Embed Size (px)
Citation preview
High Yield Topics of the ABSITE:
Critical Care and Medical Knowledge
David J. Worhunsky, MD
Pediatric Surgery Fellow
Yale University

Critical Care Knowledge for ABSITE – Outline
Cardiovascular
• Hemodynamic monitoring and parameters
• Shock
• Cardiovascular receptors and pharmacology
• Oxygen-Hemoglobin dissociation curve
• Systemic oxygenation
Pulmonary
• Pulmonary function
• Ventilator management
• ARDS
• Indications for adult ECMO
Critical Care Knowledge for ABSITE – Outline
Renal
• Acute kidney injury (AKI) and RIFLE criteria
• Evaluation for Prerenal versus Intrinsic
• Indications for hemodialysis
Infectious
• Sepsis (old and new guidelines)
• Pneumonia
• Necrotizing soft tissue infections
• C. difficile colitis
Critical Care Knowledge for ABSITE – Outline
Nutrition
• Respiratory quotient
• Refeeding syndrome
• Hypermetabolism after major stress (illness/surgery/trauma)
• High yield facts
Other
• Abdominal compartment syndrome
• Venous thromboembolism

Hemodynamic Monitoring
• Important equations:
MAP = CO x SVR (This is Ohm’s law V = IR measure of current through a conductor)
• Technically: MAP - CVP = CO x SVR
• MAP = [(2 x DP) + SP] / 3
• CO = HR x SV (where SV is determined by contractility, preload, afterload)
Cardiac Index (CI) = CO / BSA
Systemic Vascular Residence Index (SVRI) = SVR x BSA
• Normal values:
CO = 4 – 8 L/min
CI = 2.5 – 4 L/min/m2
SVR = 800 – 1400 dynes・s/cm5
SVRI = 1500 – 2400 dyn・s/cm5/m2
Types of Shock
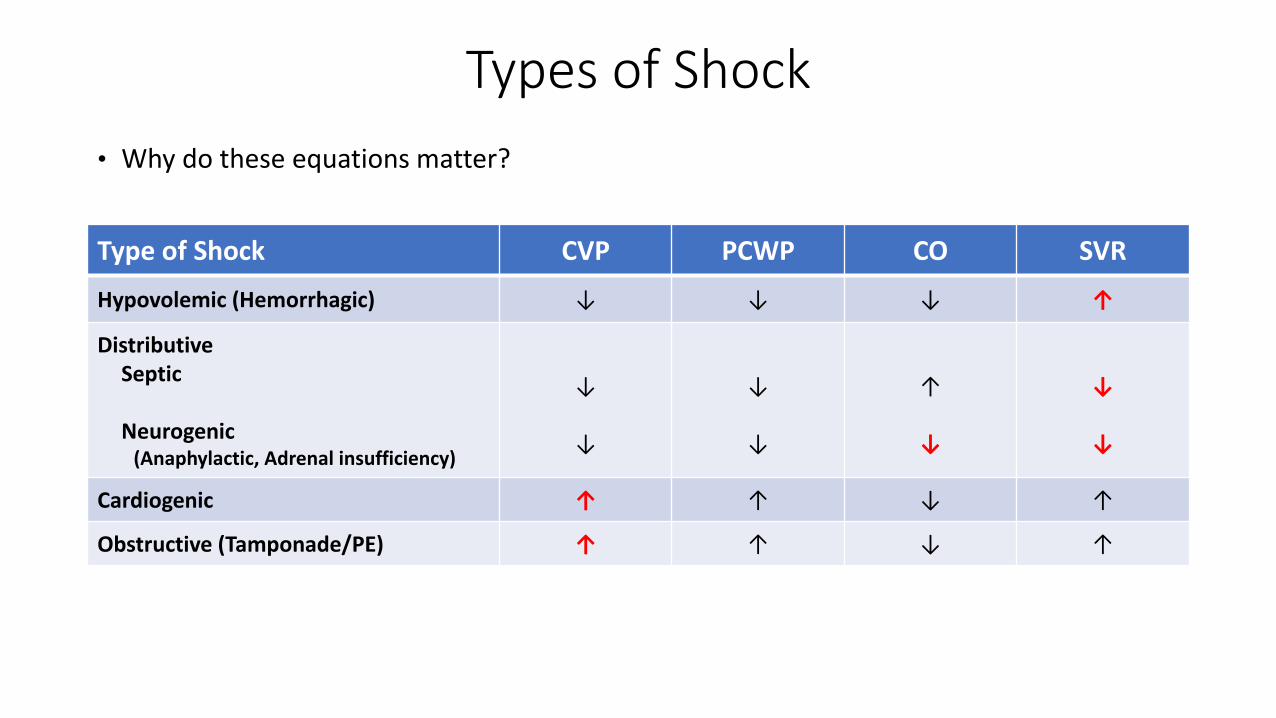
• Why do these equations matter?
Type of Shock CVP PCWP CO SVR
Hypovolemic (Hemorrhagic) ↓ ↓ ↓ ↑
DistributiveSeptic
Neurogenic(Anaphylactic, Adrenal insufficiency)
↓
↓
↓
↓
↑
↓
↓
↓
Cardiogenic ↑ ↑ ↓ ↑
Obstructive (Tamponade/PE) ↑ ↑ ↓ ↑
Cardiovascular Receptors and Medications
• Adrenergic receptors (G protein-coupled receptors)
• Alpha (𝛂) Receptors
• 𝛂-1 vasoconstriction
• 𝛂-2 smooth muscle mixed effects, CNS/PNS effects (clonidine, dexmedetomidine)
• Beta (𝛃) Receptors
• 𝛃-1 Inotropic, chronotropic effects
