Embed Size (px)
Citation preview

Research ArticleHigh-Dose Compound Heat Map for 3D-Cultured GlioblastomaMultiforme Cells in a Micropillar and Microwell Chip Platform
DongWoo Lee,1 Sang-Yun Lee,2 Il Doh,3 Gyu Ha Ryu,4 and Do-Hyun Nam2,5
1Department of Biomedical Engineering, Konyang University, Daejeon 35365, Republic of Korea2Department of Health Sciences and Technology, SAIHST, Sungkyunkwan University, Seoul 06351, Republic of Korea3Center for Medical Metrology, Korea Research Institute of Standards and Science (KRISS), Daejeon, Republic of Korea4Office of R&D Strategy & Planning, Samsung Medical Center, Seoul, Republic of Korea5Department of Neurosurgery, SamsungMedical Center, SungkyunkwanUniversity, School ofMedicine, Seoul 06351, Republic of Korea
Correspondence should be addressed to Gyu Ha Ryu; [email protected] and Do-Hyun Nam; [email protected]
Received 24 February 2017; Revised 9 June 2017; Accepted 20 June 2017; Published 18 October 2017
Academic Editor: Sara Piccirillo
Copyright © 2017 Dong Woo Lee et al.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Glioblastoma multiforme (GBM) is recognized as the most common and lethal form of central nervous system cancer. To cureGBM patients, many target-specific chemotherapeutic agents have been developing. However, 2D monolayer cell-based toxicityand efficacy tests did not efficiently screen agents due to the pool reflection of in vivo microenvironments (cell-to-cell and cell-to-extracellular matrix interaction). In this study, we used a 3D cell-based, high-throughput screening method reflecting themicroenvironments using a micropillar and microwell chip platform to draw a high-dose heat map of the cytotoxicity and efficacyof 70 compounds, with two DMSO controls. Moreover, the high-dose heat mapmodel compared the responses of four 3D-culturedpatient-derived GBM cells and astrocytes to high dosages of compounds with respect to efficacy and cytotoxicity, respectively, todiscern the most efficacious drug for GBM. Among the 70 compounds tested, cediranib (a potent inhibitor of vascular endothelialgrowth factor (VEGF) receptor tyrosine kinases) exhibited the lowest cytotoxicity to astrocytes and high efficacy to GBM cells in ahigh-dose heat map model.
1. Introduction
Glioblastoma multiforme (GBM) is the most common,aggressive, and lethal primary malignant brain tumor thatstems from astrocytes. These tumors are usually highlymalignant because the cells canmetastasize from the primarytumor without detection and invade the surrounding normalbrain tissue to form new tumor “satellites” that lead to tumorrecurrence [1]. The current standard of care is surgical resec-tion coupled with ionizing radiation (IR) and the chemother-apeutic agent temozolomide (Temodar�, Temodal�, TMZ) [2,3]. However, this treatment only provides patients with GBMa 12–14-month survival period after diagnosis [2, 3]. Despiteaggressive surgical resection and chemotherapy, almost allpatients with GBM present with tumor recurrence. Thus,many target-specific or general-chemotherapeutic agentshave been developed to cure patients with GBM. Althoughsome of the compounds exhibit good efficacy toward GBM,
the resulting cytotoxicity of normal glial cells in the centralnervous system has been an issue. To measure cytotoxicityof compounds in normal glial cells, neural stem cells orastrocytes are used [4, 5]. Astrocytes are the most abundantmember of the glial family and have a wide range of adaptivefunctions in the central nervous system (CNS). They interactwith neurons, provide structural, metabolic, and trophicsupport, participate in synaptic activity, mediate ionic andtransmitter homeostasis, and regulate blood flow [6, 7]. Sinceastrocytes play an important role in the CNS, treatment-induced toxicity of the CNS remains a major cause of mor-bidity in patients with cancer [8].Thus, a high-dose heat mapmodel comparing the responses of high-dose compounds onastrocytes and GBM cells is required to validate the mostefficacious drugs toward GBM. Previous high-dose heat mapmodels using 2D cell-based high-throughput screening arewell developed [9, 10]. However, because 2D cell-based assay
HindawiBioMed Research InternationalVolume 2017, Article ID 7218707, 7 pageshttps://doi.org/10.1155/2017/7218707

2 BioMed Research International
does not fully reflect in vivo microenvironments (cell-to-celland cell-to-extracellular matrix interaction), a 3D cell-basedassay was used to screen compounds [11–15], including ourpreviously developed system [13–17]. Especially, 3D culturedastrocyte and GBMs show more in vivo like model [18–20]. Thus, assay based on 3D cultured astrocyte and GBMswith high-throughput manner may give new potential toscreen GBM target agents. Our previous system [13–17]shows successfully data of 3D cell-based assays with high-throughput manner by comparing their own data with 2Dcell-based assay [13], gene [14], and clinical data [17]. Byapplying the abovementioned quantitative 3D-cultured cell-assay platform, astrocytes and patient-derived GBM cellswere 3D-cultured and screened to select themost representedcompounds that were not cytotoxic to normal brain cellsand were particularly efficient for patient-derived GBM cells.Figure 1 shows 3D cell-based high-throughput screeningchips culturing three-dimensionally four GBM cells andastrocyte. Since TMZ is a representative drug used in thetreatment of patients with GBM, it was used as a controlcompound to verify the high-dose heat map. By comparingTMZwith 69 other compounds, compounds in the high-doseheat map were tested for cytotoxicity and efficacy in GBMcells.
