Embed Size (px)
Citation preview


Hiltrud Kivelitz
CVP Coordinator
(February 2012 - September 2017)


1
This year has been a busy one for the Community Visitor
Program (CVP). The focus of the CVP has remained on
meeting our statutory obligations to visit facilities and
raising matters of concern in an independent, respectful
manner.
In my role as the Principal Community Visitor, I am often
reminded about the value of an independent visiting
service reaching out directly to people in facilities. A visiting
program ensures that people’s rights are protected and
reduces barriers to accessing independent assistance.
Importantly, a service such as the CVP assists people to
resolve concerns at the lowest possible level. This avoids
matters escalating into complaints, and focuses the
attention on people receiving high quality treatment and
returning to the community.
Some people will not feel empowered to speak up unless
supported to do so. When people have English as an
additional language, or have had negative experiences with
services in the past, it can be especially difficult to raise
matters.
This is where the work of the CVP is particularly valuable
in supporting the services to provide quality care and
treatment.
The CVP also takes a broader look at the service delivery
context. Moving from the individual to the systemic in its
advocacy for the rights and needs of people receiving
services.
There are a number of areas in which the CVP has been a
strong advocate for many years. The two highest priority
areas for systemic change in the Northern Territory
remain constant: greater use of accredited interpreters
(such as the Aboriginal Interpreter Service) and reducing
the use of seclusion in mental health in-patient facilities.
Part of the benefit of a visiting service is the independent
perspective that comes from having an external party
SALLY SIEVERS
PRINCIPAL
COMMUNITY VISITOR

2
involved. This is especially the case when the places being visited are otherwise ‘closed’, such
as mental health facilities and disability residences. It is even more important when people in
facilities do not often receive visits from friends or family (which may occur for a number of
reasons).
Our regular reporting to the services enables multiple views on their work to be considered.
Sometimes, the CVP will highlight areas where change is needed. Or where additional
investment in facilities may be required. Or how a policy framework has shifted from its original
intent when implemented.
This year, the CVP has made comment along those lines to each of the services we visited. For
example, the shift in the use of specialist disability facilities as supervised places for people on
orders under the Criminal Code; and the need for more investment in facilities that support
the most acutely unwell mental health consumers in Darwin.
This year has been a significant one of change. There were changes in leadership and
governance at the highest levels in the Department of Health and the area health services. The
Alcohol Mandatory Treatment (AMT) program was repealed on 1 September 2017.
While the CVP maintained its role in the facilities until the end of the program, the CVP team
also decreased in size as a substantial proportion of CVP funding came from AMT work. The
additional support provided under the AMT program provided economies of scale that enabled
the CVP to meet its statutory functions across all areas of the service. There is now additional
pressure on the CVP to sustain our current level of service, including the statutory visiting
requirements and maintaining the high quality and integrity of our work.
The work of the CVP is challenging and complex. The Northern Territory has invested in a
professional, paid visiting service. This is essential for a small region such as the Northern
Territory, where securing the right person for the job is important.
The CVP provides an essential service to people in facilities or receiving services who may be
vulnerable or have barriers to accessing help. It provides independent eyes into what can
otherwise be closed spaces. It protects the human rights of people receiving treatment and
care, including those experiencing restrictive practices. It is a valuable service that continues
to play a very important role in our community.
The CVP will need to refocus on meeting statutory obligations, while also being available and
accessible to the many people who raise matters with the CVP for advocacy or complaints
resolution. This work to support consumers, residents, carers, guardians and others with a
genuine interest is at the heart of the CVP’s work.
I would like to acknowledge that it is the people who raise issues with a Community Visitor or
CV Panel who take the first courageous step. To trust another party. To seek their support to
bridge a gap across to the service. To avoid errors or mistakes happening for them, or
sometimes, for those who come after them. To all the people who raised matters with the
CVP this year, I thank them for their courage and trust in our service.

3
REFLECTIONS FROM THE PRINCIPAL COMMUNITY VISITOR..................... 1
CHAPTER 1: OVERVIEW ..................................................................................... 6
REACHING OUT THROUGH VISITS .............................................................. 7
PEOPLE WHO USE THE CVP ......................................................................... 7
WHAT PEOPLE SAY TO US ............................................................................ 8
Issues Raised ................................................................................................... 9
Outcomes of Cases ........................................................................................ 9
AREAS OF FOCUS .......................................................................................... 10
Stronger Internal Complaints ....................................................................... 10
Use of Interpreters ....................................................................................... 10
Safety First .................................................................................................... 11
A PROFESSIONAL CVP .................................................................................. 12
Changes to the CVP Team ........................................................................... 12
A New Focus for the CVP ........................................................................... 13
CHAPTER 2: MENTAL HEALTH ....................................................................... 14
POSITIVE CHANGE ........................................................................................ 14
CULTURAL SAFETY ....................................................................................... 15
Use of Interpreters ....................................................................................... 16
SECLUSION AND RESTRAINT ...................................................................... 18
Seclusion Reduction ...................................................................................... 18
Use of Restraint ............................................................................................ 20
IMPROVING FACILITIES ................................................................................ 20
PARTNERSHIP APPROACHES ....................................................................... 22
Planning and Review ..................................................................................... 23

4
Trauma-Informed Care ................................................................................ 23
YOUTH DETENTION .................................................................................... 24
A PLACE TO LIVE WITH THE RIGHT SUPPORT ........................................ 24
FACILITY PRIORITIES & OPEN RECOMMENDATIONS ............................. 27
Top End Mental Health Service ....................................................................... 27
Central Australia Mental Health Service.......................................................... 30
CHAPTER 3: DISABILITY ................................................................................... 32
POSITIVE CHANGE ........................................................................................ 32
RESIDENT NEEDS .......................................................................................... 34
POSITIVE BEHAVIOUR CLINICAL SUPPORT .............................................. 34
Currency and Depth of Plans ....................................................................... 35
Clinical Support for Transition ..................................................................... 35
Individual Review Processes ......................................................................... 36
Quality Assurance in Clinical Planning .......................................................... 37
PERSON AT THE CENTRE ............................................................................ 37
Age-Related and Mental Health Needs ........................................................ 38
Changing Practice Framework ..................................................................... 38
Formalising Agreements with Agencies ....................................................... 39
BEING HEARD AND UNDERSTOOD .......................................................... 40
FACILITY PRIORITIES & OPEN RECOMMENDATIONS ............................. 41
Secure Care Facility ......................................................................................... 41
Other Premises ................................................................................................ 43
Appropriate Places (Criminal Code) ............................................................... 44
CHAPTER 4: ALCOHOL MANDATORY TREATMENT .................................. 45
POSITIVE NOTES ........................................................................................... 45
THE RESIDENT’S VOICE ............................................................................... 46

5
Less Cases Raised ......................................................................................... 47
CULTURAL SAFETY ....................................................................................... 47
Access to Interpreters .................................................................................. 47
Cultural Obligations...................................................................................... 49
‘LEAST RESTRICTIVE’ DECISIONS ............................................................... 50
PROGRAM MODEL (TREATMENT) .............................................................. 51
Inconsistencies across the NT ...................................................................... 52
MANAGING SAFETY ...................................................................................... 52
Domestic Violence ....................................................................................... 53
Managing Transition to Closure ................................................................... 53
FACILITY PRIORITIES & OPEN RECOMMENDATIONS ............................. 54
Statement on Program Closure ................................................................... 54
Darwin Alcohol Assessment Service ............................................................... 55
Katherine Mandatory Assessment and Rehabilitation Service ........................ 56
Alice Springs Alcohol Assessment Service ....................................................... 57
Darwin AMT Treatment Provider (‘Saltbush Mob’) ....................................... 58
Alice Springs AMT Treatment Provider (‘CAAAPU’) ..................................... 60
APPENDIX 1: DATA TABLE .............................................................................. 63
Visit Data ...................................................................................................... 63
Case (Complaints & Enquiries) Data............................................................ 63
APPENDIX 2: CVP VALUES .............................................................................. 66

6
1. A visiting service assists people to raise issues early, to resolve concerns
at the lowest possible level and improve services.
2. Independence is essential to a quality visiting service, providing
confidence to people in facilities and ensuring integrity in the process to
resolve issues.
3. Community visitors support the protection of human rights and
continuous improvement in service delivery for the most vulnerable.

7
This year, the CVP completed 354 visits to mental
health in-patient units, specialist disability facilities and
AMT facilities.
The CVP visited as part of its statutory obligation under
three pieces of legislation: the Mental Health and
Related Services Act, the Disability Services Act, and the
Alcohol Mandatory Treatment Act.1
The visits were by Community Visitors and
Community Visitor (CV) Panels.2 Some visits were for
the purpose of inspecting registers of restrictive
practices (seclusion and restraint).
The Community Visitors and CV Panels ensure that any restrictive practices are used and
documented consistent with the relevant legislation. This is a very important safeguard in the
legislation for the use of restrictive practices on people. The CVP reports on the inspections
of seclusion and restraint registers in mental health services (see chapter 2).
Community Visitors generally arrange to visit facilities once a week or fortnightly. People in
facilities can also request that a Community Visitor make contact with them. The CVP has a
statutory obligation to ensure that when this occurs, the CVP makes contact with that person
by the next working day.
Number of people 151 1 16
% Contacted Next
Working Day 97% 100% 100%
The Community Visitors are the main way by which the CVP is accessible to vulnerable
residents. Visiting is a core responsibility of the program.
1 The Alcohol Mandatory Treatment Act was repealed by the NT Legislative Assembly on 1 September 2017. 2 CV Panels are a multi-disciplinary panel of members, comprised of a legal, medical/health professional, and
community member. The exact composition of a CV Panel is provided for in the relevant legislation. CV Panels
visit relevant facilities twice a year.

8
The CVP is available to people in relevant facilities providing
involuntary care and treatment. The CVP is also able to provide
support to people receiving services in the community from the
Northern Territory mental health services. The CVP is available to
carers, guardians or other people with a genuine interest in
someone’s care and treatment.
However, the CVP knows from experience and caseload data that
people feel more comfortable raising issues with someone in
person. For this reason, the CVP visits as often as possible to
relevant facilities in Darwin and Alice Springs where people are
receiving involuntary care and treatment.
This year, the CVP received 674 cases across the Northern
Territory. As can be seen, the majority of cases are raised from
people in the Top End. The work of the CVP in the mental health
field has remained strong and steady.
This year, there has been a slight increase in the number of cases
from the disability area, and a decrease in cases from the AMT area.
This is discussed in more detail in the relevant chapters.
For all the 674 cases raised, the CVP records the main issues raised
within a case (sometimes more than one issue is raised) and the
outcome for each issue.
cases from
people receiving
services
raised in person
cases raised in
2016/2017
were enquiries
2016/2017 Cases: Mental Health (406) Disability (32) AMT (228)

9
When reviewed at its highest level, this data is a voice to and about the service from the people
who use the relevant health services, or are affected by it in some way.
Issues are recorded in the CVP database under the major headings of quality of service
provision, rights, information, advocacy, visit/support and smoking. The majority of issues
raised are in the areas of quality services and rights.
Issues Raised
In 2016/2017, there were 1237 issues raised in all cases with the CVP. The main issues raised
this year highlight the important work of the CVP in providing advocacy and information to
people, promoting their right to the ‘least restrictive’ care and treatment and culturally safe
healthcare.
The above four issues were 44% of the total issues raised this year, and represent the core of
the work of the Community Visitors and the CV Panels.
Outcomes of Cases
A central part of how the CVP
works is to seek to resolve matters
at the lowest possible level.
The work aims to resolve matters
before they escalate into
complaints or serious concerns
about quality or safety, rights or
misunderstandings.
Resolved
Ongoing Monitoring
Referred
Not Resolved
Lapsed
Withdrawn
Other

10
It is pleasing for the CVP that the outcome of cases continues to be heavily focused on
resolution. The issues that more frequently record an outcome of ‘ongoing monitoring’ or ‘not
resolved’ were those related to cultural safety and the least restrictive alternative.
Many of the cases where the issue was ‘smoking’ were also not able to be resolved due to the
Northern Territory Department of Health policy that all facilities are smoke-free. People held
in involuntary facilities who are not able to smoke often raised this as an issue of concern. This
concern is not raised in specialist disability facilities, where the Office of Disability has flexible
policies enabling residents to smoke outdoors.
The unique perspective of the CVP provides a window into the Territory-wide areas for
ongoing improvement for the Department of Health. Services vary across the Northern
Territory. Each field of practice that the CVP visits is different. What is common, however, is
the ongoing stated commitment of the services to improve.
Stronger Internal Complaints
Complaints and enquiries raised with an
independent body are an important part of quality
assurance. Building a strong, positive culture of
welcoming feedback is a challenge.
People receiving services, and their loved ones,
need to feel confident that their concerns are dealt
with in a prompt and respectful way.
In each of the relevant Acts establishing the CVP,
an important role is to inquire into and comment on the service’s own ‘internal’ complaints
procedures. This assists services to improve their own processes. Reviewing the internal
complaints procedures of the services has been a strong feature of the CVP’s work this year,
and is evident in some new recommendations for services.
Use of Interpreters
Another strong area of focus for the CVP that has
continued this year is culturally safe healthcare.
The CVP has a specific interest in the use of
accredited interpreters. This is a critically
important issue for the Department of Health and
area health services.
Clear communication between both parties, and
understanding of cultural needs and values, are
essential aspects of quality health care.

