Embed Size (px)
Citation preview

154 Aging Clin Exp Res, Vol. 19, No. 2
Aging Clin Exp Res 19: 154-159, 2007©2007, Editrice Kurtis
Key words: Aging, body composition, BMI, disability, obesity, sarcopenia.Correspondence: Mauro Zamboni, MD, Cattedra di Geriatria, Università di Verona, Ospedale Maggiore, Piazzale Stefani 1, 37126Verona, Italy.E-mail: [email protected] April 15, 2005; accepted in revised form June 7, 2006.
ABSTRACT. Background and aims: To evaluate therelation between baseline body composition and 2-year onset of functional limitation in elderly subjects atthe high end of the functional spectrum. Methods: An-thropometric measurements, physical functioning asmeasured by a modified version of the Activities of Dai-ly Living Scale, and baseline albumin, were evaluatedin 145 men and women aged 66-78 years, free offunctional limitations, selected from the general pop-ulation of Verona. In each subject, total body fat mass(FM) and appendicular FFM (ASMM) were measured bydual-energy X-ray absorptiometry; the FM (FMI) andASMM indexes (ASMMI) were also calculated by di-viding each body composition variable by heightsquared. Results: After 2 years of follow-up, 48.2% ofwomen and 40% of men had developed mild levels ofdisability, with limitations in kneeling, bending andclimbing stairs. In women, but not in men, a BMIhigher than 25 Kg/m2 or values of FMI higher than the50th percentile, were significantly associated with a 3to 5 times increased risk of limitations in climbingstairs and lower body performance. In men, a trendwas found between low values of ASMMI and an in-creased risk of limitations in kneeling and bending. Af-ter cross-tabulating categories based on the 50th per-centile of ASMMI and FMI, high values of FMI, inde-pendently of ASMMI, were significantly related withhigher incidence of limitation in climbing stairs inwomen. In women, the highest 2-year incidence oflimitation in climbing stairs was found in the group ofobese subjects. Conclusions: High body fat and highBMI values were associated with a greater probability
High baseline values of fat mass, independently ofappendicular skeletal mass, predict 2-year onset ofdisability in elderly subjects at the high end of thefunctional spectrumElena Zoico1, Vincenzo Di Francesco1, Gloria Mazzali1, Alessandra Zivelonghi1, Stefano Volpato2,Arianna Bortolani1, Andrea Dioli1, Alessandra Coin3, Ottavio Bosello1, and Mauro Zamboni11Division of Geriatric Medicine, University of Verona, Verona, 2Department of Clinical and ExperimentalMedicine, University of Ferrara, Ferrara, 3Division of Geriatric Medicine, University of Padova, Padova, Italy
of developing functional limitations 2 years later in apopulation of elderly subjects at the high end of thefunctional spectrum. Moreover, in women, high base-line values of fat mass, independently of appendicularfat-free mass, were more likely to predict the future on-set of functional limitations.(Aging Clin Exp Res 2007; 19: 154-159)©2007, Editrice Kurtis
INTRODUCTIONBody composition changes progressively with age (1,
2). To what extent the contribution of the two maincomponents of body weight, fat and muscle mass, tothe onset of physical function limitations in the elderly isstill a matter of debate (3).
To date, only a few cross-sectional epidemiological stud-ies have shown a relationship between low skeletal musclemass and physical functional limitations, with different indicesof sarcopenia (4-6). Janssen et al. (7), in a wide sample ofnon-institutionalized US population in the NHANES IIIstudy, recently identified cut-off values of skeletal musclemass associated with an increased risk of physical disability.
Conversely other cross-sectional studies show an as-sociation between high fat mass and functional limitationsin old age (8-12). Moreover, in a sample of elderly inde-pendent women, Zoico et al. (11) recently found that acomposite index of sarcopenia, as the ratio betweenskeletal muscle mass and weight, was related to functionalimpairment. Similarly, Newman et al. (13) have recentlyshown an association between appendicular lean mass ad-justed for height and body fat, and lower extremity func-tional limitations.