2. Materials and Methods
2.1. Astrocyte and Patient-Derived Cell Culture. We pur-chased NHA-astrocyte AGM (LONZA, Cat. number cc-2565). Astrocyte was cultured with ABM Basal media(LONZA, Cat. number cc-3187) added with AGM Single-Quot Kit Suppl.&Growth Factors (LONZA, Cat. number cc-4123). Patient-derived GBM cells were obtained from GBMpatients who underwent brain tumor removal surgery atthe Samsung Medical Center (Seoul, Korea). Informed con-sent was obtained from all patients. Following a previouslyreported procedure [13], surgical samples were enzymaticallydissociated into single cells. Four patient-derived cells wereobtained from four GBM patients. Dissociated GBM cellswere cultured in cell culture flasks (from Eppendorf, T-75)filledwithNeurobasal A (NBA) conditionedmedia.TheNBAconditionedmedia comprised N2 and B27 supplements (0.53each; Invitrogen) and human recombinant bFGF and EGF(25 ng/ml each; R&D Systems), hereafter, referred to as NBEcondition media. Cell flasks were placed in a humidified 5%CO2incubator (Sheldon Mfg., Inc.) at 37∘C. The cells were
routinely passed every 4 days at 70% confluence. For theexperiment, the cell suspensions were collected in a 50mlfalcon tube from the culture flask. GBM cells were then sus-pended in 5mL ofNBE conditionmedia. After centrifugationat 2000 rpm for 3min, the supernatant was removed, andthe cells were resuspended with NBA conditioned media toa final concentration of 10 × 106 cells/mL. The number ofcells in the NBA conditioned media was calculated with theAccuChip automatic cell counting kit (Digital Bio, Inc.). Therest of the cells were seeded at a concentration of 2 × 106 cellsin a T-75 flask containing 15mL of NBA conditioned media.
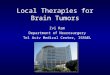
2.2. Chip Layout and Experimental Procedure. The basic lay-out of the micropillar and microwell chip for a 12-compoundscreening is shown in Figure 2.The microwell chip is dividedinto 72 lines, and each line has 6microwells for replicates. Forcompound analysis, approximately 100 cells (patient-derivedGBM cells) in 50 nL with a 0.75% alginate concentrationby volume (0.75w/w) were automatically dispensed ontoa micropillar chip by using ASFA� Spotter ST (Medical& Bio Device, South Korea). The ASFA Spotter ST usesa solenoid valve (The Lee Company, USA) for dispensingthe 50 nL droplets of the cell-alginate mixture and 1 𝜇L ofmedia or compounds. After dispensing the cells, as shown inFigure 1(b), the micropillar chip containing human cells inalginate was sandwiched (or “stamped”) with the microwellchip for 3D cell culture and compound efficacy tests. Asingle chip can screen 72 compounds with 6 replicatessimultaneously. A micropillar chip with alginate dispensedon each pillar spot and the microwell chip containing 72compounds are shown in Figure 2. The micropillar chip withcells dispensed is stamped together with its complementarymicrowell chip comprising 532 wells that are 1.2mm indiameter. One microliter of growth media was dispensedinto each microwell. The micropillar and microwell chip inthe combined form are shown in Figure 1(b). After 1 dayof incubation at 37∘C to stabilize the cells, the micropillarchip containing the cells was moved to a new microwell chipfilled with various test compounds. Next, the combined chipswere incubated for 3 days, as shown in Figure 1(b). Cellviability against the compounds was measured with CalceinAM live cell staining dye (4mM stock from Invitrogen),which stains viable cells with green fluorescence.The stainingdye solution was prepared by adding 1.0 𝜇L of Calcein AM(4mM stock from Invitrogen) to 8mL staining buffer (MBD-STA50, Medical & Bio Device, South Korea). To measurecell viability quantitatively after staining the alginate spots,cells on the micropillar chip were scanned. As shown inFigure 1(a), scanned images were obtained with an automaticoptical fluorescence scanner (ASFA Scanner ST, Medical &Bio Device, South Korea).
