Embed Size (px)
Citation preview
Heroin, Fentanyl and Other
Opioids
Steve Hanson
Heroin/Opiates


Neurotransmitter-receptor interactions
To transmit instructions to cells, neurotransmitters
interact with their receptors.receptor
neurotransmitters

Neurotransmitter Action
ReuptakeRelease of NT
Receptor

Brain Changes
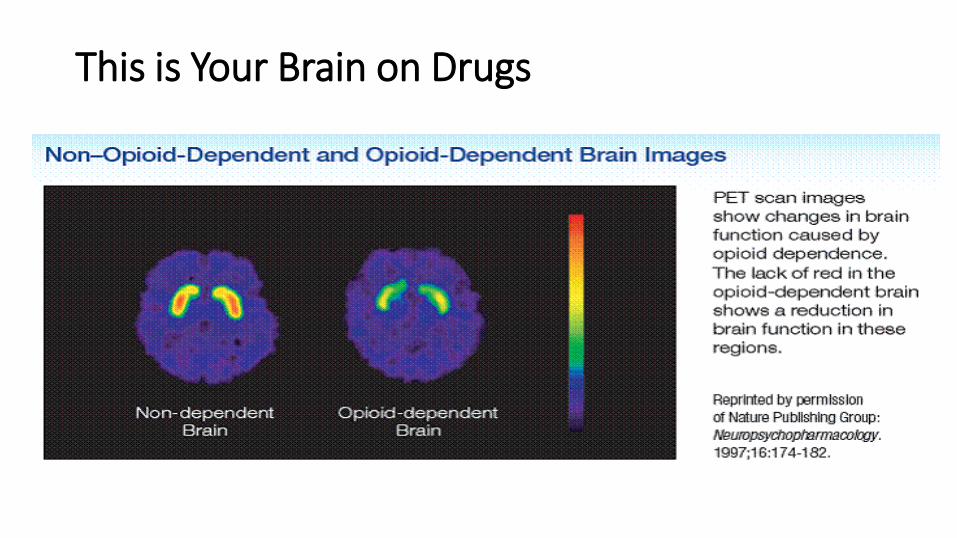
This is Your Brain on Drugs
7

