Embed Size (px)
Citation preview
Hepatoprotective activity of six polyherbal formulations in paracetamol induced liver toxicity in mice
C. Girish, B.C. Koner*, S. Jayanthi**, K.R. Rao†, B. Rajesh† & S.C. Pradhan
Departments of Pharmacology, *Biochemistry, *Biochemistry, * **Pathology & **Pathology & ** †Anatomy, Jawaharlal Institute of Postgraduate †Anatomy, Jawaharlal Institute of Postgraduate †
Medical Education & Research, Puducherry, India
Received November 14, 2007
Background & objective: Polyherbal formulations available with a wide range of indications like protective to liver, appetite and growth promoters, gastrointestinal and hepatic regulator, as treatment for hepatic dysfunction, for hepatic regeneration as well as liver stimulant and tonic. Despite the widespread use, there is a lack of scientifi c evidence on their effi cacy and safety. This study was undertaken to evaluate the hepatoprotective activity of six commercially available formulations, namely Liv 52, Livergen, Livokin, Octogen, Stimuliv and Tefroliv in acute liver toxicity in mice model induced by paracetamol (PCM).
Methods: Swiss albino mice of either sex were used, divided in 28 groups with six in each group. The dose of the polyherbal formulations was calculated from human dose (20 ml/day) using a standard conversion table. They were given as pretreatment (2.60 ml/kg/day) for 7 days by oral route twice a day prior to PCM administration. Hepatotoxicity was induced by administering a single oral dose of PCM (500 mg/kg bw) on day 8. The study parameters were conducted on day 9. The biochemical parameters included liver enzyme levels alanine tranaminases (ALT), aspartate transaminases (AST) and alkaline phosphatase (ALP). The pharmacological and pathological parameters were phenobarbitone sleeping time and macroscopic and microscopic changes of liver tissues respectively.
Results: PCM toxicity signifi cantly increased ALT, AST and ALP (321.00 ± 87.93, 273.17 ± 45.68, 257.50 ± 17.64 IU/l vs normal control, 33.33 ± 0.61, 89.33 ± 9.50, 152.17 ± 11.40 IU/l respectively, P<0.05), prolonged phenobarbitone induced sleeping time (from 277.50 ± 8.04 min to 335.83 ± 7.00 min, P<0.05). P<0.05). PWhen PCM higher dose (1g/kg p.o. single dose) was used, the liver tissue, in macroscopic appearance, showed extensive necrosis associated with haemorrhages. Low dose (500 mg/kg p.o. single dose) showed punctate haemorrhagic necrosis of liver tissue. In the microscopic studies, PCM induced toxicity showed haemorrhages, fatty changes and necrosis. The pretreatment in low doses (2.6 ml/kg/day) with liquid formulations of Liv 52 and Livergen reversed the PCM induced liver toxicity. At higher doses (5.2 ml/kg/day), all the six herbal formulations conclusively showed marked benefi cial effects in the studied pharmacological, biochemical and histological parameters.
Interpretation & conclusion: The present fi ndings demonstrated the effi cacy of polyherbal liquid formulations at two dose levels in PCM induced hepatotoxicity in mice. However, it suggests that a dose adjustment may be necessary to optimize the effects in clinical settings.
Key words Hepatoprotective - hepatotoxicity - liver enzymes - paracetamol - polyherbal formulations
Indian J Med Res 129, May 2009, pp 569-578
569

There are numerous plants and traditional formulations available for the treatment of liver diseases1,2. About 600 commercial herbal formulations with claimed hepatoprotective activity are being sold all over the world. Around 170 phytoconstituents isolated from 110 plants belonging to 55 families have been reported to possess hepatoprotective activity. In India, more than 93 medicinal plants are used in different combinations in the preparations of 40 patented herbal formulations3. However, only a small proportion of hepatoprotective plants as well as formulations used in traditional medicine are pharmacologically evaluated for their safety and effi cacy4. Some herbal preparations exist as standardized extracts with major known ingredients or even pure compounds which are being evaluated2.
Various active constituents isolated from plants are andrographolide from Andrographis paniculata, picroliv from Picrorhiza kurroa, phyllanthin and hypophyllanthin from Phyllanthus niruri and methoxy benzoic acid from Capparis spinosa, which have been reported to be antihepatotoxic5-9. These active constituents with antioxidative, antifi brotic, antiviral and other properties may serve as primary compounds for further development as hepatoprotective drugs4.
In the present study, six polyherbal hepatoprotective formulations, namely Liv 52, Livergen, Livokin, Octogen, Stimuliv and Tefroliv were randomly selected from 40 such formulations. The criteria for selection were based on (i) claimed as Ayurvedic medicine, (ii)commercially available, (iii) liquid formulations for easy administration, (iv) with known hepatoprotective activity of one or more plants, and (v) suffi cient shelf life. These herbal drugs have been traditionally used for liver diseases and the polyherbal formulations, claimed to be Ayurvedic medicines are being sold as liver tonics.
In an earlier study, antihepatotoxic activity of 18 Indian herbal formulations was investigated against carbon tetrachloride induced hepatotoxicity in rats and comparison was made with silymarin treatment3. The results of this study though justifi ed the use of various polyherbal formulations for hepatoprotection had many limitations as it was not a blinded study, liquid formulations were compared with silymarin which is a solid formulation, the drugs were administered intraperitoneally, an unusual route for humans and it lacked in histopathological evidences of hepatoprotection3.
In the present study, six selected formulations were blinded and coded and their effi cacy was studied on blinded and coded and their effi cacy was studied on blinded andbiochemical, histopathological and pharmacological parameters with the objective to ascertain whether the six hepatoprotective polyherbal formulations selected were effective against paracetamol (PCM) induced hepatotoxicity in mice.
Material & Methods
Animals: Inbred Swiss albino mice weighing 20-30 g of either sex, bred in Central Animal House, Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER), Puducherry were procured and used for the study. The animals were allowed food pellets (Hindustan Lever, Mumbai) and water ad libitum. Animals were maintained in standard lab conditions (12 h: 12 h dark and light cycle & 25±2 0C temperature). The study was approved by the Institute Animal Ethics Committee, JIPMER, Puducherry.
Six polyherbal hepatoprotective liquid formulations (Table I) were randomly selected from nearly 40 herbal preparations available in the Indian market for treating liver diseases. These formulations were blinded and coded and their effectiveness was tested against the PCM-induced hepatotoxicity in mice on biochemical, histopathological and pharmacological parameters. The formulations were decoded after the results were obtained.
The doses of polyherbal drugs were calculated to precisely match with the human doses employed according to the manufacturer’s instructions. The average recommended human dose of 20 ml/day was converted to that of mice by a standard conversion table10. The earlier work3 suggested a partial protection by using 15 ml three times a day as human dose. Similarly, we have used a common minimum of 20 ml/day as the human dose. The formulations were 10 times diluted and were given twice daily for 7 days by oral route as pretreatment (2.60 ml/kg bw/day) followed by a single oral dose of PCM on the eighth day. The effects were compared among the six polyherbal formulations. A double dose pretreatment (po 5.20 ml/kg bw/day) was also studied with the formulations after fi ve times diluting with distilled water. This was done to observe if there was hepatoprotection at two-dose levels by reversing the PCM induced hepatotoxicity. The present 40 ml/day human dose fairly matched with the earlier study of 45 ml/day as human dose3.
Treatment groups: Animals were divided into 28 groups (n=6/group), with 14 groups for biochemical
570 INDIAN J MED RES, MAY 2009
and histopathological parameters and another 14 for pharmacological parameter, i.e.; phenobarbitone induced sleeping time.
Group 1- Normal control: The animals received distilled water for 7 days.
