Embed Size (px)
Citation preview

A publication of the National Herbalists Association of Australia
Volume 26 • Issue 1 • 2014
HerbalMedicine

Phone: 1300 265 662
Order Online: www.myintegria.com
Clinical Support: 1300 211 171
www.mediherb.com.au
Use Activated Beet-Greens daily as a supplementary food for:
Patients needing cardiovascular support
Athletes and active patients needing support for performance and stamina
Those not getting adequate nutrition through their diet
Patients needing detoxification support
Patients interested in health maintenance protocols
MH1AB240 240 g $42.00 ex GST
Activated Beet-Greens
Professionally Recommended Concentrated Nutrition
At the core of many modern health problems is poor nutrition. As health care
practitioners, we know that importance of good nutrition but it can be difficult for
many patients to achieve due to their busy lifestyles.
Activated Beet-Greens contains a high dose of Beetroot containing nitrate, a high quality greens blend of Chlorella,
Spirulina and Kale, a high quality fruit blend of Blueberry, Acerola Cherry, Kiwifruit, Grape Seed and Blackcurrent
together with MediHerb quality herbs to provide a comprehensive nutritional support that will be a welcome
addition to many of your existing protocols.
Try it in your clinic today!

Quality Holistic Healthcare based on Scientifi c Research
In the fi eld of Nutritional and Natural medicines, InterClinical Laboratories is one of Australia’s leading practitioner aligned companies.
We aim to improve and make a difference in people’s lives by delivering high quality and trusted healthcare solutions based on scientifi c evidence.
InterClinical Laboratories has a passion for health and our enthusiasm and belief in a natural, holistic approach to health inspires us to excellence in everything we do.
We do not compromise our integrity or honesty and are committed to achieving the highest possible standards personally, professionally and as a business.
We offer a range of advanced and original supplements that are formulated by a local and international team of skilled researchers, practitioners and technicians in the fi elds of complementary, herbal and nutritional medicine.
We pride ourselves on the purity of our formulations, ensuring each product is created from high quality, bio-available, easily digested ingredients.
InterClinical Laboratories is an Australian owned company and all our natural, herbal and nutritional products are proudly Australian made.
Some features that make our range unique…
• Advanced formulations• Helps restore and maintain balanced
nutrient levels in the body• Support detoxifi cation processes and
assist in chelating toxic minerals and heavy metals
• Low allergenic, vegan-friendly• Extensive selection of elemental mineral
formulations including specialty minerals, such as copper, manganese, chromium and molybdenum
• Specialty multi-nutrient packs supporting bio-individuality
• Synergistic formulas• Evidence-based formulations• Optimum dosages, not mega-dosages• Full technical and advisory service from
helpful and friendly InterClinical staff
the highest possible standards personally, professionally and as a business.
We offer a range of advanced and original supplements that are formulated by a local and international team of skilled researchers, practitioners and technicians in the fi elds of complementary,
heavy metals
Advanced natural, nutritional and herbal formulations recommended by Professionals
INT058_Healthco_as.indd 1 3/08/11 5:02 PM

The Australian Journal of Herbal Medicine is a quarterly publication of the National Herbalists Association of Australia. The Journal publishes material on all aspects of western herbal medicine and is a peer reviewed journal with an Editorial Board.
Members of the Editorial Board are:
Jane Frawley MClinSc BHSc(CompMed) DBM GradCertAppSc
Katoomba NSW Australia
Stuart Glastonbury MBBS BSc(Med) DipWHM Newcastle NSW Australia
Erica McIntyre BSocSc(Psych)(Hons) BHSc DipBM Blackheath NSW Australia
Andrew Pengelly PhD BA DBM ND Laurel Maryland United States of America
Amie Steel PhD, MPH, GradCertEd, ND Brisbane Queensland Australia
Janelle Wheat PhD MMedRadSc(Nuclear Medicine) MHSc(herbal medicine) BAppSc(ra-diography) Wagga Wagga NSW Australia
Dawn Whitten BNat Hobart Tasmania Australia
Hans Wohlmuth PhD BSc Ballina NSW Australia
The Editorial Board advises on content, structure and standards for the Journal, keeping it relevant to the profession of herbal medicine. Peer reviewers will come from the Editorial Board as well as being sourced globally for their expertise in specific areas. Contributions are invited to the journal.
Aim & scopeThe Australian Journal of Herbal Medicine (AJHM) is Australia’s leading herbal publication. A thoroughly modern, peer reviewed and clinically relevant journal, the AJHM can trace its origins back to publications issued by the Association as long ago as the 1930s. Issued quarterly, the AJHM publishes material on all aspects of herbal medicine including philosophy, phytochemistry, pharmacology and the clinical application of medicinal plants.
Editorial policy• Subject material must relate to herbal medicine.• Accepted articles become the property of the NHAA.• Contributions are subject to peer review and editing.• Contributions to the Australian Journal of Herbal Medicine must not be submitted
elsewhere.
Advertising For advertising enquiries please contact the NHAA office on telephone (02) 8765 0071, fax (02) 8765 0091 email [email protected] or visit www.nhaa.org.au / Publications and Products / AJHM
Publisher: NHAA
Postal Address: Office Manager PO Box 45 Concord West NSW 2138
Follow us on facebook:www.facebook.com/pages/Australian-Journal-of-Herbal-Medicine/1416725668550367
Twitter: www.twitter.com/TheNHAA
Editor: Jane FrawleyEmail: [email protected]: +61 (0) 2 8765 0071Fax: +61 (0) 2 8765 0091Email: [email protected]: www.nhaa.org.au
Editorial Committee: Erica McIntyre (Blackheath NSW) Jane Frawley (Katoomba NSW)
Proofreaders: Greg Whitten (Hobart TAS) Kath Giblett (Perth WA)
The National Herbalists Association of Australia (NHAA) was founded in 1920 and is Australia’s oldest professional association of complementary therapists. The NHAA is a non-profit, member based association run by a voluntary board of directors and assisted by interested members. Representing Western herbalists and naturopaths, the NHAA is the only national professional association specifically concerned with the practice and education of Western herbal medicine (WHM) in Australia. Our mission is to serve and support our membership and promote and protect the profession and practice of Western herbal medicine and naturopathy.
national herbalists association of australia
ISSN 22003886 ABN 25 000 009 932 PP 23692/00006
HerbalMedicine
AustralianJournal
of
© NHAA 2014. All rights reserved. No part of this publication may be reproduced or utilised in any form whatsoever without prior written permission from the NHAA. All advertising is solely intended for the information of members and is not endorsed by the NHAA. The NHAA reserves the right to determine journal content. The views in this publication are those of the authors and may not reflect the view of the NHAA. The NHAA does not have the resources to verify the information in this publication and accepts no responsibility whatsoever for the application in whatever form of information contained in this publication.

Editorial . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Jane Frawley
CommentaryAntioxidants to abrogate free radicals: new insights to challenge currently held beliefs . . . . . . 4Janet M Schloss, Luis Vitetta
The decline of herbal medicine/naturopathy consultations: how research can help further the profession . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8David Sibbritt
ArticlesCarrot seed for contraception: a review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Gabrielle Claire Jansen, Hans Wohlmuth
Crocus sativus (saffron): a monograph . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Kaye Wright
Evaluation of the antioxidant activity and additive effects of traditional medicinal herbs from Sri Lanka . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Viduranga Y. Waisundara, Mindani I. Watawana
Case study
The integrated treatment of Blastocystis hominis in a patient with ulcerative colitis: a case study . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29Susan Hunter
MedplantCaper berry in the treatment of type 2 diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Panax quinquefolius in diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34Berberine in periodontal disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Can a memo help jog the memory? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35Disease-modifying potential of Cinnamon extract in inflammation and arthritis . . . . . . . . . . . . . . . . 36Warming yang and replenishing the kidney to treat cold-induced asthma . . . . . . . . . . . . . . . . . . . . . 37Dietary flaxseed has pronounced antihypertensive effect . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
MedjournNon-Coeliac Wheat Sensitivity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39Perinatal air pollution exposure and autism spectrum disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Effect of prebiotic and probiotic supplementation on fussiness and crying in the preterm infant . . . . 40Watermelon as a recovery aid for athletes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41Dietary interventions for prevention of gestational diabetes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42Micronutrient supplementation in HIV patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Apples and statins go head to head . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43Proton pump inhibitors associated with vitamin B12 deficiency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
AJHM based CPE questionnaire . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
CONTENTS

Australian Journal of Herbal Medicine 2014 26(1)
2 © National Herbalists Association of Australia 2014
Editorial
Welcome to the first edition of the Australian Journal of Herbal Medicine for 2014. This edition contains a commentary by Professor David Sibbritt on the decline of herbal medicine/naturopathic consultations by women despite the increase in use of herbal medicines and other complementary medicine products.1 Women are high consumers of complementary and alternative medicine (CAM) and this use appears to extend to pregnancy. A recent, nationally representative study of pregnant women in Australia (n=1,835) found that 52% of women were using some form of CAM during gestation (excluding vitamins and minerals which are commonly taken at this time).2 This is very similar to the prevalence rates of CAM use during pregnancy from other countries around the world with most falling between 20 and 60%.3 Of these therapies, herbal medicines have been found to be used commonly during gestation.
A study published last month in BMC Complementary and Alternative Medicine investigated the use of herbal medicine by pregnant women (n=9,459) across 23 countries.4 They found the use ranged from 4.3% in Sweden up to 69% in Russia. Additionally, Australia was found to have the third highest rate of herbal medicine use during pregnancy (43.8%). This is relatively consistent with prevalence rates reported from Australian studies which have revealed that between 11% and 36% of women are using herbal medicine during gestation.2, 5-7
Women appear to use herbal medicine during pregnancy due to the perception that it may be safer than conventional medicine and due to a desire for a more holistic model of healthcare.8,9 Women also report that they want a degree of choice and control in some of their healthcare decisions during pregnancy.8 The self-prescribing of herbal medicines during pregnancy may be an extension of a woman’s desire for some degree of autonomy during this time. A recent Australian study found that 34.4% of women were using herbal medicines during pregnancy and only 7.2% were consulting a naturopath or herbalist.2,10 High rates of herbal medicine self-prescription appear to be common in Australia with another study reporting up to 71% of women who use herbal medicine during pregnancy self-prescribe them.4 Whilst some herbal medicines may be innocuous,
the safety of many during pregnancy is unknown.11 Additionally, women may have an inadequate knowledge of herbal medicines that are considered harmful in pregnancy, may choose poorly or incorrectly, or may not be aware that these medicines can interact with other medications. In addition to concerns about teratogenicity and effects on uterine activity, there is the possibility that a chronic or pregnancy-related health condition may be undertreated leading to a worsening of the complaint or further complications.9
Research has also shown that pregnant women tend to seek information about the use of herbal medicine from unprofessional and informal information sources such as untrained friends and family. 3,4,9,12,13 Kennedy et al found that most women who used herbal medicine did so by their own initiative or sought advice from family and friends without consulting naturopaths, herbalists or maternity health care professionals;3 a finding that has commonly been reported in other research.3,9,12,13 If many women are using herbal medicines during pregnancy and the majority are seeking advice from family, friends and informal sources such as the internet and magazines, concern is warranted that women may receive poor quality advice that may compromise their health or the health of their baby.
It is not known how many Australian women disclose their use of herbal medicine to their maternity healthcare provider. Research from other countries has shown that the disclosure rate is generally poor8,14 with one study reporting that 76% of pregnant women did not tell their midwife or doctor they were using herbal medicine.15 Sometimes the lack of disclosure is simply because women are not being asked,16 however it also appears to be due to concerns about receptivity and the possibility of feeling disparaged.14 There has also been research presented previously in this journal17 which identified a lack of communication between maternity health professionals and naturopaths or herbalists contributing further to this gap in public safety. Research conducted in other patient cohorts in Australia18 has shown that many people do not disclose their use of herbal medicines and it is possible that this may also be the case during pregnancy. As Australian women are commonly utilising herbal medicines during
Jane Frawley Editor, Australian Journal of Herbal Medicine PO Box 45 Concord West 2138 [email protected]
Editorial: Herbal medicine use in pregnancy by Australian women: high rates of self-prescription and low rates of disclosure?

Australian Journal of Herbal Medicine 2014 26(1)
3© National Herbalists Association of Australia 2014
Editorial
pregnancy it is important to examine why women are largely self-prescribing and why consultations with herbalists and naturopaths are declining despite the growth in popularity of these medicines.1 Research is required to examine women’s attitudes towards the use of herbal medicine during pregnancy and the disclosure of this use to maternity health care professionals in order to ensure safe maternal and child outcomes.
References1. Sibbritt D. 2014. The decline of herbal medicine/naturopathy
consultations: how research can help further the profession. Aust J Herb Med 26(1): 8-9, 38.
2. Frawley J, Adams J, Sibbritt D, Steel A, Broom A, Gallois C. 2013. Prevalence and determinants of complementary and alternative medicine use during pregnancy: Results from a nationally representative sample of Australian pregnant women. Aust N Z J Obstet Gynaecol 53(4): 347-52.
3. Adams J, Lui CW, Sibbritt D, Broom A, Wardle J, Homer C, Beck,S. 2009. Women’s use of complementary and alternative medicine during pregnancy: a critical review of the literature. Birth 36(3):237-45.
4. Kennedy DA, Lupattelli A, Koren G, Nordeng H. 2013. Herbal medicine use in pregnancy: results of a multinational study. BMC Complement Altern Med 13:355.
5. Forster DA, Denning A, Wills G, Bolger M, McCarthy E. 2006. Herbal medicine use during pregnancy in a group of Australian women. BMC Pregnancy Childbirth 6:21.
6. Skouteris H, Wertheim EH, Rallis S, Paxton SJ, Kelly L, Milgrom J. 2008. Use of complementary and alternative medicines by a sample of Australian women during pregnancy. Aust N Z J Obstet Gynaecol 48(4):384-90.
7. Gaffney L, Smith C. 2004. The views of pregnant women towards the use of complementary therapies and medicines. Birth Issues
13:43–50.8. Warriner S, Bryan K, Brown AM. 2014. Women’s attitude towards
the use of complementary and alternative medicines (CAM) in pregnancy. Midwifery 30(1):138-43.
9. Nordeng H, Havnen GC. 2004. Use of herbal drugs in pregnancy: a survey among 400 Norwegian women. Pharmacoepidemiol Drug Saf 13(6):371-80.
10. Steel A, Adams J, Sibbritt D, Broom A, Gallois C, Frawley J. 2012. Utilisation of complementary and alternative medicine (CAM) practitioners within maternity care provision: results from a nationally representative cohort study of 1,835 pregnant women. BMC Pregnancy Childbirth 12:146.
11. Low Dog T. 2009. The use of botanicals during pregnancy and lactation. Altern Ther Health Med 15(1):54-8.
12. Hall HG, Griffiths DL, McKenna LG. 2011. The use ofcomplementary and alternative medicine by pregnant women: a literature review. Midwifery 27(6):817-24.
13. Pettigrew AC, King MO, McGee K, Rudolph C. 2004. Complementary therapy use by women’s health clinic clients. Altern Ther Health Med 10(6):50-5.
14. Harrigan JT. 2011. Patient disclosure of the use of complementary and alternative medicine to their obstetrician/gynaecologist. J Obstet Gynaecol 31(1):59-61.
15. Holst L, Wright D, Haavik S, Nordeng H. 2009. The use and the user of herbal remedies during pregnancy. J Altern Complement Med 15(7):787-92.
16. Furlow ML, Patel DA, Sen A, Liu JR. 2008. Physician and patient attitudes towards complementary and alternative medicine in obstetrics and gynecology. BMC Complement Altern Med 8:35.
17. Diezel, H, A Steel, J Wardle, and K Johnstone. 2013. Patterns and influences of interprofessional communication betweenmidwives and CAM practitioners: a preliminary examination of the perceptions of midwives. Aust J Herbal Med 25(1): 4-10.
18.Shorofi SA, Arbon P. 2010. Complementary and alternativemedicine (CAM) among hospitalised patients: an Australian study. Complement Ther Clin Pract 16(2):86-91.
2014 NHAA Membership Rates SPECIALSJoin now as a Full Member and get 50% off
your membership fee in the year that you join!(NB: Offer can only be used once and applies to full or pro-rata rate for the calendar year in which you join .)
JOIN NOW AS A FULL MEMBER WITHIN 12 MONTHS OF GRADUATING:• Get 50% off your membership fee in the year that you join; AND
• Get 25% off your membership fee in the following year!(NB: Offer can only be used once. 50% discount applies to full or pro-rata rate for the calendar year in which you join.)
Student membership in your final year of study is now FREE, for current members and new members joining us in their final year .
(NB. This offer can only be used once and applies to the last calendar year that you are a student, or part thereof if joining part way through the year.)
Our membership year operates on a calendar year. Rates vary between membership categories, with pro-rata rates available depending on what month you join.
For details go to www .nhaa .org .au and click on JOIN .

Australian Journal of Herbal Medicine 2014 26(1)
4 © National Herbalists Association of Australia 2014
Commentary
IntroductionAntioxidant supplements are among the most popular
health products in the world and one of the highest selling items without the requirement of a prescription.1 The reason for this influx of market value is largely due to in vitro research conducted on free radicals and the suggested benefits from antioxidant compounds in abrogating the over-production of free radicals. There has been a plethora of investigations on antioxidants and the rescuing of the purported oxidative damage to macromolecules that ensues. The conclusions emanating from in vitro and in vivo experimental models have no relevance to normal physiological function and therefore no relevance to the risk of developing a chronic disease or affecting the aging process.2 Hydrogen peroxide is the stand out substance employed in such investigations, with thousands of articles in the medical and scientific literature reporting it as causal for macromolecular damage and severe cellular toxicity. The demonstration of cellular toxicity is based on employing hydrogen peroxide levels that far exceed those observed under normal physiological conditions, otherwise it is cited that at lower levels the phenomenon is not detectable.3 The hypothesis that justifies this phenomenon is that the high levels of hydrogen peroxide are requisite in order to
demonstrate the toxic effect that hydrogen peroxide has on cells. Additional experiments investigating the levels of cellular catalase and glutathione peroxidase, which function to regulate the level of hydrogen peroxide, further postulate that these enzyme systems prevent the cellular damage that hydrogen peroxide may cause. In contrast to this, hydrogen peroxide is not a toxic compound at physiological levels.4
The human metabolome is an expression of a finely tuned dynamic equilibrium which is comprised of thousands of anabolic and catabolic reactions, and all cellular systems are finely regulated. However, there is no perfect machine and malfunctions can occur.4 If there is a small inappropriate leakage of ‘free radicals’, the mitochondria or cell can be damaged and will go into apoptosis (cell death) and cannot continue to function in a compromised state as suggested by some authors.5,6 Currently, there are no blinded human clinical trials establishing excessive systemic over-production of reactive oxygen species as the primary cause of aging or associated diseases.4
Commentary Recently, the antioxidant–free radical theory of
chronic disease and aging has been challenged.4 It
Antioxidants to abrogate free radicals: new insights to challenge currently held beliefs
Janet M Schloss 1, Luis Vitetta 1,2
1 The University of Queensland, School of Medicine, Level 5, TRI, Princess Alexandra Hospital, Ipswich Road, Woolloongabba, Brisbane, Australia 4102.2 Medlab, Sydney, Australia 2015.Correspondence: Ms Janet Schloss, The University of Queensland, School of Medicine. Level 5, TRI, Princess Alexandra Hospital, Ipswich Road, Woolloongabba, Queensland, Australia 4102Email: [email protected]
Abstract: Compounds found in foods, nutrients and herbs commonly defined as antioxidants have been posited to neutralise free radicals produced by cellular oxidation reactions in the hope of ameliorating symptoms of chronic diseases. It has been reported that the body can function effectively with low levels of free radicals but if there is an overload of reactive oxygen species (ROS) and/or reactive nitrogen species (RNS) that there is an increased risk for heart disease, cancer, and other chronic diseases. However, physiologically, the idea of neutralising a free radical with an antioxidant is very much a chimera. Five decades of in vitro and in vivo investigations on antioxidants and free radicals with no proven mechanistic understanding has confused researchers, antioxidant compound manufacturers and the public. This commentary advances a biochemical understanding as to the antioxidant / free radical connection that runs counter to decades of research dogma. The notion that an over production of free radicals such as superoxide anions and hydrogen peroxide are deleterious to health by causing cellular damage is not proven. The increased risk for chronic diseases and the aging process due to an overload of intracellular free radicals is untenable and challenged. These compounds are required for normal cellular function. Furthermore, as an example, we cite vitamin C, the bastion of the antioxidant library of molecules, as anything but an antioxidant in vivo. Vitamin C is an essential co-enzyme and plays an oxido-reductase role in the hydroxylations of, for example, pro-collagen.
Keywords: Antioxidant, free radical, oxidative damage, reactive oxygen species (ROS), reactive nitrogen species (RNS)

Australian Journal of Herbal Medicine 2014 26(1)
5© National Herbalists Association of Australia 2014
Commentary
has been posited that an industry has been built on the proposition that it is essential to prevent oxidative damage by administering small molecules designated as antioxidants for the amelioration of the aging process and treatment of chronic diseases. However there is no compelling evidence from human clinical trials to support this contention.4,7,8
Harman9 in 1956 hypothesized that free radical production (oxygen radical formation) was a major deleterious contributor to the aging process and degenerative disease due to its attack on cell constituents (macromolecules such as DNA and proteins) and connective tissue. The hypothesis that free radicals were causal for oxidative damage received strong support from an extensive set of experiments. Boveris and Chance10 in 1973 demonstrated that large amounts of superoxide anions were generated by the mitochondrial electron transport chain during the oxidative phosphorylation phase of the Kreb’s cycle, whereby complex I and II reduced coenzyme Q10 and its oxidation by complex III. Chance et al.,11 in 1979, then estimated that 1-3% of inspired oxygen was converted to reactive oxygen species (ROS), which would indeed be toxic to cells. Chance’s experiments, however, were contradicted when Staniek and Nohl12 (2000) and St-Pierre et al.,13 (2002) demonstrated that intact normally respiring mitochondria do not produce high concentrations of ROS and that the earlier extrapolations of superoxide anion and hydrogen peroxide were over-estimated by several orders of magnitude. Therefore, the high amounts of ROS were not produced in physiologically normally respiring human mitochondria and that the human cellular metabolome tightly regulates the production of ROS/ RNS. This indicated that oxidative damage did not occur unless the system was induced to do so in a non-physiological environment.
In a recent review by Tobe14 (2013), investigations on mitochondrial dysfunction and oxidative damage in major depressive disorder were discussed. The human studies described were based on brain imaging captured via magnetic resonance imaging (MRI) and post mortem histologic studies. Tobe14 suggested that the decreased size of the brain, decreased glial cell density and neuronal size linked with major depressive disorder, biopolar or schizophrenia were due to oxidative stress. There was no scientific or mechanistic explanation that confirmed this suggestion. The basis of the discussion was cited to animal studies, which had established a non-physiological environment that was causal for increased ROS production, inhibition of mitochondrial respiration and oxidative DNA damage.15-17 Such investigations reinforce and reiterate that oxidative damage does not occur under normal physiological conditions The cellular damage alluded to in these investigations occurs in a set of experiments with induced abnormal productions of ROS / RNS.
Additional recent experiments by Villanueva and Kross18 have questioned the role of antioxidant supplementation, suggesting a hypothesis that supplementation of antioxidants may cause antioxidant-induced stress whereby antioxidants overwhelm the body’s free radical production. Many investigators report benefits of antioxidant administration; however, there are only a few that question the possible harmful effects.18
Free radicals have been designated as largely harmful and thus having a negative impact on cellular metabolism and mitochondria, and being causal for macromolecular oxidative damage.19 It is posited that ROS and RNS participate in specific functions and play an important role in signal transduction in many physiological events. For example, ROS and RNS play a significant role in signal transduction of cytokine receptors, tyrosine receptors, serine/threonine kinases, G protein-coupled receptors, ion-channel linked receptors in response to angiotension II, cytokines, glutamate, epidermal growth factor, vascular endothelial growth factor, tumour necrosis factor α and platelet derived growth factor.18,19
Furthermore, hydrogen peroxide is a known mitogen.4
Villanueva and Kross18 (2012) form the argument that excess consumption of administered antioxidants can overwhelm the cellular function of ROS / RNS and therefore decrease their biological function within cells. This deleterious action then goes on to interfere with the normal cellular processes by disrupting biochemical and physiological activity required for normal cellular function. They list nine trials indicating no effect from antioxidant supplementation and six trials that found harmful effects from antioxidant supplementation versus twelve that report benefit.18 This body of evidence then raises the query as to antioxidant supplementation benefits versus safety.
The question may not only be if antioxidant supplementation is beneficial or detrimental but whether there is an antioxidant effect. What has been found is that antioxidants referred to in the literature are also pro-oxidants, inducing the formation of hydrogen peroxide, a necessary biochemical requisite for optimal cellular function. It would hence seem that antioxidants may promote healthy cellular metabolism by providing an oxido-reductase action.
An example of this is coenzyme Q10, which is a key component in the oxidative phosphorylation section of energy production and electron transport chain as well as other organelle oxido-reductase activity.4 Coenzyme Q10 has been labelled as a strict antioxidant; however, it also has a pro-oxidant function through the formation of superoxide anion and hydrogen peroxide that is a major factor in its beneficial mode of activity.8
ConclusionThe canon belief that the production of ROS and
RNS leads to random deleterious modification of

