Embed Size (px)
Citation preview
Communication Strategy
July 2009
HIPS Heath Initiatives
for the Private Sector Project
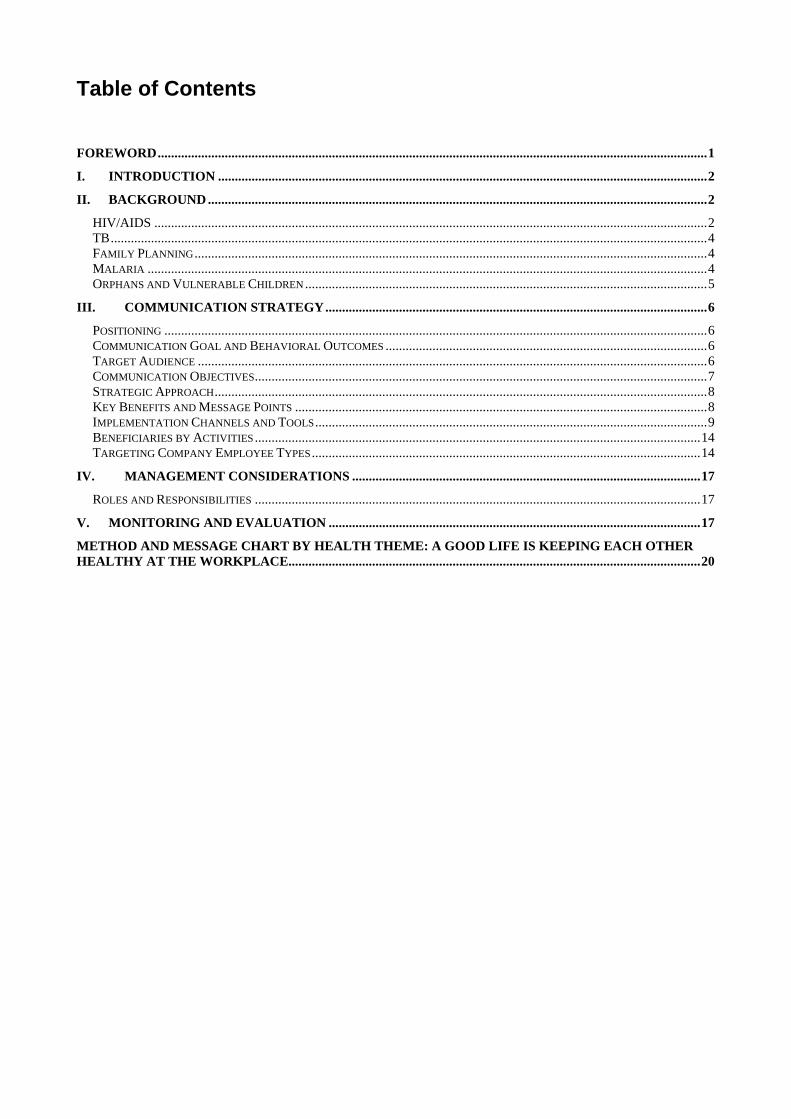
Table of Contents
FOREWORD....................................................................................................................................................................1
I. INTRODUCTION ..................................................................................................................................................2
II. BACKGROUND .....................................................................................................................................................2
HIV/AIDS .....................................................................................................................................................................2 TB..................................................................................................................................................................................4 FAMILY PLANNING.........................................................................................................................................................4 MALARIA .......................................................................................................................................................................4 ORPHANS AND VULNERABLE CHILDREN ........................................................................................................................5
III. COMMUNICATION STRATEGY..................................................................................................................6
POSITIONING ..................................................................................................................................................................6 COMMUNICATION GOAL AND BEHAVIORAL OUTCOMES ................................................................................................6 TARGET AUDIENCE ........................................................................................................................................................6 COMMUNICATION OBJECTIVES.......................................................................................................................................7 STRATEGIC APPROACH...................................................................................................................................................8 KEY BENEFITS AND MESSAGE POINTS ...........................................................................................................................8 IMPLEMENTATION CHANNELS AND TOOLS.....................................................................................................................9 BENEFICIARIES BY ACTIVITIES .....................................................................................................................................14 TARGETING COMPANY EMPLOYEE TYPES....................................................................................................................14
IV. MANAGEMENT CONSIDERATIONS ........................................................................................................17
ROLES AND RESPONSIBILITIES .....................................................................................................................................17
V. MONITORING AND EVALUATION ...............................................................................................................17
METHOD AND MESSAGE CHART BY HEALTH THEME: A GOOD LIFE IS KEEPING EACH OTHER HEALTHY AT THE WORKPLACE...........................................................................................................................20
1
Foreword
This communication strategy is a result of collective efforts of HIPS staff, peer educators, health workers in the private sector, communication specialists and company managers and tries to combine strictly strategic information with information on various terms and methods to make it understandable for people outside the communication field. It spans the entire duration of the Health Initiatives in the Private Sector (HIPS) project. It has been written to guide the work of HIPS communication and service sector staff and partners.
All HIPS activities will be positioned under the Good Life at Work platform. Originally developed by AFFORD/UHMG, the Good Life is an overarching marketing communication platform that links health products, practices and services. It aims to improve self-efficacy of audience members by breaking down health prevention and treatment practices into doable, everyday actions, thereby improving overall quality of life. The overall strategy will promote simple steps one can do every day to keep healthy and save some money, thus getting closer to a good life at work and in the community.
Through the HIPS Good Life at Work Communication Strategy we plan to ensure improved quality of life for employees, their dependants and community members through daily health practices and decisions.
We hope that our stakeholders find this tool useful and that it can become a working document in the best sense of the word.
Barbara Addy
Chief of Party
Health Initiatives for the Private Sector Project
2
I. Introduction Health Initiatives in the Private Sector (HIPS) is a USAID-funded project that works with the Ugandan business community to find cost-effective ways to improve access to and utilization of health services. The HIPS predecessor, Business PART, worked with over 50 companies to develop and implement HIV/AIDS prevention and treatment programs between 2004 and 2007. HIPS expands this approach to include additional health areas, namely family planning, malaria prevention, and TB (as part of HIV/AIDS health maintenance activities). HIPS also addresses orphans and vulnerable children (OVC) in workplace communities. The programmatic goal of HIPS is to increase access to and use of HIV/AIDS, TB RH/FP and malaria services through collaboration with mid- and large size employers with Uganda‘s private sector. In order to achieve this, HIPS has four main tasks:
1. Expand and strengthen access to and utilization of health and HIV/AIDS services in the private sector.
2. Expand the number of Global Development Alliance (GDA) Partnerships. 3. Capacity Building- Support Initiatives to strengthen private sector worker/employer
organizations. 4. Develop innovative and proven approaches to support orphans and other
vulnerable children. HIPS offers Ugandan companies a wide range of options for improving the health of their employees, the employees’ dependants, and other members of the community, including:
Health provider training and service delivery (e.g. HIV testing, AIDS treatment, palliative care, TB diagnosis and care, malaria diagnostics);
Behavior Change Communication (BCC) using peer educator training, community mobilization and outreach, IEC materials adaptation and distribution, and branding of company activities; and
Technical assistance to the Federation of Uganda Employers (FUE) and the Uganda Manufacturers Association (UMA).
HIPS will carry out BCC activities within a comprehensive communication strategy in order to achieve maximum impact. This strategy is laid out in the following chapters.
II. Background In Uganda, HIV/AIDS, TB, malaria, and a high unmet need for family planning present serious health issues for both the public and private sector. Even though messages and activities addressing all four areas have been used for more than 20 years, many social, behavioral and attitudinal barriers still prevail and need to be addressed in evidence-based, innovative and strategic ways.
HIV/AIDS
Prevention Despite strong prevention efforts in previous years1 and an overall high knowledge level among the general population, HIV prevalence rates in Uganda no longer show a
1 Uganda has made impressive progress in reducing HIV prevalence from 18% in the early 1990s to 6.4% in 2005 [Uganda HIV Sero-behavioral Survey (UHSBS) 2004 - 2005 and the Uganda Demographic and Health Survey (UDHS) 2006].

3
downward tendency (2004/05 UHSBS). Rates for men and women aged 15-49 have leveled off at 6.4%. The main risk factors driving the epidemic include high risk sex, extramarital sex in multiple concurrent partnerships, mother to child transmission of HIV, HIV discordance and non-disclosure of HIV status. Interestingly, 66% of all new infections are now estimated to take place within stable relationships2. Forty percent of all who are HIV positive have an HIV negative partner which makes discordant couples and their challenges more common in Uganda than previously expected. Nevertheless, only 25% of women and 21% of men aged 15-49 have ever been tested for HIV and received their results (2006 UDHS). Disclosure of HIV status is rare; an estimated 89% of similarly aged men and women do not know the HIV status of any of their partners (2006 UDHS). While disclosure of test results to partners was described as fairly high in one study (70% in study of 1092 individuals)3 the report also describes high fears of abandonment, abuse and blame as barriers to disclosure. The proportion of women and men with two or more sexual partners has increased to 4% and 29%, respectively, in 2006. Even though condom knowledge is fairly substantial, condoms only seem to be used by half of the population engaged in high risk sex while no more than 29% and 32.6% of women and men, respectively, are using condoms at first sex. These results match with the Business Part KAP/B study (April 2005), which used a series of focus group discussions at four companies to get an impression on HIV/AIDS related knowledge, attitudes and practices. Low testing rates, barriers towards condom use (not for pleasure), multiple partnerships as a norm and lack of condom use in long-term relationships also came out strongly. Stigma, expressed by perceiving people with HIV with a mixture of pity and scorn, was also found to be a barrier to accessing counseling and testing services.
Health Maintenance HIV adult prevalence in Uganda is 6.7%. Over 360,000 people need ARVs, however only 50% of those in need are receiving ARVs. There are 135,000 new HIV infections per year in Uganda (USAID 2009 PEPFAR meeting). Although overall knowledge that ARVs exist is high, just 43% of women and 58% of men had comprehensive or expanded knowledge of ART (UDHS 2006). Moreover, stigma still plays a big role in Uganda; merely 26% of women and 36% of men hold positive attitudes towards PLHA on key stigma indicators (UDHS 2006). Many companies have taken up ART programs themselves. However, since HIV/AIDS affects people in the most productive age groups, more efforts are needed to increase provision of services to workplace beneficiaries – not only in prevention, but also in adherence to ARVs, palliative care, and stigma reduction.
2 “Contrary to the common perception that young people were at the greatest risk of HIV infection, the report shows an unprecedented shift, with 74% of new infection among people above 25 years of age. Only 10% of new infections were recorded among single people during the period of the study.” Ouma, F. (2007) summarizing the results of the 2004/05 Uganda HIV/AIDS Sero-Behaviourial Survey; New Vision (Kampala) 3 July 2007.