2.3. Workflow of High-Dose Compound Heat Map. The high-dose compound heat map model for measuring cytotoxicityand efficacy in GBM cells was quantified using a 3D cell-based screening using a micropillar and microwell chip.The workflow of high-dose compound heat map is shownin Figure 3. 72 compounds with high dosage, includingtwo DMSO controls, were screened against astrocytes andGBM cells for measuring toxicity and efficacy, respectively.Based on astrocyte cytotoxicity and efficacy of GBM cells,compounds were divided into four groups. For this heat map,we selected the most promising compounds that exhibitedless cytotoxicity toward astrocytes and high efficacy towardGBM cells.
3. Results and Discussion
To determine the cytotoxicity against normal glial cells, wetreated astrocytes (represented as normal glial cells) to high

BioMed Research International 3
Compound
Micropillar
Microwell
Astrocyte
PDC680T PDC464T
PDC096T PDC352T
GBMsin alginate
(a)
Loading cells 1 day before incubation Compound exposure Cell staining & analysis
ASFA spotter
(b)
Figure 1: 3D cell-based high-throughput screening chips. (a) Photo and schematic view of micropillar and microwell chip platform. Greendots are 3D-cultured astrocytes and glioblastoma multiforme (GBM) cells in alginate spot on the micropillar. (b) Schematic view of theexperimental procedure. Cells are dispensed and immobilized in alginate onto the top of the micropillars and dipped in the microwellscontaining growthmedia for 1-day culture by sandwiching themicropillar andmicrowell chips. Compounds are dispensed into themicrowellsand cells are exposed to the compounds by moving the micropillar chip to a new microwell chip. 3D-cultured cells are stained with CalceinAM, and the dried alginate spot on the micropillar chip is scanned for data analysis.
dosages (20𝜇M) of 72 compounds. Among the 72 com-pounds tested, TMZ is one of most popular drugs for GBM.The lipophilic nature of TMZ permits it to penetrate theblood-brain barrier and, thereby, allows it to be administeredorally. It has also been approved by the US FDA for use inthe treatment of refractory anaplastic astrocytoma in adultssince 1999 and in newly diagnosed adult patients with GBMsince 2005. Thus, we used TMZ as a control compound forcomparing cytotoxicity of compounds toward astrocytes. Weevaluated cytotoxicity of other compounds in comparison toTMZ and evaluated the efficacy of these compounds withpatient-derived GBM cells.
3.1. Toxicity of High-Dose Compounds in Astrocytes. The via-bility of astrocytes after exposure to 72 compounds (including2 DMSO control) after the 3- and 7-day treatment is shownin Figure 4. 16 compounds, including TMZ, exhibited highastrocyte viability and increased to >50% after the 3-daycompound treatment. On the seventh day, only 7 compoundsexhibited >50% astrocyte viability: cediranib, INCB28060,
nilotinib, LDE225, sotrastaurin, vismodegib, and amoralexhibited low toxicity (with astrocyte viability >50%). How-ever, TMZ, which is widely known for its low cytotoxicity,exhibited high toxicity (with astrocyte viability < 18%) afterthe 7-day compound treatment. 20 uM of TMZ is high doseand TMZ shows high toxicity for long-day culture (7 days).Thus, based on the 3-day compound treatment, we evaluatedthe cytotoxicity of the compounds by comparing the viabilityof astrocyte after exposure with other compounds and withTMZ (over 90%). Among 16 compounds, 7 exhibited similarastrocyte viability to TMZ, cediranib, INCB28060, ABT-888,dabrafenib, vismodegib, and amoral and therefore may begood candidates to test the efficacy against patient-derivedGBM cells.