Aging Clinical and Experimental Research

Body composition and functional limitation
Aging Clin Exp Res, Vol. 19, No. 2 155
Aging Clin Exp Res 19: 154-159, 2007©2007, Editrice Kurtis
In the New Mexico Elder Health Survey (14), not on-ly sarcopenia and obesity, but also sarcopenic obesity, de-fined as sarcopenia associated with a high percentage offat mass, was related with functional impairment with an8 to 11 times increased risk of physical disabilities in oldmen and women.
The relation between body composition changes and dis-ability thus appears to be still under debate. The paucity oflongitudinal studies, together with the difficulty of obtainingdirect measures of body composition, makes the solution ofthis controversy even more complicated. To our knowledge,only a few longitudinal studies have focused on this topic,yielding contradictory results, depending on the charac-teristics of the populations studied and on the measures offunctional limitation and body composition available (15-19).
The aim of this study was therefore to investigateprospectively the relationship between body composi-tion and 2-year onset of functional limitations in a cohortof elderly healthy subjects, at the high end of the functionalspectrum, without any degree of physical functional im-pairment at baseline.
METHODSSubjects Subjects were recruited from the lists of 11 general
practitioners in Verona (Northern Italy) and were eligibleif weight-stable (no body weight fluctuations >5% in thelast year), if able to walk at least 800 meters without dif-ficulty, and free of cognitive impairment (Mini-MentalStatus Examination >24). Exclusion criteria included can-cer, renal insufficiency, heart failure (NYHA class II orhigher), serious lung disease at the beginning of thestudy, as well as participation in regular physical exercise
(>1/week) and weight changes (>5%) during the study pe-riod. All participants were volunteers and gave their con-sent to the study, the protocol of which was approved bythe Ethical Committee of University of Verona.
At baseline, 177 women and 97 men aged 66-78years were eligible and volunteered to participate in thestudy; 139 women and 75 men had complete data at fol-low-up. No significant differences in baseline characteristicswere found between those who were present for thefollow-up visit and those who did not return. Due to theaim of the study, analyses were restricted to a subgroupof subjects without functional limitation at baseline (85women, 61.2%; 60 men, 80%).
Anthropometric measurements, health and functionalstatus were evaluated at baseline and after 2 years of fol-low-up.
The characteristics of the study sample, at baseline, areshown in Table 1, separately by gender.
AnthropometryWith subjects wearing light clothes and no shoes,
body weight was measured to the nearest 0.1 Kg (Salusscale, Milan, Italy) and height to the nearest 0.5 cm on astadiometer (Salus stadiometer, Milan, Italy). BMI wascomputed as weight divided by height squared (Kg/m2).Waist circumference was measured with a tape at the nar-rowest part of the torso, viewed anteriorly. Hip circum-ference was measured at the outermost points on thegreater trochanters. The waist-to-hip ratio (WHR) was cal-culated from these circumferences.
Dual-energy X-ray absorptiometry (DXA)Total body fat (FM) and total fat-free mass (FFM) were
Table 1 - Characteristics of study population at baseline, separately by gender.
Women (n=85) Men (n=60)
Characteristics M±SD Range M±SD Range
Age (years) 71.62±2.28 66-78 71.72±2.41 67-78Weight (kg) 61.56±8.78 43.3-95.5 78.34±11.14 53-100.4Height (m) 1.56±0.06 1.41-1.69 1.70± 0.07 1.58-1.90BMI (kg/m2) 25.48±3.70 18.19-34.71 27.14±3.15 19.83-33.73Waist circumference (cm) 80.48±9.07 43-110 95.56±8.22 76-110WHR 0.84±0.07 0.42-1.03 0.97±0.05 0.87-1.13FM (Kg)* 23.96±6.49 8.86-42.90 21.78±6.52 7.1-40.53FMI (kg/m2) 9.91±2.78 3.45-18.71 7.54±2.12 2.46-12.14ASMM (Kg)* 13.34±1.85 9.95-19.44 21.52±2.79 14.6-29.43ASMMI (kg/m2) 5.50±0.71 3.99-8.05 7.46±0.81 5.83-9.81Drugs prescribed (n) 1.75±1.40 0-7 1.42±1.18 0-4Number of diseases (n) 1.80±1.32 0-6 1.63±1.10 0-5Albumin (g/L) 43.53±3.02 36.6-55 43.99±3.00 38.50-54.30
WHR: waist to hip ratio; FM: fat mass; FMI: fat mass index; ASMM: appendicular skeletal muscle mass; ASMMI: appendicular skeletal muscle mass index; *Measured by dual-energy X-ray absorptiometry.