• 𝛃-2 smooth muscle relaxation
• Dopamine receptor (G protein-coupled receptors)
• Relaxation of renal and splanchnic smooth muscle
• Vasopressin receptors (G protein-coupled receptors)
• V1 vasoconstriction
• V2 water reabsorption via aquaporin water channels, fVIII/vWF release
Cardiovascular Receptors and Medications
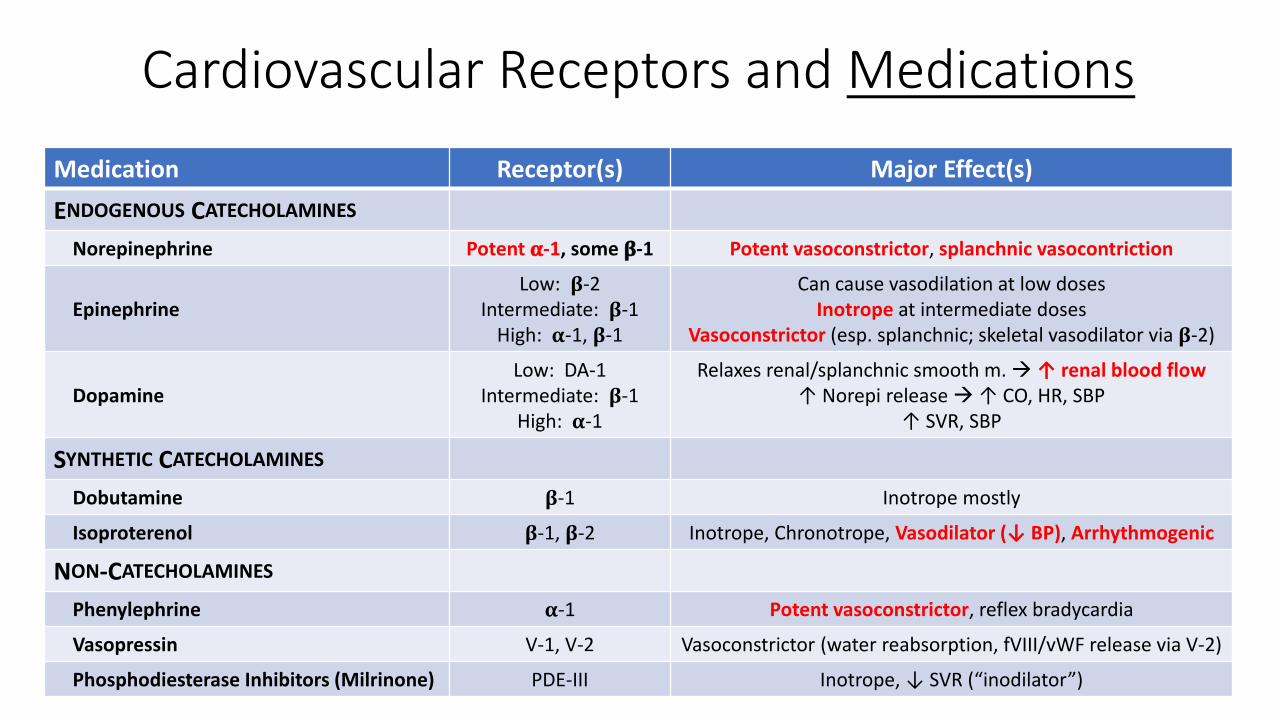
Medication Receptor(s) Major Effect(s)
ENDOGENOUS CATECHOLAMINES
Norepinephrine Potent 𝛂-1, some 𝛃-1 Potent vasoconstrictor, splanchnic vasocontriction
EpinephrineLow: 𝛃-2
Intermediate: 𝛃-1High: 𝛂-1, 𝛃-1
Can cause vasodilation at low dosesInotrope at intermediate doses
Vasoconstrictor (esp. splanchnic; skeletal vasodilator via 𝛃-2)
DopamineLow: DA-1
Intermediate: 𝛃-1High: 𝛂-1
Relaxes renal/splanchnic smooth m. ↑ renal blood flow↑ Norepi release ↑ CO, HR, SBP
↑ SVR, SBP
SYNTHETIC CATECHOLAMINES
Dobutamine 𝛃-1 Inotrope mostly
Isoproterenol 𝛃-1, 𝛃-2 Inotrope, Chronotrope, Vasodilator (↓ BP), Arrhythmogenic
NON-CATECHOLAMINES
Phenylephrine 𝛂-1 Potent vasoconstrictor, reflex bradycardia
Vasopressin V-1, V-2 Vasoconstrictor (water reabsorption, fVIII/vWF release via V-2)
Phosphodiesterase Inhibitors (Milrinone) PDE-III Inotrope, ↓ SVR (“inodilator”)
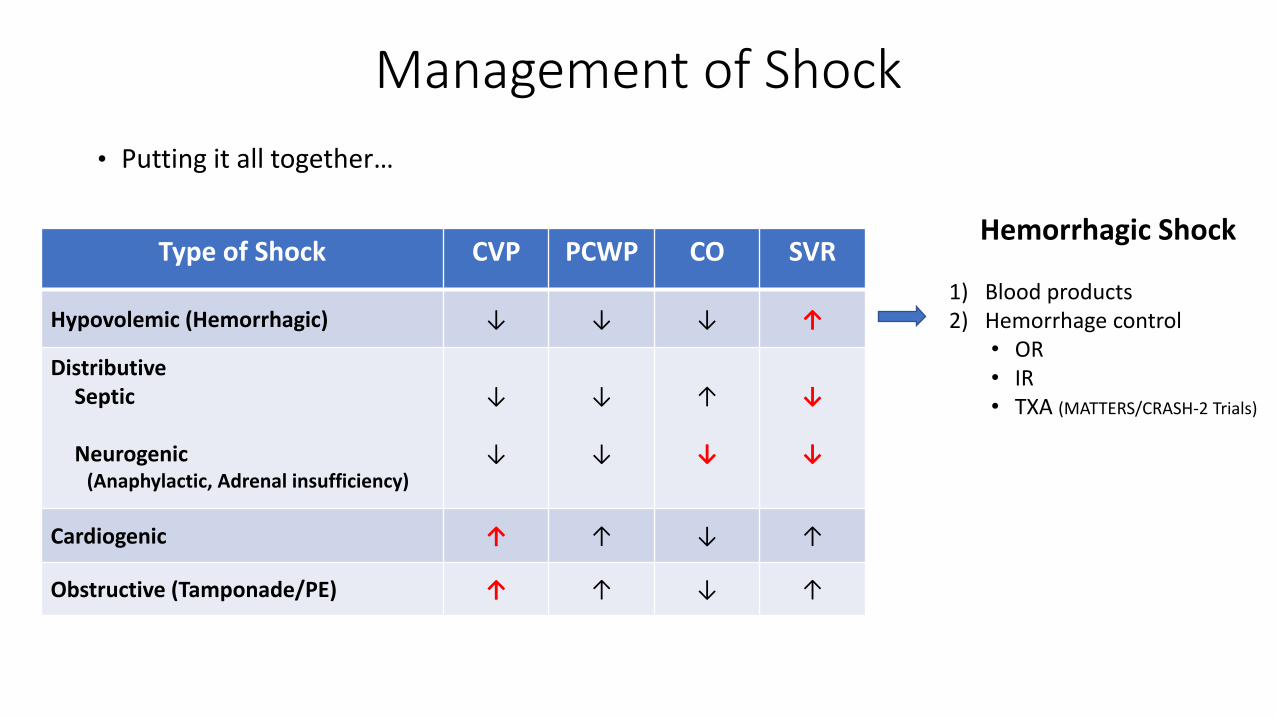
Management of Shock
• Putting it all together…
Hemorrhagic Shock
1) Blood products2) Hemorrhage control
• OR• IR• TXA (MATTERS/CRASH-2 Trials)
Type of Shock CVP PCWP CO SVR
Hypovolemic (Hemorrhagic) ↓ ↓ ↓ ↑
DistributiveSeptic
Neurogenic(Anaphylactic, Adrenal insufficiency)
↓
↓
↓
↓
↑
↓
↓
↓
Cardiogenic ↑ ↑ ↓ ↑
Obstructive (Tamponade/PE) ↑ ↑ ↓ ↑
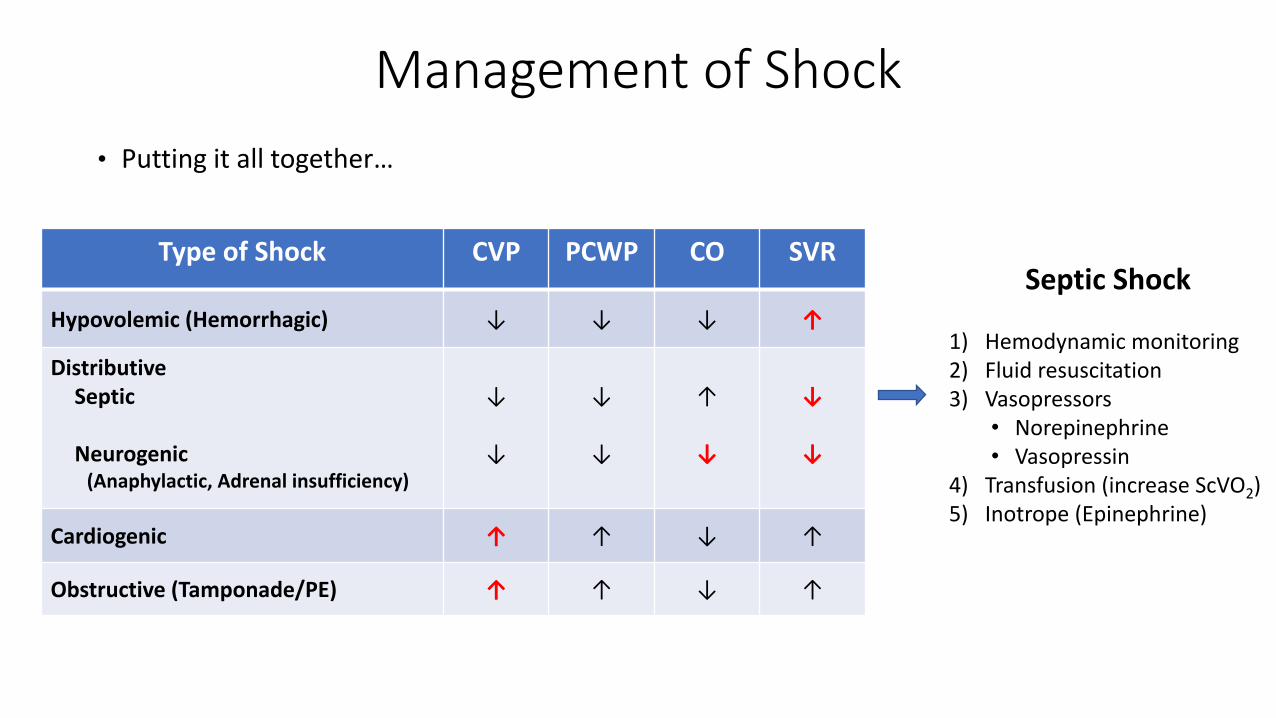
Management of Shock
• Putting it all together…
Septic Shock
1) Hemodynamic monitoring2) Fluid resuscitation3) Vasopressors
• Norepinephrine• Vasopressin
4) Transfusion (increase ScVO2)5) Inotrope (Epinephrine)
Type of Shock CVP PCWP CO SVR
Hypovolemic (Hemorrhagic) ↓ ↓ ↓ ↑
DistributiveSeptic
Neurogenic(Anaphylactic, Adrenal insufficiency)
↓
↓
↓
↓
↑
↓
↓
↓
Cardiogenic ↑ ↑ ↓ ↑
Obstructive (Tamponade/PE) ↑ ↑ ↓ ↑

