Embed Size (px)
Citation preview
Hereditary Hemorrhagic Telangiectasia (Osler-Weber-Rendu syndrome)
Scott Gabbard, MDScott Gabbard, MD
04/20/200904/20/2009
Osler-Weber-RenduOsler-Weber-Rendu
Initially described as a familial disease with abnormal vascular structures Initially described as a familial disease with abnormal vascular structures causing bleeding from the nose and GI tractcausing bleeding from the nose and GI tract
1896 - Henri Rendu describes the first classic case1896 - Henri Rendu describes the first classic case 1901 - Sir William Osler describes an inherited disease of “inadequate vessels”1901 - Sir William Osler describes an inherited disease of “inadequate vessels”
– First to suspect liver involvementFirst to suspect liver involvement 1907 - Frederick Weber publishes extensively on the subject1907 - Frederick Weber publishes extensively on the subject
OverviewOverview
Onset of diseaseOnset of disease– 50% diagnosed by 16, 90% by age 4050% diagnosed by 16, 90% by age 40
IncidenceIncidence– 1:5000 to 1:80001:5000 to 1:8000– Less common in African-AmericansLess common in African-Americans– Higher incidence in Mormons and those Higher incidence in Mormons and those
of Caribbean originof Caribbean origin
PathophysiologyPathophysiology
Autosomal dominant traitAutosomal dominant trait– Varying penetrance and expressionVarying penetrance and expression
Thought to be due to mutations in Thought to be due to mutations in Transferring Growth Factor (TGF)-beta Transferring Growth Factor (TGF)-beta signalingsignaling– Plays a role in regulation of cell proliferation, Plays a role in regulation of cell proliferation,
angiogenesis, wound healing, embryonic angiogenesis, wound healing, embryonic developmentdevelopment
PathophysiologyPathophysiology
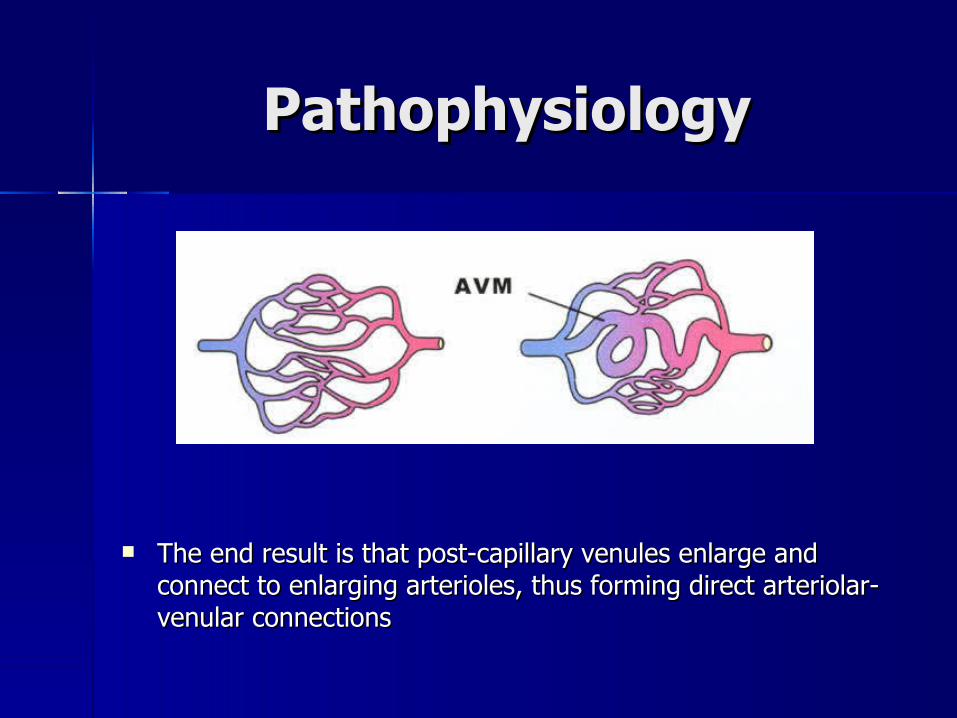
