Embed Size (px)
DESCRIPTION
medicine
Citation preview
Hepatocellular Carcinoma
GI Practice Guideline
Michael Sanatani, MD, FRCPC (Medical Oncologist)
Walter Kocha, MD, FRCPC (Medical Oncologist)
Approval Date:
October 2006
This guideline is a statement of consensus of the GI Disease Site Team regarding their views of currently accepted approaches to treatment. It is not intended to replace the independent medical judgement of the physician in the context of individual clinical circumstances to determine any patient’s care or treatment.
2
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Table of Contents Background................................................................................................................ 3 TNM Staging ............................................................................................................. 4 Overall Pathway – Hepatocellular Carcinoma........................................................... 5 Investigations – Required Work-up........................................................................... 6 AASLD (2005) Diagnostic Approach ....................................................................... 7 Investigations – Surgical Assessment........................................................................ 8 Barcelona/AASLD Approach to surgical Assessment .............................................. 9 Prognosis in U.S. Population by Surgical/Interventional .......................................... 10 Treatment Received Treatment Curative Intent ..................................................................................................... 11 Palliative Intent (localized) .................................................................................. 12 Palliative Intent (systemic) .................................................................................. 13 Overall Pathway......................................................................................................... 14 References.................................................................................................................. 15 Authors and Contact .................................................................................................. 16

3
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Hepatocellular Carcinoma GI Practice Guideline
Background • Most common in subsahara Africa, Orient. • Risk factors:
• Infection − Hep B, C esp. genotype 1b
• Cirrhosis
• Environmental - Androgenss - aflatoxins - EtOH - tobacco - N-nitrosylated compounds - algae toxins - Thorotrast contrast medium - pyrrolizidine alkaloids - ?betel nuts?
• Presentation - abdominal pain - anorexia - bone pain - intraperitoneal bleed - paraneoplastic hypoglycemia/erythrocytosis - hypercalcemia - diarrhea.

4
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
TNM Staging
Fibrosis score 5-6 (severe fibrosis or cirrhosis)F1
Fibrosis score 0-4 (none to moderate fibrosis)F0
Fibrosis Score (F)
Distant metastasisM1
No distant metastasisM0
Distant metastasis cannot be assessedMX
Distant metastasis (M)
Regional lymph node metastasisN1
No regional lymph node metastasisN0
Regional lymph nodes cannot be assessedNX