Group 2- Induction of hepatotoxicity by using PCM:The animals received distilled water for 7 days and given PCM (Themis Pharma, Mumbai) single dose, 500 mg/kg bw orally on day 8.
Groups 3 to 8- Pretreatment with polyherbal formulations at 2.60 ml/kg bw/day for 7 days (p.o) followed by a single dose of PCM on day 8.
Groups 9 to 14 - Pretreatment with polyherbal formulations at 5.20 ml/kg bw/day for 7 days (p.o) followed by a single dose of PCM on day 8.
Group 15 - Normal phenobarbitone hypnosis time:Animals received distilled water for 8 days followed
by a single dose of phenobarbitone, 40 mg/kg, ip (SPM Drugs, Chennai).
Group 16- Phenobarbitone hypnosis time after PCM toxicity: The animals received distilled water for 7 days and given PCM single dose, 500 mg/kg bw orally on day 8 followed by a single dose of phenobarbitone on day 9.
Groups 17 to 22- Pretreatment with 2.60 ml/kg bw/day of polyherbal formulations for 7 days followed by PCM on day 8 and phenobarbitone on day 9.
Groups 23 to 28- Pretreatment with 5.20 ml/kg bw/day of polyherbal formulations for 7 days followed by PCM on day 8 and phenobarbitone on day 9.
Biochemical and histopathological parameters: After 24 h of PCM administration, animals were anaesthetized using ether (TKM Pharma, Hyderabad) and 1 ml of blood was collected by cardiac puncture.
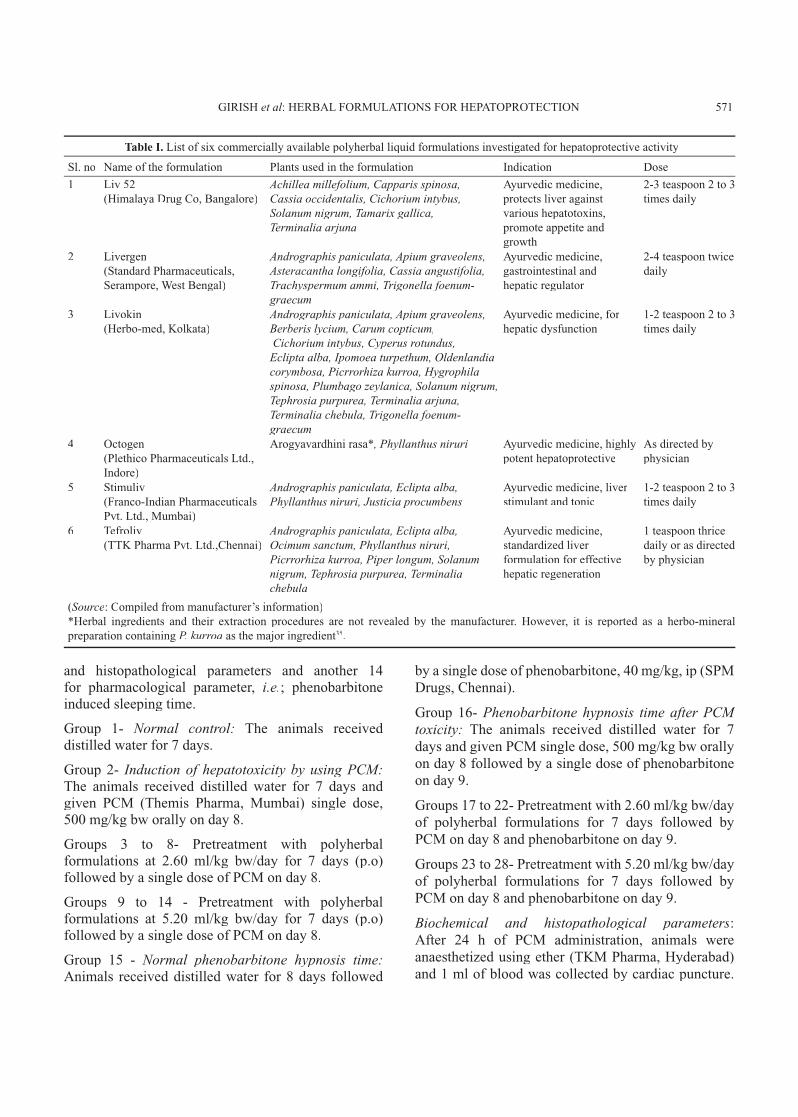
Table I. List of six commercially available polyherbal liquid formulations investigated for hepatoprotective activity
Sl. no Name of the formulation Plants used in the formulation Indication Dose
1 Liv 52(Himalaya Drug Co, Bangalore)
Achillea millefolium, Capparis spinosa, Cassia occidentalis, Cichorium intybus, Solanum nigrum, Tamarix gallica, Terminalia arjuna
Ayurvedic medicine,protects liver against various hepatotoxins, promote appetite and growth
2-3 teaspoon 2 to 3 times daily
2 Livergen(Standard Pharmaceuticals, Serampore, West Bengal)
Andrographis paniculata, Apium graveolens, Asteracantha longifolia, Cassia angustifolia, Trachyspermum ammi, Trigonella foenum- graecum
Ayurvedic medicine, gastrointestinal and hepatic regulator
2-4 teaspoon twice daily
3 Livokin(Herbo-med, Kolkata)
Andrographis paniculata, Apium graveolens, Berberis lycium, Carum copticum, Cichorium intybus, Cyperus rotundus, Eclipta alba, Ipomoea turpethum, Oldenlandia corymbosa, Picrrorhiza kurroa, Hygrophila spinosa, Plumbago zeylanica, Solanum nigrum, Tephrosia purpurea, Terminalia arjuna, Terminalia chebula, Trigonella foenum- graecum
Ayurvedic medicine, for hepatic dysfunction
1-2 teaspoon 2 to 3 times daily
4 Octogen(Plethico Pharmaceuticals Ltd., Indore)
Arogyavardhini rasa*, Phyllanthus niruri Ayurvedic medicine, highly potent hepatoprotective
As directed by physician
5 Stimuliv(Franco-Indian Pharmaceuticals Pvt. Ltd., Mumbai)
Andrographis paniculata, Eclipta alba, Phyllanthus niruri, Justicia procumbens
Ayurvedic medicine, liver stimulant and tonic
1-2 teaspoon 2 to 3 times daily
6 Tefroliv(TTK Pharma Pvt. Ltd.,Chennai)
Andrographis paniculata, Eclipta alba, Ocimum sanctum, Phyllanthus niruri, Picrrorhiza kurroa, Piper longum, Solanum nigrum, Tephrosia purpurea, Terminalia chebula
Ayurvedic medicine, standardized liver formulation for effective hepatic regeneration
1 teaspoon thrice daily or as directed by physician
(Source: Compiled from manufacturer’s information)*Herbal ingredients and their extraction procedures are not revealed by the manufacturer. However, it is reported as a herbo-mineral preparation containing P. kurroa as the major ingredient35.
GIRISH et al: HERBAL FORMULATIONS FOR HEPATOPROTECTION 571
The blood was allowed to clot and centrifuged (Remi, Mumbai) at 350 g for 10 min. The serum was separated and used for assay of alanine transaminases (ALT), aspartate transaminases (AST) and alkaline phosphatase (ALP) by standard methods using enzyme assay kits (Span Diagnostics Ltd, India) adopted to Microlab 200 semiauto analyzer (E. Merck, Germany). The animals were sacrifi ced by cervical dislocation and livers were excised, washed with phosphate buffer and dried with tissue paper. The liver was weighed by using electronic balance (Sartorius, Germany) and transferred to a 10 per cent formalin fi xative solution for 48 h. The liver tissues were processed for paraffi n embedding and sections of 5 micron thickness were taken in a microtome. After staining with haematoxylin and eosin (H&E), slides were examined under microscope (Olympus, Japan) for histopathological changes.