The end result is that post-capillary venules enlarge and The end result is that post-capillary venules enlarge and connect to enlarging arterioles, thus forming direct arteriolar-connect to enlarging arterioles, thus forming direct arteriolar-venular connectionsvenular connections
Clinical featuresClinical features
TelangiectasiaTelangiectasia EpistaxisEpistaxis GI bleedingGI bleeding Pulmonary AVMsPulmonary AVMs Cerebral AVMsCerebral AVMs Liver involvementLiver involvement
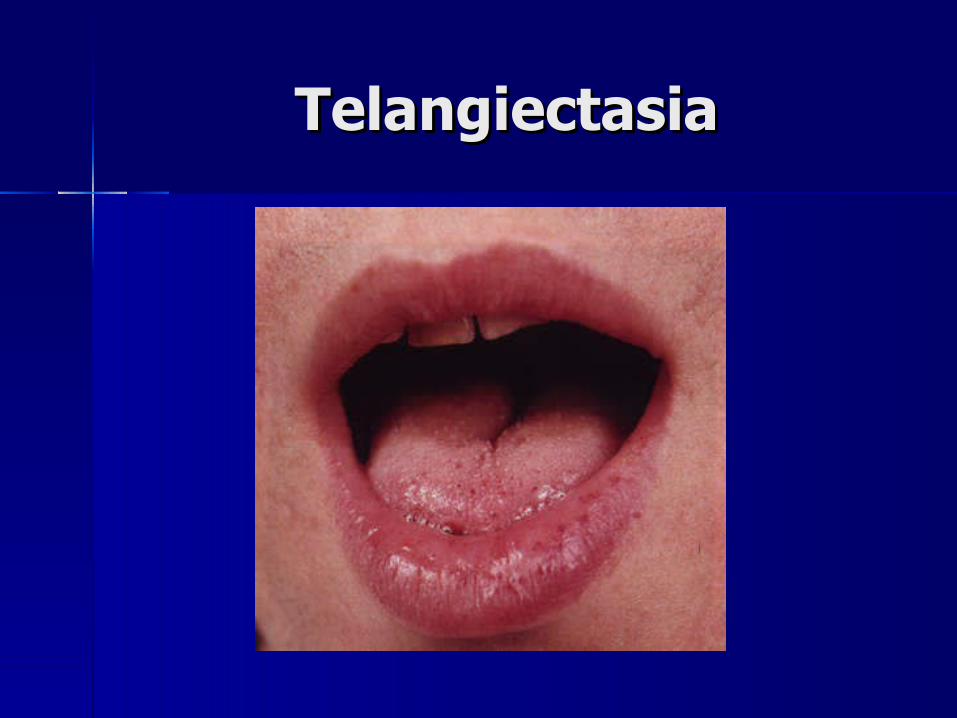
TelangiectasiaTelangiectasia

GI bleedingGI bleeding
More common to have angiodysplasia in the upper GI tractMore common to have angiodysplasia in the upper GI tract
Pulmonary AVMsPulmonary AVMs
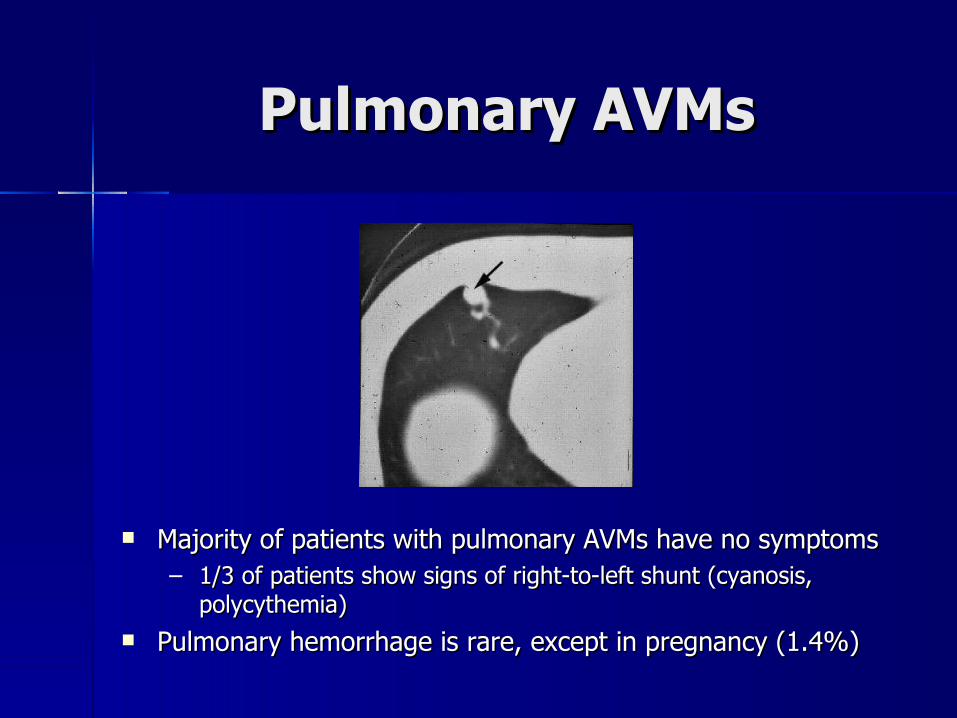
Majority of patients with pulmonary AVMs have no symptomsMajority of patients with pulmonary AVMs have no symptoms– 1/3 of patients show signs of right-to-left shunt (cyanosis, 1/3 of patients show signs of right-to-left shunt (cyanosis,
polycythemia)polycythemia) Pulmonary hemorrhage is rare, except in pregnancy (1.4%)Pulmonary hemorrhage is rare, except in pregnancy (1.4%)
Cerebral AVMsCerebral AVMs
Affect ~10% of HHT patientsAffect ~10% of HHT patients Majority are silentMajority are silent Hemorrhage is less likely with HHT than other Hemorrhage is less likely with HHT than other
causes of cerebral AVMs because of the lower causes of cerebral AVMs because of the lower association with aneurysmsassociation with aneurysms
However, HHT patients are 23x more likely to have However, HHT patients are 23x more likely to have a hemorrhagic stroke than the general populationa hemorrhagic stroke than the general population
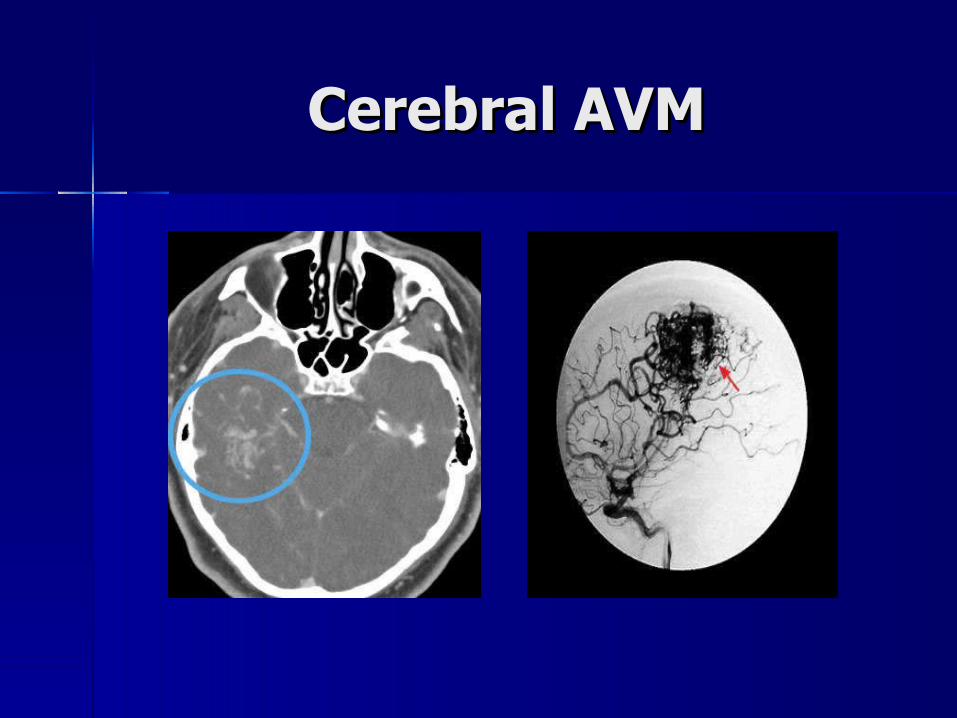
Cerebral AVMCerebral AVM
Hepatic involvementHepatic involvement
8-31% of patients with HHT8-31% of patients with HHT Left-to-Right AV shuntingLeft-to-Right AV shunting
– Hepatic artery to hepatic veinHepatic artery to hepatic vein Arterioportal shuntingArterioportal shunting