3 King et al, 2006: HIV serostatus disclosure to sexual partners of HIV-infected men and women in Uganda
4
TB TB is the leading cause of death among PLHA (30% attributable deaths). TB infection rates have increased due to HIV/AIDS with up to 80,000 new infections every year and a total number of 500,000 TB patients (MOH cited in PLUSNEWS 1/22/08). According to the 2008 Global TB Report (WHO 2008), Uganda has the lowest TB cure rate in the world, at 32%. During 2004 and 2005, Uganda even had the highest number of patients who fail to complete treatment of all countries with large TB burdens (IRIN NEWS 3/27/07). Behavioral include lack of early recognition, diagnosis delay, and the strict treatment adherence requirements over a long period which often lead to non-completion of treatment. Low awareness, low individual and social risk perception, high stigma, and external constraints (e.g. distance, transportation, economic limitations) contribute to delayed care-seeking and diagnosis. Gender differences in care-seeking behaviors are important to understand. TB stigma is wide spread and linked to fears of finding out one’s HIV status (Waisbord without date)4. Limited access to trained health services and drug stock-outs play a role as well. Not only do employers have workers that are co-infected with HIV and TB, but TB alone is a significant cause of employee absenteeism. In many countries workplace programs are increasingly important as first point of contact for detecting and treating TB. Public-private management of DOTS is an innovative way of addressing TB.
Family Planning Uganda is estimated to have one of the fastest growing populations in the world. Meanwhile, modern contraceptive use is stagnating at 18% with rising unmet need, currently among 41% of Ugandan women both for spacing and limiting of birth. As a result the proportion of mistimed and unwanted births increased steadily from 30% in 1995 to 46% in 2006. Today, one out of three mothers would have preferred to wait to have her last child; and more than half have had mistimed or unwanted births. Moreover, the quality of family planning service is deteriorating; the proportion of women citing side effects or other health reasons for not using FP is increasing because they have not been sufficiently informed or counseled. While there seems to be a slight change in the political climate lately, family planning has certainly not been a favorite topic for a long time (Schoemaker 20085). Historically, FP has been viewed as the responsibility of the public sector in Uganda, and private companies have been reluctant to get involved in what is considered to be a sensitive, and less than urgent issue. However, the need for FP services for companies with large numbers of female workers (tea, rice and flower producers) as well as the need for FP among HIV positive couples have been convincing to many Ugandan companies.
Malaria Malaria is the leading cause of illness and death at all ages in Uganda, resulting in a high disease burden and large economic costs to companies in reduced productivity. Malaria currently accounts for 25-40% of all outpatients’ visits at health facilities, 20% of hospital admissions, 9-14% of in-patient deaths, and 23% of deaths among children under 5.
4 Silvio Wasibord: Behavioral barriers in Tuberculosis control: A Literature review. The Change Project. http://one.aed.org/ToolsandPublications/upload/Behavioral%20barriers%20in%20tb%20control%20-%20lit%20review-2.pdf accessed on 4/24/08 5 Family Planning: Uganda’s lame limb in reproductive health, to be published article under peer review based on DHS data.
5
Malaria is also a major reason for miscarriage among pregnant women and a killer of refugees and internally displaced people (MOH online6). It is also known that malaria infections increase the viral load of people living with HIV. Symptoms often become life threatening.
Despite this, malaria is typically not considered severe enough to motivate insecticide treated net (ITN) purchase and use. ITNs are considered to be uncomfortable and their insecticide unsafe for small children, one of many misconceptions. According to the MOH, lack of consistency in availability of first-line drugs, emerging resistance to anti-malarials, and low levels of ITN coverage also continue to hinder achievements of the national-level program indicators. Further, the new treatment policy of the MOH, replacing its previously widely promoted Chloroquine + SP with Artimisinin Combination Therapy (ACT), has not been sufficiently communicated. The workplace is ideal to provide a captive audience to improve needed knowledge, attitudes and skills levels for both employees and providers.
Orphans and Vulnerable Children The situation of Orphans and Vulnerable Children (OVC)7 in Uganda is dire. Of the 15.3 million children under age 18, an estimated 2 million are orphans (2004) of which 45% are orphaned due to AIDS. Only 15.4% of orphans are receiving educational support, 9.7% psychosocial, 5.3% educational and 3.5% receiving food support (2004).8 There is increasing concern that the traditional care system of the extended family is getting overstretched and can no longer bear the responsibility of giving social and economic support. The Ministry of Gender strongly advocates for more resources to set up or sustain a comprehensive network of care and support services for OVCs and their households. These are supposed to help ensure that OVCs can lead meaningful and productive lives while also preventing the further spread of HIV. Nevertheless, as the slightly outdated numbers above are demonstrating, it is hard for the Ministry and support programs to keep track of and identify OVC when they are in need. Workplaces have become involved in the problem mostly through Corporate Social Responsibility Programming. In a survey conducted by the Uganda Manufacturing Association (UMA), 94% of companies surveyed stated that they supported CSR activities in their communities and 80% of the time, these CSR activities were targeted towards or benefited Orphans and Vulnerable Children. There is great opportunity to partner with Uganda Companies to improve the provision of impactful OVC programs, especially in the areas of household income security, education and health. Recently, the idea that company peer educators can play an important role in identifying OVCs in their communities and referring them to needed resources and services has taken hold and attention.
6 Accessed at http://www.health.go.ug/malaria.htm on 3/27/08 7 The term “OVC” is used to refer to children who have been affected and made vulnerable by HIV/AIDS. An orphan is a child under the age of 18 who has lost a mother, father, or both to HIV/AIDS. A vulnerable child is someone under the age of 18 who faces one or many of the following challenges: Having HIV, living without adequate support from adults, living outside of family care, being marginalised, stigmatised, or discriminated against. 8 Ministry of Gender, Labour& Social Development: What is the situation of OVC in Uganda; http://www.mglsd.go.ug/ovc/Indicators.htm accessed on 4/24/08
6
III. Communication Strategy
Positioning All HIPS activities will be positioned under the Good Life at Work platform. Originally developed by AFFORD/UHMG, the Good Life is an overarching marketing communication platform that links health products, practices and services. It aims to improve self-efficacy of audience members by breaking down health prevention and treatment practices into doable, everyday actions, thereby improving overall quality of life. Launched nationwide in April 2006 with The Good Life Show, an innovative entertainment-education game show that aired weekly on television and radio and rolled out in community road shows, the Good Life has shown initial remarkable success. To leverage this existing exposure, HIPS will adapt and implement the concept as the Good Life at Work. The overall strategy will promote simple steps one can do every day to keep healthy and save some money, thus getting closer to a good life at work and in the community. The slogan, “A Good Life is keeping each other healthy at the workplace” shows that if one person at the workplace has, for instance, HIV, the effects reverberate throughout the company and the community. This calls for collective responsibility to support changed behaviors, transformed community norms and utilization of products and services.
Communication Goal and Behavioral Outcomes The goal of the HIPS Good Life at Work Communication Strategy is improved quality of life for employees, their dependants and community members through daily health practices and decisions. Expected outcomes include:
Employees, dependants and other community members using simple steps everyday to protect their health or seek products and services for early treatment.
Employees, dependants and community members believe that staying healthy can
save money and improve their quality of life.
Target Audience The HIPS communication strategy will focus on two primary and two secondary audiences.
1. Primary Audience: a) male and female employees, b) their dependants and other community members, 18 – 45 years old living in semi urban and rural areas, who are currently not consistently preventing HIV/AIDS infection, unwanted birth, TB and malaria regardless of educational level.
The primary audience is usually comprised of people who are at risk of or are suffering from the health problem. Due to the fact that many of the companies have already reached a majority of their employees during the Business Part project with HIV/AIDS activities, a special emphasis is given to employees’ dependants and other community members as primary audience next to employees.
2. Secondary Audience: a) Workplace health providers b) Company and HR
management
7
The secondary audience is formed by people who influence health behaviors of the primary audience either in a positive or negative way. In this case, company related health providers strongly influence the primary audience’s health seeking behaviors while company and HR managers are the gatekeepers to successful and effective programming and implementation.
Communication Objectives The communication objectives below feed into HIPS Program Objective 1. “Expand and strengthen access to and utilization of health and HIV/AIDS services in the private sector.” The objectives are deliberately kept to a realistic level and manageable number as the strategy addresses a multitude of companies with varying conditions. Primary Target Audience: By the end of the project there will be an increase in the proportion of employees, dependants and other community members who: HIV/AIDS and TB
1. Have practical and relevant HIV prevention knowledge including faithfulness, partner reduction, condom use, and male circumcision.
2. Are faithful and/or reduce number of sexual partners and/or use condoms even in long-term relationships unless they know their test results.
3. Get tested for HIV and TB and receive their results (if possible together with their partner to support disclosure).
4. Believe that health maintenance while HIV positive can prolong life and is worth trying or supporting.
5. Know how to recognize TB and that it is treatable.
Malaria 6. Believe that insecticide treated mosquito nets are the best and cheapest way to
prevent malaria for all family members, especially pregnant women, children under 5 and PLHA.
7. Are aware of the dangers of malaria in pregnancy. 8. Go for IPT twice during pregnancy. 9. Know about ACTs, the new effective treatment for malaria. 10. Go for malaria treatment early.
Family Planning
11. Discuss family planning with their partner. 12. Use modern family planning methods including Long Term and Permanent
methods to prevent unwanted pregnancy.
Secondary Target Audience By the end of the project there will be an increase in the proportion of:
1. Company related health service providers who have been briefed with and are actively and correctly using HIPS job aids, support materials and products to better serve their clients.
8
2. Company and HR managers who actively inform staff of and support all Good Life at Work activities at the workplace, in the community and as part of health services they offer.
Strategic Approach The Good Life at Work will combine the following strategies:
1. Merge mutually reinforcing activities into packages tailored to types of companies. 2. Ensure ongoing company/management support through thorough briefing and
engagement in activities. 3. Use peer educators to reach employees, dependants and community members. 4. Address dependants and community members through community outreach using
Good Life entertainment-education (EE) formats. 5. Focus on EE techniques to make peer education trainings and community outreach
more attractive and empower peer educators to use these activities at the workplace.
6. Reinforce motivation and performance of peer educators, clinic providers, companies and adjacent communities through public acknowledgement during Good Life Awards.
7. Make BCC more tangible in providing products together with messages. 8. Provide and train peer educators and providers with job aids and support materials.
Key Benefits and Message Points Communication activities under the Good Life at Work Strategy should use the following key message points to address the three audience segments.
Audience Key Promise Support Statement
Primary Target Audiences Employees, dependants and community
If you follow the simple steps to a Good Life at Work you will keep healthy and save some money. That’s the way to a Good Life!
Because: A Good Life is keeping each other
healthy at the work place. A Good Life is knowing how to prevent
HIV/AIDS. A Good Life is staying strong with
HIV/AIDS. A Good Life is recognizing TB early on. A Good Life is having a small and
manageable family. A Good Life is preventing malaria. A Good Life is treating malaria correctly.
Peer educators If you follow the simple steps to a
Good Life at Work you will be seen as a role model at work and in the community.
Because a Good Life is keeping each other healthy at the work place.
Secondary Target Audiences Company health providers
If you put the Good Life at Work materials and trainings to good use, your clients will appreciate you even more.
Because: A Good Life is keeping each other healthy
at the workplace. A Good Life is knowing how to treat you
clients well. Company managers
If you support the Good Life at Work activities in your company,
Because: A Good Life is keeping each other healthy
9
Audience Key Promise Support Statement you are being a good, responsible corporate citizen and creating a healthy and therefore more productive, profitable workforce.
at the work place. A Good Life is knowing when little steps
can produce big results.
For more complete and detailed messages, please see Message and Method Chart at the end of this document.