Regional lymph nodes (N)
Tumors with direct invasion of adjacent organs other than the gallbladder or with perforation of the visceral peritoneum
T4
Multiple tumors more than 5 cm or tumor involving a major branch of the portal or hepatic vein(s)
T3
Solitary tumor with vascular invasion, or multiple tumors none more than 5 cm
T2
Solitary tumor without vascular invasionT1
No evidence of primary tumorT0
Primary tumor cannot be assessedTX
Primary Tumor (T)
Fibrosis score 5-6 (severe fibrosis or cirrhosis)F1
Fibrosis score 0-4 (none to moderate fibrosis)F0
Fibrosis Score (F)
Distant metastasisM1
No distant metastasisM0
Distant metastasis cannot be assessedMX
Distant metastasis (M)
Regional lymph node metastasisN1
No regional lymph node metastasisN0
Regional lymph nodes cannot be assessedNX
Regional lymph nodes (N)
Tumors with direct invasion of adjacent organs other than the gallbladder or with perforation of the visceral peritoneum
T4
Multiple tumors more than 5 cm or tumor involving a major branch of the portal or hepatic vein(s)
T3
Solitary tumor with vascular invasion, or multiple tumors none more than 5 cm
T2
Solitary tumor without vascular invasionT1
No evidence of primary tumorT0
Primary tumor cannot be assessedTX
Primary Tumor (T)
M1
M0
M0
M0
M0
M0
Any N
N1
N0
N0
N0
N0
Any TStage IV
Any TStage IIIC
T4Stage IIIB
T3Stage IIIA
T2Stage II
T1Stage I
Stage grouping
M1
M0
M0
M0
M0
M0
Any N
N1
N0
N0
N0
N0
Any TStage IV
Any TStage IIIC
T4Stage IIIB
T3Stage IIIA
T2Stage II
T1Stage I
Stage grouping
<3 mg/dl>3mg/dlBilirubin
>3 mg/dl<3 mg/dlAlbumin
Clinically absentClinically detectableAscites
<50 percent>50 percentTumor size*
NegativePositiveCriteria
<3 mg/dl>3mg/dlBilirubin
>3 mg/dl<3 mg/dlAlbumin
Clinically absentClinically detectableAscites
<50 percent>50 percentTumor size*
NegativePositiveCriteria
* Largest cross-sectional area of tumor to largest cross-sectional area of the liver
Three of four positivesIII
One or two positivesII
No positiveI
Stage
* Largest cross-sectional area of tumor to largest cross-sectional area of the liver
Three of four positivesIII
One or two positivesII
No positiveI
Stage
Okuda Staging System for Hepatocellular Carcinoma – The okuda system is commonly used for staging hepatocellular carcinoma. Survival correlates with the Okuda stage in untreated patients (8.3, 2.0 and 0.7 for stages I, II, and III, respectively). Adapted from Okuda, K. Ohtuiki, T, Obata, H, et al., Cancer 1985; 56:918
5
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
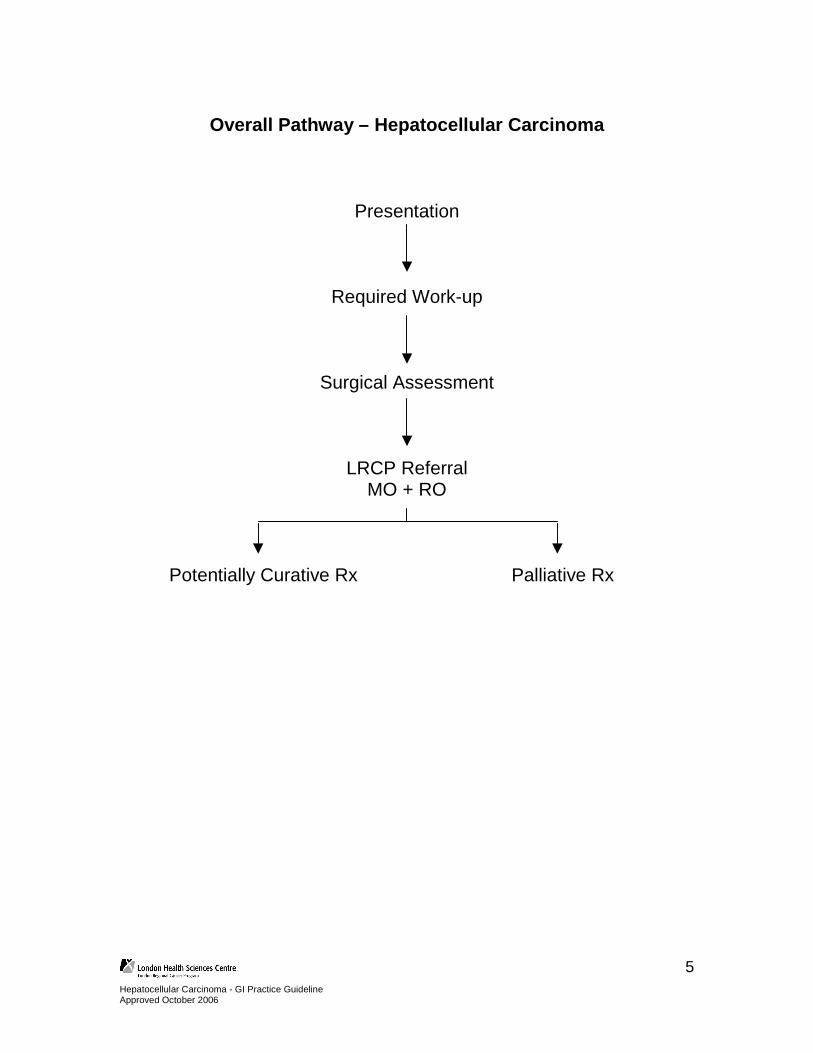
Overall Pathway – Hepatocellular Carcinoma
Presentation
Required Work-up
Surgical Assessment
LRCP Referral MO + RO
Potentially Curative Rx Palliative Rx

6
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Investigations – Required Work-up • CNCCN guidelines
- H&P - Hepatitis panel - Bilirubin - transaminases - alkaline phosphatase - LDH, PT or INR - albumin - protein - BUN - creatinine - CBC - platelets - Hepatitis B surface antigen - CT/MRI - Chest x-ray - AFP - Hepatitis C antibodies
• Biopsy if AFP < 400 ng/ml (HepB SAg-) / < 4000 ng/ml (HepB SAg+)
• American Association for the Study of Liver Diseases (AASLD)
• See next page.