Australian Journal of Herbal Medicine 2014 26(1)
6 © National Herbalists Association of Australia 2014
Commentary
macromolecular species, mitochondria and cellular metabolism, and that oxidative damage is a major contributor to aging and related systemic diseases is untenable. Furthermore, the administration of antioxidants such as vitamin A, C, E, compounds found in herbs or coenzyme Q10 that can ameliorate oxidative stress is flawed. ROS and RNS are products of normal cellular metabolism and are necessary for normal physiological functioning of the organism. This process is tightly regulated by hormones, cytokines and other mechanisms. Antioxidants can also act as pro-oxidants (e.g. ascorbate), therefore readdressing the action of these molecules to oxido-reductase molecules may serve researchers with a more appropriate mode of action for further investigations of efficacy.
The antioxidant compounds marketed still play a vital role and should be included in a prescription of health. Further clinically relevant research is required that takes into consideration that the evolutionary progression of humans has become dependent upon the production of ROS and RNS. Reassessment of the antioxidant theory and a new paradigm of thinking are certainly required.
References1. Choices. 2011. Supplements who needs them? NHS. June: 1-33.2. Linnane AW. 2010. My life as a biochemist and molecular
biologist. IUBMB Life. 62(7):527-30.3. Saeidnia S, Abdollahi M. 2013. Toxicological and pharmacological
concerns on oxidative stress and related diseases. Toxicol Appl Pharmacol. In press: doi: 10.1016/j.taap.2013.09.031.
4. Linnane AW, Kios M, Vitetta L. 2007. Healthy aging: Regulation of the metabolome by cellular redox modulation and prooxidant signaling systems: The essential roles of superoxide anion and hydrogen peroxide. Biogerontology 8(5): 445-467.
5. Parikh SM. 2013. Therapeutic targeting of the mitochondrial dysfunction in septic acute kidney injury. Curr Opin Crit Care In Press: DOI:10.1097/MCC.0000000000000038
6. Muyderman H, Chen.T. 2013. Mitochondrial dysfunction in ALS - a valid pharmacological target? Br J Pharmacol In Press: doi: 10.1111/bph.12476.
7. Linnane AW, M. Kios, Vitetta L. 2007. The essential requirement for superoxide radical and nitric oxide formation for normal physiological function and healthy aging. Mitochondrion 7(1-2):1-5.
8. Linnane AW, Kios M, Vitetta L. 2007. Coenzyme Q(10) - its role as a prooxidant in the formation of superoxide anion/hydrogen peroxide and the regulation of the metabolom. Mitochondrion 7:S51-61.
9. Harman D. 1956. Aging: a theory based on free radical and radiation chemistry. J Gerontol 11(3):298-300.
10. Boveris A, Chance B. 1973. The mitochondrial generation of hydrogen peroxide. General properties and effect of hyperbaric oxygen. Biochem J 134(3):707-16.
11. Chance B, Sies H, Boveris A. 1979. Hydroperoxide metabolism in mammalian organs. Physiol Rev 59(3):527-605.
12. Staniek K, Nohl H. 2000. Are mitochondria a permanent source of reactive oxygen species? Biochim Biophys Acta 460(2-3):268-75.
13. St-Pierre J, Buckingham JA, Roebuck SJ, Brand MD. 2002. Topology of superoxide production from different sites in the mitochondrial electron transport chain. J Biol Chem 277(47):44784-90.
PUSHPUSHPPPUUUSSSHHHPUSH
Recurring cystitis? Run for Ellura
flordis.com.au Warning: Blood in the urine warrants immediate medical attention. *Based on independent testing of PAC validated by BL-DMAC, and anti-adhesion activity, in 10 of the leading commercially available cranberry supplements (evaluated by Aztec value 11/03/2012). References: 1. Howell AB. Whole Product Anti-Adhesion Activity Report. Rutgers University. 2011. 2. Howell AB. Whole Product Anti-Adhesion Activity Report. Rutgers University. 2013. 3. Agrobio Laboratories, Report on proanthocyanidins of commercially available products. 2013. 4. Howell AB, et al. BMC Infectious Diseases. 2010;10:94. 5. Botto & Neuzillet. Scand J Urol Nephrol. 2010;44:165-8. ElluraTM is a trademark of Pharmatoka.
When recurrent cystitis strikes, no other cranberry supplement* works as effectively as new, fast-acting Ellura.1,2 Because only Ellura provides the clinically proven effective daily dosage of 36mg* bioactive proanthocyanidins (PACs) in each capsule.3,4
Ellura’s unique, high strength formulation is clinically proven to:• inhibit E. coli from adhering to the urinary
tract walls4
• flush away bacteria naturally5
Recommend once-daily Ellura to reduce the frequency of recurrent cystitis and to promote naturally better urinary tract health.
NEW
References continued on page 33

Australian Journal of Herbal Medicine 2014 26(1)
7© National Herbalists Association of Australia 2014
venu
es&
dat
es
WHY YOU NEED TO ATTEND THIS EVENT.
APRIL TO MAY 2014
There's an event venue near you!
your presenters
At Metagenics Best Practice you will learn:• How to set up systems in your clinic for optimal organisation and success.• How to set up and run success-focussed appointments that get great results, encourage compliance and
keep your patients coming back.• Tools and techniques that Metagenics offers that will support you in improving the way you practice; effectively
helping you to have the Best Practice.• How to use the tips and ideas in this event as a springboard to launch your own success!
Your Investment: $99.00 incl. GST
YOUR INVESTMENT:
ALL EVENT TIMES
Registration: 9:00 to 9:30 amStart Time: 9:30 amMorning Break: 11:00 to 11:20 amLunch Break: 1:00 to 2:00 pmConclusion: 4:15 pm
Book now! Call 1800 777 648.Metagenics reserves the right to refuse entry to any person, or competitor, or employee thereof. No tape recorders or video cameras allowed within any venue.
Angela CarrollAdvDipHSc(Nat), AdvDipHSc(Acu), DipHM, NCFM, AdvDipBus
Erica Smith BSc(CompMed), AdvDipNat, AdvDipHerbMed
Dr Damian Kristof BChiro, ND
How to Run a SuccessfulNatural Medicine Clinic.
“An essential event for every Practitioner to build a profitable and effective practice” Naturopath, Sydney
“The most valuable Metagenics event yet - should be taught at college”
Naturopath, Brisbane
MET3653 - 01/14
Adelaide Tuesday 29th April Stamford Plaza Adelaide 150 North Terrace, Adelaide
Perth Thursday 1st May Novotel Langely 221 Adelaide Terrace, Perth
Auckland Monday 5th May Novotel Ellerslie 72 - 112 Greenlane East, Ellerslie
Melbourne Wednesday 7th May Hilton on the Park Melbourne 192 Wellington Parade, Melbourne
Brisbane Monday 12th May Pullman Brisbane King George Square Corner of Ann & Roma Streets, Brisbane
Sydney Wednesday 14th May Novotel Sydney Olympic Park Olympic Boulevard, Sydney Olympic Park

Australian Journal of Herbal Medicine 2014 26(1)
8 © National Herbalists Association of Australia 2014
Commentary
At present there is much debate within the herbal medicine/naturopathy professions as to the merits of registration.1,2 Further, there is a history of division within the professions of herbal medicine and naturopathy in relation to different models of regulation.3 So, with much energy devoted to these emotive issues, it is not surprising that a relatively small amount of research is being conducted by herbalists/naturopaths – resulting in the general public and other healthcare providers knowing little of the daily practice activities of herbalists/naturopaths, as well as the health benefits that can be gained by consulting these practitioners.
In contrast to the herbal medicine/naturopathy professions, other complementary and alternative medicine (CAM) practitioner professions, including chiropractors, acupuncturists, and traditional Chinese medicine practitioners, have made the decision to be, and are now registered with, the National Registration and Accreditation Scheme. In addition, other CAM practitioner professions have made a considerable effort to increase research activities. For example, the Chiropractic Association of Australia (CAA) has recently committed nearly $500,000 to research by contracting the Australian Research Centre in Complementary and Integrative Medicine (ARCCIM) to establish the Australian Chiropractic Research Network (ACORN) project. The aim of the ACORN project is to build a critical, scientifically rigorous assessment of chiropractic care. Meanwhile, there is emerging evidence of the efficacy of some CAM therapies for the treatment of certain symptoms, such as acupuncture for the treatment of chronic knee pain4 and massage for the relief of treatment-related side effects of breast cancer.5 It is of little surprise then that evidence is emerging that the herbalist/naturopathy profession is in decline while other CAM professions are on the increase.
The Australian Longitudinal Study on Women’s Health (ALSWH) is a large (n>40,000), nationally-representative cohort of women who were recruited in 1996 and surveyed regularly to this day (http://www.alswh.org.au). The questionnaires used in the ALSWH contain items on the women’s consultations with
common CAM practitioners as well as their use of over-the-counter products. Analyses of these data reveal some alarming trends for the herbalist/naturopath profession. Over a six year period from 2004 to 2010, the percentage of women who consulted a herbalist/naturopath steadily declined from 11% to 9%. Over the same period there was an increase in the percentage of women who consulted a massage therapist (20% to 27%), chiropractor (14% to 16%), and acupuncturist (5% to 6%).
So why are consultations with herbalists/naturopaths on the decline, while consultations with practitioners from the other major CAM modalities on the increase? There are probably several reasons, but one might be that herbalists/naturopaths are the only one of the four CAM professions that has non-professional competition, through the ready availability of herbal products sold in health food stores, chemists, supermarkets and online. The other CAM modalities are manual therapies. Data from the ALSWH supports this argument. Over the period 2004 to 2010, there was a significant increase in the percentage of women who purchased vitamins, supplements or herbal products bought without a prescription at a chemist, supermarket and/or health food shop (from 58% to 69%) – this is the same period that the consultations with herbalists/naturopaths were declining.
Another answer might be that the decline in consultations with herbalists/naturopaths is related to the influence of general practitioners (GPs) on their patients. In a survey of 585 rural and regional GPs from New South Wales, GPs were asked about their attitudes towards the different CAM professions. With regard to herbalists/naturopaths, it was revealed that significant tensions appear to exist between these two groups, where there is little interaction between the herbalists/naturopaths and GPs either via referrals or professional relationships. Further, only 25% of GPs referred to a herbalist/naturopath at least a few times per year but 50% of GPs stated that they would not refer to a herbalist/naturopath under any circumstances. Interestingly, 55% of GPs indicated that they had poor or very poor knowledge of herbal medicine/naturopathy.6 (unpublished, under
review) Conversely, GP attitudes towards acupuncturists
The decline of herbal medicine/naturopathy consultations: how research can help further the profession
Professor David SibbrittAustralian Research Centre in Complementary and Integrative Medicine (ARCCIM), Faculty of Health, University of Technology Sydney, Ultimo NSW.Email: [email protected]

Australian Journal of Herbal Medicine 2014 26(1)
9© National Herbalists Association of Australia 2014
Commentary
and chiropractors were more favourable. The research revealed that a significant interface exists between GPs and acupuncturists and chiropractors, where 69% of GPs referred at least a few times per year to an acupuncturist and 65% to a chiropractor. Further, only 8% of GPs would not refer to an acupuncturist under any circumstances and 22% would not refer to a chiropractor under any circumstances. Only 28% of GPs indicated having poor or very poor knowledge of acupuncture and 33% had poor or very poor knowledge of chiropractic.7,8 As there is minimal evidence of efficacy for all of these CAMs, one could draw the conclusion that GPs are more positive towards chiropractors and acupuncturists compared to herbalists/naturopaths because they have a greater knowledge of what acupuncturist and chiropractors do in their practice. This notion has support in the literature, where GPs are indicating they would like to know more about CAM therapies.9 This is where research can help.
To date, most herbal medicine/naturopathy research has focused on clinical trials exploring safety and efficacy of medicinal plants or experimental studies investigating the pharmacology of the plants and mechanisms of action – work that is undoubtedly important to the development and standing of the herbal medicine/naturopathic profession. However, such research has been to the general neglect of other forms of research – research that would identify what happens in a consultation with
a herbalist/naturopath. For the herbalist/naturopathic profession to grow, it needs to gain the confidence of both consumers and other health professionals, in particular GPs. Recent work by Kirby et al10 (unpublished, under review) found that consumers decide to use a particular CAM treatment based more so on their knowledge and understanding of the treatment technique rather than its perceived effectiveness. As such, it is important to improve the lack of knowledge that consumers (and other health care providers) have in regard to the specifics of herbal medicine/naturopathic care, by comprehensively charting the diagnostic tools and treatment activities utilised by herbalist/naturopaths. Further, research highlighting the safety issues of particular herbal medicines and supplements will provide consumers with much needed knowledge that may deter them from purchasing herbal medicines and supplements at retail stores or online without the guidance of a herbalist/naturopath.
Clearly there is a need for herbal medicine/naturopathy research to be conducted. Unfortunately, the inclusion of research information in practitioner training curricula, either via courses or research experiences, is nonexistent or limited at best. Hence, there is an urgent need for the herbal medicine/naturopathy profession to undertake research activities and initiatives to develop research capacity if the profession is to hold a key position in the Australian health care system.
www.naturessunshine.com.au
For 40 years, Nature’s Sunshine has brought health to millions of people by developing, manufacturing and distributing the most innovative
and highest quality herbal and nutritional supplements in the industry.
PURE. POTENT. PROVEN.
References continued on page 38

Australian Journal of Herbal Medicine 2014 26(1)
10 © National Herbalists Association of Australia 2014
Article
Introduction The seeds of Daucus carota L. (DC) have been
described as an abortifacient, emmenagogue, contraceptive, and aphrodisiac in a variety of publications throughout European history. These documents also indicate use by women for over 2,000 years as a means to control fertility.1,2 More recently, ethnobotanical investigations have documented the use of DC seed as a method of fertility control by women in India3 and North American grassroots herbalists have documented its use for contraception.4 Scientific investigations have begun to assess the efficacy of DC seed as an anti-fertility agent and indicate between 40-100% anti-implantation activity in rodents.5 This paper aims to review the historical, traditional and scientific evidence in an attempt to identify the mechanisms of action and evaluate the efficacy of DC seed as an anti-fertility agent.
MethodsThe following electronic databases were searched:
Pubmed/Medline, Scopus, Web of Knowledge, Science Direct, AMED, CINAHL, EBSCO and Google Scholar. The search was conducted in May 2012 and search terms included “Daucus carota”, “Queen Anne’s Lace”, “Wild Carrot” AND/OR “seed”, “anti-fertility”, “fertility”, “contraceptive”, and “hormone”. Additional texts were included when referenced in aforementioned publications, as were a range of classic historical texts.
BotanyDaucus carota belongs to the family Apiaceae
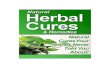
(Umbelliferae). Common names include wild carrot, Queen Anne’s lace, and Gajar in Hindi.6 Unlike the cultivated carrot, wild carrot has a small, white, fleshy taproot. The root can be eaten before the plant flowers. DC is a biennial herb with a branched stem rising 30-120 cm, leaves are finely divided, twice or thrice pinnate with upper leaves reduced in size; stems are rough with tiny hairs.7,8 The white flowers are densely clustered in terminal umbels, some containing a central purple flower which is regarded in herbal lore as an indicator of medicinal quality.9 The umbels almost completely flatten whilst in bloom but close up as the seeds ripen, to take on a nest-like appearance, giving rise to another common name, ‘Bird’s Nest’ (Figure 1). The seeds are 2-4 mm long, oblong with bristly hairs, brown in colour and have an aromatic flavour.
DC is one of 22 species in the genus Daucus, ten of these are found in Europe. Wild carrot is sometimes referred to as the subspecies carota, whereas the carotene-rich, orange-rooted cultivated carrot is D. carota subsp. sativa (Hoffm.) Arcang., with some modern cultivars crossed with D. capillifolius Gilli.10,11 It has been suggested that the carrot has been in cultivation for over 5,000 years, and it was possibly depicted in Egyptian temple drawings around 2000 BCE. DC was also discussed by ancient Greek medical writers in the
Carrot seed for contraception: a review
Jansen, Gabrielle Claire1, 2 and Wohlmuth, Hans3,4
1 School of Health and Human Sciences, Southern Cross University, Lismore NSW 2480, Australia. 2 Goulds Naturopathica, 73 Liverpool Street, Hobart TAS 7000, Australia.3 Division of Research, Southern Cross University, Lismore NSW 2480, Australia.4 Integria Healthcare, 8 Clunies Ross Court, Eight Mile Plains QLD 4113, Australia.Gabrielle JansenEmail: [email protected]
Abstract: The seeds of wild carrot (Queen Anne’s Lace, Daucus carota L., Family Apiaceae) have a long history of use relating to fertility, especially as an anti-fertility agent.
Objectives: A literature review was conducted in an attempt to evaluate the potential efficacy of carrot seed as a contraceptive and to more clearly identify the mechanisms of its reported actions.
Methods: Databases, including PubMed, Scopus, and Science Direct were searched, as were authoritative herbal and historical texts including Culpeper, Eclectic texts and Indian pharmacopoeias.
Results: The use of carrot seed for contraception and abortion is recorded throughout European history, with contemporary reports from India and the United States. Scientific in vivo and ex vivo studies suggest that several modes of action may contribute to the anti-fertility effect, including an effect on the oestrous cycle and anti-progestogenic activity.
Conclusions: Historical and ethnobotanical evidence make essential contributions to multidisciplinary research on herbal medicines. Further research is required to confirm the anti-fertility action of carrot seed and to provide a better understanding of the mechanism(s) of action and the compound(s) responsible.
Keywords: Daucus carota, wild carrot, carrot seed, anti-fertility, abortifacient, contraceptive

Australian Journal of Herbal Medicine 2014 26(1)
11© National Herbalists Association of Australia 2014
Article
first century CE. The ancestor of the cultivated carrot is native to present-day Afghanistan from where it spread to China in the 13-14th centuries and subsequently reached Europe by the 15th century. It was later introduced to North America by European settlers.8 The population of DC in North America grew from introduced weedy materials rather than escaped cultivated varieties.12 DC is now found almost worldwide and is considered an environmental weed in many temperate areas, including parts of Australia and most North American states (Figure. 2).
Most of the literature does not clearly identify the taxonomic status of the plant material used, and it has therefore not been possible to discriminate between results obtained with “wild carrot” and cultivated forms of the plant. Most chemical and pharmacological work on carrot seed has undoubtedly been conducted using cultivated material, but information is not available to establish the degree to which this may differ from “wild carrot” seed in terms of chemistry and pharmacological activity.
Chemistry of carrot seed oilThe chemical composition of steam distilled carrot
is complex and variable. Most published analyses have been of seed oil distilled from cultivated plants or from various subspecies of D. carota.
Steam distilled carrot seed oil typically contains significant amounts of the sesquiterpene alcohol carotol (<67%) and the monoterpenoid ester geranyl acetate
Figure1: Daucus carota umbels: flat umbel of flowering stage (left); curled up umbel of post-flowering stage (right). Photo: H. Wohlmuth.
Figure 2: Wild carrot growing by Niagara Falls, Ontario, Canada. Photo: H. Wohlmuth.

Australian Journal of Herbal Medicine 2014 26(1)
12 © National Herbalists Association of Australia 2014
Article
(<25%) (Figure 3), with highly variable amounts of the monoterpenoids alpha-pinene (2-25%), sabinene (<32%) and linalool (<6%), and of the sesquiterpenoids β-bisabolene (<16%) and daucol (<10%).
13,14,15,16 Three flavones, luteolin, luteolin 3′-O-β-D-glucopyranoside and luteolin 4′-O-β-D-glucopyranoside have been isolated from a methanol extract of carrot seed.17
Historical evidence
A note on identity Confusion and debate surround the correct
identification of the carrot in the classical era and it is possible that varieties of carrot and the closely related parsnip were used interchangeably. The writings of Galen and Dioscorides suggest the actions of Staphilinos, Daucos and Pastinaca were so similar one could be used in place of another. These herbs are discussed as having both fertility and anti-fertility activity, yet these ancient works do not form consensus.2
Ancient Greece to the Middle AgesA work attributed to Hippocrates (c. 460 - 370
BCE) appears to be the oldest reference to the anti-fertility activity of DC seed, which are described as an abortifacient.1 Similar uses were later recorded by Pliny, Dioscorides, Scribonius Largus and Marcellius Empericus. According to Riddle1, Pliny (Gaius Plinius Secundus 23 CE - 79 CE, also known as Pliny the Elder) was against contraception and abortion and therefore stated that DC was an emmenagogue, so as not to transmit the lore relating to its anti-fertility action. Around the same time DC appeared in an abortion-inducing recipe by Scribonius Largus (47 CE), a Roman court physician.18 DC was regarded as a strong emmenagogue by Constantine the African and was recorded in a work by Petrus Marancius later in the 13th century as an emmenagogue, but not as an abortifacient.18
The late Middle Ages and witch trialsThe confusion regarding the origins, applications and
identification of DC has not been helped by the great loss of herbal knowledge believed to have occurred in the Middle Ages. It is widely accepted that information regarding birth control was orally transmitted and therefore, as a consequence of the persecution of ‘witches’, who were often female midwives, herbalists and healers, much of this information was lost.1
CulpeperCulpeper’s Complete Herbal was first published in
England in 1653 and was considered the herbal authority for the common people of its time. Culpeper noted that DC possessed both pro- and anti-fertility actions. According to Culpeper, the carrot root and seed work similarly to promote menstrual flow (“women’s courses”) and can be used to treat “the rising of the mother”, which may refer to menstrual obstructions. Culpeper also suggested that the seed boiled in wine may help conception. Culpeper advised that DC is governed by Mercury, which is said to rule wind (colic and spasm).19
The nineteenth and early twentieth centuryDC is mentioned in a number of publications during
the 19th century, including those written by the American Eclectics and Physiomedicalists. However, some publications that include DC do not refer to either pro-fertility or anti-fertility activity,20,21,22,23,24 while other such publications contain no reference to DC at all.25,26,27,28,29,30 King’s American Dispensatory includes DC, stating that it may possess emmenagogue properties.31 Culbreth32 asserted that DC was indicated for amenorrhea, while others regarded it as a useful “deobstruent”.33,34 The recommended remedy to be taken when menstruation was absent was one third to one teaspoonful of bruised seeds, repeated as necessary.33A late nineteenth century “pharmacographia” of the medicinal plants of India includes DC and states, “In India, the seeds are popularly supposed to cause abortion and are kept by all the native druggists”.35
Ethnobotanical evidence
IndiaDC has been included in a number of Indian
materia medica and medicinal plant texts. The taproot was considered an aphrodisiac, and a decoction of the leaves and seeds was used as a uterine stimulant during parturition.36 Throughout India and specifically in the north-west state of Punjab and south-west state of Konkan the seeds were considered an aphrodisiac; in Punjab they were also given for uterine pain.36,37,38 The seeds have also been listed for procuring abortion.39,40
Ethnobotanical investigation has reported that the seeds of DC, commonly known as Gajar in India, have been traditionally used as an abortifacient.6 Tribal peoples of southern Rajasthan have used DC seed to regulate menstruation and in higher doses as an effective abortifacient.41 Tribal people in the north-west Himalayas and central Uttar Pradesh also used Gajar seeds for female fertility control; here a decoction of seeds along with old jaggri (a sugar additive) was prepared as an abortifacient.42
North AmericaThe modern use of DC seeds for female contraception
Figure 3: Major constituents of the essential oil of carrot seed: carotol (above), geranyl acetate (below).

