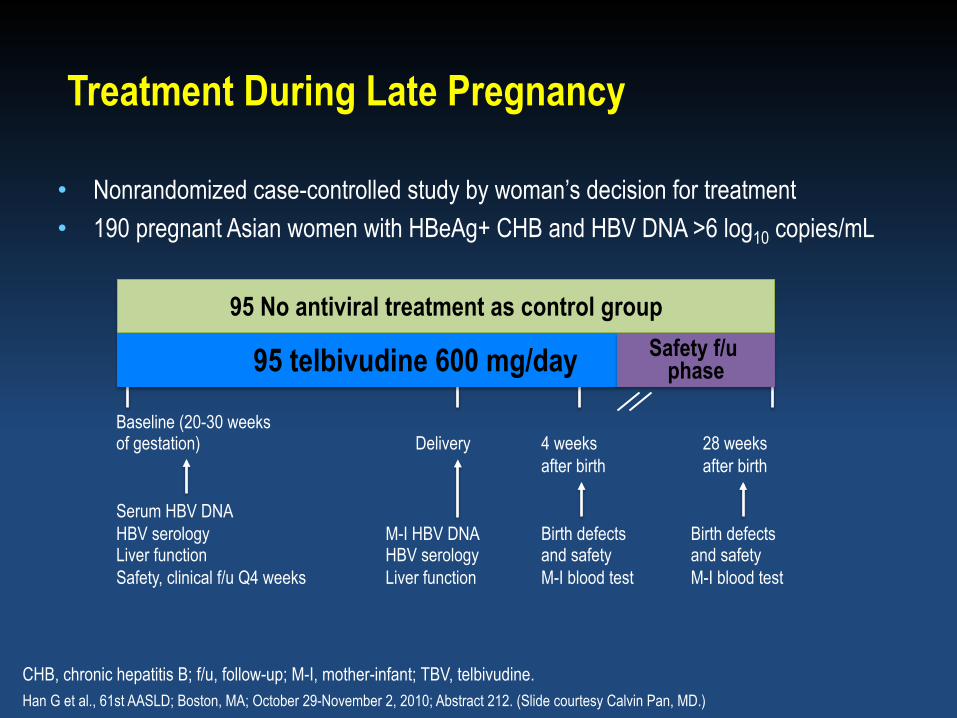
Treatment During Late Pregnancy
• Nonrandomized case-controlled study by woman’s decision for treatment • 190 pregnant Asian women with HBeAg+ CHB and HBV DNA >6 log10 copies/mL
CHB, chronic hepatitis B; f/u, follow-up; M-I, mother-infant; TBV, telbivudine. Han G et al., 61st AASLD; Boston, MA; October 29-November 2, 2010; Abstract 212. (Slide courtesy Calvin Pan, MD.)
95 No antiviral treatment as control group
95 telbivudine 600 mg/day Safety f/u phase
Baseline (20-30 weeks of gestation) Delivery 4 weeks 28 weeks
after birth after birth Serum HBV DNA HBV serology M-I HBV DNA Birth defects Birth defects Liver function HBV serology and safety and safety Safety, clinical f/u Q4 weeks Liver function M-I blood test M-I blood test
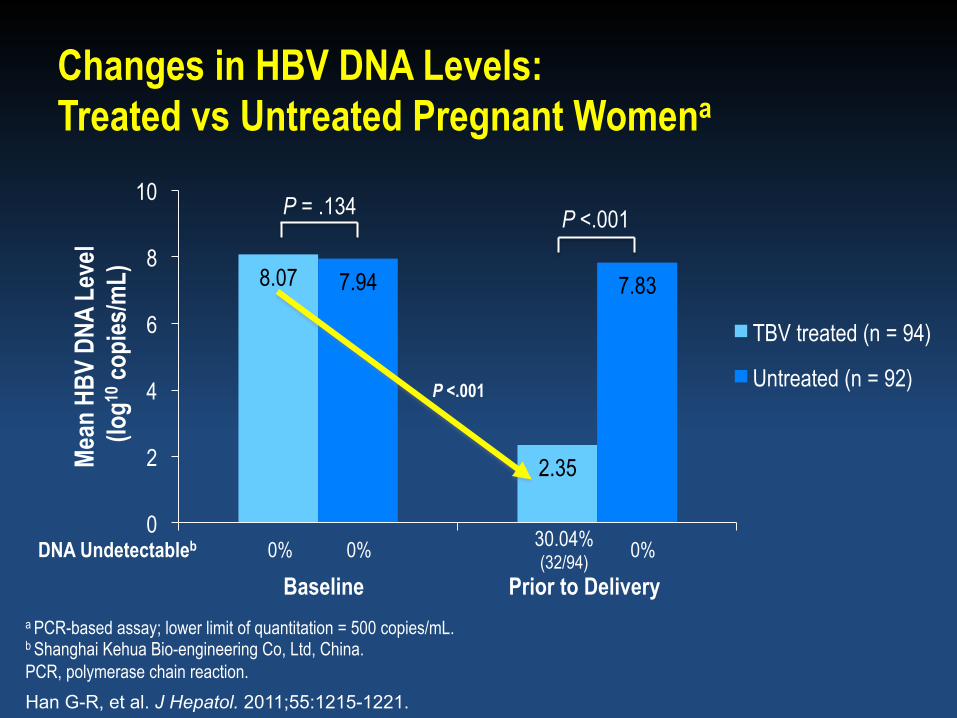
Changes in HBV DNA Levels: Treated vs Untreated Pregnant Womena
a PCR-based assay; lower limit of quantitation = 500 copies/mL. b Shanghai Kehua Bio-engineering Co, Ltd, China. PCR, polymerase chain reaction.