E. Zoico, V. Di Francesco, G. Mazzali, et al.
156 Aging Clin Exp Res, Vol. 19, No. 2
Aging Clin Exp Res 19: 154-159, 2007©2007, Editrice Kurtis
measured by dual-energy X-ray absorptiometry (DXA)(Hologic QDR 2000, Waltham, USA) (20, 21) with soft-ware version 7.2, as previously described (9). FM was ex-pressed in Kg; FFM was considered as the sum of totalbody lean mass and bone mineral mass and expressed inKg. Arm and leg compartments were also examined bythe sub-region option of the software. Appendicularskeletal muscle mass (ASMM) was calculated as the sumof arm and leg lean soft tissue masses (11). The appen-dicular skeletal muscle mass adjusted by the height squaredindex (ASMMI) was also obtained as described by Baum-gartner et al. (4). In analogy with the BMI, the FM index(FMI) was calculated by subdividing FM by height squared(22).
The coefficient of variation (CV) for double determi-nations performed on the same day, in 11 subjects (menand women aged 66-78 years), with subjects reposi-tioned between scans, was 1% for FM and 1.3% forASMM.
Reported disabilityPhysical functioning was assessed, according to Lan-
glois et al. (23), with a questionnaire containing a com-bination of three scales: the ADL scale (24), three Rosow-Breslau physical function items (25) and the IADL scale(26). The questionnaire identifies 4 levels of disability: nodisability (Level 1), ADL disability (Level 4) and two mid-levels of impaired function, mild disability (Level 2) andmoderate disability (Level 3) (21).
For analytical purposes, overall functional disabilitywas also defined dichotomously and subjects were clas-sified into two groups: 1) no physical functional limitations,and 2) physical functional limitations, if subjects reportedany difficulty in any item of the questionnaire. Lower bodyperformance was evaluated by combining two highermobility items (walking 800 meters and climbing stairs) ac-cording to Guralnik et al. (27).
Health statusThe presence of acute and chronic conditions, and use
of medications, were determined according to standard-ized questionnaires already in use in the Italian Longitu-dinal Study on Aging (28).
Albumin was determined on fasting venous bloodsamples by a colorimetric test (Vitros 950 ALB slides, J&JHealth, Cone System, Piscataway, NJ). The sensitivity ofthis assay has been shown to be 10 g/L. Intra-assayCVs were 1.3 to 1.5%.
Statistical analysesResults are shown as means ± SD. Student’s paired t-
test was used to compare mean values of baseline and 2-year follow-up variables. Various body composition cat-egories were created separately by gender, based on the50th percentile of BMI, FMI and ASMMI. Subjects were
classified in the reference group if BMI and FMI valueswere lower than the corresponding 50th percentile, or ifthe ASMMI values were higher than the corresponding50th percentile value. The odds ratio (95% CI) predictinga 2-year risk of overall disability or various types of limi-tations, based on BMI or body composition categories,were obtained separately by gender from logistic regres-sion models, after controlling for baseline age, number ofdiseases and presence or absence of osteoarthrosis. FMIand ASMMI were studied in separate regression models,and further adjustment was performed respectively forFFM or FM.
In the absence of a young reference group for bodycomposition measurements to define sarcopenia andsarcopenic obesity, an approach similar to that of Davisonet al. (10) was used, and four groups were created bycross-tabulating FMI and ASMMI categories. ASMM wasused instead of FFM as a better muscle mass indicator, es-pecially in the elderly. Sarcopenic subjects were consideredas those with FMI and ASMMI <50th percentile, obesesubjects as those with FMI and ASMMI >50th percentile,and sarcopenic-obese those with FMI >50th percentile andASMMI <50th percentile. The difference between 2-yearincidence of functional limitation according to FMI-ASMMIcross-groups was tested using chi-squared analysis.
A significance level of 0.05 was used throughout thestudy. Statistical analyses were performed with the SPSSstatistical package (version 10.0 for Macintosh).
