Embed Size (px)
Citation preview

HISTORICAL ORIGINS OF SCHIZOPHRENIA: TWO EARLY MADMEN AND THEIRILLNESS
R. WALTER HEINRICHS
Schizophrenia is a serious mental illness with a remarkably short recorded history. Unlikedepression and mania, which are recognizable in ancient texts, schizophrenia-like disorderappeared rather suddenly in the psychiatric literature of the early nineteenth century. Thiscould mean that the illness is a recent disease that was largely unknown in earlier times.But perhaps schizophrenia existed, embedded and disguised within more general conceptsof madness and within the arcane languages and cultures of remote times. Both possibili-ties present major challenges to historical and psychiatric scholarship. These challengesare explored in this paper by presenting two “new” cases of schizophrenia, one from theeighteenth and one from the fourteenth century. The cases suggest that the illness may haveexisted as early as the medieval period. However, establishing the population prevalence ofschizophrenia in earlier times—and therefore resolving the permanence-recency debate—may not be a feasible enterprise. © 2003 Wiley Periodicals, Inc.
Severe distortions of thought and feeling define schizophrenia, the most serious and dis-abling form of mental illness. Ideas of power and persecution, arguments without reason,voices at once intimate and alien, and a loss of pleasure and interest—these are the symptomsthat lay hold of the schizophrenic mind. A retreat from friends and family, education, andwork completes the grim picture for many patients. It is a disease of young people but oftenlingers for a lifetime, creating dependency, stress for relatives, and a great burden for society.Despite advances in drug treatment and increased research funding, schizophrenia continuesto be a major scientific challenge. Moreover, the challenge is not limited to finding biologi-cal causes of the illness. Schizophrenia is also a puzzle of history.
Current diagnostic criteria specify a disorder that can be traced directly to the detailedclinical descriptions of Kraepelin (1893, 1919) and Bleuler (1950/1911) at the turn of thetwentieth century. However, the accounts of Haslam (1809/1976) and Pinel (1809) are oftenregarded as the earliest cases of schizophrenia in the medical and psychiatric literature (seeGottesman, 1991, pp. 5-6; Shorter, 1997, p. 61). Prior to these seminal contributions, de-scriptions of “madness” occurred, but it is hard to discern a distinct and unmistakable schiz-ophrenia-like illness. Accordingly, the possibility has been raised that the illness was rare be-fore the nineteenth century (Hare, 1983, 1988a; Torrey, 1980, Torrey & Miller, 2001). Incontrast, a second view holds that schizophrenia-like illness has always been present in peo-ple across cultures and historical periods (Turner, 1992; Youssef & Youssef, 1996; Jeste et al.,1985). However, earlier literary, religious, biographical, and medical accounts of madness didnot distinguish schizophrenia from other forms of insanity. Therefore, it is argued, the illnesswas embedded and obscured within the broad spectrum of mental suffering describedthroughout history. Finally, a third perspective disputes both the “recency” and “permanence”views, holding that schizophrenia is first and foremost an illness concept introduced in
Journal of the History of the Behavioral Sciences, Vol. 39(4), 349–363 Fall 2003Published online in Wiley Interscience (www.interscience.wiley.com). DOI 10.1002/jhbs.10152© 2003 Wiley Periodicals, Inc.
R. WALTER HEINRICHS studied drawing, painting, and art history, as well as the art of psychotic pa-tients at the Ontario College of Art in Toronto. He obtained an undergraduate degree in psychology fromYork University and went on to graduate study in neuropsychology at the University of Toronto. He wasemployed in clinical hospital practice for several years and developed scholarly and scientific interests inthe history and neuroscience of schizophrenia. His most recent book is In Search of Madness:Schizophrenia and Neuroscience (Oxford, 2001).
349

Kraepelin’s (1893) textbook of psychiatry (Hoenig, 1995; pp. 336–347). There have beenmany forms and definitions of madness, deviance, lunacy, and insanity, each reflecting the in-terpretations and values important to people living in particular times and places. In otherwords, madness is a socially constructed interpretation of human conduct, inextricably boundto the language and beliefs of particular historical contexts (Porter, 1987, 2002; Scull, 1984).According to this view, historical schizophrenia was born in 1893 and the more elaborate con-cepts of the illness are largely products of the twentieth century.
In this article, I explore these differing views in relation to two cases of schizophrenia-like illness, one from the eighteenth century and one from the fourteenth. The cases illustratethe challenges of historical interpretation and evidence posed by a condition that reveals it-self so little in physical suffering and so extensively in a person’s mind and behavior. Theyalso suggest that the illness, if not its medical description, existed prior to the nineteenth cen-tury. However, estimation of the population prevalence of historical schizophrenia is difficultin light of the nature and limitations of case material and the special considerations that applyto each period and context.
THE MISSING ILLNESS
Madness—in the general sense of irrational, unintelligible, or uncontrolled behavior—canbe found in the Bible, in Mesopotamian, classical Greek, and Latin literature, and in the writingof many non-Western cultures (Haldipur, 1984; Hershkowitz, 1998; Jeste et al., 1985; Padel,1995). However, controversy exists about the historical presence of the kinds of symptoms seenin modern schizophrenia and about the existence of the disease state itself—a persistent psy-chosis of young people that is not a product of other medical or drug-induced conditions. Forexample, Torrey and Miller (2001) and Hare (1988a) reviewed cases of insanity prior to 1700and concluded that auditory hallucinations were seldom reported, while psychosis was usuallybrief, affected people of any age, and occurred in the presence of other medical diseases.Therefore, typical symptoms and the expected onset, duration, and “functional” nature of schiz-ophrenia were rare or absent. In contrast, Turner (1992) reviewed the same literature and arguedthat what was absent was not the illness necessarily, but a modern diagnostic system and indeedmedical involvement in cases of insanity. Early physicians might have considered the specificqualities of psychotic symptoms or the course of the condition that gave rise to these symptomsto be unimportant on the few occasions when such patients were brought to their attention.
Controversy also exists about whether the rise in cases of serious mental illness includ-ing schizophrenia during the nineteenth century was more apparent than real. Proponents ofthe recency view hold that whereas schizophrenia-like illness was statistically infrequent priorto 1800, it increased markedly in the next century, prompting the conclusion that “. . . in theworld of psychiatric disease, something new had raised its head” (Shorter, 1997, p. 64). Thecountervailing view is that physicians with psychiatric interest and expertise were rare in theeighteenth and earlier centuries and that schizophrenia was present, but simply not recognizedas a distinct syndrome or disease entity (Turner, 1992, pp. 416–418). This situation changedby the mid-nineteenth century as psychiatry and medicine became increasingly professional,assumed responsibility for care and treatment of mental illnesses like schizophrenia, andbegan to report and write about these illnesses.
In any case, medical-psychiatric texts and asylum records are not the only sources of in-formation about the nature and prevalence of psychotic illness. Literary, biographical, and au-tobiographical material also contains descriptions of madness. One such autobiography in-volved George Trosse, an English minister who had a mental breakdown in 1656 at the age
350 R. WALTER HEINRICHS