Management of Shock
• Putting it all together…
Neurogenic Shock
1) Fluid resuscitation2) Vasopressors
• Norepinephrine• Vasopressor• ~ Phenylephrine
Type of Shock CVP PCWP CO SVR
Hypovolemic (Hemorrhagic) ↓ ↓ ↓ ↑
DistributiveSeptic
Neurogenic(Anaphylactic, Adrenal insufficiency)
↓
↓
↓
↓
↑
↓
↓
↓
Cardiogenic ↑ ↑ ↓ ↑
Obstructive (Tamponade/PE) ↑ ↑ ↓ ↑

Management of Shock
• Putting it all together…
Cardiogenic Shock
1) Cardiology consult2) Volume assessment3) Vasopressors
• Dopamine• Norepinephrine
4) Inotropic Support• Dobutamine• Milrinone
5) Intra-aortic Balloon Pump…
Type of Shock CVP PCWP CO SVR
Hypovolemic (Hemorrhagic) ↓ ↓ ↓ ↑
DistributiveSeptic
Neurogenic(Anaphylactic, Adrenal insufficiency)
↓
↓
↓
↓
↑
↓
↓
↓
Cardiogenic ↑ ↑ ↓ ↑
Obstructive (Tamponade/PE) ↑ ↑ ↓ ↑

Intra-aortic Balloon Pump
• Indicated for stabilization of patient in cardiogenic shock (not definitive therapy)
• ↓ systolic LV afterload ↑ coronary perfusion pressure ↑ CO (by 40% or more)
• Catheter tip positioned 2-3 cm distal to left subclavian artery
• Inflates during diastole (mid T wave)
• Deflates during systole (peak of R wave)

