-
HISTORY OF BENZODIAZEPINES
WHAT THE TEXTBOOKS MAY NOT TELL YOU
Heather Ashton, Newcastle upon Tyne, UK
-
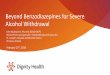
ANXIOLYTIC DRUGS THROUGH THE AGESAlcohol 8000 yearsOpium1000s of
yearsBromides1870sAlso chloral hydrate, paraldehydeBarbiturates
1903-1912Also carbromal, glutethimide, methaqualone
etcBenzodiazepines 1960 Librium; 1963 ValiumZ drugs zopiclone 1998;
eszopiclone 2005
-
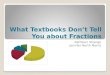
Morbidity in 50 long-term benzodiazepine users
After starting benzodiazepines:20% - took drug overdose
requiring hospital admission20% - developed incapacitating
agoraphobia18% - had GI investigations (irritable bowel)10% - had
neurological investigations(3 wrongly diagnosed as MS)62% -
received other psychotropic drugs (antidepressants)28% - were
taking 2 prescribed benzodiazepines
-
Some Common Acute Benzodiazepine Withdrawal SymptomsSymptoms
common to all Symptoms less common inanxiety states anxiety states;
relatively specific to benzodiazerpine withdrawalAnxiety, panic
attacks, agoraphobia Perceptual disturbances, sense
movementInsomnia, nightmares Depersonalisation,
derealisationDepression, dysphoria Hallucinations (visual,
auditory), Excitability, jumpiness, restlessness misperceptionsPoor
memory, concentration Distortion of body image Dizziness,
lightheadedness Tingling, numbness, altered sensation Weakness,
jelly legs Formication Tremor Sensory hypersensitivity (light,
sound, Muscle pain, stiffness taste, smell) (limbs, back, neck,
jaw, head) Muscle twitches, jerks, fasiculation Sweating, night
sweats Tinnitus Palpitations Psychotic symptoms Confusion, delirium
Fits
-
SOME PROTRACTED BENZODIAZEPINE WITHDRAWAL
SYMPTOMSAnxietyDepressionGastrointestinalNeurologicaltinnitus?peripheral
neuropathymotor - muscle spasms, ticks, jerks restless legs
syndrome?cognitive impairment
-
SOCIOECONOMIC COSTS OF INAPPROPRIATE BENZODIAZEPINE
PRESCRIBING
1. Increased mortality from overdose, suicide2. Increased risk
of accidentstraffic. Home, work, falls and fractures in elderly3.
Increased risk of aggressive behaviour, assault, antisocial acts4.
Contribution to marital/domestic disharmony5. Increased risk to
foetus, infants, children6. Contribution to job loss, unemployment,
loss of work through illness7. Cost of medical consultations,
hospital admissions/ investigations8. Dependence and withdrawal
reactions9. Recreational abuse - AIDS, hepatitis, unwanted
pregnancy10. Costs of drug NHS prescriptions11. Costs to DHSS due
to disability12. Costs of litigation
-
THERAPEUTIC ACTIONS OF BENZODIAZEPINESActionsClinical
usesHypnoticShort-term treatment of insomniaAnxiolytic
(tranquillising)Short-term treatment of severe anxietyShort-term
aid to alcohol withdrawalAcute treatment of violent
psychoticstatesAnticonvulsantEpileptic and drug-induced
convulsionsAmnesicPremedication before surgeryMuscle relaxantMuscle
spasms, dystonias
-
ADVERSE EFFECTS OF BENZODIAZEPINES1. Over-sedation Depressed
psychomotor performance, poor memory, ataxiacontribute to car
accidents, shoplifting Most marked in the elderly, may produce
mental confusioncontribute to falls and fractures2. Additive
effects with other CNS depressants e.g. alcohol, drug overdose3.
Disinhibition Aggressiveness ? Contribute to baby battering, wife
beatingDepression, emotional bluntingCognitive impairment6. Adverse
effects in pregnancy Neonatal depression7. Abuse8. Tolerance,
dependence, withdrawal effects
-
HALF-LIVES AND EQUIVALENT POTENCIES OF BENZODIAZEPINE
ANXIOLYTICSBenzodiazepine Half-life (hrs) Approximate [active
equivalent metabolite]oral dosages
(mg)_______________________________________________________Alprazolam
(Xanax)6-120.5Clonazepam (Klonepin) 18-500.5Lorazepam (Ativan)
10-20 1Diazepam (Valium) 20-100 10 [26-200]Chlordiazepoxide
(Librium) 5-30 25Clorazepate (Tranxene) [36-200] 15Oxazepam
(Serax)4-15 20
-
HALF-LIVES AND EQUIVALENT POTENCIES OF BENZODIAZEPINE
HYPNOTICSBenzodiazepineHalf-life (hrs) Approximate [active
metabolite] equivalent oral dosages
(mg)______________________________________________________Triazolam
(Halcion) 20.5Flunitrazepam (Rohypnol) 18-26 1 [36-200]Nitrazepam
(Mogadon) 15-38 10Temazepam (Restoril) 8-22 20Flunitrazepam
(Dalmane) [40-250]15-30Diazepam (Valium) 20-100 10 [36-200]
-
PATIENTS VULNERABLE TO INCREASED RISKS OF
BENZODIAZEPINESConditionRisks________________________________________Older
age (>65yrs) Mental confusion, amnesia, fallsand
fracturesChronic respiratory disease Respiratory depressionLiver
diseaseOversedationDepressionExacerbation, suicide riskOther
sedative drugsAdditive effectsPregnancyNeonatal depression,
withdrawalAlcohol/drug abuseIncreased risk of dependenceGenetic
factorsSlow metabolisers
______________________________________
-
HALF-LIVES AND EQUIVALENT POTENCIES OF Z-DRUGS Z drugHalf-life
(hrs) Approximate [active metabolite] equivalent oral dosages
(mg)________________________________________________________Zaleplon
(Sonata) 1-220Zolpidem (Ambien) 220Zopiclone (Zimovane)
5-615Eszopiclone (Lunesta) 6 3 (9 in elderly)
Diazepam (Valium) 20-10010 [36-200]
-
Basic principles1. Gradual dosage reduction- individual
withdrawal rate- adjuvant drugs2. Psychological support- simple
encouragement to psychological therapies- long term- information-
motivation
BENZODIAZEPINE WITHDRAWAL
-
ADJUVANT DRUGS IN BENZODIAZEPINE WITHDRAWALSometimes
indicatedantidepressants- depression, agoraphobia,
sedation-blockers- tremor, palpitationscarbamazepine- fits (high
dose Bz)sedative antihistaminesNot helpfulbuspirone, clonidine,
nifedipine, ? Alpidem, ? Gabapentin
-
SOME STEPS NEEDED TO REDUCE BENZODIAZEPINE PRESCRIBING (1)New
PatientsShort-term prescriptions (2-4 weeks only) in minimal
dosageAvoid potent benzodiazepines (alprazolam, lorazepam,
clonazepam)Consider rescheduling benzodiazepinesDevelop non-drug
treatments for anxiety and insomnia with suitable training and
provision of staffEducate doctors and health care workers about
potential dangers of new drugs (e.g. Z drugs and others)
-
SOME STEPS NEEDED TO REDUCE BENZODIAZEPINE PRESCRIBING
(2)Long-term patients (already dependent)Educate doctors and health
care workers in withdrawal methodsFinancial aid for patient support
groups and dedicated withdrawal clinicsGeneral measuresResearch
into long-term effects of benzodiazepinesGreater openness about
results of drug-company sponsored clinical trialsKeep up pressure
on government health authorities and the public