Opiates Increase DA Release
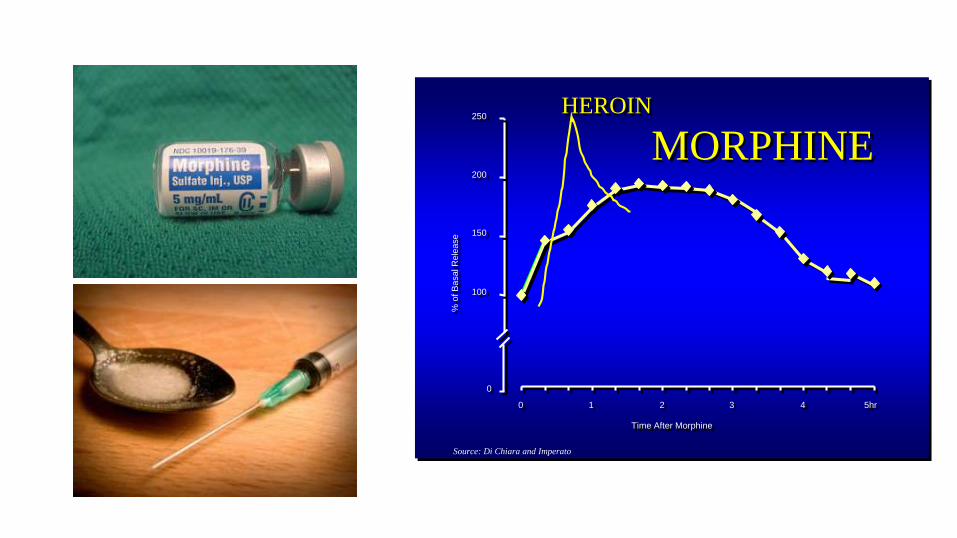
0
100
150
200
250
0 1 2 3 4 5hr
Time After Morphine
% o
f B
asal R
ele
ase
MORPHINE
Source: Di Chiara and Imperato
HEROIN
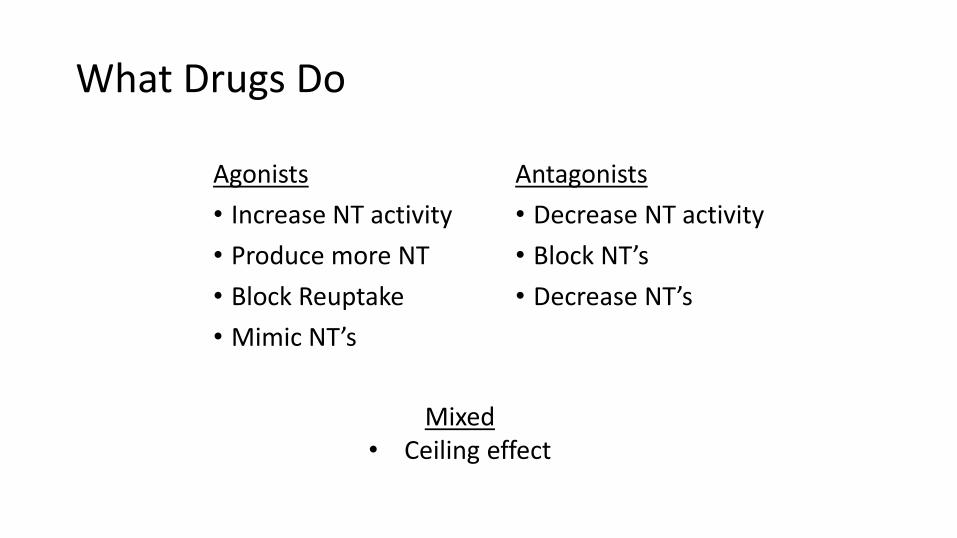
What Drugs Do
Agonists
• Increase NT activity
• Produce more NT
• Block Reuptake
• Mimic NT’s
Antagonists
• Decrease NT activity
• Block NT’s
• Decrease NT’s
Mixed• Ceiling effect

Opiates
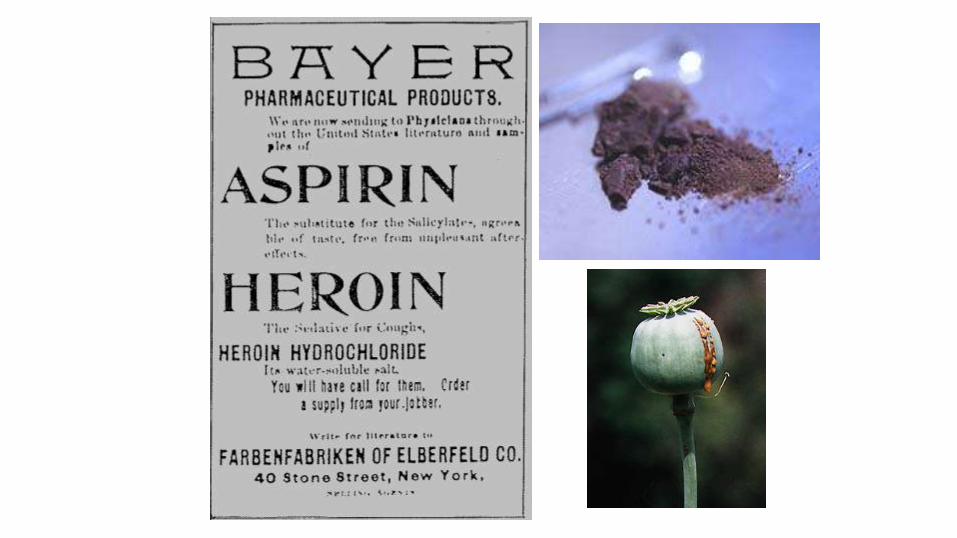
• Dates to 4,000 BC
• Mimics endorphin activity
• Natural - Opium, morphine, codeine
• Semi-synthetic- Heroin, Dilaudid
• Synthetics - Darvon, Demerol, Fentanyl
Modern History• Off and on use through until the 60’s
• “Man with the Golden Arm”
• Vietnam war – soldiers using heroin
• 1970’s – increased prevalence – urban areas
• Treatment programs – Methadone Maintenance / Therapeutic Communities
• 1980’s Hard to find – substitutes
• 1990’s – resurgence
• 2010’s – “epidemic”

