Embed Size (px)
DESCRIPTION
OBGYN history taking
Citation preview

HISTORY-TAKING & PHYSICAL EXAMINATION BY DR SAMER ABU EIDEH

HISTORY TAKING

HISTORY TAKING
IDENTIFICATION DATA
AGEPATIENTS
NAME
EXPECTED DATE OF DELIVERY
RACE
GRAVIDITY
PARITYLAST NL
MENSTRUAL PERIOD
PERIOD OF GESTATION

HISTORY TAKING
If she is pregnant we have also to mention :#gravidity : the No of pregnancies irrespective of the outcome.# parity the No of pregnancies reaching the viable stage.

HISTORY TAKING
# abortion : the No of pregnanciec terminated by any means before the viable stage.# MULTIPLE PREGNANCY IS ADDED AS A SINGLE OCCURRENCE.
##Note :Definition of other terms may used in history taken # ENND = death in 1st week of life.#NND= death within 28 days after delivery.# INFANTILE DEATH : during 1st year.# CHILD DEATH =from one year to 14 year.
n

HISTORY TAKING
# calculation of EDD and gestational age :#mentrual cycle have 2 phases :a - follicular phase (variable in length) b– luteal phase (constant in length= 14 days).# in a 28 day – cycle ovulation occurs 14 days before expected next menstruation

HISTORY TAKING
1- embryonic age( ovulation date) ( fertilization date ) which is calculated from the time of conception and equals ~266 days in a full term pregnancy.# gestational age (or menstrual age)which is calculated from the 1st day of the LMP ~ 280days or 40wks# to calculate EDD we use the NAEGELES rule
Duration of pregnancy(gest
ational age) calculated using
either

HISTORY TAKING
NAEGELES rule can only be applied when:# the cycle is regular of 28 days# the lady is not lactating or on OCPs = If the cycle is irregular then we use the revised EDD (with short cycle the EDD will be moved earlier, & with longer cycles the EDD will be moved forward)
We add 7 days to the days of the LNMP & we substract
3 mths or add 9mths.

HISTORY TAKING
# to calculate the G.A at the time or clercking, i we add 1wk for every 3mths
A lady is currently in her seventh pregnancy. She delivered 3 children prior, with 1 of
them was twin. She had history of 1 miscarriage, 1 molar and 1 ectopic
pregnancy. she will be described as: Gravida 7 Para
3(1 set of twins) + 1 abortion + 1 ectopic + 1 molar
e.g

HISTORY TAKING
Calculation of revised EDD (REDD)
In a woman whose LNMP on 15/3/2008, with menstruation occurs
every 21 days, her EDD will be on 15/12/2008 instead of 22/12/2008.
e.g

HISTORY TAKING
Calculation of period of gestation You see a lady whose LNMP was on 1/2/2008 on 1/9/2008. Therefore, she is at 30 weeks of gestation. LNMP: 1/2/2008 Date of clerking:
1/9/2008 There are 7 months (28 weeks) difference between her LNMP and the date you see her. Adding another 2 weeks to the difference (add 1 week for every 3 months),
the lady is now at 30 weeks of gestation.
e.g

HISTORY TAKING
#describes the symptom or problem that brings the patient to see the doctor #if there is more than one chief complaint, they should be arranged in a chronological order according to time of occurrence.
Chief complaint

HISTORY TAKING
Hx of presenting
illness
#the chief complaint is elaborated under this heading (describes the onset, nature, aggravating and relieving factors of the complaint and the progression of the complaints until you see the patient ).

HISTORY TAKING
Hx OF PRESENT
PREGNANCY
#The details of present pregnancy since diagnoses of pregnancy till now ,also the results of routine antenatal investigations should also be elicited.

HISTORY TAKING
PAST OBSTETRIC Hx
#The details of each previous pregnancy must be described in chronological order. # The following information is therefore important: 1. Year of delivery 2. Gestational age at delivery 3. Antenatal problems 4. Onset of labour (spontaneous or induced) 5. Mode of delivery 6. Complications occurred at delivery 7. Complications during postpartum period 8. Details about the baby: Baby’s gender Weight at delivery Viability of baby (live birth or stillbirth) Baby abnormality Breastfeeding

HISTORY TAKING
GYNAECOLOGY Hx
Menstrual cycle of the patient is recorded as follows: Age at menarche Duration of bleeding Length of menstrual cycle #Ask about menstrual problem such as intermenstrual bleeding, menorrhagia or dysmenorrhoea #ask about the past history of sepsis or sexually transmitted diseases (STD) #Cervical smear result should be asked and noted #Any gynaecology operation such as D&C and myomectomy should also been enquired#A review on contraceptive history and when and why it was stopped These information will help the doctor to decide and plan for
mode of delivery for current pregnancy.

