Embed Size (px)
Citation preview

Hepatitis B vaccinatie bij non-responders
Stijn Raven; GGD West-BrabantRIVM, CIb | EPI
Transmissiedag, 26 maart 2019
(Potential) conflict of interest See below
Potentially relevant companyrelationships in connection withevent
none
• Sponsorship or research funding
• Fee or other (financial) payment• Shareholder• Other relationship, i.e. …
this study was supported by the National Institute of Public Health and the Environment [RIVM programmabudget]
• vaccines used in this study were provided by GlaxoSmithKline and Merck Sharp &Dome
• none• none• none
Disclosure of speaker’s interests
Investigator initiated study

Terug naar 2010.....• Student verloskunde: non-responder (<10 IU/l)• Moet stoppen met de opleiding• Vraag huisarts: kan de GGD iets betekenen?
Beschermende antistoffen: anti-HBs > 1000 IU/l

Praktijkvraag• Literatuur: vaak studies met nogal wat
(methodologische) beperkingen• Richtlijn: expert opinion• Praktijk: divers beleid
Bepalen van de immunogeniciteit van:- HBVaxPro-40- Fendrix- Twinrix
Vergeleken met een standaard revaccinatie serie van 3 vaccinaties
HBVaxPro-10ofEngerix-B
Doel van de studie


480 randomised
≈640 screened for eligibility
25% declined to participate*
114 assignedHBVaxPro‐40
118 assigned Twinrix
124 assigned Fendrix
124 assigned control‐group
109 completed 3rd vaccination
114 completed 3rd vaccination
119 completed 3rd vaccination
117 completed 3rd vaccination
Trial flow diagram
* Gebaseerd op de gegevens van een deel van de centra
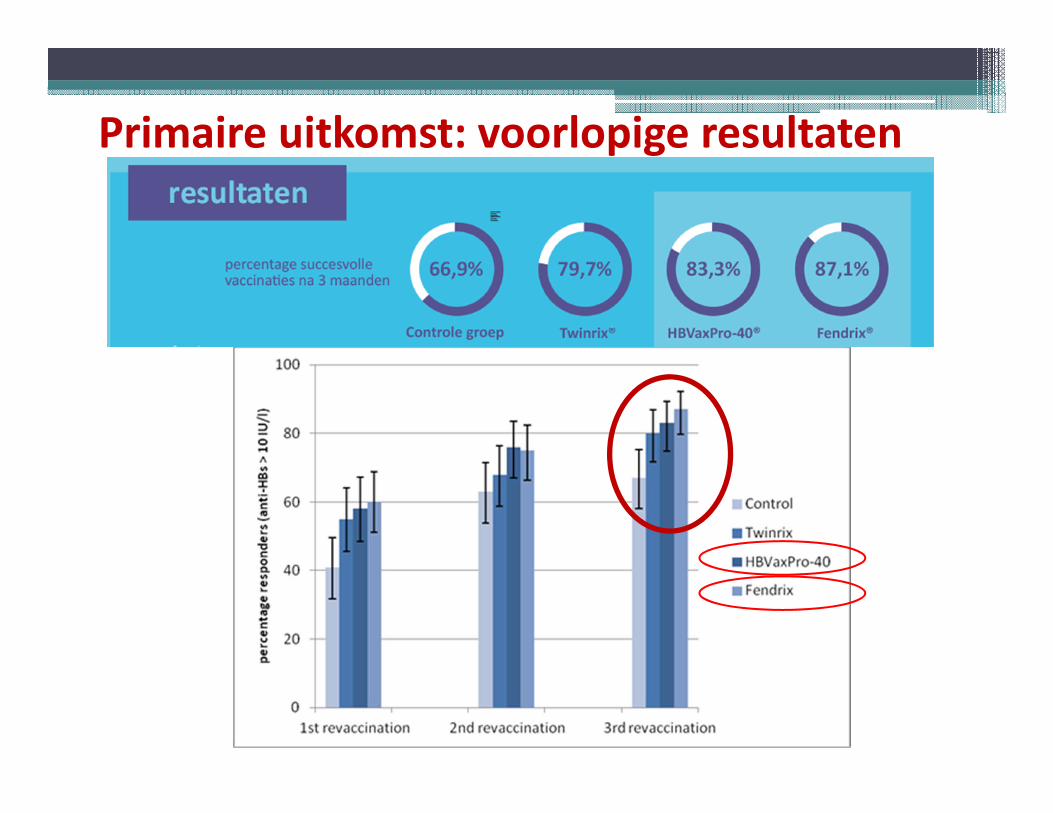
Primaire uitkomst: voorlopige resultaten

