-
Cancer Biology and Translational Studies
HER-Family Ligands Promote AcquiredResistance to Trastuzumab in
Gastric CancerA€�da Sampera1, Francisco Javier S�anchez-Martín1,
Oriol Arpí1, Laura Visa2,
Mar Iglesias3,4, Sílvia Men�endez1, �Elisabeth Gaye5, Alba
Dalmases1, Sergi Clav�e1,3,Mariona Gelabert-Baldrich1, Thomas Tuxen
Poulsen6, Michael Kragh6,Beatriz Bellosillo1,3, Joan Albanell1,2,7,
Ana Rovira1,2, and Clara Montagut1,2,7
Abstract
Despite the clinical benefit of trastuzumab, eventually
allHER2-amplified gastric cancer tumors developdrug resistance.We
aimed to identify molecular mechanisms of acquiredresistance to
trastuzumab in gastric cancer by using well-established cell
line–based preclinical models, as well assamples from patients with
HER2-positive gastric cancer trea-ted with trastuzumab. We studied
trastuzumab resistance inNCI-N87 and OE19, two gastric cancer cell
lines that over-express HER2 receptor and are trastuzumab
sensitive. Differ-ences at protein, DNA, and RNA levels between the
parentaland resistant cells were characterized and functional
studieswere performed. Paired pre- and post-trastuzumab blood
andtissue samples from patients with gastric cancer treated
withtrastuzumab were analyzed. We found that resistant cellswere
associated with increased activation of MAPK/ERK andPI3K/mTOR
pathways driven by SRC activation. Upstream,
resistant cells showed increased coexpression of
multipleHER-family ligands that allowed for compensatory
activationof alternative HER receptors upon HER2 blockade.
Simulta-neous inhibition of EGFR, HER2, and HER3 by the
novelantibody mixture, Pan-HER, effectively reverted
trastuzumabresistance in vitro and in vivo. Similarly, an increase
inHER-family ligands was observed in serum and tumor frompatients
with gastric cancer after trastuzumab therapy. Wepropose that
trastuzumab resistance in gastric cancer is medi-ated by HER-family
ligand upregulation that allows acompensatory activation of HER
receptors and maintainsdownstream signaling activation despite
trastuzumab therapy.Resistance is reverted by simultaneous
inhibition of EGFR,HER2, and HER3, thereby revealing a potential
therapeuticstrategy to overcome trastuzumab resistance in patients
withgastric cancer.
IntroductionGastric cancer is the fifth most common cancer
worldwide and
the third leading cause of cancer-related cell death (1). At
diag-nosis, most patients present inoperable locally advanced
ormetastatic disease, with a median overall survival below 1year
(2).
Approximately 20%of gastric cancer tumors, depending on
thesubtype of the tumor, overexpress the HER2 (2–4). HER2 is a
member of the HER-family of receptors and a recognized
keytherapeutic target in breast and gastric cancer. It is
associated withtumor cell proliferation, survival, angiogenesis,
migration, and itcorrelates with a poor outcome and amore
aggressive disease (5).In the ToGA trial, the addition of
trastuzumab, a mAb against theHER2 receptor, to chemotherapy
improved overall survival (OS)of patients with HER2-positive
gastric cancer in 4.2 months (2).This led to the approval of
trastuzumab in combination withcisplatin plus fluoropyrimidine as
first-line treatment for HER2-positive advanced gastric cancer or
gastro-esophageal junctionadenocarcinoma (6). Trastuzumab inhibits
tumor growthmainlythrough prevention of HER2 homodimerization and
blockade ofHER2 downstream signaling (7), inhibition ofHER2
extracellularamino-terminal domain (ECD) shedding (8), and
induction ofantibody-dependent cellular cytotoxicity (ADCC; refs.
9, 10).
Despite the significant survival benefit of trastuzumab
inpatients with gastric cancer, drug resistance invariably
devel-ops (2). Identification of molecular mechanisms of
acquiredresistance to trastuzumab in gastric cancer is crucial to
delineatemore effective therapeutic strategies in the clinical
setting.Mechanisms of resistance to trastuzumab in gastric cancer
arepoorly characterized. Preclinical evidence suggests
alternativeactivation of downstream signaling pathways, such as
overexpres-sion of FGF 3 (11). Recently, next-generation sequencing
analysisrevealed secondary alterations in ERBB2 as well as
mutations inRAS/PI3K downstream signaling pathways in
post-trastuzumabsamples from patients with gastro-esophageal
junction adeno-carcinoma (12). Remarkably, these molecular
alterations only
1Cancer Research Program, Institut Hospital del Mar
d'Investigacions M�ediques(IMIM)-CIBERONC, Barcelona, Spain.
2Department of Medical Oncology, Hos-pital del Mar-CIBERONC,
Barcelona, Spain. 3Department of Pathology, Hospitaldel Mar,
Barcelona, Spain. 4Universitat Autonoma de Barcelona, Spain.
5Onco-logie M�edicale, Institut de C�ancerologie et H�ematologie,
Morvan, Brest, France.6Symphogen A/S, Ballerup, Denmark.
7Universitat Pompeu Fabra, Barcelona,Spain.
Note: Supplementary data for this article are available at
Molecular CancerTherapeutics Online
(http://mct.aacrjournals.org/).
Current address for M. Gelabert-Baldrich: Centre for Genomic
Regulation, TheBarcelona Institute for Science and Technology,
Barcelona, Spain.
Corresponding Author: Clara Montagut, Del Mar University
Hospital, PasseigMaritim 25–29, Barcelona 08003, Spain. Phone:
34-9-3248-3137; Fax: 34-9-3248-3366; E-mail:
[email protected]
Mol Cancer Ther 2019;18:2135–45
doi: 10.1158/1535-7163.MCT-19-0455
�2019 American Association for Cancer Research.
MolecularCancerTherapeutics
www.aacrjournals.org 2135
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://crossmark.crossref.org/dialog/?doi=10.1158/1535-7163.MCT-19-0455&domain=pdf&date_stamp=2019-10-18http://crossmark.crossref.org/dialog/?doi=10.1158/1535-7163.MCT-19-0455&domain=pdf&date_stamp=2019-10-18http://mct.aacrjournals.org/
-
explain trastuzumab resistance in a subset of patients. In
thisstudy, we aimed to explore additional mechanisms of
acquiredresistance to trastuzumab in gastric cancer by using a
well-established cell line–based preclinical model, as well as
clinicalsamples from gastric cancer patients treated with
trastuzumab.
Material and MethodsCellular models and reagents
The human gastric cancer cell line NCI-N87 was purchasedfrom
ATCC and the OE19 and OTR6 (OE19 derived trastuzumabresistant)
cells were kindly provided by Symphogen A/S (13, 14).All cell lines
wereMycoplasma free and authenticity was tested bySTR DNA Profiling
analysis at the ATCC (October 2014) afterresistant cells were
generated. The number of passages betweenthawing and use in the
described experiments was 10 or less. Cellswere grown as reported
previously (15). Trastuzumab (Herceptin,Genentech, Roche) was
obtained from the Hospital del Marpharmacy. Everolimus (RAD001),
pimasertib (AS-703026;ref. 16), and saracatinib (AZD0530; ref. 17)
were purchased fromSelleckchem, and Pan-HER from Symphogen A/S
(13). Humanrecombinant EGF was from Calbiochem (Merck KGaA)
andneuregulin (NRG1) from Sigma Aldrich Co (Merck KGaA).
Generation of trastuzumab-resistant cellsNCI-N87 cells were
cultured in the presence of 15 mg/mL of
trastuzumab until cells were considered resistant (7 months;cell
viability reduction �20%; refs. 18, 19).
Single-cell–derivedresistant clones were isolated from the
resistant pools using8 mm � 8 mm diameter cloning cylinders
(Millipore, MerckKGaA) and further propagated for 3 more months in
mediacontaining 15 mg/mL trastuzumab (18, 20, 21).
