Embed Size (px)
Citation preview

Bchat
StttT
cSc
Technical Note
Hill-Sachs “Remplissage”: An Arthroscopic Solution for theEngaging Hill-Sachs Lesion
Robert J. Purchase, M.D., Eugene M. Wolf, M.D., E. Rhett Hobgood, M.D.,Michael E. Pollock, M.D., and Chad C. Smalley, M.D.
Abstract: We present an arthroscopic technique used to treat traumatic shoulder instability inpatients with glenoid bone loss and a large Hill-Sachs lesion. The procedure consists of anarthroscopic capsulotenodesis of the posterior capsule and infraspinatus tendon to fill theHill-Sachs lesion. With the patient in the lateral decubitus position, a posterior portal isestablished at the lateral aspect of the convexity of the humeral head that is centered over thelesion. After anterior-inferior and anterior-superior portals have been established, the camera isplaced in the anterior-superior portal. The Hill-Sachs lesion is freshened with a bur through theposterior portal. A cannula is inserted in the posterior portal through the deltoid but not throughthe infraspinatus or capsule, and an anchor is placed in the inferior aspect of the humeral lesion.A penetrating grasper is passed through the tendon and posterior capsule, 1 cm inferior to theinitial portal entry site to pull 1 suture limb. A second anchor is placed superiorly, and 1 suturelimb is similarly passed. The inferior suture is tied first with the knots remaining extra-articular,pulling the infraspinatus and capsule into the lesion. After completion, the Bankart lesion canthen be repaired. Key Words: Traumatic shoulder instability—Glenoid bone loss—Hill-Sachslesion—Posterior capsulodesis and infraspinatus tenodesis.
fd
dfiooadnsmSsim
roca and Hartmann recognized the problem ofengagement of the Hill-Sachs lesion on a defi-
ient glenoid in 1890, but Burkhart and De Beer1
ighlighted the role of bony defects in the failure ofrthroscopic stabilization procedures. Recognition ofhe role that glenohumeral bone deficiency plays in the
From the California Pacific Medical Center (R.J.P., E.M.W.),an Francisco, California; Mississippi Sports Medicine and Or-hopaedic Center (E.R.H.), Jackson, Mississippi; Hunterdon Or-hopaedic Specialists (M.E.P.), Flemington, New Jersey; and Cen-er for Sports Medicine & Orthopaedics (C.C.S.), Chattanooga,ennessee, U.S.A.The authors report no conflict of interest.Address correspondence and reprints requests to Robert J. Pur-
hase, M.D., California Pacific Medical Center, 3000 Californiat, San Francisco, CA 94115, U.S.A. E-mail: [email protected]
© 2008 by the Arthroscopy Association of North America
a0749-8063/08/2406-0858$34.00/0doi:10.1016/j.arthro.2008.03.015
Arthroscopy: The Journal of Arthroscopic and Related
ailure of arthroscopic shoulder stabilization proce-ures continues today.2
The question of how best to treat unstable shoul-ers with significant glenoid and humeral bone de-ects remains. Some authors have advocated limit-ng glenohumeral motion through some type ofpen capsular shift that would prevent engagementf the Hill-Sachs lesion by limiting external rotationnd abduction. Other open procedures have beenescribed such as an open transfer of the infraspi-atus tendon and capsule into the Hill-Sachs le-ion.3 More recently, several authors have describedore novel approaches to treat the engaging Hill-achs lesion.4-8 We present a procedure that con-ists of an arthroscopic posterior capsulodesis andnfraspinatus tenodesis to fill (remplissage, whicheans “to fill” in French) the Hill-Sachs lesion in
ddition to an arthroscopic Bankart repair.
723Surgery, Vol 24, No 6 (June), 2008: pp 723-726

asia
ptflt
poHptlrfepdpp
sloal2l
nSmopwab
rnaTstvpAaesHttsatvafsT
uobisolrmi
gbtw
Fp
724 R. J. PURCHASE ET AL.
TECHNIQUE
The Hill-Sachs remplissage technique is similar ton arthroscopic repair of a partial-thickness, articular-urface rotator cuff tear. It consists of fixation of thenfraspinatus tendon and posterior capsule to thebraded surface of the Hill-Sachs lesion.