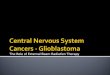
3.2. Efficacy Test of 70 Compounds for Patient-Derived GBMCells. The viabilities of astrocyte and four patient-derivedGBM cells after the 3-day compound treatment are shown inFigure 5. Most of the targeted compounds exhibited high effi-cacy with 20 uMdosages. By comparing efficacy of GBM cells

4 BioMed Research International
Cel
l spo
tsCompound 1Compound 2Compound 3Compound 4Compound 5Compound 6Compound 7Compound 8Compound 9Compound 10Compound 11Compound 12Compound 13Compound 14Compound 15Compound 16Compound 17Compound 18Compound 19Compound 20Compound 21Compound 22Compound 23Compound 24Compound 25Compound 26Compound 27Compound 28Compound 29Compound 30Compound 31Compound 32Compound 33Compound 34Compound 35Compound 36
Compoundd 1Compoundd 2Compoundd 3Compoundd 4Compoundd 5Compoundd 6Compoundd 7Compoundd 8Compoundd 9Compoundd 10Compoundd 11Compoundd 12Compoundd 13Compoundd 14Compoundd 15Compoundd 16Compoundd 17Compoundd 18Compoundd 19Compoundd 20Compoundd 21Compoundd 22Compoundd 23Compoundd 24Compoundd 25Compoundd 26Compoundd 27Compoundd 28Compoundd 29Compoundd 30Compoundd 31Compoundd 32Compoundd 33Compoundd 34Compoundd 35Compoundd 36
Compound 37Compound 38Compound 39Compound 40Compound 41Compound 42Compound 43Compound 44Compound 45Compound 46Compound 47Compound 48Compound 49Compound 50Compound 51Compound 52Compound 53Compound 54Compound 55Compound 56Compound 57Compound 58Compound 59Compound 60Compound 61Compound 62Compound 63Compound 64Compound 65Compound 66Compound 67Compound 68Compound 69Compound 70Compound 71Compound 72
Figure 2: Chip layout for high-dose 72 (including 2 DMSO controls)-compound heat map. Each compound has seven replicates.
and cytotoxicity of astrocytes, most of the compounds exhib-ited nonspecific, high toxicity for both GBM cells and astro-cytes. Among seven nontoxic compounds, INCB28060, ABT-888, vismodegib, and amoral did not suppress the patient-derived GBM cells.Thus, they may be ineffective compoundsin treating GBM. TMZ, cediranib, and dabrafenib exhibitedlowGBMcell viability inmore than one patient-derivedGBMcell. In particular, cediranib exhibited high efficacy in allfour patient-derived GBM cells and exhibited no cytotoxicitytoward astrocytes, while TMZ showed high efficacy in only
#1 GBM cell among the four patient-derived GBM cells.Previous studies [21, 22] have shown that cediranib is apotent oral inhibitor of vascular endothelial growth factor(VEGF) receptors and demonstrates improved progression-free survival in an uncontrolled phase II study of patientswith recurrent glioblastoma. The drug is administered orallyand once daily and has a manageable side-effect profile.In addition, it has potent antiedema and steroid-sparingeffects that may improve the quality of life of patients withGBM. Several clinical trials are ongoing testing cediranib

BioMed Research International 5
Astrocyte cytotoxicityviability > 90%
Drugcandidate
No effectcompound
Nonspecifichigh toxicity compound
Nonanticancercompound
GBM efficacyviability <50%
GBM efficacyviability < 50%
Compounds
Promote to next step No-go decision Promote to next step No-go decision
Yes No
Yes No Yes No
Figure 3: High-dose compound heat map for selecting low cytotoxicity and high efficacy compound.