Trastuzumabresistance was validated after a cycle of freezing and
thawing andafter drug withdrawal up to 6 months (22). Parental
cells werecultured without trastuzumab to exclude that resistance
was dueto long time culturing.
Cellular proliferation assayTo analyze the growth inhibitory
effect of trastuzumab, alone
or in combination with pimasertib, everolimus, or ligands,
orperform dose curves, with trastuzumab, Pan-HER, cetuximab,
orpertuzumab, 8–12 � 103 cells per well in a 24-well plate
weretreated for 7 days. Cells were stained for 1 hour with crystal
violetsolution at 0.1%. Quantification was evaluated with
ImageJsoftware. To perform growth curve experiments with
lapatinib,we plated 5–7 � 103 cells per well in 96-well plate. Cell
viabilitywas obtained using CellTiter 96 Aqueous One Solution
CellProliferation Assay (MTS) following the manufacturer's
proce-dures. IC50 values were calculated using CalcuSyn software.
Eachexperiment was performed at least three times and results
wereplotted as percentage of the control.
Trastuzumab binding by flow cytometryWe measured trastuzumab
binding to HER2 receptor as
reported previously (15), incubating cells with trastuzumab100
ng/mL as the primary antibody.
FISHTo assess ERBB2 copy number alterations, we applied the
PathVysion HER-2 DNA FISH Probe Kit (Abbott Molecular Inc).FISH
was performed in fixedmaterial obtained from the cell lines
after application of a conventional cytogenetic protocol.
About100 nonoverlapping cells with hybridization signals were
exam-ined for each case and amplificationwas defined as
ERBB2/CEP17ratio �2.0 (23).
ImmunocytochemistryTo study HER2 protein expression, 1 � 107 of
cells were
pelleted, fixed with formalin, and embedded with paraffin(FFPE).
HER2 expression was evaluated using HercepTest. Sec-tions of 3
mmwere placed on plus charged glass slides. The HER2antibody used
was PATHWAY anti-HER-2/neu (4B5) rabbitmonoclonal primary antibody
(Ventana Medical Systems, Inc.)and revealed with ultraView
Universal 3,30-diaminobenzidine(DAB) Detection Kit (Ventana Medical
Systems, Inc.) as thechromogen and counterstained with hematoxylin.
HER2 stainingwas performed and evaluated in the Pathology
Department ofHospital del Mar according to NCCN Guidelines
(24).
Protein detectionWhole-cell lysates were subjected to Western
blot analyses as
reported previously (20). The primary antibodies used were:EGFR,
HER3, phosphoERK1/2 (T202/Y204), ERK1/2, phos-phoAKT (S473), AKT,
phosphoS6 (S235/236), S6, phosphoSRC(Y416), and SRC purchased from
Cell Signaling Technology;HER2 from BioGenex (clone CB11);
a-Tubulin and b-Actin fromSigma-Aldrich Co (Merck KGaA).
Phospho-receptor tyrosine kinase arrayWe screened the activity
of different receptor tyrosine kinase
(RTK) and signaling nodes using PathScan RTK Signaling Anti-body
Array Kit (Chemiluminescent Readout) catalog no. 7982 ofCell
Signaling Technology following the manufacturer's proce-dures.
Image acquisition was done with the Typhoon ScannerControl v5.0
software and quantified with the ImageQuant TLv7.0. The
digitalization part was done at Centre for GenomicRegulation in
theParc deRecerca Biom�edica deBarcelona (PRBB).
Gene expression microarrayRNA isolation and gene
expressionmicroarray were performed
using the Human Gene 2.0 ST Array GeneChip (Affymetrix)
asdetailed in Supplementary Material and Methods.
qRT-PCRTotal RNA was extracted from cells in basal conditions
and
treated with trastuzumab 15 mg/mL and Pan-HER 10 mg/mL
for24hours. cDNAwas synthetized using randomprimers
andHigh-Capacity cDNA Reverse Transcription Kit (Applied
Biosystems).Samples from three independent RNA extractions were
amplifiedusing specific primers and LightCycler 480 SYBR Green I
Master(Roche) in the LightCycler 480 Real Time PCR-System
device(Roche). The primers used were: EGF Forward:
50-CGTGTCGT-GAAGGTTTTATG-30 and EGF Reverse:
50-GTTCTTTAGAT-CAACTTCACC-30; AREG Forward:
50-GCATGATTGACAGTAGTT-TATC-30 and AREG Reverse:
50-TTCTAAGCTGGACTGTAATAAC-30; TGFA Forward:
50-TGTGTCTGCCATTCTGGGTA-30 and TGFAReverse
50-GACCTGGCAGCAGTGTATCA-30; HBEGF
Forward:50-GGAGAATGCAAATATGTGAAG-30 and HBEGF Reverse:
50-TTCCACTGGGAGGCTCAG-30; NRG1 Forward: 50-CAGCCCAA-GAGCCTGTTAAG-30
andNRG1 Reverse: 50-ACTGCTCTGGGAG-CTTGTGT-30; and ATP5E Forward:
50-GATCTGGGAGTATCG-GATG-30 and ATP5E Reverse:
50-CCGGCGTCTTGGCGATTC-30.
Sampera et al.
Mol Cancer Ther; 18(11) November 2019 Molecular Cancer
Therapeutics2136
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
Gene expressionwas calculated as 2 to the power of�DDCt,
whereDDCt ¼ ðCtGene � CtATP5E or ACTIN Þ Assay.
ELISA analysisCell culture medium from 1–5 � 106 cells plated in
100 mm
culture dishwith 10mLofmedium for 72hourswas concentratedusing
Amicon Ultra-4 Centrifugal Filter Units (Millipore, MerckKGaA)
following the manufacturer's procedures. Ligands' levelsin the
medium were measured using the Human EGF DuoSet#DY236, Human
Amphiregulin DuoSet #DY262, and HumanTGF-alpha DuoSet #DY239 ELISA
(R&D Systems) according tothe manufacturer's procedures.
Subcutaneous tumorigenesisFive-week-oldmale FoxChase
SCIDBeigemicewere purchased
from Charles River Laboratories and hosted in the
pathogen-freeanimal facility at the PRBB. Animal treatments were
doneaccording to institution-approved protocols. A total of 5 �
106cells were resuspended in sterile PBS with 50% of Matrigel
(BDBiosciences) and subcutaneously injected into the flank of
themice. Tumor volume was determined twice a week from
calipermeasurements of tumor length (L) and width (W) according
tothe formula (L �W2 � 3.1416)/6. When tumor volume reached200–300
mm3, mice were randomized to three groups with 10mice in each one.
IgG isotype control, trastuzumab (20 mg/kg),and Pan-HER (60 mg/kg)
were administered intraperitoneallythree times a week until
significant effect on tumor growth wasobserved of the treatment
versus control or until tumor volumewas too large, for ethical
reasons (30 days for parental and 85daysfor resistant cells). Mice
were euthanized and part of the tumorswas FFPE for IHC studies.
IHCParaffin sections were used for IHC analysis as described
in
Immunocytochemistry section. Tumor sections were stained
withhematoxylin and eosin (H & E) to assess histologic changes.
Toevaluate proliferation and apoptosis, slices were incubated
withthe antibodies Ki-67 (clone MIB-1, Dako, Agilent
Technologies)mouse mAb at 1:100, anti-phosphorylated (Ser10)
Histone 3(Cell Signaling Technology) rabbit polyclonal antibody at
1:100,and active caspase-3 [clone ASP175 (5A1), Cell Signaling
Tech-nology] rabbit monoclonal antibody at 1:100.