Implementation Channels and Tools In order to achieve its communication objectives, the Good Life at Work Strategy will use a mix of activities by means of mutually reinforcing channels. These will include, but are not limited to, Good Life at Work manager briefings, peer education training, workplace activities, community health fairs, Men Only seminars, product promotion, provider trainings, awards, and support materials. Each of these activities is described in more detail below and summarized in a table by audience. 1. Strategic Briefing for Company Managers Company and HR managers will receive a thorough briefing on the set of activities and materials HIPS has to offer using the HIPS Menu of Services (appendix 1). Next to initial meetings and presentations, this will include a binder containing the communication strategy, the communication assessment form, the materials order list, the peer education curriculum and available hand-outs. From these briefings, managers will determine which activities their companies will implement in collaboration with HIPS. Based on the Business KAP/B study, briefings should also include consensus and an action plan on how staff can regularly be informed about HIPS related activities at the workplace. 2. Workplace Policy Development By assisting workplaces to develop and implement an HIV/AIDS, TB, Malaria policy, HIPS helps businesses to formalize a plan of action for fighting the epidemic and protecting the basic human rights of those in the workplace who are infected or affected. 3. Peer Education Peer education provides an opportunity for employees, their dependants, and the community to learn about health issues from people they know and trust, thereby increasing the credibility of the messages and the likelihood that the messages will be heard and internalized. Training and certifying employees as peer educators also serves to boost morale, and build the health education capacity of the company. As such, HIPS will train company employees as peer educators, so that they can conduct activities with co-workers, dependants, and the community. The Good Life at Work training curriculum, adapted from a previous version, uses participatory activities and key messages to improve knowledge, self efficacy and skill levels with regard to HIV/AIDS prevention and care, malaria and family planning, as well as peer education and communication more generally. The training makes health topics exciting by using games and friendly competition to break down preventive health behaviors into simple steps. Teams are formed in the very first session and compete for points throughout the workshop. Points can be won through health or non health related games; for instance, for being on time as a team. This way, all members have a way to contribute to the success of their team, and a positive learning
10
atmosphere can be maintained. Training pretests have already shown increased motivation and participation. Some of the quiz and role play games can also be used in seminars with co-workers or at health fairs. The curriculum’s flexible design is crucial when working with different companies. Because each training module takes half a day (3-4 hours) and can be trained independently, trainings can be organized to meet companies’ scheduling needs. Upon completion of the training, peer educators attend a certification ceremony, where they receive certificates of completion. The certification ceremony publicly acknowledges the peer educators, thereby ensuring that they receive the recognition they deserve, and that co-workers and community members know who their peer educators are.
4. Workplace Sessions During workplace sessions, trained peer educators use Good Life at Work knowledge and skills games with fellow employees to increase health knowledge and skills in an engaging way. Teams can be formed and a prize generated together with company management for the winning team(s). Because sessions are held during the lunch hour, the activity does not interfere with company time. Further, this ensures a captive audience. Companies also have the option of holding workplace sessions at other times throughout the workday. In addition to the games, peer educators can also choose from, show and facilitate discussions around various videos produced by CCP or AFFORD/UHMG:
The Good Life game show episodes on video/DVDs can be used to generate discussion on the different health topics. These 30 minute shows are dubbed in various languages and provide an entertaining “reality TV” alternative to long feature films. Good Life episodes are also used at night shows during Good Life at Work Community Health Fairs.
Trigger Videos are specifically made to generate discussion; peer educators will be trained using a discussion guide on request.
Various FP videos are available together with discussion guides. Men only seminars will be conducted to increase men involvement in FP
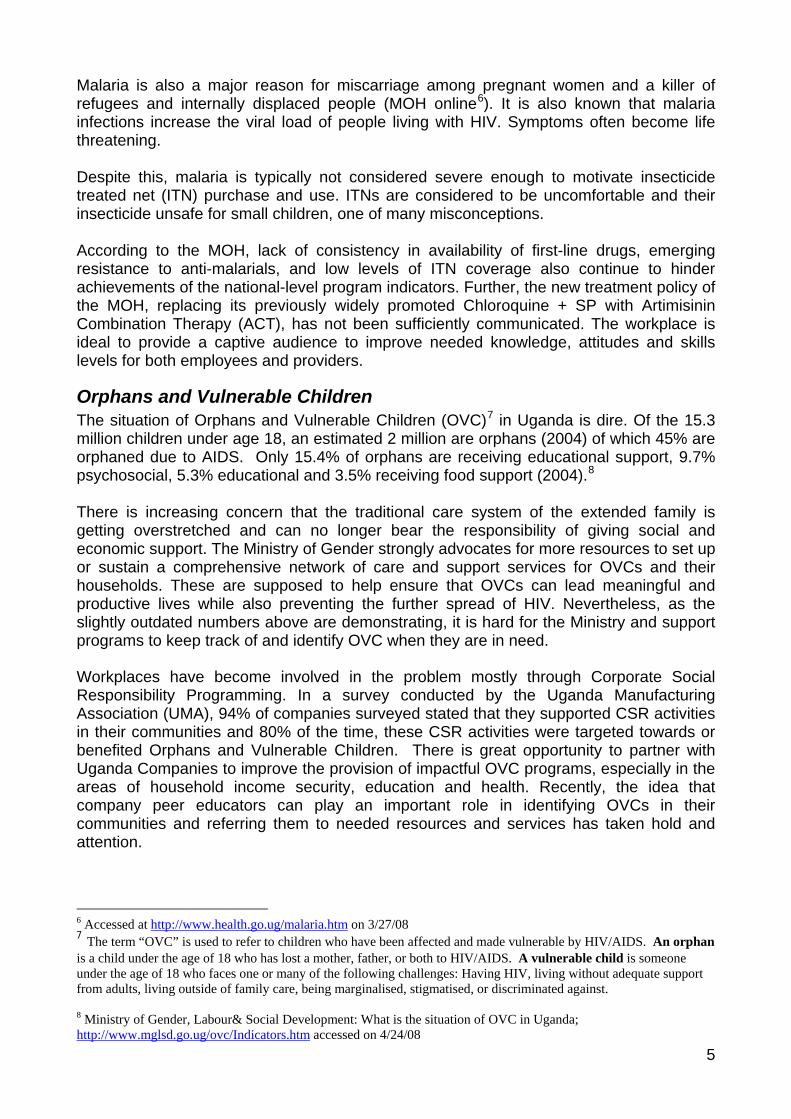
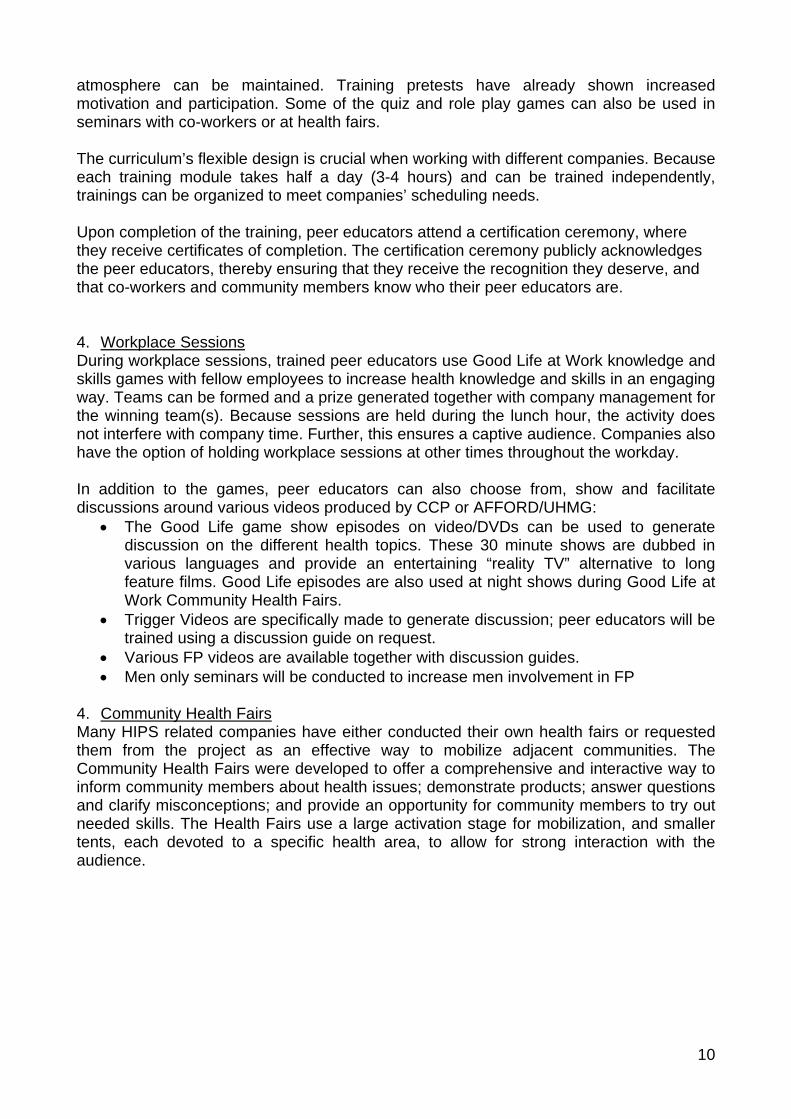
4. Community Health Fairs Many HIPS related companies have either conducted their own health fairs or requested them from the project as an effective way to mobilize adjacent communities. The Community Health Fairs were developed to offer a comprehensive and interactive way to inform community members about health issues; demonstrate products; answer questions and clarify misconceptions; and provide an opportunity for community members to try out needed skills. The Health Fairs use a large activation stage for mobilization, and smaller tents, each devoted to a specific health area, to allow for strong interaction with the audience.