1_D
MSO
2_A
EE78
8 (N
VP-
AEE
788)
3_A
fatin
ib (B
IBW
2992
)4_
BMS-
5996
26 (A
C480
)5_
Erlo
tinib
HCl
6_D
acom
itini
b (P
F299
804,
PF-0
0299
804)
7_G
efitin
ib (I
ress
a)8_
Lapa
tinib
9_N
erat
inib
(HKI
-272
)10
_CI-
1033
(Can
ertin
ib)
11_C
O-1
686
12_B
KM12
0 (N
VP-
BKM
120)
13_B
YL71
914
_XL1
4715
_Eve
rolim
us (R
AD
001)
16_A
ZD20
1417
_PF-
0521
2384
(PKI
-587
)18
_XL7
65 (S
AR2
4540
9)19
_BEZ
235
20_A
ZD53
6321
_Axi
tinib
22_C
edira
nib
(AZD
2171
)23
_Im
atin
ib (G
leev
ec)
24_P
azop
anib
HCl
25_S
uniti
nib
Mal
ate (
Sute
nt)
26_T
andu
tinib
(MLN
518)
27_T
ivoz
anib
(AV-
951)
28_R
egor
afen
ib29
_Van
deta
nib
30_C
aboz
antin
ib (X
L184
)31
_For
etin
ib (X
L880
)32
_Criz
otin
ib (P
F-02
3410
66)
33_I
NCB
2806
034
_LEE
011
35_P
D 0
3329
91 (P
albo
cicli
b H
Cl)
36_L
Y283
5219
37_A
ZD45
4738
_BG
J398
(NV
P-BG
J398
)39
_Dov
itini
b (T
KI-2
58)
40_B
osut
inib
41_D
asat
inib
(BM
S-35
4825
)42
_Nilo
tinib
(AM
N-1
07)
43_A
ZD62
44 (S
elum
etin
ib)
44_T
ram
etin
ib45
_Bor
tezo
mib
(Vel
cade
)46
_Car
filzo
mib
47_A
BT-1
99 (G
DC-
0199
)48
_ABT
-888
(Vel
ipar
ib)
49_A
UY9
22 (N
VP-
AUY9
22)
50_D
abra
feni
b51
_Ibr
utin
ib52
_LD
E225
(NV
P-LD
E225
, Eris
mod
egib
)53
_LD
K378
54_L
GK-
974
55_O
lapar
ib (A
ZD22
81)
56_P
anob
inos
tat (
LBH
589)
57_P
F-04
4499
1358
_Rux
oliti
nib
59_S
otra
stau
rin (A
EB07
1)60
_Vem
uraf
enib
61_V
ismod
egib
(GD
C-04
49)
62_P
HA-
6657
5263
_TM
Z64
_Am
oral
65_M
evas
66_A
mio
67_F
lu68
_Myc
o_ac
id69
_Ral
oxi
70_A
stem
i71
_Fer
re
63_T
MZ
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
Rela
tive c
ell v
iabi
lity
Astrocyte_3 daysAstrocyte_7 days
Figure 4: Relative cell viability of astrocytes after exposure to 70 compounds after the 3- and 7-day compound treatment. Cell viabilities arecalculated from 3D cell size.
in patients with gliomas. Through this 3D cell-based high-dose heat map model, we could also identify cediranib as avalid compound for proof-of-concept of heat map model. So,this 3D cell-based high-dose heat map could narrow downdrug candidates for GMBs. As further study, we need to drawdose response curve to measure IC
50in GBMs about agents
showing low toxicity and high efficacy.
4. Conclusion
We used a 3D cell-based, high-throughput screening tech-nique using a micropillar and microwell chip platform todetermine the effects of high dosage compounds on thecytotoxicity and efficacy on astrocytes and GBM cells, whichwere graphically represented in a high-dose heat map model.

6 BioMed Research International
1_D
MSO
5_Er
lotin
ib H
Cl
8_La
patin
ib
11_C
O-1
686
2_A
EE78
8 (N
VP-
AEE
788)
3_A
fatin
ib (B
IBW
2992
)
6_D
acom
itini
b (P
F299
804,
PF-
0029
9804
)7_
Gefi
tinib
(Ire
ssa)
9_N
erat
inib
(HKI
-272
)10
_CI-
1033
(Can
ertin
ib)
12_B
KM12
0 (N
VP-
BKM
120)
13_B
YL71
914
_XL1
47
16_A
ZD20
1415
_Eve
rolim
us (R
AD
001)
17_P
F-05
2123
84 (P
KI-5
87)
18_X
L765
(SA
R245
409)
19_B
EZ23
520
_AZD
5363
21_A
xitin
ib22
_Ced
irani
b (A
ZD21
71)