Phenobarbitone induced sleeping time: After phenobarbitone administration, sleeping time was recorded in minutes from onset of sleep to its natural arousal. The method was modifi ed from earlier report by using phenobarbitone instead of pentobarbitone6. The control sleeping time was compared with those of PCM toxicity group and polyherbal formulation pretreatment groups.
This test is based on the fact that PCM induced hepatotoxicity causes enhancement of sleeping time due to hepatic injury as barbiturate metabolism is delayed and excretion is slowed. However, hepatoprotective drugs restore the phenobarbitone induced sleeping time by reducing it even after PCM administration. Activation of hepatocellular function restores the drug metabolic activity and reduces phenobarbitone induced sleeping time.
Statistical analysis: The data were analyzed by One way ANOVA followed by Student-Newman-Keuls test using Graphpad Instat version 3.06 (GraphPad Software, Inc. CA, USA). The comparison between groups was done by calculating the percentage reduction in each parameter compared to Liv 52, considering the difference between PCM and Liv 52 treatment groups as 100 per cent. P<0.05 was considered as statistically signifi cant.
Results
PCM (500 mg/kg bw) given once orally showed hepatotoxicity after 24 h as evident from biochemical, pharmacological and histopathological parameters of the study.
PCM treatment signifi cantly increased the serum liver enzyme levels, viz., ALT, AST and ALP. The
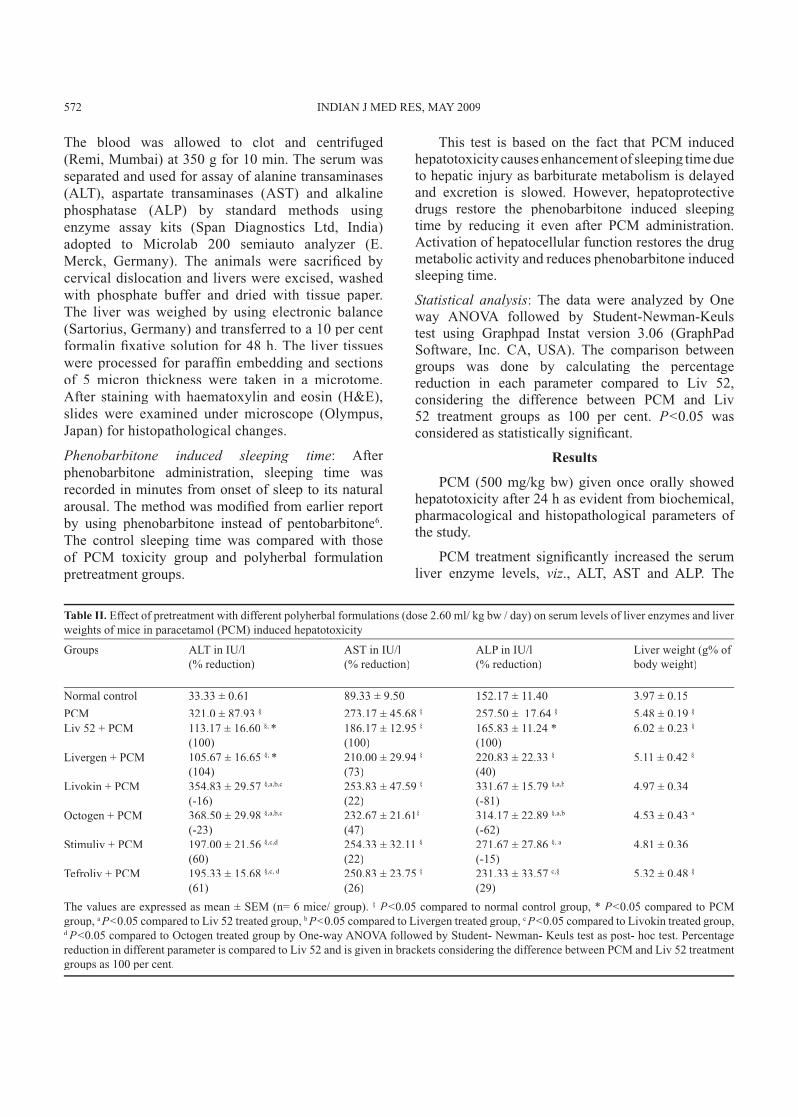
Table II. Effect of pretreatment with different polyherbal formulations (dose 2.60 ml/ kg bw / day) on serum levels of liver enzymes and liver weights of mice in paracetamol (PCM) induced hepatotoxicity
Groups ALT in IU/l(% reduction)
AST in IU/l(% reduction)
ALP in IU/l(% reduction)
Liver weight (g% of body weight)
Normal control 33.33 ± 0.61 89.33 ± 9.50 152.17 ± 11.40 3.97 ± 0.15
PCM 321.0 ± 87.93 § 273.17 ± 45.68 § 257.50 ± 17.64 § 5.48 ± 0.19 §
Liv 52 + PCM 113.17 ± 16.60 §, * (100)
186.17 ± 12.95 §
(100)165.83 ± 11.24 * (100)
6.02 ± 0.23 §
Livergen + PCM 105.67 ± 16.65 §, * (104)
210.00 ± 29.94 §
(73)220.83 ± 22.33 §
(40)5.11 ± 0.42 §
Livokin + PCM 354.83 ± 29.57 §,a,b,c
(-16)253.83 ± 47.59 §
(22)331.67 ± 15.79 §,a,b
(-81)4.97 ± 0.34
Octogen + PCM 368.50 ± 29.98 §,a,b,c
(-23)232.67 ± 21.61§
(47)314.17 ± 22.89 §,a,b
(-62)4.53 ± 0.43 a
Stimuliv + PCM 197.00 ± 21.56 §,c,d
(60)254.33 ± 32.11 §
(22)271.67 ± 27.86 §, a
(-15)4.81 ± 0.36
Tefroliv + PCM 195.33 ± 15.68 §,c, d
(61)250.83 ± 23.75 §
(26)231.33 ± 33.57 c,§
(29)5.32 ± 0.48 §
The values are expressed as mean ± SEM (n= 6 mice/ group). § P<0.05 compared to normal control group, * P<0.05 compared to PCM group, a P<0.05 compared to Liv 52 treated group, b P<0.05 compared to Livergen treated group, c P<0.05 compared to Livokin treated group, d P<0.05 compared to Octogen treated group by One-way ANOVA followed by Student- Newman- Keuls test as post- hoc test. Percentage reduction in different parameter is compared to Liv 52 and is given in brackets considering the difference between PCM and Liv 52 treatment groups as 100 per cent.
572 INDIAN J MED RES, MAY 2009
activity of ALT (321.00 ± 87.93 IU/l), AST (273.17 ± 45.68 IU/l) and ALP (257.50 ± 17.64 IU/l) was signifi cantly higher (Psignifi cantly higher (Psignifi cantly higher ( <0.05) in PCM treated group in comparison to normal control (ALT 33.33 ± 0.61; AST 89.33 ± 9.50; ALP 152.17 ± 11.40 IU/l) indicating a marked hepatocellular injury (Table II).
Six polyherbal formulations namely Liv 52, Livergen, Livokin, Octogen, Stimuliv and Tefroliv were given for 7 days prior to PCM. The pretreatment with Liv 52 in lower doses signifi cantly (Pwith Liv 52 in lower doses signifi cantly (Pwith Liv 52 in lower doses signifi cantly ( <0.05) reduced ALT and ALP values. As compared to Liv 52 (100%), there was a 104 per cent reduction in serum levels of ALT in Livergen pretreated group.