Australian Journal of Herbal Medicine 2014 26(1)
13© National Herbalists Association of Australia 2014
Article
has been documented in North America. Here some herbalists have described DC seeds as an ‘implantation preventer’, suggesting that oral administration of the seeds causes the endometrium to become inhospitable for the implantation of a fertilized embryo to occur. The suggested method of using DC seeds for the prevention of pregnancy is to chew one teaspoonful of seeds once daily for up to one week at the time of ovulation or immediately following unprotected intercourse during the fertile period of the menstrual cycle.9,43 An anonymous gynaecological self-help publication lists DC seeds as an emmenagogue, an implantation inhibitor or abortifacient, and states that this activity may be attributed to oestrogenic activity and/or inhibition of progesterone synthesis.44 Traditional evidence is regularly cited as informing dosage, viz. one teaspoonful chewed after intercourse or daily around ovulation.44
There have been a number of anecdotal reports of contemporary women in the Appalachian mountains and Watauga County, North Carolina, using DC seeds for their anti-fertility activity. One such report concerns a woman who allegedly took one tablespoon of DC seeds with water immediately following intercourse for over ten years, and only became pregnant once when she had been on holidays with her husband and left the DC seeds at home.1
Uncontrolled human studiesTwo ‘grass-roots studies’ using DC seed as an anti-
fertility agent have been reported by North American herbalists. These trials have not claimed to be scientific and lacked the rigour to be considered as such (e. g. they were uncontrolled and did not use a standardised intervention or a standardised dosage regimen), and they do not provide evidence for DC seed being an effective contraceptive in women. However these observational studies remain the only documented attempts at investigating the efficacy of DC seed as a sole means of contraception in a human population and they highlight the continued usage of this herb by contemporary women.
In the first of these studies, thirteen women charted their menstrual cycles including times of ovulation and instances of intercourse.9 Also recorded was the dose and mode of administration of DC seeds. Reported dosage regimens for the study were: (1) one teaspoon of DC seeds chewed once daily, or (2) one teaspoon of DC seeds chewed once daily prior to, during and three days post ovulation, or (3) one teaspoon of DC seeds chewed once daily for seven days immediately following sexual intercourse. DC seeds were not always the sole form of contraception used by the participants. Three pregnancies were reported during the eleven month study.
A second study assessed DC seeds taken postcoitally.4 Thirty women aged 18-50 years participated in the year-long study. Women consumed alcoholic tincture made from seeds and flowers of DC, 15 drops of flower and
15 drops of seed extract taken after each occasion of intercourse, three times with doses eight hours apart. Women also kept a record of menstrual cycles and charted occasions of intercourse and DC usage. Five participants completed the entire year with no pregnancies reported. Nine pregnancies were recorded amongst the greater cohort, some occurring when DC was not used as indicated. No abnormalities were recorded in infants born to mothers who had used DC seeds.
Scientific investigations The anti-fertility activity of DC seed has sparked
interest in the scientific community, and a number of animal studies have been conducted in an attempt to elucidate its pharmacological actions and potential efficacy. The following section reviews current scientific understanding. It should be noted that almost certainly, all scientific studies have employed carrot seed obtained from cultivation.
Ex vivo studiesEx vivo studies have been carried out to study the
activity of DC seed extract on isolated tissues.An early study isolated choline from the alcoholic
extract of DC seeds, but it was unclear if this was a native constituent of the seed or an artefact formed during the multi-step isolation process.45 Predictably, the isolated choline had a spasmodic effect on smooth muscles of rabbit, guinea pig ileum and dog trachea, an inhibitory effect on the force and rate of contraction of perfused frog’s heart, and caused a hypotensive effect in the anaesthetised dog. In a later study, the effect of the methanolic fraction of a petrol (sic) extract of DC seed on the isolated rat uterus was evaluated, with both spontaneous and oxytocin evoked responses being inhibited.46 Spontaneous activity was inhibited at 0.2 mg/mL, and a dose of 0.5 mg/mL significantly reduced responses evoked by low and high concentrations of oxytocin. Additionally, the extract caused a marked reduction of histamine-induced contractions in isolated guinea pig ileum. Inhibitory effect on the rat uterus was concluded to contribute to the anti-fertility activity of carrot seeds, though the mechanism was not elucidated.
In vivo studies Animal studies of the anti-fertility activity of DC began
in the 1970s, with scientists attempting to demonstrate efficacy and understand the actions of DC extract in rodents. The anti-fertility action of DC seed successively extracted with petroleum ether, 95% ethanol and water was tested on early pregnancy in albino rats.47
At 100 and 500 mg/kg body weight (BW), the ethanolic residue prevented implantation in 40% and 67% of animals, respectively. The corresponding figure was 60% for the aqueous residue at 100 mg/kg BW, but the number of animals in each group was low. Petroleum ether extract at 100mg/kg BW did not prevent implantation in any rats, whilst 500mg/kg inhibited

Australian Journal of Herbal Medicine 2014 26(1)
14 © National Herbalists Association of Australia 2014
Article
implantation in 40% of animals. Abortifacient activity of the extract was also noted in some animals. When the aqueous residue was administered at 500 mg/kg BW, implantation was inhibited in only 20% rats, while the abortifacient activity increased to 60%. The decrease of implantation inhibition and increase in abortifacient activity at a higher dose of the aqueous residue was not explained and may have been a product of the small number of animals used. In follow-up research, the effects of different chromatographic fractions of DC seed on fertility in albino rats were investigated.72 Rats were fed DC seed extracts in gum acacia for 1-7 days of pregnancy. Results showed that pregnancy was inhibited most effectively by chloroform and methanol fractions of the petroleum ether extract; of five rats fed 20 mg/kg BW orally for days 1-7, none littered. Another five rats were fed a chloroform+methanol (9:1 v/v) fraction of the alcoholic extract at 50 mg/kg BW with one rat littering three pups. The chloroform and ethyl acetate fractions of the aqueous extract showed similar results with one rat littering three pups (chloroform) and no littering in the ethyl acetate group. No abnormalities were detected in young born to treated mothers, tested up to one month of age.
Further research was undertaken by Garg49 to assess the time course of anti-fertility activity in rats. The chloroform and methanol fractions of the petroleum ether extract and chloroform:methanol (9:1 v/v) fraction of the alcoholic DC seed extract significantly inhibited pregnancy on days 1-3 of pregnancy at 50 mg/kg BW. It was suggested that these fractions were anti-zygotic. It was also concluded that the chloroform fraction of the aqueous extract acts as a blastocystotoxic and/or anti-implantation agent, as pregnancy was inhibited in most rats when it was administered orally on days 4 and 5, or 6 and 7. The ethyl acetate fraction of the aqueous extract showed 80% anti-fertility activity when administered on days 1-3 and days 4-5 of pregnancy. Hence, this fraction may be an anti-zygotic and/or blastocystotoxic agent.
Another study assessing the efficacy of different extracts and their fractions was undertaken, demonstrating that alcoholic (500 mg/kg BW) and aqueous extracts (100 mg/kg BW) of DC seeds inhibited pregnancy in rats by 67% and 60%, respectively.50 Interestingly, anti-fertility activity increased to 80% when rats were administered 50 mg/kg BW of the chloroform-methanolic (9:1 v/v) fraction of the alcoholic extract. At the higher dose of 100 mg/kg BW the chloroform and ethyl acetate fractions of the aqueous extract showed 80% and 100% anti-fertility activity, respectively. The chloroform and methanol fractions of the petroleum ether extract (100mg/kg BW) demonstrated 100% efficacy, however the number of animals in each experimental group was low (5-10). Complete anti-implantation activity was found for the chlorofom and methanol fractions of a petroleum ether extract at 20 mg/kg BW.51
The (presumably steam distilled) oil of DC seed had 40% anti-implantation activity when administered 1-7 days post-coitally in rats at 500 mg/kg BW.51 The volatile oil of DC seeds was also found to terminate pregnancy in mice and rats, with an ED50 of 2.9 mL/kg BW in mice for the terpenoid fraction administered subcutaneously. The peripheral plasma concentration of progesterone in pregnant rats decreased significantly 24 and 48 hours after subcutaneous injection, suggesting the anti-fertility activity may be related to the inhibition of progesterone.52
An alcoholic extract of DC seed was evaluated for oestrogenicity and anti-implantation effects in mice. The extract completely inhibited implantation when given orally at doses of 80 or 120 mg/mouse 4-6 days post-coitally, whereas when administered 8 to 10 days post-coitally pregnancy remained unaffected.53 DC seed extract at doses of 60 and 120 mg/mouse caused a significant (p<0.001) increase in uterine weight of ovariectomised mice, indicative of oestrogenic activity, but this effect was very weak compared with that of oestradiol. Conversely, when administered concurrently with the hormone, the DC seed extract significantly inhibited the uterotrophic effect of estradiol and thus exhibited anti-oestrogenic activity, likely via competitive inhibition at the oestrogen receptor.
A study of the anti-ovulatory activity of an alcohol extract of DC seeds in rabbits showed a 40% inhibition in ovulation with 100 mg/kg BW orally once daily for three days.54 Ovulation was stimulated using a 0.4% solution of cupric acetate i.v. A petroleum ether extract of carrot seeds (0.2-0.8 mL per 100 g BW) administered subcutaneously on days 7-13 of pregnancy caused abortion in most rats, with profuse vaginal bleeding within three days. Uterine and ovarian weight was considerably reduced, and adrenal weight significantly increased, although it was difficult to ascertain whether adrenal hypertrophy was caused by stress, toxicity or weak oestrogenic effect.55
Another study evaluating the abortifacient effect of DC seed extract found that pregnancy was terminated in rats subcutaneously administered petroleum ether extract of DC at 0.2 mL/100 g BW from day 7 of pregnancy onwards.56 The same study found that progesterone administered at 4-6 mg/100 g BW maintained pregnancy in 82-89% of rats when given alongside the DC extract on days 7-19 of pregnancy. Progesterone treatment also increased ovarian and uterine weight that had decreased with DC treatment. Adrenal glands hypertrophied with both DC and progesterone treatment, though this may have been an indicator of stress.
The ability of progesterone to maintain implantation in rats treated with DC seed extract has been evaluated further. A subcutaneous injection of petroleum ether extract of DC seeds 0.6 mL/100 mg BW in rats from day 1-7 of pregnancy inhibited implantation, and 2-8 mg/100 g BW of progesterone on the same days was found to reverse this effect.57 A significant reduction in the uterine

Australian Journal of Herbal Medicine 2014 26(1)
15© National Herbalists Association of Australia 2014
Article
weight and significant increase in the adrenal weight was observed in rats administered the DC seed extract. These results concur with those found previously and support the hypothesis that the anti-implantation activity of DC seed extract could be due to either gonadotrophin inhibition affecting ovarian steroidogenesis or to a progesterone-oestrogen imbalance.
A study was conducted to further evaluate the post-coital contraceptive activity of DC seed extract and assess the mode of action.58 An ethanolic extract of DC seed was administered intramuscularly to rats for three consecutive days post coitus at dosages of 50-250 mg/kg BW. At a lower dose (50 mg/kg BW), the extract produced an anti-oestrogenic effect, inhibiting implantation with cessation of the oestrous cycle and continuous diestrus, suggesting secretion of oestrogen from the ovary was not occurring. At a higher dose (250 mg/kg BW administered on day 14-16 post-coitus), the extract had oestrogenic activity, prolonging the oestrous phase and causing foetal resorption (89% by day 20). At 100-250 mg/kg BW the extract caused a dose-dependent decrease in myometrial and endometrial mast cell populations. The author suggested this disruption of mast cells may have been associated with increased release of histamine, which may in turn have disrupted the luminal epithelium and attachment of the embryo, causing rejection of the foetus.
Another potential mechanism for the anti-fertility activity of DC seeds emerged from a study that found that in mice, a DC seed petroleum ether extract and a fatty acid fraction thereof (both injected intraperitoneally) significantly lowered levels of two key enzymes involved in ovarian steroidogenesis, 3-β-hydroxy steroid dehydrogenase and glucose-6-phosphate dehydrogenase.59 This study also found that both the extract and the fatty acid fraction arrested the oestrous cycle; the extract at 10 and 3 mg/kg BW produced this effect after six days of treatment, while the fatty acid fraction (3 mg/kg BW) did so after just two days. Both treatments significantly reduced the weight of the ovaries. Of five chromatographic fractions of the extract, only the fatty acid fraction was active; hence it was concluded that the activity of the petroleum ether extract resided in this fraction.
More recently, a study investigating the anti-fertility activity of an aqueous extract and aqueous suspension of DC seed powder administered orally to female mice and rats revealed a significant disruption to the oestrous cycle in both groups of animals, resulting in a continuous dioestrous phase.60 This study also found an accumulation of cholesterol and ascorbic acid in the ovaries, suggestive of hypofunctioning of the steroidogenic activity of the ovary. Simultaneously, a considerable reduction in enzymatic activity of 3-β-hydroxy steroid dehydrogenase and glucose-6-phosphate dehydrogenase was found, suggesting this as the possible mechanism for anti-fertility activity. After withdrawal of treatment, regular
oestrous cycle returned from day 10 post treatment, and animals showed no abnormalities in hepato-renal function. This study did employ various chemicals during the extraction procedures, but failed to adequately control for any potential effects of these chemicals.
Safety and toxicologyInadequate evidence exists regarding the safety of
long-term administration of DC seed by women or children born to those women. However, anecdotal evidence indicates conception is possible following a ten-year usage of DC seed for contraception but does not provide information about potential health impacts on mother or child.18 In one study no abnormalities were detected in pups born to rats orally administered DC seed extract during days 1-7 of pregnancy, with testing up to one month of age.48 Ethnobotanical evidence reports the “healthy pregnancy and healthy baby” in the case of a woman, who stopped taking DC seed in order to conceive.9 The duration and dosage regime of seeds was not recorded, neither was the time between ceased usage of carrot seeds and subsequent conception, nor was there follow-up data relating to the health of women or children.
At present there is clearly inadequate information about the safety and potential toxicity of DC seed, and until further information is available, DC seed should not be used during pregnancy.
DiscussionThe scientific evidence relating to the anti-fertility
activity of DC seed reviewed above gives rise to three potential, not mutually exclusive, modes of action. They are discussed in more detail below.
Disruption of antioxidant protection Glucose-6-phosphate dehydrogenase (G6PD) was
significantly inhibited in the ovaries of mice treated with DC seed extracts.59,60 G6PD is a cytoprotective enzyme that protects the embryo from oxidative stress and DNA damage. G6PD plays a role in the hexose monophosphate shunt (HMS) pathway, which regenerates nicotinamide adenine dinucleotide phosphate (NADPH). NADPH is essential for maintaining glutathione, required for detoxification of reactive free radicals and lipid hydroperoxides. Ribose is also produced by the HMS and is relevant for the synthesis of nucleotides used in RNA and DNA replication, and hence cell division and DNA repair.61 As G6PD is essential for normal development of the embryo, the inhibition of this critically important enzyme by DC seed may result in the blastocyst not being adequately protected from oxidative stress, with negative ramifications for RNA and DNA replication. Under these circumstances the blastocyst may not survive.
Anti-progestogenic activityProgesterone is necessary for the development and

Australian Journal of Herbal Medicine 2014 26(1)
16 © National Herbalists Association of Australia 2014
Article
growth of the embryo, and inhibition of this hormone may contribute to the anti-fertility activity of DC seed. The enzyme 3β-hydroxysteroid dehydrogenase (3β-HSD) is required for the production of steroid hormones and is responsible for the conversion of pregnenolone to progesterone.62,63 Two studies have found DC seed extract to significantly inhibit 3β-HSD in the ovaries of treated mice.59,60 These findings suggest that ovarian progesterone production may be impaired as a result of DC seed administration.
Significant lowering of progesterone levels and abortion were seen in rats following subcutaneous injection of DC seed volatile oil.52 However, co-administration of megestrol acetate, a potent progesterone receptor agonist, reversed the abortifacient effect. Similarly, Kaliwal & Ahamed57 found that co-administration of progesterone reversed the anti-implantation effect of DC seed extract in rats. These results strongly suggest that the anti-fertility effect of DC seed is at least partly due to its anti-progestogenic activity.
Effect on oestrous cycleTreatment of ovariectomized mice and rats with DC
seed preparations has shown a significant increase in uterine weight.53,58 Since endogenous oestrogen is not present in ovariectomized animals, this is suggestive of estrogenic activity of DC seed. However, in comparison with oestradiol, DC seed extract was only very mildly oestrogenic, and the extract exhibited anti-oestrogenic properties when co-administered with estradiol.53 These results suggest that DC seed extract acts as a competitive inhibitor of oestrogen binding to oestrogen receptors. Lower doses of DC seed extract (3-100 mg/kg BW) arrested the oestrous cycle and prolonged diestrus, while higher doses (150-250 mg/kg BW) prolonged the oestrous stage of the cycle.58,59,60 Bhatnagar58 found that the effects of lower doses were consistent with anti-oestrogenic effects resulting in anti-implantation effects, while higher doses produced an oestrogenic response resulting in abortifacient activity.
These results demonstrate that DC seed affects the oestrous cycle in rodents, likely through interaction with oestrogen receptors. Whether this interaction results in an oestrogenic or anti-oestrogenic response may depend on the endogenous oestrogen status and the dose of DC seed preparation.
ConclusionDue to the great loss of oral herbal traditions,
knowledge about fertility herbs and their applications has diminished. Historical and ethnobotanical evidence makes an essential contribution to multi-disciplinary research which broadens our understanding and appreciation of medicinal plants, and can offer clues to their therapeutic action.
Carrot seed has an extensive history of use as an anti-fertility agent, but further research is required to confirm
and evaluate this activity in humans. Current evidence, based on rodent studies, suggests that the anti-fertility action of DC seed may be due to anti-progestogenic activity, disruption of the oestrous cycle, and/or disruption of antioxidant protection of the blastocyst. Further research is needed to elucidate the mechanism of action and identify the compound(s) responsible.
References1. Riddle J. 1997. Eve’s Herbs: A history of contraception and abortion
in the west. Cambridge, Massachusetts: Harvard University Press.2. Tobyn G, Denham A, Whitelegg M. 2011. The Western Herbal
Tradition: 2000 Years of Medicinal Plant Knowledge. Edinburgh: Churchill Livingstone.
3. Maurya R, Srivastava S, Kulshreshta D, Gupta C. 2004. Traditional remedies for fertility regulation. Curr Med Chem 11(11):1431-1450.
4. Bennett R, Schuler M. 2011. Wild Carrot Study - Final Summary. Retrieved on July 15th, 2012 from http://robinrosebennett.com/articles/wild-carrot-study-final-summary-august-2011/
5. Kamboj V. 1988. A review of Indian medicinal plants with interceptive activity. Indian J Med Res 87(88):336-355.
6. Kumar D, Kumar A, Prakash O. 2012. Potential antifertility agents from plants: A comprehensive review. J Ethnopharmacol 140(1):1-32.
7. Grieve M. 1931. A Modern Herbal. London: Harcourt, Brace & Company.
8. Ross I. 2010. Medicinal Plants of the World, Volume 3: Chemical Constituents, Traditional and Modern Medicinal Uses. New Jersey: Humana Press.
9. Bennett R. 1993. Wild Carrot Seeds for Herbal Contraception – Summary of findings from a 1992Study.WiseWomanHealingWays. New York. Retrieved on July 15th, 2012 from http://robinrosebennett.com/articles/wild-carrot-daucus-carota-a-plant-for-conscious-natural-contraception/
10. Mabberley D. 2008. Mabberley’s plant-book: a portable dictionary ofplantstheirclassificationanduses.3rd ed. Cambridge: Cambridge University Press.
11. The Plant List 2013. URL: http://www.theplantlist.org/ (accessed 24 October 2013)
12. Bradeen J, Bach I, Briard M, Clerc V, Grzebelus D, Senalik D, Simon P. 2002. Molecular diversity analysis of cultivated carrot (Daucus carota L.) and wild Daucus populations reveals a genetically nonstructured composition. J Am Soc Hortic Sci 127(3):383-391.
13. Lawrence BM. 1988. Progress in essential oils. Perfumer & Flavorist 13:61-64.
14. Lawrence BM. 1990. Progress in essential oils. Perfumer & Flavorist 15:67-69.
15. Lawrence BM. 1992. Progress in essential oils. Perfumer & Flavorist 17: 71-72.
16. Lawrence BM. 1999. Progress in essential oils. Perfumer & Flavorist 24:7-8.
17. Kumarasamy Y, Nahar L, Byres M, Delazar A, Sarker S. 2005. The assessment of biological activities associated with the major constituents of the methanol extract of ‘wild carrot’ (Daucus carota L) seeds. J Herbal Pharmacother, 5(1):61-72.
18. Riddle J, Estes J. 1992. Oral contraceptives in ancient and medieval times. American Scientist 80(3):226-233.
19. Culpeper N. 1653. Culpeper’s Complete Herbal and English Physician. Avon, Bath: Pitman Press Ltd. (1981)
20. Britton N, BrownA. 1913.An illustrated flora of the northernUnited States, Canada and the British possessions. 2nd ed. New York, Scribner’s Sons.
21. Cook W. 1869. The Physiomedical Dispensatory. Cincinatti: WM.H.Cook.
22. Fox, W. 1924. The working man’s model Family Botanic Guide.

Australian Journal of Herbal Medicine 2014 26(1)
17© National Herbalists Association of Australia 2014
Article
23rded.Sheffield,GreatBritain:WilliamFoxandSons.23. Remington JP, Horatio C, editors. 1918. The Dispensatory of the
United States of America. 20th ed. Philadelphia: Lippincott-Raven.24. Sturtevant E. 1919. Sturtevant’s edible plants of the world. Albany,
USA: J.B.Lyon..25. Colby B. 1846. A Guide to health Part III. Materia Medica. Milford:
John Burns.26. Ellingwood F. 1919. American Materia Medica, Therapeutics and
Pharmacognosy. Portland: Eclectic Medical Publications.27. Felter H. 1922. The Eclectic Materia Medica, Pharmacology and
Therapeutics. Cincinnatti, Ohio: J.K. Scudder.28. Fyfe J. 1903. The Essential of Modern Materia Medica and
Therapeutics. Cincinnatti: The Scudder Brothers Company.29. Lloyd J. 1911. History of the Vegetable Drugs of the Pharmacopeia
of the United States. Cincinnatti, Ohio: Lloyd Library.30. Sayre L. 1917. Manual of Materia Medica and Pharmacognosy. 4th
ed. Philidelphia: P.Blakiston’s Son & Co.31. Felter H, Lloyd J. 1898. King’s American Dispensatory.
Cincinnatti: Ohio Valley Co.32. Culbreth DMR. 1927. A manual of Materia Medica and
Pharmacology. 7th ed. Philadelphia: Lea & Febiger.33. Hool R. 1918. Health from British Wild Herbs. Southport: W.H.
Webb34. Ward H. 1936. Herbal manual. London: L.N. Fowler & Co. Ltd.35. Dymock W. Hooper D, Warden CJH.1891. Pharmacographia
indica: A history of the principal drugs of vegetable origin met with in British India. London: Kegan Paul, Trench Trubner & Co.,
36. Kirtikar K, Basu B. 1946. Indian Medical Plants. 3rd ed. Allahabad: Lalit Mohan Basu.
37. Chopra I, Chopra R, Nayar S. 1956. Glossary of Indian Medicinal Plants.NewDelhi:CouncilofScientificandIndustrialResearch.
38. Chopra I, Handa K, Kapoor L. 1958. Indigenous Drugs of India. Culcutta: Dhur, U.N. and Sons Pvt. Ltd.
39. Chopra I, Chopra R. 1955. A review of work on Indian medicinal plants (Vol. Special report series). New Delhi: Indian Council of Medical Research.
40. Nadkarni K., Nadkarni A. 1976. Indian Materia Medica.Vol. 1.Bombay: Popular Prakashan Pvt. Ltd.
41. Jain A, Katewa SS, Chaudhary BL, Galav P. 2004. Folk herbal medicines used in birth control and sexual diseases by tribals of southern Rajasthan, India. J Ethnopharmacol, 90(1):171-177.
42. Singh S, Laxmi V. 1986. Folklore Claims by Tribals and Experimental Evaluation of some medicinal Plants with Special Reference to Contraception. Tribal Health Inter-India Publications 339-346.
43. Weed S. 1985. Wise Woman Herbal for the Childbearing Year. New York: Ash Tree Publishing.
44. Sage-Femme Collective. 2008. Natural Liberty: Rediscovering Self-Induced Abortion Methods. Las Vegas: Sage-Femme Collective.
45. Gambhir S, Sanyal A, Sen S, Das P. 1966. Studies on Daucus carota Linn. II. Cholinergic activity of the quaternary base isolated from water-soluble fraction of alcoholic extract of seeds. Indian J Med Res 54(11):1053-1056.
46. Dhar V. 1990. Studies on Daucus carota seeds. Fitoterapia, 61(3):255-258.
47. Garg S, Garg G. 1971a. Antifertility screening of plants. Part VII Effectoffiveindigenousplantsonearlypregnancyinalbinorats.Indian J Med Res 59:302-306.
48. Garg S, Mathur V. 1972. Effect of chromatographic fractions of Daucus carota Linn (seeds) on fertility in female albino rats. J Reprod Fertil 31:143-145.
49. Garg S. 1975. Antifertility effect of some chromatographic fractions of Daucus carota. Indian J Pharmacol 7(1):40-42.
50. Garg S, Mathur VS, Chaudhury RR. 1978. Screening of Indian plants for antifertility activity. Indian. J Exp Biol 16(10):1077-1079.
51. Kamboj V, Hawan B. 1982. Research on plants for fertility regulation in India. J Ethnopharmacol, 6(2):191-226.
52. Chu Y, Zhou M, Li Q, Bao Y. 1985. Antifertility effect of volatile oil of Daucus carota seeds. Reprod Contracept 5(1):37-40.
53. Sharma M, Lal G, Jacob D. 1976. Estrogenic and pregnancy interceptory effects of carrot Daucus carota seeds. Indian J Exp Biol 14(4):506-508.
54. KapoorM,GargS,MathurV.1974.Antiovulatoryactivityoffiveindigenous plants in rabbits. Indian J Med Res, 62(8):1225-1227.
55. Kaliwal B, Ahamed R, Rao M. 1984b. Dose and temporal effect of carrot seed (Daucus carota) extract on pregnancy in albino rats. Comp Physiol Ecol 9(3):173-177.
56. Kaliwal B, Ahamed R, Rao M. 1984a. Abortifacient effect of carrot seed (Daucus carota) extract and its reversal by progesterone in albino rats. Comp Physiol Ecol 9:70-74.
57. Kaliwal B, Ahamed R. 1987. Maintenance of implantation by progesterone in carrot seed Daucus carota extract treated albino rats. Indian J Physical Natural Sciences Section A7:10-14.
58. Bhatnagar U. 1995. Postcoital contraceptive effects of an alcoholic extract of the Daucus carota Linn seed in rats. Clin Drug Investig 9(1):30-36.
59. Majumder P, Dasgupta S, Mukhopadhaya R, Mazumdar U, Gupta M. 1997. Anti-steroidogenic activity of the petroleum ether extract and fraction 5 (fatty acids) of carrot (Daucus carota L.) seeds in mouse ovary. J Ethnopharmacol 57(3):209-212.
60. Das P, Gupta M, Mazumdar U. 2008. Studies on the antifertility activities of the aqueous extract and aqueous suspension of Carrot (Daucus carota L.) seed powder through oral administration on mice and rat. Biosci Biotechnol Res Asia 5(1):245-254.
61. Nicol CJ, Zielenski J, Tsui LC, Wells P. 2000. An embryoprotective role for glucose-6-phosphate dehydrogenase in developmental oxidative stress and chemical teratogenesis. FASEB Journal 14(1):111-127.
62. Chapman J, Polanco J, Min S, Michael S. 2005 Mitochondrial 3 beta-hydroxysteroid dehydrogenase (HSD) is essential for the synthesis of progesterone by corpora lutea: An hypothesis. Reprod Biol Endocrinol 3:11.
63. Von Teichman A, Joerg H, Werner P, Brenig B, Stranzinger G. 2001. cDNAcloningandphysicalmappingofporcine3β-hydroxysteroiddehydrogenase/Δ5-Δ4isomerase.Animal Genetics 32(5):298-302.