24_P
azop
anib
HCl
25_S
uniti
nib
Mal
ate (
Sute
nt)
26_T
andu
tinib
(MLN
518)
27_T
ivoz
anib
(AV-
951)
28_R
egor
afen
ib29
_Van
deta
nib
30_C
aboz
antin
ib (X
L184
)31
_For
etin
ib (X
L880
)
33_I
NCB
2806
034
_LEE
011
35_P
D 0
3329
91 (P
albo
cicli
b H
Cl)
36_L
Y283
5219
37_A
ZD45
4738
_BG
J398
(NV
P-BG
J398
)39
_Dov
itini
b (T
KI-2
58)
40_B
osut
inib
41_D
asat
inib
(BM
S-35
4825
)42
_Nilo
tinib
(AM
N-1
07)
43_A
ZD62
44 (S
elum
etin
ib)
44_T
ram
etin
ib45
_Bor
tezo
mib
(Vel
cade
)46
_Car
filzo
mib
47_A
BT-1
99 (G
DC-
0199
)48
_ABT
-888
(Vel
ipar
ib)
49_A
UY9
22 (N
VP-
AUY9
22)
50_D
abra
feni
b51
_Ibr
utin
ib52
_LD
E225
(NV
P-LD
E225
, Eris
mod
egib
)53
_LD
K378
54_L
GK-
974
55_O
lapar
ib (A
ZD22
81)
57_P
F-04
4499
1358
_Rux
oliti
nib
59_S
otra
stau
rin (A
EB07
1)60
_Vem
uraf
enib
62_P
HA-
6657
5263
_TM
Z64
_Am
oral
65_M
evas
66_A
mio
67_F
lu68
_Myc
o_ac
id69
_Ral
oxi
70_A
stem
i71
_Fer
re
0.00.10.20.30.40.50.60.70.80.91.01.11.2
1.0 0.0 0.0 0.0 0.31.0 0.0 0.0 0.1 0.71.0 0.1 0.0 0.5 0.51.1 0.0 0.0 0.3 0.61.0 0.0 0.0 0.2 0.6
Astrocyte#1#2#3#4
22_C
edira
nib
(AZD
2171
)
63_T
MZ
High-dose heat mapRe
lativ
e cel
l via
bilit
y
0.0 0.0 0.0 0.3 0.1 0.1 0.1 0.0 0.0 0.1 0.2 0.0 0.2 0.3 0.0 0.5 0.9 0.0 0.3 0.0 0.0 0.3 0.0 0.0 0.4 0.0 0.0 1.1 0.6 0.0 0.0 0.0 0.2 0.3 0.0 0.0 0.6 0.1 0.1 0.0 0.0 0.0 0.9 0.0 1.0 0.0 0.7 0.0 0.7 0.4 0.0 0.7 0.1 0.5 0.3 1.2 0.0 0.9 1.1 0.5 0.7 0.1 0.6 0.0 0.0 0.30.0 0.0 0.0 0.8 0.7 0.1 0.2 0.5 0.5 0.2 0.5 0.2 0.5 0.6 0.3 0.5 0.0 0.2 0.6 0.0 0.1 0.4 0.3 0.0 0.3 0.0 0.0 0.8 0.7 0.0 0.0 0.1 0.7 0.5 0.0 0.0 0.8 0.4 0.5 0.1 0.2 0.6 0.8 0.3 0.8 0.3 0.7 0.0 0.7 0.7 0.0 0.9 0.4 0.3 0.8 0.8 0.0 0.2 0.7 0.8 0.4 0.7 0.7 0.2 0.1 0.60.1 0.1 0.1 0.5 0.4 0.1 0.3 0.3 0.3 0.1 0.3 0.3 0.3 0.4 0.5 0.8 0.0 0.2 0.7 0.0 0.2 0.3 0.2 0.1 0.4 0.0 0.0 1.0 0.8 0.1 0.0 0.0 0.5 0.0 0.0 0.1 0.7 0.3 0.2 0.3 0.3 0.3 0.9 0.3 0.6 0.2 0.7 0.0 0.8 0.7 0.2 0.6 0.4 0.2 0.7 0.8 0.6 0.9 0.8 0.6 0.1 0.8 0.1 0.2 0.5 0.30.0 0.2 0.1 0.1 0.2 0.1 0.4 0.5 0.4 0.1 0.5 0.4 0.4 0.6 0.8 0.8 0.1 0.5 0.7 0.0 0.2 0.6 0.3 0.1 0.4 0.0 0.0 0.9 0.5 0.0 0.0 0.1 0.6 0.2 0.0 0.1 0.6 0.3 0.4 0.2 0.2 0.1 0.9 0.5 0.5 0.0 1.0 0.0 0.8 0.6 0.1 0.7 0.3 0.5 0.4 0.9 0.0 0.8 0.8 0.8 0.5 1.0 0.6 0.7 0.4 0.40.0 0.0 0.4 0.5 0.5 0.1 0.3 0.4 0.3 0.3 0.3 0.3 0.4 0.5 0.5 0.6 0.0 0.2 0.6 0.0 0.2 0.7 0.2 0.0 0.6 0.0 0.0 0.9 0.3 0.0 0.0 0.0 0.4 0.0 0.1 0.3 0.6 0.3 0.4 0.2 0.3 0.4 1.0 0.5 0.7 0.3 0.8 0.0 0.7 0.5 0.1 0.7 0.4 0.3 0.3 1.0 0.1 0.8 0.8 0.6 0.7 0.7 0.5 0.6 0.1 0.7
Astrocyte#1#2
#3#4
61_V
ismod
egib
(GD
C-04
49)
56_P
anob
inos
tat (
LBH
589)
32_C
rizot
inib
(PF-
0234
1066
)
23_I
mat
inib
(Gle
evec
)
4_BM
S-59
9626
(AC4
80)
Figure 5: High-dose compound heat map. Astrocytes and four patient-derived glioblastoma multiforme (GBM) cells were treated with 70compounds for 3 days. In the high-dose heat map (table over graph), red solid filling denotes astrocytes with viability >90% and blue solidfilling denotes GBM cells with viability <50%.