“Heroin Chic”

Opiates
•Heroin more potent -60-80% - <10% in ‘70’s
•Younger age group - High School
•Users start with snorting - IV within 12 months
•Withdrawal painful - not deadly

NATURAL OPIATES
MorphineCodeineThebaine
OPIUM
Semi-synthetics
Heroin Dilaudid
Morphine
Synthetics
• Demerol
• Fentanyl
• Methadone
• Darvon

Opiates
• Fat solubility – Heroin – high – rush
• Morphine – lower – longer onset
• Heroin metabolized into morphine
• Morphine metabolized by the liver
• Metabolite is 10-20X more powerful
• Detectable in urine for 2-4 days

The Action ofHeroin(Morphine)
Tolerance
• Rapid tolerance with continued use
• Initial dose of 50mg/day can go to 500mg/day in as little as 10 days
• Cell sensitivity thought to be the tolerance mechanism.
Opiates & Reward Pathway

Opiates Increase DA Release

Agonists, Mixed and Antagonists

Heroin
Effects
• Analgesia - change in pain perception
• Euphoria - intense• Sedation - “on the nod”• Respiratory depression• Cough suppression• Nausea/vomiting• Constipation
Withdrawal
• Pain• Depression• Alert• Rapid breathing• Coughing• Nausea/vomiting• Diarrhea• 3-5 days

Addiction/Dependency Cycle
•Opioids trigger reward system – euphoria – leads to continued use – addiction
•Withdrawal symptoms are significant – regular use to avoid withdrawal - dependence
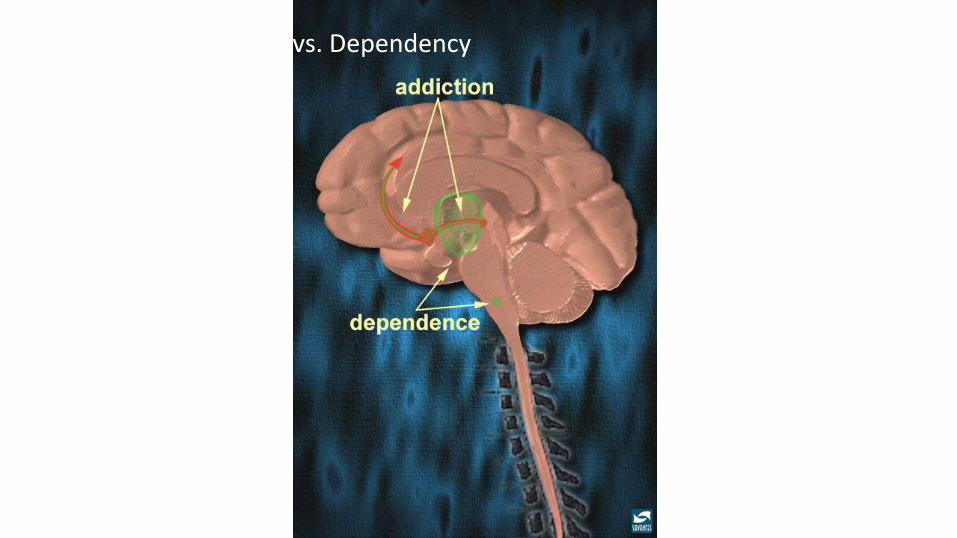
Addiction vs. Dependency

Natural History of Opioid Dependence

Potency Factors by Weight
• Morphine 1
• Heroin 3
• Codeine 0.1
• Dilaudid 8
• Demerol 0.05
• Fentanyl 300 - 1000

Potency
NIDA

Heroin usage patterns
•Highly addictive and dependence producing
•Significant tolerance up to 35X
• Increased cost
•Tolerance management (Tx, jail, etc.)
•Mixing with other opiates and other drugs (speedballing/cocaine)