RESULTSAfter 2 years of follow-up, only 47% of women and
53.3% of men were still free of any degree of disability(data not shown in table). Subjects without disability atbaseline mainly developed mild levels of disability (48.2%of women, 40% of men), whereas moderate or ADLdisability appeared only in a small proportion of thestudy population in both genders (respectively 2.4% and2.4% in women, 5% and 1.7% in men). In both genders,the items for which limitations of any degree were morefrequently reported were kneeling and bending (36.5% ofwomen, 28.3% of men), climbing stairs (23.6% of wom-en, 16.7% of men) and doing heavy housework (24.7%of women, 10% of men).
The onset of functional limitation, after 2 years offollow-up, was paralleled by a significant increase in thenumber of diseases and medications, in both women(respectively M±SD: 1.8±1.32 to 2.62±1.44, p<0.001and 1.75±1.40 to 2.28±1.60, p<0.001) and men (re-spectively M±SD: 1.63±1.10 to 2.15±1.16, p<0.001and 1.42±1.18 to 1.90±1.45, p<0.01). However, nei-ther men nor women had any significant changes intheir weight or BMI after 2 years of follow-up (in men,M±SD: 78.1±11.3 to 78.0±11.0 kg and 27.1±3.2 to27.3±3.1 Kg/m2; in women, M±SD: 62.1±8.5 to61.8±8.7 kg and 25.7±3.6 to 25.6±3.5 Kg/m2).

Body composition and functional limitation
Aging Clin Exp Res, Vol. 19, No. 2 157
Aging Clin Exp Res 19: 154-159, 2007©2007, Editrice Kurtis
Tables 2 and 3 present, separately by gender, variouslogistic regression models, in which overall disability or sin-gle items of the questionnaire were the dependent vari-ables, and age, number of diseases, osteoarthrosis, BMI,FMI or ASMMI categories the independent variables. Inwomen, a BMI higher than 25 Kg/m2 or FMI valueshigher than the 50th percentile were significantly associ-ated with a 3 to 5 times increased risk of limitations inclimbing stairs and lower body performance, even after ad-justment for baseline age, number of diseases, os-teoarthrosis and FFM (Table 2). In men, a trend toward anincreased risk of limitations in climbing stairs and lowerbody performance was found for subjects with FMI in thehigher group (Table 3). Moreover, men with ASMMIlower than the 50th percentile showed a trend toward anincreased risk of impairment in kneeling and bending(Table 3).
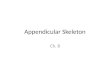
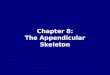
To study the joint contribution of fat mass and skeletalmuscle mass to 2-year risk of functional limitation, fourgroups were created by cross-tabulating FMI and ASMMIcategories separately in men and women. Women withhigh values of FMI, independently of their ASMMI, had asignificantly higher 2-year incidence of limitation in climb-ing stairs (χ2=0.024) (Fig. 1). Similar but non-significantresults were found in the group of men, with 50% and
20% of all disabled subjects respectively in the groupwith high values of FMI and ASMMI and in that with highvalues of FMI but low values of ASMMI (data not shownin figure). In women, the highest 2-year incidence oflimitation in climbing stairs was found in the group ofobese subjects (Fig. 1).
Table 2 - Odds ratio from logistic regression models predicting total and different types of disability after 2-year follow-up, based on BMI,FMI and ASMMI in women (n=85).
Total Lower body Climbing Kneeling and disability performance stairs bending
OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI)
BMI <25 Kg/m2* 1.00 1.00 1.00 1.00BMI >25 Kg/m2* 1.69 (0.69-4.14) 3.54 (1.09-11.49) 3.96 (1.21-12.99) 1.23 (0.48-3.12)FMI <9.9 Kg/m2† 1.00 1.00 1.00 1.00FMI >9.9 Kg/m2† 1.46 (0.58-3.69) 4.95 (1.41-17.41) 5.54 (1.57-19.62) 1.12 (0.42-2.92)ASMMI <5.4 Kg/m2‡ 0.73 (0.30-1.81) 0.45 (0.15-1.39) 0.55 (0.18-1.63) 0.69 (0.27-1.77)ASMMI >5.4 Kg/m2‡ 1.00 1.00 1.00 1.00
FMI: fat mass index; ASMMI: appendicular skeletal muscle mass index; *adjusted for baseline age, number of diseases, and osteoarthrosis; †adjusted for base-line age, number of diseases, osteoarthrosis and FFM; ‡adjusted for baseline age, number of diseases, osteoarthrosis and FM.