The patient is placed in the lateral decubitusosition and leaned back approximately 30° withhe shoulder in 30° of abduction and 15° of forwardexion. The arm is suspended with 15 lb of distal
raction.The glenohumeral joint is entered through a posterior
ortal that is placed at the lateral aspect of the convexityf the humeral head so that it is centered directly over theill-Sachs lesion (Fig 1). This remplissage posteriorortal will allow initial visualization and evaluation ofhe joint as well as working access to the Hill-Sachsesion. After an anterior-inferior portal is made in theotator interval, which will be the primary working portalor the anterior labral repair, an anterior-superior portal isstablished at the anterior margin of the acromion. Thisortal should enter immediately behind the biceps ten-on. The arthroscope is switched from the posteriorortal to the anterior-superior portal, and a cannula islaced into the posterior portal.While viewing from the anterior-superior portal, the
urgeon assesses the Hill-Sachs lesion, glenoid boneoss, and anterior labral lesion, as well as the locationf the posterior portal. Posterior portal placement isppropriate if it is located directly over the Hill-Sachsesion and at an angle that will allow the placement ofanchors. If the posterior portal is not appropriate, its
IGURE 1. Left shoulder in lateral decubitus position showingroper placement of posterior remplissage portal.
ocation is optimized with the assistance of a spinal a
eedle at this time. The surface of the engaging Hill-achs lesion is gently freshened with a bur in reverseode with care taken to remove the minimum amount
f surface bone. In addition, the surface of the entireosterior and inferior capsule is freshened with ahisker blade. In anticipation of a Bankart repair, the
nterior labrum and glenoid neck must be preparedefore one proceeds with the remplissage.While maintaining the camera in the anterior-supe-
ior portal, the surgeon carefully withdraws the can-ula in the posterior portal from the posterior capsulend infraspinatus tendon but not through the deltoid.herefore the mouth of the cannula is in the subdeltoidpace. The anchor cannula with obturator is passedhrough the infraspinatus tendon and posterior capsuleia the pre-existing portal, and the first anchor islaced in the inferior aspect of the Hill-Sachs lesion.
penetrating grasper is passed through the tendonnd posterior capsule, 1 cm inferior to the initial portalntry site, to grasp and pull 1 suture limb (Fig 2A). Aecond anchor is placed in the superior aspect of theill-Sachs lesion, and a grasper penetrator is used in
he same fashion to pass 1 suture limb 1 cm superioro the initial portal entry site (Fig 2B). The inferioruture is tied first with the knots remaining extra-rticular in the subdeltoid space. The superior suture isied to complete the remplissage. The knots can beisualized by opening the posterior wall of the sub-cromial bursa. These mattress sutures draw the in-raspinatus and posterior capsule to the abraded bonyurfaces, thus filling the Hill-Sachs lesion (Fig 3A).he Bankart repair can then be completed (Fig 3B).Postoperative care and immobilization are individ-
alized and based on the patient’s history and pathol-gy, but in general, we require the use of an immo-ilizer for 6 weeks. Patients are allowed to remove themmobilizer for “controlled” activities of daily livinguch as eating, showering, and computer use within 1r 2 days. They can remove it for these activities asong as the arm is not abducted and does not externallyotate beyond neutral. Active and resistive range ofotion is started at 6 weeks. No “at-risk” work activ-
ties or contact sports are allowed for 6 months.
DISCUSSION
Several authors have recognized the contribution oflenoid deficiency to the recurrence of anterior insta-ility.1,2 Typically, less attention has been focused onhe significance of the Hill-Sachs lesion. However, itas recognized, in 1948, that a dislocation might recur
fter repair of the capsule and labrum in the presence
oatoa
aiwatf2tH
a
ttaih
F
Ftsi
725HILL-SACHS “REMPLISSAGE”
f a sizable Hill-Sachs lesion.9 It was suggested thatbduction and external rotation of the arm would bringhe Hill-Sachs lesion to engage with the anterior rimf the glenoid, thereby levering the humeral head outnteriorly.