Systemic Oxygenation
• Oxygen Saturation (SO2)
• SO2 = Oxygenated Hb / Total Hb
• Determined by the tendency of Hb to bind O2
Oxyhemoglobin Dissociation Curve
• Right Shift
• ↑ oxygen release
• ↑ temp; CO2; 2,3-DPG; H+ (↓ pH)
• Left Shift
• ↑ oxygen uptake
• ↓ temp; CO2; 2,3-DPG; H+ (↑ pH)
Marino’s The ICU Book, 4th Ed 2014
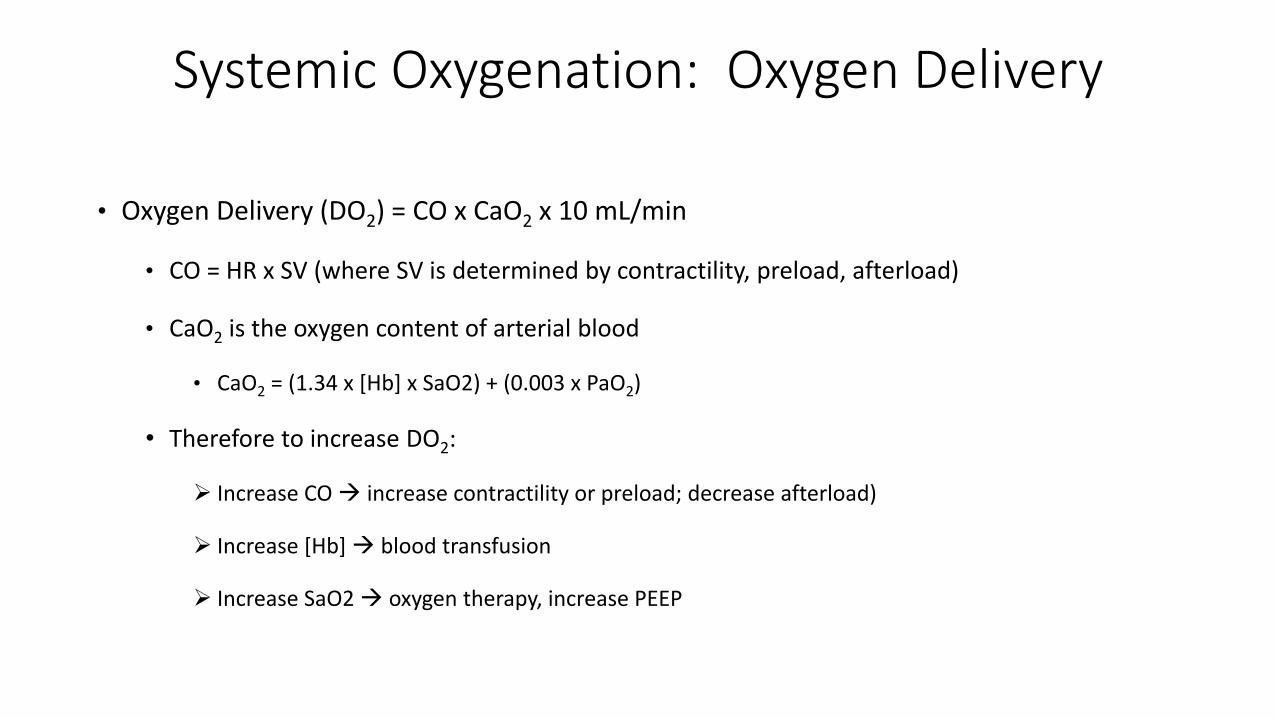
Systemic Oxygenation: Oxygen Delivery
• Oxygen Delivery (DO2) = CO x CaO2 x 10 mL/min
• CO = HR x SV (where SV is determined by contractility, preload, afterload)
• CaO2 is the oxygen content of arterial blood
• CaO2 = (1.34 x [Hb] x SaO2) + (0.003 x PaO2)
• Therefore to increase DO2:
Increase CO increase contractility or preload; decrease afterload)
Increase [Hb] blood transfusion
Increase SaO2 oxygen therapy, increase PEEP

Pulmonary Function – Lung Volumes
• TLC = Total Lung Capacity
• RV = Residual Volume
• VC = Vital Capacity
• FRC = Functional Residual Capacity
• FEV1 = Forced Expiratory Volume in 1 sec
• Obstructive Disease (Asthma, Emphysema)
↑ TLC and RV; ↓ FEV1
• Restrictive Disease (Chest wall, Neuromuscular)
↓ TLC, RV, FVCWeinberger Principles of Pulmonary Medicine, 6th Ed 2014

Pulmonary Function – Lung Volumes
• TLC = Total Lung Capacity
• RV = Residual Volume
• VC = Vital Capacity
• FRC = Functional Residual Capacity
• FEV1 = Forced Expiratory Volume in 1 sec
• Aging
↓ VC and FEV1; ↑ FRC
• PEEP
↑ FRC maintains alveolar recruitment
improves oxygenationWeinberger Principles of Pulmonary Medicine, 6th Ed 2014
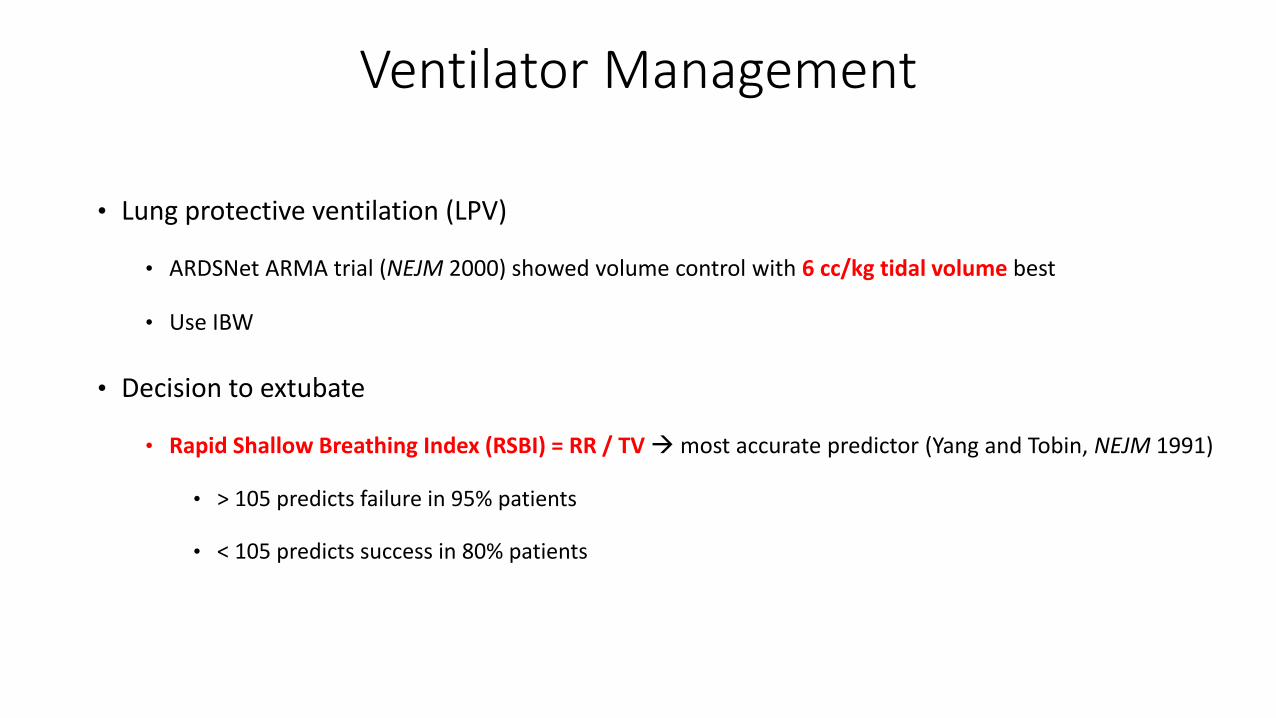
Ventilator Management
• Lung protective ventilation (LPV)
• ARDSNet ARMA trial (NEJM 2000) showed volume control with 6 cc/kg tidal volume best
• Use IBW
• Decision to extubate
• Rapid Shallow Breathing Index (RSBI) = RR / TV most accurate predictor (Yang and Tobin, NEJM 1991)
• > 105 predicts failure in 95% patients
• < 105 predicts success in 80% patients