Prescription Opiates

OxyContin
OxyContin
• Oxycodone – synthesized from thebaine (part of opium)
• OxyContin – 1995• Crush the tablet for quicker high• Oral, snort, inject
• Percocet – oxycodone & acetaminophen
• Percodan – oxycodone & aspirin

Vicodin

Vicodin
•Hydrocodone and acetaminophen
• Lorcet, Lortab
•Schedule III – high psychological/medium physical
•Pain and post-surgical use (pain)

Drug Overdose Rate Higher than Motor Vehicle Death Rate
5/22/2018 37Source: CDC

Drug Poisoning Deaths Involving Opioids: USA, 2000-2013
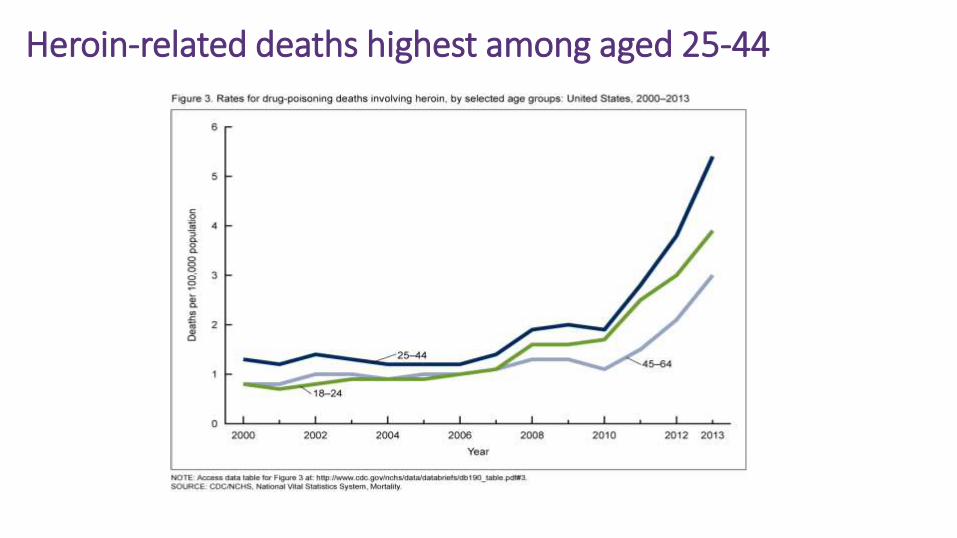
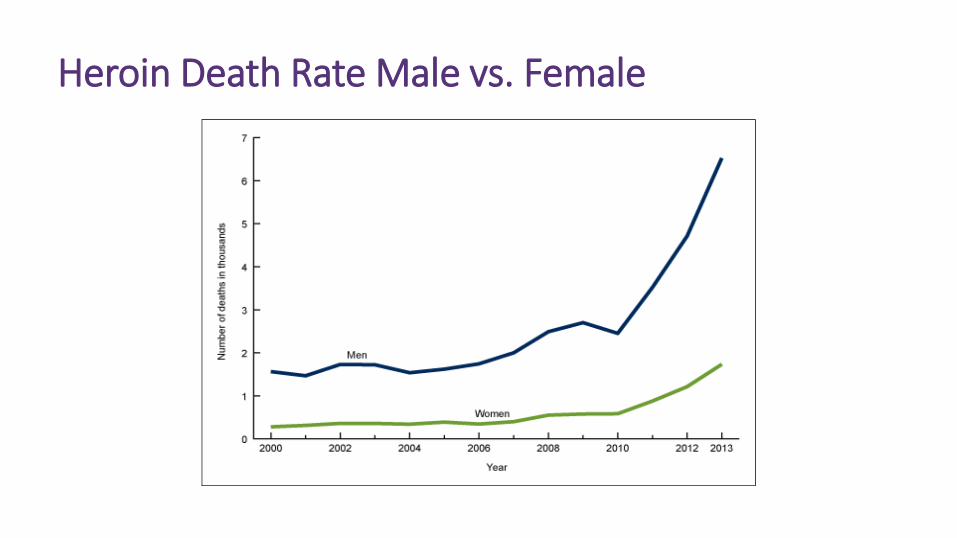
Heroin-related deaths highest among aged 25-44