Table 3 - Odds ratio from logistic regression models predicting total and different types of disability after 2-year follow-up, based on BMI,FMI and ASMMI in men (n=60).
Total Lower body Climbing Kneeling and disability performance stairs bending
OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI)
BMI <27 Kg/m2* 1.00 1.00 1.00 1.00BMI >27 Kg/m2* 0.47 (0.16-1.41) 2.33 (0.57-9.51) 2.36 (0.53-10.61) 0.52 (0.15-1.74)FMI <7.7 Kg† 1.00 1.00 1.00 1.00FMI >7.7 Kg† 1.35 (0.46-3.95) 3.92 (0.83-18.42) 3.62 (0.71-18.63) 1.29 (0.38-4.33)ASMMI <7.6 Kg/m2‡ 1.63 (0.54-4.89) 0.29 (0.06-1.28) 0.42 (0.09-1.92) 2.48 (0.70-8.76)ASMMI >7.6 Kg/m2‡ 1.00 1.00 1.00 1.00
FMI: fat mass index; ASMMI: appendicular skeletal muscle mass index; *adjusted for baseline age, number of diseases, and osteoarthrosis; †adjusted for base-line age, number of diseases, osteoarthrosis and FFM; ‡adjusted for baseline age, number of diseases, osteoarthrosis and FM.
0
20
40
60
ASMMI>50th perc.
ASMMI<50th perc.
10
50
30
10
%
χ2=0.024
FMI <50th perc.FMI >50th perc.
Women (n=85)
Fig. 1 - Percentage of women reporting difficulty in climbing stairsafter 2-year follow-up, according to ASMMI-FMI cross-groups

E. Zoico, V. Di Francesco, G. Mazzali, et al.
158 Aging Clin Exp Res, Vol. 19, No. 2
Aging Clin Exp Res 19: 154-159, 2007©2007, Editrice Kurtis
DISCUSSIONOur study showed that, even after a relatively short fol-
low-up, about 48% of women and 40% of men aged 66to 78 years at baseline, selected to be representative of thehigh end of the functional spectrum, developed mild andmoderate levels of disability. The main finding of this studywas that elderly women with high baseline values ofFMI, independently of ASMMI, were more likely to de-velop functional limitations 2 years later.
The longitudinal association between fat-free mass atbaseline and incident disability was generally weak inour population. A trend was found between low values ofASMMI and disability only in men, and only in one itemof the questionnaire. The small sample size and lack of ob-jective assessment of physical function may have re-duced the strength of the association between musclemass and disability. However, in 3694 elderly subjects ofthe Cardiovascular Health Study, severe sarcopenia wasonly a modest independent risk factor for the developmentof disability over the 8-year follow-up period (19). In ad-dition in a sample of 451 elderly men and women in theNew Mexico Aging Process Study, Baumgartner et al. (17)found that sarcopenia, in the absence of obesity, was nota significant risk factor for disability. In a large populationof elderly men and women, Visser et al. (15) observed thatonly high values of fat mass at baseline were predictive ofdisability 3 years later, whereas in yet another studyboth increased fat mass and decreased fat-free masswere prospectively associated with decreased functionalstatus (16).
Together, these findings (15-17,19) have led to hy-potheses that the effects of low muscle mass on the de-velopment of disability may not be as strong as previouslythought, based on cross-sectional observations (4-7).However, the means by which sarcopenia is classified,how muscle mass is measured, as well as the character-istics of the populations studied and the length of their fol-low-up, all seem to be crucial aspects in determining thestrength of the association between sarcopenia and func-tional status. The great effect of sarcopenia on the risk ofdisability was also described in the Health Aging andBody Composition (ABC) Study, in which mid-thigh mus-cle was measured by computed tomography (18).