Acute Respiratory Distress Syndrome (ARDS)
• Heterogenous diagnosis of acute, diffuse, inflammatory lung injury
• Clinical hallmarks include hypoxemia and bilateral radiographic opacities
• Four components in the definition of ARDS (The Berlin Definition, JAMA 2012)
(No more Acute Lung Injury ARDS)
1) Timing – clinical insult to respiratory compromise < 1 week
2) Imaging – CXR with bilateral fluffy infiltrates
3) Edema origin – cannot be explained by cardiac failure/fluid overload (PAWP ≤ 18)
4) Oxygenation – defined by P/F ratio; PEEP ≥ 5
• Mild ARDS: PaO2 / FiO2 ≤ 300
• Moderate ARDS: PaO2 / FiO2 ≤ 200
• Severe ARDS: PaO2 / FiO2 ≤ 100

Extracorporeal Membrane Oxygenation (ECMO)
• Proven outcomes in treatment of neonatal respiratory failure
• Venovenous (VV)-ECMO used with pulmonary compromise
• Venoarterial (VA)-ECMO used with cardiopulmonary compromise
• Use in adults increasing
• CESAR trial (Lancet 2009) potential benefit when ECMO an option in adult respiratory failure
• Indications
• P/F < 80 despite high PEEP
• Uncompensated hypercapnia with pH < 7.15
• Plateau pressures > 35 cm H2O
• Contraindications
• Any condition precluding use of anticoagulation
• High pressure ventilation with high FiO2 for > 7 days (relative)

Acute Kidney Injury (AKI)
• 10-15% risk of postoperative AKI following major abdominal surgery
• Postoperative AKI independently associated with morbidity (including CKD) and mortality
• RIFLE criteria widely accepted definition of AKI
• Risk: ↑ Cr x 1.5 over baseline or UOP < 0.5 cc/kg/h for 6 hours (Stage I AKI)
• Injury: ↑ Cr x 2.0 over baseline or UOP < 0.5 cc/kg/h for 12 hours (Stage 2 AKI)
• Failure: ↑ Cr x 3 over baseline or UOP < 0.3 cc/kg/h for 24 hours or Anuria x 12 hours (Stage 3 AKI)
• Loss: Persistent AFR > 3 weeks
• End-Stage Kidney Disease: Failure > 3 months

Evaluation of Acute Kidney Injury
• Start with renal ultrasound (rule out postrenal obstruction)
• Fractional Excretion of Sodium (FENa) = (Urine Na/Cr) / (Plasma Na/Cr) x 100
• Fractional Excretion of Urea (FEU) = (Urine Urea/Cr) / (Plasma Urea/Cr) x 100
• FENa can be falsely elevated by diuretics or CRI; FEU not influenced by diuretics
• Prerenal cause of AKI (e.g., hypotension)
• FENa < 1%
• FEU < 35%
• BUN/Cr > 20
• Urine Na < 20
• Intrinsic cause of AKI (e.g., ATN, AIN)
• FENa > 2%
• FEU > 50%
• Urine Na > 40

Renal Replacement Therapy (RRT)
• 6% of patients with AKI require RRT
• Options: Intermittent hemodialysis and continuous venovenous hemofiltration (CVVH)
• Intermittent hemodialysis offers rapid clearance of small solutes (few hours)
• CVVH best for patients with hemodynamic instability given lower flow rates required
• Indications for RRT A-E-I-O-U
1) Acidemia
2) Electrolytes (hyperkalemia)
3) Intoxications (toxins such as ethylene glycol)
4) Overload
5) Uremia (with coagulopathy or encephalopathy)
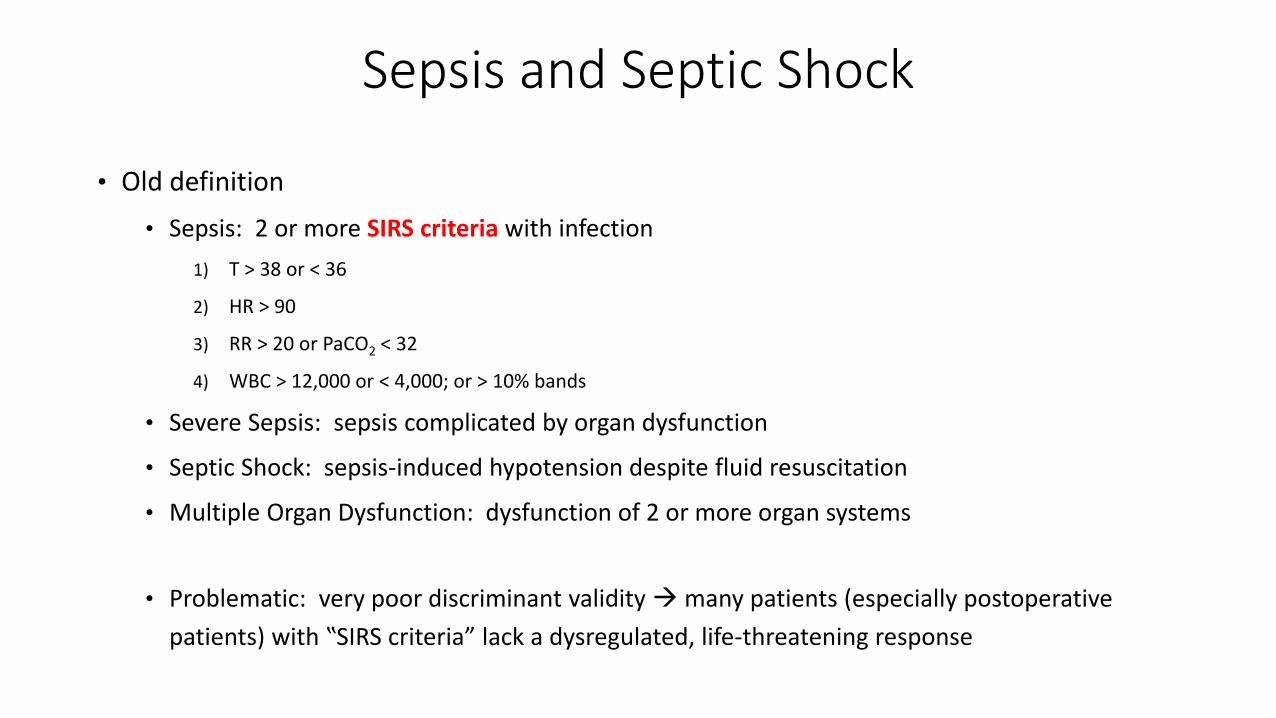
Sepsis and Septic Shock
• Old definition
• Sepsis: 2 or more SIRS criteria with infection
1) T > 38 or < 36
2) HR > 90
3) RR > 20 or PaCO2 < 32
4) WBC > 12,000 or < 4,000; or > 10% bands
• Severe Sepsis: sepsis complicated by organ dysfunction
• Septic Shock: sepsis-induced hypotension despite fluid resuscitation
• Multiple Organ Dysfunction: dysfunction of 2 or more organ systems
• Problematic: very poor discriminant validity many patients (especially postoperative
patients) with ‟SIRS criteria” lack a dysregulated, life-threatening response