Burkhart and De Beer1 have recently refocusedttention on the role of the engaging Hill-Sachs lesionn recurrent instability. In their series of 194 patientsith recurrent shoulder instability treated with suture
nchors, there were 21 failures (10.8%). However,hose patients who did not have significant bony de-ects had a failure rate of 4%. It was noted that 14 of1 recurrences (67%) had significant bone defects inhe form of anterior-inferior glenoid loss and/or largeill-Sachs lesions.Several open techniques have been developed to
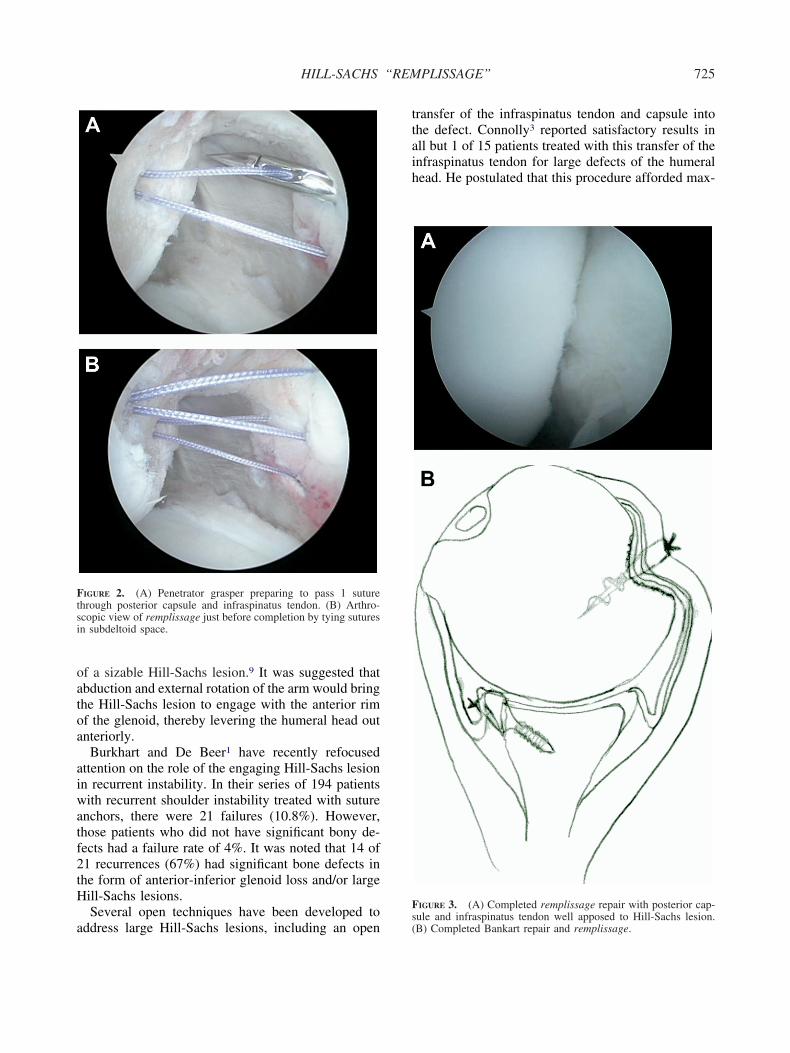
IGURE 2. (A) Penetrator grasper preparing to pass 1 suturehrough posterior capsule and infraspinatus tendon. (B) Arthro-copic view of remplissage just before completion by tying suturesn subdeltoid space.
ddress large Hill-Sachs lesions, including an opens(
ransfer of the infraspinatus tendon and capsule intohe defect. Connolly3 reported satisfactory results inll but 1 of 15 patients treated with this transfer of thenfraspinatus tendon for large defects of the humeralead. He postulated that this procedure afforded max-
IGURE 3. (A) Completed remplissage repair with posterior cap-
ule and infraspinatus tendon well apposed to Hill-Sachs lesion.B) Completed Bankart repair and remplissage.
imltp
bsfnsa
tShpHtda
odsLaias
rSligp
cicpTatba
1
2
3
4
5
6
7
8
9
726 R. J. PURCHASE ET AL.
mum stability by only affecting gliding of the hu-eral head rather than rotation, thus minimizing the
imitation of external rotation in the overhead posi-ion. This is essentially the reverse of the McLaughlinrocedure.Interestingly, an arthroscopic technique has recently
een described by Krackhardt et al.5 to fix the sub-capularis into the anterior humeral head impressionracture. This technique uses suture anchors in a man-er similar to the technique described for the remplis-age. Short-term results of 12 patients treated with therthroscopic McLaughlin procedure are pending.