• More emphasis on imaging characteristics and size (>1 cm)
• AFP cutoff for biopsy <200 ng/ml
Biopsy risks controversial • Seeding of needle tract reported in 0 – 5% of patients in series.
7
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
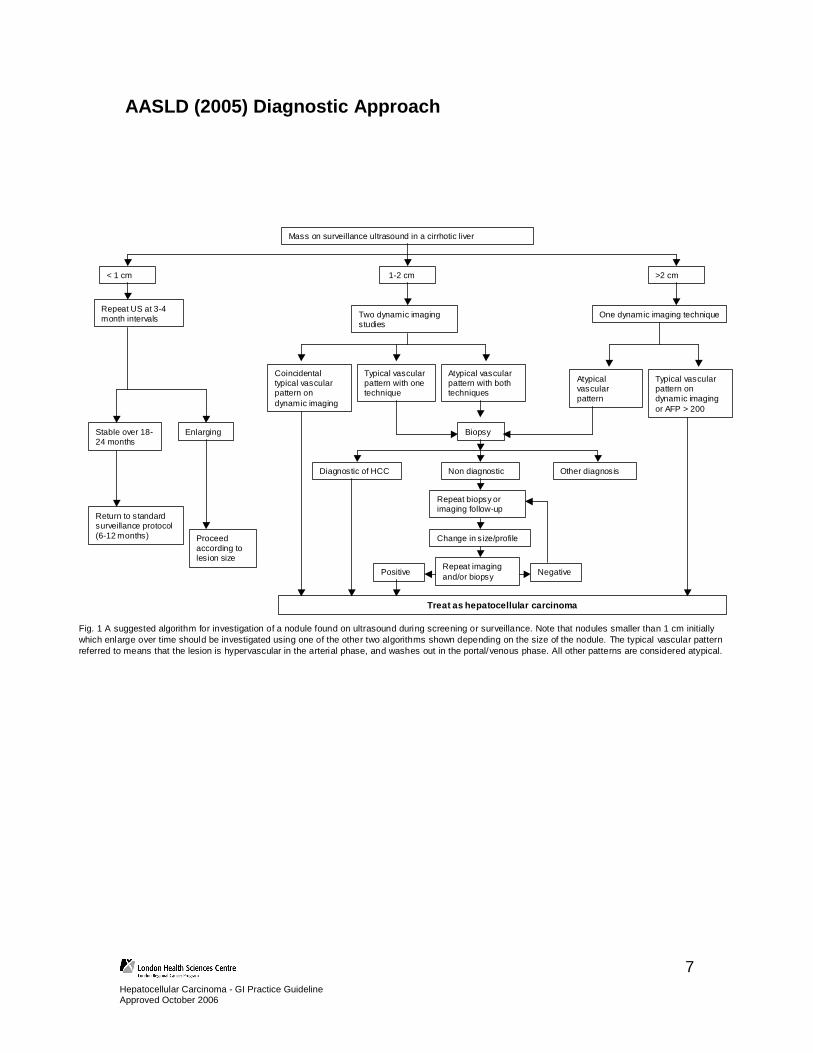
AASLD (2005) Diagnostic Approach
Mass on surveillance ultrasound in a cirrhotic liver
Two dynamic imaging studies
Repeat US at 3-4 month intervals
< 1 cm 1-2 cm >2 cm
One dynamic imaging technique
Coincidental typical vascular pattern on dynamic imaging
Typical vascular pattern with one technique
Atypical vascular pattern with both techniques
Stable over 18-24 months
Return to standard surveillance protocol (6-12 months) Proceed
according to lesion size
Atypical vascular pattern
Typical vascular pattern on dynamic imaging or AFP > 200
Biopsy
Treat as hepatocellular carcinoma
Enlarging
Diagnostic of HCC Non diagnostic Other diagnosis
Repeat imaging and/or biopsy
Change in size/profile
Repeat biopsy or imaging follow-up
Positive Negative
Fig. 1 A suggested algorithm for investigation of a nodule found on ultrasound during screening or surveillance. Note that nodules smaller than 1 cm initially which enlarge over time should be investigated using one of the other two algorithms shown depending on the size of the nodule. The typical vascular pattern referred to means that the lesion is hypervascular in the arterial phase, and washes out in the portal/venous phase. All other patterns are considered atypical.