11
T H E H E A L T H M A R K E T I N G I N I T I A T I V ET H E H E A L T H M A R K E T I N G I N I T I A T I V E
Good Life Community Fun Fairs
Activation Stage
HIV
Palliative
Family Planning
Malaria Children’s Tent
VCT
Audience
Shops
HIV Prevention
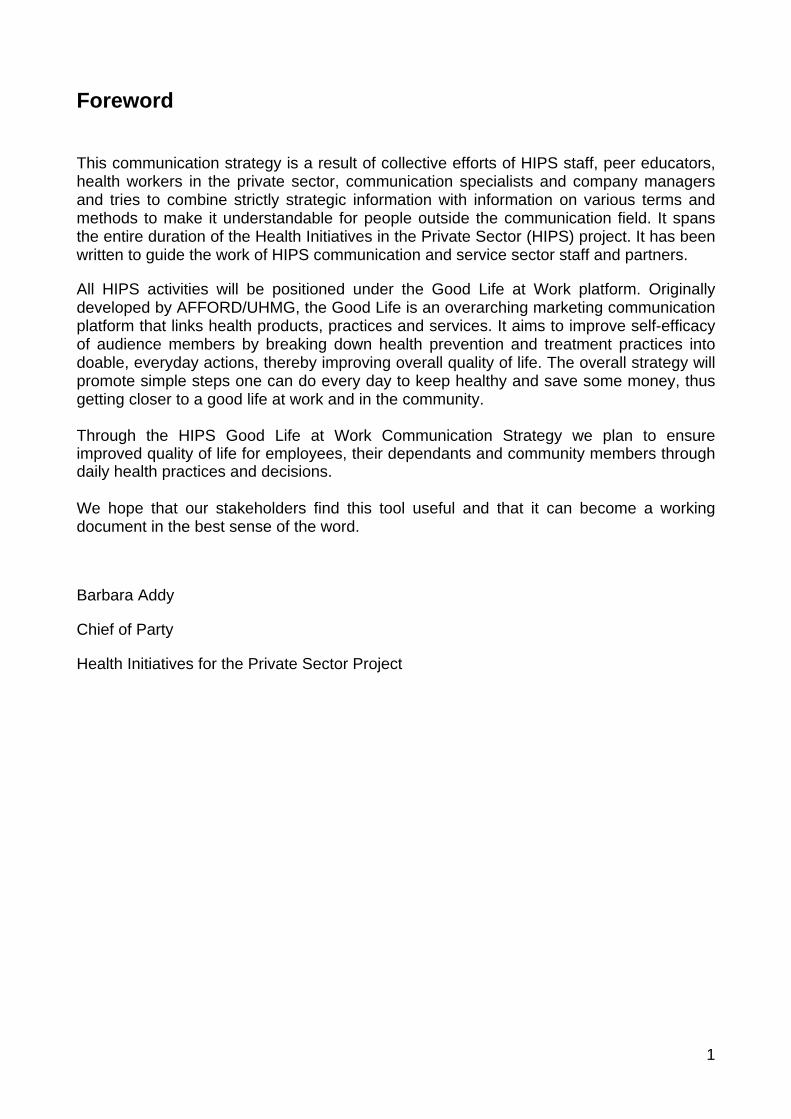
Activities include forum theatre approaches and live game show events on the large stage, and interactive sessions on HIV/AIDS prevention, health maintenance, malaria and family planning in the smaller tents. The concept allows for easy integration of company based HIV counseling and testing services and activities of company or community based drama groups. Health fairs can be all day events and can end with night film shows using the Good Life game show episodes. 5. Good Life Products The Good Life products include a range of prescription and over the counter products socially marketed by AFFORD/UHMG. They represent an integral part of the Good Life at Work strategy based on the observation that behavior change becomes a lot easier when a tangible product can be offered with one’s message. Peer educators, providers and shop owners on the company vicinity will be trained on the correct use of the products and will have promotional materials available. A list of Good Life products by health area can be found on the next page. For easier recognition, all product packaging, detailing and promotional materials are marked with the campaign logo as Good Life Products. They will be made available at clinics and community shops and during the Good Life at Work Health Fairs. 6. Provider Training Service providers linked to workplace clinics will be trained on Good Life at Work job aids, materials and products to be able to improve their services to clients. Trainings will be integrated as much as possible with the clinical trainings performed by Mild may and other partners. HIPS staff will follow up regularly to monitor use and distribution of materials, job aids and products.

12
Health Area Products
HIV/AIDS Prevention
HIV/AIDS Health Maintenance
Family Planning
Malaria Prevention Long Lasting Insecticide Treated Nets
Malaria Treatment Private Sector ACT Brands
13
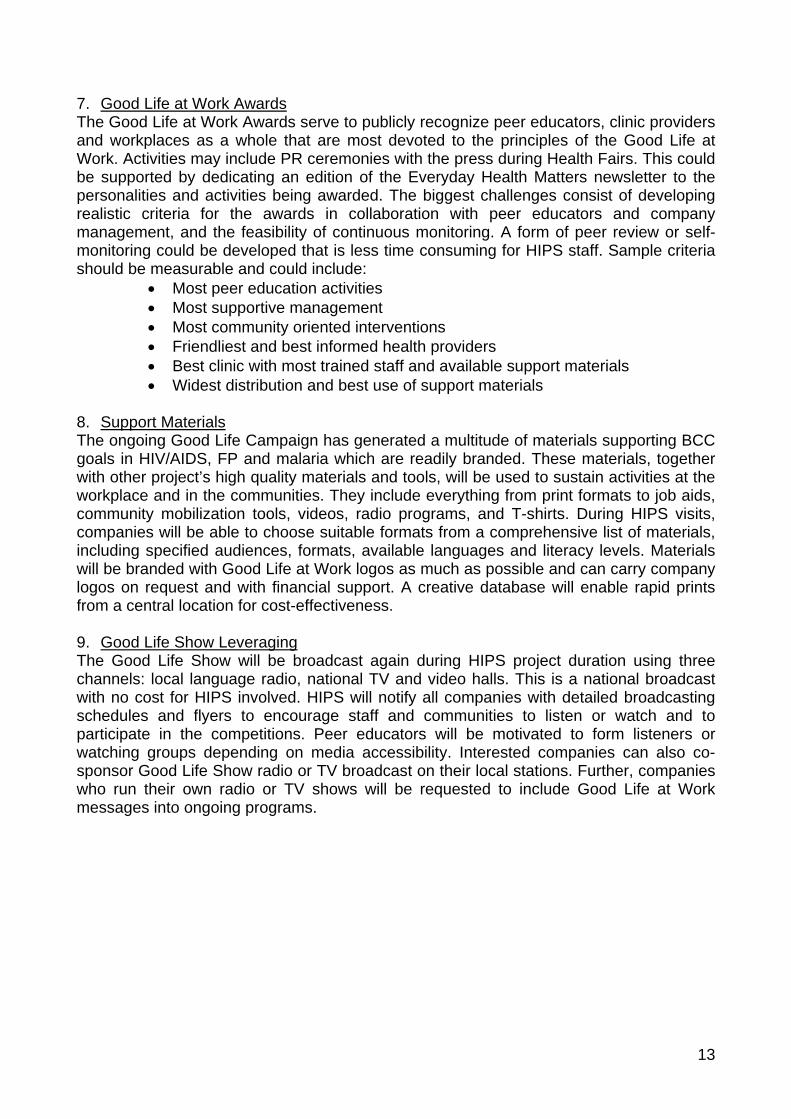
7. Good Life at Work Awards The Good Life at Work Awards serve to publicly recognize peer educators, clinic providers and workplaces as a whole that are most devoted to the principles of the Good Life at Work. Activities may include PR ceremonies with the press during Health Fairs. This could be supported by dedicating an edition of the Everyday Health Matters newsletter to the personalities and activities being awarded. The biggest challenges consist of developing realistic criteria for the awards in collaboration with peer educators and company management, and the feasibility of continuous monitoring. A form of peer review or self-monitoring could be developed that is less time consuming for HIPS staff. Sample criteria should be measurable and could include:
Most peer education activities Most supportive management Most community oriented interventions Friendliest and best informed health providers Best clinic with most trained staff and available support materials Widest distribution and best use of support materials
8. Support Materials The ongoing Good Life Campaign has generated a multitude of materials supporting BCC goals in HIV/AIDS, FP and malaria which are readily branded. These materials, together with other project’s high quality materials and tools, will be used to sustain activities at the workplace and in the communities. They include everything from print formats to job aids, community mobilization tools, videos, radio programs, and T-shirts. During HIPS visits, companies will be able to choose suitable formats from a comprehensive list of materials, including specified audiences, formats, available languages and literacy levels. Materials will be branded with Good Life at Work logos as much as possible and can carry company logos on request and with financial support. A creative database will enable rapid prints from a central location for cost-effectiveness. 9. Good Life Show Leveraging The Good Life Show will be broadcast again during HIPS project duration using three channels: local language radio, national TV and video halls. This is a national broadcast with no cost for HIPS involved. HIPS will notify all companies with detailed broadcasting schedules and flyers to encourage staff and communities to listen or watch and to participate in the competitions. Peer educators will be motivated to form listeners or watching groups depending on media accessibility. Interested companies can also co-sponsor Good Life Show radio or TV broadcast on their local stations. Further, companies who run their own radio or TV shows will be requested to include Good Life at Work messages into ongoing programs.
14
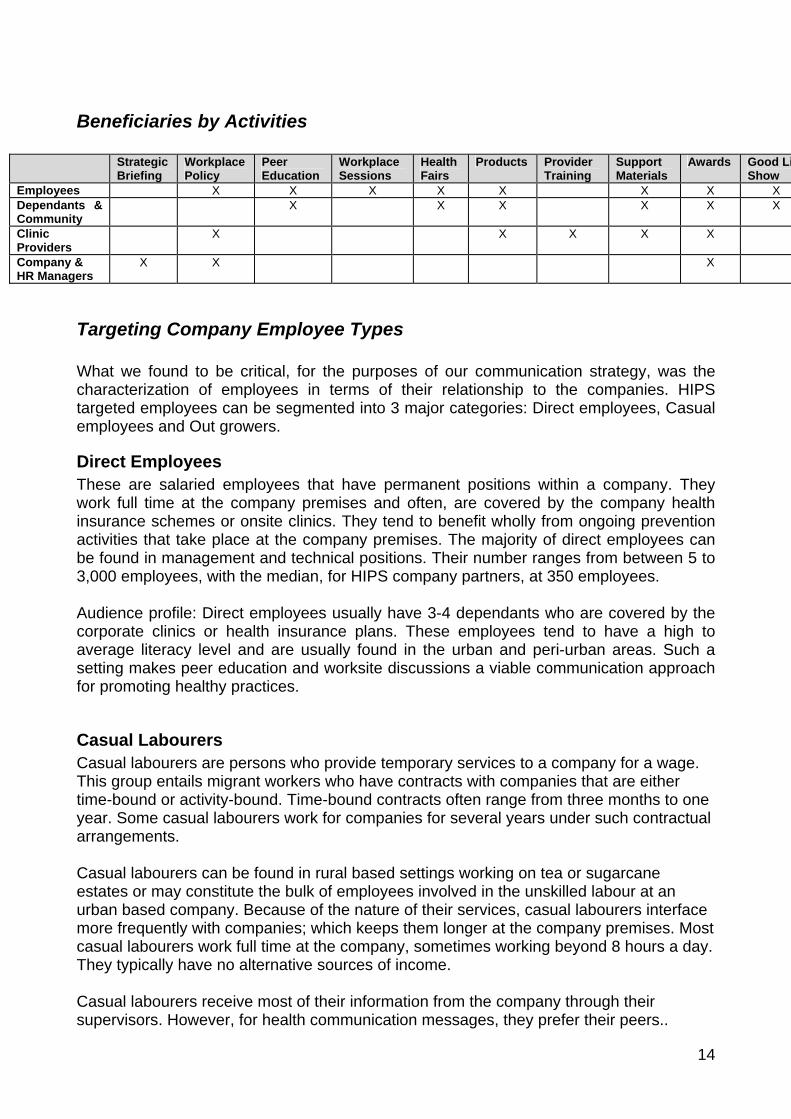
Beneficiaries by Activities
Strategic Briefing
Workplace Policy
Peer Education
Workplace Sessions
Health Fairs
Products Provider Training
Support Materials
Awards Good LiShow
Employees X X X X X X X X Dependants & Community
X X X X X X
Clinic Providers
X X X X X
Company & HR Managers
X X X
Targeting Company Employee Types What we found to be critical, for the purposes of our communication strategy, was the characterization of employees in terms of their relationship to the companies. HIPS targeted employees can be segmented into 3 major categories: Direct employees, Casual employees and Out growers.
Direct Employees These are salaried employees that have permanent positions within a company. They work full time at the company premises and often, are covered by the company health insurance schemes or onsite clinics. They tend to benefit wholly from ongoing prevention activities that take place at the company premises. The majority of direct employees can be found in management and technical positions. Their number ranges from between 5 to 3,000 employees, with the median, for HIPS company partners, at 350 employees. Audience profile: Direct employees usually have 3-4 dependants who are covered by the corporate clinics or health insurance plans. These employees tend to have a high to average literacy level and are usually found in the urban and peri-urban areas. Such a setting makes peer education and worksite discussions a viable communication approach for promoting healthy practices.