Antigen–antibodyreaction was detected by incubation with an
anti-mouse/rabbitIg–dextran polymer coupled with peroxidase (Flexþ,
Dako, Agi-lent Technologies). Sections were then visualized with
DAB aschromogen and counterstainedwith hematoxylin. H& E and
IHCstaining was performed and evaluated in the Pathology
Depart-ment of Hospital del Mar. Data were presented as the
percentageof positive tumor cells.
Patient samplesBlood samples and tumor specimens frompatients
withHER2-
positive gastric cancer and gastro-esophageal junction
adenocar-cinoma that received trastuzumab and chemotherapy
treatmentwere collected at diagnosis (pre-trastuzumab) and after
trastuzu-mab therapy (post-trastuzumab) at Hospital del Mar.
Ligandlevels of serum samples were measured by ELISA as described
inELISA analysis. In FFPE tumor tissue samples, RNA was
extractedusing the MagMAX FFPE DNA/RNA Ultra Kit catalog no.
A31881(Thermo Fisher Scientific) and EGF expression analysis was
per-formed as described in qRT-PCR section.
Statistical analysisStatistical analyseswere carriedout
usingone-wayANOVA tests
followed by post hoc Tukey adjustment or Student t test. Prism
5.0software (GraphPad) was used for the statistical analyses.
Datashown is mean � SD of three independent replicates.
ResultsGeneration and characterization of
trastuzumab-resistantgastric cancer cells
To identify potential mechanisms of acquired resistance
totrastuzumab, we performed an extensive screening on gastriccancer
cell lines that could be used to generate resistance totrastuzumab
and mimic the clinical setting. The requirementswere: gastric
cancer adenocarcinoma, HER2 receptor amplifica-tion and
overexpression, and high sensitivity to trastuzumab.Only two cell
lines (NCI-N87 and OE19) fulfilled these require-ments. NCI-N87
cells were selected to generate single-cell trastu-zumab-resistant
derivatives and characterize the resistance(Fig. 1A and B). Then
results were confirmed in the OTR6 cells(OE19-derived trastuzumab
resistant). Differences in cell mor-phology were observed between
parental and resistant cells,showing the latter a flatter
morphologic appearance (Fig. 1B).To explore potential mechanisms of
resistance, we performednext-generation sequencing to analyze
hotspot regions of a panelof genes commonly altered in cancer and
related to HER2 sig-naling, including ERBB2, EGFR, KRAS, NRAS,
BRAF, and PIK3CA(listed in Supplementary Material and Methods). We
did notidentify the emergence of mutations in these genes in
resistantcompared with parental cells.
Trastuzumab-resistant cells grow independently of HER2To exclude
the role of HER2 in the resistant phenotype, we
determined whether there were substantial differences in
HER2receptor amplification, expression, and activation in
resistantcompared with parental cells. Trastuzumab-resistant cells
main-tained ERBB2 gene amplification similar to parental cells,
asassessed by FISH analysis (Fig. 1B). Moreover, genomic
analysisdid not detect pointmutations in ERBB2 gene. IHC
showedHER23þ immunoscore in both parental and resistant cells,
although asmall reduction in protein staining was observed in
resistantcompared with parental cells that was confirmed byWestern
blotanalysis (Figs. 1B, 2A, 3E, and 4B).
The HER2 inhibitor lapatinib did not affect the viability
ofresistant cells compared with parental cells (Fig. 1C;
Supplemen-tary Fig. S1), suggesting that resistant cells were no
longer depen-dent on HER2 for their growth and survival. Although
we hadexcluded the role of a secondary mutation in ERBB2 gene as
amechanism of resistance, it remained possible that reduced
drug-receptor binding affinity was involved in resistance (21, 25).
Totest whether trastuzumab was actively recognizing the cell
surfaceof HER2, we performed flow cytometry analysis which
revealedthat trastuzumab was binding to 100% of the cells in both
theparental and resistant cells (Fig. 1D).
Resistance to trastuzumab is associated with
SRC-mediatedactivation of MAPK/ERK and PI3K/AKT pathways
To explore the role of HER2 cell signaling in resistance,
wecharacterized HER2 downstream effectors in parental and
resis-tant cells. Resistant cells had an increase in basal levels
of SRC,ERK 1/2, and S6 phosphorylation, which was confirmed by
a
HER-Family Ligands in Trastuzumab-Resistant Gastric Cancer
www.aacrjournals.org Mol Cancer Ther; 18(11) November 2019
2137
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
phospho-array analysis (Fig. 2A and B; Supplementary Fig. S2).
Asexpected, trastuzumab treatment reduced phosphorylation ofHER2
downstream proteins SRC, AKT, ERK 1/2, and S6 inparental cells.
However, HER2 downstream effectors persistedactivated in the
resistant cells (Fig. 2A).
To establish whether the MAPK/ERK and PI3K/mTOR path-ways played
a role in maintaining survival and cell growth in theresistant
cells, functional pharmacologic studies were performedwith the MEK
inhibitor pimasertib and the mTOR inhibitoreverolimus. Each drug
effectively targeted ERK and S6, respec-tively, and partially
inhibited cell viability of resistant cells. Ofnote, the addition
of trastuzumab had no additional effect,
supporting the limited role of HER2 in driving resistance(Fig.
2C; Supplementary Figs. S3, S4A and S4B). Simultaneousinhibition of
both ERK and PIK3 pathways by the combination ofpimasertib and
everolimus resulted in higher cell viability inhi-bition compared
with each drug alone, suggesting that bothMAPK/ERK and PIK3/mTOR
pathways were critical in maintain-ing cell growth and survival in
the resistant cells (Fig. 2C; Sup-plementary Fig. S3).
To assess whether persistent activation of MAPK/ERK andPI3K/mTOR
pathways in resistant cells was driven by the com-mon upstream
activator SRC, we treated resistant cells with thesmall molecule
SRC kinase inhibitor saracatinib. Saracatinib
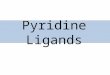
Figure 1.
Proliferation of trastuzumab-resistant cells is independent of
HER2. A, Cell viability analyzed by staining the cells with crystal
violet after treating the cells withtrastuzumab (15 mg/mL) for 7
days. ��� , P < 0.001. B, Representative images of parental and
resistant cells under light microscopy (top images).
ERBB2amplification by FISH: ERBB2 gene in red and centromere of
chromosome 17 (CEP17) in green (middle images). HER2 overexpression
by IHC (bottom images).C,Dose curve of lapatinib by MTS assay after
72 hours. IC50 values of lapatinib: IC50 parental cells¼ 0.26
mmol/L (SD 0.09); IC50 values for resistant cells notreached. ���,
P < 0.001. Molecular effects in Supplementary Fig. S1. D,
Histogram representing mean fluorescence intensity of
trastuzumab-PE (Tz-PE)-expressing cells corresponding to 10,000
events. Parental and resistant cells (in dark and light gray,
respectively) were incubated with trastuzumab (100 ng/mL)and a goat
anti-human IgG conjugated with phycoerythrin (PE) as secondary
antibody.
Sampera et al.
Mol Cancer Ther; 18(11) November 2019 Molecular Cancer
Therapeutics2138
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
significantly decreased cell viability in the resistant cells
(Fig. 2C;Supplementary Fig. S3), which was correlated with
effectivesuppression of HER2 downstream effectors
(SupplementaryFig. S4C). Of note, because SRC mutations have been
shown todrive lapatinib resistance inagastric
cancerpreclinicalmodel (26),we sequenced the whole SRC gene. SRC
mutations were neitherdetected in parental nor resistant cells.
Taken together, these results strongly suggested that
sustainedactivation of both MAPK/ERK and PI3K/mTOR pathways
medi-ated by SRC was critical to the maintenance of cell survival
inresistant cells.
MultipleHER-family ligands areoverexpressed in
trastuzumab-resistant cells
To explore upstreammechanismsof SRC-mediatedMAPK/ERKand
PI3K/mTOR pathways activation in the trastuzumab-resistant cells,
we analyzed expression of HER-family receptorsand related ligands.