Treatment
• Traditional Recovery Based/NA
• Naltrexone - Antagonist/Blocker
• Opiate Maintenance Tx – withdrawal management• Methadone- daily
• Buprenorphine/Suboxone
• Methadone to abstinence models
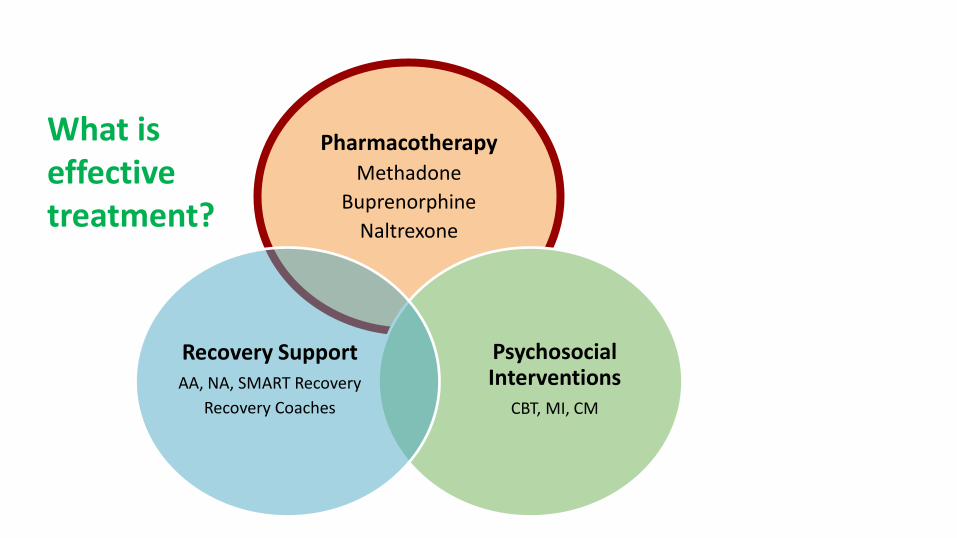
PharmacotherapyMethadone
Buprenorphine
Naltrexone
Psychosocial Interventions
CBT, MI, CM
Recovery SupportAA, NA, SMART Recovery
Recovery Coaches
What is effective treatment?

Detox
• Detox: Medical risk with opioid withdrawal is low, while discomfort is very high • Inpatient • Outpatient
• Only recommended during 2nd trimester of pregnancy if mother is invested
• Otherwise methadone stabilization is in best interest of mother and fetus

Levels of Care
• Inpatient rehabilitation• 5-21 days length of stay• Focus on medical/psychiatric stabilization• May initiate Suboxone for opiates
• Community residence (halfway houses)• Supportive living environment• 3-12 months

Levels of Care
• Intensive Residential
▪ Supportive environment – therapeutic community
▪ Longer term stays 6-24 months
▪ Focus on rehabilitation/sober living skills
• Outpatient
▪ Intensive outpatient
Federal Position
• Drug courts that receive federal dollars will no longer be allowed to ban the kinds of medication-assisted treatments that doctors and scientists view as the most effective care for opioid addicts, Botticelli announced in a conference call with reporters. (Michael Botticelli ONDCP Director)
• "We've made that clear: If they want our federal dollars, they cannot do that. We are trying to make it clear that medication-assisted treatment is an appropriate approach to opioids.” (Pamela Hyde, SAMHSA’s Administrator)
5/22/2018 46
BJA GrantsApplicants must demonstrate that the drug court for which funds are being sought will not:
1.deny any appropriate and eligible client for the drug court access to the program because of their medically necessary use of FDA-approved medication assisted treatment (MAT) medications (methadone, injectable naltrexone, non-injectable naltrexone, disulfiram, acamprosate calcium, buprenorphine) that is in accordance with an appropriately authorized physician's prescription; and
2.mandate that a drug court client no longer use medically necessary MAT as part of the conditions of the drug court if such a mandate is inconsistent with a physician's recommendation or prescription. Under no circumstances may a drug court judge, other judicial official, or correctional supervision officer connected to the identified drug court deny the use of these medications when medically necessary and when available to the clients and under the conditions described above.
5/22/2018 47
Pharmacological Approaches
Goals – Provide:• relief from withdrawal symptoms,
• prevent drugs from working,
• reduce craving,
• aversive reactions
These actions are helpful in
reducing relapse and increasing
retention in programs