Although some compounds exhibited good efficacy towardGBM, cytotoxicity toward normal glial cells in the centralnervous system was an impending issue. Thus, we useda high-dose heat map model and considered both cyto-toxicity and efficacy by comparing the response of high-dose compound on 3D-cultured GBM cells and astrocytesto screen the most efficacious drugs for GBM. Seventycompounds with dosage of 20 uM, including specific-targetgeneral-chemotherapeutic agents, were used against fourpatient-derived GBM cells and astrocytes to compare thecytotoxicity and efficacy of the compounds. For simulatingan in vivo microenvironment, GBM cells and astrocytes wereencapsulated with alginate and 3D-cultured in a micropillarand microwell chip platform. Among the 70 compoundstested, cediranib exhibited the lowest cytotoxicity towardastrocyte and showed high efficacy toward GBM. Thus, inearly stage of the drug development, the micropillar andmicrowell chip platform could culture patient-derived GBMswith 3D manner and be used for screening toxicity andefficacy of many lead compounds targeted GBMs beforeanimal tests or clinical trials.
Conflicts of Interest
The authors declared no potential conflicts of interest withrespect to the research, authorship, and/or publication of thisarticle.
Acknowledgments
This research was supported by the Bio & Medical Technol-ogy Development Program of the NRF funded by the KoreanGovernment, MSIP (NRF-2015M3A9A7029740).
References
[1] C. L. Smith, O. Kilic, P. Schiapparelli et al., “Migration phe-notype of brain-cancer cells predicts patient outcomes,” CellReports, vol. 15, no. 12, pp. 2616–2624, 2016.
[2] U. Linz, “Commentary on effects of radiotherapywith concomi-tant and adjuvant temozolomide versus radiotherapy alone onsurvival in glioblastoma in a randomised phase III study: 5-Yearanalysis of the EORTC-NCIC trial (Lancet Oncol. 2009;10:459-466),” Cancer, vol. 116, no. 8, pp. 1844–1846, 2010.
[3] R. Stupp, W. P. Mason, and M. J. van den Bent, “Radiotherapyplus concomitant and adjuvant temozolomide for glioblas-toma,” Oncology Times, vol. 27, no. 9, pp. 15-16, 2005.
[4] G. Yount, L. Soroceanu, H.-J. Wang et al., “Selective toxicityof a highly potent camptothecin analogue: a pilot study withglioblastomamultiforme cells,”Anticancer Research, vol. 36, no.11, pp. 5845–5848, 2016.
[5] S. Dolma,H. J. Selvadurai, X. Lan et al., “Inhibition of dopaminereceptor D4 impedes autophagic flux, proliferation, and sur-vival of glioblastoma stem cells,” Cancer Cell, vol. 29, no. 6, pp.859–873, 2016.

BioMed Research International 7
[6] I. Markiewicz and B. Lukomska, “The role of astrocytes in thephysiology and pathology of the central nervous system,” ActaNeurobiol Exp (Wars), vol. 66, no. 4, pp. 343–358, 2006.
[7] E. O’Brien, C. Howarth, and N. R. Sibson, “The role of astro-cytes in CNS tumours: pre-clinical models and novel imagingapproaches,” Frontiers in Cellular Neuroscience, vol. 7, no. 40, pp.1–13, 2013.