8.07
2.35
7.94 7.83
0
2
4
6
8
10
Mean
HBV
DNA
Lev
el (l
og10
copi
es/m
L)
TBV treated (n = 94)
Untreated (n = 92)
P = .134 P <.001
DNA Undetectableb 0% 0% 30.04% (32/94) 0%
Baseline Prior to Delivery
P <.001
Han G-R, et al. J Hepatol. 2011;55:1215-1221.
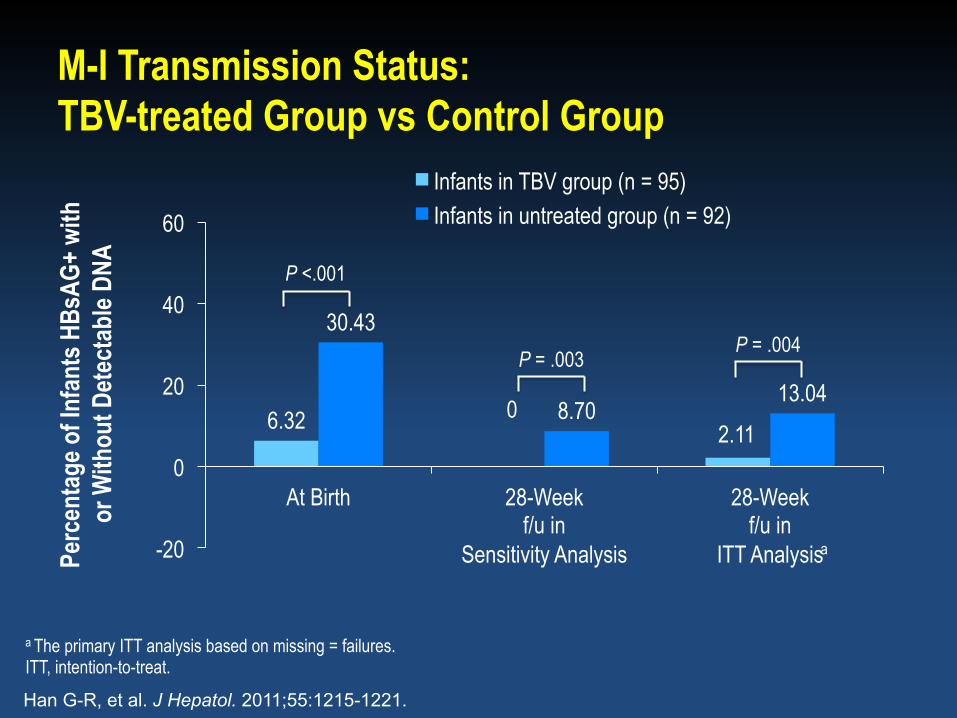
a The primary ITT analysis based on missing = failures. ITT, intention-to-treat.
M-I Transmission Status: TBV-treated Group vs Control Group
6.32 0 2.11
30.43
8.70 13.04
-20
0
20
40
60
At Birth 28-Week f/u in
Sensitivity Analysis
28-Week f/u in
ITT Analysis
Infants in TBV group (n = 95) Infants in untreated group (n = 92)
P <.001
P = .003 P = .004
Perc
enta
ge o
f Inf
ants
HBs
AG+ w
ith
or W
ithou
t Det
ecta
ble D
NA
a
Han G-R, et al. J Hepatol. 2011;55:1215-1221.