11
Nearly all of the people in AMT facilities were Aboriginal
Territorians. All of the people in specialist disability residences
visited by the CVP are Aboriginal Territorians. Many people in
mental health facilities are Aboriginal Territorians. The
Aboriginal Interpreter Service (AIS) therefore is a key partner
for the health services.
In the CVP’s work this year, the majority of cases were raised
by Aboriginal Territorians.3 The CVP database shows that half
of these cases were raised by people needing an interpreter.
This demonstrates the significant proportion of cases raised by
people who have English as an additional language.
The Community Visitors and CV Panels have
conducted visits and inspections, reviewing any
registers of interpreter use, enquiring about staff
training, and promoting liaison with the Aboriginal
Interpreter Service.
Overall, while there are some instances of good
practice, the CVP still does not see a culture of
consistent commitment to and use of interpreters
across the Northern Territory. This needs to
change.
Safety First
The safety of people in involuntary facilities remains a top priority for the CVP. The Community
Visitors and CV Panels ensure that issues related to safety are prioritised in matters raised with
the service and, if necessary, raised at a senior level.
Safety issues that are discussed include the availability of medical staff, the authorisation of
medication, transport to other places or services, absconding, duress alarms and risk
management systems. If necessary, the CVP will move directly to formal recommendations if
the safety concerns need urgent attention.
This year, the CVP kept a close eye on issues related to safety in the AMT program as it moved
towards closure. Understandably, there were challenges for the services in maintaining staffing
levels. High turnover of staff and gaps in staffing while positions are being recruited creates
risks to safety. It was pleasing to see that there were no significant safety issues arise in the
AMT field at this challenging time.
3 The CVP notes that the percentage of cases raised by Aboriginal Territorians varies across the three areas. In
AMT, 94% of cases were raised by Aboriginal Territorians; in disability, 81% of cases (being a small number in
total) were raised by Aboriginal Territorians; in mental health, 43% of cases were raised by Aboriginal
Territorians.
CVP cases were
raised by
Aboriginal
Territorians

12
The CVP would also like to acknowledge the efforts of staff to establish the AMT program in
a short space of time and respond to the issues arising throughout the program. It was a
significant undertaking over the past four years and this work is acknowledged.
The CVP has continued to develop the professional skill base of CV Panel members and
Community Visitors. The CVP welcomes new members to the service, and provides
orientation and support for the role.
The CVP policy and procedure manual is in the final stages of being completed, with
amendments being made to account for the repealing of the Alcohol Mandatory Treatment Act.
An orientation manual was completed by a social work student on placement with the CVP in
Central Australia. The CVP will continue to support students on placement as part of its
commitment to building the professional knowledge and skill base for official visiting
throughout Australia.
Community Visitors who are employed on a permanent basis in the program receive external
peer supervision. This is provided by a professional supervisor with experience in official
visiting. The external supervision sessions are supported by the CVP to safeguard the skills,
resilience and reflective practice of permanent staff performing the work on a daily basis.
Changes to the CVP Team
The Principal Community Visitor, Sally Sievers, was re-appointed in this role for a further three
year period. New CV Panel members were appointed in all fields, in Central Australia and the
Top End.
The CVP welcomed Dr Antonella Ventura, Samantha Bowden, Jared Sharp, Kim McRae, Greg
Betts, Kenton Winsley, Michelle Alleman, Andrea Rennals, Andreea Lachsz, Linda Zargoskis,
Katherine Whitfield, Kate Manley and Seranie Gamble. All were permanently appointed in
2016-2017.4
A long standing CV Panel member, and Community Visitor, Mr Mark O’Reilly resigned from
the CVP after commencing as a member of the NT Civil and Administrative Tribunal. The CVP
wishes Mr O’Reilly well in his role on the Tribunal.
With the repealing of the Alcohol Mandatory Treatment Act on 1 September 2017, the CVP also
ceased to provide services to AMT facilities. Three positions in the CVP were funded by AMT.
The CVP thanks Andrea Rennals, Jennifer Ryder and two administrative staff (Sarah Coe and
then Kate James) for their hard work in the CVP team.
4 Since being appointed, Jared Sharp, Kenton Winsley and Linda Zargoskis have resigned their appointments.

13
A New Focus for the CVP
This year, the CVP restructured its team to enable a more dedicated focus on the work in the
disability field. This decision reflected the importance of the CVP’s role in this dynamic area,
including as the National Disability Insurance Scheme (NDIS) started to rollout across the
Northern Territory.5
As service providers and the CVP become more familiar with areas of practice, new avenues
of inquiry and systemic advocacy emerge. In that sense, the work of continuous improvement
and supporting individual client rights never ceases.
The CVP is keen to continue to support the important work of visiting the most vulnerable
people in our community, many of whom may not have independent people who know them
or can advocate for their rights and needs.
With the reduction in the CVP staffing arising from the end of the AMT program, the CVP
needs to carefully consider how the program can meet statutory obligations with its reduced
resources. It is clear that funding from the expansion into the AMT field provided necessary
capacity and supported the work of the CVP across all three areas of practice.
As the CVP moves into this next phase of its development, the practical limitations of the work
with reduced funding has been raised with the Department of Health.
Quality assurance frameworks are a central aspect of professional service delivery. Official
visitor programs, such as the CVP have an important role in the broader quality assurance
framework for services. Further to this, the CVP enables rights and protections of legislation,
including the right to individual care and treatment, to be given a voice.
The CVP will continue to speak up for people in facilities, supporting them to raise their
matters of concern and working respectfully with services to resolve these matters.
5 Chapter 3 provides more context for the changes that the CVP have observed in visiting to disability residential
facilities.
‘Quotes’ used in the Annual Report faithfully represent the issues and matters raised by
people in facilities. They are not intended to be read as direct, word for word statements.
By including the ‘quotes’, the CVP does not imply that there were errors or failings in
the service in response to any matters raised or represented.
The CVP notes that the Annual Report does not raise all issues that arise over the course
of the year. Some serious matters are not reported on for confidentiality reasons or in
the interests of fairness to the services overall.

14
The mental health services in the Northern Territory6 provide a very
important service for all Territorians. The staff of the services are dedicated
to helping consumers to get well, stay well and live a meaningful life in the
community. Recovery-oriented practice, and care and treatment in the
community, are cornerstones of
contemporary mental health care and
treatment.
This year, the CVP has seen some areas of
positive change in mental health services.
The main area is in youth mental health. In
general, across the Northern Territory,
there are now less children held in mental
health in-patient units with adults.
6 Top End Mental Health Services (TEMHS) and Central Australia Mental Health Services (CAMHS).
1. Increase the use of interpreters for consumers with English as an
additional language
2. Maintain progress to reduce the use of restrictive practices
3. Sustained commitment to improve the Top End facility for acutely
unwell consumers (the Joan Ridley Unit)

15
The new Youth In-Patient Program (YIPP) in Darwin is providing a very good service for
children, and is sometimes used for youth (consumers over 18 years) if possible. 7
The Youth In-Patient Program space is well-equipped. Staff in the program have shown a
strong culture of working closely with children and carers. They are sensitive to the possible
trauma histories of young people. Family members are encouraged to stay with their children
as boarders. The program values the generally positive impact and emotional stability this
provides to children. There has been only a very small number of re-admissions to the Youth
In-Patient Program. This indicates that discharges are well prepared and care in the community
is successful.
At a broader level, the CVP has observed that both the Top End Health Service and the Central
Australia Health Service have been working actively to strengthen their quality and safety
reporting. The services have identified a number of projects for quality improvement that,
when fully implemented, aim to improve client care and treatment.
The reporting of involuntary admissions (‘Form 10s’) has also improved, indicating an
appropriate attention to documentation of the basis for involuntary admission and the
communication of people’s rights on admission.
A high percentage of mental health consumers in the
Northern Territory are Aboriginal. There are also
consumers from culturally and linguistically diverse
backgrounds. This demonstrates the need for mental
health services to be culturally safe for all consumers.8
This year, about 40% of the mental health enquiries and
complaints raised with Community Visitors were made
by Aboriginal Territorians. When this data is combined
with that raised by people with a culturally and
linguistically diverse background, it increases to just over
half of all CVP mental health enquiries and complaints.
During visits, Community Visitors have observed a number of practices that demonstrate the
services focus on cultural safety. There are ‘talking posters’ at the in-patient facilities to explain
patient’s rights in several local languages. Conversations are usually in plain English where
needed.
7 For clarity, in the report, the term child/children is used to mean any person under the age of 18 years and the
term ‘youth’ is used to mean people aged 18-25 years. The ‘Youth In-Patient Program’ is the name of the facility
for child consumers, however it sometimes accommodates youth at the discretion of the service. 8 Standing Council of Health, Mental Health Statement of Rights and Responsibilities 2012, p 6 (Part 1, Inherent
dignity and equal protection …(e) culturally and linguistically diverse communities receive culturally and
linguistically appropriate services.)

16
Family members from remote areas are helped to
board with their relative at in-patient facilities. Some
doctors who treat consumers in the hospital also are
able to visit that person’s home community,
providing continuity of care. In Central Australia in
particular the attendance of traditional healers is
actively supported.
However, consumers from culturally diverse
backgrounds have raised concerns with the
Community Visitors on many occasions. This has
included on issues such as access to or use of interpreters and Aboriginal mental health
workers, supporting cultural obligations or respecting cultural needs. The CVP’s data on issues
raised in the mental health field confirms the frequency of matters relating to cultural safety.9
Use of Interpreters
For several years the CVP has had particular concerns about the low use of qualified
interpreters in mental health services across the Northern Territory. Qualified interpreters
are bound by a code of conduct (including confidentiality) and receive specialist training to
interpret. This includes interpreting in challenging contexts when a person is mentally unwell.
Consumers who speak an additional language to English have raised with Community Visitors
about being uncertain about things such as their diagnosis, treatment, discharge, physical health
needs or procedures. Some consumers talked about not being able to fully express their
concerns or ask all the questions they had in mind.
Diagnosis and treatment decisions in mental health care rely largely on effective
communication. The responsibility for effective communication rests with the service.
There are concerns whether the service had done everything possible to use an interpreter
for key conversations, such as a person’s rights on admission or in distressing situations, for
example seclusions and restraints. Alternatively, if interpreters are not available on a regular
basis, the services need to liaise proactively with relevant booking organisations10 about the
needs of consumers for interpreters.
To support this, the CVP has advocated for registers of interpreter bookings and outcomes to
be established and kept current. The registers provide valuable information to demonstrate
the service’s commitment to using interpreters and the outcomes of efforts to meet consumer
needs. At times, the CVP has observed that registers have not been current or not used to
inform service liaison.
9 See Appendix 1. 10 The relevant booking organisations include the Northern Territory Aboriginal Interpreter Service (AIS), the
national Translating and Interpreting Service (TIS), and the National Auslan Interpreting Booking Service (NABS).

17
Further to this, Community Visitors have observed that the use of interpreters is not
consistent. There remain many misconceptions among staff about the use of interpreters and
a person’s capacity to fully participate in their treatment in English.
Even if consumers navigate everyday situations in
English reasonably well, there still are many
obstacles to communication. These include how
stressful it can be to be unwell, away from home
and family support, and in an unfamiliar hospital
environment.
The words used in healthcare settings are different
from everyday English words. Some staff may be
difficult to understand for a range of reasons.
Many factors might affect how the consumer
engages in the discussion. The ‘power imbalance’ between staff and consumers may be even
harder to negotiate across language barriers.
The disadvantage consumers experience when no interpreters are being used is even greater
for clients with hearing impairments. Many Deaf people from remote areas do not
communicate in standard Auslan (the Australian sign language). Instead they have developed
their own communication methods with families and their communities. 11 This can be isolating
when the person needs to communicate with others.
A common misunderstanding is that family members might be able to help services to
communicate by ‘interpreting’. However, professional standards require that families are not
used as interpreters.12 Having to interpret is a demanding task with specific skills. It requires
an independent, accredited person who has had training and professional support in the area.
Over recent years, the Aboriginal Interpreter Service has developed more options to increase
the availability of interpreters (for example, phone and video link). The CVP knows that at
times it can be difficult to get interpreters at the time they are needed.
A close collaboration between the mental health services with the Aboriginal Interpreter
Service in particular is needed to resolve service problems together. The CVP is pleased to
see that a quality improvement project to achieve this goal has commenced in the Central
Australia mental health service.
11 Sign language interpreters can be booked in the Northern Territory through the National Auslan Booking
Service (NABS). The CVP’s experience in using the local Auslan interpreter is that this service has developed a
very good knowledge of local clients. The use of NABS to improve communication for clients with a hearing
impairment is essential. 12 Commonwealth Ombudsman, Talking in language: Indigenous language interpreters and government
communication, 2011; Medical Board of Australia, Code of Conduct for Doctors in Australia; Northern Territory
Government, NT Language Services Policy, 2012.