Gene expression array showed no significantdifferences in basal
expression of total HER receptors in resistantcompared with
parental cells. Following trastuzumab therapy, atrend toward an
increase in total EGFR, ERBB3, and ERBB4 wasobserved compared with
parental lines (Fig. 3A). Strikingly,HER-family ligands including
epidermal growth factor (EGF),
amphiregulin (AREG), transforming growth factor alpha
(TGFA),heparin-binding EGF-like growth factor (HBEGF),
andneuregulin1 (NRG1) were significantly overexpressed in resistant
comparedwith parental cells (Fig. 3A and B). In addition, increased
levels ofAREG and TGFa were detected in the cell culture medium
ofresistant cells compared with parental cells (Fig. 3C). NRG1
andEGF could not be assessed in medium because of a very low
limitof detection. Hence, we hypothesized that simultaneous
over-expression of several HER-family ligands allowed for a
compen-satory effect to maintain the activation of downstream
signalingpathways upon HER2 blockade in the resistant cells.
HER-family ligand overexpression protects from
trastuzumabinhibition
To explore whether HER-family ligands were able to
inducetrastuzumab resistance, we exposed the parental cells to
highconcentrations of ligands. Incubationof parental cellswith
EGForNRG1 stimulated cell growth (Fig. 3D). The addition of
eitherligand reduced the inhibitory effect of trastuzumab (Fig.
3D;Supplementary Fig. S5). Accordingly, biochemical
analysisrevealed an activation of HER downstream effectors
followingligand stimulation, which was not completely abrogated by
theaddition of trastuzumab (Fig. 3E).
Figure 2.
Resistance to trastuzumab is driven by activation of SRC and
downstream MAPK and PIK3 signaling. A, Biochemical analysis of HER2
and downstream effectorsin basal conditions and following
trastuzumab therapy. Cells were cultured in the presence of
trastuzumab (15 mg/mL) for 24 hours. Immunoblots wereperformed
using antibodies to the indicated proteins. B, Cell lysates of
parental and resistant cells in basal conditions were incubated
with a phospho-array.Antibodies against RTK and signaling nodes are
spotted in duplicates. Gray squares indicate the most relevant
changes in intensity. Quantification of thephospho-array is shown
in Supplementary Fig. S2. C, Cell viability was analyzed by
staining the cells with crystal violet after treating the cells
with the indicateddrugs for 7 days. �� , P < 0.01; ��� , P <
0.001. Representative images are shown in Supplementary Fig. S3
andmolecular effects in Supplementary Fig. S4.
HER-Family Ligands in Trastuzumab-Resistant Gastric Cancer
www.aacrjournals.org Mol Cancer Ther; 18(11) November 2019
2139
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
To evaluate whether simultaneous complete blockade of allmembers
of the HER-family of receptors could prevent ligand-induced
downstream activation, we used Pan-HER: a novel anti-body mixture
comprised of synergistic pairs of antibodies target-ing EGFR, HER2,
and HER3 in nonoverlapping epitopes (13).Pan-HER significantly
reduced cell viability of parental cells evenin the presence of
ligands (Fig. 3D; Supplementary Fig. S5) andthis was correlated
with effective inhibition of EGFR, HER2,HER3, and downstream
signaling in biochemical analysis specif-ically pAKT/pS6/pERK for
EGF and pAKT/pS6 for NRG1 (Fig. 3E).
Simultaneous inhibition of EGFR, HER2, and HER3 by Pan-HER
overcomes acquired resistance to trastuzumab in vitro
Because Pan-HER was blocking HER-family downstream acti-vation
even in the presence of ligands, we aimed to explorewhether Pan-HER
could revert trastuzumab acquired resistancein our model. Notably,
Pan-HER significantly reduced cell via-bility of
trastuzumab-resistant cells and this was correlated with
asuccessful depletion of EGFR, HER2, and HER3 as well as
aninhibition of the downstream effectors (Fig. 4; SupplementaryFig.
S7). To study whether triple blockade of EGFR, HER2, andHER3 was
necessary to overcome trastuzumab resistance, wetreated resistant
cells with specific EGFR (cetuximab) orHER2/HER3
(pertuzumab)-targeted therapies. Neither cetuxi-
mab nor pertuzumab were able to revert trastuzumab
resistance(Fig. 4A; Supplementary Fig. S7). Such results, together
with thesimultaneous upregulation of several HER-family ligands
(Fig. 3BandC) confirmed that compensatory ligand-induced
coactivationof alternative HER-family members is involved in
driving resis-tance to trastuzumab. Therefore, complete and
simultaneousblockade of all HER-family members is necessary to
revert tras-tuzumab resistance in our model.
Mechanisms of resistance to trastuzumab are confirmed inanother
preclinical model
Remarkably, results were confirmed in the OTR6-resistant
cellsderived from the trastuzumab-sensitive HER2-amplified OE19cell
line. Trastuzumab was less effective in reducing ERK 1/2 andS6
phosphorylation in OTR6-resistant cells compared with theparental
cells (Supplementary Fig. S8A). In addition, NRG1,AREG, and EGF
ligands were overexpressed in OTR6-resistantcells (Supplementary
Fig. S8B), and a high increase in NRGexpression was observed upon
trastuzumab treatment in OE19parental cells (Supplementary Fig.
S8C). Similar toNCI-N87 cells,EGF and NRG1 stimulation reduced
trastuzumab growth inhib-itory rate inOE19parental cells, and
simultaneous blockade of allHER-family of receptors by Pan-HER was
able to prevent ligand-induced downstream activation (Supplementary
Fig. S9A and
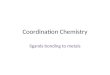
Figure 3.
Resistant cells overexpress multiple HER-family ligands, and
HER-family ligand overexpression protects from trastuzumab
inhibition. A, Heatmap representationof 15 selected gene
expressions. Columns represent the mean of the intensities in the
groups of triplicates parental control, parental trastuzumab,
resistantcontrol, and resistant trastuzumab. Cells were cultured in
the presence of trastuzumab (15 mg/mL) for 48 hours. Columns are
clustered with ward. D2 method androws are clustered with
averagemethod using in both cases correlation distances. Color
intensity means degree of gene expressionmodulation. B, Analysis
ofindicated gene expression by qRT-PCR. Gene expression levels were
normalized to ATP5E as the housekeeping gene. Resistant cell data
were normalized to therespective parental cell expression level
(set at 1, dotted line). ���, P < 0.001. C, Levels of AREG and
TGFa protein in cell culture medium of resistant cellsnormalized to
the respective parental levels (set at 1, dotted line) measured by
ELISA. � , P < 0.05. D, Cell viability was analyzed by staining
the cells with crystalviolet after treating the cells with
trastuzumab (15 mg/mL), Pan-HER (10 mg/mL), EGF (1 nmol/L), or NRG1
(5 nmol/L) during 7 days. �, P < 0.05 and ��� , P <
0.001.Representative images in Supplementary Fig. S5. E,
Biochemical analysis of HER-family receptors and downstream
effectors following ligand stimulation. Cellswere cultured in the
presence of trastuzumab (15 mg/mL) or Pan-HER (10 mg/mL) for 24
hours, followed by 15 minutes with EGF (1 nmol/L) or NRG1 (5
nmol/L).Immunoblots were performed using antibodies to the
indicated proteins.
Sampera et al.
Mol Cancer Ther; 18(11) November 2019 Molecular Cancer
Therapeutics2140
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
S9B). At amolecular level, Pan-HERhad amore profound effect
inreducing EGFR, HER2, HER3, and downstream effectors
phos-phorylation compared with trastuzumab, even in the presence
ofligands (Supplementary Fig. S9C). Moreover, Pan-HER
signifi-cantly reduced cell viability of OTR6 trastuzumab–resistant
cellsand this was correlated with a successful depletion of
EGFR,HER2, and HER3 and inhibition of the downstream
effectors(Supplementary Fig. S10).