of 25 and kept a journal of the experience (Hunter & Macalpine, 1982, pp. 154–157). Trossedescribed hearing divine and satanic voices and he experienced visions and suicidal “tempta-tions.” He recovered and then relapsed over a period of weeks or months. Jeste et al. (1985)went so far as to apply criteria from the Diagnostic and Statistical Manual of MentalDisorders (DSM-III; American Psychiatric Association, 1980) retrospectively to the autobi-ography and concluded that Trosse had schizophrenia. However, Hare (1988b) reviewed thesame case material in more detail and noted that Trosse was so drunk on the day the illnessbegan that he fell from his horse and had to be put to bed. Indeed, alcoholic psychosis andmood disorder in a man who certainly abused ethanol were regarded as the most plausible di-agnoses.
Differing conclusions from retrospective diagnosis and the disputed discovery of casesof early schizophrenia illustrate the different standards of evidence applied to the same mate-rial by proponents of recency and permanence viewpoints. Recency advocates tend to be crit-ical and selective in evaluating putative cases of early schizophrenia. Proponents of the per-manence view are more liberal in their evaluation of early cases, but more critical in assessingevidence for low prevalence of the illness prior to 1800. For example, Bark (1985) regardedthe simulation of madness by Edgar in Shakespeare’s King Lear as evidence for the existenceof schizophrenia in the early seventeenth century. However, recency advocates Hare (1988a)and Torrey and Miller (2001) also considered this material and emphasized the uncertain re-lation of a feigned illness expressed in literary form to the actual existence of a similar illnessin the population. On the other hand, the same recency authors accepted Napier’s case notesof his seventeenth-century medical practice in rural England and MacDonald’s (1981) retro-spective analysis of these notes in arguing for extremely low base rates of insanity prior to1800. Richard Napier was a clergyman-physician who left records on approximately 60,000patients, including 2,039 cases of “mental or emotional disturbance” seen in the course of 37years of practice. However, at most, 157 of these were regarded as psychotic or insane—avery low number in light of the time span and population base of Napier’s practice. Yet Turner(1992) built his case against the recency view by questioning the adequacy of Napier’s expo-sure to poorer classes of patients as well as the symptom interpretations and classificationsemployed by MacDonald. Therefore, the frequency and adequacy of both medical and non-medical descriptions of insanity and schizophrenia prior to 1800 have been disputed and sup-ported by advocates of each position.
LOOKING AT THE PAST THROUGH THE LENS OF THE PRESENT
What would a convincing case of pre-nineteenth-century schizophrenia look like? Ofcourse, many of the interpretive difficulties involved in finding the illness, especially before1800, involve the dangers of presentism—the unquestioning imposition of current views, as-sumptions, and concepts of illness onto the experience of people in the past. An obvious ex-ample of presentism would be the uncritical application of diagnostic criteria from the DSMto biographical or clinical case material from previous centuries. Thus the current (DSM-IV;American Psychiatric Association, 1994) symptom criteria for schizophrenia can be satisfiedon the basis of an auditory hallucination wherein a person hears a voice commenting on theirbehavior. But how would this kind of experience have been understood in, say, twelfth-cen-tury Europe, a time of strong religious convictions? Perhaps devout people were expected to“hear voices” from God or Satan and such experiences may have been viewed as evidence ofdivine or satanic communication and without reference to medical notions of illness and dis-
HISTORICAL ORIGINS OF SCHIZOPHRENIA 351