– Hepatic artery to portal veinsHepatic artery to portal veins Recurrent encephalopathy is common in patients Recurrent encephalopathy is common in patients
with large shuntwith large shunt Lesions may be embedded in dense fibrous tissue, Lesions may be embedded in dense fibrous tissue,
leading to a nodular appearance of the liver leading to a nodular appearance of the liver (pseudocirrhosis)(pseudocirrhosis)
High-output heart failureHigh-output heart failure
High-output heart failure often described in High-output heart failure often described in patients with left-to-right intrahepatic patients with left-to-right intrahepatic shuntsshunts– Almost always hepatic artery to hepatic veinAlmost always hepatic artery to hepatic vein– Occurs once shunt output is > 20%Occurs once shunt output is > 20%
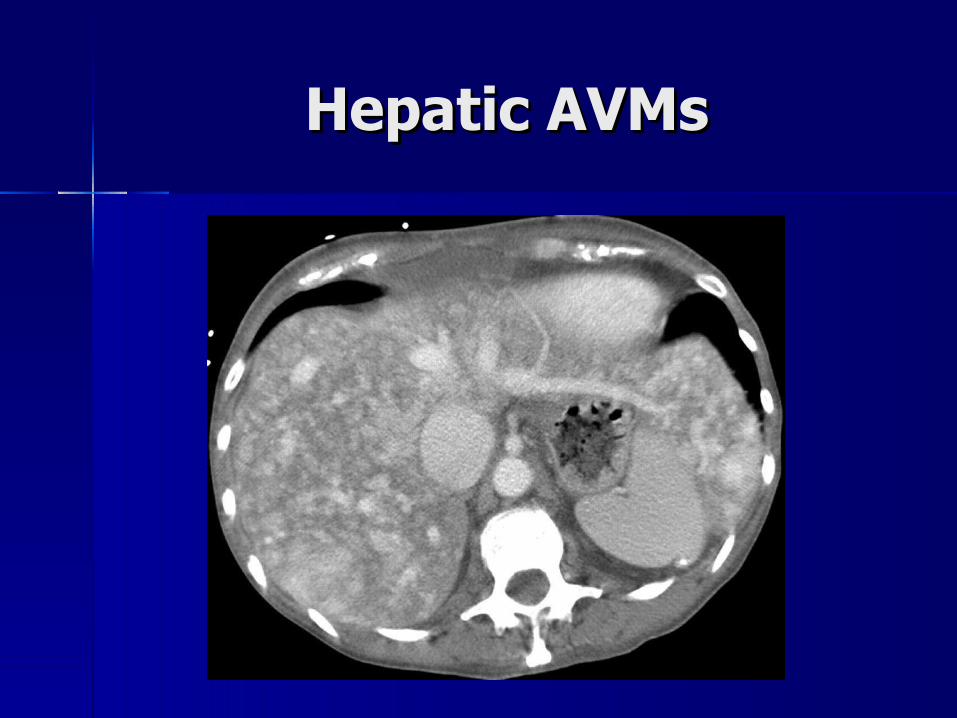
Hepatic AVMsHepatic AVMs

HHT diagnosisHHT diagnosis
Three out of four is considered “definite”Three out of four is considered “definite”– Spontaneous and recurrent epistaxisSpontaneous and recurrent epistaxis– Multiple mucocutaneous telangiectasiasMultiple mucocutaneous telangiectasias– Visceral involvementVisceral involvement
Diagnose by doppler US, CT angiography, MRI, Diagnose by doppler US, CT angiography, MRI, angiographyangiography
– First degree relative with HHTFirst degree relative with HHT
HHT - TreatmentHHT - Treatment
Most common complications of HHT: Most common complications of HHT: epistaxis and GI bleedingepistaxis and GI bleeding– Treat patients similar to those without Treat patients similar to those without
HHTHHT Iron deficiency anemia is commonIron deficiency anemia is common
Treatment of AVMsTreatment of AVMs
Pulmonary AVMs are treated with embolotherapy, Pulmonary AVMs are treated with embolotherapy, usually with a detachable balloonusually with a detachable balloon