Casual Labourers Casual labourers are persons who provide temporary services to a company for a wage. This group entails migrant workers who have contracts with companies that are either time-bound or activity-bound. Time-bound contracts often range from three months to one year. Some casual labourers work for companies for several years under such contractual arrangements. Casual labourers can be found in rural based settings working on tea or sugarcane estates or may constitute the bulk of employees involved in the unskilled labour at an urban based company. Because of the nature of their services, casual labourers interface more frequently with companies; which keeps them longer at the company premises. Most casual labourers work full time at the company, sometimes working beyond 8 hours a day. They typically have no alternative sources of income. Casual labourers receive most of their information from the company through their supervisors. However, for health communication messages, they prefer their peers..
15
Casual labourers have access to and do use radio as a major source of information as it uses local language. Following radio, community meetings and direct word of mouth are the most preferred methods of communication. Medical or health personnel are a highly trusted source for health-related information. Peers and village health teams are also recommended channels of communication. Casual labourers are often members of local area career-related associations, like the ‘sugar cane cutting association’, ‘flower pickers association’, or ‘truck loaders association’, but are not likely to be members of associations within the communities they hail from. Additionally, employees are often migrant workers with two families; one on the estate and one "back home." Considerable peer pressure exists that a man needs to have more than one woman. Poverty levels among their dependants and the surrounding community are high. Their number of casual labourers ranges from anywhere between 1 to 10,000 employees, with the median, for HIPS partner companies, at 800 employees.
Out growers Out growers are defined as persons providing a produce input to a company, typically cotton ginneries, coffee buyers or sugar plantations. Out growers usually have their own land and often form associations that the companies then buy from. These types of out growers sometimes outsource the services of casual workers to pick their crop. They also buy from smaller out growers and sell to the companies. Another type of out growers are those that are typically contracted by the company, often on an annual basis, if the company contributes to the production of the crop. The contribution can be through helping to clear the land with tractors and readying it for planting or providing seeds and pesticides. Out growers that provide their own agricultural inputs are not likely to be bound by a contract. They also often have alternative sources of income and trade. Out growers’ interface with the company is usually only when bringing the supply or clearing land for planting. They normally supply the produce on a daily basis, while payment is done fortnightly. When dealing with companies, they operate mostly through their associations or middle men. These structures are an effective resource for mobilization, as well as a good forum to facilitate linkages between the companies and out growers. Radio is the most used source of information, as it uses local language and can be accessed any time. This makes community radio discussions using pre recorded sessions a viable approach to dissemination of health messages in this target group. Following radio, community meetings and direct word of mouth are the most preferred methods of communication. Community meetings are more likely to be attended when they are organized during times of less work at the farms, such as off-peak season. Medical or health personnel are the most trusted source for health-related information, while peers and village health teams are also recommended channels of communication. While outgrowers are usually aware of the health services offered by their employers, the services are less accessible to outgrowers than to casual labourers.
16
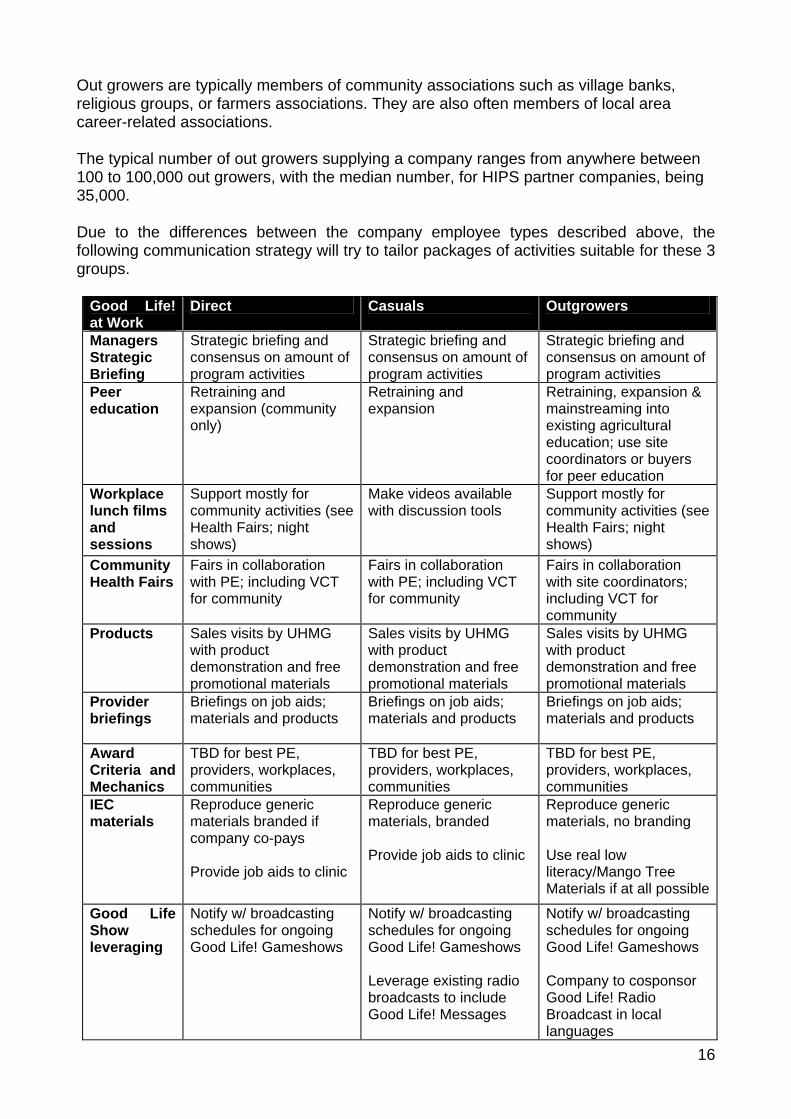
Out growers are typically members of community associations such as village banks, religious groups, or farmers associations. They are also often members of local area career-related associations. The typical number of out growers supplying a company ranges from anywhere between 100 to 100,000 out growers, with the median number, for HIPS partner companies, being 35,000. Due to the differences between the company employee types described above, the following communication strategy will try to tailor packages of activities suitable for these 3 groups.
Good Life! at Work
Direct Casuals Outgrowers
Managers Strategic Briefing
Strategic briefing and consensus on amount of program activities
Strategic briefing and consensus on amount of program activities
Strategic briefing and consensus on amount of program activities
Peer education
Retraining and expansion (community only)
Retraining and expansion
Retraining, expansion & mainstreaming into existing agricultural education; use site coordinators or buyers for peer education
Workplace lunch films and sessions
Support mostly for community activities (see Health Fairs; night shows)
Make videos available with discussion tools
Support mostly for community activities (see Health Fairs; night shows)
Community Health Fairs
Fairs in collaboration with PE; including VCT for community
Fairs in collaboration with PE; including VCT for community
Fairs in collaboration with site coordinators; including VCT for community
Products Sales visits by UHMG with product demonstration and free promotional materials
Sales visits by UHMG with product demonstration and free promotional materials
Sales visits by UHMG with product demonstration and free promotional materials
Provider briefings
Briefings on job aids; materials and products
Briefings on job aids; materials and products
Briefings on job aids; materials and products
Award Criteria and Mechanics
TBD for best PE, providers, workplaces, communities
TBD for best PE, providers, workplaces, communities
TBD for best PE, providers, workplaces, communities
IEC materials
Reproduce generic materials branded if company co-pays Provide job aids to clinic
Reproduce generic materials, branded Provide job aids to clinic
Reproduce generic materials, no branding Use real low literacy/Mango Tree Materials if at all possible
Good Life Show leveraging
Notify w/ broadcasting schedules for ongoing Good Life! Gameshows
Notify w/ broadcasting schedules for ongoing Good Life! Gameshows Leverage existing radio broadcasts to include Good Life! Messages
Notify w/ broadcasting schedules for ongoing Good Life! Gameshows Company to cosponsor Good Life! Radio Broadcast in local languages
17
IV. Management Considerations
Roles and Responsibilities Key implementers of the Good Life at Work strategy are seconded staff of HIPS partner CCP, notably the BCC coordinator, trainer and community mobilizer. The dedicated UHMG person will mainly support product promotion and distribution, but also peer education training and setting up and monitoring of the Good Life at Work Health Fairs and Awards. HIPS partner Mildmay will be responsible to train providers on selected job aids, while HIIPS services staff will help monitor IEC material availability at company clinics. The UPMA/FUE coordinator will work in close collaboration with the BCC coordinator in order to provide TA with regard to Good Life at Work tools, training, and activities.