ease. Hence it is hard to justify any assumption that twenty-first-century disease terms andconcepts map precisely onto earlier usage and relationships that do exist probably weaken asthe illness trail recedes further into previous centuries, civilizations, languages, and cultures.
These considerations suggest that the expression of schizophrenic illness in a person’sthought, feeling, and behavior will be highly specific to the person’s historical and culturalsituation. However, this does not mean that modified forms of retrospective diagnosis are in-valid. After all, many modern psychiatric and neurological illnesses, including stroke (Denig,1995, pp. 72–94), epilepsy (Porter, 1995, pp. 164–173), and mental retardation (Berrios,1995, pp. 225–238) bear at least a family resemblance to their historical antecedents. In thecase of depression and mania, the degree of resemblance between ancient and modern de-scriptions is often pronounced (Porter, 1995, pp. 409–420). It seems reasonable to suggestthat retrospective diagnosis may have validity if modern terms and concepts are not blindlyimposed on the past and if case material is extensive and interpreted in relation to the histor-ical period as well as in relation to modern disease concepts (see Hume, 1999). It does not,however, seem reasonable to expect that such a syndrome would necessarily be recognized asa distinct illness or even as an illness at all during the period in question.
Consider, therefore, the possibility that the pathophysiology of the modern illness ex-isted in the past, with its expression in behavior strongly influenced, but not completely de-termined, by cultural and historical processes. If a core syndrome existed in previous centuriesthen it would have several characteristics that relate the syndrome to modern schizophrenia.First, it would have been a disease of young adults and one that was not transitory, but per-sisted for years. Second, it would have developed in the absence of drug and alcohol use ormedical conditions that can give rise to psychosis. Third, it would have involved key symp-toms, including beliefs considered implausible by the culture of the time (delusions), as wellas unusual sensory and perceptual experiences (hallucinations). Symptoms might also haveincluded forms of communication and thought considered incoherent, inappropriate, and ir-rational at the time, as well as behaviors suggesting withdrawal, disinterest, and removal fromeveryday life (negative symptoms). Finally, it would have been a condition that had an impacton a person’s social and occupational functioning, making it hard to maintain previous rolesand activities.
In support of this perspective, I present two cases of a schizophrenia-like illness. Thesecases are known to art historians and to psychoanalytic writers with an interest in culture andcreativity (e.g., Kris, 1952). However, they are not to be found in English language medical orpsychiatric texts and have been overlooked by previous historical searches for the illness (e.g.,Jeste et al., 1985; Persaud, 1993; Torrey & Miller, 2001; Turner, 1992). They not only predateHaslam’s (1809) and Pinel’s (1809) accounts, they provide pictures of a serious mental disor-der that bears considerable resemblance to the schizophrenia of the twenty-first century.
FRANZ XAVER MESSERSCHMIDT AND THE DEMON OF PROPORTION
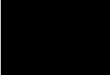
The more recent case of possible schizophrenia stems from the mid-eighteenth century,the same century that Hare (1988a) declared to be devoid of clear examples of the illness.Messerschmidt (1736–1783) was born and studied in Munich and then moved to Vienna tocontinue his artistic training. By the time he was 21 years of age, he had learned how to castbronze and other metals and was employed in the Imperial Armory. During the 1760s, hecompleted portrait sculptures commissioned by the aristocracy and the imperial court, appar-ently with considerable success, and by 1769 he was an assistant professor of sculpture (seeFigure 1a). There is no doubt that Messerschmidt was an artist of major talent and many con-
352 R. WALTER HEINRICHS

HISTORICAL ORIGINS OF SCHIZOPHRENIA 353
FIGURE 1.Figure 1a. Franz Xaver Messerschmidt (1736–1783), “Kaiser Franz I” (detail). Reproduced with permission of theOesterreichische Galerie Belvedere Vienna. Figure 1b. Franz Xaver Messerschmidt (1736–1783), “Der Gähner.”(“The Yawner”). Reproduced with permission of the Szépmüvészeti Múzeum, Budapest. Figure 1c. Franz XaverMesserschmidt (1736–1783), “Ein Schalksnarr.” (“A Buffoon”). Reproduced with permission of the OesterreichischeGalerie Belvedere Vienna. Figure 1d. Franz Xaver Messerschmidt (1736–1783), “Zweiter Schnabelkopf.” (“SecondBeak Head”). Reproduced with permission of the Oesterreichische Galerie Belvedere Vienna.
1a. 1b.
1c. 1d.

temporaries recognized him as an outstanding portraitist (see Pötzl-Malikova, 1982). Yet signsof mental illness entered the picture soon after his academic appointment and this seems tohave caused a permanent decline in his career. For example, it is known that he was passedover for academic promotion in 1774. The Prime Minister, who was responsible for such ap-pointments, described reasons for this situation in a note to the Empress Maria Teresa:
The most important objection, as far as this man is concerned, is the fact that for threeyears he has shown signs of some confusion—perhaps owing to his poverty or to a nat-ural disposition. Although that confusion in his head has meanwhile subsided, permittinghim to work as he had done before, it occasionally is still evident in a not perfectlyhealthy imagination . . . in that he believes all other professors and directors to be his en-emies: he still has odd and peculiar whims and therefore can never be completely com-posed. (Translated and cited by Kris, 1952, p. 130.)
Messerschmidt’s teaching duties were curtailed at this time, because it was felt that hecould not be “entrusted” with students. He was offered financial support in the form of anImperial pension but the troubled sculptor refused and left Vienna for Munich. He revealed aglimpse of his state of mind in a letter to his brother who lived in Bratislava: “. . . since al-ready for eight years—persecuted by my enemies—I have not been able to find employmentcommensurate with my artistic skill . . . indeed, it seems that all Germany feels obliged to per-secute me.” (translated and cited by Kris, 1952, p. 131). He soon moved to Bratislava, livingwith his brother for three years before moving to a house on his own where he resided in iso-lation on the outskirts of the city until his death from pneumonia in 1783.
It is in these last years of the sculptor’s life that evidence bearing on his mental state ismost detailed. The evidence takes the form of a visitor’s account of Messerschmidt’s livingsituation and artistic production, written by Friedrich Nicolai in 1785. This account requiresclose examination. Nicolai visited the sculptor in 1781 and apparently gained his trust.Messerschmidt showed the writer his studio and explained his artistic production. Of specialinterest from the standpoint of psychopathology were the sculptor’s descriptions of nocturnalvisits by demons. These demons tortured him “ . . . despite having lived a life of chastity.” Onedemon in particular was troublesome and referred to as the “demon of proportion.” Thisdemon was envious because the artist had almost achieved perfect proportion in his sculpture.Part of the demon’s torture involved causing Messerschmidt pain in his lower abdomen andthighs, especially when he was sculpting a part of the face that “. . . is analogous to a certainpart of the lower region of the body.” In order to control such demons, Messerschmidt pinchedhimself in the right side under the ribs and simultaneously grimaced into a mirror “ . . . in theexact required relationship to the pinching of his flesh. . . ” According to Nicolai the sculptorworked on his piece, looked into the mirror at half-minute intervals, and made “ . . . with thegreatest exactitude, precisely that grimace which he just needed.” (Translated and cited byKris, 1952, p. 137.)
And what were the sculptures like that Messerschmidt produced during this period?More than 60 sculpted heads were found in his studio at the time of his death and 49 have sur-vived in museums and private collections. They represent a variety of facial expressions,which led contemporaries to give them fanciful labels like “The Yawner” (Figure 1b) or “TheBuffoon” (Figure 1c) and to describe them as studies in physiognomy. The heads and theirfeatures range from rigid “empty” expressions to frowning to screaming contortions of theface. Given Nicolai’s description of how Messerschmidt worked, without models and withconstant reference to his own face in the mirror, some of the busts must be self-portraits. Theexpressions, it follows, are the grimaces evoked by his pain sensations, self-induced pinching,and attempts to fend off the demon of proportion.
354 R. WALTER HEINRICHS