18
Seclusion and restraint13 can traumatise consumers. There is no evidence that these practices
have any therapeutic benefit for consumers.14 Under the law, seclusion and restraint are only
allowed to be used in very limited circumstances.15
The services have policies and procedures in place on how the seclusion and restraint laws are
implemented. The CVP is obligated to review the records the services keep on restrictive
practices and comment on the findings.
Evidence shows that restrictive practices in mental health facilities can be significantly
reduced.16 In the last two years, both area health services have made considerable efforts to
reduce the use of seclusion and restraint.
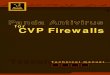
Seclusion Reduction
Projects based on the ‘Safe
Wards’ model have been
implemented in Darwin and
Alice Springs, with the model
adapted for the Northern
Territory context.
The projects have focussed in
particular on trying to reduce
conflict and build stronger,
more positive relationships
with consumers.17
13 Seclusion is defined as the “confinement of a patient at any time of the day or night alone in a room or area
from which free exit is prevented”, and restraint is the “application by health care staff of hands-on immobilisation
or the physical restriction of a person to prevent the person from harming himself/herself or endangering others
or to ensure the provision of essential medical treatment” (Australian Institute for Health and Welfare). 14 Melbourne Social Equity Institute: Seclusion and Restraint Project-Overview, August 2014;
The National Centre of Mental Health Research, Information and Workforce Development Best Practice in the
Reduction and Elimination of Seclusion and Restraint, Prepared for the National Mental Health Commission. Te
Pou:: Seclusion: Time for Change, 2008 15 Mental Health and Related Services Act, ss 61-62. The Act only allows seclusion and mechanical restraint to be
used to prevent harm to the person or others, prevent the person from absconding or persistently destroying
property. 16 Melbourne Social Equity Institute: Seclusion and Restraint Project-Overview, August 2014;
Kevin Ann Hucksthorn: Reducing Seclusion & Restraint Use in Mental Health settings: Core Strategies for
Prevention: Journal of Psychosocial Nursing and Mental Health Services, September 2004-Vol. 42-Iss9, pp.22-33 17 Examples given: know each other, clear mutual expectations, calm down methods, bed news mitigation,
soft/positive words, talk down, reassurance, discharge messages
15 12 3197 93 83
47
185243 198
171243
192180
0
50
100
150
200
250
300
350
400
2010-2011 2011-2012 2012-2013 2013-2014 2014-2015 2015-2016 2016-2017
Seclusion Events by Financial Year
CAHS TEHS
227

19
Last year, the CVP reported on the success of the
Top End project (called ‘SafeCARE’). There were less
seclusion events and, if events did occur, consumers
were in seclusion for shorter periods of time.18
This year, the Central Australian ‘Safe Wards’ project
has led to a reduction in seclusion events. There has
also been a decrease in the number of seclusion
events for children in Central Australia.19
Unfortunately, the initial positive trends in the Top
End were not sustained this year. While there was a
significant decrease in seclusion events in the first half
of 2016, the number of seclusion events in the Top
End has returned to similar levels as previous years.
The CVP has noted that some strategies in the Top
End were not consistently maintained this year.20
While nurses and other staff were involved in ongoing
SafeCARE training, the CVP was told that medical
practitioners were not.
As with previous years, there remain particular
concerns about the use of restrictive practices with
Aboriginal Territorians. Of those people secluded,
Aboriginal men are more frequently secluded and for
longer periods. The reasons for this are unclear.
The documentation the services keep shows that
interpreters and Aboriginal Mental Health Workers
are rarely used in the context of seclusions.
This might mean that a person who is already
mentally unwell may spend many hours in seclusion
without understanding what is happening or why.
18 Reduction from 159 seclusion events in July-December 2015 to 20 events in January to June 2016. 19 In Alice Springs in particular, seclusions of children were reduced from 33 events in 2015-2016 to 2 events in
2016-2017. 20 Strategies that were not as consistently implemented this year in the high security ward (Joan Ridley Unit)
included the availability of structured activities, access to outdoor spaces, debriefing for consumers after seclusion,
and reviews by consultant psychiatrists for all seclusions over 6 hours.
Seclusion Events CAHS TEHS Total
Over Four Hours 13 58 71
Seclusion events in the
Northern Territory in
2016/17
adults secluded
children secluded
Aboriginal
people secluded

20
The CVP also has had concerns for the wellbeing of other
vulnerable people, for example people with medical or physical
problems, for example hearing loss, or a known history of
trauma.
Use of Restraint
With respect to restraints, the CVP has also made comments
this year about the importance of using consistent, nationally
agreed definitions for restraint. By using consistent definitions,
the service is able to monitor restrictive practices with integrity. The CVP noted a record in
which restraints were described as ‘safe hold’ and not recorded in the physical restraint
register. This was raised as a concern with the service concerned.
With respect to mechanical restraint, this is defined in the Mental Health and Related Services
Act. The CV Panel for the Central Australia Health Service made specific mention this year of
restrictive practices as they apply to prisoners who are admitted for care and treatment under
mental health legislation.
The services need to ensure that positive developments in seclusion reduction are sustained
over time. Similarly, the service needs to maintain consistency in recording and monitoring the
use of restraints. A culture of preventing restrictive practices need to be led and supported at
all levels and in all professions of the service.
Overall, while there has been positive outcomes for the Alice Springs mental health services in
reducing seclusion, the lessons learned in the Top End are timely. It is essential to maintain
consistency and a strong focus in each successive year. Sustaining reductions in seclusion and
restraint is a long term project for the services.
Over many years, the CVP has raised concerns about
the state of the ‘high dependency’ mental health unit in
Royal Darwin Hospital.21 This facility is called the Joan
Ridley Unit (JRU). JRU has 8 beds and is the largest ‘high
dependency unit’ for the Northern Territory.
21 ‘Intensive’ care and treatment for acutely unwell consumers is normally provided on a separate ward. These
wards are usually called a ‘high dependency unit’ or ‘low stimulus unit’. There are a number of wards in the Royal
Darwin Hospital for mental health patients, therefore the CVP will refer to the specific unit of concern by its
name, being the Joan Ridley Unit.
seclusion events
of a child

21
Towards the end of this reporting year, long anticipated renovations started. These are still
underway at the time of writing.22 This work has made a difference in the general appearance
of the ward.
While these changes are positive, major structural problems and overcrowding continue to
exist. It is not uncommon for there to be 3 to 5 patients on the ward, above the designated
capacity. At times consumers sleep on mattresses, rather than beds, in an interview room.
Overcrowding leads to significant problems of safety, privacy, dignity and wellbeing. The CVP
has concerns regarding the lack of private spaces, the overall cleanliness of the ward, and
bathroom amenity. Of particular concern, female consumers report feeling unsafe.
The frequent presence of correctional officers to guard patients from prisons, and uniformed
safety officers for other high risk patients, further contributes to an impression that JRU is a
prison rather than a hospital ward.
The conditions of JRU impact negatively on
consumers every day, and this is what Community
Visitors hear when they visit the unit. As evidence
of this, in Central Australia, safety concerns were
only raised once this year. In the Top End, safety
concerns were raised on 20 occasions.
Staff of the Top End mental health service share
many of the CVP’s concerns. Submissions have
been made to try and improve the safety and
facilities of the ward. To date no changes or
improvements have been announced, beyond the
current renovation work.
The CVP is of the view that it is not acceptable that
the most unwell and vulnerable consumers
(including those who require higher levels of
security) are required to be held in an outdated,
unclean and unsafe environment.
The CVP acknowledges the work staff undertake at
JRU and their advocacy for consumers. They are
supporting consumers with high levels of acute
mental illness and agitation. They are doing so,
however, while also dealing with a challenging
environment
22 The renovations include painting of walls and doors, concrete block beds replaced by modern beds, and carpets
replaced by vinyl flooring. Nurses have also improved the garden area.

22
Consideration should be given to the urgent need for a contemporary facility for acutely unwell
consumers in the Northern Territory. Such investment also needs to address endemic
concerns with the infrastructure in adjoining wards (such as poor water pressure and
temperature control in the bathrooms).
While JRU is the priority, an in-depth analysis of the issues (including community supports,
discharge planning, and care in the community) needs to take place.
A partnership approach to care and treatment with
consumers, carers and staff is required by national
practice guidelines.23 This is supported also by the
legislation.24
In general, interactions with staff are positive. The
CVP often receives feedback about the helpful,
supportive and caring attitude of staff.
Nevertheless, there remain a number of cases raised
with the Community Visitors where consumers and
carers were not sufficiently involved in their treatment
and care.
The CVP has noted that this can occur in particular when consumers are being treated against
their wishes (‘involuntary’) and do not agree with the treatment decisions. The CVP
acknowledges that the services have a duty of care, and often carry a high risk when making
decisions about treatment and imposing restrictions.
However, people lose trust with services if they feel
disrespected or control of their own lives is taken
away from them. When people do not want to
engage with the services because of lack of trust, it
can result in the services making more restrictive
decisions.
The service is responsible for making every effort to
avoid this occurring and to act in a way that supports
people to engage in their care as much as possible.
A culture of working in partnership with consumers
and carers is required. Consumers’ dignity and right
23 National Standards for Mental Health Services 2010, Standard 3. National Mental Health Strategy: National
Practice Standards for the Mental Health Workforce 2013: Part 3, Standard 2.
Northern Territory: Mental Health Service Strategic Plan 2015-2021, Priority Area 4 24 Mental Health and Related Services Act, s12

23
to decide their own lives, as much as possible,
needs to be protected. Staff need to listen carefully
to consider how consumers and carers can
contribute to treatment planning.
In recent years, both services have created peer
worker positions.25 These are valuable roles.
Although the rights of consumers and carers to be
involved in treatment planning is part of the law,26
the CVP would like to see a stronger focus on this
in practice. There needs to be more evidence of
the service’s obligation to work in a genuine
partnership with consumers and carers.
Planning and Review
Planning is an essential part of effective treatment
and care. Plans need to be developed in a proactive
and timely way together with consumers and carers,
reviewed together for their effectiveness.
Although there has been some positive evidence of
good planning, many cases raised with Community
Visitors showed a lack of genuine involvement of
consumers and carers, limited care planning, ad hoc
responses and unclear responsibilities.
Sometimes there was very limited information
about the person’s goals and care needs and how
these would be supported.
Community Visitors observed that this delayed progress for the consumer for example,
consumers remaining on the ward for longer periods of time, re-admissions soon after
discharge, and repeated use of crisis services. This is also affecting the scarce resources of the
services.
Trauma-Informed Care
The CVP has continued to pay close attention to the care of people who are vulnerable due
to their experience of trauma. There is a strong link between mental health conditions and
trauma, especially when experienced in childhood. Being admitted to a mental health in-patient
25 In Central Australia two part-time positions for one carer and one consumer consultant, in the Top End one
full-time position for a consumer and carer consultant. 26 Mental Health and Related Services Act and Carers Recognition Act.

24
facility against your will, and possible experiencing other restrictions, can traumatise people
further.
While there has been examples of good planning and practice to avoid re-traumatising people,
at times consumers or carers have told Community Visitors about how services have caused
further distress and added to their trauma.
The CVP considers that trauma-informed care remains a high priority for the NT mental health
services, to ensure the best quality service for some of the most vulnerable people in the
community.
The need for specialist trauma-informed care for some people is particularly evident for young
people in correctional facilities (‘youth detention’). In previous years, the CVP has raised
concerns about mental health care of children and young people. There has been some positive
changes for children and youth in the community.
For children in youth detention, however, the CVP’s concerns about the lack of mental health
services remain. In the past year, there has been improved procedures for review of ‘at risk’
youth detainees. This is a limited improvement.
Children in youth detention still only receive a comprehensive mental health assessment if they
need to be admitted to an emergency department. In the CVP’s view there needs to be
substantial improvements in meeting the mental health needs of youth detainees. This includes
the need for routine mental health assessments and integrated care for children coming into
and out of detention.27
This care needs to be supported by the involvement of child and youth psychiatrists wherever
possible. This is particularly important considering the history of trauma that is known to be
experienced by youth detainees.28
Affordable, secure and (for some people) supported accommodation is a cornerstone of
wellbeing and recovery in mental health.29 In the Northern Territory Mental Health Services
27 This is particularly important considering the interim findings of the Royal Commission into the Protection and
Detention of Children in the Northern Territory (31 March 2017). The interim report noted the complex needs
of youth detainees, including cognitive disabilities, mental illness, addiction to nicotine, alcohol and other drugs as
well as physical deficits such as poor hearing and sight, and, in some cases, also functional illiteracy (p 38). 28 Royal Australian and New Zealand College of Psychiatrists: Maximising Opportunities for Recovery, Submission
for the Royal Commission in to the Protection and Detention of Children in the Northern Territory, 2016
Strathis, S.L.; Harden, S.; Martin, G. and Chalk, J: Challenges in establishing forensic mental health services within
Australian youth detention centres, Psychiatry, Psychology and Law, 20(6), 2013 29 Standing Council of Health, Mental Health Statement of Rights and Responsibilities 2012, p 7 (Part II, Non-
discrimination and social inclusion…(g) equal opportunities to access and maintain housing.)