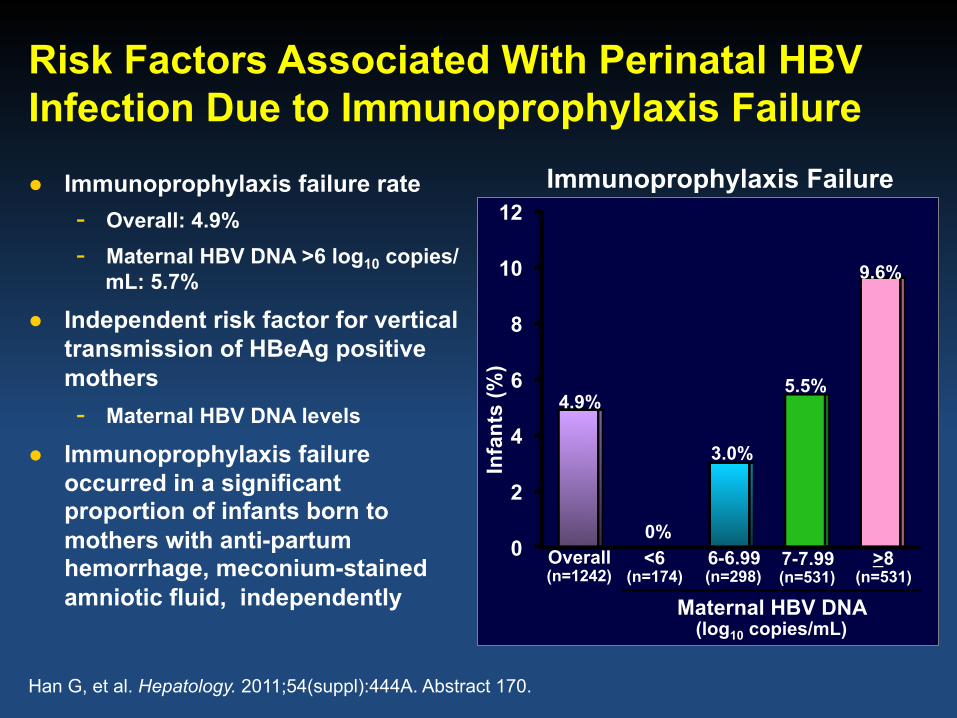
Risk Factors Associated With Perinatal HBV Infection Due to Immunoprophylaxis Failure
0
2
4
6
8
10
12
Infa
nts
(%)
4.9%
3.0%
Immunoprophylaxis Failure
Overall (n=1242)
Maternal HBV DNA (log10 copies/mL)
Han G, et al. Hepatology. 2011;54(suppl):444A. Abstract 170.
<6 (n=174)
6-6.99 (n=298)
7-7.99 (n=531)
>8 (n=531)
0%
5.5%
9.6%
● Immunoprophylaxis failure rate - Overall: 4.9% - Maternal HBV DNA >6 log10 copies/
mL: 5.7%
● Independent risk factor for vertical transmission of HBeAg positive mothers - Maternal HBV DNA levels
● Immunoprophylaxis failure occurred in a significant proportion of infants born to mothers with anti-partum hemorrhage, meconium-stained amniotic fluid, independently
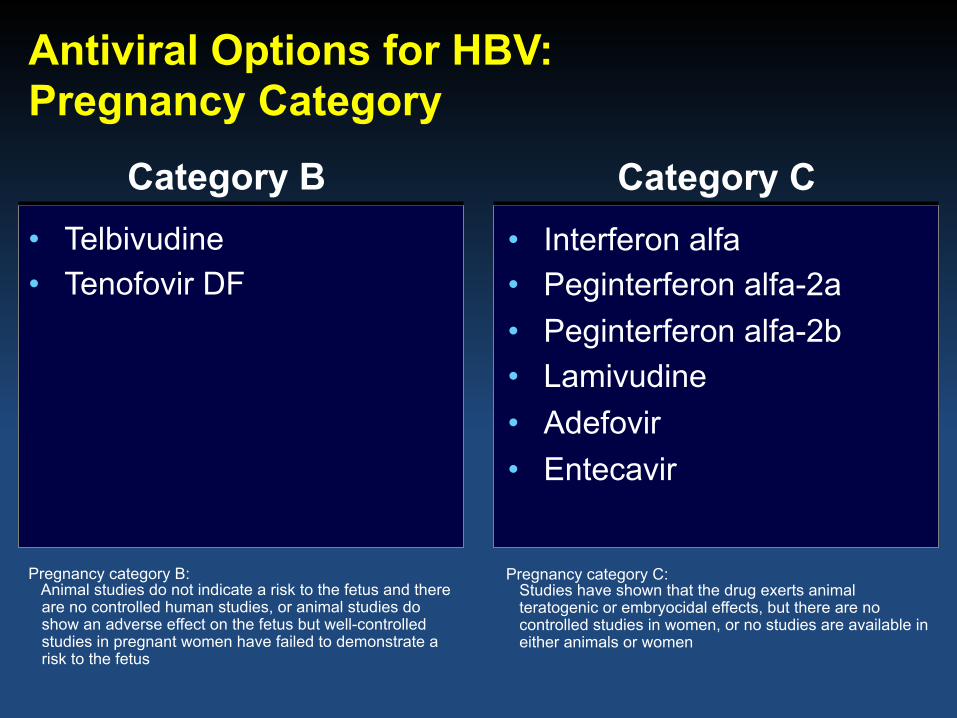
Antiviral Options for HBV: Pregnancy Category
• Telbivudine • Tenofovir DF
• Interferon alfa • Peginterferon alfa-2a • Peginterferon alfa-2b • Lamivudine • Adefovir • Entecavir
Category B Category C
Pregnancy category B: Animal studies do not indicate a risk to the fetus and there are no controlled human studies, or animal studies do show an adverse effect on the fetus but well-controlled studies in pregnant women have failed to demonstrate a risk to the fetus