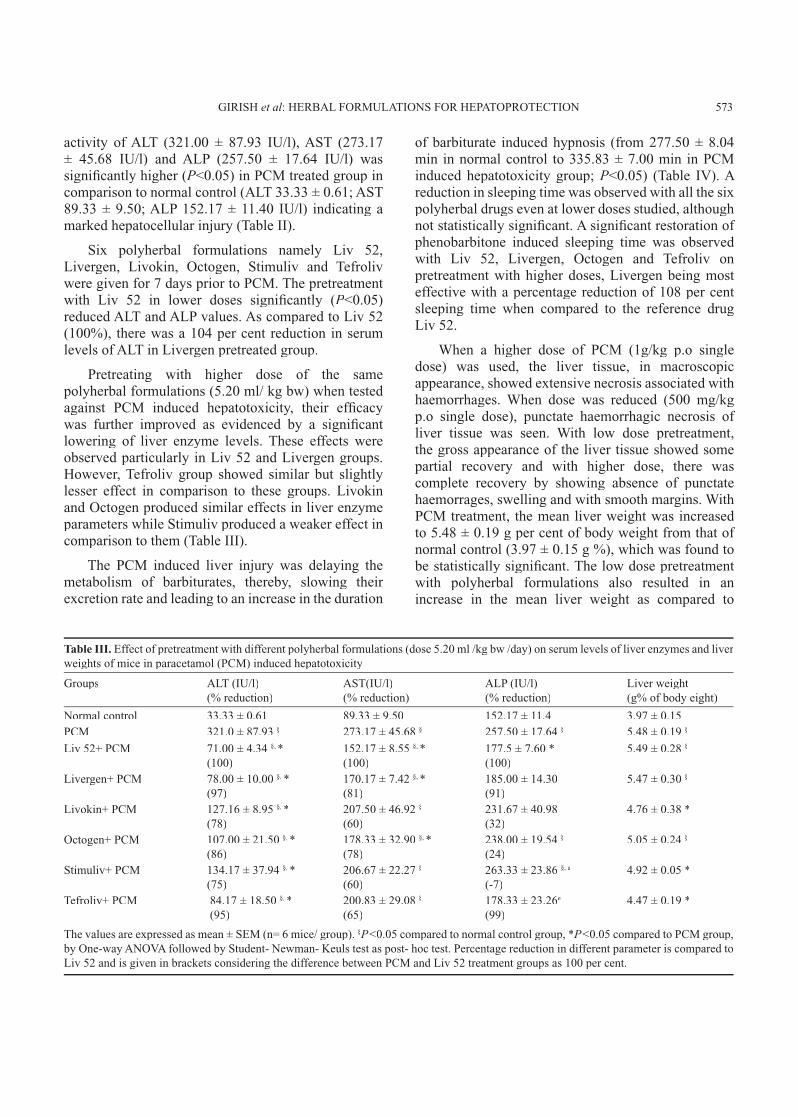
Pretreating with higher dose of the same polyherbal formulations (5.20 ml/ kg bw) when tested against PCM induced hepatotoxicity, their effi cacy was further improved as evidenced by a signifi cant lowering of liver enzyme levels. These effects were observed particularly in Liv 52 and Livergen groups. However, Tefroliv group showed similar but slightly lesser effect in comparison to these groups. Livokin and Octogen produced similar effects in liver enzyme parameters while Stimuliv produced a weaker effect in comparison to them (Table III).
The PCM induced liver injury was delaying the metabolism of barbiturates, thereby, slowing their excretion rate and leading to an increase in the duration
of barbiturate induced hypnosis (from 277.50 ± 8.04 min in normal control to 335.83 ± 7.00 min in PCM induced hepatotoxicity group; P<0.05) (Table IV). A reduction in sleeping time was observed with all the six polyherbal drugs even at lower doses studied, although not statistically signifi cant. A signifi cant restoration of phenobarbitone induced sleeping time was observed with Liv 52, Livergen, Octogen and Tefroliv on pretreatment with higher doses, Livergen being most effective with a percentage reduction of 108 per cent sleeping time when compared to the reference drug Liv 52.
When a higher dose of PCM (1g/kg p.o single dose) was used, the liver tissue, in macroscopic appearance, showed extensive necrosis associated with haemorrhages. When dose was reduced (500 mg/kg p.o single dose), punctate haemorrhagic necrosis of liver tissue was seen. With low dose pretreatment, the gross appearance of the liver tissue showed some partial recovery and with higher dose, there was complete recovery by showing absence of punctate haemorrages, swelling and with smooth margins. With PCM treatment, the mean liver weight was increased to 5.48 ± 0.19 g per cent of body weight from that of normal control (3.97 ± 0.15 g %), which was found to be statistically signifi cant. The low dose pretreatment with polyherbal formulations also resulted in an increase in the mean liver weight as compared to
Table III. Effect of pretreatment with different polyherbal formulations (dose 5.20 ml /kg bw /day) on serum levels of liver enzymes and liver weights of mice in paracetamol (PCM) induced hepatotoxicity
Groups ALT (IU/l)(% reduction)
AST(IU/l)(% reduction)
ALP (IU/l)(% reduction)
Liver weight (g% of body eight)
Normal control 33.33 ± 0.61 89.33 ± 9.50 152.17 ± 11.4 3.97 ± 0.15PCM 321.0 ± 87.93 § 273.17 ± 45.68 § 257.50 ± 17.64 § 5.48 ± 0.19 §
Liv 52+ PCM 71.00 ± 4.34 §, * (100)
152.17 ± 8.55 §, * (100)
177.5 ± 7.60 *(100)
5.49 ± 0.28 §
Livergen+ PCM 78.00 ± 10.00 §, * (97)
170.17 ± 7.42 §, * (81)
185.00 ± 14.30 (91)
5.47 ± 0.30 §
Livokin+ PCM 127.16 ± 8.95 §, *
(78)207.50 ± 46.92 §
(60)231.67 ± 40.98 (32)
4.76 ± 0.38 *
Octogen+ PCM 107.00 ± 21.50 §, * (86)
178.33 ± 32.90 §, * (78)
238.00 ± 19.54 §
(24)5.05 ± 0.24 §
Stimuliv+ PCM 134.17 ± 37.94 §, * (75)
206.67 ± 22.27 §
(60)263.33 ± 23.86 §, a
(-7)4.92 ± 0.05 *
Tefroliv+ PCM 84.17 ± 18.50 §, * (95)
200.83 ± 29.08 §
(65)178.33 ± 23.26e
(99)4.47 ± 0.19 *
The values are expressed as mean ± SEM (n= 6 mice/ group). §P<0.05 compared to normal control group, *P<0.05 compared to PCM group, by One-way ANOVA followed by Student- Newman- Keuls test as post- hoc test. Percentage reduction in different parameter is compared to Liv 52 and is given in brackets considering the difference between PCM and Liv 52 treatment groups as 100 per cent.
GIRISH et al: HERBAL FORMULATIONS FOR HEPATOPROTECTION 573
normal, which was statistically signifi cant in Liv 52, Livergen and Tefroliv groups. However, pretreatment with high dose resulted in similar outcomes excluding Tefroliv group, but Octogen group also showed an increase in liver weight gain.