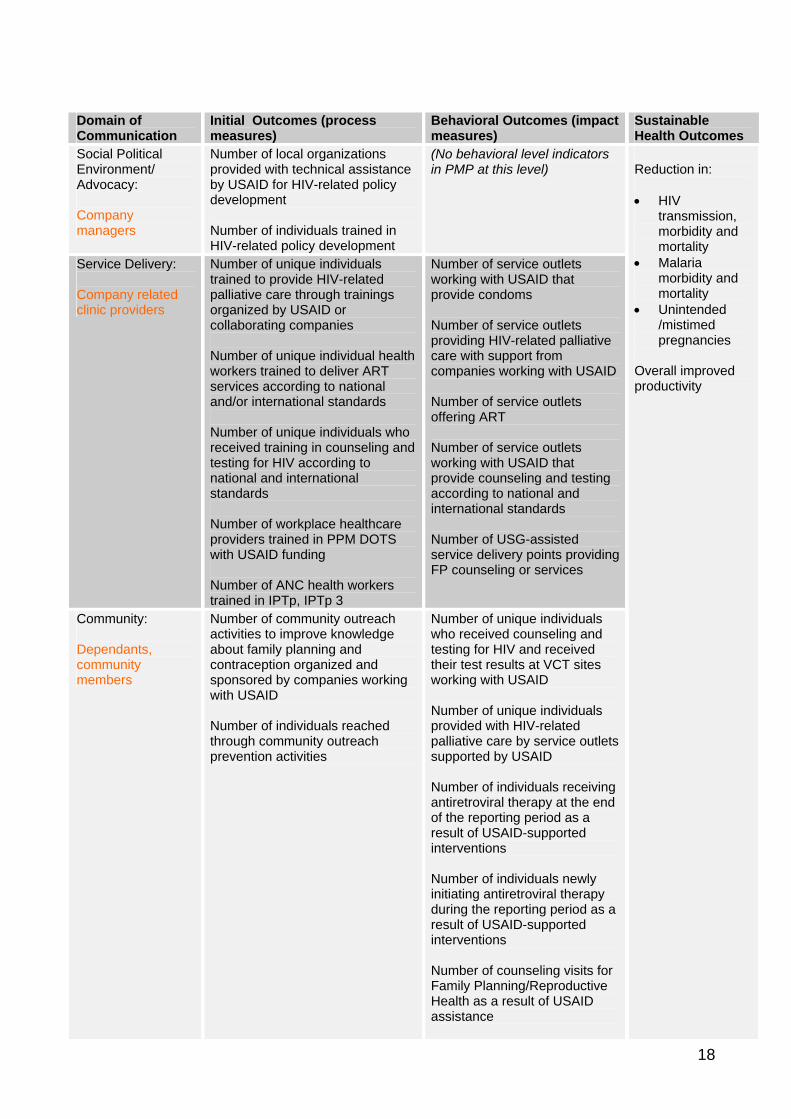
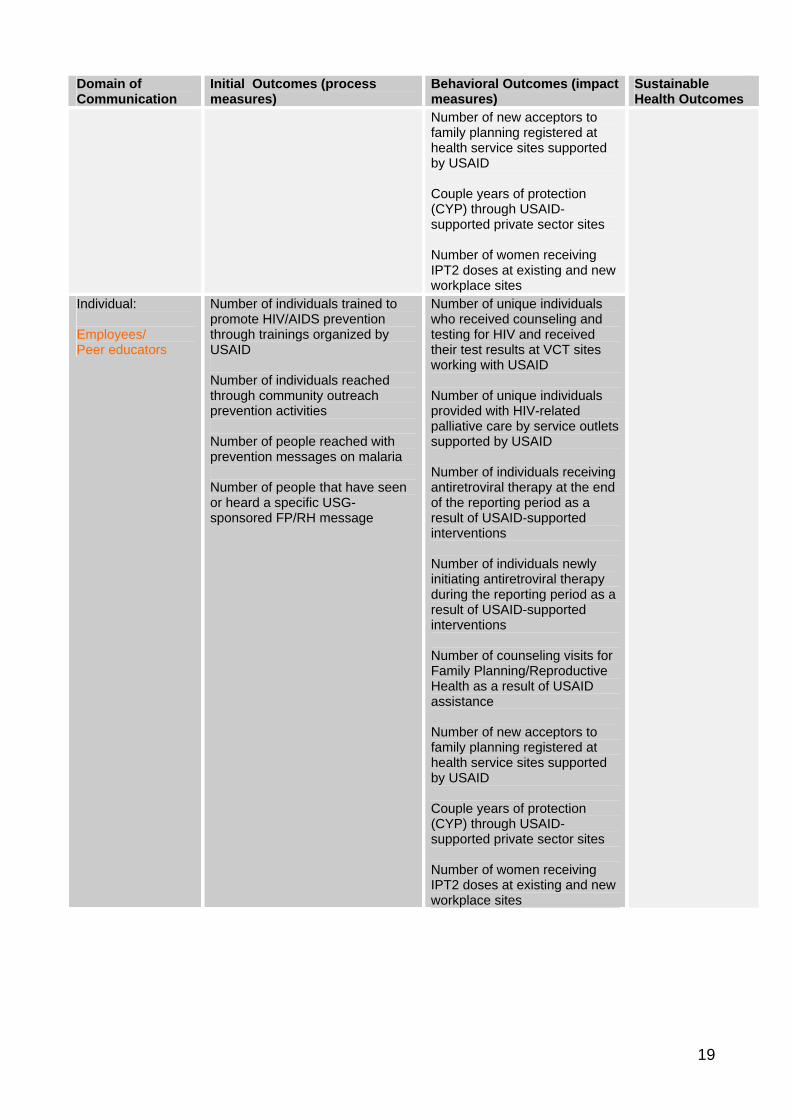
V. Monitoring and Evaluation The table below highlights the applicable communication-related HIPS PMP indicators. The table is organized according to the Pathways to a Health Competent Society9 conceptual model, which integrates all levels related to an individual’s capacity to change: Social Political Environment/Advocacy, Service Delivery, Community, and Individual. This table should be used to measure progress and impact of the activities outlined in this strategy.
9 Developed by the Health Communication Partnership
18
Domain of Communication
Initial Outcomes (process measures)
Behavioral Outcomes (impact measures)
Sustainable Health Outcomes
Social Political Environment/ Advocacy: Company managers
Number of local organizations provided with technical assistance by USAID for HIV-related policy development Number of individuals trained in HIV-related policy development
(No behavioral level indicators in PMP at this level)
Service Delivery: Company related clinic providers
Number of unique individuals trained to provide HIV-related palliative care through trainings organized by USAID or collaborating companies Number of unique individual health workers trained to deliver ART services according to national and/or international standards Number of unique individuals who received training in counseling and testing for HIV according to national and international standards Number of workplace healthcare providers trained in PPM DOTS with USAID funding Number of ANC health workers trained in IPTp, IPTp 3
Number of service outlets working with USAID that provide condoms Number of service outlets providing HIV-related palliative care with support from companies working with USAID Number of service outlets offering ART Number of service outlets working with USAID that provide counseling and testing according to national and international standards Number of USG-assisted service delivery points providing FP counseling or services
Community: Dependants, community members
Number of community outreach activities to improve knowledge about family planning and contraception organized and sponsored by companies working with USAID Number of individuals reached through community outreach prevention activities
Number of unique individuals who received counseling and testing for HIV and received their test results at VCT sites working with USAID Number of unique individuals provided with HIV-related palliative care by service outlets supported by USAID Number of individuals receiving antiretroviral therapy at the end of the reporting period as a result of USAID-supported interventions Number of individuals newly initiating antiretroviral therapy during the reporting period as a result of USAID-supported interventions Number of counseling visits for Family Planning/Reproductive Health as a result of USAID assistance
Reduction in: HIV
transmission, morbidity and mortality
Malaria morbidity and mortality
Unintended /mistimed pregnancies
Overall improved productivity
19
Domain of Communication
Initial Outcomes (process measures)
Behavioral Outcomes (impact measures)
Sustainable Health Outcomes
Number of new acceptors to family planning registered at health service sites supported by USAID Couple years of protection (CYP) through USAID-supported private sector sites Number of women receiving IPT2 doses at existing and new workplace sites
Individual: Employees/ Peer educators
Number of individuals trained to promote HIV/AIDS prevention through trainings organized by USAID Number of individuals reached through community outreach prevention activities Number of people reached with prevention messages on malaria Number of people that have seen or heard a specific USG-sponsored FP/RH message
Number of unique individuals who received counseling and testing for HIV and received their test results at VCT sites working with USAID Number of unique individuals provided with HIV-related palliative care by service outlets supported by USAID Number of individuals receiving antiretroviral therapy at the end of the reporting period as a result of USAID-supported interventions Number of individuals newly initiating antiretroviral therapy during the reporting period as a result of USAID-supported interventions Number of counseling visits for Family Planning/Reproductive Health as a result of USAID assistance Number of new acceptors to family planning registered at health service sites supported by USAID Couple years of protection (CYP) through USAID-supported private sector sites Number of women receiving IPT2 doses at existing and new workplace sites
20
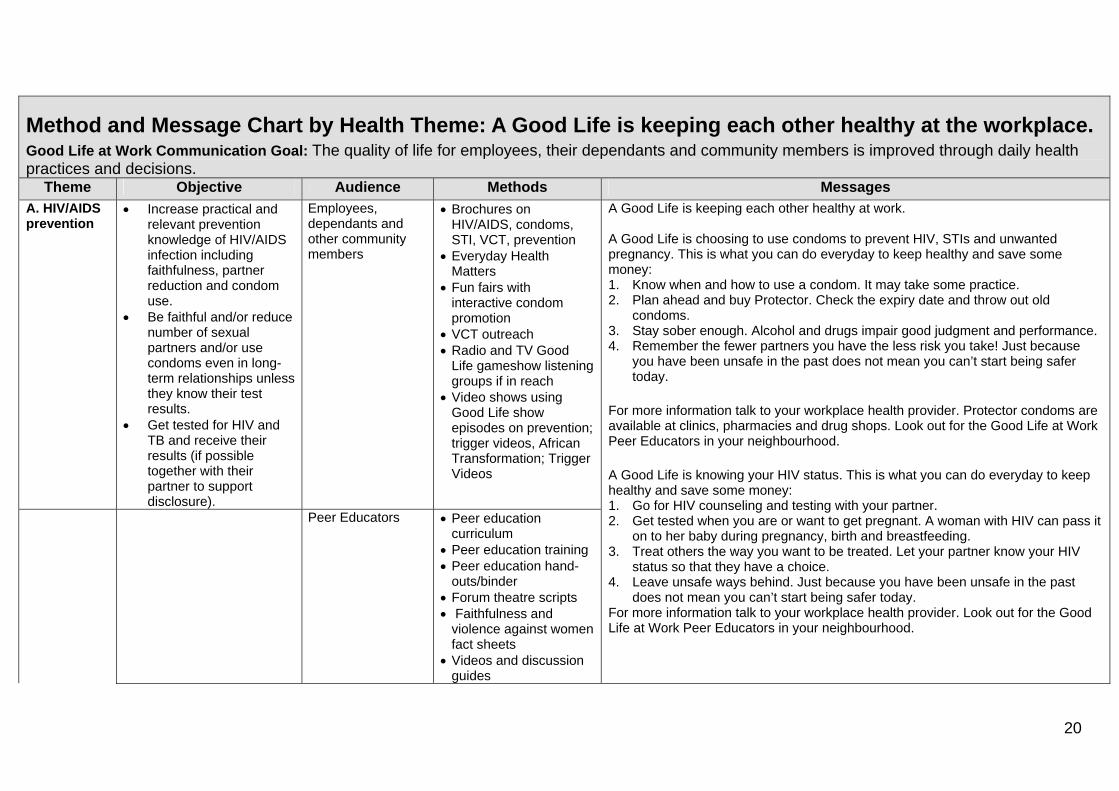
Method and Message Chart by Health Theme: A Good Life is keeping each other healthy at the workplace. Good Life at Work Communication Goal: The quality of life for employees, their dependants and community members is improved through daily health practices and decisions.
Theme Objective Audience Methods Messages
A. HIV/AIDS prevention
Increase practical and relevant prevention knowledge of HIV/AIDS infection including faithfulness, partner reduction and condom use.
Be faithful and/or reduce number of sexual partners and/or use condoms even in long-term relationships unless they know their test results.
Get tested for HIV and TB and receive their results (if possible together with their partner to support disclosure).
Employees, dependants and other community members
Brochures on HIV/AIDS, condoms, STI, VCT, prevention
Everyday Health Matters
Fun fairs with interactive condom promotion
VCT outreach Radio and TV Good
Life gameshow listening groups if in reach
Video shows using Good Life show episodes on prevention; trigger videos, African Transformation; Trigger Videos
Peer Educators Peer education curriculum
Peer education training Peer education hand-
outs/binder Forum theatre scripts Faithfulness and
violence against women fact sheets
Videos and discussion guides
A Good Life is keeping each other healthy at work. A Good Life is choosing to use condoms to prevent HIV, STIs and unwanted pregnancy. This is what you can do everyday to keep healthy and save some money: 1. Know when and how to use a condom. It may take some practice. 2. Plan ahead and buy Protector. Check the expiry date and throw out old
condoms. 3. Stay sober enough. Alcohol and drugs impair good judgment and performance. 4. Remember the fewer partners you have the less risk you take! Just because
you have been unsafe in the past does not mean you can’t start being safer today.
For more information talk to your workplace health provider. Protector condoms are available at clinics, pharmacies and drug shops. Look out for the Good Life at Work Peer Educators in your neighbourhood.