Australian Journal of Herbal Medicine 2014 26(1)
18 © National Herbalists Association of Australia 2014
Article
Historical noteNative to the Middle East and the countries of the
Mediterranean (with Spain and Iran now providing in excess of 80% of the world’s production), the fine thread-like stigmas of saffron have a long history of use for medicinal, culinary and cosmetic purposes.1 With three stigmas to every flower, approximately 150,000 flowers must be harvested to produce one kilo of dried saffron and thus it is considered to be the most expensive spice in the world.1
Common nameSaffron
Botanical name/familyCrocus sativus/Iridaceae
Plant part usedTraditionally, it is the red-orange stigma which has
been used for its medicinal purposes.2 However, authors state that difficulty in obtaining the stigma results in it being an extremely expensive raw material and consequently, products containing the stigma extract are at risk of adulteration or substitution. As a result, some researchers2 have examined the potential efficacy of an extract of the petal (currently a by-product of saffron production) in the treatment of depression. The same weight (120g) of either petal or stigma was extracted in 1800ml ethanol (80%) and both were standardised to 0.3-0.35mg safranal. Further research may pave the way for the use of the petal as a viable and less expensive alternative to the stigma.
Chemical componentsTo date, four main active constituents in saffron have
been identified. These are crocin and crocetin picrocrocin and safranal.3
Actions supported by clinical evidence• Thymoleptic• Aphrodisiac• Antioxidant
Clinical use
DepressionA systematic review from 2011 examined alternative
herbal medicines (other than St John’s wort) for the treatment of depression.4 The review included five studies for saffron (three using the stigma and two using the petal). These were all randomised, double-blind trials ranging from 6-8 weeks in duration, comparing saffron to placebo (two studies), fluoxetine (two studies) or imipramine (one study). The authors reported positive findings for the treatment of mild to moderate depression. A dried ethanol extraction of the stigma at a dose of 30mg/day has been shown to be as effective as imipramine (100mg/day) and fluoxetine (20mg/day) as measured by the Hamilton Rating Scale for Depression (HAM-D). Similar results were found for a comparison of the dried petal (30mg/day) to fluoxetine (20mg/day). Furthermore, tolerance for saffron was shown to be similar to or better than fluoxetine and better than imipramine. A further (sixth) study compared use of the dried petal to the dried stigma. Results were comparable showing 60% reduction in HAM-D scores for the stigma group and 54% reduction for the petal group (p=0.0001).
Other uses
Sexual dysfunctionFluoxetine-induced sexual dysfunctionSexual dysfunction is a commonly reported side-
effect of some anti-depressant medication.5 This author conducted a randomised, double-blind, placebo controlled study looking at the efficacy and safety of saffron in women aged 18-45 diagnosed with major depressive disorder (per DSM-IV). The women’s depression symptoms had responded positively to fluoxetine at a stable dose of 40mg/day; however, they reported subjective feelings of sexual dysfunction. Thirty-eight women were assigned to receive capsules containing the equivalent of 15mg of dried petal extract twice a day or placebo for four weeks. Outcomes were assessed on
Crocus sativus (saffron): a monograph
Kaye WrightEmail: [email protected] Website: www.lavidahealth.com.au
Abstract: Crocus sativus (saffron) is best known for its use as a culinary spice but it also has traditional usage as a medicine, sparking an interest in the medicinal properties and potential clinical uses of saffron. Research has identified the main chemical components as crocin, crocetin, safranal and picrocrocin, and the main actions as thymoleptic, aphrodisiac and antioxidant. To date, the strongest evidence for the use of saffron has been in the treatment of depression with randomised controlled trials showing it to be as effective as fluoxetine and imipramine. It also shows some potential for the treatment of sexual dysfunction, Alzheimer’s disease, pre-menstrual syndrome, retinal disease and weight loss. There is no long-term safety data at this time.

Australian Journal of Herbal Medicine 2014 26(1)
19© National Herbalists Association of Australia 2014
Article
the basis of the Female Sexual Function Index which looks at desire, lubrication, arousal, orgasm, satisfaction and pain. The author found the saffron extract showed positive results (p<0.05, 95% CI) when compared to placebo for arousal (p=0.028), lubrication (p=0.035) and pain (p=0.016) but did not reach statistical significance for the measures of desire, orgasm and satisfaction.
An earlier randomised, double-blind, placebo controlled study, looking at fluoxetine-induced erectile dysfunction in 36 men with major depressive disorder showed similarly positive results with significant improvements in erectile function (p<0.001), intercourse satisfaction (p=0.001) and total scores (p<0.001) but insignificant difference for orgasmic function (p=0.095), overall satisfaction (p=0.334) and sexual desire (p=0.517) as measured by the International Index of Erectile Function scale. The incidence of side effects in the two groups were found to be similar.6F (1.444, 40.434
Non-drug induced erectile dysfunctionSaffron has also been studied in men with non-drug
induced erectile dysfunction with mixed results. One small uncontrolled trial suggested positive results in men after administration of 200mg/day for 10 days; 7 however, a more recent randomised, crossover study comparing 60mg/day of saffron to on-demand sildenafil over 12 weeks reported disappointing results for saffron.8 It is worthy to note that wide variation of dose between the two studies; larger, well designed trials are needed to assess the efficacy of saffron in this area of men’s health.
Alzheimer’s diseaseA randomised, double-blind, controlled trial of
54 people over the age of 55 studied the effect of administration of 15mg BD of saffron in capsule form in comparison to donepazil (5mg BD).9 Outcomes were assessed as changes in the Alzheimer’s disease Assessment Scale-cognitive subscale (ADAS-cog) and Clinical Dementia Rating Scale-Sums of Boxes (CDR-SB) scores. Results showed similar effects in both groups after 22 weeks. Adverse events were at a similar frequency in both groups, although vomiting was significantly more common in the donepezil group.
An earlier randomised, double-blind, placebo-controlled study of 46 patients with mild to moderate Alzheimer’s disease was conducted to assess the safety and efficacy of saffron over a 16-week period.10 Patients were randomly assigned to receive a twice-daily capsule of saffron (15mg of dried ethanol-extracted stigma) or placebo. Patients were assessed using the ADAS-cog and CDR-SB measures and showed significant improvement compared to placebo at the endpoint. According to the authors, adverse events were mild to moderate and did not result in any dropouts.
Premenstrual syndromeA randomised, placebo-controlled, double-blind trial
compared the administration of 30mg/day of saffron
(15mg capsule twice daily) to placebo in 50 women aged 20-45.11 The authors included women who had regular menstrual cycles but with symptoms of PMS for at least six months prior to the study. Baseline data was gathered over two cycles followed by administration of treatment for a further two cycles. Outcomes measured were the Daily Symptom Report of 17 symptoms as well as the HAM-D scale. Seventy-six percent of the saffron group reported a reduction in PMS symptoms of 50% or more compared to 8% of the placebo group (p<0.0001). Furthermore, 60% of the saffron group reported a positive response (i.e. greater than 50% reduction in symptoms) as measured on the HAM-D scale compared with 4% of the placebo group (p<0.0001).
Retinal diseaseThere has been one small (n=25) placebo-controlled
clinical trial studying the effect of saffron supplementation (20mg/day for 90 days) in the treatment of age-related macular degeneration. 12 The primary measure of outcome was a change in retinal flicker sensitivity as assessed using focal electroretinograms (fERGs). The results were positive for the saffron group as compared to placebo. The authors concluded replication of this trial was warranted to determine clinical significance.
Weight lossA proprietary product, Satiereal® capsules (Inoreal
Ltd, Plerin, France), was tested in a small randomised placebo-controlled trial of 60 mildly overweight (weight 73.9kg ± 1.7kg, BMI 26.8 ± 0.1 kg/m²), otherwise healthy women (age range 25-45 years).13 Each woman was given either 2 capsules of Satierial® or placebo with no caloric restriction for a period of eight weeks. The Satiereal® was made by extracting 120g of dried stigma in 1200ml of 30% ethanol then dried to produce a capsule containing 88.25mg of the dried extract. The study did not report standardisation. Primary outcomes were body weight and snacking events. The group taking the Satierial® showed a 55% reduction in snacking events compared to 28% reduction in the placebo group with small loss of body weight (0.96kg ±0.26 compared with 0.01 ± 0.26 for the placebo group). The authors postulated this may be due to a positive effect of saffron on mood suggesting this study may highlight a possible use for saffron in patients with mood-related weight problems.
Future possibilitiesAlthough randomised controlled trials are lacking,
saffron has shown some promise in the areas of male fertility, and cancer prevention and treatment. The effects of saffron supplementation on semen parameters were evaluated in an uncontrolled study.14 After three months of taking 50mg of saffron three times per week, sperm morphology and motility had improved, but not sperm count.
Preliminary in vivo and in vitro research into the

Australian Journal of Herbal Medicine 2014 26(1)
20 © National Herbalists Association of Australia 2014
Article
antioxidant and antitumour properties of saffron or its active constituent crocin has highlighted potential in the prevention or treatment of cancer via reduced cell proliferation and progression along with increased cell apoptosis; however, further research is required.15, 16
DoseTo date, all randomised controlled trials have used
saffron at a dose of 30mg of dried ethanol extract of stigma in capsule form.4-6, 9-11 Where reported, standardisation has been to 0.13-0.15mg of safranal and 1.65-1.75mg of crocin.9, 10
ToxicityBased on in vivo and in vitro testing, saffron is
considered to be non-toxic.17
Adverse reactionsThere are no large-scale long term clinical trials
incorporating an examination of adverse reactions. A 2013 randomised, placebo controlled, double-
blind study evaluating the use of saffron in women taking 40mg of fluoxetine for major depressive disorder reported similar frequency and type of side effects between the two groups.5 Side effects reported by the authors included changes to appetite, nausea, dizziness, insomnia, headache, sedation and sore throat; however, the authors concluded that the saffron treatment was as safe as the fluoxetine treatment. Another recent paper looked at systematic reviews specifically for the purpose of identifying adverse effects of herbal medicine.18 In this paper, the authors noted Crocus sativus had adverse effects of allergic reaction and dermatitis but these were considered to be very minor.
Interactions, contraindications and precautions
There is limited research examining the safety profile of saffron as a medicinal herb or its potential for herb/drug interactions. One small double-blind, placebo-controlled study looked at the effects of administration of 200mg or 400mg tablets of saffron stigma in healthy adults for one week.19 In this study, it was noted that standing systolic blood pressure and mean arterial pressures decreased significantly in the group receiving 400mg/day. This study highlights a potential risk in patients with low blood pressure or taking medication for the lowering of blood pressure. The same study also reported some other changes to haematological measures including haemoglobin, haematocrit, platelets and red blood cells.19 Although they were considered to be within normal ranges, the authors suggested further research is required to establish whether these changes would be significant in patients with low blood counts or other haematological concerns.
A more recent small randomised, double-blind, placebo-controlled trial evaluated the safety of the
saffron-constituent, crocin, in healthy volunteers, administering 20mg/day of crocin for one month.3 A broad range of blood and urine parameters were measured. The parameters which showed any significant change were a decrease in amylase, partial thromboplastin time and MXD% (monocytes, eosinophils and basophils). The clinical relevance of this was not discussed and further studies at higher doses and for longer duration were recommended by the authors.
Pregnancy and lactation useThere is a lack of data determining the safe use of
saffron in pregnancy or lactation and so its use is not recommended.17
ConclusionTo date, a systematic review suggests saffron is
an effective thymoleptic for the treatment of mild to moderate depression. It has been demonstrated to be as effective as fluoxetine or imipramine with a similar or better tolerance profile. Current research also suggests that saffron shows some promise for the treatment of sexual dysfunction, Alzheimer’s disease, premenstrual syndrome, retinal disease and weight loss. Further research will add to this body of knowledge as it becomes available.
References1. Aytekin A, Acikgoz AO. 2008. Hormone and Microorganism
Treatments in the Cultivation of Saffron (Crocus Sativus L.) Plants Molecules 13(5):1135–47.
2. Akhondzadeh BA, Ghoreishi S, Noorbala AA, Akhondzadeh S, Rezazadeh S. 2008. Petal and Stigma of Crocus sativus L. in the Treatment of Depression: A Pilot Double-blind Randomized Trial. J Med Plants 7(4):29–36.
3. Mohamadpour AH, Ayati Z, Parizadeh M-R, Rajbai O, Hosseinzadeh H. 2013. Safety Evaluation of Crocin (a constituent of saffron) Tablets in Healthy Volunteers. Iran J Basic Med Sci 16(1):39–46.
4. Dwyer A, Whitten DL, Hawrelak JA. 2011. Herbal medicines, other than St. John’s Wort, in the Treatment of Depression. Altern Med Rev 16(1):40–9.
5. Kashani L, Raisi F, Saroukhani S, Sohrabi H, Modabbernia A,NasehiA-A, et al. 2013. Saffron for treatment of fluoxetine-induced sexual dysfunction in women: randomized double-blind placebo-controlled study. Hum Psychopharmacol 28(1):54–60.
6. Modabbernia A, Sohrabi H, Nasehi A-A, Raisi F, Saroukhani S, JamshidiA, et al. 2012. Effect of saffron on fluoxetine-inducedsexual impairment in men: randomized double-blind placebo-controlled trial. Psychopharmacology (Berl) 223(4):381–8.
7. Shamsa A, Hosseinzadeh H, Molaei M, Shakeri MT, Rajabi O. 2009. Evaluation of Crocus sativus L. (saffron) on male erectile dysfunction: a pilot study. Phytomedicine 16(8):690–3.
8. SafarinejadMR, ShafieiN, Safarinejad S. 2010.An open label,randomized, fixed-dose, crossover study comparing efficacy andsafetyof sildenafil citrate and saffron (Crocus sativus Linn.) for treating erectile dysfunction in men naïve to treatment. Int J Impot Res 22(4):240–50.
9. Akhondzadeh S, Shafiee Sabet M, Harirchian MH, Togha M,Cheraghmakani H, Razeghi S, et al. 2010. A 22-week, multicenter, randomized, double-blind controlled trial of Crocus sativus in the treatment of mild-to-moderate Alzheimer’s disease. Psychopharmacology (Berl) 207(4):637–43.

Australian Journal of Herbal Medicine 2014 26(1)
21© National Herbalists Association of Australia 2014
Article
10. Akhondzadeh S, Sabet MS, Harirchian MH, Togha M, Cheraghmakani H, Razeghi S, et al.2010. Saffron in the treatment of patients with mild to moderate Alzheimer’s disease: a 16-week, randomized and placebo-controlled trial. J Clin Pharm Ther 35(5):581–8.
11. Agha-Hosseini M, Kashani L, Aleyaseen A, Ghoreishi A, Rahmanpour H, Zarrinara AR, et al. 2008. Crocus sativus L. (saffron) in the treatment of premenstrual syndrome: a double-blind, randomised and placebo-controlled trial. BJOG 115(4):515–9.
12. Falsini B, Piccardi M, Minnella A, Savastano C, Capoluongo E, FaddaA, et al. 2010. Influence of saffron supplementation onretinalflickersensitivityinearlyage-relatedmaculardegeneration.Invest Ophthalmol Vis Sci 51(12):6118–24.
13. Gout B, Bourges C, Paineau-Dubreuil S. Satiereal. 2010. a Crocus sativus L extract, reduces snacking and increases satiety in a randomized placebo-controlled study of mildly overweight, healthy women. Nutr Res 30(5):305–13.
14. Heidary M, Vahhabi S, Reza Nejadi J, Delfan B, Birjandi M, Kaviani H, et al.2008. Effect of saffron on semen parameters of infertile men. Urol J 5(4):255–9.
15. Zhang Z, Wang C-Z, Wen X-D, Shoyama Y, Yuan C-S. 2013. Role of saffron and its constituents on cancer chemoprevention. Pharm Biol 51(7):920–4.
16. D’Alessandro AM, Mancini A, Lizzi AR, De Simone A, Marroccella CE, Gravina GL, et al. 2013. Crocus sativus stigma extract and its major constituent crocin possess significantantiproliferative properties against human prostate cancer. Nutr Cancer 65(6):930–42.
17. Natural Standard. 2013. Saffron [Monograph]. Retrieved from: http://nhaa.naturalstandard.com/databases/herbssupplements/all/saffron.asp
18. Posadzki P, Watson L, Ernst E. 2013. Adverse effects of herbal medicines: an overview of systematic reviews. Clin Med 13(6).
19. Modaghegh M-H, Shahabian M, Esmaeili H-A, Rajbai O, Hosseinzadeh H. 2008. Safety evaluation of saffron (Crocus sativus) tablets in healthy volunteers. Phytomedicine 15(12):1032–7.
BioMedica Nutraceuticals Please visit www.biomedica.com.au or call P +61 2 9698 7683 for more information
• Mag FXTM contains multiple highly bioavailable forms of magnesium including magnesium citrate, magnesium
orotate and magnesium Chelazome® • Contains a unique blend of USDA certified organic
wholefoods providing natural sources of nutrients; derived from curry, guava, lemon, amla, holy basil and annatto• Mag FXTM contains natural, premium ingredients
selected to meet the highest benchmarks for quality• Mag FXTM Berry Complex also contains a blend of
sustainably sourced superfood berry extracts
Citrus Complex & Berry Complex
A comprehensive magnesium formula in a nutritive wholefood base
Mag FXTM

Australian Journal of Herbal Medicine 2014 26(1)
22 © National Herbalists Association of Australia 2014
Article
IntroductionSri Lanka has been gifted with a wide assortment of
plant species due to its location in the tropics as well as the variability of climatic zones. For generations, the plants have been consumed as cures for ailments, disease prevention or simply for the purpose of maintaining health and wellness. The range of diseases being treated through the herbal medicines has been diverse due to the vast array of flora and fauna available within the country.1-3 Although the methods of treatment and remedies have not been systematically documented, the preparation methods of the herbs have been transmitted verbally across the generations and can even be seen practiced to date.4-6 However, the need for scientific evidence in support of the traditional medicines has been highlighted as a necessity due to the increased demand from locals as well as overseas consumers in the form of tourists visiting the country for medical treatment through the traditional methods.7
When it comes to the local population, despite being a developing country, there is a significant rate of urbanization in Sri Lanka which comes hand-in-hand with an increased literacy level and a wider
exposure to science and technology.8-10 Thus, through the dissemination of science and the availability of information resources, the selection of indigenous medicines for medicinal treatment by local consumers has been observed to be based on scientific evidence rather than traditional knowledge which has been passed down the generations. Nevertheless, since a successful cure for diseases such as diabetes or cancer are virtually nonexistent in the Western medicinal equivalents, the tendency for individuals contracted with these diseases to seek alternative remedies has been observed to be on the rise – a trend which has greatly benefited Sri Lankan traditional medicinal practitioners due to the increase in the number of patients requesting their expertise for the cure or containment of such diseases.11,12
Compared with traditional Indian or Chinese herbal medicinal practices, the Sri Lankan counterpart has more unexplored territories which are open for scientific research. Although several thousands of years of clinical evidence exists on the efficacy of certain herbal remedies, the amount of scientific research done on the Sri Lankan traditional medicinal system is comparatively less. In addition, these indigenous medicines are yet to reach the
Evaluation of the antioxidant activity and additive effects of traditional medicinal herbs from Sri Lanka
Viduranga Y . Waisundara* †, Mindani I . Watawana** Institute of Fundamental Studies, Hantane Road, Kandy, Sri Lanka† Corresponding author details:Mailing address: Institute of Fundamental Studies, Hantane Road, Kandy, Sri LankaE-mail: [email protected]
Abstract
Background: Located in the tropics, Sri Lanka has an assortment of medicinal plants which have been utilised for generations. Despite the history, the therapeutic properties of many herbs have not been scientifically evaluated. Claims even exist that certain herbs have the potency to cure diseases such as diabetes.
Aim: This study was designed to evaluate the antioxidant activity of five selected Sri Lankan medicinal herbs which are commonly used as anti-diabetic remedies. The additive effects of the two most potent antioxidant herbs in combination with the remaining three were also explored.
Method: The leaves of the following herbs were authenticated for the study: Coccinia grandis, Costus specious, Desmodium gangeticum, Mimosa pudica and Psidium guava. The leaves were sun-dried and ground into powders. One gram of each herb was added to 20 mL of water at 1000C, cooled to room temperature, centrifuged, and the supernatant collected for analysis. DPPH scavenging activity and the total phenolic content were evaluated. For evaluation of the herbal combinations, the powders were added at a 1:1 weight ratio and the extracts were similarly prepared.
Results: Coccinia grandis and Costus specious had the highest DPPH scavenging activities and thus were combined with the remaining three herbs. Coccinia grandis had additive effects only on Desmodium gangeticum and Mimosa pudica, while Costus specious had additive effects on Desmodium gangeticum, Mimosa pudica as well as Psidium guava.
Conclusions: Coccinia grandis and Costus specious were identified as potent antioxidants capable of having additive effects on herbs which are less effective in this aspect.
Key words: Anti-diabetic, antioxidant, herbal medicine, Sri Lanka

Australian Journal of Herbal Medicine 2014 26(1)
23© National Herbalists Association of Australia 2014
Article
overseas masses since quality control measures for these remedies have not been implemented to date in order to be mass-produced to meet the regulatory standards involved in exporting.13 As a result, the application and availability of Sri Lankan medicines is mostly contained to the locals as well as medical tourists – despite the historical and contemporary claims on their efficacy.
As a step towards adding the scientific background to some of the commonly used herbal medicines of Sri Lanka, this study was carried out to investigate the antioxidant activity of the following five herbs which are mostly used for anti-diabetic purposes: Coccinia grandis, Costus specious, Desmodium gangeticum, Mimosa pudica and Psidium guava (Table 1).14-17 These herbs were selected primarily because only their leaves are being used for the treatment of the disease. In general, from a biochemical and environmental perspective, the leaf contains the highest amount of antioxidant compounds compared with the bark and the root since their contact with sunlight and its radiation effects is higher.18 As highlighted in literature, because of the tropical climate of Sri Lanka and the ample exposure to sunlight, the leaves contain more defenses, in the form of phytochemicals (i.e. antioxidants), to withstand the naturally harsh weather and environmental conditions – especially against solar radiation, which leads to them being more concentrated with compounds of therapeutic potential.19,20
As for the usage of these selected herbs, they are evergreen plants which are abundantly found in household backyards, making them readily available for consumption. Better yet, Costus specious, Desmodium gangeticum and Mimosa pudica are even considered weeds due to their potentially high growth rate.
Although these herbs are primarily used for anti-diabetic purposes, they are used as remedies for a wide variety of diseases – a characteristic which demonstrates the versatility of the herbs.21-23 The variety of diseases being treated also exhibits the availability of many bioactive compounds in these herbs with wide-ranging medicinal properties and applications.
It is also necessary to highlight that these herbs are most often consumed as concoctions. The scientific basis behind these combinations of herbs requires further elucidation, although from traditional knowledge, it may be assumed that the optimum ratios were ascertained merely through trial-and-error. However, in this study, the herbal concoctions were prepared solely based on the antioxidant activity of the individual herbs.
The two herbs with the highest antioxidant activities were separately added to the remaining three, resulting in six concoctions consisting of two herbs each, to observe any synergistic, antagonistic or additive effects. The DPPH radical scavenging activity assay was selected to determine the antioxidant capacity of the herbs and the concoctions. The total phenolic content was determined
of the herbs and the concoctions as well.In summary, for the first time, the antioxidant activity
of some popular Sri Lankan herbs was revealed in this study. The synergistic, antagonistic or additive effects of the herbal combinations prepared using these herbs was also clearly elucidated. As a result, the study could be considered as a stepping stone for identification and screening of herbs which have a significant antioxidant potency, providing a focal point for future studies for further identification and isolation of novel compounds.
MethodsAll chemicals used for this study were purchased
from Sigma-Aldrich (Bangalore, India), Fluka (USA) or Sigma Chemicals (USA) unless otherwise specified.
Preparation of Herb Extracts and ConcoctionsThe aerial parts of Coccinia grandis (CG), Costus
specious (CS), Desmodium gangeticum (DG), Mimosa pudica (MP) and Psidium guava (PG) were collected from the central province of Sri Lanka and identified by comparison with the respective herbarium specimen available at the National Herbarium of the Peradeniya Botanical Gardens in Kandy, Sri Lanka. A voucher specimen was deposited at the Institute of Fundamental Studies, Hantane Road, Kandy, Sri Lanka. The herbs were intensively sun-dried for 8 hours and ground to powder. Twenty milliliters of water at 600C was added to one gram each of the powders to prepare a decoction and allowed to cool to room temperature at 250C. The mixtures were centrifuged at 1000 rpm and the supernatants were separated for analysis.
For preparation of the herbal combinations, the two herbs with the highest antioxidant activities were selected and their powders were added at a 1:1 weight ratio separately to each of the remaining three herbs. Altogether, six decoctions were formulated following the same method of preparation as the individual herbs. For the purpose of making comparisons, the two herbs with the highest antioxidant activities were combined with each other as well and subjected to the assays.
Determination of DPPH Radical Scavenging ActivityExtracts of individual herbs or herbal combinations
at concentrations of 100, 50, 25 and 12.5 µg/mL were prepared by dilution with 75 mM phosphate buffer (pH=7.40). A 96-well microplate was used for the analysis where 140 µL of the extracts of the individual herbs or the combinations were pipetted along with 60 µL of 400 µM DPPH (prepared in the phosphate buffer solution). Blank wells consisted of 200 µL of the phosphate buffer solution, while the control wells consisted of 140 µL of the phosphate buffer solution and 60 µL of the DPPH solution. The microplate was incubated at 370C for 30 min and the absorbance was measured at 517 nm using a Thermo Scientific Multiskan FC Microplate Reader. Each sample concentration was added in triplicates