Nicolai noticed two exceptions to this series of grimacing heads. In a corner ofMesserschmidt’s studio were two smaller and dramatically different pieces (see Figure 1d).These heads were severely distorted and had protruding chins. Growing straight out beneatheach nose was an elongated shape like a beak instead of a mouth. Here is Nicolai’s accountof the sculptor’s remarks concerning these “beak heads”:
. . . Messerschmidt glanced at these busts briefly with fixed eyes, and quickly turned hishead away . . . “That one” had pinched him, and he in turn pinched the demon and thesefigures were the result of it. “I thought, at last I will subdue you, but . . . nearly died inthis effort.” From what he said I realized that these caricatures of human faces were ac-tually the figures in which the deluded fantasy of Messerschmidt saw the demons of pro-portion. (Translated and cited by Kris, 1952, p. 146.)
There is little doubt that Messerschmidt was mentally disturbed, but did he suffer fromschizophrenia? There is no evidence that he was ever hospitalized for insanity, although hemay have consulted physicians including, perhaps, Franz Mesmer (see Pötzl-Malikova,1987). His contemporaries viewed him as “confused” and with an unhealthy “imagination.”Nicolai observed his behavior firsthand and recognized the sculptor’s implausible ideas as“deluded fantasies.” The travel writer described him as a man with a “fiery imagination”who was “. . . inclined to peculiarity” (Nicolai, 1785, p. 405, translated by the author). Butthis trait was related to Messerschmidt’s “love of independence” and single-minded dedica-tion to his art. Nicolai felt that most people would view the sculptor as either an “extraordi-nary person” or as a “fool” (Nicolai, p. 408, translated by the author). The only inference re-garding insanity was the conjecture that both “sicknesses of the mind” (“Krankheiten desGeistes”) and sicknesses of the body reflect the presence and development of a person’s “nat-ural forces” including, possibly, forces like imagination and genius (Nicolai, 1785, p. 408,translated by the author). He also mentioned that Messerschmidt knew of other peoplewhose minds were disturbed by visions of ghosts (Nicolai, 1785, p. 419). However, commoneighteenth-century German words for insanity like “Wahnwitz,” “Wahnsinn,” and“Verrücktheit” were not used by Nicolai in relation to Messerschmidt (see Crighton, 1996).By the early nineteenth century, the term “Narrheit” or foolishness was employed in relationto insanity, but it is unclear whether Nicolai had this in mind when describing his percep-tions of the artist. On the whole, it seems unlikely that Messerschmidt’s contemporaries re-garded him as insane, although he was certainly viewed as difficult, suspicious, peculiar, un-employable, and given to unwarranted and fantastic beliefs.
In light of the biographical and artistic evidence, it is possible to make a good retrospec-tive case for the presence of the four features of schizophrenia-like illness described earliereven though these features were not regarded as part of a disease syndrome in Messerschmidt’sown time. The sculptor was in his mid thirties when his disturbed mental state and behavior be-came noteworthy to other people. If this is used as an illness onset age it is somewhat olderthan the contemporary median onset age for schizophrenia in men (see Gottesman, 1991, pp.68–69), but still compatible with the idea of an illness that develops in young adults. Moreover,the surviving letters and documents suggest that Messerschmidt suffered from his disorder forat least a decade, which fits the idea that schizophrenia is a chronic condition and not a transi-tory reaction to traumatic events or experiences. In terms of symptoms, his experience of beingpersecuted by envious demons who could be controlled by sculpted facial expressions is a goodcandidate for being a bizarre delusion. Moreover, the sculptor’s letters and the observations ofhis employer in Vienna suggest that he experienced persecutory thoughts that were regarded asunwarranted and “unhealthy” by contemporaries. These thoughts may have amounted to per-secutory delusions and seem to have persisted over a protracted period of time. Nicolai’s report
HISTORICAL ORIGINS OF SCHIZOPHRENIA 355