A Good Life is knowing your HIV status. This is what you can do everyday to keep healthy and save some money: 1. Go for HIV counseling and testing with your partner. 2. Get tested when you are or want to get pregnant. A woman with HIV can pass it
on to her baby during pregnancy, birth and breastfeeding. 3. Treat others the way you want to be treated. Let your partner know your HIV
status so that they have a choice. 4. Leave unsafe ways behind. Just because you have been unsafe in the past
does not mean you can’t start being safer today. For more information talk to your workplace health provider. Look out for the Good Life at Work Peer Educators in your neighbourhood.
21
Method and Message Chart by Health Theme: A Good Life is keeping each other healthy at the workplace. Good Life at Work Communication Goal: The quality of life for employees, their dependants and community members is improved through daily health practices and decisions.
Theme Objective Audience Methods Messages
Games sheets
Actively and correctly use HIPS job aids, support materials and products to serve their clients better.
Providers HCT flipchart STI job aid
A Good Life Is keeping each other healthy at work. Or A Good Life is knowing how to treat your clients well.
Actively support all Good Life at Work activities at the workplace, in the community and as part of health services they offer.
Company managers
Briefing binder A Good Life is keeping each other healthy at the work place. or A Good Life is knowing when little steps can produce big results
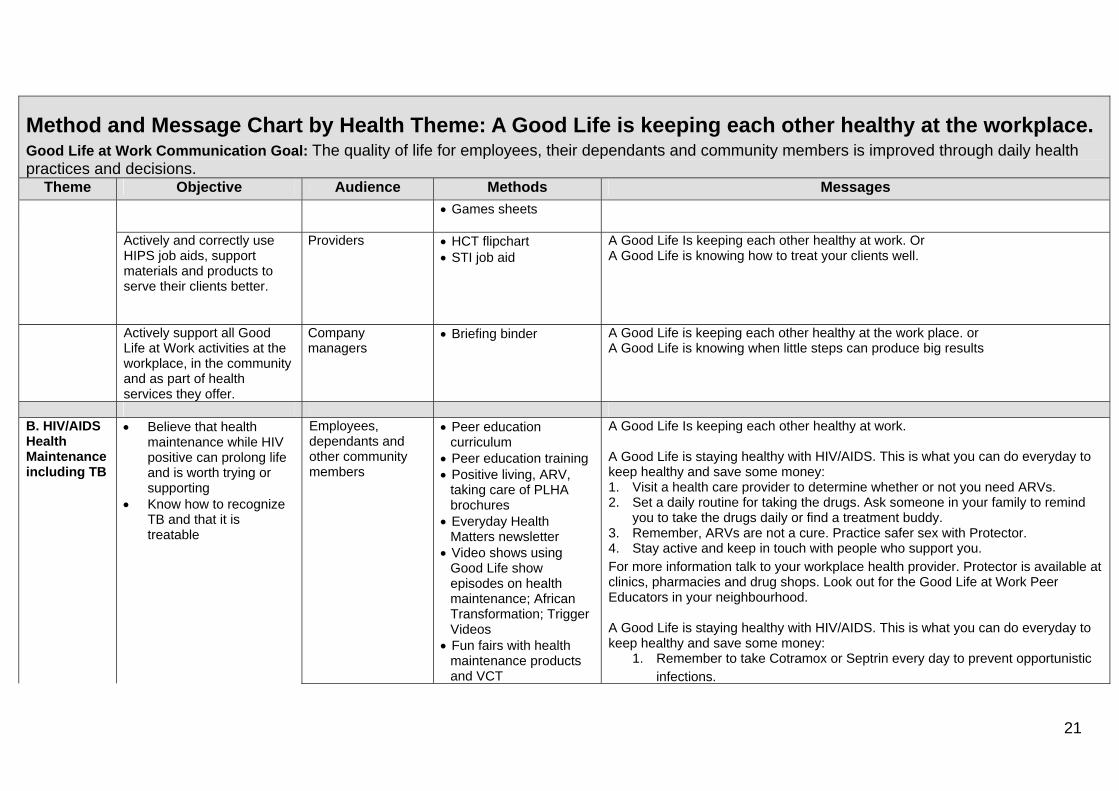
B. HIV/AIDS Health Maintenance including TB
Believe that health maintenance while HIV positive can prolong life and is worth trying or supporting
Know how to recognize TB and that it is treatable
Employees, dependants and other community members
Peer education curriculum
Peer education training Positive living, ARV,
taking care of PLHA brochures
Everyday Health Matters newsletter
Video shows using Good Life show episodes on health maintenance; African Transformation; Trigger Videos
Fun fairs with health maintenance products and VCT
A Good Life Is keeping each other healthy at work. A Good Life is staying healthy with HIV/AIDS. This is what you can do everyday to keep healthy and save some money: 1. Visit a health care provider to determine whether or not you need ARVs. 2. Set a daily routine for taking the drugs. Ask someone in your family to remind
you to take the drugs daily or find a treatment buddy. 3. Remember, ARVs are not a cure. Practice safer sex with Protector. 4. Stay active and keep in touch with people who support you. For more information talk to your workplace health provider. Protector is available at clinics, pharmacies and drug shops. Look out for the Good Life at Work Peer Educators in your neighbourhood. A Good Life is staying healthy with HIV/AIDS. This is what you can do everyday to keep healthy and save some money:
1. Remember to take Cotramox or Septrin every day to prevent opportunistic infections.
22
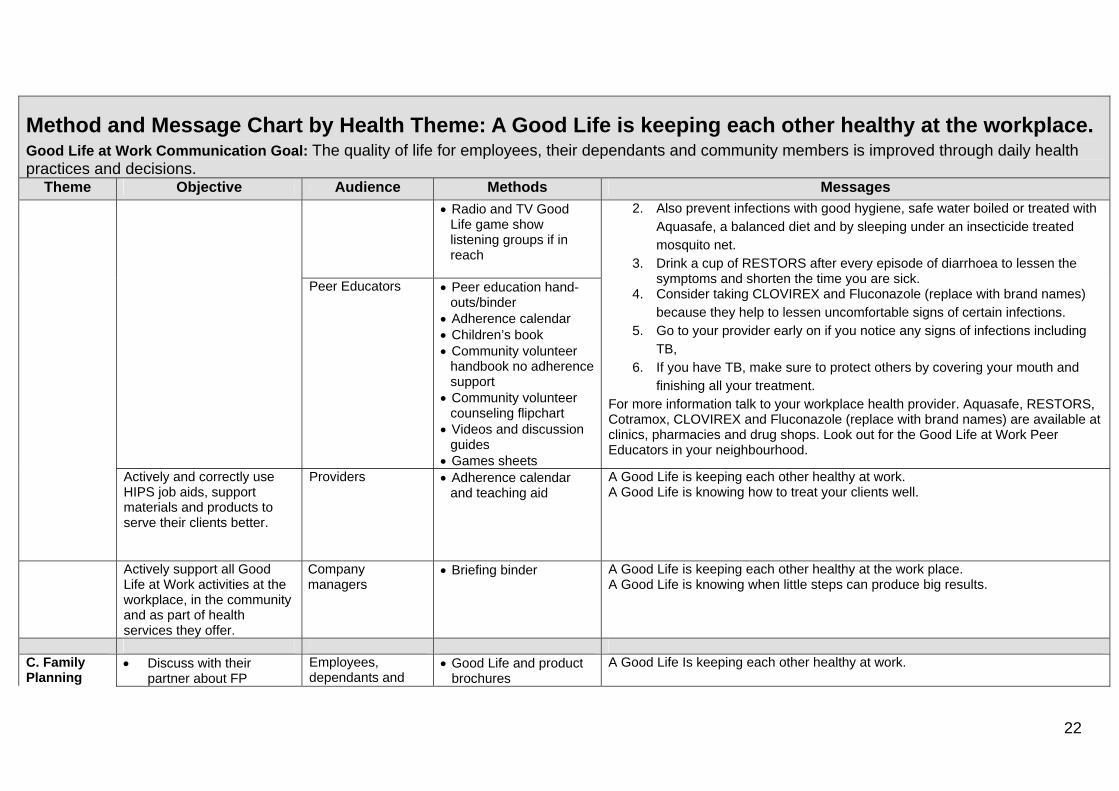
Method and Message Chart by Health Theme: A Good Life is keeping each other healthy at the workplace. Good Life at Work Communication Goal: The quality of life for employees, their dependants and community members is improved through daily health practices and decisions.
Theme Objective Audience Methods Messages
Radio and TV Good Life game show listening groups if in reach
Peer Educators Peer education hand-
outs/binder Adherence calendar Children’s book Community volunteer
handbook no adherence support
Community volunteer counseling flipchart
Videos and discussion guides
Games sheets
2. Also prevent infections with good hygiene, safe water boiled or treated with Aquasafe, a balanced diet and by sleeping under an insecticide treated mosquito net.
3. Drink a cup of RESTORS after every episode of diarrhoea to lessen the symptoms and shorten the time you are sick.
4. Consider taking CLOVIREX and Fluconazole (replace with brand names) because they help to lessen uncomfortable signs of certain infections.
5. Go to your provider early on if you notice any signs of infections including TB,
6. If you have TB, make sure to protect others by covering your mouth and finishing all your treatment.
For more information talk to your workplace health provider. Aquasafe, RESTORS, Cotramox, CLOVIREX and Fluconazole (replace with brand names) are available at clinics, pharmacies and drug shops. Look out for the Good Life at Work Peer Educators in your neighbourhood.
Actively and correctly use HIPS job aids, support materials and products to serve their clients better.
Providers Adherence calendar and teaching aid
A Good Life is keeping each other healthy at work. A Good Life is knowing how to treat your clients well.
Actively support all Good Life at Work activities at the workplace, in the community and as part of health services they offer.
Company managers
Briefing binder A Good Life is keeping each other healthy at the work place. A Good Life is knowing when little steps can produce big results.
C. Family Planning
Discuss with their partner about FP
Employees, dependants and
Good Life and product brochures
A Good Life Is keeping each other healthy at work.
23
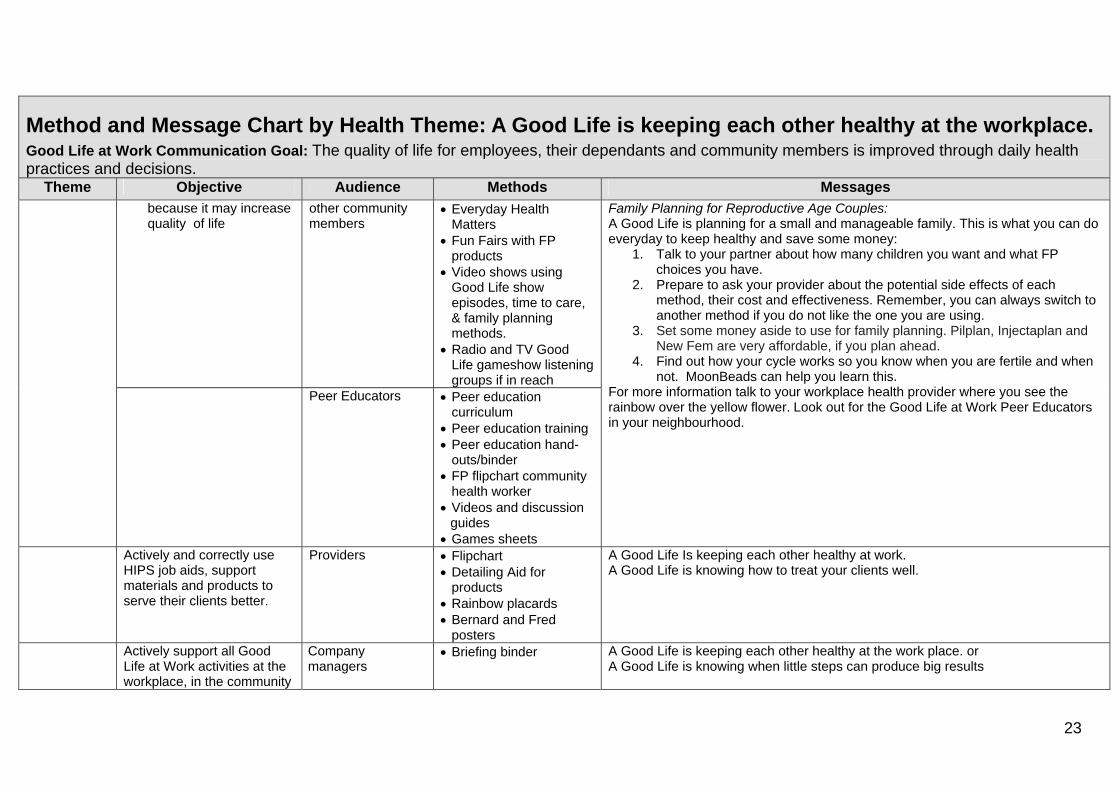
Method and Message Chart by Health Theme: A Good Life is keeping each other healthy at the workplace. Good Life at Work Communication Goal: The quality of life for employees, their dependants and community members is improved through daily health practices and decisions.