Does Treatment Work?
• Medications +psychosocial therapy bothbenefit brain function and recovery.
• Each affects different partsof brain and inopposite ways.
PET scans adapted and retouched from Goldapple et al. 2004
Pharmacological Approaches
Methadone – Opiate addiction – reduces craving, mediates withdrawal symptoms, helps restore normal functioning
Buprenorphine (Suboxone) – similar to methadone, may be prescribed by an MD with special training)

Pharmacological Approaches
Naltrexone (Vivitrol) – stops opiates from working, changes alcohol action for some – reduction in relapse – 30 day dose.
Baclofen – possible reduction in cocaine cravings
Patient Needs
Diabetes
• Some can control with diet
• Some can control with medication
• Some are insulin dependent
• Without adequate treatment -many will die
Opiod Addicts
• Some can quit on own
• Some can remain abstinent with “regular” treatment
• Some need ORT
• Without adequate treatment -many will die

Methadone EffectivenessGunne & Gronbladh, 1984
H H HH
H H HH
H H HH
H H HH
H
H H HH
H H HH
H H HH
H H HH
H
Methadone Regular Outpatient Rx.
Baseline
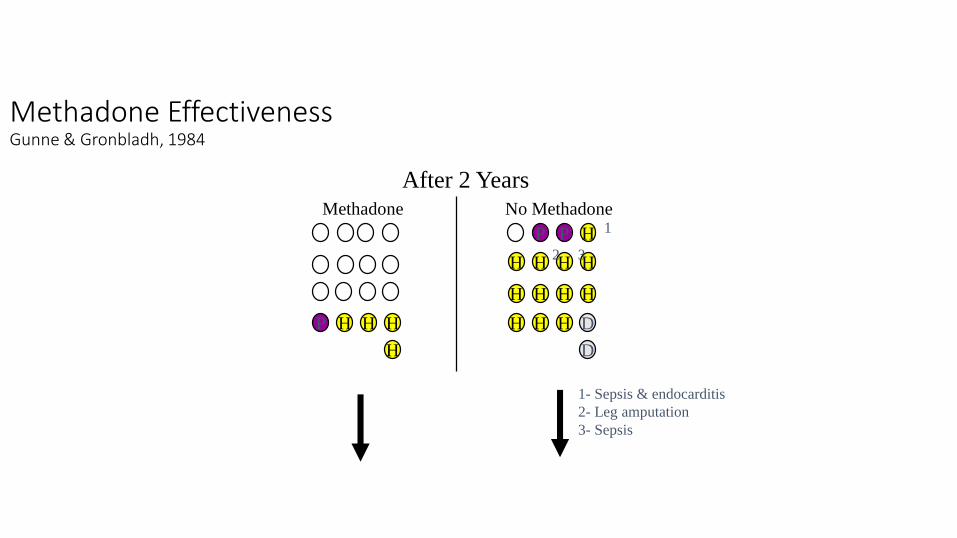
Methadone EffectivenessGunne & Gronbladh, 1984
After 2 Years
1- Sepsis & endocarditis
2- Leg amputation
3- Sepsis
P H HH
H
P HP
H H HH
H H HH
H H H
Methadone No Methadone1
32
D
D
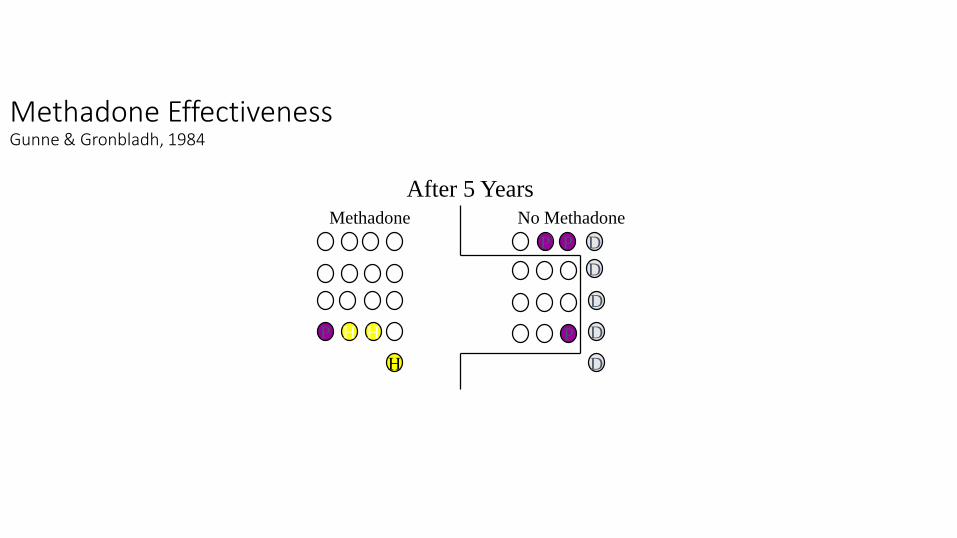
Methadone EffectivenessGunne & Gronbladh, 1984
P H H
H
P
Methadone No Methadone
After 5 Years
P P D
D
D
D
D