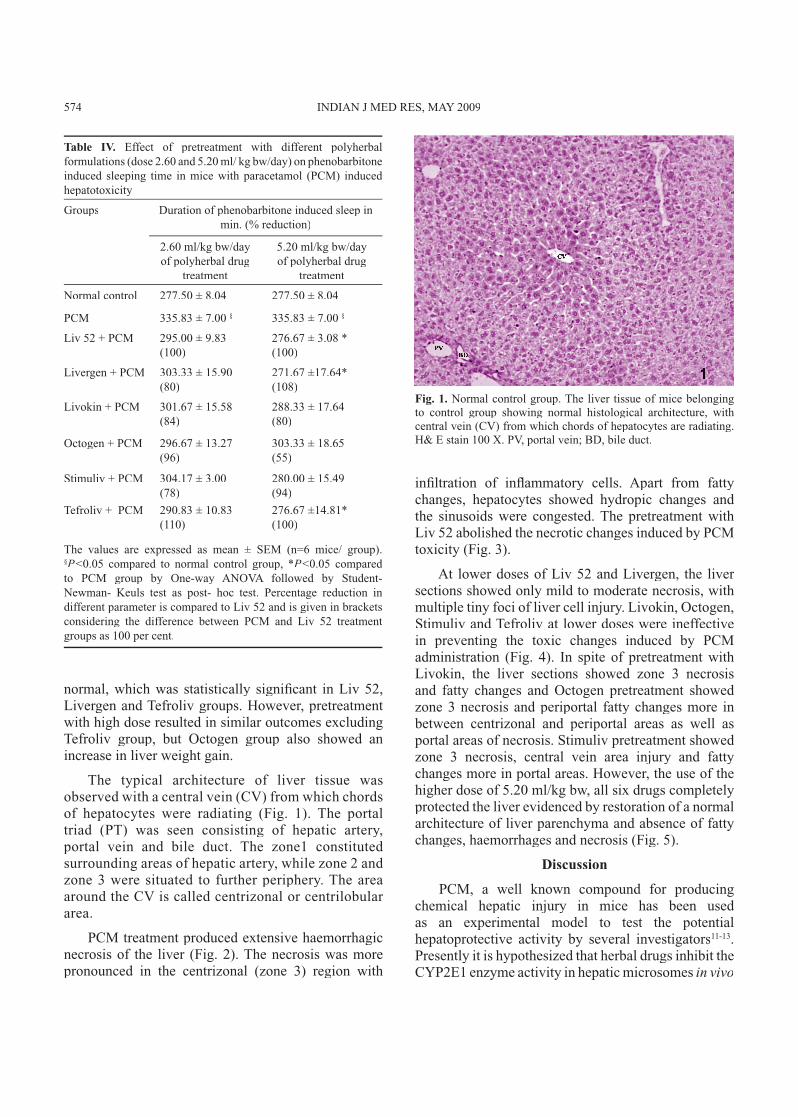
The typical architecture of liver tissue was observed with a central vein (CV) from which chords of hepatocytes were radiating (Fig. 1). The portal triad (PT) was seen consisting of hepatic artery, portal vein and bile duct. The zone1 constituted surrounding areas of hepatic artery, while zone 2 and zone 3 were situated to further periphery. The area around the CV is called centrizonal or centrilobular area.
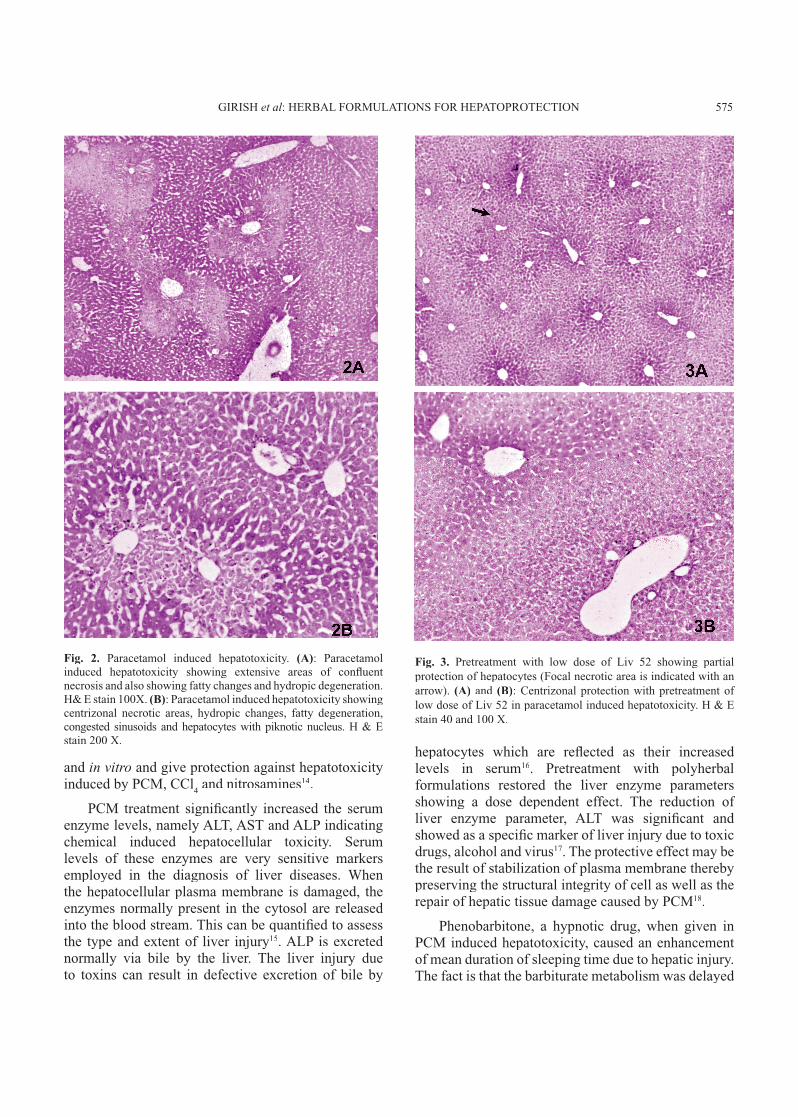
PCM treatment produced extensive haemorrhagic necrosis of the liver (Fig. 2). The necrosis was more pronounced in the centrizonal (zone 3) region with
infi ltration of infl ammatory cells. Apart from fatty changes, hepatocytes showed hydropic changes and the sinusoids were congested. The pretreatment with Liv 52 abolished the necrotic changes induced by PCM toxicity (Fig. 3).