25
Strategic Plan 2015-2021, a key priority area is increasing access to appropriate and supported
housing.
The CVP has continued to raise the ongoing urgent need to increase the availability of secure
and supported housing. Over the past few years, the Northern Territory mental health
services have sought to expand supported accommodation options for acute or complex
clients of the service.30
While positive, these successes have only provided a small number of additional beds.
Concerns have also been raised about a lack of clear procedures and guidelines for protection
of consumer rights.
The CVP has made comment in every annual report since 2003-2004 about the need for
appropriate accommodation options for people living with mental illness. In 2011-2012, the
CVP advocated for a comprehensive needs analysis on accommodation and support options
to support service planning.31
Following this, a housing project was supported by the Department of Health. The scope and
focus of the project moved away from needs analysis. The project resulted in housing officer
positions being funded within the area mental health services. These staff work to help close
accommodation gaps for consumers and support inter-agency collaboration.
The CVP remains concerned that at present the needs of certain vulnerable consumers remain
inadequately met. Cases raised with the CVP this year have shown that some individuals
remain in restrictive environments or receive insufficient support in the community.
In the past year, several people with high care needs have remained on the mental health in-
patient wards for extended periods (sometimes 6 months and longer) due to lack of
appropriate supported community-based accommodation.
The pressures of an acute care setting may also mean that these consumers’ needs are not as
high priority on a daily basis. The consumer is at risk of becoming institutionalised and lose life
skills.
The planning processes for these complex consumer needs are often very slow, especially
when multiple stakeholders are involved and responsibilities are unclear. The CVP is
particularly concerned about the impact on individuals when they remain in an acute care
setting that is not appropriate to their needs.
The need for appropriate supported accommodation for people living with mental illness is
evident throughout the Northern Territory. There have been some additional initiatives put in
place for the Top End. The Northern Territory Government’s strategic policy for mental
30 In Alice Springs the sub-acute facility was opened in 2013-2014. In Darwin, the Top End mental health service
took over operation of an established facility in May 2017. 31 CVP Annual Report, 2011-2012, p8.

26
health32 includes a funded trial project to provide support and tenancy stability for people with
mental illness living in public housing in Darwin and Palmerston.33
The trial project includes partner agencies such as Territory Housing, NT Mental Health
Coalition, NT Shelter and the Top End mental health services. Partner agencies are working
together to determine tenancy support needs of current public housing tenants with mental
illness. The project is seeking to develop a viable model, with psychosocial support to be
provided by community-managed mental health services.
The various housing projects supported by the Department of Health provide some limited
benefits, primarily in inter-agency coordination and collaboration. The tangible benefits for
consumers across the Northern Territory, including those not currently in public housing, are
less obvious.
It also remains unclear how the various projects inform strategic planning on the overall
housing and support needs for people with mental illness in the Northern Territory. The CVP
has observed that this lack of an evidence-based approach has affected the planning.
While various housing projects have been undertaken, there remains a lack of proactive,
strategic approaches for the Northern Territory. There remains insufficient information to
clearly determine the needs, and then put in place strategies to meet the needs for short and
long term housing and support for consumers.
The CVP continues to strongly advocate for a more strategic approach to mental health
housing and support needs. There needs to be active work to develop and fund a range of
different accommodation options. This requires a ‘whole of government’ approach.
32 Northern Territory Government, Strengthening Mental Health Policy, 2012. 33 Northern Territory Government, Strengthening Mental Health Policy, 2012, ‘The housing accommodation
support initiative’. This trial project proposes to invest $3 million over four years to provide ‘wrap-around’
support system including clinical services, tenancy and psychosocial support. It is proposed that the wrap around
services will support 50 consumers in the first year

27
Achievements o 9 CVP recommendations closed.
o Improvement of record keeping of restrictive practices.
o Consistent very good provision of meaningful and diverse activities in Cowdy ward,
with the facility also used by consumers in nearby wards.
o Some pro-active planning processes to support complex clients and some evidence
of collaborative care planning with consumers and carers.
o For the youth in-patient program, a strong culture of client-centred, trauma-
informed care with transparent work with families and carers
o Flexible use of the youth in-patient space for other vulnerable consumers and
carers, and expanded admission criteria to improve services to children in acute
crisis situations.
o Renovation work in Cowdy ward common areas, and the Joan Ridley Unit (beds
replaced, bedrooms painted, garden improved, with work still underway).
o Improved outdoor area for clients in Cowdy ward who smoke.
o Taken responsibility for management of a pre-existing accommodation facility for
consumers with specific needs.
Areas for Improvement o A stronger focus on consumer rights, in particular relating to protections for
consumers to communicate (section 98), accessing information before a tribunal
hearing (section 132), and rights on involuntary admission and voluntary admission.
o Improved access to reliable complaints mechanisms.
o Strengthen planning processes and decision-making when consumers remain in the
in-patient ward due to lack of accommodation (and providing additional resources
to address the needs of these long term consumers).
o Consistently applying principles of trauma-informed and recovery-oriented care.
o Developing policies, including on the rights and responsibilities of consumers and
carers, for people living in the newly acquired accommodation facility.
o Addressing the problems with water pressure and temperature in bathrooms in
Cowdy ward.
Priority Issues o Need for consistent use, and recording of the requests for and use of qualified
interpreters for consumers who require interpreters.
o Substantially improving standards of facility and safety in the ‘high dependency
ward’ known as the Joan Ridley Unit.
o Refocusing on pro-active strategies to reduce seclusion and restraint, including
implementing policies that promote shorter and less frequent seclusions and
reducing the use of restrictive practices on children.
o Engaging in genuine partnership with consumers and carers.

28
CVP Recommendations Made By Date Status
1. That a comprehensive accommodation and
support model is developed, adequately resourced
and provided in the Top End of Northern
Territory. (Reworded, 2016)
CV Panel34 Nov
2006
Open
2. That the Mental Health Service ensure that
interpreters are present at assessment for all
consumers whose first language is not English. It is
further recommended that interpreter assistance
is then arranged for all further assessments and to
assist the consumer at any hearing before the
Mental Health Review Tribunal.
CV Panel May
2007
Open
3. That the service provide evidence that in the
process of involuntary admissions that there is
adequate explanation of rights to consumers,
including legal status on admission, offering of
interpreters and early access to the Mental Health
Review Tribunal. (Reworded, 2016)
CV Panel Nov
2011
Open
4. That the Top End Mental Health Service (TEMHS)
implement strategies to ensure the cultural safety
of clients with a particular focus on the needs of
Indigenous clients in line with TEMHS values and
objectives.
Community
Visitor
May
2013
Open
5. That management request a report from the
Director of ECT on evidence of quality activities,
demographics of clients receiving ECT, the nature
of consent and key clinical indicators for ECT
across the patient population.
CV Panel Apr
2013
Open
6. It is recommended that clear, culturally and
therapeutically safe arrangements be made for the
management of women consumers on the Joan
Ridley Unit (JRU).
CV Panel Mar
2016
Open
7. The TEMHS review and improve processes
related to the service’s applications to the Mental
Health Review Tribunal, in particular to ensure
client access to information consistent with the
expectation of natural justice and section 132 of
the Mental Health and Related Services Act
(MHRSA).
Community
Visitor
Nov
2016
Open
34 The CV Panel for Top End mental health in-patient facility was not convened for the period January-June 2017.
The CV Panel visit occurred on 7 November 2016 and open recommendations date from this visit report.

29
8. That TEMHS address the need for improved JRU
infrastructure to meet the requirements for all
clients, but particularly women with high care
needs to have a safe and therapeutic hospital
environment.
Community
Visitor
Nov
2016
Open
9. That the interior and exterior environment of the
High Dependency Unit (HDU) of Cowdy be
refurbished and activities be made available on
HDU to ensure an appropriate therapeutic
environment for consumers.
CV Panel Dec
2016
Open
10. a) That TEMHS urgently develops and implements
appropriate recovery-oriented care plans for long
term clients in the In-Patient Unit (IPU).
b) That the service develop a policy that triggers
recovery-orientated nursing plans and
interventions for clients who are likely to remain
on the ward for longer periods and provides
appropriate resources for this.
Community
Visitor
Mar
2017
Open
11. That TEMHS develop policies and procedures
clarifying the use of section 98 restrictions to
ensure that clients only have their rights restricted
in line with legislation.
Community
Visitor
May
2017
Open
12. That TEMHS establish and advise the service’s
targets to improve trauma-informed care.
(reworded)
Community
Visitor
Jul
2017
Open
13. That TEMHS provide to the CVP the terms of
reference/performance indicators how current
seclusion reviews and analyses contribute to
seclusion reduction, both for individuals and
systemically.
Community
Visitor
Aug
2017
Open

30
Achievements o 12 CVP recommendations closed.
o Increased focus on SafeWards seclusion reduction initiative, including training for
staff and strategies to de-escalate behaviours of concern.
o Significant decrease in the use of seclusion on children.
o Transition of a long-term consumer on the ward to more appropriate
accommodation.
Areas for Improvement o Greater focus on the use of trauma-informed care.
o More detailed discharge planning, including collaboration with all stakeholders.
o Increased focus on the needs of Aboriginal consumers, in particular those
experiencing or at risk of restrictive practices.
o Increased consumer and carer involvement in care planning and decision-making.
o More robust internal complaints procedures and follow-up, including for matters
seen as minor, to avoid escalation of concerns.
o Greater clarity in governance of forensic mental health services, including the role
and responsibilities of the Top End Health Service.
o Clarify responsibilities, leadership and decision making pathways for consumers who
are also cared for by other departments, in particular Office of Disability.
Priority Issues o Building strong relationship with Aboriginal Interpreter Service to ensure greater
availability of qualified interpreters for Aboriginal Territorians.
o Focus on staff training in the professional use of accredited interpreters to improve
assessments, reviews and consumer information about rights.
o Develop policies and rights and responsibilities of consumers and carers for the sub-
acute facility.
o Consistent recording of restraints according to national guidelines and to promote
continuous improvement.
CVP Recommendations Made By Date Status
1. That the Mental Health Unit review its seclusion
practices and introduce strategies aimed at
reducing the rates of seclusion, with a special focus
on de-escalation techniques. (Reworded)
CV Panel Dec
2013
Open
2. That significant efforts are made to recruit to the
Aboriginal Mental Health Worker position within
the Forensic Mental Health Team, including any
development required to upskill a suitable
applicant. (Reworded)
Community
Visitor
Aug
2014
Open

31
3. That the CAHS and TEHS Boards formalise
arrangements for responsibility for forensic mental
health services in the Central Australian region,
including the provision of appropriate and
accessible mental health support to Central
Australian youth and adult detainees.
Community
Visitor
Dec
2016
Open
4. That CAHS and TEHS urgently provide integrated
mental health services to youth detainees in the
Northern Territory, supported by child and
adolescent psychiatrists or forensic psychiatrists
with adolescent experience.
Community
Visitor
Dec
2016
Open
5. That CAHS Mental Health review processes to
improve effectiveness of processing both internal
and external complaints and provides CVP with
the service complaints register.
Community
Visitor
Jun
2017
Open
6. That a new policy be developed in accordance
with professionally accepted standards and the
least restrictive principles as required by the
Mental Health and Related Services Act to ensure
that adopted practices in the Mental Health Unit
(MHU) comply with the fundamental principles of
the Act when a prisoner becomes a mental health
patient, to revert to prisoner status when out of
the facility
CV Panel Jun
2017
Open
7. That CAHS Mental Health actively pursue
negotiations with Aboriginal Interpreter Service
(AIS) management in Alice Springs with a view to
improve interpreter attendance in matters related
to mental health and insist on the human right of
mental health consumers to be heard and
understood in their primary language to ensure the
best possible outcome in their care and treatment.
CV Panel Jun
2017
Open
8. That existing seclusion policies and procedures
include detailed strategies to reduce the use and
impact of seclusion on minors. (Reworded)
Community
Visitor
Jul
2017
Open
9. That CAHS Mental Health demonstrate in the
review of its policy and procedures how National
Best Practice is embedded in the definition, use
and recording of episodes of restraint when used
across the Mental Health Unit (MHU).
Community
Visitor
Jul
2017
Open

32
The CVP is pleased to report a number of positive events this year in the
work of the CVP and the Office of Disability in specialist disability places.
While concerns remain in key areas, the CVP has seen some good progress
and outcomes. The positive changes that particularly stand out are long
term residents moving to community accommodation and a stronger focus
on building staff capacity.
This year, there has been a significant increase in the number of matters raised with a
Community Visitor for assistance. The total number of residents in disability places covered by
the work of the CVP has remained about the same. However, the number of cases raised by
residents and others in the specialist disability area has increased by 88% over twelve months.
This increase in cases is positive. Many residents are long-term clients. Over time, the residents
and others in the specialist disability area have come to see Community Visitors as familiar
faces. Residents better understand the role of the CVP.
The majority of residents in specialist disability places speak English as an additional language.
This past year Community Visitors have worked hard to make sure, as much as possible, that
interpreters are available on visits. The Community Visitors have reported that some residents
who previously were quieter are now raising issues.
1. Better quality clinical treatment and oversight, especially in Positive
Behaviour Support Plans and client reviews.
2. Formal agreements with other agencies involved with resident care
and treatment.
3. Use of independent accredited interpreters for significant clinical and
management discussions with residents.