also suggests the presence of an elaborate and grandiose delusional system as well as halluci-nations involving tactile sensations and verbal communication with the demons of proportion.Thus it appears likely that Messerschmidt suffered from persecutory and grandiose delusionsas well as from auditory, tactile, and possibly visual hallucinations.
However, there is more to schizophrenia than symptoms. The illness involves a reduc-tion in social and occupational role functioning and it constrains and prevents normal de-velopment and quality of life. This aspect is seen in Messerschmidt’s career decline, loss ofincome, and subsequent social isolation for the last decade of his life. With respect to co-existing disorders, it is sometimes difficult to discriminate schizophrenia from mood dis-orders because depression and mania can include psychotic symptoms. In Messerschmidt’scase, there is little in Nicolai’s account or in the correspondence related to his employmentor relationship with his brother to suggest the presence of depression. The sculptor in-creasingly showed the negative symptoms of schizophrenia-like withdrawal and isolation.Yet the energy and motivation required to complete over 60 detailed sculptures argueagainst severe depression and most of his expressed thought content seems related to per-secutory and control-related delusions rather than to self-deprecation and other commondepressive themes. Mania can manifest itself in delusions, but other common manic symp-toms like distractibility, verbosity, and heightened sexual, motor, or social activity do notappear in the biographical material. There is also no evidence in the observations of con-temporaries that Messerschmidt abused alcohol or other drugs. He probably died of pneu-monia, but no mention is made of any chronic physical disease that might have affectedmental functions.
In summary, although Messerschmidt’s contemporaries may not have regarded him asbeing insane, they did consider his thinking bizarre and implausible and his behavior was seenas grounds for loss of employment and increased social isolation. The information on his lifeand mental state is highly suggestive of a schizophrenia-like condition—and this from a cen-tury declared devoid of medical and psychiatric accounts of the illness. Now consider a muchearlier madman.
OPICINUS DE CANISTRIS AND THE SECRETS OF GEOGRAPHY
The second historical case of possible schizophrenia is less clear-cut and more chal-lenging because of its distance in time. Fortunately, extensive autobiographical material hassurvived and been translated to provide an account of this man (Salomon, 1936, 1953).Opicinus de Canistris (1296–1350) was born in Lomello, Italy, and grew up in Pavia. He wasa mediocre student, with an interest in poetry and drawing, but found employment as a tutorby the age of 20. Opicinus and family had to leave Pavia because of conflict between polit-ical factions in his native city. He learned the craft of book illustration and illumination inGenoa, but returned to Pavia to enter holy orders and accept a position at the cathedral. By1323, he was rector of a small parish and this position lasted for five years until financialand political problems again led to emigration. He was extremely poor during this time andbegan to write poems and articles on religious topics. One of his pamphlets addressed a po-litical conflict between Pope John XXII and the Holy Roman Emperor. It was dedicated tothe Pope and brought Opicinus attention and employment as a “scriptor” at the Papal officesin Avignon, France, until 1348.
Opicinus’s life becomes interesting from a psychiatric standpoint with his own accountof a “sickness” that struck on March 31, 1334. He described himself as being near death forseveral days. On regaining consciousness he could not move his limbs, but felt “reborn”:
356 R. WALTER HEINRICHS

I had forgotten everything and could not even remember how the world looked outside ofour dormitory. On June 3, after Vespers, I saw a vessel in the clouds. In consequence of thedisease I was mute, my right hand was lame and I had lost in a miraculous way a great dealof my literal memory (= positive knowledge). In the night of August 15, I saw in a dreamthe Virgin with the child in her lap, sadly sitting on the ground; and through her merits shehas given me back not the knowledge but a double spirit. Since February 1, 1335, I beganto retire, bit by bit, from my work in our office (the Poenitentiaria) because of the weaknessof my hand. In a spiritual work however this same hand proved stronger than before: sincethen it has drawn all these pictures without any human help. At present my lost literalknowledge is replaced twofold by spiritual knowledge; my right hand is weak in worldlywork, but strong in spiritual endeavors. (Translated and cited by Salomon, 1953, p. 47.)
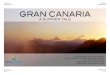
At first glance the description could apply to the results of a unilateral stroke in the leftor language dominant cerebral hemisphere. Such a neurological event could certainly causeweakness or even paralysis of the right hand along with expressive aphasia and writing dis-ability. However, the putatively weak hand was only weak in “worldly” respects. In “spiritualknowledge” it was strong, as demonstrated by two series of drawings, annotations, and writ-ings. The first comprised 52 large drawings on parchment, some three feet in length, that werecarefully and neatly produced with ruler and compasses as well as freehand and without anysign of motor weakness, tremor, or poor control. Most of the drawings depicted religious fig-ures and zodiac symbols set in geometric backgrounds. However, the spaces between figuresand the margins, and sometimes the designs themselves, contained autobiographical notes re-lating Opicinus’s personal life to constellations, dates, place names, and Biblical material.Figure 2a is a detail from a parchment that showed 40 concentric rings inscribed with autobi-ographical notes, each corresponding to a year of his life. Such personal detail from a cler-gyman was extremely rare in this historical period. Similarly, Figure 2b shows Opicinus at thecenter of a wheel of religious and allegorical symbols, with a crucifix at the center of his ab-domen. Several parchments showed a preoccupation with what could be termed “interpretivegeography.” Europe was drawn in the shape of a man, with North Africa a woman whisperingin his ear. The annotations indicate that Europe was Adam and Africa was Eve and their junc-tion at Gibraltar symbolized the origin of all evil. The notes were replete with references like“Avinio pectoralis,” “Roma tibialis,” and “Lombardia ventralis,” clearly tying cities and geo-graphic regions to body parts. Other drawings integrated these maps into depictions ofOpicinus himself along with comments about his inner life and character. For example, Figure3a shows a self-portrait that Opicinus labeled “The overbearing Pharisee” according toSalomon (1953, pp. 48–49). He is depicted with the inscription “thus I look inwardly in mypride.” The chest is open and shows a miniature map of the Mediterranean done as a mirrorimage, with Europe drawn as a man and Africa as a woman, the symbol of sin. The inscrip-tion reads: “Thus I am inwardly in my pride” (all quotations translated by Salomon).
After the initial series of 52 drawings he embarked on a second manuscript in 1337. Thiscontains 20 maps of the Mediterranean region that are smaller in scale and drawn on paper.The manuscript includes many pages of religious, allegorical, and autobiographical commen-tary. The map drawings show more variation in design than the first series (see Figure 3b).Sometimes Europe was portrayed as female and Africa as male and sometimes gender is re-versed. Spain was usually the head, southern France the breast, northern Italy the abdomenand the rest of Italy was the leg of a man or woman. The Mediterranean basin took on theform of a bearded man and represented the Devil. The commentary was written in Latin and,according to Salomon (1953), included many enigmatic, illogical, and incoherent passages:“involuntary and irresistible associations provoked by a single word or name cut across theway of his thought and lead his argumentation astray, not rarely into mere verbiage.” The
HISTORICAL ORIGINS OF SCHIZOPHRENIA 357