Sepsis and Septic Shock
• New definition of Sepsis (Sepsis-3, JAMA 2016):
• Life-threatening organ dysfunction caused by dysregulated host response to infection
• Organ dysfunction identified as an acute change in SOFA score ≥ 2 points
Respiratory: P/F ratio < 400
Coagulation: Platelet count < 150
Liver: Total bilirubin > 1.2
Cardiovascular: MAP < 70
CNS: GCS < 15
Renal: Cr > 1.2
• Quick SOFA (qSOFA) Criteria for rapid screening
1) RR ≥ 22
2) SBP ≤ 100
3) Altered mentation
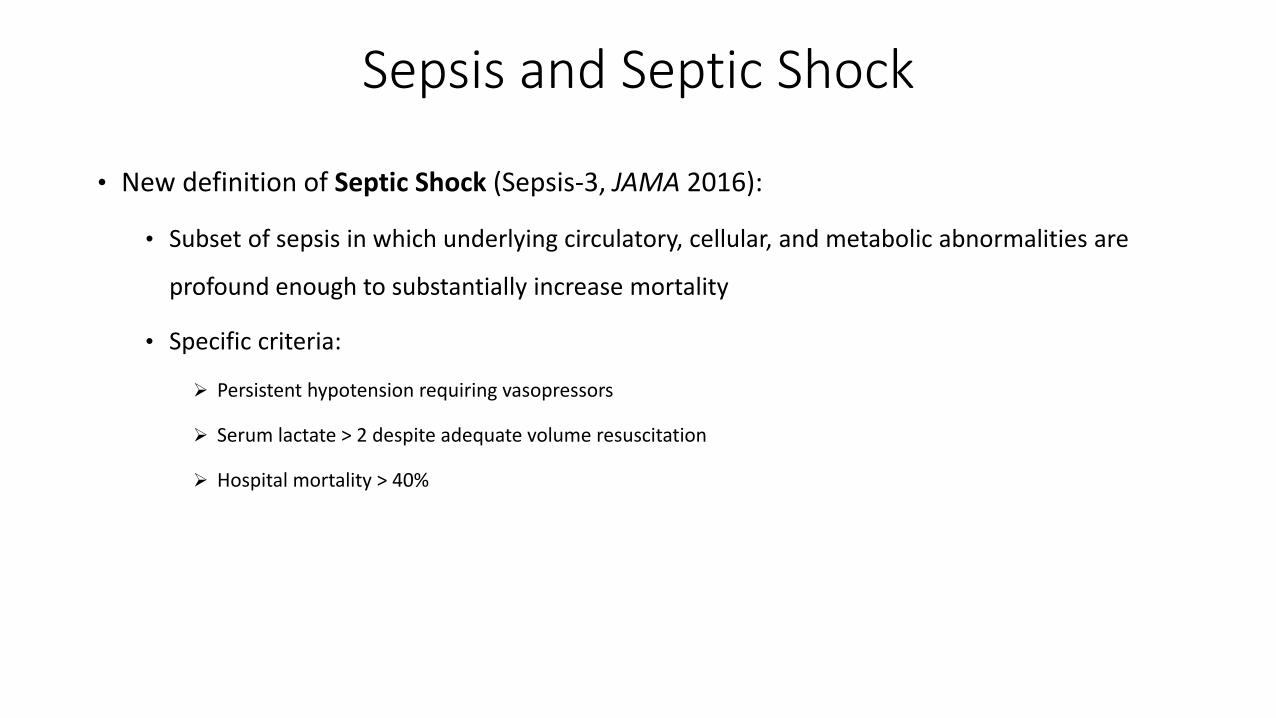
Sepsis and Septic Shock
• New definition of Septic Shock (Sepsis-3, JAMA 2016):
• Subset of sepsis in which underlying circulatory, cellular, and metabolic abnormalities are
profound enough to substantially increase mortality
• Specific criteria:
Persistent hypotension requiring vasopressors
Serum lactate > 2 despite adequate volume resuscitation
Hospital mortality > 40%
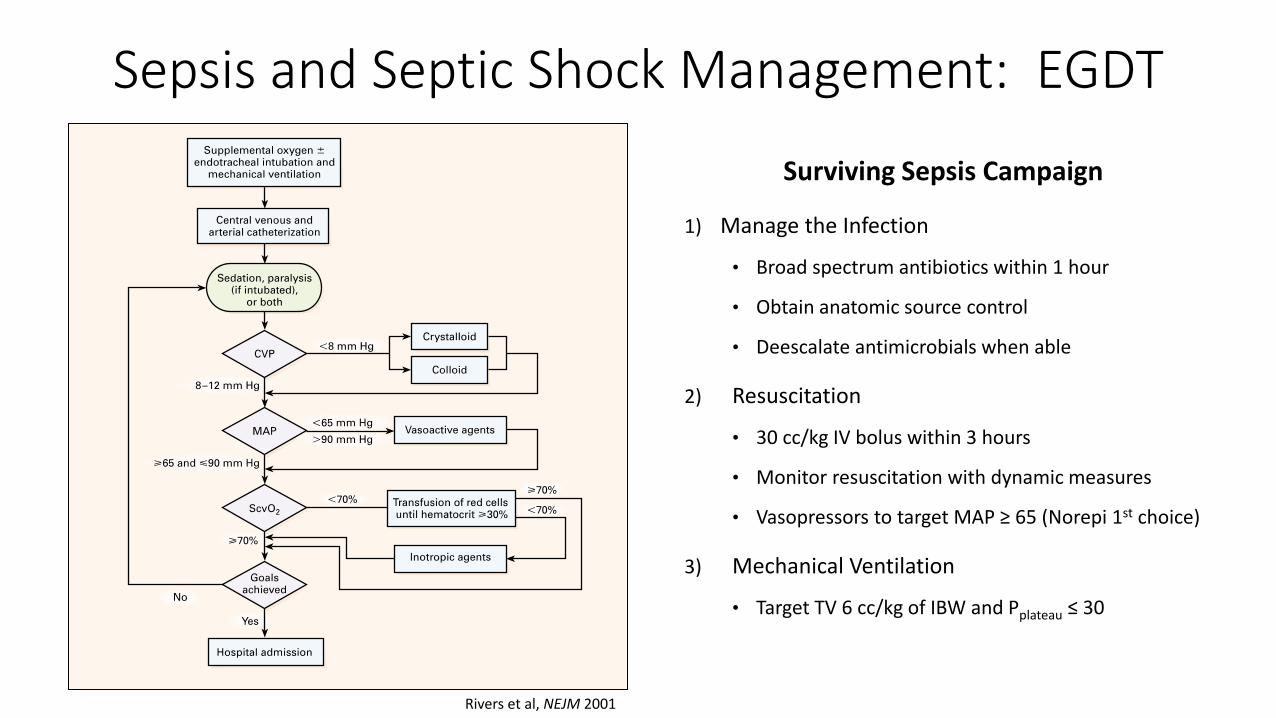
Sepsis and Septic Shock Management: EGDT