33
From the service perspective, the CVP has seen the service improve in a number of ways. For
the past two annual reports, the CVP asked how residents were being supported to move to
community-based accommodation. This year, four long-term residents moved into the
community while still receiving direct support from the Office of Disability.
Moving to a house in the community was a significant and much anticipated move for the
residents. The pleasure on the faces of residents when showing Community Visitors their new
house was obvious.
The Office of Disability has had some staffing challenges this year, with turnover in senior staff
positions in facilities and the organisation more broadly. Despite this, in general terms the
organisation managed to maintain quality care for residents during these periods.
The Community Visitors have noticed that there was increased clinical input from professional
staff and consultants working on-site. Professional staff have focussed in particular on
supporting disability workers to build their skills and
knowledge.
Over the year, Community Visitors were also told
about a move towards a ‘key worker’ model of
staffing support. This model assigns workers to the
same resident, which in turn increases staff
knowledge, rapport and understanding of how best
to support residents. The CVP supports this
direction.
Importantly, there was an overall reduction in
restrictive interventions used on residents. Alongside this were more robust processes,
especially in Central Australia, for debriefing and learning from incidents of concern with all
staff involved. This is further evidence of the service’s increasing focus on staff skills and a ‘least
restrictive’ approach to care and treatment.
The quality of staff interactions with residents continues to be observed as generally very good.
When difficulties with staff were raised directly by residents or other staff, the Community
Visitors saw evidence that these concerns were taken seriously.
In this year, especially in Central Australia, the service recruited a number of Aboriginal staff.
A cultural advisor with language skills was appointed in the Secure Care Facility. When a female
resident moved into one facility, there were more female staff recruited and issues related to
her care were well managed.
These achievements are positive steps towards client care and a quality service. The CVP
commends the Office of Disability for the above improvements.

34
The most common issue raised with the
Community Visitors by residents is their
strong desire and interest to have more
contact with their families and
communities. All residents visited by the
Community Visitors are Aboriginal
Territorians.
The desire to see family and go home to
their communities is a human need, but for
Aboriginal residents it is also one of cultural
safety in the provision of services by the Office of Disability. The Community Visitors observed
that, in general, there was a strong commitment to support more family contact.
Where family members are well known to the service, this contact usually occurs for residents
in a timely way. The Community Visitors have noted the service taking residents overnight to
communities, or supporting them if staying overnight on their own at a family member’s
residence.
Unfortunately, some residents may be disconnected
from their families, or their families live remote from the
residential facilities. This can present challenges for the
service to get to know families and consistently
encourage positive contact.
The CVP encourages the service to keep working
towards greater contact with families and communities.
This is a right for all people with disabilities, and part of
Australia’s national disability standards.
For the past few years the CVP has commented on the need for greater clinical depth in
developing, implementing and reviewing residents’ positive behaviour support plans (PBSPs).
The CVP’s concerns in this area remain constant.
These concerns are based on the need to move beyond care and compassion in resident
treatment. The service needs to provide clinical support that enables a ‘least restrictive’
approach to care and treatment. This approach helps residents progress to accommodation in
the community with the right supports, without the need for supervision.
“Can you really help me with
[visiting home]? I could give
the little ones a hug.”
C/2017/179
“There’s ceremony there, I
want to go.” C/2016/735

35
Currency and Depth of Plans
The CVP remains concerned about the currency of residents’ PBSPs. The plans have
information on the person’s social history, their likes and dislikes, how to recognise early
warning signs of behaviours, and what responses to behaviours are authorised under the plan.
There is very little detail however about the therapeutic goals for working with the person,
the clinical hypothesis for the person’s behaviours of concern, the ways in which staff will
specifically support the development of alternative behaviours, and how these interventions
will be measured.35 Even though PBSPs have to be reviewed on a yearly basis, there was little
evidence that this occurred in a robust manner.
One of the observations made by the Community Visitors is that staff are often not aware of
the detail of an individual’s plan. Sometimes there is little evidence that general strategies
described in the plan are used. A plan that is not well understood cannot be faithfully
implemented.
It is clear that clinical staff know longer term residents well, having worked with them for years.
This depth of knowledge is not always reflected in updated PBSPs nor updated therapeutic
strategies to address new or emerging needs of residents.
The CVP continues to assert that the PBSPs need to be current, dynamic, more specific and
detailed for the person and their individual circumstances. The PBSPs also need to be
supported by detailed and current functional assessments.
Clinical Support for Transition
Even though a number of long term residents
transitioned into community houses this year, the
PBSPs were not updated to reflect this significant
change. Many of the plans stress the importance
of routine for residents, and yet with such
significant change to a resident’s living situation,
the plans remained silent.
35 In making this statement, the CVP has noted the range of information that is included in policy and procedure
documents for other similar services in Australia (for example, in NSW:
http://www.adhc.nsw.gov.au/sp/delivering_disability_services/behaviour_support_services/behaviour_support_
policy_and_practice_manual; in Victoria: http://www.dhs.vic.gov.au/__data/assets/pdf_file/0003/845346/New-
Toolkit-Section-2-How-to-complete-a-BSP-Planning-Guide-2017.pdf; and in Queensland:
https://www.communities.qld.gov.au/resources/disability/key-projects/positive-behaviour-support/positive-
behaviour-support-plan.pdf). The CVP recognises that the NT service is a smaller service than other Australian
States, nevertheless the scope of a quality positive behaviour support plan would be constant regardless of the
size of the service.

36
Neither the PBSPs nor transition plans reviewed by Community Visitors clearly stated the risks,
behaviours and intervention strategies for residents on transition.
Unfortunately, for some residents who moved into the community, there was a temporary
escalation in the use of restrictive interventions. In the CVP’s view, the lack of planning
increases the risk of behaviours occurring during transition.
For one resident with complex medical needs, there was an exponential increase in the use of
chemical restraint over a period of three months. Following a comprehensive clinical review,
and changes to this person’s management in the community, there was a reduction in
restraints. The resident’s behaviour settled. The success of this intensive clinical work
reinforces the need for detailed clinical planning and support on-site.
For newer residents, there appears to be very limited clinical assessment in preparation for
new clients moving into facilities. Some residents who have been in the disability places now
for some months do not have PBSPs.
The lack of detailed preparation for new
residents, and the lack of planning to enable
staff to manage behaviours that arise, is
concerning. Some residents with limited
planning and support documentation have
returned to prison during transition
periods. This has happened after serious
incidents, usually involving assault of a
support worker.
Individual Review Processes
The CVP understands work in this field is dynamic and unpredictable. Nevertheless, the CVP
has commented for the past three years on the importance of robust individual client review
processes.
Although the Disability Services Act requires a formal review with the person themselves and
their guardian on an annual basis, there was no evidence to show this is a standard practice.
The formal review is an annual requirement. There was also limited evidence of regular,
individual reviews throughout the year.
Such reviews need to be informed by detailed knowledge of client behaviours. Reviews need
to be informed by evidence from planned therapeutic interventions, measured over time.
Reviews need to link to updated or new plans.
For evidence of review processes, the CVP was directed towards minutes of staff meetings,
and emails exchanged between senior staff. These sources were not detailed. The information
was more informal and not stored on individual client records. There was no evidence of
objective measures of client review.

37
There was no clear evidence of structured, individual review processes involving all relevant
people. The CVP has formed the view that there is not enough evidence of robust individual
client review processes. The limited changes to the PBSPs on an annual basis reflect the low
quality of clinical review throughout the year.
Quality Assurance in Clinical Planning
Each year the CVP has noted the importance of the positive behaviour support ‘Review Panel’
as a way to oversight the quality of plans. Section 40 of the Disability Services Act provides this
mechanism as a way to review restrictive interventions in a PBSP.
Until recently, the Office of Disability has taken a narrow view on the legislative scope of this
Review Panel. The CVP maintains that the Panel provides an important way to independently
review PBSPs. If the Review Panel were established, it would be a very useful addition to the
quality assurance framework for residents more generally.
Overall, the CVP notes that the nature of clients transitioning into and living in specialist
disability places are those who present the greatest risk to themselves or others. The greatest
burden of risk is held by the client. The person with a disability is at risk of returning to a more
restrictive environment (for example, prison).
The obligation to support the person to avoid such restriction is with the service. The best
way to meet this obligation is by careful, detailed planning and high quality clinical support and
review. This is an area in which the Office of Disability needs to invest more to ensure quality
care for their clients.
The CVP notes that with the introduction of the National Disability Insurance Scheme (NDIS),
agreement has been reached for a national quality and safeguards framework. The Northern
Territory has agreed to an approach for implementing this framework with local disability
providers.36
In the CVP’s view, the same expectations for a quality service need to apply to the Office of
Disability’s own direct service provision. The CVP notes in particular the requirements for all
disability providers to have person-centred planning, safeguarding of rights, and culturally safe
services.
The CVP has seen a small increase in new residents in the specialist disability residences in the
past year. The number of residents seen by the CVP is around fourteen, however some people
may transition in or out at any point in time.
36 Northern Territory Government, NT Quality and Safeguarding Framework 2016.

38
One of the trends among the new residents is the increasing complexity of residents who are
mutual clients of other agencies. The agencies most relevant are corrections, mental health,
public health, aged care and public guardians.
Some departments have frequent interactions with the Office of Disability (such as the
Department for Corrections). Some residents may be mutual clients of both agencies for many
years.
Age-Related and Mental Health Needs
This year, a small number of residents had
questions raised about the appropriateness of
their placement in residential facilities operated
by the Office of Disability. The use of
residential facilities for people with other needs
presents a significant challenge to the service.
For some residents, the Office of Disability
provides the day to day support, however
other health services are responsible for
treatment and transition out of the facility.
Some clients transitioning into residences have
been identified to the Community Visitors as
needing accommodation and support from an
aged care framework, more than disability
services. There have been delays in organising
appropriate transition arrangements as staff
need to plan for and negotiate more
appropriate aged care support.
Some residents have been in disability
residential facilities for extended periods of
time, even if it was anticipated that they have a
short stay. In some cases, the legal and administration arrangements for such residents have
been complicated and confusing. The CVP has raised these concerns with the service.
Changing Practice Framework
These complex clients moving into specialist residential facilities are on custodial supervision
orders made by the Supreme Court. They are stepping down from prison to the less restrictive
environment of a supervised residence. Corrections staff are often closely involved in
monitoring and the transition and responding to incidents of concern.

39
While the CVP strongly supports ‘least restrictive’ principles and approaches to care, the
original intent of the Secure Care Facility (and other appropriate places managed by the Office
of Disability) is changing in practice.
The Secure Care Facility and other appropriate places run by the Office of Disability are for
clients with a complex cognitive impairment, a disability, and who could benefit from ‘goal-
oriented’ therapeutic services. This is the main expertise and skill set of staff, and the basis on
which policies and programs are delivered.
For clients presenting with complex needs, the primary ‘service’ being offered by the Office of
Disability is supervised accommodation. These clients need for supervision may come from a
mental health and/or age-related impairment, rather than an intellectual disability. This changes
the nature of support being provided and required on transition.
This change needs to be acknowledged and new agreements put in place with other relevant
agencies to better manage the needs of these residents in disability facilities. These agreements
would also assist in avoiding unintended outcomes, such as lengthy transition planning out of
the residences.
Formalising Agreements with Agencies
The CVP is of the view that formal agreements
with agencies who commonly have mutual clients
with the Office of Disability is beneficial.
Streamlined agreements that respond to the
unique needs of both agencies are beneficial for all
concerned, providing safety and support for all
involved.
Agreements with the area health services, in
particular mental health and aged care services, are
needed. It would be useful to formalise agreements with emergency departments, as this can
also be a place where residents’ behaviour can escalate and present risks to all.
Some agencies have a high level of interest in the work of the Office of the Disability, and
would benefit from having agreements in place for communication and information sharing.
The Office of the Public Guardian and the CVP are two such agencies.
The CVP has an existing protocol with the Office of Disability. This was a useful starting point
for clarifying mutual roles and responsibilities. Towards the end of this reporting period, there
has been good progress towards revising and updating this protocol.
The work of the Office of Disability in specialist disability residences has evolved over the past
few years. The complexity of clients has increased. The need for clarity in roles and
responsibilities of other agencies has become more evident.