Centers for Disease Control (2011)
Retention in treatmentHeilig, Lancet 2003
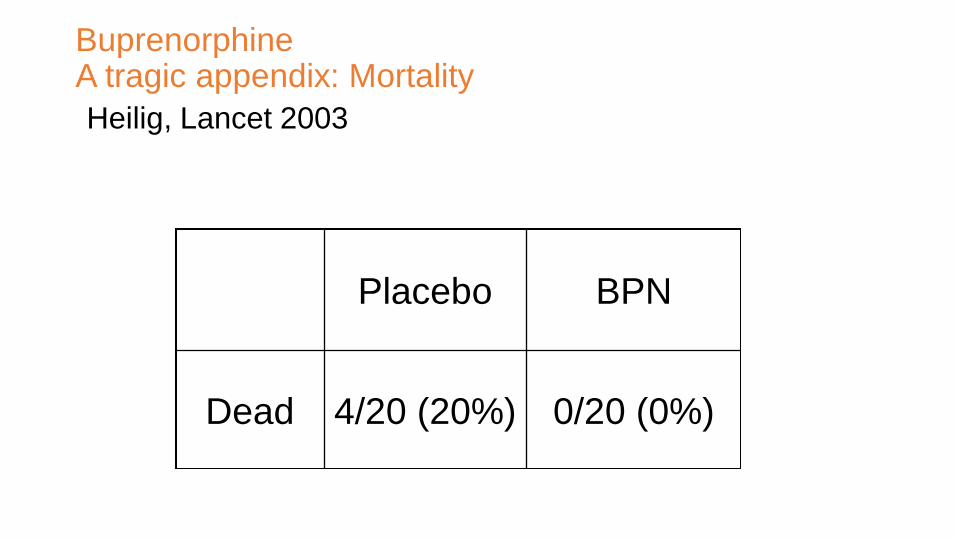
BuprenorphineA tragic appendix: Mortality
Heilig, Lancet 2003
Placebo BPN
Dead 4/20 (20%) 0/20 (0%)

Vivitrol•Long Acting Injectable
•Helps with compliance
•Non-Addicting

Is Vivitrol “THE ANSWER”?
2015 Vermont Review
• Research is limited. FDA approval based on a single 6 month trial in Russia.
• Health Risk – Liver toxicity, Death (51 from 2006-2010)
• Overdose Risk upon termination
• Effective for Some – still to be defined