Triple inhibition of EGFR, HER2, and HER3 by Pan-HERovercomes
trastuzumab resistance in vivo
To expand our studies to in vivomodels, the Pan-HER
antibodymixture was tested in parental and
trastuzumab-resistant–derivedxenografts. As expected, in parental
xenografts both trastuzumaband Pan-HER significantly reduced tumor
growth compared withthe control group (Fig. 5A). In resistant
xenografts, resistance totrastuzumab was observed after 1.5 months
of treatment, whileno tumor growth was observed under treatment
with Pan-HERduring 3months (Fig. 5B).H&E staining of parental
and resistantxenografts showed that Pan-HER–treated tumors were
smallerwith less percentage of ischemic necrosis and more
hyalinizedfibrosis compared with control or trastuzumab-treated
tumors(Fig. 5C; Supplementary Table S1A). IHC analysis showed
lowerstaining percentage of the proliferative markers Ki-67 and
phos-
phorylated (S10) Histone H3 (pHist H3) in Pan-HER–treatedtumors
compared with control or trastuzumab group (Fig. 5C;Supplementary
Table S1B). Staining of the apoptosis markercleaved caspase 3
(c-casp 3) did not totally reflect Pan-HERsuperiority, probably
because Pan-HER–induced apoptosisoccurred previous to mice
sacrifice (Fig. 5C; SupplementaryTable S1B). Altogether, histologic
analysis confirmed a higherPan-HER antitumor efficacy compared with
control and trastu-zumab effect.
HER-family ligands are increased in clinical samples
frompatients with gastric cancer treated with trastuzumab
To explore whether HER-family ligands were involved in
tras-tuzumab resistance in patients, we analyzed pre-trastuzumaband
post-trastuzumab paired samples from 5 patients withHER2-positive
gastric cancer. Clinical characteristics of thepatients are
summarized in Supplementary Table S2. Of note,rebiopsy and
collection of post-trastuzumab samples was limitedbecause of
patient fragility and difficulty in tumor access. Anincrease in
median EGF, AREG, and TGFa concentration wasobserved in
post-trastuzumab compared with pre-trastuzumabserum samples (Fig.
6A; Supplementary Fig. S11A). In tissuesamples, EGF expression was
2.7 times higher in post-trastuzumab tumor biopsy compared with
pre-treatment tumor
Figure 4.
Simultaneous inhibition of EGFR, HER2, and HER3 is necessary to
inhibit cell growth in trastuzumab-resistant cell lines. A, Cell
viability analyzed by stainingresistant cells with crystal violet.
Cells were treated with trastuzumab, cetuximab, pertuzumab, and
Pan-HER dose curves for 7 days. IC50 values of resistant cells:IC50
Pan-HER¼ 26.20 mg/mL (SD 0.96); IC50 values of trastuzumab,
cetuximab, or pertuzumab not reached. �� , P < 0.01; ��� , P
< 0.001. Representative imagesare shown in Supplementary Fig.
S7. B, Biochemical analysis of HER-family receptors and downstream
effectors following trastuzumab and Pan-HER treatment.Cells were
cultured in the presence of trastuzumab (15 mg/mL) or Pan-HER (10
mg/mL) for 24 hours. Immunoblots were performed using antibodies to
theindicated proteins.
HER-Family Ligands in Trastuzumab-Resistant Gastric Cancer
www.aacrjournals.org Mol Cancer Ther; 18(11) November 2019
2141
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
sample (Fig. 6B; Supplementary Fig. S11B). Other markers
couldnot be characterized because of insufficient tumor
sampleavailability.
DiscussionThe approval of trastuzumab for patients with
HER2-positive
gastric cancer represented a breakthrough in the treatment of
thisdisease. Unfortunately, responses are transient and resistance
totrastuzumab invariably emerges. To study themolecularmechan-isms
underlying trastuzumab resistance, we studied two
trastu-zumab-resistant cell lines and as proof-of-concept confirmed
thefindings in patients' samples. Our preclinical results showed
thatacquired resistance to trastuzumab was driven by mRNA
increaseof multiple HER-family ligands that allowed compensatory
acti-vation of MAPK/PIK3K downstream signaling in the presence
of
trastuzumab. The novel antibody mixture Pan-HER
effectivelyreverted trastuzumab resistance both in vitro and in
vivo.Accordingly, analysis of clinical samples showed an increase
inHER-family ligands levels after treatment with trastuzumab.
To our knowledge, there is limited evidence on the role
ofHER-family ligands in innate and acquired resistance to
trastuzumab inpatients with gastric cancer. Preclinical models have
shown apotential involvement inEGF ligandupregulation in
trastuzumabresistance in patients with gastric cancer (27, 28).
Similarly, inbreast cancer cell lines, ligand-induced activation of
HER recep-tors has been linked to trastuzumab resistance (29). Also
apotentially broad role of widely expressed receptor-tyrosinekinase
ligands has been shown in innate and acquired resistanceto
small-molecule tyrosine-kinase inhibitors (30). For the firsttime
in gastric cancer, our findings are supported by proof-of-concept
data from a small group of patients treated with
Figure 5.
Pan-HER in vivo efficacy on parental and resistant xenograft
models.A and B, Effects of trastuzumab and Pan-HER on gastric
cancer tumor xenografts. Micewere injected subcutaneously in the
dorsal flank with parental or resistant cells. After tumor reached
an average tumor size of 200–300mm3, mice were
treatedintraperitoneally three times aweek with IgG isotype
control, trastuzumab (20mg/kg), or Pan-HER (60mg/kg). Each group
consisted of 10 mice. Tumorvolumeswere normalized individually to
the volume at the first day of treatment. Pan-HER significantly
reduced tumor volume compared with trastuzumab inboth xenografts.
�, P < 0.05; �� , P < 0.01; ��� , P < 0.001. C,
Representative images of H & E staining and immunostaining for
Ki-67, pHist H3, or c-casp 3 of parentaland resistant xenograft
tumor sections. Scale bar is 5 mm in H & E and 200 mm in IHC
images. Red arrows point to representative positive cells in IHC
images.
Sampera et al.
Mol Cancer Ther; 18(11) November 2019 Molecular Cancer
Therapeutics2142
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
trastuzumab, who showed an increase in HER-family ligands
inserum and tumor tissue after trastuzumab-based therapy.
Coexpression of multiple RTK and compensatory
downstreamsignaling activation has been shown to limit the efficacy
of single-target drugs in other cancer types (29, 31–33). Of note,
in breastcancer models, long-term treatment with trastuzumab leads
tooverexpression of EGFR and HER3, which circumvents HER2inhibition
(31). This suggests that inhibition of multiple RTKsis potentially
necessary to reach a complete abrogation of redun-dant downstream
signaling activation. According to the results inJacobsen and
colleagues, simultaneously targeting of EGFR,HER2, andHER3was
necessary to prevent trastuzumab resistanceinduced by EGF and NRG1
ligand stimulation and by the com-pensatory upregulation of
HER-family of receptors in several celllines (13). Upon receptor
binding, Pan-HER induces internali-zation and degradation of EGFR,
HER2, and HER3, preventingligand binding to the receptors.