8
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
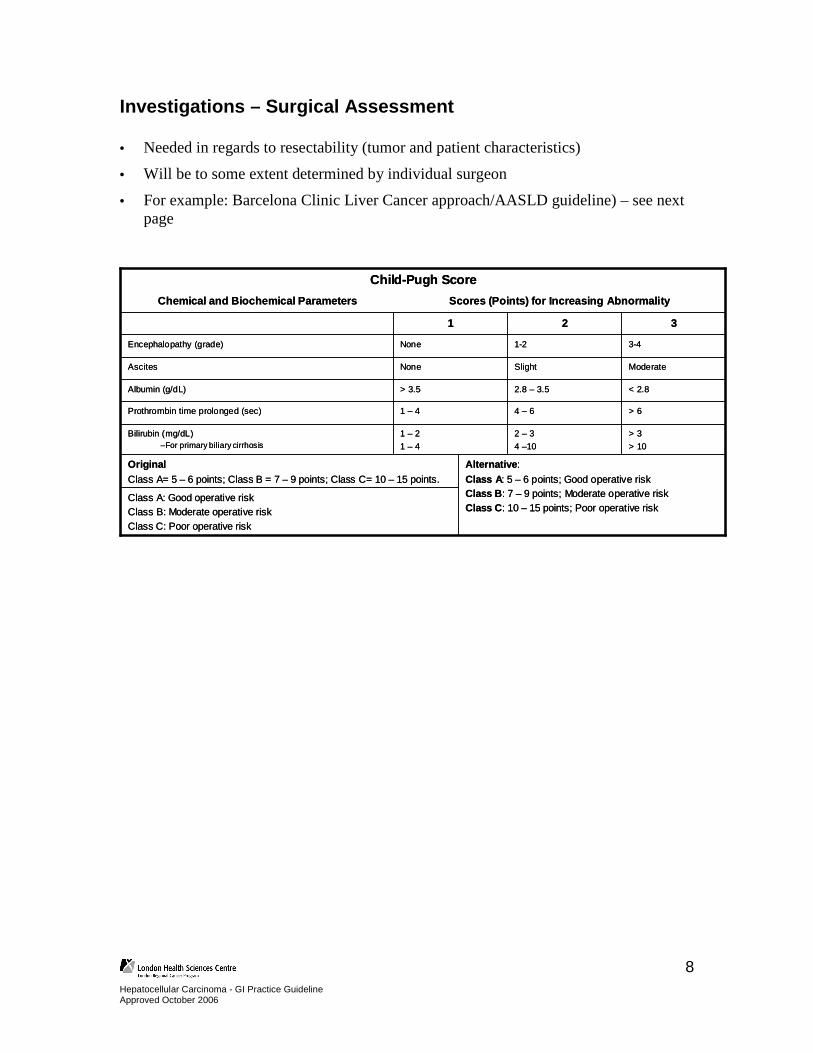
Investigations – Surgical Assessment • Needed in regards to resectability (tumor and patient characteristics) • Will be to some extent determined by individual surgeon
• For example: Barcelona Clinic Liver Cancer approach/AASLD guideline) – see next page
Alternative:
Class A : 5 – 6 points; Good operative riskClass B : 7 – 9 points; Moderate operative riskClass C : 10 – 15 points; Poor operative risk
Class A: Good operative riskClass B: Moderate operative riskClass C: Poor operative risk
OriginalClass A= 5 – 6 points; Class B = 7 – 9 points; Class C= 10 – 15 points.