Australian Journal of Herbal Medicine 2014 26(1)
24 © National Herbalists Association of Australia 2014
Article
into the microplate. Vitamin C was used as the positive control. The antioxidant activity was calculated as % DPPH radical scavenging activity by substituting the absorbance values into the following equation:
% DPPH Radical Scavenging Activity
=AbsControl - AbsExtract X 100
AbsControl
The % DPPH scavenging activity of 10 replicates of
each sample was used to calculate the EC50 values of the individual herbs and their combinations.
Determination of the Total Phenolic ContentThe method as described by Singleton and Rossi24 was
used for determining the total phenolic content of the extracts of the individual herbs and their combinations. However, the assay was carried out in the 96-well microplate format. Gallic acid was used as the standard to plot a curve where concentrations of 50.0, 25.0, 12.5,
Table 1: Images of the herbs selected for the study, their botanical & family names and their Sanskrit & Sinhala names of reference
Botanical name Family Sanskrit / Sinhala name Image of the Herb
Coccinia grandis Cucurbitaceae Kowakka
Costus specious Zingiberaceae Thebu
Desmodium gangeticum Fabaceae Undupiyaliya
Mimosa pudica Fabaceae Nidikumba
Psidium guava Myrtaceae Pera

Australian Journal of Herbal Medicine 2014 26(1)
25© National Herbalists Association of Australia 2014
Article
6.2 and 3.1 mg/mL were prepared by carrying out serial dilutions using deionized (DI) water. Extracts of the individual herbs or their combinations in concentrations of 100, 50, 25 and 12.5 µg/mL were prepared by dilution with DI water as well. The following constituent volumes were added to a single well: Folin-Ciocalteu reagent – 100 µL, sample / blank (DI water) / gallic acid standard – 20 µL, Na2CO3 (30g/L) – 80 µL. The microplate was incubated at room temperature for 15 min following which the absorbance was read at 540 nm using the Thermo Scientific Multiskan FC Microplate Reader.
Statistical AnalysisIBM SPSS Statistics version 21.0 (released on August
2012) for Windows was used for the calculation of the EC50 values of the herbs. Results were calculated and expressed as mean ± SEM of ≥3 independent analyses. P values of >0.05 were considered to be significant.
ResultsThe percentage inhibition of DPPH of the individual
herb concentrations, their EC50 values and the total phenolic contents are shown in Figure 1. In comparing the percentage inhibition of DPPH and the EC50 values, CG and CS had the highest antioxidant activities which did not have a statistically significant difference compared with vitamin C (P <0.05). This comparison showed that the antioxidant capacity of CG and CS was comparable with vitamin C. The total phenolic contents of all the herbs were observed to be proportionate to their DPPH radical scavenging activities. Based on these results, CG and CS were chosen to be added to DG, MP and PG to observe any synergistic, antagonistic or additive effects.
The percentage inhibition of DPPH of the herb combinations prepared with CG, their EC50 values and the total phenolic contents are shown in Figure 2. With the exception of PG, the rest of the two herbs showed additive effects in terms of the antioxidant activity in combination with CG. When combined with PG, it was observed that an antagonistic effect was initiated upon CG since the EC50 of CG+PG was statistically significantly lower than that of CG alone. Overall, none of the combinations displayed a synergistic effect. The total phenolic content had statistically significantly increased in the combinations of CG+DG and CG+MP compared with the individual herbs and the increase was proportionate to the observed EC50 values (P <0.05). The total phenolic content had increased even in the instance of CG+PG. With the exception of CG+PG, it could be hypothesized that the observed additive effects in terms of the antioxidant capacities were due to the increase in the total phenolic contents of the herbal combinations.
The percentage inhibition of DPPH of the herbal combinations prepared with CS, their EC50 values and the total phenolic contents are shown in Figure 3. All three herbs showed additive effects in terms of the antioxidant activity in combination with CS. It was noted that the
antagonistic effect of PG was absent when combined with CS, indicating that PG is better combined with CS than CG. Nevertheless, as with CG, none of the herbal combinations displayed a synergistic effect. In similar fashion as with CG, the total phenolic content of these combinations had also proportionately increased with the EC50 values indicating that the additive effect was due to the increased presence of phenolic compounds.
Figure 1: (A) The percentage inhibition of DPPH with the herb concentrations, (B) their EC50 values in comparison with vitamin C (*P <0.05 with vitamin C) and (C) the total phenolic contents. Results are expressed as the mean ± SEM.

Australian Journal of Herbal Medicine 2014 26(1)
26 © National Herbalists Association of Australia 2014
Article
As shown in both Figures 2 and 3, the EC50 value of CG+CS was not statistically significantly different from the EC50 values individual herbs. An antagonistic effect could have taken place given that the phenolic compounds of the combined extract was comparable to the total phenolic concentrations present in the individual herbs. However, this effect could be considered as being mild compared with the CG+PG combination where the
reduction in the percentage inhibition and the EC50 values was more evident.
DiscussionThis study focused only on determining the antioxidant
activity of selected herbs, along with determining one of the constituents (i.e. total phenolic content) present in all the extracts. Antioxidant activity has been identified
Figure 2: (A) The percentage inhibition of DPPH of the combinations of herbs with CG (B) their EC50 values in comparison with vitamin C (*P <0.05 with vitamin C, † P <0.05 with CG) and (C) the total phenolic contents. Results are expressed as the mean ± SEM.
Figure 3: (A) The percentage inhibition of DPPH of the combinations of herbs with CS (B) their EC50 values in comparison with vitamin C (*P <0.05 with vitamin C, † P <0.05 with CS) and (C) the total phenolic contents. Results are expressed as the mean ± SEM.

Australian Journal of Herbal Medicine 2014 26(1)
27© National Herbalists Association of Australia 2014
Article
as a characteristic which is mostly present in phenolic compounds. Thus, due to this correlation, only these two parameters were explored in this investigation. In addition, although the herbs have been traditionally used for anti-diabetic purposes, the rationale for assessing their antioxidant activity was simply because this aspect of the herbs has not been sufficiently elucidated in previous studies.25
The ability of these herbs to reduce blood glucose levels in diabetic patients has been clinically proven, and traditional medicinal practitioners of Sri Lanka have amassed a collection of case studies which provide substantial evidence as to their anti-hyperglycemic activity.26, 27 Therefore, addition of further evidence in support of their anti-hyperglycemic efficacies will only prove to be redundant, although investigating their mechanisms of action for lowering the blood glucose levels will be of scientific value. Thus, as an extension from the results of this investigation, the pharmacological effects of the herbs could be examined in future studies.
Another aspect which is worthy of exploring is the bioactive compounds present in the herbal extracts – especially CS and CG. An exhaustive characterization of the phytochemicals present in any of the herbs evaluated in this study has not been carried out to date. Despite the detection of phenolic compounds in this instance, it is possible that the bioactive compound(s) responsible for the anti-hyperglycemic and antioxidant effects belong(s) to a different category altogether. Given this void, it is vital to evaluate the aqueous extract of the herbs.
Generally, investigations being carried out on the identification of bioactive compounds tend to be carried out on various types of solvent extracts. However, it has to be borne in mind that the traditional medicinal decoctions were always prepared using water – either lukewarm or boiled.28 If the desired therapeutic effect
has been observed through clinical applications using the traditional means of preparing the herbs, it is obvious that the bioactive compound(s) could be extracted using water.
The traditional methods of herbal preparation and the frequency of administration to diabetic patients are shown in Table 2. Thus, the study was carefully carried out to mimic the actual preparation conditions when they are being consumed as medicines. The dried form of the herbs were used for analysis due to ease of preparation. Traditionally, it was the dried herbs which were utilized for decoctions because they were stored in medicinal halls as powders rather than in their fresh form which had a comparatively lower shelf-life.29 When conducting studies on traditional medicines, it is important to simulate the traditional methods of preparation – especially the form in which the medicine was used (dried or fresh) and the temperature conditions. There have been instances where the preparation methods have deviated or were modified owing to the usage of modern laboratory equipment, resulting in the complete destruction of the bioactivity of the phytochemicals and leading to inaccurate conclusions.31,32 Although primeval, the methods used by traditional practitioners for preparation of medicines have been tested and made perfect across generations of clinical trials, making it virtually impossible to match the level of optimization and accuracy through modern scientific interpretations.
Most Sri Lankans are able to identify the herbs growing within their area of residence. As a result, some local diabetic patients could be observed consuming these herbs to control their disease condition without the advice of a traditional medicinal practitioner as they are familiar with the usage of these herbs because of the traditional knowledge passed down by the ancestors. It has also been observed that diabetic patients nowadays tend to try out
Table 2: Traditional methods of preparation and frequency of administration of Coccinia grandis, Costus specious, Desmodium gangeticum, Mimosa pudica and Psidium guava . Some of the herbs have more than one method of preparation and administration .
Herb Traditional Method of Preparation and Administration
Coccinia grandisDecoction is prepared with 120g of dried or fresh leaves or the entire creeper added to 1 L of water and approximately 120 mL of the extract is administered twice per day
Costus specious
Decoction is prepared with approximately 20g of dried or fresh leave or the entire creeper added to 1 L of water and approximately 120 mL of the extract is administered twice per dayA salad is prepared where the leaves are cut into thin slices, added with scraped coconut, a pinch of salt, turmeric and mixed well . This salad is consumed with riceA rice porridge is prepared with the leaves and consumed in the morning
Desmodium gangeticum
Decoction is prepared with approximately 20g of dried or fresh leave or the entire creeper added to 1 L of water and approximately 120 mL of the extract is administered twice per dayA rice porridge is prepared with the leaves and consumed in the morning
Mimosa pudicaDecoction is prepared with 120g of dried or fresh leaves or the entire creeper and approximately 120 mL of the extract is administered twice per day
Psidium guavaDecoction is prepared with 120g of dried or fresh leaves or the entire creeper and approximately 120 mL of the extract is administered twice per day

Australian Journal of Herbal Medicine 2014 26(1)
28 © National Herbalists Association of Australia 2014
Article
combinations of medicinal herbs, anticipating a higher efficacy.33 As demonstrated through the combination of CG+PG and even CG+CS, these personal investigations may not necessarily have a positive outcome, especially due to the antagonistic effects of the phytochemicals present in either of the constituent herbs. Therefore, adhering to the traditional treatment methods, proportions and preparation techniques is an essential aspect for obtaining the desired therapeutic effects of the herbs.
ConclusionsIn conclusion, the study was able to successfully
demonstrate the antioxidant effects of Coccinia grandis, Costus specious, Desmodium gangeticum, Mimosa pudica and Psidium guava. The additive effects of Coccinia grandis and Costus specious was also elucidated. Although emphasised on only one aspect, the study could be considered as essential in view of the existing gap between traditional knowledge and scientific proof – a matter which requires resolution before dissemination of the traditional medicinal practices of Sri Lanka to the global market.
AcknowledgementsThe authors wish to acknowledge the support provided
by Dr. Lalith Jayasinghe of the Institute of Fundamental Studies, Kandy, Sri Lanka for the analytical support provided via the Thermo Scientific FC Multiskan plate reader.
References1. Devalaraja S, Jain S, Yadav H. 2011. Exotic fruits as therapeutic
complements for diabetes, obesity and metabolic syndrome. Food Res Int 44:1856-1865.
2. Attanapola WMIK, Udugama JMM, Jayasinghe-Mudalige UK. 2012. Determinants of the consumption of functional ingredients: Evidence from the professionals living in urban areas in Kurunegala district. Nutr Soc Sri Lanka 2012:18.
3. Buddhadasa R. 1962. Sushrutha Samahitha (text with Sinhala translation). Colombo, Sri Lanka. Department of Languages, University of Colombo.
4. Ediriweera ERHSS, Ratnasooriya WD. 2009. A review on herbs used in treatment of Diabetes Mellitus by Sri Lankan Ayurvedic and traditional physicians. Ayu 30:373-391.
5. Fernando MF, Thabrew I, Karunanayake EH. 1990. Hypoglycemic activity of some medicinal plants in Sri Lanka. Gen Pharm 21:779-782.
6. Fernandopulle BMR, Karunanayake EH, Ratnasooriya WD. 1994. Oral hypoglycemic effects of Mormordica charantia in rats. J Med Sci 22:137-139.
7. Karunanayake EH, Welihinda J, Sirimanna SR, Sinnadorai G. 1984. Oral hypoglycemic activity of some medicinal plants of Sri Lanka. J Ethnopharmacology 11:223-231.
8. Tissera HMA, Thabrew MI. 2001. Medicinal plants and Ayurvedic preparations used in Sri Lanka for the control of Diabetes Mellitus. Colombo, Sri Lanka: Department of Ayurveda, University of Colombo.
9. Karalliedde L, Gawarammana IB. 2008. Traditional Herbal Medicines: A guide to its safer use. London, United Kingdom: Hammersmith Press Ltd.
10. Kokil GR, Rewatkar PV, Verma A, Thareja S, Naik SR. 2010. Pharmacology and chemistry of diabetes mellitus and anti-diabetic drugs: A critical review. Curr Med Chem 17:4405-4423.
11. Patel DK, Kumar R, Laloo D, Hemalatha S. 2012. Natural medicines from plant source used for therapy of diabetes mellitus: An overview of its pharmacological aspects. Asia Pac J Trop Dis 2:239-250.
12. Tundis R, Loizzo MR, Menichini F. 2010. Natural products as alpha-amylase and alpha-glucosidase inhibitors and their hypoglycemic potential in the treatment of diabetes: An update. Mini Rev Med Chem 10:315-331.
13. Cakici I, Hurmoglu C. 1994. Hypoglycemic effect of Mormordica charantia extracts in normoglycemic or cyprohepatidine-induced hyperglycemic mice. J Ethnopharmacology 44:117-121.
14. Wijesinghe Y. 1994. Checklist of woody perennial plants of Sri Lanka. Colombo, Sri Lanka: Forestry Information Division, Forest Department.
15. Samad A, Shams MS, Ullah Z, Wais M, Nazish I, Sultana Y, Aqil M. 2009. Status of herbal medicines in the treatment of diabetes (review). Curr Diab Rev 5:102-111.
16. Shahidi F. 2004. Functional foods: Their role in health promotion and disease prevention. J Food Sci 69:R146-R149.
17. Tierney LM, McPhee SJ, Papadakis MA. 2002. Current medical Diagnosis & Treatment. New York, USA: Lange Medical Books/McGraw-Hill.
18. Rother KI. 2007. Diabetes treatment: Bridging the divide. N Engl J Med 356:1499-1501.
19. Marles RJ, Farnsworth NR. 1995. Anti-diabetic plants and their active constituents. Phytomedicine 2:133-139.
20. Chopra RN, Nayar SL, Chopra IC. 1956. Glossary of Indian Medicinal Plants. New Delhi, India: CSIR Publications.
21. Dhawan BN, Dubey MP, Mehrotra BN, Rastogi RP, Tandon JS. 1980. Screening of Indian plants for biological activity. Indian J Exp Biol 18:594-606.
22. Pietta PG. 2000. Flavonoids as antioxidants. J Nat Prod 63:1035–1042.
23. Bandaranayake WM, Sultanbawa MUS. 1991. A list of the endemic plants of Sri Lanka. Colombo, Sri Lanka: Forestry Information Division, Forest Department.
24. Singleton VL, Rossi JA. 1965. Colorimetry of total phenolics with phosphomolybdic-phosphotungstic acid reagents. Am J Enol Vitic 16:144-1658.
25. Ou B, Huang D, Hampsch-Woodill M, Flanagan JA, Deemer EK. 2002. Analysis of antioxidant activities of common vegetables employing oxygen radical absorbance capacity (ORAC) and ferric reducing antioxidant power (FRAP) assays: a comparative study. J Agric Food Chem 50:3122-3128.
26. Finkel T. 2000. Oxidants, oxidative stress and the biology of aging. Nature 408:239-248.
27. Halliwell B. 1996. Antioxidants in human and disease. Ann Rev Nutr 16:33-50.
28. Sultanbawa MUS, Wannigama GP, Bandaranayake WM, Kumar V, Gunatilaka AAL, Marikar FA, Balasubramaniam S, Arsecularatne SN. 1978. Chemical investigation of Ceylonese plants: A survey of plants of Sri Lanka (Ceylon) for alkaloids. J Nat Prod 41:597-633.
29. Kikuchi T, Matsuda S, Kadota S, Tai T. 1985. Studies on the constituents of medicinal and related plants in Sri Lanka: Novel sesquilignans from Hedyotis lawsoniae. Chem Pharm Bull 33:1444-1451.
30. Jayasinghe ULB, Kumarihamy BMM, Bandara AGD, Vasquez EA, Kraus W. 2003. Nematicidal activity of some Sri Lankan plants. Nat Prod Res 17:259-262.
31. Leong LP, Shui G. 2002. An investigation of antioxidant capacity of fruits in Singapore markets. Food Chem 76:69-75.
32. Bandara BMR, Illangasekara NK, Jayasinghe ULB, Karunaratne V, Wannigama GP, Bokel M, Kraus W, Sotheeswaran S. 1990. Isolation of phaeanthine from Cyclea burmanni. Planta Medica 56:245-246.
33. Jayasinghe ULB, Bandara AGD, Hara N, Fujimoto Y. 2001. A new norneohopane caffeate from Filicium decipiens. Fitoterapia 72:737-742.

Australian Journal of Herbal Medicine 2014 26(1)
29© National Herbalists Association of Australia 2014
Case Study
Introduction ‘Dave’ was aged 52 when he came for a naturopathic
consultation. He was a self-employed sole parent with two teenage children. His primary complaint was digestive upset with intestinal bloating, abdominal pain and frequent bouts of diarrhoea. Dave had been diagnosed with ulcerative colitis (UC) seven years earlier and felt that his current condition was a ‘flare’ that had lasted six months. He was not taking any medication to manage his symptoms and had last taken Mesalamine (Pentasa) five years ago. Six months ago Dave had changed to a Palaeolithic diet and reported that his symptoms had begun around the same time.
Ulcerative colitis is a chronic inflammatory bowel disease (IBD) characterized by inflammation of the mucosal lining of the colon.1 UC is increasing in incidence and prevalence in many parts of the world, including Australia, North America and Northern Europe.2 In Australia there has been an 11-fold increase in the incidence of UC since the early 1990s.3 Signs and symptoms commonly experienced include bloody diarrhoea with or without mucus, urgency/tenesmus, fever, abdominal pain, anorexia, arthralgia and weight loss.2 Risk factors of developing UC include recent Salmonella or Campylobacter infection, living in a Western country, living at higher latitudes and a family history of inflammatory bowel disease.4
There are many predisposing factors associated with the development of UC, including vitamin D deficiency.5 UC is most prevalent in northern climates and high incidence of low serum vitamin D levels are also observed in these regions.5 The use of non-steroidal anti-inflammatories is also associated with increased number of relapses in
UC patients6 and individuals who have undergone an appendectomy are at 69% less risk of developing UC.6 A diet high in animal protein increases both the risk of developing inflammatory bowel disease and of suffering subsequent relapses.7 Additionally a diet high in omega 6 polyunsaturated fatty acids predisposes individuals to UC whilst omega-3 fatty acids are considered to be protective.7 A diet high in soluble and fermentable fibre, especially fruit reduces the risk of Crohn’s disease (CD) but is not protective against UC.8 Dave had never smoked but interestingly smoking is protective against UC with smokers 40% less likely to develop the condition.6 Smoking, however, can induce the onset of (CD) and increase the severity and progression of the disease.9
On further questioning, it was established that Dave was experiencing anorexia, increased urgency and frequency to defecate, watery stools and left-sided lower abdominal pain. Dave was moving his bowels two to three times a day and the stool would vary from soft to liquid. In the last eight weeks bright red blood and mucus were also intermittently in the stool. In the eight weeks prior to the consultation Dave had further restricted his diet by eating minimal dairy foods, which reduced the incidences of bloating. Dave was tired (rating his energy levels at 6/10) and reported that he was experiencing weight loss but was unsure how much as he had not weighed himself recently. Dave had not been to see his general practitioner (GP) or gastroenterologist and had been taking an over the counter multi-vitamin and cod liver oil for the last four months.
Medical history Dave was diagnosed with UC seven years ago after
a colonoscopy found the sigmoid colon was affected. In
The integrated treatment of Blastocystis hominis in a patient with ulcerative colitis: a case study
Susan Hunter Sunnybrook Healing Clinic, Melbourne, Australia 553A North Road, Ormond, 3204 Phone: 0410 957 059 Email: [email protected]
Abstract: Blastocystis hominis is a common protozoan in the human intestinal tract that can cause anorexia, diarrhoea and abdominal pain. Ulcerative colitis is a chronic inflammatory bowel disease that, when active, may present with similar signs and symptoms to a Blastocystis infection. A patient with ulcerative colitis presented with anorexia, increased urgency and frequency of defecation. He had watery, bloody stools with mucus and left-sided lower abdominal pain. Further testing was required to identify the cause of symptoms. A stool test detected Blastocystis hominis and blood tests indicated inflammatory markers were within range, ruling out an ulcerative colitis flare. Treatment included the use of metronidazole, Saccharomyces boulardii, Lactobacillus rhamnosus (HN001), Bifidobacterium animalis spp. lactis BB-12, Lactobacillus acidophilus LA-5 and anti-parasitic herbs and was successful in resolving all digestive symptoms. Taking an integrated approach with antibiotic therapy, probiotics and anti-parasitic herbs may be an effective treatment for eradication of Blastocystis hominis in the symptomatic patient.

Australian Journal of Herbal Medicine 2014 26(1)
30 © National Herbalists Association of Australia 2014
Case Study
the past, UC flares would last for two months then stop. Dave mentioned that he thought that stress was the main trigger for flare-ups of the disease.
Family and social historyDave was a sole parent with two teenage children and
reported that when parenting became stressful in the past it had been a trigger for flare-ups. He felt that currently stress was not an issue.
Dave was keen to remain on the Palaeolithic diet. His diet included red meat (4/7 days), poultry (3/7 days), eggs (4/7 days) and fish (1/7 days). He ate a variety of vegetables and 2-3 serves of fruit a day. Dave consumed nuts, seeds, psyllium husks, coconut oil and coconut milk daily. Dave did not drink caffeinated drinks and rarely drank alcohol. He did struggle to drink water. Dave reported that his sleep was good and he exercised five times a week.
Pathology & investigation No testing to investigate Dave’s symptoms had been
conducted in the last 12 months.
Observations and physical examination Dave is of Anglo-Australian descent. He weighed 70kg
and was 178cm tall (BMI of 22.1). His blood pressure was normal at 120/80. On examination Dave reported tenderness in the left lower quadrant on palpation.
Provisional diagnosis Dave was presenting with many of the symptoms of
an UC flare, however there was the possibility that he may have a bowel infection.
Treatment Based on Dave’s symptoms he was prescribed a
nutritional and herbal formula (Gut Relief, Nutrition Care Pharmaceuticals, Keysborough Australia)
Each 5gm contains:
Glutamine 2 .5gm
Quercetin 200mg
Glucosamine hydrochloride 500mg
Aloe barbadensis leaf extract equivalent 500mg
Ulmus rubra (Slippery elm) bark powder 500mg
Guar gum 100mg
Pectin 100mg
Sodium phosphate dibasic 260mg
Peppermint oil 3mg
Cumerone® providing Curcumin (total curcuminoids approx . 3 .705mg)
3 .037mg
Dose: One teaspoon morning and night to reduce inflammation of the gastric mucosa.
Dave was also prescribed a supplement containing Saccharomyces boulardii and Lactobacillus rhamnosus.
The supplement (Ultra flora SB Dysbiosis, Health World, Northgate, Australia) contained the following:
Saccharomyces cerevisiae (Boulardii) 7 .5 billion CFU (organism)
Lactobacillus rhamnosus (HN001) 500 million CFU (organism)
Dose: 2 capsules morning and night after meals. Dave was to continue taking one teaspoon a day of
his cod liver oil as omega-3 fatty acids have been found to suppress inflammatory responses in UC.10 Nordic Naturals arctic cod liver oil contained: purified arctic cod liver oil, d-alpha tocopherol and rosemary extract. Each 5ml dose contains:
EPA (eicosapentanoic acid) 410mg
DHA (docosahexaenoic acid) 600mg
Other omega-3’s 225mg
Oleic acid (omega 9) 600mg
It was recommended that Dave reduce his red meat and chicken intake, fill in a diet diary and take a re-hydration formula daily to reduce electrolyte loss caused by the frequent loose stool. Dave’s relatively high meat intake was a concern as high omega-6 fatty acid intake and meat intake have been found to increase risk of developing, or relapse of, UC.10
Further investigation After the initial consultation further testing was
suggested, including stool testing to look at lactoferrin levels and the presence of pathogenic infection. Increased lactoferrin levels have been shown to be associated with chronic inflammation and relapses in IBD.11 Calprotectin may have also been a useful test to conduct as calprotectin can differentiate between active and inactive UC and between IBD and irritable bowel syndrome and therefore may predict relapse especially in UC.11
The test results provided some interesting insights as to why Dave experienced the signs and symptoms he did. A three-day stool parasitology found Dave was positive for Blastocystis hominis. Other results included:
S 25OH Vitamin D 38 nmol/L (ref . range 75-250)
High sensitivity CRP 1 .6 mg/L (ref . range <5)
ESR 12 mm/hr (ref . range 2-14)
Plasma Zinc 9 umol/L (ref . range 9-19)
Plasma Copper 10 .2 umol/L (ref . range 11-22)
Iron 32 umol/L (ref . range 5-30)
Ferritin 102 ng/ml (ref . range 30-500)
Trf Sat 53% (ref . range 10-45)
Total red cell folate 1663 nmol/L (ref . range >800)
Total vitamin B12 476 pmol/L (ref . range 200-700)
Urea Creatinine ratio 49%
Fasting Blood Glucose 5 .7 mmol/L (ref . range 3 .6-6)