Theme Objective Audience Methods Messages
because it may increase quality of life
other community members
Everyday Health Matters
Fun Fairs with FP products
Video shows using Good Life show episodes, time to care, & family planning methods.
Radio and TV Good Life gameshow listening groups if in reach
Peer Educators Peer education curriculum
Peer education training Peer education hand-
outs/binder FP flipchart community
health worker Videos and discussion
guides Games sheets
Family Planning for Reproductive Age Couples: A Good Life is planning for a small and manageable family. This is what you can do everyday to keep healthy and save some money:
1. Talk to your partner about how many children you want and what FP choices you have.
2. Prepare to ask your provider about the potential side effects of each method, their cost and effectiveness. Remember, you can always switch to another method if you do not like the one you are using.
3. Set some money aside to use for family planning. Pilplan, Injectaplan and New Fem are very affordable, if you plan ahead.
4. Find out how your cycle works so you know when you are fertile and when not. MoonBeads can help you learn this.
For more information talk to your workplace health provider where you see the rainbow over the yellow flower. Look out for the Good Life at Work Peer Educators in your neighbourhood.
Actively and correctly use HIPS job aids, support materials and products to serve their clients better.
Providers Flipchart Detailing Aid for
products Rainbow placards Bernard and Fred
posters
A Good Life Is keeping each other healthy at work. A Good Life is knowing how to treat your clients well.
Actively support all Good Life at Work activities at the workplace, in the community
Company managers
Briefing binder A Good Life is keeping each other healthy at the work place. or A Good Life is knowing when little steps can produce big results
24
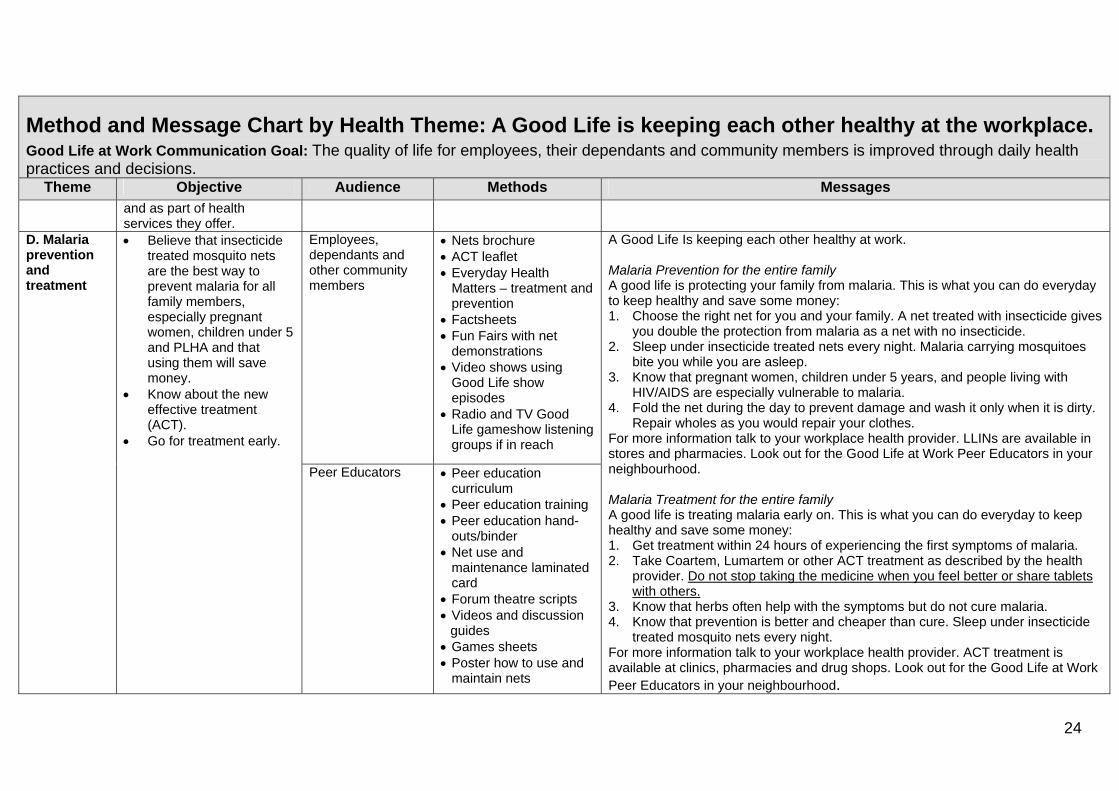
Method and Message Chart by Health Theme: A Good Life is keeping each other healthy at the workplace. Good Life at Work Communication Goal: The quality of life for employees, their dependants and community members is improved through daily health practices and decisions.
Theme Objective Audience Methods Messages
and as part of health services they offer.
D. Malaria prevention and treatment
Believe that insecticide treated mosquito nets are the best way to prevent malaria for all family members, especially pregnant women, children under 5 and PLHA and that using them will save money.
Know about the new effective treatment (ACT).
Go for treatment early.
Employees, dependants and other community members
Nets brochure ACT leaflet Everyday Health
Matters – treatment and prevention
Factsheets Fun Fairs with net
demonstrations Video shows using
Good Life show episodes
Radio and TV Good Life gameshow listening groups if in reach
Peer Educators Peer education curriculum
Peer education training Peer education hand-
outs/binder Net use and
maintenance laminated card
Forum theatre scripts Videos and discussion
guides Games sheets Poster how to use and
maintain nets
A Good Life Is keeping each other healthy at work. Malaria Prevention for the entire family A good life is protecting your family from malaria. This is what you can do everyday to keep healthy and save some money: 1. Choose the right net for you and your family. A net treated with insecticide gives
you double the protection from malaria as a net with no insecticide. 2. Sleep under insecticide treated nets every night. Malaria carrying mosquitoes
bite you while you are asleep. 3. Know that pregnant women, children under 5 years, and people living with
HIV/AIDS are especially vulnerable to malaria. 4. Fold the net during the day to prevent damage and wash it only when it is dirty.
Repair wholes as you would repair your clothes. For more information talk to your workplace health provider. LLINs are available in stores and pharmacies. Look out for the Good Life at Work Peer Educators in your neighbourhood. Malaria Treatment for the entire family A good life is treating malaria early on. This is what you can do everyday to keep healthy and save some money: 1. Get treatment within 24 hours of experiencing the first symptoms of malaria. 2. Take Coartem, Lumartem or other ACT treatment as described by the health
provider. Do not stop taking the medicine when you feel better or share tablets with others.
3. Know that herbs often help with the symptoms but do not cure malaria. 4. Know that prevention is better and cheaper than cure. Sleep under insecticide
treated mosquito nets every night. For more information talk to your workplace health provider. ACT treatment is available at clinics, pharmacies and drug shops. Look out for the Good Life at Work Peer Educators in your neighbourhood.
25
Method and Message Chart by Health Theme: A Good Life is keeping each other healthy at the workplace. Good Life at Work Communication Goal: The quality of life for employees, their dependants and community members is improved through daily health practices and decisions.
Theme Objective Audience Methods Messages
Actively and correctly use
HIPS job aids, support materials and products to serve their clients better.
Providers Act dosage chart Malaria in pregnancy wall chart and Gestation Wheel; Prevention Flipchart Malaria website
A Good Life Is keeping each other healthy at work. A Good Life is knowing how to treat your clients well.
Actively support all Good Life at Work activities at the workplace, in the community and as part of health services they offer.
Company managers
Briefing binder A Good Life is keeping each other healthy at the work place. A Good Life is knowing when little steps can produce big results.

26
USAID/HIPS MENU OF SERVICES
HEALTH SERVICES HIV/AIDS TB MALARIA OVC FP/RH Cost Share Description
WORKPLACE POLICY DEVELOPMENT � � � � � � Developing HIV/AIDS & TB policies. Enhancing local organizations' capacity to implement workplace programs
PEER EDUCATION � � � � � � Training of Trainers, Training of employees, support staff and community members to share health information
HEALTH FAIRS � � � � � � Employee & Community Entertainment & Education fun day focused on health issues and products. Includes VCT
VOLUNTARY COUNSELING & TESTING � � Community outreaches, Onsite facility-based VCT, Provision of Counselor s and Test kits
HEALTH COMMUNICATION MATERIALS � � � � � � Handbooks, Job Aids, Brochures, Posters, Banners, Leaflets, Charts, Flyers, DVDs, Cassettes, Screensavers.
LOW COST HEALTH COMMODITIES � � � � Long lasting Treated mosquito nets, Moon beads, Water purifier, Condoms, Oral Rehydration salts & contraceptives
PRIVATE CLINICS MOH ACCREDITATION � �
Collaborate with Ministry of Health to accredit Private health providers receive drugs and establish referral links
ACCESS TO FREE ARV'S/TB DRUGS/IPT2 FOR MALARIA � � �
Linkages, Trainings & technical assistance to receive free MOH ARV's & TB drugs. It includes support for pregnant mothers
LAB. EQUIPMENT & TRAINING � � � �
Equipment (e.g. microscope, colorimeter), Reagents for diagnosis & treatment of TB, Malaria & some STI’s
CLINICAL & COMMUNITY BASED TRAININGS � � � � �
Trainings in the Use of ARV's, TB, Palliative Care, Counseling & Testing, and Pediatrics. Also entails Training of OVC Care givers

27


![Upper cervical fractures (Occiput-C2) measurements1].pdf65.2% male Osteoarthritis (159 hips, 75.7%), Perthes (6 hips, 2.9%), hip dysplasia (17 hips, 8.1%), osteonecrosis (5 hips, 2.4%),](https://img.pdfslide.net/doc/110x75/5f3a0f2f662728190240d629/upper-cervical-fractures-occiput-c2-measurements-1pdf-652-male-osteoarthritis.jpg)


