> 3
> 10
2 – 3
4 –10
1 – 2
1 – 4
Bilirubin (mg/dL)–For primary biliary cirrhosis
> 64 – 61 – 4Prothrombin time prolonged (sec)
< 2.82.8 – 3.5> 3.5Albumin (g/dL)
ModerateSlightNoneAscites
3-41-2NoneEncephalopathy (grade)
321
Scores (Points) for Increasing AbnormalityChemical and Biochemical Parameters
Child-Pugh Score
Alternative:
Class A : 5 – 6 points; Good operative riskClass B : 7 – 9 points; Moderate operative riskClass C : 10 – 15 points; Poor operative risk
Class A: Good operative riskClass B: Moderate operative riskClass C: Poor operative risk
OriginalClass A= 5 – 6 points; Class B = 7 – 9 points; Class C= 10 – 15 points.
> 3
> 10
2 – 3
4 –10
1 – 2
1 – 4
Bilirubin (mg/dL)–For primary biliary cirrhosis
> 64 – 61 – 4Prothrombin time prolonged (sec)
< 2.82.8 – 3.5> 3.5Albumin (g/dL)
ModerateSlightNoneAscites
3-41-2NoneEncephalopathy (grade)
321
Scores (Points) for Increasing AbnormalityChemical and Biochemical Parameters
Child-Pugh Score

9
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Barcelona / AASLD Approach to Surgical Assessment
HCCPST 0, Child-Pugh A PST 0-2, Child-Pugh A-B PST >2, Child-Pugh C
Very early stage
Single < 2cm
Early stage
Single or 3 nodules <3cm, PS 0
Intermediate stage
Multinodular, PS 0
Advanced stage
Portal invasion, N1, M1, PS 1-2
Terminal stage
3 nodules <3cmSingle
Portal pressure/ bilirubin
Associated diseases
Normal
Increased
No Yes No Yes
Portal invasion, N1, M1
Resection Liver Transplantation (CLT / LDLT
PEI/RF
Chemoembolization New Agents
Curative Treatments Randomized controlled trials Symptomatic
Fig. 2 Strategy for staging and treatment assignment in patients diagnosed with HCC according to the BCLC proposal
10
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
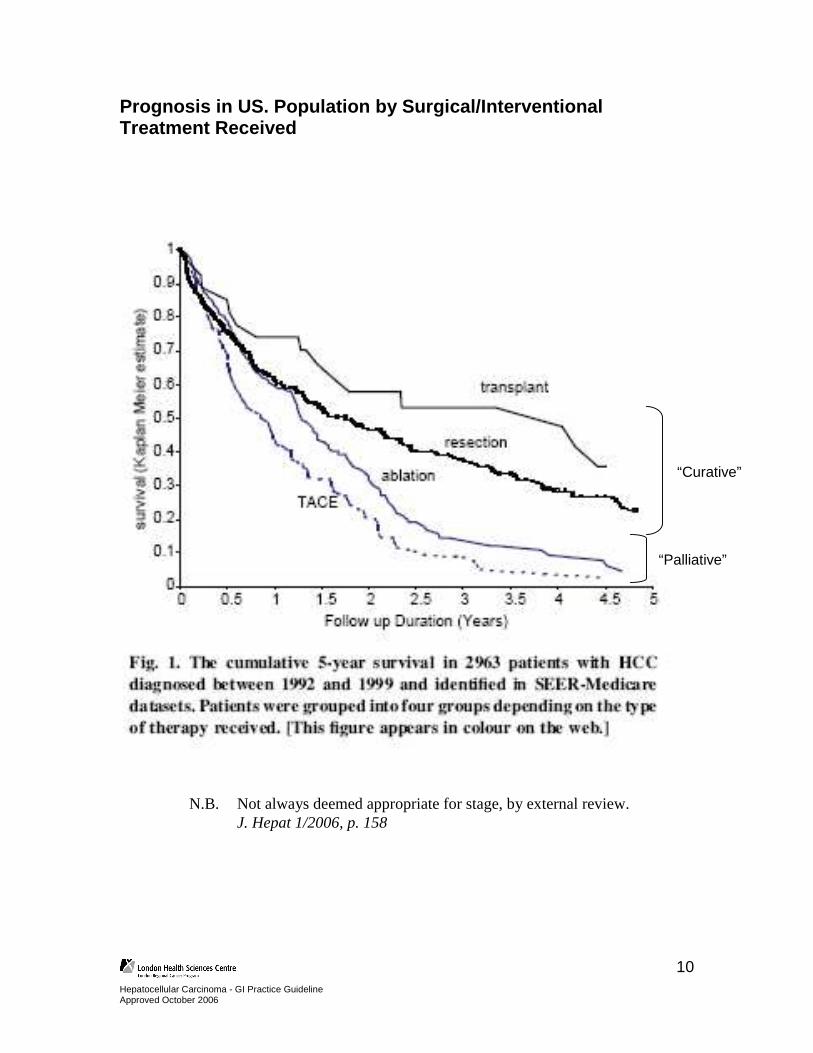
Prognosis in US. Population by Surgical/Interventio nal Treatment Received
N.B. Not always deemed appropriate for stage, by external review. J. Hepat 1/2006, p. 158
“Curative”
“Palliative”
11
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Treatment – Curative Intent • Treatment in addition to surgery – curative intent