In our study, despite the relatively small sample size, theclearly unfavorable effect of fat mass on functional statuswas found, confirming previous cross-sectional observa-tions (8-12). The 2-year risk of impairment in lower mo-bility tasks was 3 to 5 times increased in women withbaseline BMI higher than 25 Kg/m2 and FMI higherthan the 50th percentile, with a trend in the group of men.Interestingly, in the Health ABC Study, total body fat masswas a strong predictor of incident mobility limitation,independently of thigh muscle mass measured by CT,muscle strength and muscle mass fat infiltration (18).These findings suggest that interventions aimed at pre-
venting or delaying disability should focus on optimizingboth compartments of body composition. Thus, future re-search on body composition and physical function shouldtarget the joint contribution of both compartments inthe disabling process.
To our knowledge, few cross-sectional (10, 11, 14)and only one longitudinal study (17) have previously an-alyzed the joint effect of fat-free mass and fat mass ondisability risk. Subjects with sarcopenic obesity at base-line were 3 times more likely to report onset of IADLdisability during the 8-year follow-up period than sar-copenic or obese subjects (17). After cross-tabulatingFMI and ASMMI, our results support the hypothesis thathigh baseline values of fat mass, independently of theamount of appendicular fat-free mass, are more likelyto predict 2-year onset of functional limitations. Obesityin the elderly thus seems to act synergistically withsarcopenia to maximize disability, creating a vicious cir-cle in which increased weakness due to sarcopenia is as-sociated with the need to carry greater weight, due toobesity (29).
Our study has some limitations that deserve com-ment: first, a relatively small sample size. However, oursubjects were free of several potential confounders likeweight changes prior to and during the study period,changes in physical activity profiles, poor nutritional orfunctional status, and high comorbidity at baseline. Furtherlongitudinal studies with larger sample sizes are thus re-quired to confirm and expand our results. Second, ourstudy population was limited to relatively healthy oldsubjects, and thus cannot be considered representative ofa normal aging population. Third, our study lacked per-formance-based measures of physical function.
In conclusion, our study shows that body compositioncompartments are significant predictors of the onset offunctional decline in the elderly. High body fat and highBMI values were associated with a greater probabilityof functional limitations in a population of elderly subjectsat the high end of the functional spectrum. Obesity in theelderly is still associated with a greater likelihood of dis-ability. However, further longitudinal studies, evaluating thejoint effect of fat and fat-free mass on physical function,are mandatory, in order to develop interventions aimed atpreventing the burden of disability in the elderly.
ACKNOWLEDGEMENTSThis work was supported by grants from MIUR, COFIN 2003 n
2003069951_002.
REFERENCES1. Baumgartner RN, Stauber PM, McHugh D, Koehler KM, Garry
PJ. Cross-sectional age differences in body composition in persons60+ years of age. J Gerontol Med Sci 1995; 50A: 307-16.
2. Kehayias JJ, Fiatarone MA, Zhuang H, Roubenoff R. Totalbody potassium and body fat: relevance to aging. Am J Clin Nu-tr 1997; 66: 904-10.

Body composition and functional limitation
Aging Clin Exp Res, Vol. 19, No. 2 159
Aging Clin Exp Res 19: 154-159, 2007©2007, Editrice Kurtis
3. Fried LP, Guralnik JM. Disability in older adults: evidence re-garding significance, etiology and risk. J Am Geriatr Soc 1997;45: 92-100.
4. Baumgartner RN, Koehler KM, Gallagher D, et al. Epidemiologyof sarcopenia among the elderly in New Mexico. Am J Epi-demiol 1998; 147: 755-63.
5. Melton LJ, Khosla S, Crowson CS, O’Connor MK, O’Fallon WM,Riggs BL. Epidemiology of sarcopenia. J Am Geriatr Soc 2000;48: 625-30.
6. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass(sarcopenia) in older persons is associated with functional impairmentand physical disability. J Am Geriatr Soc 2002; 50: 889-96.
7. Janssen I, Baumgartner RN, Ross R, Rosenberg IH, Roubenoff R.Skeletal muscle cutpoints associated with elevated physical dis-ability risk in older men and women. Am J Epidemiol 2004; 159:413-21.
8. Visser M, Harris TB, Langlois J, et al. Body fat and skeletal mus-cle mass in relation to physical disability in very old men and wom-en of the Framingham Heart Study. J Gerontol Med Sci 1998;53A: 214-21.