Australian Journal of Herbal Medicine 2014 26(1)
31© National Herbalists Association of Australia 2014
Case Study
Cholesterol 6 .5 mmol/L (ref . range 3 .5-5 .5)
LDL –CHOL 4 .3 mmol/L (ref . range <3 .5)
HDL -CHOL 1 .79 mmol/L (ref . range >1)
Slightly elevated serum iron was most likely due to high red meat intake. Dave’s ESR and high sensitivity CRP levels were in range indicating no evidence of an UC flare. Vitamin D was very low. Interestingly, despite a high protein diet, Dave’s urea creatinine ratio indicated low protein uptake and his zinc levels were borderline low. Dave’s cholesterol levels were high and his intake of red meat was more than likely contributing to this.
The treatment focus at this point was to eradicate the Blastocystis hominis as its presence may be the reason for Dave’s gastrointestinal symptoms. The focus was to enhance non-specific host immunity by improving colonic microflora, colonic mucous layer and general immunity. It was also important to address Dave’s vitamin D levels. Low vitamin D is common in IBD and improving levels has been found to reduce the severity of colitis by down-regulating genes associated with tumour necrosis factor-α, an important anti-inflammatory cytokine.12
Follow up At his follow up appointment Dave reported the stool
firmed up initially but had deteriorated since. Watery stools were returning less frequently. Dave was now moving his bowels twice a day. The urgency to go was still present. There had been no blood or mucus in the stool. The anorexia continued but without further weight loss. Dave had not used a re-hydration formula or reduced his red meat intake as recommended.
The GP had prescribed metronidazole (Flagyl). We discussed success of eradication using antibiotics, as a recent review found that metronidazole was successful in achieving 88% clinical remission and 80% six month faecal clearance; however, at the 6-month follow-up an elevated occurrence of parasitological relapses was observed.13 The use of herbal anti-parasitics was also discussed and Dave chose to take the Flagyl and to follow up with herbs to increase the possibility of eradication and successful treatment.
TreatmentThe previously prescribed treatment of Gut Relief
and Ultra Flora SB Dysbiosis was continued. The Saccharomyces cerevisiae (boulardii) was well indicated as it has been found to have a 94% clinical cure rate when administered with Flagyl.14
The following supplements were added to the prescription: Vitamin D drops (D3 Drops Forte, Fit-Bioceuticals, Alexandria, Australia), 8 drops a day (8000IU/day).
Cholecalciferol equivalent to Vitamin D3
25 μg1000IU
A probiotic was added to the prescription (Eagle Intestobalance, Integria Health Care, Eight Mile Plains, Australia) at two capsules a day.
Bifidobacterium animalis spp . lactis BB-12 12 .5 billion CFU (organisms)
Lactobacillus acidophilus LA-5 12 .5 billion CFU (organisms)
A zinc supplement was prescribed (Zinc citrate, Bio Concepts, Eagle Farm, Australia) at 1 capsule a day. Each capsule contains:
Zinc citrate dehydrate 30mg
A herbal anti-parasitic was also prescribed to follow the course of Flagyl once it had been completed. Herbs with strong Blastocystis hominis eradication activity such as Coptis chinensis and Punica granatum were difficult to source for treatment so Dave was to take an alternative herbal formula at 2 capsules three times a day for six weeks. Each capsule (Bactrex, Healthworld, Northgate, Australia) contained:
Phellodendron amurense stem bark dry (phellodendron)
750mg
Origanum vulgare leaf essential oil (oregano) 100mg
Syzgium aromaticum leaf essential oil (clove) 50mg
Thymus vulgaris flowering herb essential oil (thyme)
50mg
The formula was selected as Phellodendron amurense and Origanum vulgare leaf essential oil have been found to inhibit and reduce Blastocystis hominis growth and replication.15,16 Dave was also crushing and consuming two cloves of fresh garlic (Allium sativum) twice a day for to its strong inhibitory effect on Blastocystis hominis.17 He was also consuming 3gm of Nigella sativa seeds morning and night as part of eradication because of Nigella’s inhibitory effects found in an in vitro study.18
Dave was to focus on eating a high soluble fibre diet and aim to drink three to four cups of organic green tea (sourced from Southern Light, Maldon, Australia) a day. The green tea was added to reduce colonic pH, assist in increasing Lactobacilli and Bifidobacterium species in the bowel and to increase production of short chain fatty acids (SCFAs).19
Follow up At our follow up appointment Dave reported that he
tolerated Flagyl, Bactrex, garlic and nigella seeds well. He was symptom-free. The stool was much firmer and the urgency to move his bowels was gone. He no longer had bloating and his appetite was back, having gained two kilograms. The abdominal pain was also gone and there

Australian Journal of Herbal Medicine 2014 26(1)
32 © National Herbalists Association of Australia 2014
Case Study
was no blood or mucus in his stool. Dave was sporadic with drinking the green tea. He had not increased his consumption of high fibre foods and wanted to continue being grain-free.
TreatmentThe focus now was to improve bowel bacteria and
correct nutritional deficiencies. Dave continued on the previous script but stopped the anti-parasitic formula. Dave was asymptomatic and did not want to continue with eradication treatment. The Gut Relief powder was discontinued. The vitamin D was reduced to 5000IU a day to be reviewed in three months.
No follow up testing Dave did not return for a follow up despite the
importance of addressing gut repair, nutritional deficiencies, the current diet and hypercholesterolaemia. Intestinal Permeability testing (lactulose/mannitol test) or faecal calprotectin and lactoferrin testing may have been useful in this case as disruptions of essential elements of the intestinal barrier lead to permeability defects which exacerbate the immune system and result in tissue damage in IBD.20 Increased intestinal permeability and faecal calprotectin are reliable markers for mucosal healing.11 A follow-up stool test would have determined if Blastocystis had been eradicated. Dave was satisfied with being symptom free and not continuing treatment beyond the last prescription.
Discussion When seeing a case with long-standing digestive
symptoms in a patient with UC the initial conclusion drawn would be that the UC is active. It is always important to consider other differential diagnoses and carry out pathology tests to rule out other causes or contributing factors. ESR and CRP were not elevated ruling out an UC flare and in this case Blastocystis hominis was present.
Whether the presence of Blastocystis requires treatment is contentious. It is one of the most common parasites found in humans, colonizing between one and two billion people globally.21 Clinical significance is now thought to be reliant on subtype of the parasite.22 However, testing methods to identify subtypes were not available at the time of this case. Studies have found Blastocystis in individuals displaying gastrointestinal symptoms, but it has also been detected in an almost equal number of people that remain asymptomatic.22 Despite the presence of controversy as to the clinical effects of Blastocystis, it was considered important to eradicate the infestation in this case due to the possibility that it was causing the patient’s symptoms, and its potential effects on the colon which may in turn increase the UC symptoms.23
The use of antibiotic therapy and/or herbal anti-parasitic therapy is another interesting consideration in a case like this. The success rate of antibiotic therapy varies,
with 22-100% efficacy rate using metronidazole in some studies22 while others found very low eradication rates, with one study finding no patients clearing the organism following treatment with metronidazole or trimethoprim/sulfamethoxazole.24 There is also the possibility of dysbiosis developing post treatment. The use of herbal anti-parasitic therapy is promising, but the success of using herbs has not been studied extensively. The use of Nigella sativa and Allium sativum have, however, been found to be more effective than metronidazole treatment for stopping the growth of Blastocystis hominis.17,18 The two treatment approaches can be used effectively together and have been shown to have high clinical success and parasitological cure rates when treating patients with metronidazole and Saccharomyces boulardii.14
In conclusion, this case is a reminder that it is vital to look beyond the obvious to consider other possible diagnoses. By taking an integrated approach to Blastocystis hominis eradication complete symptom resolution and pathogen clearance is a possibility.
References1. Torres J, Danese S, Colombel JF. 2013. New therapeutic avenues
in ulcerative colitis: thinking out of the box. Gut 62(11):1642-52.2. Danese S & Fiocchi, C. 2011. Ulcerative Colitis. N Engl J Med
365:1713-25.3. Schildkraut V, Alex G, Cameron DJ, Hardikar W, Lipschitz B,
Oliver MR, Simpson DM, Catto-Smith AG. 2013. Sixty year study ofincidenceofchildhoodulcerativecolitisfinds11foldincreasebeginning in 1990s. Inflamm Bowel Dis 19(1):1-6.
4. Adams SM, Bornemann HM. 2013. Ulcerative Colitis. Am Fam Physician 87(10)699-705.
5. Nicholson I, Dalzell MA, El-Matary W. 2012. Vitamin D as a therapy for colitis: A systematic review. J Crohns Colitis 6(4):405-11.
6. Di Sabatino A, Biancheri P, Rovedatti L, MacDonald TT, Corazza GR. 2012. Recent advances in understanding ulcerative colitis. Intern Emerg Med 7(2):103-11.
7. Andersen V, Olsen A, Carbonnel F, Tjønneland A, Vogel U. Diet and riskofinflammatoryboweldisease.Dig Liver Dis 44(3):185-94.
8. Anthankrishnan AN, Khalili H, Konijeti GG, Higuchi LM, de Silva P, Korzenik JR, Fuchs CS, Willett WC, Richter JM, Chan AT.2013.Aprospectivestudyoflong-termintakeofdietaryfiberand risk of Crohn’s disease and ulcerative colitis. Gastroenterology 145(5):970-7.
9. Kennelly RP, Subramaniam T, Egan LJ, Joyce MR. 2013. Smoking andCrohn’sDisease:Activemodificationof an independent riskfactor (Education alone is not enough). J Crohns Colitis 7(8):631-5.
10 Sung MK, Park MY. 2013. Nutritional modulators of Ulcerative Colitis: Clinical efficacies and mechanistic view. World J Gastroenterol 19(7):994-1004.
11. Stragier E, Van Assche G. 2013. The use of fecal calprotectin and lactoferrin in patients with IBD: review. Acta Gastroenterol Belg 76(3):322-8.
12. Mouli VP, Ananthakrishnan AN. 2014. Review article: vitamin D and inflammatory bowel disease. Aliment Pharmacol Ther 39(2):125-36.
13. Sekar U, Shanthi M. 2013. Blastocystis: Consensus of treatment and controversies. Trop Parasitol 3(1):35-9.
14. Dinleyici EC, Eren M, Dogan N, Reyhanioglu S, Yargic ZA. 2011. Saccharomyces boulardii or metronidazole in symptomatic children with Blastocystis hominis infection. Parasitol Res 108(3):541-5.
15. Yang LQ, Mulkit Singh EH, Yap GC, Xu HX, Sim KY. 1996. In

Australian Journal of Herbal Medicine 2014 26(1)
33© National Herbalists Association of Australia 2014
Case Study
vitro response of Blastocystis hominis against traditional Chinese medicine. J Ethnopharmacol 55(1):35-42.
16. Force M, Sparks WS, Ronzio RA. 2000. Inhibition of enteric parasites by emulsified oil of oregano in vivo. Phytother Res 14(3):213-4.
17. Yakoob J, Abbas Z, Beg MA, Naz S, Awan S, Hamid S, Jafri W. 2011. In vitro sensitivity of Blastocystis hominis to garlic, ginger, white cumin and black pepper in the diet. Parasitol Res 109(2):379-85.
18. El-Wakil SS. 2007. Evaluation of the in vitro effect of Nigella sativa aqueous extract on Blastocystis hominis isolates. J Egypt Soc Parasitol 37(3):801-13.
19. Goto KS, Kanaya S, Nishikawa, T. 1998. The influence of teacatechins on fecal flora of elderly residents in a long-term carefacilities. J Nutr Sci Vitaminol 45(1):135-41.
20. Salim SY, Soderholm, JD. 2011. Importance of disrupted intestinal barrier in inflammatory bowel disease. Inflamm Bowel Dis 17(1):362-81.
21. Scanlan PD, Stansvoid CR. 2013. Blastocystis: Getting to grips with our guileful guest. Trends Parasitol 29(11):523-9.
22. Stansvold CR, Nielsen HV, Molbak K, Smith HV. 2009. Pursuing theclinicalsignificanceofBlastocystis–diagnosticimplications. Trends Parasitol 25(1):23-5.
23. Wei-Ping W, Pin-Jin H, Jing W, Xiang-Chun, L. 2011. Six ulcerative colitis patients with refractory symptoms co-infective with Blastocystis hominis infection. Parasitol Res 108(5):1207-10.
24. Nagel R, Cuttell L, Stensvold CR, Mills PC, Bielefeldt-Ohmann H, Traub RJ. 2012. Blastocystis subtypes in symptomatic and asymptomatic family members and pets in response to therapy. Intern Med J 42(11):1187-95.
14. Tobe EH. 2013. Mitochondrial dysfunction, oxidative stress, and major depressive disorder. Neuropsychiatr Dis Treat 9:567-73.
15. Lee HM, Reed J, Greeley GH Jr, Englander EW. 2009. Impaired mitochondrial respiration and protein nitration in the rat hippocampus after acute inhalation of combustion smoke. Toxicol Appl Pharmacol 235(2):208-15.
16. Lee HM, Greeley GH, Herndon DN, Sinha M, Luxon BA, Englander EW. 2005. A rat model of smoke inhalation injury: influenceof combustion smokeongene expression in thebrain.Toxicol Appl Pharmacol 208(3):255-65.
17. Lee HM, Greeley GH Jr., Englander EW. 2011. Transgenic overexpression of neuroglobin attenuates formation of smoke-inhalation-induced oxidative DNA damage, in vivo, in the mouse brain. Free Radic Biol Med 51(12):2281-7.
18. Villanueva C, Kross R. 2012. Antioxidant-induced stress. Int J Mol Sci 13(2): 2091-109.
19. Valko M, Leibfritz D, Moncol J, Cronin MT, Mazur M, Telser J. 2007. Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol 39(1):44-84.
Antioxidants to abrogate free radicals; new insights to challenge currently held beliefs continued from page 6

Australian Journal of Herbal Medicine 2014 26(1)
34 © National Herbalists Association of Australia 2014
MedPlant
Caper berry in the treatment of type 2 diabetes
Fallah Huseini H, Hasani-Rnjbar S, Nayebi N, Heshmat R, Sigaroodi FK, Ahvazi M, Alaei BA, Kianbakht S. 2013. Capparis spinosa L. (Caper) fruit extract in treatment of type 2 diabetic patients: A randomized double-blind placebo-controlled clinical trial. Complement Ther Med 21:447-452.
Capparis spinosa (caper) belongs to the Capparidaceae family, and is thought to have originated in the dry regions of west or central Asia. The caper fruits (also known as caper berries) and flower buds have traditionally been used in treatment of diabetic patients and some experimental studies have demonstrated hypoglycaemic and hypolipidemic effects.
This randomised, double-blind, placebo-controlled study is the first controlled human study to assess the anti-hyperglycaemic effects of caper fruit extract in type 2 diabetic patients. Sixty Iranian men and women aged 45-60 years, with confirmed diabetes mellitus type 2, and who had been on a diabetic food regimen for the two months prior to commencing the study , had not had herbal medicine, and had not altered anti-diabetic medications or dosages, were randomised to take either 400mg dried caper fruit capsule or placebo capsule three times a day before meals for two months. The total daily dose of 1200mg extract was selected as it was equivalent to 5g dry caper fruit, consistent with the average dose range of 2-8g/day recommended by local herbalists.
Fasting blood glucose (FBG), glycated hemoglobin (HbA1c), cholesterol, low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglyceride (TG), serum glutamic oxaloacetic transaminase (SGOT), serum glutamic pyruvic transaminase (SGPT), alkaline phosphatase (ALP), blood urea nitrogen (BUN) and creatinine levels were measured at baseline and after 2 months study treatment. After two months significant decreases were observed for FBG, HbA1c and TG in the caper group. There was no significant difference in cholesterol, LDL, HDL, SGOT, SGPT, ALP, BUN and creatinine levels between the caper and placebo arms. The caper treatment was well tolerated with no hepatic, renal or other adverse event observed.
Caper fruit may have a role in the treatment of type 2 diabetes with improvements observed in hyperglycaemic and hypertriglyceridemic measures. The mechanism of action is unclear, with a previous study in rats reporting a hypoglycaemic activity independent of insulin secretion.
This clinical trial is limited by its small sample size, lack of identification of the constituents responsible, and through non-reporting of compliance of participants in taking their study medications. Despite this, and whilst awaiting additional clinical trials to evaluate long-term safety and efficacy data, the addition of caper fruit to treatments of patients with type 2 diabetes may be appropriate.
Panax quinquefolius in diabetes
Sen S, Querques MA, Chakrabarti S. 2013. North American ginseng (Panax quinquefolius) prevents hyperglycemia and associated pancreatic abnormalities in diabetes. J Med Food 16(7):587-592.
Diabetes mellitus is a chronic metabolic disorder characterised by hyperglycaemia. Type 1 diabetes is an autoimmune condition that leads to the destruction of pancreatic β-cells whilst type 2 diabetes results largely from peripheral insulin resistance which progressively leads to loss of β-cell mass and function.
Extracts of ginseng root, berries and leaves have previously been reported to have hypoglycaemic effects in animal models of type 1 and type 2 diabetes, and the recognised bioactive components are the ginsenosides. Panax quinquefolius, also called North American ginseng (NAG) or American ginseng, has previously been shown to prevent chronic diabetic complications. The purpose of this randomised, controlled study was to investigate the anti-hyperglycaemic efficacy of NAG root extract in mouse models of type 1 and type 2 diabetes and explore its effects on insulin secretin and pancreatic β-cells.
Four year-old NAG roots were sourced from Canada, and the dried ginseng root samples were used to make an extract with a total ginsenoside content of 28.25%. Mouse models of type 1 and type 2 diabetes were created and randomised for monitoring of NAG treatment of 200mg/kg body weight for 4 or 8 weeks. The diabetic mice (D) and the diabetic + NAG (D+NAG) mice were compared to a control group without diabetes. There were 5 animals in each group (controls, D and D+NAG) for both the type 1 and type 2 investigations. For all animals, body weight and blood glucose were measured before and every 7 days after the onset of treatment with NAG. Glycated haemoglobin (GlycoHb) levels, plasma insulin, and serum C-peptide levels were measured after 4 and 8 weeks of NAG treatment. After the follow period, animals were sacrificed and the pancreases were collected for the analysis of the islet/pancreas area ratio.
Reviews of articles on medicinal herbs
Tessa Finney-Brown, Jodie TesterThese abstracts are brief summaries of articles which have appeared in recent issues of herbal medicine journals, some of which may be held in the NHAA library .

Australian Journal of Herbal Medicine 2014 26(1)
35© National Herbalists Association of Australia 2014
MedPlant
Significant anti-hyperglycaemic effects of NAG root was observed for both type 1 and type 2 diabetic mice, measured by significant reduction in blood glucose levels and GlycoHb levels after NAG treatment for 4 or 8 weeks. Treatment with NAG was associated with a significant amelioration of the weight loss in the type 1 diabetic mice and with a significant reduction in weight gain in the type 2 diabetes group. In the type 1 D+NAG group, significant increases in insulin levels were observed at week 4 with even more pronounced increases at week 8. In the type 2 models, NAG treatment significant reduced the hyperinsulinaemia state observed in the diabetic models. The C-peptide levels, which are indicative of the synthetic activity of the β-cells, were improved in both type 1 and type 2 models treated with NAG. In both type 1 and type 2 groups, histological analysis revealed significant increase of the islet/pancreas area ratio after NAG treatment for 8 weeks.
The authors suggest that the beneficial and protective effects of NAG resulted in partial correction of both blood glucose and glycated Hb levels, which they believe was mediated to some degree through regeneration of the β-cells resulting in increased insulin secretion. Additionally, the weight-lowering effect of NAG in type 2 diabetic mice may have also contributed to the improved glucose parameters.
This study provides good evidence of the beneficial effects of P. quinquefolius in diabetes, with insight into how the ginseng might exert its effects. Future studies in humans will provide further insight into its therapeutic role in type 1 and type 2 diabetes mellitus.
Berberine in periodontal disease
Tu HP, Fu M, Kuo PJ, Chin YT, Chiang CY, Chung CL, Fu E. 2013. Berberine’s effect on periodontal tissue degradation by matrix metalloproteinases: an in vitro and in vivo experiment. Phytomedicine 20:1203-1210.
Berberine is an isoquinoline alkaloid found in numerous herbs including Hydrastis canadensis, Berberis aquifolium (syn. Mahonia aquifolium), Berberis vulgaris, Coptis chinensis (and some other Coptis spp.), Phellodendron amurense and Phellodendron chinense. The numerous therapeutic actions of berberine include antimicrobial, anti-inflammatory, anti-cyclooxygenase, anti-inducible nitric oxide synthase and anti-matrix degradation properties.
Periodontal disease is an inflammatory condition that can lead to tooth loss as the inflammation damages surrounding cells and tissue structures including the alveolar bone. Dental plaque bacteria in the inflamed periodontal tissue induce leukocyte infiltration, oedema and vascular dilation. Complex interactions among various inflammatory mediators and tissue degradation may be involved in periodontal pathogenesis, one of which includes overexpression of matrix metalloproteinases (MMP), which influence extracellular matrix degradation.
The effect of berberine on the periodontal expression of MMPs was examined in vitro on human gingival fibroblasts (HGF) and in vivo on the dental alveolar bony level of rats with periodontitis caused by ligation around the molars. The in vitro experiment treated the HGF with Porphyromonas gingivalis to stimulate MMP activity and local inflammation, and then assessed the effects of berberine at concentrations of 0, 1, 10 and 100μM for 24 and/or 48 hours. The berberine treatments significantly decreased the activities of MMPs in a dose dependant manner.
In the in vivo model, 12 male rats were randomised into three groups; a control group, a group with periodontitis, and a group with periodontitis treated with berberine at a dose of 75mg/kg/day. Periodontitis was induced by ligature around the molars. The rats were sacrificed after 8 days and the maxillary and mandibular specimens (including gingivae, teeth and bones) were examined histologically and using micro-computerised tomography to assess the destruction of dental alveolar bone. The berberine-treated group showed less increase in collagen deposit when compared to the non-berberine-treated ligation group which authors suggested reflected a reduced inflammatory condition by berberine. The berberine treatment attenuated the degradation process of periodontal tissue and reduced the number of gingival cells stained positive for MMPs on the histological examination. The authors proposed the berberine may attenuate the degradation of periodontal tissue by inhibition of MMPs, and as such may have preventative potential in periodontal tissue degradation during inflammation.
This study demonstrates that berberine may act partly through the inhibition of MMP activity and that berberine is effective in the treatment of periodontitis through reduced inflammation and attenuated degradation of tissue.
Can a memo help jog the memory?
Yakoot M, Salem A, Helmy S. 2013. Effect of Memo®, a natural formula combination, on Mini-Mental State Examination scores in patients with mild cognitive impairment. Clin Interv Aging 8: 975-81.
One of the major concerns of an ageing population is the increased load on families, carers and the health system (and of course the effects on the individual) of decreased cognitive functioning. Mild cognitive impairment is a term used to encompass the spectrum between age-related cognitive changes and dementia. Amongst the elderly, Alzheimer’s disease and vascular dementia are the most prevalent causes of severe cognitive impairment. Of the two, the latter is more heterogenous (and thus more predictable) in its origin, pathogenesis and clinical course. Given the concern over increasing rates of these diseases, there is an understandable desire to discover clinically effective medications to prevent