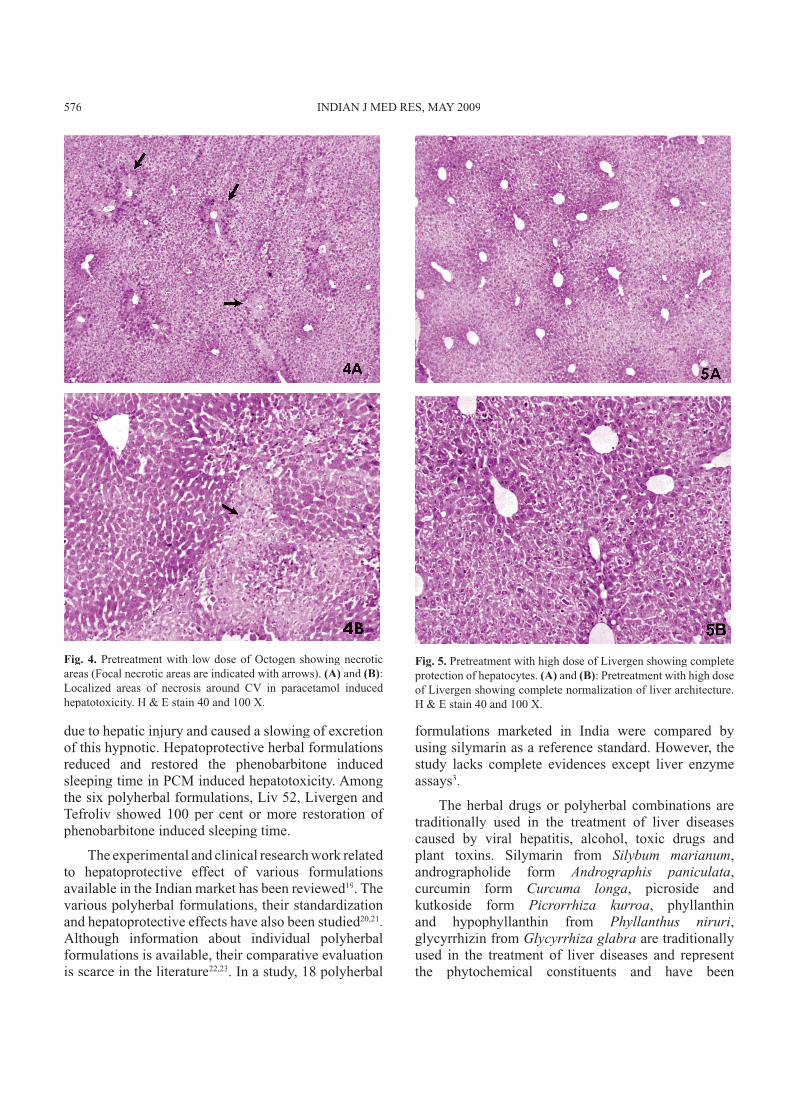
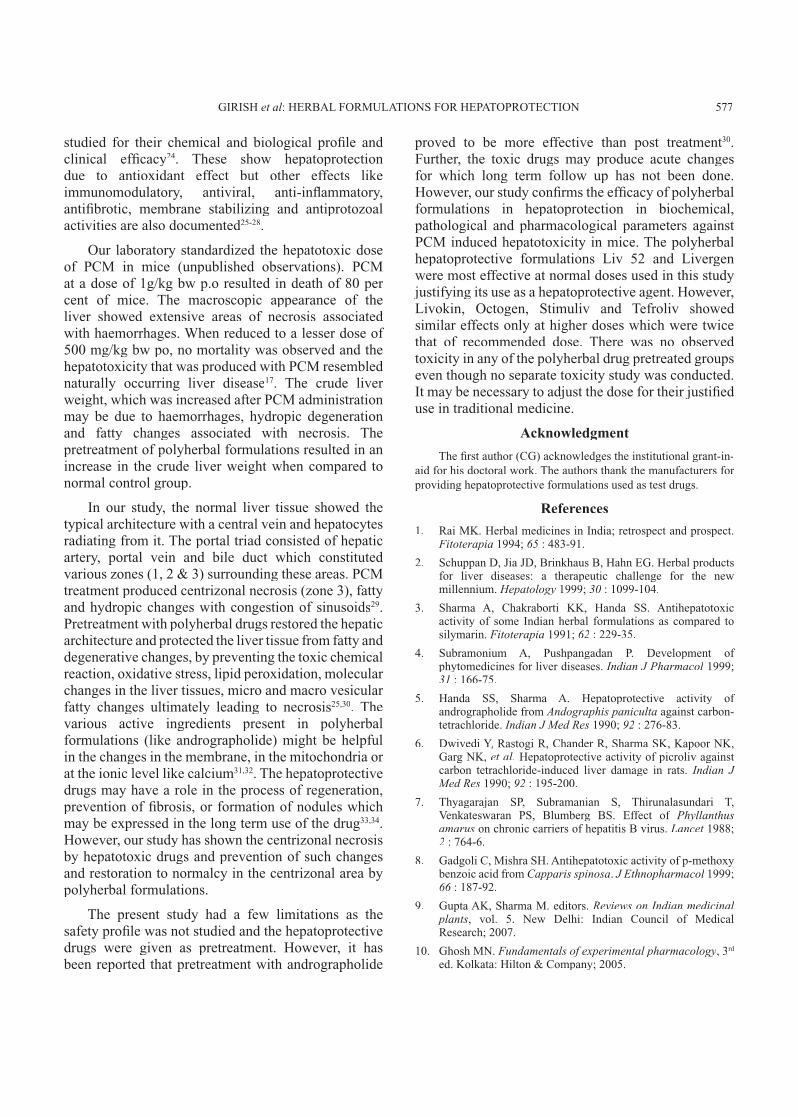
At lower doses of Liv 52 and Livergen, the liver sections showed only mild to moderate necrosis, with multiple tiny foci of liver cell injury. Livokin, Octogen, Stimuliv and Tefroliv at lower doses were ineffective in preventing the toxic changes induced by PCM administration (Fig. 4). In spite of pretreatment with Livokin, the liver sections showed zone 3 necrosis and fatty changes and Octogen pretreatment showed zone 3 necrosis and periportal fatty changes more in between centrizonal and periportal areas as well as portal areas of necrosis. Stimuliv pretreatment showed zone 3 necrosis, central vein area injury and fatty changes more in portal areas. However, the use of the higher dose of 5.20 ml/kg bw, all six drugs completely protected the liver evidenced by restoration of a normal architecture of liver parenchyma and absence of fatty changes, haemorrhages and necrosis (Fig. 5).
Discussion
PCM, a well known compound for producing chemical hepatic injury in mice has been used as an experimental model to test the potential hepatoprotective activity by several investigators11-13. Presently it is hypothesized that herbal drugs inhibit the CYP2E1 enzyme activity in hepatic microsomes in vivo
Table IV. Effect of pretreatment with different polyherbal formulations (dose 2.60 and 5.20 ml/ kg bw/day) on phenobarbitone induced sleeping time in mice with paracetamol (PCM) induced hepatotoxicity
Groups Duration of phenobarbitone induced sleep in min. (% reduction)
2.60 ml/kg bw/day of polyherbal drug
treatment
5.20 ml/kg bw/day of polyherbal drug
treatment
Normal control 277.50 ± 8.04 277.50 ± 8.04
PCM 335.83 ± 7.00 § 335.83 ± 7.00 §
Liv 52 + PCM 295.00 ± 9.83 (100)
276.67 ± 3.08 * (100)
Livergen + PCM 303.33 ± 15.90 (80)
271.67 ±17.64* (108)
Livokin + PCM 301.67 ± 15.58 (84)
288.33 ± 17.64 (80)
Octogen + PCM 296.67 ± 13.27 (96)
303.33 ± 18.65 (55)
Stimuliv + PCM 304.17 ± 3.00 (78)
280.00 ± 15.49 (94)
Tefroliv + PCM 290.83 ± 10.83 (110)
276.67 ±14.81* (100)
The values are expressed as mean ± SEM (n=6 mice/ group). §P<0.05 compared to normal control group, *P<0.05 compared to PCM group by One-way ANOVA followed by Student- Newman- Keuls test as post- hoc test. Percentage reduction in different parameter is compared to Liv 52 and is given in brackets considering the difference between PCM and Liv 52 treatment groups as 100 per cent.
Fig. 1. Normal control group. The liver tissue of mice belonging to control group showing normal histological architecture, with central vein (CV) from which chords of hepatocytes are radiating. H& E stain 100 X. PV, portal vein; BD, bile duct.
574 INDIAN J MED RES, MAY 2009
hepatocytes which are refl ected as their increased levels in serum16. Pretreatment with polyherbal formulations restored the liver enzyme parameters showing a dose dependent effect. The reduction of liver enzyme parameter, ALT was signifi cant and showed as a specifi c marker of liver injury due to toxic drugs, alcohol and virus17. The protective effect may be the result of stabilization of plasma membrane thereby preserving the structural integrity of cell as well as the repair of hepatic tissue damage caused by PCM18.