40
The CVP is of the view that formal agreements will help address the range of needs for clients,
provide improved clarity about each service’s roles and responsibilities, and ensure high quality
and timely care for residents residing in these facilities.
As noted above, in this year, the Community Visitors have seen an increase in the number of
issues raised during their discussions with residents. There are challenges in communication
that come from the nature of people’s disabilities.
For most residents who the CVP visits in specialist
disability places, however, these challenges can be
reduced. One of the most useful ways of doing so is to
communicate in the person’s preferred language.
Unfortunately, the CVP has observed that there has been
very little engagement by the Office of Disability with the
need for independent, accredited interpreters for
residents in their care. When asked directly, the service
responded that interpreters were not regularly used.
The service has directed the CVP towards its recruitment
of multilingual staff as evidence of its commitment to good
communication. While multilingual staff are very important
part of culturally safe client care, these staff are not
independent and trained as interpreters.
The obligation to use interpreters rests with the service,
to communicate fully with residents, understand their
needs and to respond to those needs in a professional
manner.37 When these matters of quality, professional
responsibility for communication were raised with the
service, the CVP found the responses to be disappointing.
Communicating everyday matters in English may work when a resident is very familiar with
routine. Communicating about significant matters with people with a disability, such as
obtaining information to do an assessment, review or debriefing, is another story. The CVP
considers the use of interpreters for such significant conversations as essential and best
practice.38
Within that broader context of hearing and understanding resident needs, the CVP has raised
with the service the importance of having a robust internal complaints system. The Disability
37 Northern Territory Government, NT Health Aboriginal Cultural Security Framework 2016-2026, domain 2
(communication). 38 Australian Government, National Standards for Disability Services, standard 3.
“If the client does not
understand something, it is
more related to cognition
than language, therefore
the language it is delivered
in is not relevant”
(L231116)

41
Services Act requires this to be in place.39 These systems
are not working in the residential facilities.
An internal complaints system, which has a broad
definition of a ‘complaint’ (recognising that the person
has a disability), is a central part of any service. It is
important as part of its commitment to resident
participation and responsiveness, quality assurance and
continuous improvement.40
The Office of Disability requires government funded
disability providers to have such systems in place. It is
critical that the Office of Disability’s own direct services have the same system in place to hear,
understand and respond with integrity to resident concerns. To give residents a voice in their
own care and treatment.
Achievements
o Three recommendations closed
o Recruitment of a more diverse workforce, including Aboriginal and female staff
o Employed an Aboriginal cultural advisor
o Improved incident debriefing and documentation
Areas for Improvement
o Building staff knowledge and skills in the use of accredited interpreters
o Improving processes for individual client review
o Formalising agreements with agencies involved in resident care and treatment
Priority Issues
o Need for on-site clinicians to support management and disability support workers in
their roles
o Finalising procedures related to site safety, risk management (including in houses
managed by SCF group home manager), and robust internal complaints procedures
o Working with mental health services collaboratively to resolve transition of a long
term mental health client out of the facility into more appropriate accommodation
o Ensuring senior level clinical staff attend the next CV Panel visit to enable the Panel
to consider closing or amending recommendations
39 Disability Services Act (NT), Part 5. 40 Australian Government, National Standards for Disability Services, standard 6.

42
CVP Recommendations Made By Date Status
1. That adequate duress alarms for staff and visitors
are installed. (Reworded)
Community
Visitor
May
2013
Open
2. That the service provides the quality assurance framework documentation and process that underpin quality assurance for the Secure Care Facility and appropriate places.
Community
Visitor
Aug
2014
Open
3. That the Positive Behaviour Support Panel be established in accordance with sections 36 and 40 of the Disability Services Act.
Community
Visitor
Aug
2014
Open
4. That Secure Care Facility management and the
Aboriginal Interpreter Service meet to organise an
orientation session for interpreters called to have
language and cultural assistance with the Secure
Care Facility residents.
CV Panel Oct
2014
Open
5. That Secure Care Facility management explore
options for accommodating women within the
facility separate from men.
CV Panel Oct
2014
Open
6. That information available about early childhood of
residents is taken into consideration when Positive
Behaviour Support Plans (PBSP) are established.
CV Panel May
2015
Open
7. That a clear individualised transition plan be
established for each resident at the facility upon
admission, showing steps achieved towards exit.
CV Panel May
2015
Open
8. It is recommended that an on-site clinical role be
filled at the Secure Care Facility. (Reworded)
Community
Visitor
Jul
2015
Open
9. That to ensure proper consideration of biological
and/or psychiatric causes of significant difficult
behaviour incidents, a clear procedure should be
developed for notifying the General Practitioner
and psychiatrists of such incidents and of
subsequent actions taken by both.
CV Panel Jun
2016
Open
10. That the Secure Care Facility update each
resident’s Positive Behaviour Support Plan with a
more detailed therapeutic program of specific and
measurable interventions, including related to
transition. (Reworded)
Community
Visitor
Jul
2016
Open
11. That the Secure Care Facility implement a quality
data analysis and measurement process related to
each client’s therapeutic program, including
improved processes for individual client review.
Community
Visitor
Jul
2016
Open

43
12. That the CVP is notified in a timely way of all new
and transitioning residents in residential facilities
covered by the Disability Services Act, including
being provided with all relevant documentation on
new and transitioning residents.
Community
Visitor
Feb
2017
Open
13. That the Secure Care Facility establish an effective
internal complaints register and report on
complaint handling according to section 49 of the
Disability Services Act.
Community
Visitor
May
2017
Open
14. That the Secure Care Facility establish a register to
record the booking and use of interpreters for
clients.
Community
Visitor
May
2017
Open
Note: Information is very general to protect people’s privacy. There is one house in the community
that is visited by the CVP.
Priority Concerns
o That planning for transition to the National Disability Insurance Scheme is prioritised
to ensure a smooth transition for the resident.
Nil Recommendations

44
Note: Information is very general to protect people’s privacy. In the Top End, there is a facility
near the Darwin Correctional Centre and a house in the community. In Central Australia, there
are three houses in the community.
Achievements
o In the Top End, additional clinician position recruited on-site
o Increase in mentoring and support for disability workers
o Signification reduction in restrictive interventions for some residents
o Some long-term residents have moved to community-based accommodation
Areas for Improvement
o Building staff knowledge and skills in the use of accredited interpreters
o Formalising agreements with agencies involved in resident care and treatment, in
particular the Department of Corrections (especially for transitioning clients)
Priority Concerns
o For the Top End, a better understanding of the legislation in relation to the use of
restrictive interventions is required. The use and recording of restrictive
interventions must relate to a person’s individual PBSP and the actions of staff
employed the Office of Disability.
CVP Recommendations Made By Date Status
1. That the Office of Disability develop a
Memorandum of Understanding with the
Department of Corrections to ensure a
collaborative and ‘least restrictive’ approach to
shared clients.
Community
Visitor
Dec
2016
Open
2. That the Office of Disability improve the review
processes of Positive Behaviour Support Plans
(PBSP) in line with section 39 of the Disability
Services Act and best practice guidelines.
Community
Visitor
Dec
2016
Open
3. That the Office of Disability provide evidence of
the systematic implementation of strategies
described in the Positive Behaviour Support Plans
(PBSP) and evidence-based changes to the PBSPs.
Community
Visitor
Dec
2016
Open

45
In the past year, the AMT evaluation was completed.41 This was
a milestone in the program. The CVP has raised the need for a
robust evaluation throughout the course of the program.
As noted in previous reports, the CVP remains of the view that the most
effective evaluation frameworks are those that are designed and
implemented at the start of a
program.
The Community Visitors continued to observe that
many people in AMT facilities felt safe and were
treated well. These positive comments were made
despite many people not supporting the involuntary
nature of the program.
The CVP maintained a regular schedule of visits as
the AMT program moved towards closure. There
41 PwC Indigenous Consulting and Menzies School of Health Research (January 2017), Evaluation of the Alcohol
Mandatory Treatment Program.
1. Greater use of interpreters, in particular as the majority of people in
AMT facilities have English as an additional language.
2. Consistent attention and focus on the ‘least restrictive’ principle in all
aspects of decision-making.
3. A consistent service for all people in AMT facilities across the Northern
Territory, regardless of the place of admission, with a strong focus on
safety and therapeutic objectives.

46
are inherent risks to client safety that can
arise in such situations, especially as staff
turnover increases and it is difficult to recruit
new staff. It was pleasing to see that despite
the many challenges of the transition
towards closure, safety of people in facilities
was maintained.
Overwhelmingly, people in AMT facilities
who spoke to Community Visitors stated that they did not
wish to be there. The concerns about the involuntary
nature of the AMT program were a frequent theme in
issues raised over the past three years.
The loss of people’s freedom to choose where they lived
and how they engaged with services was deeply felt.
Matters related to the ‘least restrictive alternative’ were
about a quarter of the total AMT issues raised this year.
Often issues were raised on practical
matters, such as access to mobile phones,
shopping and a desire to smoke.
Although sometimes seen as minor, these
concerns are part of daily life and
freedoms. They are about spending time
with family and friends, and making
personal choices that are available to
others in the community.
For people who are smokers, some raised
that it did not make sense for them to be
detained for alcohol misuse and also be
required to give up smoking. This issue
caused a lot of stress and potential
behaviour issues at most of the AMT
facilities.
Sometimes issues were related to cultural
safety or needing more information.
These are discussed later in this chapter in
more detail.

47
Less Cases Raised
The CVP noted that this year there has been a decrease in complaints and enquiries raised
with Community Visitors.42
As the program moved towards closure, the numbers in AMT treatment centres decreased.
There was a decline in residents numbers at some AMT facilities, in particular Katherine and
(for some of the year) Darwin.
Since December 2016 the Katherine Mandatory Assessment Rehabilitation Services had not
admitted any people to their service. Numbers in Darwin also fluctuated throughout the
reporting period.
The CVP also made the decision to reduce the number of visits to AMT treatment centres to
fortnightly (instead of weekly). As residents are in AMT treatment centres for three months,
and in response to capacity and other issues at various points throughout the year, the CVP
extended the visiting timeframe.
The CVP considers that some of the reduction in AMT cases this year may be due to less
frequent visits. A regular visiting service helps the CVP be more accessible. Many people feel
more comfortable raising issues in person, rather than contacting someone for support by
telephone or asking staff of the service. This may be particularly relevant when people have
English as an additional language, such as in AMT facilities.
The vast majority of people affected by the provisions
of the Alcohol Mandatory Treatment Act were
Aboriginal Territorians. It is not surprising therefore
that issues related to cultural safety continued to be a
big feature of the cases raised with the Community
Visitors.
The two most frequently raised issues of this nature
were related to communication (in particular, the use
of interpreters) and people’s need to meet their
cultural obligations.
Access to Interpreters
The Alcohol Mandatory Treatment Act required that a person must receive certain information
in a language that they can adequately communicate in.43 Many people in AMT facilities do not
42 There has been a 30% decrease in cases raised (326 cases were raised in 2015-2016 compared to 228 cases in
this reporting period). 43 Alcohol Mandatory Treatment Act, ss 15(3), 55(3), 116

48
have English as their first language. Access to interpreters is therefore an important part of the
program.
In cases raised with Community Visitors and on visits, the CVP noted times when people did
not understand why they were in the facility. This included what would be happening next
(such as attending AMT Tribunal) and possible outcomes from the assessment.
At times, the Community Visitors observed
that the services may have over-estimated a
person’s level of English required for the
discussion. This is not an uncommon issue for
the provision of health services to someone
with English as an additional language.44
In the CVP’s view, it is essential that the
service discharge its professional and legal
obligation to ensure clear communication.
This may mean booking an interpreter when
there is any doubt about the person’s
language skills.
The CVP has noted throughout the year that accessing interpreters was sometimes difficult.
Interpreters are required to assist with explaining Right Statements, conducting assessments,
at the AMT Tribunal and in treatment centres.
At times, interpreters were not available and the assessment could not be completed within
the required 96 hour timeframe. This resulted in the person being released from an AMT
assessment facility.
To support communication, Rights Statements were produced in an audio book format. These
were available in several commonly spoken languages for the region. The CVP commented on
a number of occasions that certain languages (such as Kriol, Pitjantjatjara and Anmatyerr) were
not available to people in AMT facilities.
The use of audio books to ensure client rights are understood is a positive communication tool.
It was disappointing that these common languages remained absent from the program’s
resources.
44 The Aboriginal Interpreter Service information sheet ‘How to decide if you should work with an interpreter –
Health’ notes that untrained people ‘tend to significantly underestimate the amount of miscommunication that
occurs when communicating with someone for whom English is a second language’. The information sheet further
notes that when an interaction uses ‘specialised language and unfamiliar situation’, there is a greater need for
consideration of an interpreter.

49
The Community Visitors observed that there was greater use of interpreters in AMT
assessment facilities compared to AMT treatment centres.45 Although the context and length
of stay in both facilities is different, there is unlikely to be a significant difference in the
communication capacities of people between the two phases of the program. This suggests
that there was insufficient use of interpreter in AMT treatment centres.
The work of the CVP in the AMT field this year highlights the importance of engaging with the
Aboriginal Interpreter Service to resolve service availability issues, and ensuring resources are
available in all relevant languages.
Cultural Obligations
A consistent issue raised with the Community
Visitors was the need for people in AMT facilities to
meet their cultural obligations. This included
obligations such as participating in or attending
funerals and ‘sorry’ business.
It was clear that staff in AMT assessment facilities
and treatment centres recognised the importance
of cultural obligations. In the main, efforts were
made to work with communities and the person
concerned to identify the details required to
consider leave.
It is very concerning, however, that some requests
to meet cultural obligations were not resolved in a
timely way. Some people reported that they missed
out on funerals.
The CVP raised these concerns with the services
involved. Over the course of the year, some
positive change to address the issues raised was
noted. Nevertheless the Community Visitors
regularly received enquiries or complaints related
to this issue throughout the year.
With such a large number of Aboriginal people in
AMT facilities, the services have an obligation to
ensure that cultural obligations can be met and the
‘least restrictive’ decisions are made in the interests
of the person.
45 As registers of interpreter use were not consistently kept in all AMT facilities, it is not possible to comment
more definitively than this observation.