Australian Journal of Herbal Medicine 2014 26(1)
36 © National Herbalists Association of Australia 2014
MedPlant
and treat their effects. Thus far, guideline based therapies recommended are cholinesterase inhibitors and an N-methyle-D-aspartate antagonist, both of which have a high cost, frequent adverse effects, weaker efficacy in more progressed cases and rapid reversal of efficacy after withdrawal. Other agents that have been advocated include vitamin E, non-steroidal anti-inflammatory drugs, hormones, and herbal preparations, predominantly of Gingko biloba and Panax ginseng.
This recent clinical trial evaluated the effects of a particular extract (Memo®) on Mini-Mental State Examination (MMSE) scores in patients with mild cognitive impairment. The supplement combined lyophilized royal jelly 750mg with standardised extracts of G. biloba leaf extract 120mg (standardised to contain 24% flavonoid glycosides and 6% terpenoid) and P. ginseng root extract 150mg (standardised to contain 40 -80% ginsenosides). It was a randomised, double-blind, placebo-controlled pilot study conducted in an outpatient setting. The 66 patients were enrolled over roughly two years from two outpatient clinics in Alexandria, Egypt. They were aged between 50 and 80 years and subject to various exclusion criteria. The intervention was one capsule of supplement (or placebo) daily before breakfast for four weeks. The MMSE was used as the outcome measure as it is the most simple and widely recognised measurement tool for cognitive impairment.
After four weeks of treatment, 60 patients remained in the trial (others were lost to follow up, or excluded due to poor compliance). In the group treated with Memo®, there was a statistically significant improvement in the MMSE score (by paired samples t-test) after four weeks of treatment. The placebo group did not exhibit this. The statistical significant remained after adjustment of raw data for age and education level. Gender was not found to have an effect on the outcome variable.
Neither group reported serious adverse effects, although similar numbers in both groups (around three) complained of side effects such as mild nausea and dyspepsia, and a mild transient headache. Five subjects in the active and three in the control group experienced mild flushing and palpitations during the first three days of treatment. Interestingly, the men treated with Memo® also reported an improvement in sexual performance and libido, but this did not reach statistical significance.
This was only a pilot study, and should be replicated with larger sample sizes, but it does suggest that this combination may be a promising intervention in those suffering from mild cognitive impairment. There are a number of reasons that it may have been effective, including the antioxidant, nutritive and neuroprotective properties of the constituents. Prior studies have also shown G. biloba to improve the fluidity of neuronal membranes and increase the density of cholinergic, adrenergic and dopaminergic transmission in the brain; and to stimulate ligand-binding at muscarinic receptors in
the hippocampus. Royal jelly has been found to promote neurogenesis of neural stem cells in vitro, and contains adenosine monophosphate N1-oxide, which facilitates astrogenesis. Further study is recommended on these ingredients, in both isolated and combination to forms, to assess both individual and synergistic effects.
Disease-modifying potential of Cinnamon extract in inflammation and arthritis
Vetal S, Bodhankar S, Mohan V, Thakurdesai P. 2013. Anti-inflammatory and anti-arthritic activity of type-A procyanidine polyphenols from bark of Cinnamomum zeylanicum in rats. Food Science and Human Wellness 2(2):59-67.
Cinnamomum zeylanicum (cinnamon) has been traditionally used for a variety of indications, including conditions of inflammation- and pain-related disorders. Anti-inflammatory effects have been reported in a number of trials and have been attributed to its polyphenolic components including tannins and procyanidins. The procyanidins are classified as Types A, B or C based on linkage between successive monomeric units. Immunomodulatory effects have also been reported for cinnamon bark including inhibitory activity against complement formation and immunosuppressive activity. The combined anti-inflammatory and immunomodulatory effects of cinnamon make it a potential treatment option for arthritic conditions.
The study was designed to evaluate the efficacy and safety of Type-A procyanidine polyphenols (TAPP) isolated from cinnamon bark in animal models of acute inflammation and rheumatoid arthritis in rats. The TAPP was a standardised extract of C. zeylanicum bark with pentameric type-A procyanidine flavonoid as a marker compound (75.9% purity). Two models of inflammation were investigated in the study.
In the first, anti-inflammatory activity was assessed on inhibition in carrageenan-induced paw oedema (CPE). Groups of six rats were treated orally with either 2, 4, 8 or 25 mg/kg TAPP, 5mg/kg diclofenac sodium or control, one hour before a carrageenan injection causing inflammation and oedema. Paw volume was measured immediately after injection, and at 1, 3, 6 and 24 hours post. The NSAID, diclofenac, caused significant reduction in oedema at 1 hour until 6 hours compared to the control group. The TAPP treatment demonstrated anti-inflammatory effects at 4mg/kg, 8mg/kg and 25mg/kg but no significant effect at 2mg/kg. The time to onset of effect was 3 hours, 3 hours and 1 hour for the 4, 8 and 25mg/kg doses respectively.
In the second model, rats with adjuvant-induced established arthritis (AIA) were used in the assessment of treatment with diclofenac (1mg/kg) or TAPP (8mg/kg) to a control group based on parameters including body weight, pain latency of inflamed paw, ankle diameter, arthritis score and serum CRP levels. Significant reductions in the ankle diameter, CRP levels and total arthritis score were

Australian Journal of Herbal Medicine 2014 26(1)
37© National Herbalists Association of Australia 2014
MedPlant
observed for both the diclofenac and TAPP groups, with no observable changes in the control group. The TAPP and diclofenac groups were significantly protective from cachexia due to arthritis induction. No change in pain latencies were observed for any group. Additionally, the gastric histology for one rat in each group was assessed with the mucosal epithelial layer of the stomach from the control and TAPP groups were found to be normal. The superficial gastric mucosa of the diclofenac-treated rat had multiple areas of erosions and haemorrhage.
Whilst the current medical treatments for arthritis are effective, side effects are common and often serious. As observed in this study, NSAIDs are commonly associated with gastrointestinal events including ulceration, perforation and bleeding. In this study, TAPP displayed anti-inflammatory and anti-arthritic effects without ulcerogenic effects or analgesic activity in rats. Cinnamon bark isolate of TAPP may potentially be an effective disease-modifying treatment in arthritic conditions. Further studies are needed to further understand the mechanism of anti-inflammatory actions and to determine effectiveness in human populations.
Warming yang and replenishing the kidney to treat cold-induced asthma
Tang B, Shi K, Li X, Wang H, Fang H, Xiong B, Wu Y. 2013. Effect of “yang-warming and kidney essence-replenishing” herbal paste on cold-related asthma exacerbation. J Tradit Chin Med 33: 468-72.
In Traditional Chinese Medicine (TCM), the common cold is viewed as being caused by the invasion of exterior pathogenic factors that closely involve the Qi of the body. Defensive lung Qi usually protects the body from exterior pathogenic factors but if that is weakened, the resultant loosening of striae and interstice make it easier for exterior pathogenic factors to invade. Traditional beliefs also indicate that this lung-defensive Qi stems from the lower-energiser, the kidney. If this is weak (for example, due to recurrent disease), there may be a resultant weakening of lung-defensive Qi.
Asthmatic patients often suffer exacerbations due to viral infections, including the common cold. In TCM, this may be interpreted as being due to disordered warming function, loss of nourishment to the upper energiser, and resultant weakness of lung-defensive Qi due to deficiency of kidney Yang and insecurity of kidney-Qi.
Thus, the way to treat such a condition or presentation may be with a Yang-warming and kidney essence-replenishing herbal paste. This study investigated the effects of such treatment via a randomised controlled clinical trial. 150 patients were recruited from the outpatient department of a number of hospitals in Shanghai. They all met the diagnosis of asthma (based upon the Global Strategy for Asthma Management and Prevention (2005)) and kidney-deficiency syndrome (according to TCM syndrome differentiation). Patients
were randomised into treatment or control group and underwent medication for 8 weeks. Both groups were given the same basic medication, including inhaled glucocorticoids and beta-2 agonists. In addition, those in the treatment group were given a herbal paste (components below), and told to take 25g orally (with warm water) twice a day for 60 days (beginning from the winter solstice). The researchers measured: (a) general condition, including sociological information, course of disease, and severity rating; (b) frequency of diurnal symptoms; (c) frequency of nocturnal symptoms; (d) frequency of exacerbation; (e) frequency of catching cold; (f ) frequency of cold-related exacerbation; (g) Asthma Control Test (ACT) score; and (h) kidney-deficiency syndrome score. Data was collected at baseline, and then once a month for one year.
Of the 143 patients that completed the trial, the treatment group experienced significant reduction in the frequency of asthma exacerbation and frequency of catching a cold. They also had significantly less chance of a cold-related exacerbation of their asthma when compared to the control group. After treatment both groups experience significant improvement in their ACT scores but there was no difference between groups. Finally, the treatment group experienced a significant change in their kidney-deficiency score; in comparison to the control sample.
This study suggests that winter consumption of a yang-warming, kidney essence-replenishing herbal paste may help to prevent cold-related asthma exacerbations throughout the subsequent year. TCM theory attributes this to amelioration of kidney-Yang deficiency, improved defensive function of the lung, thus blocking the invasion of exogenous pathogens.
The herbal paste was composed of: Yinyanghuo (Herba Epimedii Brevicornus), Bajitian (Radix Morindae Officinalis), Huangqi (Radix Astragali Mongolici), Dangshen (Radix Codonopsis), Heshouwu (Radix Polygoni Multiflori), Huangjing (Rhizoma Polygonati Sibirici), Shudihuang (Radix Rehmanniae Preparata), Shanzhuyu (Fructus Corni), Maidong (Radix Ophiopogonis Japonici),Yeqiaomaigen (Fagopyrum Dibotrys Hara), Hutuiye (Lithocarpus Elaeagnifolia), Huangjingzi (Fructus Viticis Negundo), Fabanxia (prepared Pinellia Tuber), Pugongying (Herba Taraxaci Mongolici), Ejiao (Colla Corii Asi-ni), Guijiaiiao (Colla Carapacis Et Plastri Testudinis), Gejie (Gecko), Ziheche (Placenta Hominis), Baishen (White Ginseng), crystal sugar, and maltose.
Dietary flaxseed has pronounced antihypertensive effect
Rodriguez-Leyva D, Weighell W, Edel A, LaVallee R, Dibrov E, Pinneker R, Maddaford T, Ramjiawan B, Aliani M, Guzman R, Pierce G. 2013. Potent antihypertensive action of dietary flaxseed in hypertensive patients. Hypertension 62: 1081-9.

Australian Journal of Herbal Medicine 2014 26(1)
38 © National Herbalists Association of Australia 2014
MedPlant
One of the most important risk factors for cardiovascular (CVD) and cerebrovascular diseases is hypertension. Primary hypertension, defined as a systolic blood pressure (BP) ≥140mmHg, or a diastolic BP ≥90mmHg is very common amongst the population and places a large economic burden on the health care system. The direct and indirect costs of hypertension in America alone totalled $76 billion three years ago. Thus it is important to develop and continue to investigate treatments for the condition.
Amongst the proposed nutritional interventions are omega-3 fatty acids, fibre and antioxidants. Flaxseed is one of the few vegetable food sources of omega-3 fatty acids, fibre and lignans which are potent antioxidants. It has been shown in animal studies to have the capacity to reduce CVD via anti-inflammatory and anti-atherogenic effects, as well as through improvements in vascular contractile function. It has also shown to exert an antiarrhythmic effect during ischaemic cardiac challenge.
Few studies have utilised this food source in human trials, so researchers from Cuba and Canada teamed up to do just that. They enrolled 110 patients with peripheral arterial disease (for ≥ 6 months, with an ankle brachial index ≤0.9). There was an average age of 67 years, 90% of patients were current or ex-smokers, 75% were hypertensive, 32% diabetic and 79% hyperlipidemic.
Some but not all were on blood sugar–lowering, lipid-lowering, antihypertensive, or antithrombotic medication. They were fed a number of foods (bagels, bread, biscuits, pasta, muffins, bars) that either contained 30g milled flaxseed or 30g of placebo (wheat, sometimes with a small amount of molasses or bran). One of these products was ingested each day for the six months of the trial.
At baseline, and after six months, BMI and body weights were similar between the two groups
(flaxseed and placebo). After the trial, plasma levels of enterolignans in the active group increased substantially (10 fold increase for enterolactone and 50 fold increase for enterodiol), as did levels of the ω-3 fatty acid ALA (by 2 fold). EPA levels also increased significantly but DHA did not change. There were no changes in blood levels for any of the compounds in the placebo group.
The drop in blood pressure for the treatment group was statistically significant, from an average of 143/77 mmHg to 136/72 mmHg. In contrast, systolic BP rose in the placebo group, and diastolic BP remained the same (146/79 mmHg). Overall the dietary intervention maintained systolic BP at 10mmHg, and diastolic BP at 7mmHg lower than placebo. Subgroup analyses indicated that these results were more pronounced in those with higher systolic BP at baseline.
The study indicates that the introduction of dietary flaxseed may have potent antihypertensive effects in hypertensive patients, and that this may be a simple strategy to improve the health of patients and reduce the costs of CVD and cerebrovascular disease.
References1. Baxter J. 2009. Regulation of the profession. Aust J Herb Med
21(2):25-30.2. Wardle J. 2010.The National Registration and Accreditation Scheme:
what would inclusion mean for naturopathy and Western herbal medicine? Part I: The legislation. Aust J Herb Med 22(4):113-118.
3. Wardle J, Steel A, McIntyre E. 2013. Independent registration for naturopaths and herbalists in Australia: the coming of age of an ancient profession in contemporary healthcare. Aust J Herb Med 25(3):101-6.
4. White A, Foster NE, Cummings M, Barlas P. 2007. Acupuncture treatment for chronic knee pain: a systematic review. Rheumatology 46(3):384-90.
5. Pan YQ, Yang KH, Wang YL, Zhang LP, Liang HQ. Massage interventions and treatment-related side effects of breast cancer: a systematic review and meta-analysis. Int J Clin Oncol (in press).
6. Wardle J, Sibbritt D, Adams J. The interface between naturopathy and rural primary health care: A survey of referral practices of general practitioners in rural and regional New South Wales, Australia (unpublished, under review).
7. Wardle JL, Sibbritt D, Adams J. Acupuncture referrals in rural primary healthcare: a survey of general practitioners in rural and regional New South Wales, Australia. Acupunct Med (in press).
8. Wardle JL, Sibbritt DW, Adams J. 2013. Referrals to chiropractors and osteopaths: a survey of general practitioners in rural and regional New South Wales, Australia. Chiropr Man Therap 21:5.
9. van Haselen RA, Reiber U, Nickel I, Jakob A, Fisher PAG. 2004. Providing Complementary and Alternative Medicine in primary care: the primary care workers’ perspective. Complement Ther Med 12(1):6-16.
10. Kirby E, Broom A, Adams J, Sibbritt D, Refshauge K. What drives women’s practitioner choices for back pain? A qualitative study (unpublished, under review).
The decline of herbal medicine/naturopathy consultations; how research can help further the profession continued from page 9

Australian Journal of Herbal Medicine 2014 26(1)
39© National Herbalists Association of Australia 2014
MedJourn
Non-Coeliac Wheat Sensitivity
Carroccio A, Mansueto P, D’Alcamo A, Iacono G. 2013. Non-celiac wheat sensitivity as an allergic condition: Personal experience and narrative review. Am J Gastroenerol. In press. DOI:10.1038/ajg.2013.353.
A review on non-coeliac wheat sensitivity (NCWS) was recently published in the American Journal of Gastroenterology. The article provides an overview of NCWS, re-evaluates the results of a double-blind placebo-controlled (DBPC) food challenge in patients with irritable bowel syndrome (IBS), and reviews the roles of DBPC food challenges, serum immunoglobulin G (IgG) antibodies, basophil activation assay and histology in food allergy diagnosis.
Using data and subjects from a previous trial, the authors reviewed results of DBPC challenges in an IBS patient population. All patients in the previous study were prescribed a standard elimination diet with the exclusion of wheat, cow’s milk (CM), eggs, tomato and chocolate. Patients who self-reported food hypersensitivity were asked to avoid ingestion and/or contact with the foods causing symptoms. After 4 weeks on elimination diet patients underwent the DBPC crossover challenges. The wheat challenge involved administering flour in capsules, taken separate from food three times daily to total of 13g, the equivalent of 20g of bread. Flour or placebo capsules were given for up to two consecutive weeks and then following a washout period of one week, the patients received the other capsules (placebo or flour) for up to another two weeks. The DBPC challenge for CM was similar with patients being administered capsules containing casein, lactoalbumin and lactoglobulin at least 4 weeks before or after the wheat challenge, while the patients were still on the elimination diet and were asymptomatic. Xylose was used as the placebo. The challenges were stopped when clinical reactions occurred for at least two consecutive days.
Of the 920 study participants, 276 patients were diagnosed with NCWS using a DBPC wheat challenge after having their IBS resolve on the elimination diet and relapsed into symptoms on the DBPC wheat challenge. Interestingly, of the 276 patients with NCWS, 206 also reacted to the DBPC CM challenge suggesting multiple food hypersensitivity. The group with NCWS and IBS were compared to controls with IBS not due to food sensitivity (i.e. no improvement on elimination diet). Compared to the control group, patients with NCWSS
and multiple food sensitivity revealed significantly higher incidence of food allergy in the paediatric age group, and in the groups with coexistent atopic diseases, positive serum IgG anti-gliadin antibodies (AGAs) and IgG anti-betalactoglobulin antibodies, in vitro basophil activation, and eosinophil presence in the colon mucosa biopsies. The authors propose that the clinical, laboratory and histological characteristics of patients with NCWS and multiple food sensitivity suggest they might suffer from non-Immunoglobulin E (non-IgE) -mediated food allergy.
Despite the study reporting higher levels of AGA and IgG anti-betalactoglobulin antibodies in patients with NCWS and multiple food hypersensitivity, the authors suggest the elimination of foods based on IgG food antigen assays should be discouraged in line with a number of international allergy and immunological guidelines. They did however propose that serum IgG AGA may be useful as a marker of NCWS. The positive basophil activation assay or basophil activation test (BAT), which was also associated with NCWS, has previously been demonstrated as a highly specific tool for food allergy including CM allergy. Despite this, changes in methods of the BAT assay have not produced more accurate results and consequently the authors report that BAT accuracy in NCWS diagnosis is excessively influenced by a method that is not standardised and reproducible and do not recommend that commercial BAT assays be used in NCWS diagnosis. With regard to duodenal histology in NCWS, findings are reported as normal or characterised by an infiltration of intraepithelial lymphocytes (IEL) in the absence of villi atrophy. Whilst the authors reported 90% of the 276 NCWS patients showing an IEL increase, it was suggested that as IEL infiltration can be due to several causes and is not specific to wheat sensitivity. Mucosal eosinophil infiltrate, observed in 75% of NCWS patients compared to 0% of the control group, may be a more appropriate histological marker. However authors acknowledged that its presence should not be considered a diagnostic marker of NCWS, but may be appropriate to use to identify patients who should attempt an elimination diet and DBPC challenge to confirm diagnosis.
In concluding the review, the authors describe NCWS as a heterogenous condition includes different subgroups of patients. The different subgroups include a coeliac disease-like subgroup whose characteristics resemble coeliac disease although they do not presently fulfil
These abstracts are brief summaries of articles in recent issues of medical journals . Articles selected are of a general nature for the information of practitioners of herbal medicine . A dominant theme is often present throughout the journals which will be reflected in the reviews .
Tessa Finney-Brown, Jodie Tester
Reviews of medical journal articles

Australian Journal of Herbal Medicine 2014 26(1)
40 © National Herbalists Association of Australia 2014
MedJourn
current diagnostic criteria; patients with an allergy-like presentation; a FODMAP effect group who show no signs of histological inflammation and benefit from a low Fermentable, Oligo-, Di-, Mono-saccharides And Polyols (FODMAP) diet; and show a typical IBS picture with psychosomatic mechanisms. The authors suggested that the allergy-like presentation is likely to the most common form of NCWS and that the pathogenesis of patients suffering from NCWS alone is likely to be different to those suffering from multiple food sensitivity.
This review provides a good overview of NCWS as a potential non-IgE-mediated allergic condition, and highlights the relevance of clinical and laboratory investigations in diagnosis as well as providing discussion around non-immune mediated pathogenic mechanisms. Further research in this area is required, but the article’s publication in a reputable medical journal is a positive step in this field.
Perinatal air pollution exposure and autism spectrum disorder
Roberts AL, Lyall K, Hart JE, Laden F, Just AC, Bobb JF, Koenen KC, Ascherio A, Weisskopf MG. 2013. Perinatal air pollutant exposures and autism spectrum disprders in the children of Nurses’ Health Study II participants. Environ Health Perspect 121:978-984.
Whilst the aetiology of autism spectrum disorder (ASD) is poorly understood, environmental exposures during gestation have been implicated with recent studies reporting associations between perinatal exposure to air pollution and ASD in children. Air pollution contains many toxicants known to affect neurological function including arsenic, cadmium, mercury, nickel, styrene, trichloroethylene, methylene chloride, vinyl chloride and diesel particulate matter amongst others. All of which have previously been associated with ASD.
This retrospective study was designed to test the hypothesis that perinatal exposure to hazardous air pollutants increases risk of ASD by estimating associations between the US Environmental Protection Authority (EPA) -modelled levels of hazardous air pollutants at the time and place of birth with ASD in children of participants in a national prospective longitudinal cohort. Data was collected from the Nurses’ Health Study II, a cohort of over 11,000 female nurses from across USA that was established in 1989. Some 325 cases of reported ASD (including autism, Asperger syndrome and pervasive developmental disorder) in children were compared to 22,098 controls. Exposure assessment was performed using data from the EPA National Air Toxics Assessments of 1990, 1996, 1999 and 2002 which provides an inventory of outdoor sources of air pollution concentrations in different locations. The mailing address used for the Nurses’ Health Study II at the approximate time of the subject’s birth was used to identify residential air pollutants from the EPA data.
The study found significant positive linear trends between pollutant concentration and ASD for diesel particulate matter, lead, manganese, methylene chloride, mercury, nickel and overall metal score. Cadmium, diesel, lead, manganese, mercury, methylene chloride, and nickel showed roughly linear dose-response relationships between concentration and odds ratio of ASD. The highest concentrations of diesel particulate matter and mercury were most strongly associated with ASD with an odds ratio of 2. Despite this, the authors were unable to establish if one or two specific pollutants were most responsible for driving the association with ASD, possibly because of using estimates of modelled exposure rather than actual exposure or due to insufficient statistical power.
Whilst previous studies had examined air pollution and ASD, they generally had not examined gender differences in the relationship between ASD and air pollutants. In this study most of the air pollutant associations with ASD were stronger for boys than girls however this must be interpreted with caution as a smaller number of girls with ASD were included in the analysis.
Limitations of the study include using a modelled estimate of air pollutants instead of actual. Ideally, individual variations including time spend outdoors, commuting, indoor exposure and seasonal fluctuations would be accounted for. Also the EPA records may not adequately assess for or account for pollutants from indoor sources such as lead paints, drinking water, household chemicals etc. Additionally, the location of birth used for cases from the Nurses’ Health Study II may not have been accurate nor reflect the location during pregnancy. The strengths of the study are its large size and varied location of participants from all across the USA and the adjustments for a range of socioeconomic indicators to minimise ascertainment bias.
Further research is needed to fully understand the implications of personal exposure to toxicants during gestation and risk of ASD, as well as more research investigating toxicant levels in the blood of newborns to understand levels and risk of ASD. Nevertheless, perinatal exposure to air pollutants may increase risk for ASD and should be a consideration in preconception care and for expecting mothers.
Effect of prebiotic and probiotic supplementation on fussiness and crying in the preterm infant
Partty A, Luoto R, Kalliomaki M, Salminen S, Isolauri E. 2013. Effects of early prebiotic and probiotic supplementation on development of gut microbiota and fussing and crying in preterm infants: A randomized, double-blind, placebo-controlled trial. J Pediatr 163:1272-7.
In the young infant, balanced host-microbe interactions are critical for healthy intestinal and immunological development. The microbiome develops though pregnancy

Australian Journal of Herbal Medicine 2014 26(1)
41© National Herbalists Association of Australia 2014
MedJourn
and is influenced by numerous factors including mode of delivery, perinatal antibiotic exposure, mode of feeding and skin-to-skin contact. The microbial community of preterm infants has been identified to consist of fewer beneficial species, lower bacterial diversity and more pathogens compared to healthy term infants. This study was designed to investigate whether early modification of the gut microbiota with specific probiotics and prebiotics could provide benefit through enhancing infant wellbeing and result in reducing crying and fussing.
A randomised, double-blind, placebo-controlled study was conducted involving 94 preterm infants who were recruited between days 1 and 3 of life between June 2008 and May 2011. Study entry requirements included gestational age between 32+0 and 36+6 weeks, birth weight >1500g, and absence of any congenital defects in the gastrointestinal system or other defects preventing enteral nutrition. Subjects were randomly assigned to one of three groups to receive: a prebiotic mixture (polydextrose and galacto-oligosaccharides 1:1, 600mg once daily from day 1-30 and 600mg twice daily from day 31-60); a probiotic (10 billion Lactobacillus rhamnosus GG [ATCC 53103], once daily from day 1-30 and twice daily from day 31-60); or placebo. After enrolment, follow up consultations were conducted at 1, 2, 4, 6, and 12 months with parents reporting infant’s behavioural patterns, including sleep patterns, fussing, crying, irritability, feeding, vomits, stools, infection, other disease and medications. Infants were classified as excessive crying and irritability for >3hour/day causing clinical concern without underlying medical conditions during the 1- and 2- month visits. Faecal samples were collected from diapers at the age of 1 month for microbiota analysis.
Of the 94 infants enrolled, 72% completed the 1-year study, and at which point, mean weight and height were comparable between all groups. During the first two months of life 29% of infants were classified as excessive criers with significantly less excessive criers in the prebiotic and probiotic groups compared to placebo (19%, 19% and 47% respectively). Stool frequency was higher in the prebiotic group compared to the probiotic and control however consistency was similar between the groups. In analysing the gut microbiota, a significantly lower proportion of Clostridium histolyticum bacteria were observed in the probiotic group compared to placebo and prebiotics groups. Further analysis of gut microbiota of excessive criers compared to contented infants found a higher proportion of Lactobacillus-Lactococcus-Enterococcus and C. histolyticum, and a lower proportion of Bifidobacterium infantis.
The author’s report their microbiota findings suggest a decreased number or delayed colonisation of B. infantis combined with immature gut barrier function to be potential risk factors for crying and irritability in preterm infants. Additionally, the higher rate of C. histolyticum in
the placebo group suggests L. rhamnosus GG promotes gut health by reducing the C. histolyticum colonisation through mechanisms including competitive exclusion.
The author’s noted that whilst differences in the gut microbiota were observable for the prebiotic and probiotic groups, the clinical outcomes were similar. A proposed explanation included that the prebiotic group experienced a higher stool frequency compared to the probiotic and placebo groups. The increased frequency may have lessened abdominal distension and flatulence and this may have contributed to the lowered irritability seen in this group.
This study extends knowledge about prebiotic and probiotic supplementation in the preterm infant finding benefit and potential to improve overall wellbeing. Importantly, the outcomes measured in this trial represent an important everyday occurrence which impacts on the overall wellbeing of the infant and parents. Additionally, further understanding of specific bacterial strains and functions assists with appropriate selection of supplements.
Watermelon as a recovery aid for athletes
Tarazona-Diaz M, Alacid F, Carrasco M, Martinez I, Aguayo E. 2013. Watermelon Juice: Potential Functional Drink for Sore Muscle Relief in Athletes. J. Agric. Food Chem 61:7544-7528.
L-citrulline is a non-protein amino acid found in high concentrations in watermelons, but not many other natural foods. It is an antioxidant with hydroxyl radical scavenger activity, and combined with the ability to generate nitric oxide, may have a potential therapeutic role in conditions characterised by oxidative stress and decreased arginine availability. Suggested uses include hypertension, heart failure, atherosclerosis, erectile dysfunction and athletic performance. Previous studies have found citrulline supplementation to be associated with smooth muscle relaxation, enhanced anaerobic athletic performance, relieved muscle soreness and accelerated lactic acid removal. This two-part study was designed to determine the in-vitro bioavailability of L-citrulline from a natural or synthetic standard watermelon juice and determine the in-vivo effect of watermelon juice in athletic performance.
The in-vitro part of the study was to assess the absorption, absorption speed and apparent permeability of L-citrulline from an unpasteurised natural watermelon juice (NW), a pasteurised watermelon juice (PW) or control of L-citrulline + water. Caco-2 cells, which are derived from a human colon adenocarcinoma and have morphological and functional similarities to human intestinal epithelial cells, were treated with the NW, PW or control to assess the absorption parameters.
Absorption (%), absorption speed, and permeability of Caco-2 cells were higher when the L-citrulline was supplied as a NW juice, with the pasteurisation treatment reducing the percentage, speed and permeability of