• Neoadjuvant − 131-I – Lipiodol intra-arterial treatment
• case series 19/34 pts objective response
• Intra-arterial chemotherapy – conflicting series. Most show reduction in size but no large survival difference – One controlled trial of resectable tumours demonstrated worse survival in Rx
group, presumably because of delay to surgery (Br J Surg 1995 Jan;82(1):122-6) – Not recommended by AASLD guidelines – Should be reserved for tumours of borderline resectability only
• Adjuvant − Adjuvant therapy: most positive study is Lau et al (Lancet 1999) with I-131
Lipiodol 85 vs 46% 3YS. Current (Oct 2006) Phase III trial at NCI ongoing and open to accrual (NCT00027768)
− Bland or chemoembolization data less positive (Izumi et al., Hepatology 1994 Aug;20(2):295-301).
− Polyprenoic acid may reduce new HCC's (Muto et al, N Engl J Med 1996; 334:1561-1568).

12
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Treatment – Palliative-intent therapy (localized) • Radiofrequency ablation / Percutaneous ethanol ablation
• neither of these has directly been compared to BSC alone, however, survivals and local control rates are generally better than what would be expected; > 75-80 % at 2 years. Some consider this “curative”. Studies limited by short f/u (2-5 years)
− External beam radiation research protocol
− Transarterial embolisation with 131Iodine lipiodol
• One randomized trial with benefit in pts with portal vein thrombosis.
− 6 month survival 48% vs 0% (27 pts total), 9 month survival 7% vs 0%. (Nucl Med 1994 Nov;35(11):1782-7)
− Transarterial chemotherapy/embolisation (‘HACE’ or ‘TACE’)
• Benefit very dependent on patient selection. Recommended by AASLD
− A prognostic index of the survival of patients with unresectable hepatocellular carcinoma after transcatheter arterial chemoembolization, Cancer 2000 Jan 1;88(1):50-7
− Transarterial chemotherapy/embolisation + lipiodol (‘HALCE’)
• Two randomized trials with survival benefit e.g. Hepatology 2002 May;35(5):1164-71, HR 0.49.
− Transarterial chemotherapy/embolisation + 131I- lipiodol
• Unique to LRCP?