[8] C. Soussain, D. Ricard, J. R. Fike, J.-J. Mazeron, D. Psimaras,and J.-Y. Delattre, “CNS complications of radiotherapy andchemotherapy,” The Lancet, vol. 374, no. 9701, pp. 1639–1651,2009.
[9] R. H. Shoemaker, “The NCI60 human tumour cell line anti-cancer drug screen,” Nature Reviews Cancer, vol. 6, no. 10, pp.813–823, 2006.
[10] J.-P. Mpindi, P. Swapnil, B. Dmitrii et al., “Impact of normaliza-tion methods on high-throughput screening data with high hitrates and drug testing with dose-response data,” Bioinformatics,vol. 31, no. 23, pp. 3815–3821, 2015.
[11] M.-Y. Lee, R. A. Kumar, S. M. Sukumaran, M. G. Hogg,D. S. Clark, and J. S. Dordick, “Three-dimensional cellularmicroarray for high-throughput toxicology assays,” Proceedingsof the National Academy of Sciences of the United States ofAmerica, vol. 105, no. 1, pp. 59–63, 2008.
[12] Y.-C. Tung, A. Y. Hsiao, S. G. Allen, Y.-S. Torisawa, M. Ho, andS. Takayama, “High-throughput 3D spheroid culture and drugtesting using a 384 hanging drop array,” Analyst, vol. 136, no. 3,pp. 473–478, 2011.
[13] D. W. Lee, S. H. Yi, S. H. Jeong, B. Ku, J. Kim, and M.-Y. Lee,“Plastic pillar inserts for three-dimensional (3D) cell culturesin 96-well plates,” Sensors and Actuators, B: Chemical, vol. 177,no. 1, pp. 78–85, 2013.
[14] D.W. Lee, Y.-S. Choi, Y. J. Seo et al., “High-throughput screening(HTS) of anticancer drug efficacy on a micropillar/microwellchip platform,” Analytical Chemistry, vol. 86, no. 1, pp. 535–542,2014.
[15] D. W. Lee, Y.-S. Choi, Y. J. Seo et al., “High-throughput,miniaturized clonogenic analysis of a limiting dilution assay ona micropillar/microwell chip with brain tumor cells,” Small, vol.10, no. 24, pp. 5098–5105, 2014.
[16] D.W. Lee, M.-Y. Lee, B. Ku, and D.-H. Nam, “Automatic 3D cellanalysis in high-throughput microarray using micropillar andmicrowell chips,” Journal of Biomolecular Screening, vol. 20, no.9, pp. 1178–1184, 2015.
[17] D. W. Lee, S. Lee, L. Park et al., “High-throughput clonogenicanalysis of 3D-Cultured patient-derived cells with a micropillarand microwell chip,” Slas Discovery: Advancing Life SciencesR&D, vol. 22, no. 5, pp. 645–651, 2017.
[18] A. M. Pasca, S. A. Sloan, L. E. Clarke et al., “Functional corticalneurons and astrocytes from human pluripotent stem cells in3D culture,” Nature Methods, vol. 12, no. 7, pp. 671–678, 2015.
[19] N. Gomez-Roman, K. Stevenson, L. Gilmour, G. Hamilton, andA. J. Chalmers, “A novel 3D human glioblastoma cell culturesystem for modeling drug and radiation responses,” Neuro-Oncology, vol. 19, no. 2, pp. 229–241, 2017.
[20] E. East, N. Johns, M. Georgiou et al., “A 3D in vitro modelreveals differences in the astrocyte response elicited by potentialstem cell therapies for CNS injury,” Regenerative Medicine, vol.8, no. 6, pp. 739–746, 2013.
[21] J. Dietrich, D. Wang, and T. T. Batchelor, “Cediranib: profileof a novel anti-angiogenic agent in patients with glioblastoma,”ExpertOpinion on InvestigationalDrugs, vol. 18, no. 10, pp. 1549–1557, 2009.
[22] T. T. Batchelor, E. R. Gerstner, K. E. Emblem et al., “Improvedtumor oxygenation and survival in glioblastoma patients whoshow increased blood perfusion after cediranib and chemora-diation,” Proceedings of the National Academy of Sciences, vol.110, no. 47, pp. 19059–19064, 2013.

Submit your manuscripts athttps://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com