Australian Journal of Herbal Medicine 2014 26(1)
42 © National Herbalists Association of Australia 2014
MedJourn
absorption. Absorption of NW was also greater than in the control indicating that watermelon juice is a more suitable vehicle for transport than a pure standard. In all of the samples, the absorption speed decreased with time, which may suggest that L-citrulline bioavailability may be limited by its intestinal absorption.
The athletic performance part of the trial was conducted in 7 male subjects with a mean 22.7 years age; body mass 68.9kg; height 170.8cm; body mass index 24.0; and who were not competitive athletes but participated regularly in different sports. Subjects were not taking any medication or suffered from injuries that could interfere with athletic performance. On the day prior to the completion of the tests, subjects were instructed to not practice any vigorous exercise nor consume alcoholic beverage or stimulants. Subjects were to eat a carbohydrate rich meal at least 3 hours prior to starting testing and consumed the 500mg test beverage 1hour before the test. Three treatment drinks were trialled. These were: an unpasteurised natural watermelon juice (NWJ) containing 1.17g of citrulline; an unpasteurised enriched watermelon juice (EWJ) with 6g of citrulline and a colour-similar placebo infusion of fruit-flavoured plants with a sugar content similar to the watermelon juices. All subjects tested each drink sample with a separation of 5 days between each test. The exercise protocol included a standardised 5-minute warm-up on a cycle ergometer and then completed an 11minute cycling test of with a recovery of 3 minutes. Blood lactate samples were taken through the test and during the recovery. Perceived exertion was assessed during the testing and subjects self-reported their soreness at 24 and 48 hours after each session of testing (NWJ, EWJ and placebo).
The study did not demonstrate improvement in athletic performance as assessed by pedalling speed, nor any difference in perceived exertion or blood lactate levels after ingestion of NWJ or EWJ compared to placebo. Muscle soreness was significantly reduced at 24 hours but not 48 hours when the NWJ or EWJ drinks were consumed. Muscle soreness at 24 hours was similar between the NWJ and EWJ juices indicating that enrichment with L-citrulline did not produce additional benefits in reducing muscle soreness. The heart rates of subjects throughout the exercise tests were all similar however a trend of greater heart rate reduction after 1 and 3 minutes recovery was observed when the NWJ or EWJ juices were consumed, although this was not significant. Although significance was not reached, this trend may be worth additional research in a study with a larger population.
This is a small study that suggests a potential role for watermelon juice in exercise recovery by reducing muscle soreness and possibly reducing heart rate recovery time. Importantly, the bioavailability of L-citrulline was greater in its natural form as a non-pasteurised watermelon juice, highlighting the role of food as medicine.
Dietary interventions for prevention of gestational diabetes
Bao W, Bowers K, Tobias D, Hu F, Zhang C. 2013. Pre pregnancy dietary protein intake, major dietary protein sources, and the risk of gestational diabetes mellitus: a prospective cohort study. Diabetes Care 36: 2001–8.
Gestational diabetes mellitus (GDM) is a growing concern in Australia, particularly amongst high-risk groups including Aboriginal and Torres Strait Islander women, and women from a South Asian background. The condition is defined as impaired glucose tolerance with the onset or first recognition in pregnancy and it is associated with long-term adverse health outcomes for both mother and child. In order to help prevent the condition, it is important to identify potential contributory/risk factors.
Dietary proteins and individual amino acids are known to be important dietary modulators of glucose metabolism, and diets high in protein may potentially impact upon glucose homeostasis by promoting insulin resistance and increasing gluconeogenesis. The association between dietary protein and GDM has, until now, not been clear. Emerging evidence suggests however that not all dietary protein sources or amino acids impact glucose metabolism in the same way, which makes evaluating the connection between dietary macronutrients and GDM even more complicated.
In this cohort study, researchers examined data from pregnant women in the Nurses’ Health Study II (between 1991 and 2001). They included 21, 457 singleton pregnancies that were free of chronic diseases prior to pregnancy and free of previous GDM. After adjustment for age, parity, non-dietary and dietary factors and BMI, they were able to evaluate the prevalence of GDM amongst those women with different quintiles of animal and vegetable protein intake.
Results showed that higher intake of animal proteins, in particular red meat, were significantly associated with a greater risk of developing GDM. In contrast, higher intakes of vegetable protein, particularly nut, was associated with a significantly lower risk. In women who substituted 5% of energy from vegetable protein for animal protein, and/or other healthy protein sources (poultry, fish, nuts, legumes) for red meat there was also a lower risk of GDM.
Previous authors have hypothesised that higher intakes of total protein and animal protein (shown in studies to increase the risk of T2DM) may contribute to poor glucose homeostasis from an accelerated “fatigue” or “failure” of pancreatic islets. The results may also be attributable to other beneficial nutrients co-existent in protein foods, (but not saturated fat or cholesterol, as the result remained significant, even after adjusting for these factors). The researchers in this study note that BCAA content is much higher in animal proteins and these have been implicated in the development of insulin resistance

Australian Journal of Herbal Medicine 2014 26(1)
43© National Herbalists Association of Australia 2014
MedJourn
in previous trials. There are a number of limitations to the current study, not least the potential misclassification of dietary proteins, use of cumulative averages for participants with more than one pregnancy and third, the fact that a majority of participants were Caucasian Americans, which limits generalizability.
Nonetheless, the results of this current cohort study suggest that practitioners may wish to consider advising their pregnant clients of the importance of consuming good vegetable sources of protein throughout their pregnancies, as it may help to decrease the risk of developing GDM. Further studies, including clinical trials would be beneficial.
Micronutrient supplementation in HIV patients
Baum M, Campa A, Lai S, Sales Martinez S, Tsalaile L, Burns P, Farahani M, Li Y, van Widenfelt E, Page J, Bussmann H, Fawzi W, Moyo S, Makhema J,Thior I, Essex M, Marlink R. 2013. Effect of micronutrient supplementation on disease progression in asymptomatic, antiretroviral-naïve, HIV infected adults in Botswana: a randomized clinical trial. JAMA 310: 2154-63.
Human immunodeficiency virus (HIV) is a disease which is challenging worldwide, but perhaps nowhere more so than Africa. In this condition, micronutrient deficiencies, which are known to affect immune function, are present long before the development of HIV-related symptoms and are associated with increased disease progression. In countries such as Botswana, which has one of the highest rates of HIV in the world, along with a more severe strain (HIV subtype C), cost-effective interventions are needed to slow progression early in the disease. This is not only beneficial for patients and their families, but would allow increased time for resource-limited countries to prepare their healthcare systems and allot needed resources for HIV interventions such as anti-retroviral therapy (ART).
Other clinical trials have shown micronutrient interventions to improve markers of HIV progression and mortality but most of these were conducted in the late stages of the disease, or in pregnant women. The current study is the first to test the effects of long-term micronutrient supplementation in the early stage of the disease, in ART-naïve patients. Amongst those nutrients known to have beneficial effects on the immune system are B vitamins, vitamin C and E and the trace mineral selenium. Selenium in particular may have an important role in preventing HIV replication. Thus, in this study, groups received a daily supplement of multivitamins alone, selenium (200 μg) alone, the combination of multivitamins plus selenium or placebo, taken as 1 pill per day. A total of 878 patients participated in the trial and were randomised into one of the four groups. They took the supplements daily and attended monthly follow-ups for 24 months. Both participants and personnel of the study were blinded to the randomisation.
The main goals of the trial were to determine whether the supplements could enhance the immune system and slow HIV disease progression during the early stages of the disease. Thus, outcome measures reflected this – they included CD4 count, HIV viral load, plasma micronutrients and blood chemistries, as well as data on morbidity and mortality. The primary endpoint was HIV disease progression.
After 24 months, treatment with multivitamins + selenium compared to placebo significantly reduced the risk of reaching the primary endpoint of a CD4 count of 250/μL or less. Selenium supplementation alone had no effect on this parameter. For the secondary outcome of the composite of a CD4 count of 250/μL or less, AIDS-defining conditions or AIDS-related death, supplementation with multivitamin + selenium was again significantly better than placebo.
These and other secondary and tertiary outcomes showed that a single supplement of B vitamins, vitamins C and E, and selenium, as compared with placebo, (administered early in HIV disease) reduced the risk of reaching a CD4 cell count of 250/μL or less in 2 years. There was also an evident benefit with an earlier end point of a CD4 cell count of 350/μL or less, which is the current standard for providing ART in Botswana. Thus, it shows promise in slowing HIV disease progression in HIV-infected, ART-naïve patients, and may be recommended as a beneficial intervention to help delay the need to begin ART. In developing nations, this may give governments and policy-makers more time to gather their resources and develop the necessary programs of implementation.
N.b. (The multivitamins included thiamine, 20mg; riboflavin, 20mg; niacin, 100mg; vitaminB6, 25mg; vitaminB12, 50μg; folic acid, 800 μg; vitamin C, 500 mg; and vitamin E, 30 mg.)
Apples and statins go head to head
Briggs A, Mizdrak A Scarborough P. 2013. A statin a day keeps the doctor away: comparative proverb assessment modelling study. BMJ 347: f7267.
Statins are amongst the most frequently prescribed drugs in the world, and are the only drug class in the United Kingdom (and other nations) to be considered for primary prevention at a population level. All other official health recommendations for primary prevention of vascular disease (in particular) are diet and lifestyle related. This dates back to the well-known Victorian adage of “an apple a day keeps the doctor away”.
In seeking to evaluate how drugs or, indeed apples, might compare in terms of primary prevention, researchers from the BHF Health Promotion Research Group designed a particular type of modelling study. They modelled the effect on vascular mortality of prescribing everyone in the UK over 50 years old either an apple (Malus domestica) or a statin, each to be taken daily. They compared the estimated number of adverse

Australian Journal of Herbal Medicine 2014 26(1)
44 © National Herbalists Association of Australia 2014
MedJourn
effects and the costs of taking the drug or the fruit daily.Commonly available UK datasets were used in the
analysis. Data regarding the effects on cardiovascular mortality came from the Cholesterol Treatment Trialists’ meta-analysis, the results of which indicated that reducing cholesterol with a statin reduces the relative risk of vascular mortality by 12% per 1.0 mmol/L reduction in LDL. That study also showed that LDL was reduced by an average of 1.08mmol/L over one year of treatment. People were assumed to be taking the prevention dose of 40mg/day. Data for the apple a day modelling was modelled using PRIME, a comparative risk calculator that compared the relation between nutritional parameters and chronic disease mortality. The standard apple weight was estimated at 100g (and calorie intake of participants was assumed to remain constant). Compliance for either treatment was estimated to be 70%.
Overall, the model predicted that prescribing either apples or statins to everybody in the UK over 50 years (with a 70% compliance rate) may prevent vascular deaths by rates of 8500 and 9400 respectively. Thus, either intervention is likely to have a similar effect on population vascular mortality. In addition, statin dosing at these rates would be estimated to be linked with 1200 extra cases of myopathy, 200 cases of rhabdomyolysis, and 12 300 diagnoses of diabetes mellitus. Choosing the apples over the statins would likely prevent these. On the downside, the total cost of an apple intervention was greater than that of a statin ($260 million v $180 million per year).
This was of course only a modelled assessment and authors concede that the predicted effects of such interventions/health policies could vary for a number of reasons, including differing compliance, individual factors (sex, age, cardiovascular risk profiles) and dietary preference. Overall, the main value of the study is to show that small dietary changes, in addition to, or instead of increased statin use at the population level may significantly reduce vascular mortality.
Proton pump inhibitors associated with vitamin B12 deficiency
Lam J, Schneider J, Zhao W, Corley D. 2013. Proton Pump Inhibitor and Histamine 2 Receptor Antagonist Use and Vitamin B12 Deficiency. JAMA 310: 2435 – 2442.
Acid-suppressing medications, including Proton pump inhibitors (PPI) and H2 receptor antagonists (H2RA), are among the most commonly used medications in developed countries. They are often prescribed for gastritis, GORD and peptic ulcer disease. As they suppress gastric production of hydrochloric acid there is the theoretic potential to impair the digestion of protein and protein-bound nutrients, such as vitamin B12. In the past, there has been no scientific evidence to support this claim and many pharmacists have assumed that no adverse impact is caused.
Vitamin B12 is a nutrient found bound to animal-proteins in the diet. Deficiency is fairly common, particularly amongst the elder population and has been associated with dementia, neurological damage, anaemia and other complications that are potentially irreversible.
Research recently published in JAMA has finally elucidated a link between the use of PPI and H2RA, and B12 deficiency. Researchers evaluated the link using a case-control study design, in community dwelling population in Northern California. They analysed 25 956 patients with incident diagnoses of vitamin B12 deficiency (between the period of 1997 – 2011), with 184 199 patients without B12 deficiency. They ascertained exposures and outcomes via the use of electronic pharmacy, laboratory and diagnostic databases. [nb. There is a detailed discussion on the potential for confounding and statistical analysis methods in the article itself if practitioners wish to find out more about the research methods].
Overall, a new diagnosis of B12 deficiency was more common amongst patients with a 2 year supply or greater of PPIs and H2RAs, compared with non-users. Using the highest daily dose of medications (both PPIs and H2RAs) was more strongly associated with deficiency of the vitamin, as was a longer duration of PPI use. The strength of association between the two variables diminished after discontinuation of the medication, which suggests a causative, rather than simply a correlative relationship. The relationship between acid-suppressing medication use and B12 deficiency was present in patients with no other risk factors for vitamin deficiency, as well as amongst those with 1 or more risk factors. Interestingly, the association was strongest in those under 30 years of age, and also among women.
Although previous, smaller studies have evaluated the correlation between acid inhibitor use and B12 deficiency, this large-scale, longer-term analysis extends the results. The findings in the study suggest a causal relationship between the two variables including the strength of the association, temporality of the effect, evidence of a dose-relationship, plausibility and consistency. The researchers also conducted supplemental analyses that suggested that the finding were not solely explained by health service utilisation.

Australian Journal of Herbal Medicine 2014 26(1)
45© National Herbalists Association of Australia 2014
CPE
AJHM based CPE QuestionaireThe AJHM based CPE questionnaire system is a voluntary system designed to assist members in the accumulation of NHAA CPE points . Questions are divided into the appropriate subject categories (herbal medicine and medical science) and each question refers to an article in this issue of the Australian Journal of Herbal Medicine . Points accumulated through completion of these questions should be recorded in the NHAA CPE diary . Each completed question is worth one mark in the relevant category . Your completed CPE diary should be returned with your membership renewal at the end of the financial year . For further information please see the NHAA CPE Member’s Manual on the NHAA website www .nhaa .org .au .
Herbal medicine questions – AJHM 25(4)1 . From the study regarding cinnamon bark in
arthritis and inflammation, TAPP was: a) shown to be an effective treatment with significant
reduction in ankle diameter, CRP levels, pain latency and total arthritis score;
b) shown to be an effective treatment with significant reduction in ankle diameter, CRP levels and total arthritis score;
c) associated with erosion and haemorrhage of the superficial gastric mucosa;
d) shown to be anti-inflammatory at 2mg/kg, 4mg/kg, 8mg/kg and 25mg/kg.
2 . With reference to the study on watermelon juice in athletes, which is most true?
a) Blood lactate concentration during exercise was reduced in the natural watermelon or L-citrulline enriched watermelon juice trials compared to placebo;
b) Pasteurisation does not affect the absorption or bioavailiability of L-citrulline from watermelon juice;
c) Recovery heart rate after exercise with natural watermelon or L-citrulline enriched watermelon juice was significantly reduced compared to placebo;
d) Muscle soreness after exercise with natural watermelon or L-citrulline enriched watermelon juice was reduced compared to placebo.
3 . Regarding the use of probiotics and prebiotics for preterm infants, which is most true?
a) Prebiotic supplementation was associated with reduced excessive crying, increased stool frequency and reduced Clostridium histolyticum colonisation;
b) Probiotic supplementation was associated with reduced excessive crying, increased stool frequency and reduced Clostridium histolyticum colonisation;
c) Prebiotic supplementation was associated with reduced excessive crying and reduced Clostridium histolyticum colonisation;
d) Probiotic supplementation was associated with reduced excessive crying and reduced Clostridium histolyticum colonisation.
4 . Caper fruit was demonstrated to improve hypoglycaemic and:
a) hypertriglyceridemic measures in patients with type 2 diabetes mellitus at doses of 400mg/daily;
b) anti-hypertriglyceridemic in patients with type 2 diabetes mellitus at doses of 400mg/daily;
c) anti-hypertriglyceridemic measures in patients with type 2 diabetes mellitus at doses of 1200mg/daily;
d) hypertriglyceridemic measures in patients with type 2 diabetes mellitus at doses of 1200mg/daily.
Medical science questions – AJHM 25(4)1 . With reference to the study on Panax
quinquefolius in diabetes, which is most true?a) Significant anti-hyperglycaemic effects of NAG root
was observed for both type 1 and type 2 diabetic mice, measured by significant reduction in blood;
b) Treatment with NAG was associated with a significant reduction in weight gain in the type 1 diabetes group;
c) Treatment with NAG was associated with significant increases in insulin levels at week 8 in the type 1 and type 2 models;
d) Significant increase of the islet/pancreas area ratio was seen in both type 1 and type 2 models after NAG treatment for 8 weeks.
2 . Referring to the study on berberine in periodontal disease, which is most true:
a) Berberine was found to reduce tissue inflammation and tissue degradation, with increased activity of matrix metalloproteinases;
b) Berberine may be effective in the inflammatory condition of periodontitis through inhibition of matrix metalloproteinases;
c) Berberine may be effective in the inflammatory condition of periodontitis through activation of matrix metalloproteinases;
d) Berberine was found to reduce tissue inflammation and tissue degradation and increase collagen deposit.
3 . From the study assessing air pollution exposure and ASD, the study found:
a) significant positive linear trends between air pollution concentration and household chemical exposure and ASD;
b) significant positive linear trends between pollutant concentration and ASD for diesel particulate matter, lead, manganese, methylene chloride and mercury;
c) the highest concentrations of lead were most strongly associated with ASD;
d) diesel was solely responsible for the association with ASD.4 . From the review of non-coeliac wheat sensitivity
(NCFS), which of the following is true?a) NCFS does not commonly coexist with atopic diseases
in the paediatric age;b) The authors suggest the elimination of foods based on
IgG food antigen assays should be discouraged in line with international guidelines;
c) 90% of NCWS patients show an intraepithelial lymphocytes increase suggesting it is an appropriate and specific diagnostic marker;
d) Mucosal eosinophil infiltrate was observed in 75% of NCWS patients and can be considered an appropriate diagnostic marker.

QUALITY UPDATE
a division of Value through expertiseIMCD
Network Nutrition has a longstanding leadership position in the herbal medicine industry as a quality medicinal herbal extracts producer and supplier. Quality in the herbal medicine industry is difficult to achieve due to starting material (herb) variability. Often, highly skilled quality assurance professionals debate the methodologies to identify and to quantify quality markers in individual extracts.
Identifying and eliminating low quality and adulterated extract material is an important part of a quality assurance paradigm, especially in view of high usage in the Australian community. Herbal medicine extracts are used in many complementary medicine supplements that are being delivered in both practitioner only and the retail environment. The ANAO Audit report on Complementary Medicines (2011-12 pp. 34) stated in 1996, “surveys in Victoria and South Australia found 50% of the people used alternative medicine. By 2009, the National Institute of Complementary Medicine figures indicated that two-thirds of Australians use these medicines every year.” It is believed that healthcare professionals are compounding this due to increased research and education of this sector.
Quality Parameters in Herbal Medicine The Extract People™
The Department of Innovation, Industry, Science and Research (ANAO 2011, pp. 34) estimated the value of sales in Australia to be $1.2 billon per year, and the estimation of market growth is between three and 12 annually. Therefore with global sourcing of starting materials, and the high demands on the marketplace, it is critical that stringent quality questions must be posed daily.
Network Nutrition is dedicated to developing processes for identification of adulteration and trends in batch variations.
“The Network Nutrition, technical and R&D teams constantly update research and market literature for
our extract porfolio. Being proactive and innovative, we are quick to
resolve technical issues relating to adulteration in herbal extract material in the market place” says Dr. Suresh Govindaraghavan, Head of Research and Development, Network Nutrition.
The aim for the Network Nutrition Program for Adulteration Detection is to provide ‘economically motivated integrity’ in the supply chain. Based on research literature updates, industry insight and market place information, we have embarked on developing novel methodologies to ensure the purity and quality of high value standardised extracts. This involves: starting material authentication; cGMP in extract manufacture; authentication of extracts (HPLC profile) and their compositional ratios; comparison with pharmacopoeial references; and computation of multi-batch data.
Network Nutrition is passionate about identifying issues in the industry and will continue to dedicate resources in providing the highest quality extracts. We are “The Extract People”.TM
www.networknutrition.com ph: +61 2 8814 4999 fax: + 61 2 8814 4900
“Herbal medicine adulteration is akin to theft, and weeding out adulterated
herbal extracts is a confronting challenge. Methods of adulteration are becoming increasingly sophisticated,
and it seems that as we ‘catch the crooks’, they are already well on their way to scheming their next heist! The
sad reality is, this is a task that does not appear to be going away.”
Ryan Gorman, Brand Director, Network Nutrition

Dr. Lise Alschuler is a naturopathic doctor with board certification in naturopathic oncology and has been practicing since 1994. In this two part DVD presentation, Dr. Lise Alschuler discusses the use of botanicals in cancer prevention and co-management. The February lecture focuses on the evidence-based use of botanicals in reducing cancer risk through targeting the three stages of cellular carcinogenesis. The March lecture details the use of botanicals in co-management of cancer, including reducing the toxic side-effects from chemotherapeutic drugs as well as their use as an adjuvant therapy. With the ever-increasing rise of cancer diagnosis, these lectures are invaluable clinical tools for every practitioner.
Optimal Rx Introduces Magnolia....The bark from Magnolia (Magnolia officinalis) has been used for over 1,000 years in the Traditional Medicinal Systems of China and Japan, and was revered as a plant that replenishes Chi, the essence of life. What makes Magnolia such a profound and unique plant is its broad range of therapeutic actions that supports its use in a vast number of chronic diseases. While its historical use as an anxiolytic and antidepressant continues to be relevant today, recent research has also demonstrated that it may possess anti-cancer, anti-atherosclerotic, cardioprotective, anti-obesity, and insulin-sensitising properties. Optimal Rx is excited about the range of therapeutic applications for Magnolia and is certain it will make an irreplaceable addition to your herbal medicine dispensary.
Oborne Health SuppliesP 1300 887 188
Natural Remedies Group P 1300 138 815
BettaLife Distributors P 1300 553 223
Rener Health Products P 1300 883 716
Optimal RxP 1300 889 483
Contact Optimal Rx OR Your Distributors NOW
SESSIONS w i t h t h e INTERNATIONAL MASTERS
February Lecture:Botanical Considerations in Reducing
Cancer Risk
March Lecture:Botanicals for Co-management in Cancer
Care
$39.95 each or FREE with Monthly Specials

BRISBANE, QLD Saturday 15 March 2014
Traders Hotel 159 Roma St, Brisbane
8.30am Registration Seminar 9am – 1.30pm
SYDNEY, NSW Saturday 29 March 2014
Y Hotel 5-11 Wentworth Ave, Sydney
8.30am Registration Seminar 9am – 1.30pm
MELBOURNE, VIC Sunday 30 March 2014
Karstens 123 Queen St, Melbourne
11.30am Registration Seminar 12noon – 4.30pm
PERTH, WA Sunday 6 April 2014
Esplanade River Suites 112 Melville Pde, Como 11.30am Registration
Seminar 12noon – 4.30pm
For more information or to register, go to:www.nhaa.org.au/events/national-seminar-series
or call the office on 02 8765 0071
From Gattefossé to today – Aromatic Medicine, the real Aromatherapy! This exciting
and informative seminar will explain how aromatic medicine fits within aromatherapy and
botanical medicine. Learn about safe use and interactions, dose and application methods,
where and how to prescribe and details on commonly used aromatics. With case studies
and practical tips throughout, this is one you won’t want to miss.
2014 National Seminar Series
AROMATIC MEDICINE:A Potent New Tool
for Herbalists
Featuring Mark Webb
SEMINAR SCHEDULE:
The seminar will include a half hour morning or afternoon tea break.












![PROFILE ON HERBAL COSMETICS - ::krishna::krishna.nic.in/PDFfiles/MSME/Herbal/herbal cosmetics[1].pdf · 2 SECTION I PRODUCT CHARACTERISTICS Herbal Cosmetics consists of herbal based](https://img.pdfslide.net/doc/110x75/5a9e561f7f8b9a0d7f8d5810/profile-on-herbal-cosmetics-krishna-cosmetics1pdf2-section-i-product-characteristics.jpg)