Pregnancy category C: Studies have shown that the drug exerts animal teratogenic or embryocidal effects, but there are no controlled studies in women, or no studies are available in either animals or women
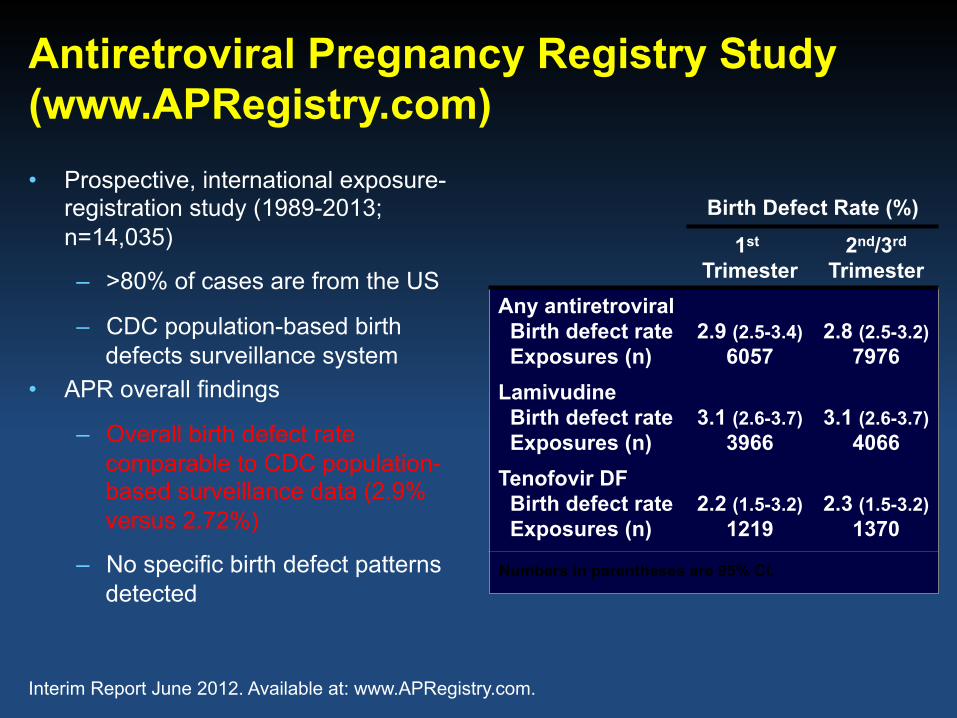
Antiretroviral Pregnancy Registry Study (www.APRegistry.com) • Prospective, international exposure-
registration study (1989-2013; n=14,035)
– >80% of cases are from the US
– CDC population-based birth defects surveillance system
• APR overall findings
– Overall birth defect rate comparable to CDC population-based surveillance data (2.9% versus 2.72%)
– No specific birth defect patterns detected
Birth Defect Rate (%)
1st Trimester
2nd/3rd
Trimester Any antiretroviral Birth defect rate Exposures (n)
2.9 (2.5-3.4)
6057
2.8 (2.5-3.2)
7976 Lamivudine Birth defect rate Exposures (n)
3.1 (2.6-3.7)
3966
3.1 (2.6-3.7)
4066 Tenofovir DF Birth defect rate Exposures (n)
2.2 (1.5-3.2)
1219
2.3 (1.5-3.2)
1370
Numbers in parentheses are 95% CI.