50
The Alcohol Mandatory Treatment Act was
based on a principle that ‘least restrictive’
decisions are made in relation to each person
affected by the law.46 What is ‘least restrictive’
for one person will not be the same for
another person. The decision must be made
on an individual basis.
As with previous years, the CVP has
continued to express concern that the ‘least
restrictive’ principle was not fully understood
or being applied consistently.
The AMT evaluation report also noted similar
points.47 Building understanding of the ‘least
restrictive’ principle was the responsibility of
the Department of Health.
The CVP offered to participate in a training
workshop to build AMT staff knowledge and
understanding about the ‘least restrictive’
principle. This workshop did not proceed as it
was not seen by the Department of Health as
an ‘action item’ within their area of interest or
expertise to progress.
This year a quarter of the issues that were
raised by people in facilities with Community Visitors were related to the ‘least restrictive’
principle. About half of these cases were resolved, while a quarter were withdrawn.48
Some people in AMT facilities expressed a very limited understanding of the concept of
mandatory treatment. Some raised the issue of discrimination.
46 Alcohol Mandatory Treatment Act, section 6, principles: “The following general principles must be applied by a
person when exercising power or performing a function under this Act: (a) involuntary detention and involuntary
treatment of a person are to be used only as a last resort when less restrictive interventions are not likely to be
effective or sufficient to remediate the risks presented by the person; (b)‘the least restrictive interventions are to
be used when a person is being treated or dealt with under this Act; (c) any interference with the rights and
dignity of a person are to be kept to the minimum necessary”. 47 PwC Indigenous Consulting and Menzies School of Health Research (January 2017), Evaluation of the Alcohol
Mandatory Treatment Program, 24. 48 The analysis of the cases that were withdrawn shows that most of the cases came from the AMT assessment
facilities, and were related to the person not wanting an involuntary treatment order. Those that did come from
AMT treatment centres mostly related to concerns about the decision to make an involuntary residential
treatment order.

51
Some people raised their need to care for others, including children. Or that they had only
come into urban areas recently and were not usually drinking to excess.
Being free in the community is a fundamental human right. When a person’s liberty is removed
for therapeutic purposes, the ‘least restrictive’ decisions for that individual are the guiding
principle.
The CVP recognises that the services and AMT Tribunal have the responsibility to make the
final decision on least restrictive decisions. The CVP respects these decisions.
However, throughout this year, the number of cases relating to the ‘least restrictive’ principle
suggests that people subject to involuntary detention in AMT facilities may not feel fully heard.
In light of the cultural and linguistic diversity of people detained in AMT facilities, this points to
the need for greater attention to ways of listening, hearing and understanding people in
facilities. This is needed so that staff can consider their preferences and work towards decisions
that are the least restrictive and likely to have a therapeutic benefit.
One of the concerning aspects of the AMT program has been the frequency of people
returning through AMT facilities. Some were admitted more than once in a quarter or had
multiple admissions over the course of the program. The AMT evaluation affirmed the high
percentage of people who ‘cycle in and out of the AMT system’.49
The CVP acknowledges that repeated attempts at change are not uncommon when addressing
addictions. The involuntary nature of the AMT program, however, raises ethical issues related
to the restriction of people’s liberty to achieve a therapeutic purpose.
For this reason, the CVP has maintained a close interest in the program model and therapeutic
benefits and has raised this throughout the course of the AMT program.50 The AMT evaluation
acknowledged that the program was attempting to address a complex issue ‘without the
benefit of a comparison model and with insufficient time to develop a sound program logic.’51
The AMT evaluation also found that as a result of some of the flaws in the initial design of the
program, it ‘evolved over time and worked differently in different regions’.52
49 PwC Indigenous Consulting and Menzies School of Health Research (January 2017), Evaluation of the Alcohol
Mandatory Treatment Program, iii. 50 CVP Annual Report, 2014-2015, p 70 and CVP Annual Report, 2015-2016, p46. 51 PwC Indigenous Consulting and Menzies School of Health Research (January 2017), Evaluation of the Alcohol
Mandatory Treatment Program, ii. 52 PwC Indigenous Consulting and Menzies School of Health Research (January 2017), Evaluation of the Alcohol
Mandatory Treatment Program, ii-iii.

52
Inconsistencies across the NT
Over the course of the program, the CVP repeatedly raised issues with the Department of
Health related to the program model of care and treatment. This included regional variations
in the program unrelated to individual or local service needs.
While the AMT program is underpinned by legislation and common policies and procedures,
there remained significant inconsistencies across regions. This lead to inequitable outcomes for
people in AMT treatment facilities based on where they were admitted to the AMT program.
One of the main variations noted in this year’s
visit to AMT facilities was the charging of fees
for people in AMT treatment centres. Although
the Alcohol Mandatory Treatment Act53 allows
treatment providers to charge clients for
‘consumables’, there was inconsistent
application of this provision across the
Northern Territory.
In Darwin, the AMT treatment provider
stopped charging fees in August 2016. People
subject to a mandatory residential treatment order in Alice Springs, however, were required
to pay fees for their mandatory order to stay at the AMT treatment centre.54
In response to concerns raised about fees, the CVP reviewed processes related to informed
consent. In Alice Springs, while people could decline to pay the fees, very few did so. This was
surprising considering that fees were paid out of the person’s Centrelink benefits. The issue of
informed consent was not definitely resolved even after liaising with staff and reviewing
documentation.
The capacity of the AMT treatment providers to make decisions about the charging of fees
appeared to be different. The Alice Springs AMT treatment provider advised the CVP that fees
paid by involuntary clients contributed to the financial sustainability of the program. It is very
concerning that inequitable impacts occurred based on the person’s place of admission.
Robust structures and procedures are necessary to ensure quality care, in particular the safety
of people in facilities. The CVP maintained close attention to safety and risk management, and
53 Alcohol Mandatory Treatment Act, s70. Consumables is defined in this section of the Act to include ‘food,
medication and other consumables’. 54 Most people subject to a mandatory residential treatment order at the Central Australian Aboriginal Alcohol
Programmes Unit (CAAAPU) were charged $175 per week towards their living expenses for the period of the
three month order.

53
raised concerns as needed with the service either through regular reporting or direct liaison
for more urgent matters.
Domestic Violence
Concerns related to domestic violence were
raised in both AMT assessment and treatment
facilities (mostly in the Top End, where there
were greater numbers of people in facilities).
Some people in AMT facilities were either in
relationships or had previous relationships with a
known history of violence.
For the most part the services did recognise these
potential volatile situations and implemented
measures to reduce risks and provide a safe place
for all people in AMT facilities. However, there were some cases raised by the CVP where
people with a known history of domestic violence were in the same facility or recommended
to be in the same facility.
The Northern Territory’s Domestic and Family Violence Act55 states that a person must report
domestic violence to the police if a person has caused or is likely to cause harm to another
person. The services have a duty of care to all people in AMT facilities, to comply with both
the ‘least restrictive’ principle and ensure a safe environment. Specific protocols and policies
to manage these situations were required. As such the CVP raised the need for these with the
relevant services.
Managing Transition to Closure
On 1 September 2017 the Alcohol Mandatory Treatment Act was repealed. Until the Act was
repealed, all AMT services needed to be provided consistent with the legislation.
In May 2017, the CVP was provided with information about how the transition plan would be
implemented. The main focus of the Department of Health’s transition plan was to reduce bed
capacity and to provide for mandatory orders to be varied.
Throughout the transition period, the CVP maintained a strong focus on ensuring that safety
and quality of care was maintained. In general, AMT facilities responded well to the challenges
of transition.
Although this was a stressful time period, with staff numbers changing, the wellbeing and safety
of people in AMT facilities remained a priority. AMT treatment providers continued to conduct
55 Domestic and Family Violence Act, s124A.

54
therapeutic programs, provide medical care where required, and maintained social outings as
much as possible.
Despite this, the CVP noted a lack of communication and unclear planning in the transition
period. The initial plans were changed and sometimes services providers were unaware what
was happening and what was expected. The initial plan focused on the administrative elements
of reducing beds and varying orders.
There was an observed lack of involvement of AMT clinicians. At times, there appeared to be
a lack of client-centred focus. The CVP expressed concerns that the therapeutic needs of the
clients did not seem to be at the forefront of planning.
Questions were raised about ethical and clinical issues related to admitting clients when those
clients would be release shortly afterwards. There were inconsistencies between regions. The
Top End Health Service, based on advice from their clinicians, chose to close their admission
service earlier than the original transition plan. The changing decisions to close one assessment
service and have the other one remain open illustrates a lack of attention to exploring and
resolving such issues in the transition planning process.
The AMT program started in haste. In the CVP’s view, the way in which the program moved
towards closure demonstrated a similar lack of attention to planning.
Statement on Program Closure
The CVP acknowledges that the AMT program has ceased at the time of submitting this report.
The services worked hard to ensure client safety in the transition phase to close the facilities.
Numerous open recommendations were reviewed and closed. In some cases, the service
responded that as the program was known to be ceasing in 2017, there would be no action
taken towards closing the recommendation or item of concern.
Some outstanding open recommendations made
by the CVP could not be closed due to the
significance of the matters. These areas remain as
unresolved and open recommendations. These
open recommendations may inform any relevant
policy development and planning for services in
this field in the future.

55
Achievements
o Eight CVP recommendations closed.
o Aboriginal Liaison Officers were supportive and attentive to people’s needs, in
particular supporting decisions on cultural obligations such as funerals.
o An increase in Community Treatment Orders (CTO) recommendations by the end
of the year, applying the ‘least restrictive’ principle.
o Audio Rights Statements in multiple languages were accessible.
o People often commented that they felt respected by staff and the food was good.
Priority Issues
o There remained issues with people in the facility not being able to challenge the
basis of their detention (that is, the basis of the protective custody event made by
the police).
o There remained inconsistent outcomes in relation to being taken to the facility by
police (some people were detained after three protective custody events as per
the Act, while others received many more before being detained).
o Some people were released hours before the 96 hour assessment timeframe when
it was evident from much earlier that their assessment would not be completed
within the prescribed time.
CVP Recommendations Made By Date Status
Top End Health Service
1. That Assessable Persons with cognitive
impairments of other needs beyond the Darwin
Alcohol Assessment Service’s scope of practice are
referred in a timely and appropriate way.
(Reworded)
Community
Visitor
Mar
2014
Open
2. That protocols be developed in relation to urgent
guardianship applications and referral of
Assessable Persons to NT Aged and Disability
Services.
Community
Visitor
Mar
2015
Open

56
Achievements
o Two CVP recommendations closed.
o The service made positive steps to improve the outdoor area.
o People spoke positively about staff members and their experience at the facility.
o Assessments were completed in a timely manner and peoples were seen by the
AMT Tribunal at the earliest time available.
Priority Issues
o Difficulty recruiting Senior Assessment Clinicians, which led to people not being
admitted to the facility from November 2016.
o Need for an audio Rights Statement in Kriol.
o Need for more clarification of policies when a person is on leave and is
apprehended by the police.
CVP Recommendations Made By Date Status
Department of Health
1. That policies be clarified by Department of Health
regarding the processes to be followed in
situations where Assessable Persons who are
subject to Community Treatment Orders (CTOs)
or Mandatory Residential Treatment Order
(MRTO) leave conditions are apprehended by
police at a significant distance from the relevant
treatment centre.
Community
Visitor
Jul
2015
Open
Top End Health Service
2. That steps be taken to provide an accessible and
appropriate outdoor areas for sole use by MARS
clients.
Community
Visitor
Jul
2015
Open

57
Achievements
o Three CVP recommendations closed.
o Generally there was a good level of attention to booking interpreters for people
requiring one, and the interpreter register was well maintained.
o Positive comments from people in the facility regarding staff
o Staff focused on applying the ‘least restrictive’ principle.
o Calm and effective transition towards closure of the program.
Priority Issues
o Need for audio Rights Statements in Pitjantjatjara and Anmatyerr.
o Shortage of senior clinical staff, with one person acting as both the Senior
Assessment Clinician and the Nurse Manager.
o Issues related to the lack of activities in the facility, with feeling ‘bored’
CVP Recommendations Made By Date Status
Department of Health
1. That the Department of Health develops clear
policies and procedures for management of
Assessable Persons with diagnosed or suspected
cognitive impairment within the Alcohol
Mandatory Treatment Program.
Community
Visitor
Jun
2014
Open