13
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Treatment – Palliative-intent therapy (systemic) • Tamoxifen – negative RCTs
• Octreotide – negative RCTs however follow-up too short. Ongoing HECTOR trial in Europe pending final analysis
• Chemotherapy • Doxorubicin vs. BSC 10.6 vs 7.5 weeks OS (Lai et al, Cancer 1988;62(3):479-83) • Resp rate around 20%, higher than 5FU or etoposide, but no OS difference
• Gemcitabine, Capecitabine [11% RR] also in series only
• Combination therapy: cisplatin/5FU, cisplatin/doxorubicin, gemcitabine/cisplatin etc. RR around 10-45% in series − ECF: 15% RR in 21 pts (1/21 pCR)
Boucher et al Cancer Chemother Pharmacol 2002 Oct;50(4):305-8
• Little if any QOL data
• Adding interferon – inc RR? but not survival − A randomized phase III study of doxorubicin versus cisplatin/interferon alpha-
2b/doxorubicin/fluorouracil (PIAF) combination chemotherapy for unresectable hepatocellular carcinoma. J Natl Cancer Inst 2005 Oct 19;97(20):1532-8
• Trials – preferable – over 50 active trials at clinicaltrials.gov as of Oct 2006
14
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
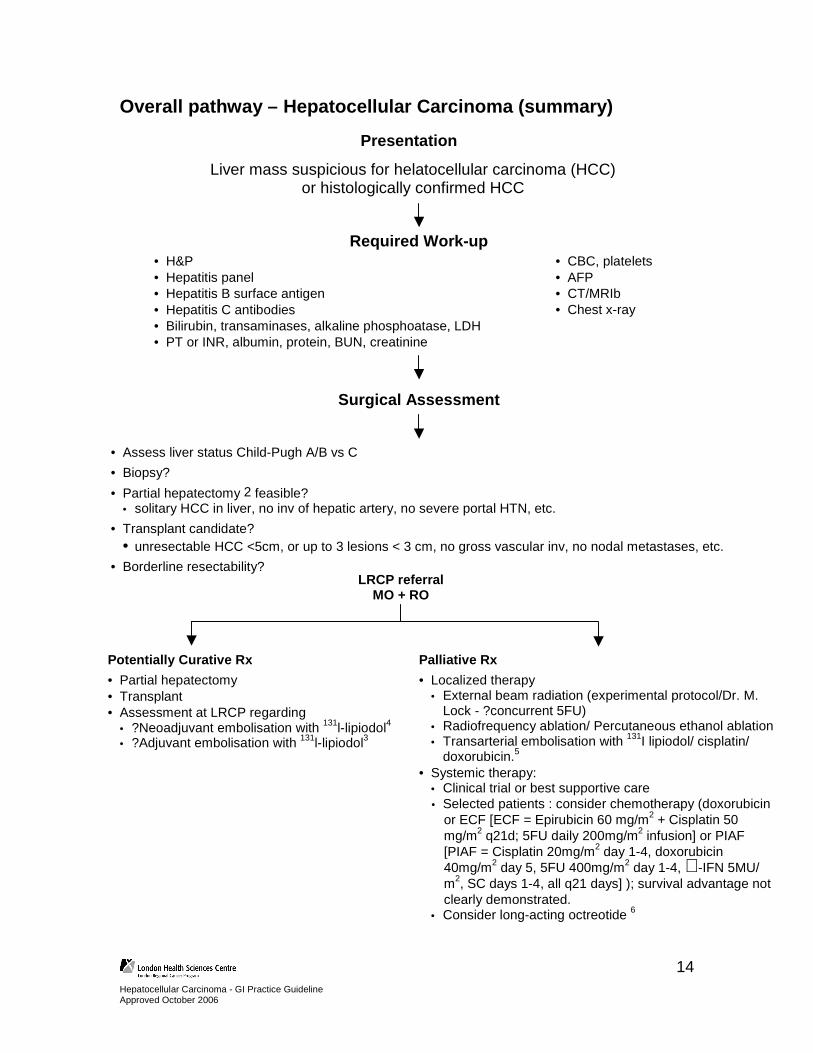
Overall pathway – Hepatocellular Carcinoma (summary )
Presentation
Liver mass suspicious for helatocellular carcinoma (HCC) or histologically confirmed HCC
• Assess liver status Child-Pugh A/B vs C
• Biopsy?
• Partial hepatectomy 2 feasible? • solitary HCC in liver, no inv of hepatic artery, no severe portal HTN, etc.
• Transplant candidate? • unresectable HCC <5cm, or up to 3 lesions < 3 cm, no gross vascular inv, no nodal metastases, etc.
• Borderline resectability?
Surgical Assessment
LRCP referral MO + RO
Required Work-up • H&P • Hepatitis panel • Hepatitis B surface antigen • Hepatitis C antibodies • Bilirubin, transaminases, alkaline phosphoatase, LDH • PT or INR, albumin, protein, BUN, creatinine
• CBC, platelets • AFP • CT/MRIb • Chest x-ray
Potentially Curative Rx
• Partial hepatectomy • Transplant • Assessment at LRCP regarding
• ?Neoadjuvant embolisation with 131l-lipiodol4 • ?Adjuvant embolisation with 131l-lipiodol3
Palliative Rx
• Localized therapy • External beam radiation (experimental protocol/Dr. M.