Is naltrexone (XRN) effective?
1. XRN vs. Placebo RCT (Lancet 2011)a.Setting: Russia; Funder: Alkermesb.Enrolled patients post-detoxification (≥7 days since last use)c.Outcome: XRN: ↑ retention; ↑ opioid free weeks; ↓cravings
2. XRN vs. Usual Care RCT (NEJM 2016)a.Setting: USA; Funder: NIDA; Alkermes donated XRNb.Enrolled justice-involved pts preference for “opioid free” txc.Outcome: XRN: ↑ time to relapse (10.5 weeks vs 5.0 weeks)
3. Two Comparative XRN vs. Bupe Studies (2017)

XRN vs. Bupe1. XRN vs. Bupe RCT (Tanum, JAMA 2017)
a.Setting: Norway; Funder: RCN; Alkermes allowed commentsb.Recruited; sent for detoxification; then enrolled/analyzedc.232 recruited → 165 included (51 refused; 6 failed detox)d.Outcome: XRN and Bupe similar in reducing opioid use
2. XRN vs. Bupe RCT (Lee, Lancet 2017)a.Setting: USA; Funder: NIDA; Indivior donated Suboxoneb.Recruited; stratified; analyzed both per-protocol and ITTc.ITT: Bupe>XRN; 28% of XRN vs. 6% bupe never started TXd.PP: Of those who started, relapse rates similar for both

Naltrexone group
72% successfully inducted
Patients successfully inductedPatients not inducted on medication
Buprenorphine group
94% successfully inducted
Patients less likely to successfully start naltrexone than bupe.
XRN vs. Bupe
Slide courtesy of NYC DOHMH
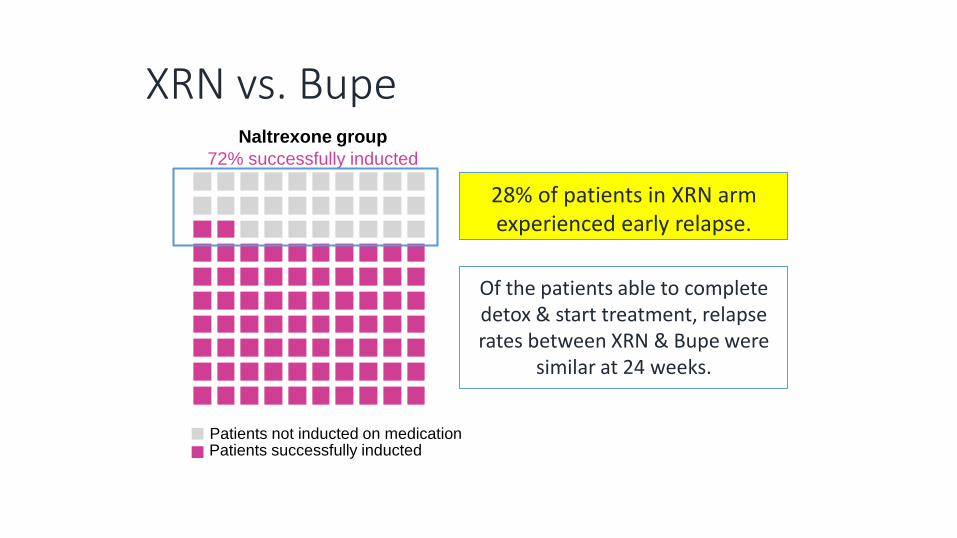
XRN vs. BupeNaltrexone group
72% successfully inducted
Patients successfully inductedPatients not inducted on medication
28% of patients in XRN arm experienced early relapse.
Of the patients able to complete detox & start treatment, relapse rates between XRN & Bupe were
similar at 24 weeks.
NARCAN - Overdose Reversal Kits
5/22/2018 65

Summary
1. Opioid addiction is a chronic condition associated with multiple harms, including fatal overdose, and that requires ongoing social support and medical care.
2. Drug possession/use and crime committed to pay for drugs and prevent opioid withdrawal result in frequent criminal justice exposure.
3. Treatment exists and is effective at reducing harms of opioid addiction. Medications for Addiction Treatment (MAT) such as methadone & buprenorphine have the strongest evidence base, with emerging evidence to support naltrexone in highly motivated patients.
4. Ultimately, all treatment options should be available to patients and decision regarding treatment modality should be made between patient and health care provider.