Interim Report June 2012. Available at: www.APRegistry.com.
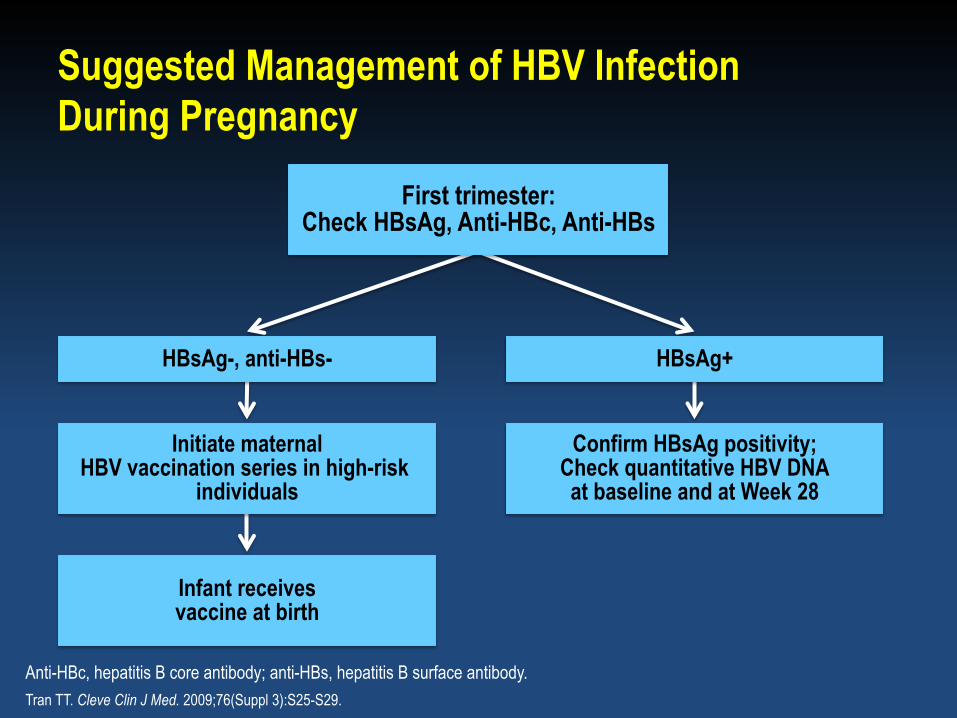
Suggested Management of HBV Infection During Pregnancy
Anti-HBc, hepatitis B core antibody; anti-HBs, hepatitis B surface antibody. Tran TT. Cleve Clin J Med. 2009;76(Suppl 3):S25-S29.
First trimester: Check HBsAg, Anti-HBc, Anti-HBs
Confirm HBsAg positivity; Check quantitative HBV DNA at baseline and at Week 28
Infant receives vaccine at birth
Initiate maternal HBV vaccination series in high-risk
individuals
HBsAg+ HBsAg-, anti-HBs-

Suggested Management of HBV Infection During Pregnancy (cont’d)
a May consider treatment if previous child HBV+. Tran TT. Cleve Clin J Med. 2009;76(Suppl 3):S25-S29.