Lock - ?concurrent 5FU) • Radiofrequency ablation/ Percutaneous ethanol ablation • Transarterial embolisation with 131I lipiodol/ cisplatin/
doxorubicin.5 • Systemic therapy:
• Clinical trial or best supportive care • Selected patients : consider chemotherapy (doxorubicin
or ECF [ECF = Epirubicin 60 mg/m2 + Cisplatin 50 mg/m2 q21d; 5FU daily 200mg/m2 infusion] or PIAF [PIAF = Cisplatin 20mg/m2 day 1-4, doxorubicin 40mg/m2 day 5, 5FU 400mg/m2 day 1-4, ∝-IFN 5MU/ m2, SC days 1-4, all q21 days] ); survival advantage not clearly demonstrated.
• Consider long-acting octreotide 6
15
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
References Re: biopsy Percutaneous fine-needle aspiration cytology in the diagnosis and management of liver tumours. Br J Surg 2002 Jun;89(6):757-62 (3% seeding rate); Assessment of the benefits and risks of percutaneous biopsy before surgical resection of hepatocellular carcinoma. J Hepatol 2001 Aug;35(2):254-8 (1.6%); Comparison of liver biopsy and noninvasive methods for diagnosis of hepatocellular carcinoma. Clin Gastroenterol Hepatol. 2006 Mar;4(3):361-8 (0%)
1. AFP (a – fetoprotein) sensitivity 41-65%, spec 80-94%; +’ve likelihood ratio 3.1-6.8; -’ve LR 0.4-0.6 using cutoffs of 16-100 µg/L
2. Partial hepatectomy: 5YS 30-90%. Requires Child-Pugh A or B with good PS. Consider preoperative portal vein embolization to induce hypertrophy.
3. Adjuvant therapy: most positive study is Lau et al (Lancet 1999) with I-131 Lipiodol 85 vs 46% 3YS. Bland or chemoembolization data less positive (Izumi et al., Hepatology 1994 Aug;20(2):295-301). Polyprenoic acid may reduce new HCC's (Muto et al, N Engl J Med 1996; 334:1561-1568).
4. Neoadjuvant I-131 Lipiodol in development Br J Surg. 2003 Nov;90(11):1379-83. Case series, 25/34 pts objective response or histological necrosis, 19/34 obj. resp.
5. 50-60% RR. Need KPS>60-70, no severe weight loss. HALCE contraindications: PV thrombus, encephalopathy, biliary manipulation Hx/obstr; relative: bili>35, AST>100, >50% of liver replaced by tumour, CHF/CRF, ascites, variceal bleed, low plts. I-131 lipiodol/chemoembolisation at LRCP; other centres use only one modality/no radiolabelled oil – evidence controversial for that (e.g. lipiodol alone insuff.: N Engl J Med 1995;332:1256-61.)
6. Evidence controversial. Hepatology 2002(3):687 negative but OS only 2 mos each arm and 60% no Rx or only 1 dose. HECTOR study ongoing. Kuroumalis et al. 1998; Gut 62 : positive but retrospective.

16
Hepatocellular Carcinoma - GI Practice Guideline Approved October 2006
Authors, Contact Information
Michael Sanatani, MD, FRCPC (Medical Oncologist) London Regional Cancer Program London Health Sciences Centre 790 Commissioners Road East London, Ontario, Canada N6A 4L6 Telephone: 519.685.8600 Ext. 58640 Barbara Fisher, MD, FRCPC (Radiation Oncologist) London Regional Cancer Program London Health Sciences Centre 790 Commissioners Road East London, Ontario, Canada N6A 4L6 Telephone: 519.685.8600 Ext. 58650
This guideline is a statement of consensus of the GI Disease Site Team regarding their views of currently accepted approaches to treatment. It is not intended to replace the independent medical judgement of the physician in the context of individual clinical circumstances to determine any patient’s care or treatment.