Phenobarbitone, a hypnotic drug, when given in PCM induced hepatotoxicity, caused an enhancement of mean duration of sleeping time due to hepatic injury. The fact is that the barbiturate metabolism was delayed
Fig. 2. Paracetamol induced hepatotoxicity. (A): Paracetamol induced hepatotoxicity showing extensive areas of confl uent necrosis and also showing fatty changes and hydropic degeneration. H& E stain 100X. (B): Paracetamol induced hepatotoxicity showing centrizonal necrotic areas, hydropic changes, fatty degeneration, congested sinusoids and hepatocytes with piknotic nucleus. H & E stain 200 X.
and in vitro and give protection against hepatotoxicity induced by PCM, CCl
4 and nitrosamines14.
PCM treatment signifi cantly increased the serum enzyme levels, namely ALT, AST and ALP indicating chemical induced hepatocellular toxicity. Serum levels of these enzymes are very sensitive markers employed in the diagnosis of liver diseases. When the hepatocellular plasma membrane is damaged, the enzymes normally present in the cytosol are released into the blood stream. This can be quantifi ed to assess the type and extent of liver injury15. ALP is excreted normally via bile by the liver. The liver injury due to toxins can result in defective excretion of bile by
Fig. 3. Pretreatment with low dose of Liv 52 showing partial protection of hepatocytes (Focal necrotic area is indicated with an arrow). (A) and (B): Centrizonal protection with pretreatment of low dose of Liv 52 in paracetamol induced hepatotoxicity. H & E stain 40 and 100 X.
GIRISH et al: HERBAL FORMULATIONS FOR HEPATOPROTECTION 575
due to hepatic injury and caused a slowing of excretion of this hypnotic. Hepatoprotective herbal formulations reduced and restored the phenobarbitone induced sleeping time in PCM induced hepatotoxicity. Among the six polyherbal formulations, Liv 52, Livergen and Tefroliv showed 100 per cent or more restoration of phenobarbitone induced sleeping time.
The experimental and clinical research work related to hepatoprotective effect of various formulations available in the Indian market has been reviewed19. The various polyherbal formulations, their standardization and hepatoprotective effects have also been studied20,21. Although information about individual polyherbal formulations is available, their comparative evaluation is scarce in the literature22,23. In a study, 18 polyherbal
formulations marketed in India were compared by using silymarin as a reference standard. However, the study lacks complete evidences except liver enzyme assays3.
The herbal drugs or polyherbal combinations are traditionally used in the treatment of liver diseases caused by viral hepatitis, alcohol, toxic drugs and plant toxins. Silymarin from Silybum marianum, andrographolide form Andrographis paniculata, curcumin form Curcuma longa, picroside and kutkoside form Picrorrhiza kurroa, phyllanthin and hypophyllanthin from Phyllanthus niruri, glycyrrhizin from Glycyrrhiza glabra are traditionally used in the treatment of liver diseases and represent the phytochemical constituents and have been
Fig. 4. Pretreatment with low dose of Octogen showing necrotic areas (Focal necrotic areas are indicated with arrows). (A) and (B): Localized areas of necrosis around CV in paracetamol induced hepatotoxicity. H & E stain 40 and 100 X.
Fig. 5. Pretreatment with high dose of Livergen showing complete protection of hepatocytes. (A) and (and (and B): Pretreatment with high dose of Livergen showing complete normalization of liver architecture. H & E stain 40 and 100 X.
576 INDIAN J MED RES, MAY 2009
studied for their chemical and biological profi le and clinical effi cacy24. These show hepatoprotection due to antioxidant effect but other effects like immunomodulatory, antiviral, anti-infl ammatory, antifi brotic, membrane stabilizing and antiprotozoal activities are also documented25-28.
Our laboratory standardized the hepatotoxic dose of PCM in mice (unpublished observations). PCM at a dose of 1g/kg bw p.o resulted in death of 80 per cent of mice. The macroscopic appearance of the liver showed extensive areas of necrosis associated with haemorrhages. When reduced to a lesser dose of 500 mg/kg bw po, no mortality was observed and the hepatotoxicity that was produced with PCM resembled naturally occurring liver disease17. The crude liver weight, which was increased after PCM administration may be due to haemorrhages, hydropic degeneration and fatty changes associated with necrosis. The pretreatment of polyherbal formulations resulted in an increase in the crude liver weight when compared to normal control group.
In our study, the normal liver tissue showed the typical architecture with a central vein and hepatocytes radiating from it. The portal triad consisted of hepatic artery, portal vein and bile duct which constituted various zones (1, 2 & 3) surrounding these areas. PCM treatment produced centrizonal necrosis (zone 3), fatty and hydropic changes with congestion of sinusoids29. Pretreatment with polyherbal drugs restored the hepatic architecture and protected the liver tissue from fatty and degenerative changes, by preventing the toxic chemical reaction, oxidative stress, lipid peroxidation, molecular changes in the liver tissues, micro and macro vesicular fatty changes ultimately leading to necrosis25,30. The various active ingredients present in polyherbal formulations (like andrographolide) might be helpful in the changes in the membrane, in the mitochondria or at the ionic level like calcium31,32. The hepatoprotective drugs may have a role in the process of regeneration, prevention of fi brosis, or formation of nodules which may be expressed in the long term use of the drug33,34. However, our study has shown the centrizonal necrosis by hepatotoxic drugs and prevention of such changes and restoration to normalcy in the centrizonal area by polyherbal formulations.
The present study had a few limitations as the safety profi le was not studied and the hepatoprotective drugs were given as pretreatment. However, it has been reported that pretreatment with andrographolide
proved to be more effective than post treatment30. Further, the toxic drugs may produce acute changes for which long term follow up has not been done. However, our study confi rms the effi cacy of polyherbal formulations in hepatoprotection in biochemical, pathological and pharmacological parameters against PCM induced hepatotoxicity in mice. The polyherbal hepatoprotective formulations Liv 52 and Livergen were most effective at normal doses used in this study justifying its use as a hepatoprotective agent. However, Livokin, Octogen, Stimuliv and Tefroliv showed similar effects only at higher doses which were twice that of recommended dose. There was no observed toxicity in any of the polyherbal drug pretreated groups even though no separate toxicity study was conducted. It may be necessary to adjust the dose for their justifi ed use in traditional medicine.
Acknowledgment
The fi rst author (CG) acknowledges the institutional grant-in-aid for his doctoral work. The authors thank the manufacturers for providing hepatoprotective formulations used as test drugs.
References
1. Rai MK. Herbal medicines in India; retrospect and prospect. Fitoterapia 1994; 65 : 483-91.
2. Schuppan D, Jia JD, Brinkhaus B, Hahn EG. Herbal products for liver diseases: a therapeutic challenge for the new millennium. Hepatology 1999; 30 : 1099-104.
3. Sharma A, Chakraborti KK, Handa SS. Antihepatotoxic activity of some Indian herbal formulations as compared to silymarin. Fitoterapia 1991; 62 : 229-35.
4. Subramonium A, Pushpangadan P. Development of phytomedicines for liver diseases. Indian J Pharmacol 1999; Indian J Pharmacol 1999; Indian J Pharmacol31 : 166-75.
5. Handa SS, Sharma A. Hepatoprotective activity of andrographolide from Andographis paniculta against carbon- tetrachloride. Indian J Med Res 1990; 92 : 276-83.
6. Dwivedi Y, Dwivedi Y, Dwivedi Y Rastogi R, Chander R, Sharma SK, Kapoor NK, Garg NK, et al. Hepatoprotective activity of picroliv against carbon tetrachloride-induced liver damage in rats. Indian J Med Res 1990; 92 : 195-200.