Rivers et al, NEJM 2001
Surviving Sepsis Campaign
1) Manage the Infection
• Broad spectrum antibiotics within 1 hour
• Obtain anatomic source control
• Deescalate antimicrobials when able
2) Resuscitation
• 30 cc/kg IV bolus within 3 hours
• Monitor resuscitation with dynamic measures
• Vasopressors to target MAP ≥ 65 (Norepi 1st choice)
3) Mechanical Ventilation
• Target TV 6 cc/kg of IBW and Pplateau ≤ 30
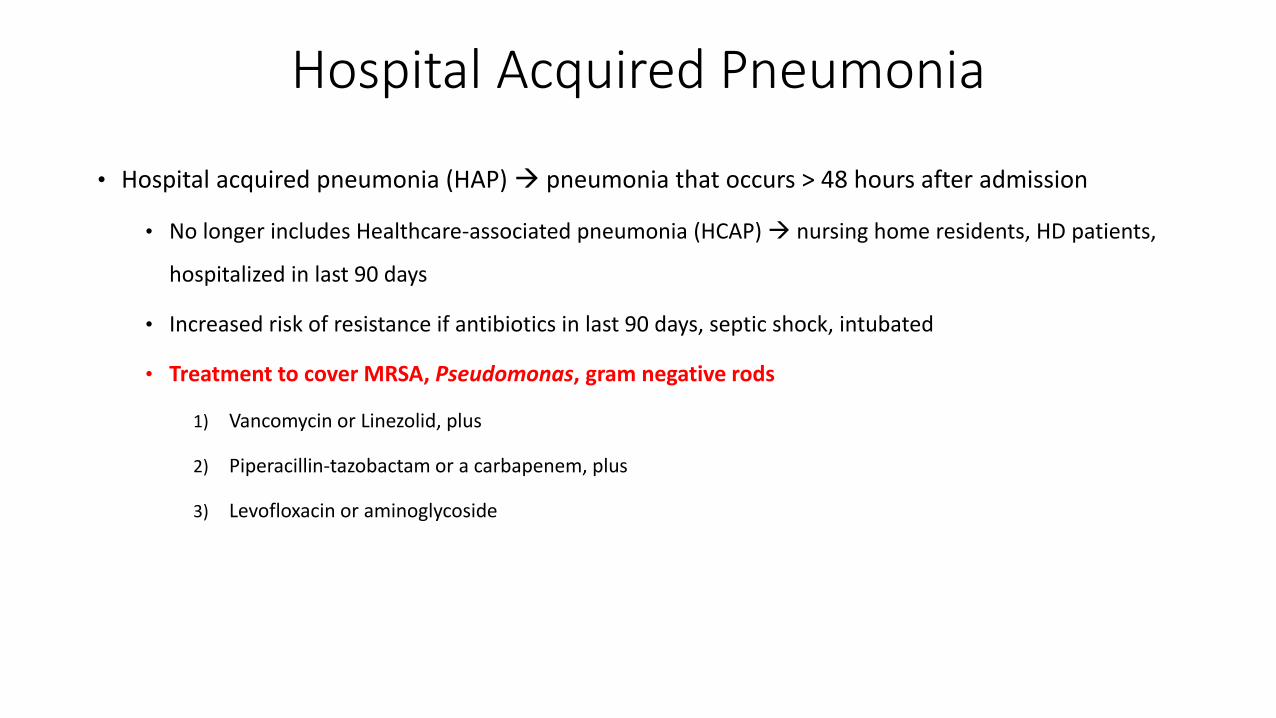
Hospital Acquired Pneumonia
• Hospital acquired pneumonia (HAP) pneumonia that occurs > 48 hours after admission
• No longer includes Healthcare-associated pneumonia (HCAP) nursing home residents, HD patients,
hospitalized in last 90 days
• Increased risk of resistance if antibiotics in last 90 days, septic shock, intubated
• Treatment to cover MRSA, Pseudomonas, gram negative rods
1) Vancomycin or Linezolid, plus
2) Piperacillin-tazobactam or a carbapenem, plus
3) Levofloxacin or aminoglycoside