HBV DNA <108 copies/mLa
HBV DNA >108 copies/mL
Infant receives HBIG + HBV vaccine at birth
Refer for consideration for treatment with 3TC, TDF, or TBV at Week 32
Yes
HBsAg+
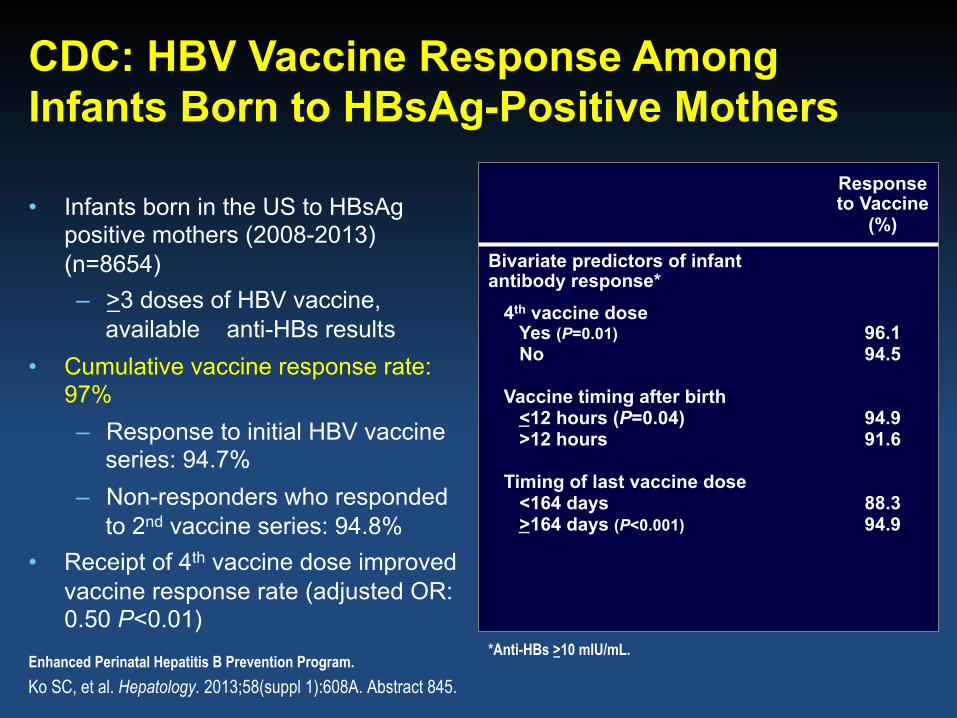
CDC: HBV Vaccine Response Among Infants Born to HBsAg-Positive Mothers
• Infants born in the US to HBsAg positive mothers (2008-2013) (n=8654) – >3 doses of HBV vaccine,
available anti-HBs results • Cumulative vaccine response rate:
97% – Response to initial HBV vaccine
series: 94.7% – Non-responders who responded
to 2nd vaccine series: 94.8% • Receipt of 4th vaccine dose improved
vaccine response rate (adjusted OR: 0.50 P<0.01)
Ko SC, et al. Hepatology. 2013;58(suppl 1):608A. Abstract 845.
Response to Vaccine
(%)
Bivariate predictors of infant antibody response* 4th vaccine dose Yes (P=0.01) No Vaccine timing after birth <12 hours (P=0.04) >12 hours Timing of last vaccine dose <164 days >164 days (P<0.001)
96.1 94.5
94.9 91.6
88.3 94.9
*Anti-HBs >10 mIU/mL. Enhanced Perinatal Hepatitis B Prevention Program.
HBV Flares Postpartum
• 38 pregnancies in 31 chronic HBsAg+ women – 24 (63%) HBeAg+; 14 (37%) HBeAg-
• Significant increase in liver-disease activity was seen after delivery – Defined as 3x increase in ALT within 6 months of delivery
• 17 (45%) with exacerbations postpartum • Median maximal ALT increase 4 x ULN • None led to decompensation
ALT, alanine aminotransferase; ULN, upper limit of normal. Ter Borg MJ et al. J Viral Hepat. 2008;15(1):37-41.

Elective Cesarian Delivery and Risk of Perinatal Transmission of HBV
HB
V In
fect
ion
in In
fant
s (%
)
Transmission of HBV Infection (7-12 Months of Age)
3.4% 4.2%
1.4%*
Pan CQ, et al. Clin Gastroenterol Hepatol. 2013;Apr 29. [Epub ahead of print].
HBsAg-Positive Mothers (n=673/240/496)
Vaginal delivery Emergency cesarian Elective cesarian
Retrospective, single-center, chart review study. All infants received standard HBV prophylaxis (2007-2011). *P<0.05 versus vaginal delivery and emergency cesarian.
6.3%
7.6%
2.6%*
7.2%
8.7%
2.9%*
HBeAg-Positive Mothers (n=365/131/273)
Mothers With HBV DNA >6 log10 Copies/mL (n=319/115/238)
Conclusions
• Vaccination/immunoprophylaxis is the MOST important preventative strategy
• Perinatal transmission risk is greatest in those with high maternal viremia: HBV DNA >8 logs
• Third-trimester treatment may reduce the risk of HBV transmission, but data are limited