Furthermore, in this study weshow that Pan-HER more effectively
inhibits cell viability com-pared with trastuzumab alone in
parental cells, suggesting theincreased benefit of triple
inhibition of RTKs even in HER2-addicted cells. This concept is
reinforced in the NCI-N87 trastu-zumab-resistant cells, where
single RTK mAbs, cetuximab, tras-tuzumab, or pertuzumab, or dual
RTK inhibitor, lapatinib, had alimited effect compared with the
more powerful inhibitory effectof Pan-HER. Similar to our data, in
breast cancer xenografts withtrastuzumab resistance, Pan-HER, but
not trastuzumab emtan-sine (T-DM1) or the combination of
trastuzumab with pertuzu-mab or lapatinib, was able to arrest tumor
growth (33). In ourmodel, tumors derived from trastuzumab-resistant
cells did notcompletely recapitulate the in vitro resistant
phenotype after beinginoculated subcutaneously inmice. However,
after 1.5months of
treatment, these tumors were able to grow acquiring resistance
totrastuzumab. Differences between tumor cells behavior in
2Dcultures in vitro and in vivo exist even in terms of
proliferationrate (34). Now it is accepted that there are a number
of situationswhere a particular in vitro phenotype can only be
reproduced insolid tumors when cells have grown as 3D multicellular
tumorspheroids (35, 36). Moreover, resistance can even vary
whenresistant xenografts are reimplanted into untreated mice (37).
Inour resistant xenograft, trastuzumab resistance is not the result
ofa permanent genetic change in the tumor cells, but rather
ismediated by HER-family ligands upregulation. For this
reason,resistance could be affected by reversible changes that
likely tooccur in the tumor and/or its microenvironment. Therefore,
itmight explain thedelayed trastuzumab resistance
observed.Nota-bly, no tumor growth was observed under treatment
with Pan-HER during 3 months indicating the role of HER-family
ligandsand receptors in trastuzumab resistance.
In line with our results of downstream signaling activationunder
HER-family ligand stimulation, Wilson and colleaguesobserved that
EGF preferentially activated the MAPK/ERK path-way, whereas NRG1
mainly mediated PI3K/mTOR pathway acti-vation (30). This suggests
that dual activation of ERK1/2 and S6 inour gastric cancer
trastuzumab-resistant model may potentiallybe caused by a
combination of EGF, NRG1, or other HER ligandsupregulation.
Moreover, it supports the concept that extensiveredundancy
activation of RTKs signaling is observed in cancercells. RTKs
downstream activation including activation of thePI3K/mTOR
signaling pathway or the common-node SRC hasbeen linked to both
preclinical and clinical resistance toHER2-targeted therapy in
different cancer types (12, 26, 38–44).Similarly, in our gastric
cancer trastuzumab-resistant model,
Figure 6.
HER-family ligands increase after trastuzumab treatment in
clinical samples from patients with HER2-positive gastric cancer.
A, Scatter plot of EGF, AREG, andTGFa serum concentration from
paired pre- and post-trastuzumab samples from patients with
HER2-positive gastric cancer (n¼ 5) measured by ELISA. B, EGFmRNA
levels from FFPE tumor tissue from paired pre-trastuzumab and
post-trastuzumab samples (n¼ 3) by qRT-PCR (�� , P < 0.01).
HER-Family Ligands in Trastuzumab-Resistant Gastric Cancer
www.aacrjournals.org Mol Cancer Ther; 18(11) November 2019
2143
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/
-
MAPK/ERK and PI3K/mTOR activation was mediated byincreased SRC
phosphorylation, as a common node downstreamof RTKs ligand-induced
activation. Drug inhibition of SRC (orconcomitant inhibition of ERK
and PI3K) would therefore be agood therapeutic strategy to revert
trastuzumab resistance, asshown in our preclinical cell-culture
model. However, small-molecule inhibitors do not trigger the immune
system, whereasPan-HER induces ADCC and enhanced
complement-dependentcytotoxicity activation similar to trastuzumab
(13). Therefore,Pan-HER would be a more powerful clinical
therapeutic strategyto overcome trastuzumab resistance taking into
consideration theessential role of the immune system in cancer
therapy. Pan-HER isa promising candidate not only in reverting
resistance to trastu-zumab but also as a targeted therapy against
EGFR, HER2, orHER3. Clinical trials with Pan-HER are ongoing.
Taken together, the data presented herein suggests that
ligand-induced redundant activation of HER-family of receptors is
apotential mechanism of resistance to trastuzumab in gastriccancer,
supported by proof-of-concept evidence in a small cohortof
patients. Simultaneous inhibition of all members of the HER-family
of receptors is therefore necessary to revert or preventtrastuzumab
resistance. Potential clinical implications of ourfindings are (i)
the need to dynamically evaluate levels of HERligands before,
during, and after trastuzumab therapy and (ii) theneed to evaluate
Pan-HER as a potential therapeutic strategy toovercome trastuzumab
resistance in clinical trials.
Disclosure of Potential Conflicts of InterestB. Bellosillo has
received speakers bureau honoraria from Qiagen, Thermo
Fisher Scientific, and Hoffman-LaRoche. J. Albanell has received
speakersbureau honoraria from Roche, Amgen, Pfizer, and Novartis,
and has consul-tant/advisory board relationships with Roche,
Pfizer, and Amgen. C. Montagutreports receiving a commercial
research grant from Symphogen, has receivedspeakers bureau
honoraria fromRoche and Symphogen, and has an consultant/
advisory board relationship with Symphogen. No potential
conflicts of interestwere disclosed by the other authors.
Authors' ContributionsConception and design: A. Sampera, F.J.
S�anchez-Martín, C. MontagutDevelopment ofmethodology: A. Sampera,
O. Arpí, T.T. Poulsen, B. Bellosillo,C. MontagutAcquisition of data
(provided animals, acquired and managed patients,provided
facilities, etc.): A. Sampera, O. Arpí, L. Visa, M. Iglesias, S.
Clav�e,M. Gelabert-Baldrich, B. Bellosillo, C. MontagutAnalysis and
interpretation of data (e.g., statistical analysis,
biostatistics,computational analysis): A. Sampera, F.J.
S�anchez-Martín, O. Arpí, L. Visa,A. Dalmases, T.T. Poulsen, B.
Bellosillo, C. MontagutWriting, review, and/or revision of the
manuscript: A. Sampera, F.J. S�anchez-
Martín, L. Visa, �E. Gaye, T.T. Poulsen, M. Kragh, B.
Bellosillo, J. Albanell,A. Rovira, C. MontagutAdministrative,
technical, or material support (i.e., reporting or organizingdata,
constructing databases): S. Men�endez, S. Clav�e, M.
Gelabert-Baldrich,M. Kragh, J. Albanell, C. MontagutStudy
supervision: F.J. S�anchez-Martín, A. Rovira, C. Montagut
AcknowledgmentsThis work was supported by ISCiii (CIBERONC
CB16/12/00481, PIE15/
00008, PI18/00006, and PI18/00323), Generalitat de Catalunya
(2017 SGR507), andAECC (11964). C.Montagutwas supported
byDepartament de Salut,Generalitat deCatalunya (PERIS
SLT006/17/00055).MARBiobanc is supportedby ISCiii/FEDER
(PT17/0015/0011) and the "Xarxa de Bancs de tumors"sponsored by Pla
Director d' Oncologia de Catalunya (XBTC). We thankFundaci�o Cellex
(Barcelona) for a generous donation to Hospital del MarMedical
Oncology Service.
The costs of publicationof this articlewere defrayed inpart by
the payment ofpage charges. This article must therefore be hereby
marked advertisement inaccordance with 18 U.S.C. Section 1734
solely to indicate this fact.
Received May 2, 2019; revised July 28, 2019; accepted August 27,
2019;published first September 4, 2019.
References1. Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J, Jemal A. Global cancer
statistics, 2012. CA Cancer J Clin 2015;65:87–108.2. Bang YJ,
Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et
al.
Trastuzumab in combination with chemotherapy versus
chemotherapyalone for treatment of HER2-positive advanced gastric
or gastro-oesophageal junction cancer (ToGA): a phase 3,
open-label, randomisedcontrolled trial. Lancet 2010;376:687–97.
3. Tanner M, Hollm�en M, Junttila TT, Kapanen AI, Tommola S,
Soini Y, et al.Amplification of HER-2 in gastric carcinoma:
association with topoisom-erase IIalpha gene amplification,
intestinal type, poor prognosis andsensitivity to trastuzumab. Ann
Oncol 2005;16:273–8.