Cerebral AVMs are treated with Cerebral AVMs are treated with embolectomy, surgical removal, or stereotactic radiotherapy
Hepatic involvementHepatic involvement
Arterial embolizationArterial embolization– Associated with 43% risk of serious/fatal Associated with 43% risk of serious/fatal
complications, most are related to hepatic/biliary complications, most are related to hepatic/biliary necrosisnecrosis
Liver TransplantLiver Transplant– Recent review article documented 28 OLT Recent review article documented 28 OLT
attemps for patients with HHT, 24 patients were attemps for patients with HHT, 24 patients were still living at the time of publishstill living at the time of publish
– One patient with high-output CHF underwent One patient with high-output CHF underwent OLT, her cardiac index fell from 6.7 to 3.8 and OLT, her cardiac index fell from 6.7 to 3.8 and she was doing well at last reportshe was doing well at last report
ReferencesReferences
Geneva Foundation for Medical Education and Research http://www.ajronline.org/content/vol187/6_Supplement/images/large/12_05_http://www.ajronline.org/content/vol187/6_Supplement/images/large/12_05_1602_01c.jpeg1602_01c.jpeg
Liver disease in hereditary hemorrhagic telangiectasia, Larson AM, Journal of Clinical Gastroenterology. 2003 Feb;36(2):149-58
Liver involvement in hereditary hemorrhagic telangiectasia: consensus recommendations. Buscarini et al. Liver Int. 2006 Nov;26(9):1040-6
MedGadget, http://medgadget.com/archives/2005/03/triactiv_balloo.htmlhttp://medgadget.com/archives/2005/03/triactiv_balloo.html
St. John Health System, http://www.stjohn.org/images/Services/ed_avmart.jpghttp://www.stjohn.org/images/Services/ed_avmart.jpg
The Role of Liver Transplantation in the Treatment of Hereditary Hemorrhagic Telangiectasia: A Short Literature Review. Scelzo et al. Transplantation Proceedings. Volume 39, Issue 6, July-August 2007, Pages 2045-2047
Uptodate.com




