notes indicate that Opicinus identified himself with the Europe-man. They explain how thedistribution of hair growth on his body signified the distribution of vineyards in severalEuropean countries. He expanded this kind of reasoning to bodily functions and currentevents. Thus Opicinus’s constipation over several days represented political problems in the“abdomen” of Europe-Lombardy in northern Italy. Similarly, the pain of rheumatism in hisleft hand, which made it hard for him to touch his shoulder, “indicated” the failure of aprospective German assault on France, because France was the “shoulder” of his European
358 R. WALTER HEINRICHS
FIGURE 2.Figure 2a. Opicinus de Canistris (1296–1350), Drawing No. 11 (detail). Codex Vaticano Palatino 1993 © BibliotecaApostolico Vaticana (Vatican). Figure 2b. Opicinus de Canistris (1296–1350), Drawing No. 16 (detail). CodexVaticano Palatino 1993 © Biblioteca Apostolico Vaticana (Vatican).
2a.
2b.

map-man. He made it clear that his “discovery” of the “meaning” of these maps was a turn-ing point in his life and developed in the wake of his “sickness”:
I never saw maps being drawn nor was I interested in that because my ignorance did notallow me to know such things. God alone gave me the understanding so that I becameable to copy a map without anybody showing me how to do it. I did not know howeverwhat mystery was hidden in them until 1335 after I had recovered from my terrible dis-ease. (Cited in Salomon, 1953, p. 52.)
The case of Opicinus de Canistris differs from Messerschmidt in that no opinions orjudgments bearing on mental state and behavior are available from contemporaries.Therefore, the burden of evidence rests largely on autobiographical writings and on the draw-ings and maps. Fortunately, excellent art historical analyses and some psychological perspec-tives are available to provide information on stylistic and expressive conventions of the timeas well as on Opicinus’s violations of such conventions (e.g., Kris, 1952, pp. 118–127;Salomon, 1936, 1953; Roux & Laharie, 1997). It turns out, for example, that religious andsymbolic interpretation of the world and world events and the search for meaning and spiri-tual significance in mundane occurrences and coincidences were common pursuits in theMiddle Ages. Moreover, anthropomorphic interpretation of geography had precedents in me-
HISTORICAL ORIGINS OF SCHIZOPHRENIA 359
FIGURE 3.Figure 3a. Opicinus de Canistris (1296–1350), Drawing No. 22 (reverse, detail). Codex Vaticano Palatino 1993 ©Biblioteca Apostolico Vaticana (Vatican). Figure 3b. Opicinus de Canistris (1296–1350), Drawing No. 61. CodexVaticano Latina 6435 © Biblioteca Apostolico Vaticana (Vatican).
3a. 3b.

dieval writing. On the other hand, the late medieval period was a time when explicit autobi-ography of any kind was almost unknown (see Salomon, 1953, pp. 47–56). Yet here was aman, a lowly clerk, who not only wrote about himself in great detail but also injected this ma-terial into grand religious and geopolitical representations. The maps represented his sins, thecountries were his body and soul, and his destiny was written in the configuration of conti-nents. Opicinus departed from any norms of his religious, social, and cultural context in iden-tifying himself with the Europe-man depicted in his maps. The conviction that his body partsand sensations corresponded to both the geography of Europe and to political events is con-sistent with the kind of grandiose and self-referential delusions experienced by many schizo-phrenia patients. In addition, he may have experienced other symptoms including visual hal-lucinations—a “vessel in the clouds”—as well as thought and language disorders likederailment and incoherence expressed in his idiosyncratic writing. However, these symptomsare more difficult to separate from his reports of dream experiences and from the allegoricalwordplay and religious interpretations that had precedents in medieval Europe.
It is hard to determine the duration of Opicinus’s illness, which seems to have had anacute phase from which he “recovered” as well as a more chronic phase where he developedhis “spiritual knowledge.” Nonetheless, he produced his bizarre anthropomorphic maps andautobiography over a period between 1334 and 1341, which certainly suggests a prolongedperiod of active symptoms. In addition, it is important to note that Opicinus withdrew fromfull-time employment in the papal office because of the illness and subsequent loss of “literalmemory.” This employment was his highest level of occupational functioning and its reduc-tion was a consequence of his mental state. He seems to have remained in Avignon until 1348and may have been partly employed or resumed his duties at various points. But there is noevidence that he ever returned to his previous level of functioning. Healing “pilgrimages”from Avignon to recover from his illness are alluded to in his writings and many of his notessuggest social isolation and withdrawal. Hence the idea that schizophrenia is a chronic or re-current illness, with periods of active symptoms, leading to occupational decline and socialwithdrawal, is certainly satisfied in this case.
Some of the autobiographical entries translated and described by Salomon (1936, 1953)suggest self-deprecation and depression and raise the challenge of excluding mood disorderas an explanation for his behavior. However, Opicinus’s apparent delusion of having a handwith special spiritual powers seems to have preceded these mood-related entries. Moreover,like Messerschmidt, he demonstrated considerable energy and productivity during his illnesseven though it prevented normal occupational functioning. This too is inconsistent with thepresence of a major depressive disorder, especially in terms of vegetative symptoms.Opicinus’s detailed, intricate, and controlled drawings are hard to relate to a manic episodeand there are few suggestions of impulsive or uninhibited behavior in the autobiographicalpassages translated by Salomon (1936, 1953). Finally, although many passages are confes-sional, there are no signs of any struggle with alcohol or substance abuse in Opicinus’s man-uscripts. The existence of contributing medical conditions like hemiparesis and aphasia dueto left cerebral hemisphere stroke is not supported by the line quality of the drawings.Accordingly, a reasonable case can be made for the presence of a schizophrenia-like illness.
SCHIZOPHRENIA OLD AND NEW AND THE VAGARIES OF HISTORY
Are these early madmen tips of a vast schizophrenia iceberg or the exceptions that provethe rule of illness recency? Paradoxically, the case histories of Messerschmidt and Opicinusmay illustrate both the historical existence of the illness and the difficulties involved in find-
360 R. WALTER HEINRICHS