4. Gravalos C, JimenoA.HER2 in gastric cancer: a new prognostic
factor and anovel therapeutic target. Ann Oncol 2008;19:1523–9.
5. Yarden Y, SliwkowskiMX.Untangling the ErbB signalling
network. Nat RevMol Cell Biol 2001;2:127–37.
6. Genentech� 2019. FDA Approves Herceptin For HER2-Positive
MetastaticStomach Cancer [Internet]. Media/Press Releases. [cited
2019 Feb 4].Available from:
https://www.gene.com/media/press-releases/13007/2010-10-20/fda-approves-herceptin-for-her2-positive.
7. Junttila TT, Akita RW, Parsons K, Fields C, Lewis Phillips
GD, Friedman LS,et al. Ligand-independent HER2/HER3/PI3K complex is
disrupted bytrastuzumab and is effectively inhibited by the PI3K
inhibitor GDC-0941. Cancer Cell 2009;15:429–40.
8. Molina MA, Codony-Servat J, Albanell J, Rojo F, Baselga J.
Trastuzumab(Herceptin), a humanized anti-HER2 receptor monoclonal
antibody,inhibits basal and activated HER2 ectodomain cleavage in
breast cancercells. Cancer Res 2001;61:4744–9.
9. Clynes Ra, Towers TL, Presta LG, Ravetch J V. Inhibitory Fc
receptorsmodulate in vivo cytotoxicity against tumor targets. Nat
Med 2000;6:443–6.
10. Hudis CA. Trastuzumab–mechanism of action and use in
clinical practice.N Engl J Med 2007;357:39–51.
11. Piro G, Carbone C, Cataldo I, Di Nicolantonio F, Giacopuzzi
S, Aprile G,et al. An FGFR3 autocrine loop sustains acquired
resistance to trastuzumabin gastric cancer patients. Clin Cancer
Res 2016;22:6164–75.
12. Janjigian YY, Sanchez-Vega F, Jonsson P, ChatilaWK, Hechtman
JF, KuGY,et al. Genetic predictors of response to systemic therapy
in esophagogastriccancer. Cancer Discov 2018;8:49–58.
13. JacobsenHJ, Poulsen TT, Dahlman A, Kjær I, Koefoed K, Sen
JW, et al. Pan-HER, an antibody mixture simultaneously targeting
EGFR, HER2, andHER3, effectively overcomes tumor heterogeneity and
plasticity.Clin Cancer Res 2015;21:4110–22.
14. Pedersen MW, Jacobsen HJ, Koefoed K, Dahlman A, Kjaer I,
Poulsen TT,et al. Targeting three distinct HER2 domains with a
recombinant antibodymixture overcomes trastuzumab resistance. Mol
Cancer Ther 2015;14:669–80.
15. S�anchez-Martín FJ, Bellosillo B, Gelabert-Baldrich M,
Dalmases A,Ca~nadas I, Vidal J, et al. The first-in-class anti-EGFR
antibody mixtureSym004 overcomes cetuximab resistance mediated by
EGFR extracel-lular domain mutations in colorectal cancer. Clin
Cancer Res 2016;22:3260–7.
16. National Center for Biotechnology Information. PubChem
Database.Pimasertib, CID¼44187362 [Internet]. [cited 2019 Sep 6].
Available
from:https://pubchem.ncbi.nlm.nih.gov/compound/Pimasertib.
Mol Cancer Ther; 18(11) November 2019 Molecular Cancer
Therapeutics2144
Sampera et al.
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
https://www.gene.com/media/press-releases/13007/2010-10-20/fda-approves-herceptin-for-her2-positivehttps://www.gene.com/media/press-releases/13007/2010-10-20/fda-approves-herceptin-for-her2-positivehttps://www.gene.com/media/press-releases/13007/2010-10-20/fda-approves-herceptin-for-her2-positivehttps://pubchem.ncbi.nlm.nih.gov/compound/Pimasertibhttps://pubchem.ncbi.nlm.nih.gov/compound/Pimasertibhttp://mct.aacrjournals.org/
-
17. National Center for Biotechnology Information. PubChem
Database.Saracatinib, CID¼10302451 [Internet]. [cited 2019 Sep 6].
Availablefrom:
https://pubchem.ncbi.nlm.nih.gov/compound/Saracatinib.
18. Zazo S, Gonz�alez-Alonso P, Martín-Aparicio E, Chamizo C,
Crist�obal I,Arpí O, et al. Generation, characterization, and
maintenance of trastuzu-mab-resistant HER2þ breast cancer cell
lines. Am J Cancer Res 2016;6:2661–78.
19. O'Brien NA, Browne BC, Chow L, Wang Y, Ginther C, Arboleda
J, et al.Activated phosphoinositide 3-kinase/AKT signaling confers
resistance totrastuzumab but not lapatinib. Mol Cancer Ther
2010;9:1489–502.
20. MontagutC, Sharma SV, Shioda T,McDermottU,UlmanM,Ulkus LE,
et al.Elevated CRAF as a potential mechanism of acquired resistance
to BRAFinhibition in melanoma. Cancer Res 2008;68:4853–61.
21. Montagut C, Dalmases A, Bellosillo B, Crespo M, Pairet S,
Iglesias M, et al.Identification of a mutation in the extracellular
domain of the epidermalgrowth factor receptor conferring cetuximab
resistance in colorectal cancer.Nat Med 2012;18:221–3.
22. McDermott M, Eustace AJ, Busschots S, Breen L, Crown J,
Clynes M,et al. In vitro development of chemotherapy and targeted
therapy drug-resistant cancer cell lines: a practical guide with
case studies.Front Oncol 2014;4:40.
23. Bartley AN, Washington MK, Colasacco C, Ventura CB, Ismaila
N, BensonAB, et al. HER2 testing and clinical decision making in
gastroesophagealadenocarcinoma: guideline from the College of
American Pathologists,American Society for Clinical Pathology, and
the American Society ofClinical Oncology. J Clin Oncol
2017;35:446–64.
24. National Comprehensive Cancer Network, Inc. [Internet]. NCCN
Guide.Clin. Resour. [cited 2018 Jun 12]. Available from:
https://www.nccn.org/professionals/physician_gls/default.aspx.
25. Arena S, Bellosillo B, Siravegna G, Martínez A, Ca~nadas I,
Lazzari L, et al.Emergence of multiple EGFR extracellular mutations
during cetuximabtreatment in colorectal cancer. Clin Cancer Res
2015;21:2157–66.
26. Hong YS, Kim J, Pectasides E, Fox C, Hong S-W, Ma Q, et al.
Src mutationinduces acquired lapatinib resistance in
ERBB2-amplified human gastro-esophageal adenocarcinoma models. PLoS
One 2014;9:e109440.
27. Zheng L, Tan W, Zhang J, Yuan D, Yang J, Liu H. Combining
trastuzumaband cetuximab combats trastuzumab-resistant gastric
cancer by effectiveinhibition of EGFR/ErbB2 heterodimerization and
signaling. CancerImmunol Immunother 2014;63:581–6.
28. Li G, Zhao L, Li W, Fan K, Qian W, Hou S, et al. Feedback
activation ofSTAT3 mediates trastuzumab resistance via upregulation
of MUC1 andMUC4 expression. Oncotarget 2014;5:8317–29.
29. Ritter CA, Perez-TorresM,Rinehart C,GuixM,Dugger T, Engelman
JA, et al.Human breast cancer cells selected for resistance to
trastuzumab in vivooverexpress epidermal growth factor receptor and
ErbB ligands and remaindependent on the ErbB receptor network. Clin
Cancer Res 2007;13:4909–19.