9. Zamboni M, Turcato E, Santana H, et al. The relationship be-tween body composition and physical performance in olderwomen. J Am Geriatr Soc 1999; 47: 1403-8.
10. Davison KK, Ford ES, Cogswell ME, Dietz WH. Percentage ofbody fat and body mass index are associated with mobility limi-tations in people aged 70 and older from NHANES III. J Am Geri-atr Soc 2002; 50: 1802-9.
11. Zoico E, Di Francesco V, Guralnik JM, et al. Physical disability andmuscular strength in relation to obesity and different body com-position indexes in a sample of healthy elderly women. Int J Obes2004; 28: 234-41.
12. Santana H, Zoico E, Turcato E, et al. Relation between body com-position, fat distribution, and lung function in elderly men. Am JClin Nutr 2001; 73: 827-31.
13. Newman AB, Kupelian V, Visser M, et al. Sarcopenia: alternativedefinitions and associations with lower extremity function. J AmGeriatr Soc 2003; 51: 1602-9.
14. Baumgartner R. Body composition in healthy aging. Ann N YAcad Sci 2000; 904: 437-48.
15. Visser M, Langlois J, Guralnik JM, et al. High body fatness,but not low fat-free mass, predicts disability in older men andwomen: Cardiovascular Health Study. Am J Clin Nutr 1998; 68:584-90.
16. Broadwin J, Goodman-Gruen D, Slymen D. Ability of fat and fat-free mass percentages to predict functional disability in older menand women. J Am Geriatr Soc 2001; 49: 1641-5.
17. Baumgartner RN, Wayne SJ, Waters DL, Janssen I, Gallagher D,Morley JE. Sarcopenic obesity predicts instrumental activities of dai-ly living disability in the elderly. Obes Res 2004; 12: 1995-2004.
18. Visser M, Goodpaster BH, Kritchevsky SB, et al., for the HealthABC Study. Muscle mass, muscle strength, and muscle fat infil-tration as predictors of incident mobility limitations in well-func-tioning older persons. J Gerontol Med Sci 2005; 60A: 324-33.
19. Janssen I. Influence of sarcopenia on the development of phys-ical disability: the Cardiovascular Health Study. J Am Geriatr Soc2006; 54: 56-62.
20. Mazess RB, Barden HS, Bisek JP, Hanson J. Dual-energy X-rayabsorptiometry for total-body and regional bone-mineral andsoft-tissue composition. Am J Clin Nutr 1990; 51: 1106-12.
21. Pietrobelli A, Formica C, Wang Z, Heymsfield SB. Dual-energy X-ray absorptiometry body composition model: review of physicalconcepts. Am J Physiol 1996; 271: E941-51.
22. Van Itallie TB, Yang MU, Heymsfield SB, Funk RC, Boileau R.Height-normalized indices of the body’s fat-free mass and fat mass:potentially useful indicators of nutritional status. Am J Clin Nutr1990; 52: 953-9.
23. Langlois JA, Maggi S, Harris T, et al. Self-report of difficulty inperforming functional activities identifies a broad range of disabilityin old age. J Am Geriatr Soc 1996; 44: 1421-8.
24. Katz SC, Ford AB, Moskovitz RW. Studies of illness in the aged.The Index of ADL: a standardized measure of biological and psy-chosocial function. JAMA 1963; 185: 914-9.
25. Rosow I, Breslau N. A Guttman health scale for the aged. JGerontol Med Sci 1966; 21A: 556-9.
26. Lawton MP, Brody EM. Assessment of older people: self-main-taining and instrumental activities of daily living. J Gerontol MedSci 1982; 37A: 91-9.
27. Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, WallaceRB. Lower-extremity function in persons over the age of 70 yearsas a predictor of subsequent disability. N Engl J Med 1995;332: 556-61.
28. The Italian Longitudinal Study on Aging Working Group. Preva-lence of chronic diseases in older Italians: comparing self-re-ported and clinical diagnoses. Int J Epidemiol 1997; 26: 995-1002.
29. Roubenoff R. Sarcopenic obesity: the confluence of two epi-demics. Obes Res 2004; 12: 887-8.