ing it and resolving the recency-permanence debate. On the one hand, the illness that is “miss-ing” from medicine and psychiatry may be present in early biographical, autobiographical,literary, and artistic material. This is a primary contention of scholars who argue for the “per-manence” position that schizophrenia has always existed (see Turner, 1992). However, thekind of case material represented by Opicinus and Messerschmidt may be rare even if the ill-ness was common in the past. Most people with schizophrenia do not leave written accountsof their conditions and only become the subjects of biographies when they do something ex-ceptional or remarkable. Kris (1952, pp. 88–89) estimated that less than 2% of psychotic pa-tients engaged spontaneously in creative activity. And this was in the era before antipsychoticmedication. Schizophrenia has a disabling, inhibitory influence on many forms of productiveactivity and if a similar illness syndrome existed in the past this influence was probably alsopresent. Therefore it is likely that the telltale signs of schizophrenic illness may be few andfar between even when the search expands beyond psychiatry and medicine.
Another possible source of information about early schizophrenia derives from situa-tions where people with the illness came into conflict with social conventions. For example,descriptions of alleged witchcraft are interesting from a psychiatric standpoint. However,legal records of seventeenth-century prosecutions are difficult to understand and interpretwithout expert linguistic and cultural analysis (see Burr, 1975; Mather, 1916). It seems that aunique combination of skills is needed to track serious mental illness into the past. Theseskills include a clinician’s knowledge and experience with modern schizophrenia, a historian’sknowledge of the madman’s—or madwoman’s—time period, a linguist’s knowledge ofchanges in language forms and usage, and an art scholar’s knowledge of aesthetic and stylis-tic conventions. It is perhaps not surprising that so few convincing early cases of schizophre-nia have been identified in light of the need for detailed biographical material and the needfor special interpretive skills to understand this material.
Opicinus and Messerschmidt illustrate the importance of interpretive skill insofar asboth were subjects of detailed art-historical analysis (e.g., Pötzl-Malikova, 1982; Salomon,1936). In the absence of such studies, these madmen might have remained unknown or mis-understood despite their value in the search for historical schizophrenia. Indeed,Messerschmidt’s psychiatric status was not considered unusual throughout the nineteenth cen-tury because of presumed links between genius, creativity, social alienation, and madness (seeKris, pp.149–150). The sculptor was a “misunderstood visionary” and not a gifted man whosecareer was destroyed by mental illness. At the same time, presentism may obscure the effortsof modern psychiatric historians. The medieval world inhabited by Opicinus de Canistris wasso different from current culture that it is easy to “pathologize” medieval ideas and behaviors.Many seemingly abnormal ideas were in fact expressions of a time when everyday life waspervaded with religious thought, mysticism, symbolism, and allegory. On the other hand, ide-ologies that developed with the Renaissance, like humanism and individualism, also make iteasy for the modern researcher to miss the forest for the trees. Thus Opicinus’s injection ofhighly personal autobiographical material into his religious illustrations would have been seenas an outrageous act of grandiosity for a lowly cleric of the fourteenth century. Yet self-ex-pression and introspection are commonplace in the present and so Opicinus’s writings seemless remarkable from a modern perspective. Extremely careful scholarship will be needed toclarify the historical and cultural situation of any putative cases of early schizophrenia re-ported in the future.
On balance, it seems probable that reports of a schizophrenia-like syndrome will con-tinue to be rare in the historical record prior to 1800. The scarcity may reflect the scarcity ofthe syndrome itself, or simply the relative absence of its personal and biographical artifacts.
HISTORICAL ORIGINS OF SCHIZOPHRENIA 361