Primaire uitkomst: voorlopige resultaten
Δ responders anti-HBs in IU/L
Control (66.9%): ref. 62
Twinrix (79.7%) vs Control: 12·7% (1·6-23·9) 85
HBVaxPro-40(83.3%) vs Control: 16·4% (5·4-27·4) 111
Fendrix(87.1%) vs Control: 20·2% (9·7-30·6) 234
(p-value)
0·31
< 0·0005
< 0·0005

Secundaire uitkomst: indeling naar primaire titerhoogte
Poor-responderZero-responder

HBVax-Pro-40 Twinrix Fendrix Control
Systemic
myalgia 44,1% 27,4% 67,3% 32,7%
fever 3,3% 3,2% 1,9% 1,0%
Local
pain 16,5% 22,3% 59,4% 19,4%
erythema 7,7% 9,6% 11,5% 7,1%
edema 6,6% 9,6% 27,6% 3,1%
Serious adverse events
0 0 1* 0
Secondary outcome: adverse events
Table: reactogenicity within seven days after the first revaccination pervaccine group

• Revaccinatie met Fendrix of HBVaxPro-40 resulteerde in eenhoger percentage responders en hogere anti-HBs titers.
• Voor non-responders hebben de vaccins Fendrix en HBVaxPro-40 de voorkeur bij een revaccinatie, zeker bij de ‘zero-responders’
• Rol van de primaire titer (‘zero-responders’ en ‘poor-responders’) kan gebruikt worden in de beslissing van vaccinkeuze. Dit vraagt nog nader onderzoek voor beter begrip entoepasbaarheid.
Conclusie & aanbevelingen

Dank jullie wel!
National Institute for Public Health and the Environment [RIVM programmabudget] funded this work. GlaxoSmithKline and Merck Sharp & Dohme provided the vaccines used in this study. We thank all the participating centres for their support; Marita Werner, and Marga Smit at the South Limburg Public Health Service; Mieke Croughs, and Maddy van Lent at Regional Public Health Service Hart voor Brabant, Fleur Groenendijk at Regional Public Health Service Zeeland, Kitty Suijk at Leiden University Medical Centre, Leiden; all the travel nurses and Bert Doornekamp at Ease travel Clinic & Health Support; Astrid Oude Lashof at the Department of Medical Microbiology, Maastricht University Medical Center (Maastricht UMC+), Maastricht; Adrie van ‘t Hof, Ellen Verspuij-Van der Eijk at Regional Public Health Zuid Holland Zuid; John van Gulik, Diana Pols, and Angelique Blom at the Regional Public Health Service Rotterdam-Rijnmond; Yvonne Sterken at the Regional Public Health Service Gelderland-Zuid; Yvette Donkers, and Anja Kruis at the Regional Public Health Service Brabant-Zuidoost; Carol Niesen at the Regional Public Health Service Limburg-Noord; Marijke van Cooten, Leanne van der Hoek, Johan Versteegen, and Kees Dirksen at the Regional Public Health Service Den Haag, Annemarie Siebelink, and Maaike Bosschart at the Regional Public Health Service Gelderland Midden; Greet Boland at Utrecht University Medical Centre, Utrecht; Anne de Vries, and Nicole Leerssen at the Regional Public Health Service Kennemerland; We thank Ashis Brahma Lieke Winkeler, and Marieke Laheij, at the Regional Public Health Service Noord- en Oost-Gelderland. José A. Ferreira from the National Institute for Public Health and the Environment for his valuable comments on the data analysis. We thank the laboratory staff and Domenique van Adrichem for their contribution to the laboratory tests at the Department of Medical Microbiology of Leiden University Medical Center.

Dank jullie wel!

Maastricht UMC+:Christian Hoebe
RadboudUMC:Jeannine Hautvast
Rijksinstituut voor Volksgezondheid en MilieuJim van Steenbergen
LUMC:• Leo Visser • Ann Vossen• Anna Roukens• Domenique van Adrichem





