58
Achievements
o Four CVP recommendations closed.
o Participant Advisory Board is available for people in the facility to raise issues of
concern and provide suggestions for Saltbush Mob.
o Saltbush Mob staff have all been trained in P3 (use of force training).
o People who had engaged in the program came back voluntarily to Saltbush Mob to
engage in vocational skills for employment.
o Saltbush Mob recruited a female Therapeutic Counsellor to teach the ‘Footprints’
program to women in the facility.
o High number of Aboriginal staff employed who assisted with cultural liaison.
o Top End Health Services and Saltbush Mob worked together well to address
medical needs. There was a doctor available at least once a week.
o Saltbush improved their process to meet cultural obligations (funerals), and
increased the priority placed on responding to these needs.
o Saltbush Mob adhered to the Department of Health transition plan and continued
to provide therapeutic interventions and supports throughout the transition.
Priority Issues
o Ongoing concerns about the ‘rewards’ program set up by Saltbush Mob, which did
not appear to have the intended motivational impact. This led to some people not
being able to go on outings for a period of weeks.
o Concerns were raised by people in the AMT treatment centre about the shop,
including the cost of items compared to shopping in the community and the loss of
their right to choose where they spent their money.
o Processes for media access to the centre, to ensure people’s rights and privacy are
protected.
o The use of interpreters appeared to be minimal, despite many people speaking
English as an additional language. The CVP raised issues related to the use of
interpreters and its impact on the therapeutic objectives of the program.
o The need for policies to address safety issues specifically relating to issues of
domestic violence.
o Greater attention to the need for ‘least restrictive’ decisions on an individual case-
by-case basis.
CVP Recommendations Made By Date Status
Department of Health
1. The Department of Health reviews the suitability
of the facility for mandatory alcohol treatment,
considering Affected Persons’ potential risk of
suicide/ self-harm.
CV
Panel
Sep
2015
Open

59
2. Policies and procedures regarding tobacco are
reconsidered by Department of Health with a
particular emphasis on their impact on alcohol
rehabilitation.
CV
Panel
Sep
2015
Open
3. The Department of Health provide furniture at the
Centre to enable Affected Persons to store
personal items securely as a matter of priority and
at least one lockable drawer being available for all
Affected Persons.
CV
Panel
Mar
2016
Open
4. That Department of Health review the health care
services provided by other similar types of centres,
such as prisons, detention centres, and residential
mental health facilities to ensure the proper health
care of the affecter person, notwithstanding the
contract arrangements between Department of
Health and Saltbush Mob. That the record being
kept by Department of Health and Saltbush Mob
are adequately maintained and accessible to on-call
doctor or hospital (as the case may be), as well as
the senior Saltbush Mob staff.
CV
Panel
Jun
2016
Open
5. That the Department of Health ensure there are
detailed policies and procedural guidelines for
mandatory alcohol treatment facilities. Such
guidelines must take account of the complexity of
the governance environment, any associated risks
to client safety and risk management, and the
principle of the ‘least restrictive’ treatment and
care in decision-making. (Reworded)
Community
Visitor
Jun
2017
Open
6. If the Northern Territory Government decides to
embark on another alcohol treatment program it
should consider closely the findings and
recommendations to the report56, and put a
proper structure in place to facilitate the best
outcomes for the intended clients. Corporate
knowledge is easily lost when a facility closes, so
efforts should be made to minimise this occurring.
CV
Panel
Jun
2017
Open
Top End Health Service and AMT Treatment Provider
7. Less restrictive interventions are thoroughly and
systematically considered for all affected persons.
CV
Panel
Sep
2015
Open
56 Evaluation of the Alcohol Mandatory Treatment Program, PWC’s Indigenous Consulting with Menzies School
of Health Research January 2017

60
AMT Treatment Provider
8. That the therapeutic programs are reviewed by an
appropriately qualified addiction specialist to
consider and enhance their effectiveness.
CV
Panel
Mar
2016
Open
9. That a safe way of placing coverings on the
windows be explored and implemented as a
matter of priority.
CV
Panel
Mar
2016
Open
10. Saltbush Mob review the arrangement with the
medical practitioner and consider whether it
meets the need of mandatory alcohol treatment
for clients with complex and chronic conditions.
CV
Panel
Jun
2016
Open
11. That consent forms be amended immediately to
remove any references to photographs, and
Saltbush Mob review its policy and consider
whether it is necessary in relation to the services
they had been contracted to provide.
CV
Panel
Apr
2017
Open
12. Equity issues be reviewed in accordance with the
‘least restrictive’ requirement under the legislation
CV
Panel
Apr
2017
Open
Achievements
o Six CVP recommendations closed.
o Improvements to the use and currency of the interpreter register.
o A continued focus on cultural safety as a top priority.
o Regular liaison and interaction with the funded organisation providing aftercare.
o A broad range of activities that people in the facility enjoying participating in.
o Training staff members in contemporary Alcohol and Other Drug resources.

61
Priority Issues
o Lack of theoretical and practical knowledge for staff in key clinical positions,
including skills and knowledge required under section 133 of the Alcohol Mandatory
Treatment Act.
o Need for greater focus on implementing clear treatment plans, with plans accurate
and appropriate for the person’s individual therapeutic needs.
o The Primary Health Care Nurse position was vacant for an extended period.
o Questions regarding the informed consent process for people electing to pay fees
while on a mandatory residential treatment order.
o Ongoing high level of people who abscond, which raises concerns about risks and
how these critical incidents are reported and strategies put in place to reduce the
risks.
CVP Recommendations Made By Date Status
Department of Health
1. That the Senior Treatment Clinician (STC) be
given clear direction by the Department of
Health and Department of Health provide
training to the STC to ensure they are
appropriately qualified and understand their role
according to the AMT Act.
CV
Panel
Oct
2016
Open
Central Australian Health Service
2. That the Department of Health urgently improve
the responsiveness of the referrals of Affected
Persons to Aged Care, Disability Services and for
cognitive assessment so that relevant
assessments can be undertaken whilst an
Affected Person is in treatment at the Treatment
Centre.
Community
Visitor
Jul
2014
Open
3. That urgent attention be given to the availability
of appropriately qualified medical staff at all
times, so that non-medically trained staff are not
being required to make medical decisions.
CV
Panel
Dec
2014
Open
AMT Treatment Provider
4. That the use of interpreters in communicating
client rights, and during treatment, is significantly
increased, and records kept of request for, and
use of, interpreters.
CV
Panel
Sep
2015
Open
5. That the complaints policy is reviewed, and staff
receive training in same
CV
Panel
Apr
2016
Open

62
6. That the record keeping systems are reviewed
and if possible amalgamated into one system.
CV
Panel
Apr
2016
Open
7. That CAAAPU incorporate Department of
Health AMT procedures into the CAAAPU
Treatment Manual and that the Department of
Health and CAAAPU develop clear guidelines for
the reporting and follow up of incidents.
Community
Visitor
Jun
2016
Open
8. That the process and explanation of charging
fees, choice to pay fees and authority of
deductions is clear to clients to ensure that
informed consent is provided.
CV
Panel
Oct
2016
Open
9. That the incident policy is reviewed, and staff
receive training in same.
CV
Panel
May
2017
Open

63
Visit Data
Mental Health Disability Alcohol Mandatory Treatment Other
CAHS TEHS Total
Secure Care
Appropriate Place
Other (DSA)
Total Assessment
(CAHS) Assessment
(TEHS) Treatment (CAAAPU)
Treatment (Saltbush
Mob) Total TOTAL
VISITS 64 86 150 16 13 4 33 51 50 39 31 171 354
Community Visitor 59 81 140 15 13 4 32 51 50 37 29 167 339
Inspection 3 4 7 7
CV Panel 2 1 3 1 1 2 2 4 8
Case (Complaints & Enquiries) Data
CAHS TEHS Total Secure
Care
Appropriate Place
Other (DSA)
Total Assessment
(CAHS) Assessment
(TEHS) Treatment (CAAAPU)
Treatment (Saltbush
Mob) Total Total TOTAL
CASES 106 300 406 21 11 0 32 54 91 26 57 228 8 674
Complaints 7 53 60 2 0 0 2 2 3 2 8 15 0 77
Enquiries 99 247 346 19 11 0 30 52 88 24 49 213 8 597
Cases ‘Raised By’
People/Consumer 84 222 306 16 9 0 25 51 91 20 50 212 2 545
Carer/Relative 8 32 40 0 0 0 0 0 0 0 0 0 2 42
Service Provider/Case Manager
4 25 29 3 2 0 5 3 0 5 7 15 3 52
Nurse/Doctor 9 16 25 0 0 0 0 0 0 1 0 1 1 27
Guardian 1 0 1 2 0 0 2 0 0 0 0 0 0 3
Friend 0 5 5 0 0 0 0 0 0 0 0 0 0 5

64
Case Issues CAHS TEHS Total Secure
Care
Appropriate Place
Other (DSA)
Total Assessment
(CAHS) Assessment
(TEHS) Treatment (CAAAPU)
Treatment (Saltbush
Mob) Total Total TOTAL
ISSUES RAISED 202 566 768 41 20 0 61 119 121 56 103 399 9 1237
Quality of Service Provider
78 218 296 21 10 0 31 45 41 21 53 160 0 487
Assessment & Treatment
10 32 42 1 1 0 2 2 1 4 2 9 0 53
Cultural Safety 12 39 51 5 6 0 11 16 25 5 18 64 0 126
Management Plan 3 18 21 2 1 0 3 3 3 1 5 12 0 36
Activities 5 3 8 1 0 0 1 6 1 0 5 12 0 21
Discharge Planning 14 24 38 3 0 0 3 0 0 2 0 2 0 43
Facilities 1 13 14 0 0 0 0 1 0 1 1 3 0 17
Relationship with Staff
8 26 34 4 0 0 4 1 4 0 5 10 0 48
Aftercare 2 3 5 0 0 0 0 1 0 0 0 1 0 6
Health – Physical / Mental
5 28 33 3 1 0 4 8 1 3 2 14 0 51
Procedures 7 14 21 2 1 0 3 3 2 4 7 16 0 40
Consultation Carers/Consumers
10 15 25 0 0 0 0 1 4 0 1 6 0 31
Other 1 3 4 0 0 0 0 3 0 1 7 11 0 15
Rights 48 114 162 9 0 0 9 25 69 12 23 129 0 300
Least Restrictive Alternative
17 28 45 1 0 0 1 11 64 6 15 96 0 142
Legal 8 18 26 1 0 0 1 3 2 0 3 8 0 35
CV Information on Rights
5 2 7 0 0 0 0 3 0 0 1 4 0 11
Detention/Early Review of Detention
0 6 6 0 0 0 0 2 0 1 0 3 0 9
Community Accommodation
9 2 11 4 0 0 4 0 0 1 1 2 0 17
Respect for Dignity 6 9 15 0 0 0 0 0 0 1 2 3 0 18
Safety 1 20 21 0 0 0 0 2 1 1 1 5 0 26
Voluntary/ Involuntary
2 13 15 0 0 0 0 0 0 1 0 1 0 16
Transport by Police 0 2 2 0 0 0 0 4 0 0 0 4 0 6
Location of Admission
0 10 10 0 0 0 0 0 2 0 0 2 0 12
Other 0 4 4 3 0 0 3 0 0 1 0 1 0 8

65
Information 14 64 78 3 0 0 3 14 4 7 4 29 7 117
Request for information from CVP
5 23 28 3 0 0 3 4 1 3 0 8 0 39
Information Provided
7 27 34 0 0 0 0 9 3 3 1 16 0 50
Other 2 14 16 0 0 0 0 1 0 1 3 5 7 28
Advocacy 40 59 99 5 1 0 6 26 3 10 16 55 2 162
Smoking 7 20 27 0 0 0 0 1 1 0 1 3 0 30
Visit/Support 7 34 41 2 6 0 8 3 2 4 4 13 0 62
Other 2 27 29 0 0 0 0 2 1 2 2 7 0 36
Medication 6 30 36 1 3 0 4 3 0 0 0 3 0 43
Case Issues - Outcomes
CAHS TEHS Total Secure
Care
Appropriate Place
Other (DSA)
Total Assessment
(CAHS) Assessment
(TEHS) Treatment (CAAAPU)
Treatment (Saltbush
Mob) Total Total TOTAL
Resolved 109 248 357 16 13 0 29 56 76 27 44 203 4 593
Ongoing Monitoring 58 30 88 18 7 0 25 27 1 13 6 47 0 160
Not Resolved 7 54 61 2 0 0 2 10 7 1 16 34 0 97
Referred 18 59 77 2 0 0 2 21 9 9 0 39 5 123
Lapsed 2 46 48 0 0 0 0 3 10 3 22 38 0 86
Withdrawn 2 38 40 0 0 0 0 1 18 0 11 30 0 70
Other 2 73 75 3 0 0 3 1 0 3 4 8 0 86
(Open) 4 18 22 0 0 0 0 0 0 0 0 0 0 22

66
We value the voice and opinion of our client group, staff and service
providers by respecting knowledge and expertise, acting courteously at all
times, respecting others’ privacy, being inclusive and ensuring cultural safety.
We walk alongside our clients, seeing the situation from their perspective,
appreciating that all points of view are valid, striving to understand their
journey and maintaining hope at all times.
We provide a robust service to our clients by giving frank comment,
advocating for them, having the courage to communicate an outcome even if
it may not be welcome or well received, and challenging services which are
not respectful of the rights of individuals, including their right to high quality
treatment and standards of care.
We act ethically, openly, honestly and fairly by identifying and avoiding any
conflict of interest, maintaining confidentiality, resolving complaints
impartially and fairly and being accountable.