Ventilator Acquired Pneumonia
• Ventilator acquired pneumonia (VAP) pneumonia develops > 48 hours after intubation
• High risk of MDR pathogens
• IV antibiotics within 90 days, septic shock, ≥ 5 day hospitalization, RRT prior to VAP
• Treatment to cover MRSA, Pseudomonas, gram negative rods (same as HAP)
• Prevention with VAP Bundles
1) Ventilator-weaning protocols (regular spontaneous breathing trials)
2) Interrupt sedation daily (sedation holidays)
3) Selective oral decontamination (Chlorhexidine mouth wash)
4) Use endotracheal tubes of subglottic aspiration port
5) Maintain head of bed above 30-40°

Necrotizing Soft Tissue Infections (NSTI)
• Exceedingly rare with incidence of about 1000 cases per year in the US
• Three types
Type I Clostridial infections (most strongly associated with historical disease; GS with GPR, toxin production)
Often polymicrobial (GPC, GNR, anaerobes)
Patients typically older with more comorbidities
Type II group A β-hemolytic streptococci (GAS) alone or in combination with staphylococcal species
GAS produces superantigen M
Patients typically younger and healthier with history of trauma, surgery, or IV drug use
Type III gram negative marine organisms
Hakkarainen et al, Curr Probl Surg 2014
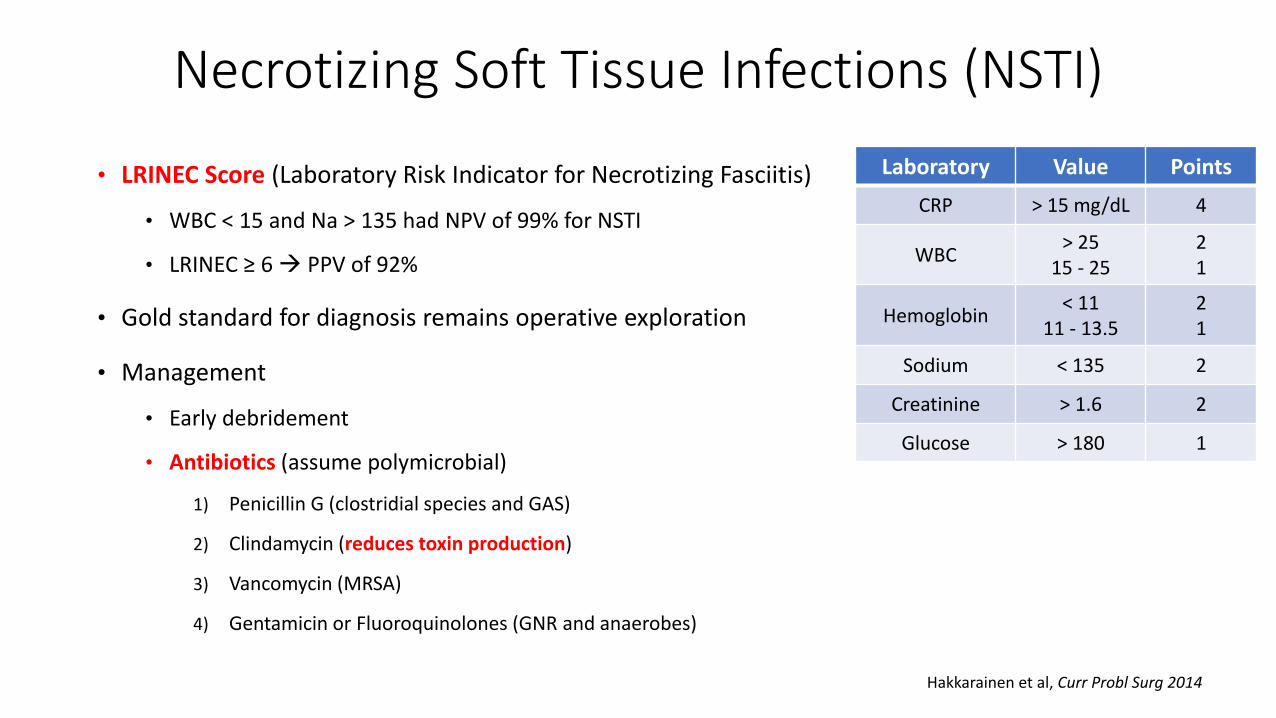
Necrotizing Soft Tissue Infections (NSTI)
• LRINEC Score (Laboratory Risk Indicator for Necrotizing Fasciitis)
• WBC < 15 and Na > 135 had NPV of 99% for NSTI
• LRINEC ≥ 6 PPV of 92%
• Gold standard for diagnosis remains operative exploration
• Management
• Early debridement
• Antibiotics (assume polymicrobial)
1) Penicillin G (clostridial species and GAS)
2) Clindamycin (reduces toxin production)
3) Vancomycin (MRSA)
4) Gentamicin or Fluoroquinolones (GNR and anaerobes)
Laboratory Value Points
CRP > 15 mg/dL 4
WBC> 25
15 - 2521
Hemoglobin< 11
11 - 13.521
Sodium < 135 2
Creatinine > 1.6 2
Glucose > 180 1
Hakkarainen et al, Curr Probl Surg 2014

Clostridium difficile Colitis
• Most common cause of healthcare-associated diarrhea
• Most common nosocomial pathogen in North America and Europe (overtook MRSA)
• Clinical presentation: ≥ 3 loose stools in 24 hours, abdominal pain/cramping, fever, leukocytosis
• Diagnosis: multiple laboratory stool tests available; protocol hospital-dependent
1) PCR for genes specific to toxigenic strains (tcdB – toxin B gene)
• May detect asymptomatic carriers
2) Enzyme immunoassay (EIA) for GDH antigen (↑ sensitivity) and/or toxins A and B (↑ specificity)
3) Lower endoscopy (sigmoidoscopy) diagnostic if pseudomembranes seen

Clostridium difficile Colitis
• Management of initial infection based on disease severity
• Severe disease (1 or more of the following):
1) WBC > 15
2) Cr > 1.5 times baseline level
3) Age > 60
4) Albumin < 2.5

Clostridium difficile Colitis
• Treatment
• Mild/moderate infection
• PO vancomycin for 10 days (or PO metronidazole, but increased treatment failure)
• Severe infection
1) PO vancomycin (can increase from 125 mg QID to 500 mg TID), plus
2) IV metronidazole if ileus
3) Consider addition of vancomycin enema with ileus
4) Consider PO fidaxomicin in lieu of vancomycin if not improving
• Surgery indicated in fulminant disease with toxic megacolon, perforation, progressive organ
failure
• Disease recurrence best treated with PO vancomycin in pulsed-tapered fashion
• Emerging data with success using fecal transplant

Nutrition
• High yield subject straightforward questions, straightforward answers next question
• Respiratory Quotient
• Ratio of CO2 produced to O2 consumed: RQ = VCO2 / VO2
• Used to calculate the basal metabolic rate
• Pure carbohydrate oxidation: RQ = 1.0
• Pure protein oxidation: RQ = 0.8
• Pure fat oxidation: RQ = 0.7

Respiratory Quotient
• RQ > 1.0
• Overfeeding with lipogenesis leads to increased CO2 production and potential ventilator issues
• Treatment: decrease calories, specifically carbohydrates
• RQ < 0.7
• Starvation with use of endogenous fat stores to meet caloric needs ketosis
• Treatment: increase calories and carbohydrates

Refeeding Syndrome
• Potentially fatal shifts of fluids and electrolytes in malnourished patients receiving artificial refeeding
• Increased risk: BMI < 16, weight loss > 15% over 3 months, low intake for > 10 days
• Hallmark is hypophosphatemia
• Mechanism: ↑ glucose ↑ ADP/ATP production and ↑ 2,3-dPG ↓ phosphate
• Other potential imbalances:
Hypokalemia
Hypomagnesemia
Abnormal sodium and fluid balance
Changes in glucose, protein, and fat metabolism
Thiamine deficiency

Hypermetabolism
• Hypermetabolism: increased energy expenditure with increased O2 consumption in response to
major stress (e.g., burns, sepsis, surgery, trauma)
Major Stress
↑ catecholamines, cortisol, glucagon, inflammatory mediators
↑ gluconeogenesis from from protein stores in skeletal muscle
Mixed oxidative fuel source (RQ 0.8 – 0.95)