7. Thyagarajan SP, Subramanian S, Thirunalasundari T, Venkateswaran PS, Blumberg BS. Effect of Phyllanthus amarus on chronic carriers of hepatitis B virus. Lancet 1988; Lancet 1988; Lancet2 : 764-6.
8. Gadgoli C, Mishra SH. Antihepatotoxic activity of p-methoxy benzoic acid from Capparis spinosa. J Ethnopharmacol 1999; J Ethnopharmacol 1999; J Ethnopharmacol66 : 187-92.66 : 187-92.66
9. Gupta AK, Sharma M. editors. Reviews on Indian medicinal plants, vol. 5. New Delhi: Indian Council of Medical Research; 2007.
10. Ghosh MN. Fundamentals of experimental pharmacology, 3rd
ed. Kolkata: Hilton & Company; 2005.
GIRISH et al: HERBAL FORMULATIONS FOR HEPATOPROTECTION 577
11. Gupta AK, Misra N. Hepatoprotective activity of aqueous ethanolic extract of Chamomile capitula in paracetamol intoxicated albino rats. Am J Pharmacol Toxicol 2006; Am J Pharmacol Toxicol 2006; Am J Pharmacol Toxicol 1 : 17-20.
12. Wendel A, Feuerstein S, Konz KH. Acute paracetamol intoxication in starved mice leads to lipid peroxidation in vivo. Biochem Pharmacol 1979; Biochem Pharmacol 1979; Biochem Pharmacol 28 : 2051-5.
13. Dash DK, Yeligar VC, Nayak SS, Ghosh T, Rajalingam D, Sengupta P, et al. Evaluation of hepatoprotective and antioxidant activity of Ichnocarpus frutescens (Linn.) R.Br. on paracetamol-induced hepatotoxicity in rats. Trop J Pharmaceut Res 2007; 6 : 755-65. 6 : 755-65. 6
14. Hwang YP, Choi CY, Chung YC, Jeon SS, Jeong HG. Protective effects of puerarin on carbon tetrachloride-induced hepatotoxicity. Arch Pharm Res 2007; 30 : 1309-17.
15. Sallie R, Tredger JM, Williams R. Drugs and the liver. Part 1: Testing liver function. Biopharm Drug Dispos 1991; 12 : 251-9.
16. Rajesh MG, Latha MS. Preliminary evaluation of the antihepatotoxic activity of Kamilari, a polyherbal formulation. J Ethnopharmacol 2004; J Ethnopharmacol 2004; J Ethnopharmacol 91 : 99-104.
17. Sherlock S, Dooley J. Drugs and the liver. In: Diseases of liver and Biliary system. 11 ed. Oxford: Blackwell Scientifi c Publications; 2002. p. 322-56.
18. Pari L, Murugan P. Protective role of tetrahydrocurcumin Murugan P. Protective role of tetrahydrocurcumin Murugan Pagainst erythromycin estolate-induced hepatotoxicity. Pharmacol Res 2004; 49 : 481-6.
19. Dahanukar SA, Kulkarni RA, Rege NN. Pharmacology of medicinal plants and natural products. Indian J Pharmacol2000; 32 : S81-118.
20. De Smet PAGM. The role of plant derived drugs and herbal medicines in health care. Drugs 1997; 54 : 801-40.
21. Thyagarajan SP, Jayaram S, Gopalakrishnan V, Hari R, Jeyakumar P, Sripathi MS. Herbal medicines for liver diseases in India. J Gastroenterol Hepatol 2002; J Gastroenterol Hepatol 2002; J Gastroenterol Hepatol 17 : S370-6. 17 : S370-6. 17
22. Najmi AK, Pillai KK, Pal SN, Aqil M. Free radical scavenging and hepatoprotective activity of Jigrine against galactosamine induced hepatopathy in rats. J Ethnopharmacol 2005; J Ethnopharmacol 2005; J Ethnopharmacol 97 : 97 : 97521-5.
23. Huseini HF, Alavian SM, Heshmat R, Heydari MR, Abolmaali K. The effi cacy of Liv-52 on liver cirrhotic patients: a
Reprint requests: Dr S.C. Pradhan, Department of Pharmacology, Jawaharlal Institute of Postgraduate Medical Education & Research Dhanwanthri Nagar, Puducherry 605 006, Indiae-mail: [email protected]
randomized, double-blind, placebo-controlled fi rst approach. Phytomedicine 2005; 12 : 619-24.
24. Negi AS, Kumar JK, Luqman S, Shanker K, Gupta MM, Khanuja SP. Recent advances in plant hepatoprotectives: a Khanuja SP. Recent advances in plant hepatoprotectives: a Khanuja SPchemical and biological profi le of some important leads. Med Res Rev 2007; 28 : 746-72.
25. Koul IB, Kapil A. Effect of diterpenes from Andrographis paniculata on antioxidant defense system and lipid peroxidation. Indian J Pharmacol 1994; Indian J Pharmacol 1994; Indian J Pharmacol 26 : 296-300.26 : 296-300.26
26. Fu Y, Fu Y, Fu Y Zheng S, Lin J, Ryerse J, Chen A. Curcumin protects the rat liver from CCl
4-caused injury and fi brogenesis by
attenuating oxidative stress and suppressing infl ammation. Mol Pharmacol 2008; Mol Pharmacol 2008; Mol Pharmacol 73 : 399-409.
27. Shin MS, Kang EH, Lee YI. A fl avonoid from medicinal plants blocks hepatitis B virus-e antigen secretion in HBV-infected hepatocytes. Antiviral Res 2005; 67 : 163-8.67 : 163-8.67
28. Kang EH, Kown TY, Kown TY, Kown TY Oh GT, Park WF, Park SI, Park SK, et al.The fl avonoid ellagic acid from a medicinal herb inhibits host immune tolerance induced by the hepatitis B virus-e antigen. Antiviral Res 2006; 72 : 100-6.
29. Grawford JM. Liver and biliary tract. In: Kumar V, Abbas AK, Fausto N, editors. Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia: Elsevier; 2005. p. 877-937.
30. Handa SS, Sharma A. Hepatoprotective activity of andrographolide against galactosamine & paracetamol intoxication in rats. Indian J Med Res 1990; 92 : 284-92.
31. Rang HP, Dale MM, Ritter JM, Moore PK. Harmful effects of drugs. In: Pharmacology, 5 ed. Churchill Livingstone. Edinburgh; 2003. p. 724-37.
32. Choudhury BR, Poddar MK. Andrographolide and Kalmegh (Andrographis paniculata(Andrographis paniculata( ) extract: in vivo and in vitroeffect on hepatic lipid peroxidation. Methods Find Exp Clin Pharmacol 1984; Pharmacol 1984; Pharmacol 6 : 481-5.
33. Srivastava S, Srivastava AK, Srivastava S, Patnaik GK, Dhawan BN. Effect of picroliv and silymarin on liver regeneration in rats. Indian J Pharmacol 1994; Indian J Pharmacol 1994; Indian J Pharmacol 26 : 19-22.26 : 19-22.26
34. Thresiamma KC, Kuttan R. Inhibition of liver fi brosis by ellagic acid. Indian J Physiol Pharmacol 1996; Indian J Physiol Pharmacol 1996; Indian J Physiol Pharmacol 40 : 363-6.
35. Satyavati GV, Gupta AK, Tandon N, editors. Medicine plants of India, vol. 2. New Delhi: Indian Council of Medical Research; 1987.
578 INDIAN J MED RES, MAY 2009





