30. Wilson TR, Fridlyand J, YanY, Penuel E, Burton L, Chan E, et
al.Widespreadpotential for growth-factor-driven resistance to
anticancer kinase inhibi-tors. Nature 2012;487:505–9.
31. Narayan M, Wilken JA, Harris LN, Baron AT, Kimbler KD,
Maihle NJ.Trastuzumab-induced HER reprogramming in "resistant"
breast carcino-ma cells. Cancer Res 2009;69:2191–4.
32. Yonesaka K, Zejnullahu K, Okamoto I, Satoh T, Cappuzzo F,
Souglakos J,et al. Activation of ERBB2 signaling causes resistance
to the EGFR-directedtherapeutic antibody cetuximab. Sci Transl Med
2011;3:99ra86.
33. Schwarz LJ, Hutchinson KE, Rexer BN, Estrada MV, Gonzalez
Ericsson PI,Sanders ME, et al. An ERBB1-3 neutralizing antibody
mixture with highactivity against drug-resistant HER2þ breast
cancers with ERBB ligandoverexpression. J Natl Cancer Inst
2017;109:1–10.
34. Ma Y, Lin Z, Fallon JK, Zhao Q, Liu D, Wang Y, et al.
Newmouse xenograftmodel modulated by tumor-associated fibroblasts
for human multi-drugresistance in cancer. Oncol Rep
2015;34:2699–705.
35. Langhans SA. Three-dimensional in vitro cell culture models
in drugdiscovery and drug repositioning. Front Pharmacol
2018;9:6.
36. Jaroch K, Jaroch A, Bojko B. Cell cultures in drug discovery
and develop-ment: the need of reliable in vitro-in vivo
extrapolation for pharmacody-namics and pharmacokinetics
assessment. J Pharm Biomed Anal 2018;147:297–312.
37. Zhang L, Bhasin M, Schor-Bardach R, Wang X, Collins MP,
Panka D, et al.Resistance of renal cell carcinoma to sorafenib is
mediated by potentiallyreversible gene expression. PLoS One
2011;6:e19144.
38. Gambardella V, Gimeno-Valiente F, Tarazona N,
Martinez-Ciarpaglini C,Roda D, Fleitas T, et al. NRF2 through RPS6
activation is related to anti-HER2 drug resistance in
HER2-amplified gastric cancer. Clin Cancer Res2019;25:1639–49.
39. Kataoka Y, Mukohara T, Shimada H, Saijo N, Hirai M, Minami
H.Association between gain-of-functionmutations in PIK3CA and
resistanceto HER2-targeted agents in HER2-amplified breast cancer
cell lines.Ann Oncol 2010;21:255–62.
40. Han S, Meng Y, Tong Q, Li G, Zhang X, Chen Y, et al. The
ErbB2-targetingantibody trastuzumab and the small-molecule SRC
inhibitor saracatinibsynergistically inhibit ErbB2-overexpressing
gastric cancer. MAbs 2014;6:403–8.
41. JinMH,NamAR, Park JE, Bang JH, Bang YJ, OhDY.
Resistancemechanismagainst trastuzumab in HER2-positive cancer
cells and its negation by Srcinhibition. Mol Cancer Ther
2017;16:1145–54.
42. Zhang S, Huang WC, Li P, Guo H, Poh SB, Brady SW, et al.
Combatingtrastuzumab resistance by targeting SRC, a common node
down-stream of multiple resistance pathways Siyuan. Nat Med
2011;17:461–70.
43. Berns K, Horlings HM, Hennessy BT, Madiredjo M, Hijmans EM,
Beelen K,et al. A functional genetic approach identifies the PI3K
pathway as a majordeterminant of trastuzumab resistance in breast
cancer. Cancer Cell 2007;12:395–402.
44. Díaz-Serrano A, Angulo B, Dominguez C, Pazo-Cid R, Salud A,
Jim�enez-Fonseca P, et al. Genomic profiling of HER2-positive
gastric cancer:PI3K/Akt/mTOR pathway as predictor of outcomes in
HER2-positiveadvanced gastric cancer treated with trastuzumab.
Oncologist 2018;23:1092–102.
www.aacrjournals.org Mol Cancer Ther; 18(11) November 2019
2145
HER-Family Ligands in Trastuzumab-Resistant Gastric Cancer
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
https://pubchem.ncbi.nlm.nih.gov/compound/Saracatinibhttps://www.nccn.org/professionals/physician_gls/default.aspxhttps://www.nccn.org/professionals/physician_gls/default.aspxhttps://www.nccn.org/professionals/physician_gls/default.aspxhttp://mct.aacrjournals.org/
-
2019;18:2135-2145. Published OnlineFirst September 4, 2019.Mol
Cancer Ther Aïda Sampera, Francisco Javier Sánchez-Martín, Oriol
Arpí, et al. in Gastric CancerHER-Family Ligands Promote Acquired
Resistance to Trastuzumab
Updated version
10.1158/1535-7163.MCT-19-0455doi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2019/09/04/1535-7163.MCT-19-0455.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/18/11/2135.full#ref-list-1
This article cites 40 articles, 15 of which you can access for
free at:
E-mail alerts related to this article or journal.Sign up to
receive free email-alerts
Subscriptions
Reprints and
[email protected]
To order reprints of this article or to subscribe to the
journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take
you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/18/11/2135To request
permission to re-use all or part of this article, use this link
on June 1, 2021. © 2019 American Association for Cancer
Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst September 4, 2019; DOI:
10.1158/1535-7163.MCT-19-0455
http://mct.aacrjournals.org/lookup/doi/10.1158/1535-7163.MCT-19-0455http://mct.aacrjournals.org/content/suppl/2019/09/04/1535-7163.MCT-19-0455.DC1http://mct.aacrjournals.org/content/18/11/2135.full#ref-list-1http://mct.aacrjournals.org/cgi/alertsmailto:[email protected]://mct.aacrjournals.org/content/18/11/2135http://mct.aacrjournals.org/
/ColorImageDict > /JPEG2000ColorACSImageDict >
/JPEG2000ColorImageDict > /AntiAliasGrayImages false
/CropGrayImages false /GrayImageMinResolution 200
/GrayImageMinResolutionPolicy /Warning /DownsampleGrayImages true
/GrayImageDownsampleType /Bicubic /GrayImageResolution 300
/GrayImageDepth -1 /GrayImageMinDownsampleDepth 2
/GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true
/GrayImageFilter /DCTEncode /AutoFilterGrayImages true
/GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict >
/GrayImageDict > /JPEG2000GrayACSImageDict >
/JPEG2000GrayImageDict > /AntiAliasMonoImages false
/CropMonoImages false /MonoImageMinResolution 600
/MonoImageMinResolutionPolicy /Warning /DownsampleMonoImages true
/MonoImageDownsampleType /Bicubic /MonoImageResolution 900
/MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000
/EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode
/MonoImageDict > /AllowPSXObjects false /CheckCompliance [ /None
] /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false
/PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000
0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true
/PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ]
/PDFXOutputIntentProfile (None) /PDFXOutputConditionIdentifier ()
/PDFXOutputCondition () /PDFXRegistryName () /PDFXTrapped
/False
/CreateJDFFile false /Description > /Namespace [ (Adobe)
(Common) (1.0) ] /OtherNamespaces [ > /FormElements false
/GenerateStructure false /IncludeBookmarks false /IncludeHyperlinks
false /IncludeInteractive false /IncludeLayers false
/IncludeProfiles false /MarksOffset 18 /MarksWeight 0.250000
/MultimediaHandling /UseObjectSettings /Namespace [ (Adobe)
(CreativeSuite) (2.0) ] /PDFXOutputIntentProfileSelector /NA
/PageMarksFile /RomanDefault /PreserveEditing true
/UntaggedCMYKHandling /LeaveUntagged /UntaggedRGBHandling
/LeaveUntagged /UseDocumentBleed false >> > ]>>
setdistillerparams> setpagedevice