There have been more recent attempts to developechniques to solve the problem of the engaging Hill-achs lesion. Re et al.6 have described a “trans-umeral head plasty” by use of a deltopectoral ap-roach in which the depressed, compacted bone of theills-Sachs lesion is tamped up from below. Another
echnique, using a limited posterior approach, wasescribed to fill the humeral head defect with osteo-rticular allograft.7
As instruments and techniques are refined, the rolef arthroscopy has expanded. Chapovsky and Kelly4
escribed an all-arthroscopic technique to fill the le-ion, also using osteoarticular allograft. In addition,afosse et al.8 recently described a technique for anrthroscopic Latarjet procedure for anterior shouldernstability. They admit that their technique is complexnd requires experience but report that the early re-ults of 44 cases are promising.
Remplissage is an arthroscopic technique that di-ectly addresses the problem of the engaging Hill-achs lesion. The filling of the abraded Hill-Sachs
esion effectively obliterates it and converts the lesionnto an extra-articular one. Therefore it prevents en-agement. In an unpublished review, only 2 of 24
atients (7%) treated with remplissage have had re-urrent instability. In both, this occurred after signif-cant trauma. Furthermore, there were no significantomplications. In particular, the concern that the rem-lissage would limit rotation did not materialize.here was no significant loss of motion in any planefter the procedure. Remplissage is an effective ar-hroscopic approach in a difficult subgroup of insta-ility patients with a significant potential for failurefter a standard arthroscopic Bankart repair.
REFERENCES
. Burkhart SS, De Beer JF. Traumatic glenohumeral bone defectsand their relationship to failure of arthroscopic Bankart repairs:Significance of the inverted pear glenoid and the humeral en-gaging Hill-Sachs lesion. Arthroscopy 2000;16:677-694.
. Kropf EJ, Tjoumakaris FP, Sekiya JK. Arthroscopic stabiliza-tion: Is there ever a need to open? Arthroscopy 2007;23:779-784.
. Connolly JF. Humeral head defects associated with shoulderdislocation—Their diagnostic and surgical significance. InstrCourse Lect 1972;21:42-54.
. Chapovsky F, Kelly JD IV. Osteochondral allograft transplantationfor treatment of glenohumeral instability. Arthroscopy 2005;21:1007.e1-1007.e4. Available online at www.arthroscopyjournal.org.
. Krackhardt T, Schewe B, Albrecht D, Weise K. Arthroscopicfixation of the subscapularis tendon in the reverse Hill-Sachslesion for traumatic unidirectional posterior dislocation of theshoulder. Arthroscopy 2006;22:227.e1-227.e6. Available onlineat www.arthroscopyjournal.org.
. Re P, Gallo RA, Richmond JC. Transhumeral head plasty forlarge Hill-Sachs lesions. Arthroscopy 2006;22:798.e1-798.e4.Available online at www.arthroscopyjournal.org.
. Kropf EJ, Sekiya JK. Osteoarticular allograft transplantationfor large humeral head defects in glenohumeral instability.Arthroscopy 2007;23:322.e1-322.e5. Available online atwww.arthroscopyjournal.org.
. Lafosse L, Lejeune E, Bouchard A, Kakuda C, Gobezie R,Kochhar T. The arthroscopic Latarjet procedure for the treat-ment of anterior shoulder instability. Arthroscopy 2007;23:1242.e1-1242.e5. Available online at www.arthroscopyjournal.org.
. Palmer I, Widen A. The bone block method for recurrentdislocation of the shoulder joint. J Bone Joint Surg Br
1948;30:53-58.




