This evidential situation means that it will be hard to resolve the recency-permanence debateconcerning the illness. It is one thing to say that schizophrenia occurred before 1800 and an-other to say that it was as common then or less common than it is today. Yet, unless a defen-sible estimate of historical prevalence is derived, there is no way of supporting or rejecting ei-ther the recency or permanence positions with respect to schizophrenia. What may be feasibleis resolution of the debate in terms of more inclusive illness categories that do not distinguishschizophrenia from other potentially psychotic disorders like bipolar illness (see Torrey &Miller, 2001, pp. 335–338). In the process, however, schizophrenia will be returned oncemore to the broad spectrum of madness from which it was extracted only a century ago.
I would like to thank Professors Hanna Pötzl-Malikova and Herb Ranharter for advising me and assisting myresearch on Franz Xaver Messerschmidt. Thanks are also due to Frau Hannelore Steindl of the Austrian Museum inVienna for help in locating reproductions of Messerschmidt’s work. Professor Thomas Teo of York University and Dr.Renate Heinrichs helped compensate for my rusty German and John Dawson provided expert photographic servicesand advice. Several people at the Biblioteca Apostolico Vaticano (Vatican) were indispensable during my study ofOpicinus’s manuscripts. They included Sister Catherine Mary Clarke, Father Louis Duval-Arnould, Irma Schuler, andDon Raffaele Farina. Finally, I thank Eleanor Sam for her special presence, support, and encouragement. This proj-ect was assisted by a sabbatical leave fellowship grant from York University in 2001–2002.
REFERENCES
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.).Washington, DC: American Psychiatric Press Inc.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.).Washington, DC: American Psychiatric Press Inc.
Bark, N. M. (1985). Did Shakespeare know schizophrenia? The case of poor Mad Tom in King Lear. British Journalof Psychiatry, 146, 436–438.
Berrios, G. (1995). Chapter 9 Mental retardation: clinical section II. In G. Berrios & R. Porter (Eds.), A history ofclinical psychiatry (pp. 225–238). London: Athlone Press.
Bleuler, E. (1950). Dementia praecox, or the group of schizophrenias (J. Zinkin, Trans.). New York: InternationalUniversities. (Original work published in 1911.)
Burr, G. L. (1975). Narratives of the witchcraft cases, 1648–1706. New York: Barnes & Noble.Crighton, J. (1996). Some descriptions of schizophrenia-like illness in the German literature of the early 19th cen-
tury. History of Psychiatry, 6, 31–54.Denig, T. R. (1995). Chapter 3 Stroke and other vascular disorders: clinical section. In G. Berrios & R. Porter (Eds.),
A history of clinical psychiatry (pp. 72–85). London: Athlone Press.Gottesman, I. I. (1991). Schizophrenia genesis: the origins of madness. New York: W. H. Freeman.Haldipur, C. V. (1984). Madness in ancient India; Concept of insanity in Charaka Samhita (1st century A.D.).
Comprehensive Psychiatry, 25, 335–344.Hare, E. (1983). Was insanity on the increase? British Journal of Psychiatry, 142, 439–455.Hare, E. (1988a). Schizophrenia as a recent disease. British Journal of Psychiatry, 153, 521–531.Hare, E. (1988b). Schizophrenia before 1800? The case of the Revd George Trosse. Psychological Medicine, 18,
279–285.Haslam, J. (1809/1976). Observations on madness and melancholy. New York: Arno Press.Hershkowitz, D. (1998). The madness of epic: reading insanity from Homer to Statius. Oxford: Clarendon.Hoenig, J. (1995). Chapter 13 Schizophrenia: clinical section. In G. Berrios & R. Porter (Eds.), A history of clinical
psychiatry (pp. 336–348). London: Athlone Press.Hume, R. D. (1999). Reconstructing contexts. New York: Oxford.Hunter, R., & Macalpine, I. (1982). Three hundred years of psychiatry 1535–1860 (2nd ed.). Hartsdale, NY: Carlisle. Jeste, D. V., del Carmen, R., Lohr, J. B., & Wyatt, R. J. (1985). Did schizophrenia exist before the eighteenth cen-
tury? Comprehensive Psychiatry, 26, 493–503.Kraepelin, E. (1893). Psychiatrie: Ein Lehrbuch für Studierende und Ärzte (4th ed.). Leipzig: Barth.Kraepelin, E. (1919). Dementia praecox and paraphrenia. (R. M. Barclay, Trans.; G. M. Robertson, Ed.) (pp. 1–331).
Edinburgh: E. & S. Livingstone.Kris, E. (1952). Psychoanalytic explorations in art. New York: International Universities Press.MacDonald, M. (1981). Mystical bedlam. Cambridge, UK: Cambridge University Press. Mather, C. (1916). Curious cases and amusing actions at law: including some trials of witches in the seventeenth cen-
tury. London: Sweet & Maxwell.Nicolai, F. (1785). Beschreibung einer Reise durch Deutschland und die Schweiz im Jahre 1781. Band 6. Leipzig:
Author.
362 R. WALTER HEINRICHS

Padel, R. (1995). Whom gods destroy: elements of Greek and tragic madness. Princeton, NJ: Princeton UniversityPress.
Persaud, R. (1993). The reporting of psychiatric symptoms in history: the memorandum book of Samuel Coates,1785–1825. History of Psychiatry, 4, 499–510.
Pinel, P. (1809). Traité médico-philosophique sur l’aliénation mentale (2nd ed.). Paris: Brosson.Porter, R. (1987). Mind-forg’d manacles: a history of madness in England from the restoration to the regency.
London: Athlone Press.Porter, R. (1995). Chapter 15 Mood disorders: social section. In G. Berrios & R. Porter (Eds.), A history of clinical
psychiatry (pp. 409–420). London: Athlone Press.Porter, R. (2002). Madness: a brief history. Oxford: Oxford University Press. Pötzl-Malikova, M. (1982). Franz Xaver Messerschmidt. Vienna: Jugend und Volk.Pötzl-Malikova, M. (1987). Zur Beziehung Franz Anton Mesmer-Franz Xaver Messerschmidt. Wiener Jahrbuch für
Kunstgeschichte, Band XL, pp. 257–267. Roux, G., & Laharie, M. (1997). Art et Folie au Moyen Age. Paris: Le Léopard d’Or.Salomon, G. (1936). Opicinus de Canistris. London: Warburg Institute.Salomon, G. (1953). A newly discovered manuscript of Opicinus de Canistris. Journal of the Warburg and Courtauld
Institutes, 16, 45–57.Scull, A. (1984). Was insanity increasing? A response to Edward Hare. British Journal of Psychiatry, 144, 432–436.Shorter, E. (1997). A history of psychiatry. New York: Wiley.Torrey, E. F. (1980). Schizophrenia and civilization. London: Aronson.Torrey, E. F., & Miller, J. (2001). The invisible plague: the rise of mental illness from 1750 to the present. New Jersey:
Rutgers University Press.Turner, T. H. (1992). Schizophrenia as a permanent problem: some aspects of historical evidence in the recency (new
disease) hypothesis. History of Psychiatry, 3, 413–429.Youssef, H. A., & Youssef, F. A. (1996). Evidence for the existence of schizophrenia in medieval Islamic society.
History of Psychiatry, 7, 55–62.
HISTORICAL ORIGINS OF SCHIZOPHRENIA 363