HISTORY TAKING
PAST MEDICAL AND SURGICAL Hx
#Major medical problems such as diabetes, HTN, heart disease, renal disease & any psychiatric problems should be asked #Any surgical Hx should be detailed separately

HISTORY TAKING
DRUG AND ALLERGY Hx
# Details of the drugs (prescribed drugs, OTC drugs, modern as well as traditional medications) taken by the patient should be elicited # Some of the medications are contraindicated to pregnancy and need to be stopped, whilst some should be continued but of different form or at different dose #History of allergy to any medication as well as food ,so that these allergens can be avoided during pregnancy.

HISTORY TAKING
FAMILY Hx
#Ask whether there has been any congenital abnormality in the family #Ask about family hx of diabetes mellitus, hypertension, tuberculosis, multiple pregnancy etc #Some of the problems in the family can be passed to the patient, thus putting them at high risk to develop the same problem during pregnancy# Some of the diseases need the patient to be screened during the current pregnancy (e.g. diabetes mellitus)

HISTORY TAKING
SOCIAL Hx
…Employment#home condition #the length of relationship, are all of great importance when assessing the prospects for recovery from the illness or the support of the child.

HISTORY TAKING
Systemic review
…Description about other symptoms experienced by the patient that may be a sequel of patient’s problem should be recorded.
At the end of the history, a summary should be prepared to state briefly the details of the case#Age, gravidity, parity, period of gestation and chief complain are the most important information to be stated#Important positives and negatives points in history should be briefly stated#list of possible differential diagnosis for the patient
summary


PHYSICAL EXAMINATION
# you should never examine any patient alone.#You should introduce yourself to the Pt and explain the purpose of the examination. # you should stand on the right side of the patient

PHYSICAL EXAMINATION
GENERAL EXAMINATION
….look for # pallor, #palmar erythema (may be normal during pregnancy), # koilonychias(sign for iron deficiency anemia), #clubbing, # peripheral cyanosis #count the pulse rate of the patient(note rate, rhythm & volume).
hands

PHYSICAL EXAMINATION
GENERAL EXAMINATION
…. Take blood pressure #the cuff should be wide enough to cover about 2/3rd of the arm or upper thigh#Patient should be seated with the examination arm on the table or she should rest comfortably on her right side with 15 to 30˚ tilt and the right upper arm is at the level of the heart.
arms
PHYSICAL EXAMINATION
GENERAL EXAMINATION
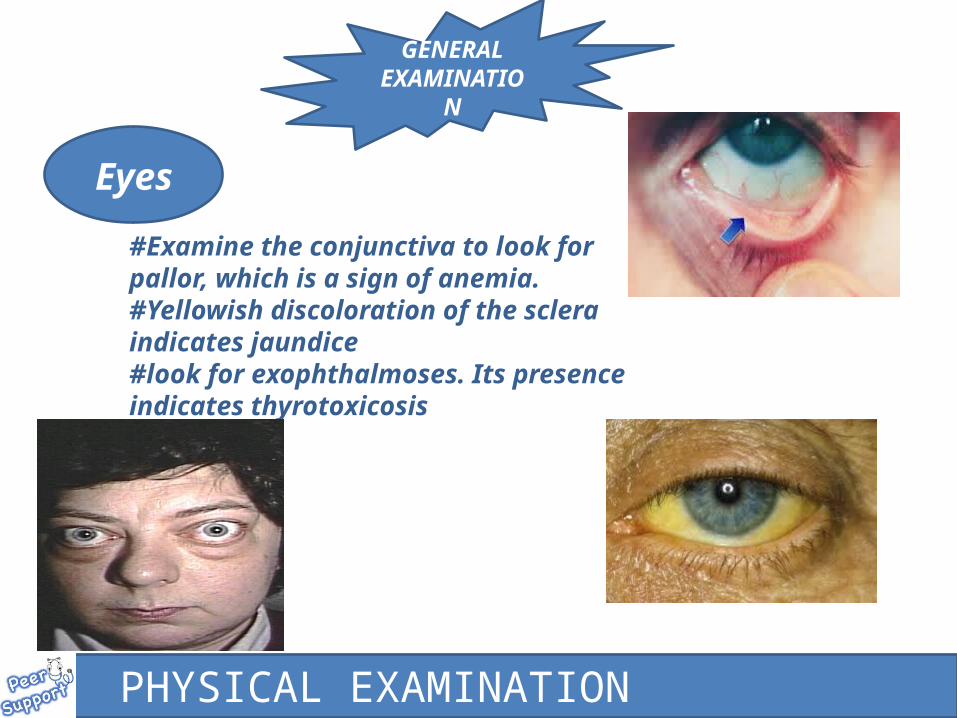
#Examine the conjunctiva to look for pallor, which is a sign of anemia.#Yellowish discoloration of the sclera indicates jaundice#look for exophthalmoses. Its presence indicates thyrotoxicosis
Eyes
PHYSICAL EXAMINATION
GENERAL EXAMINATION
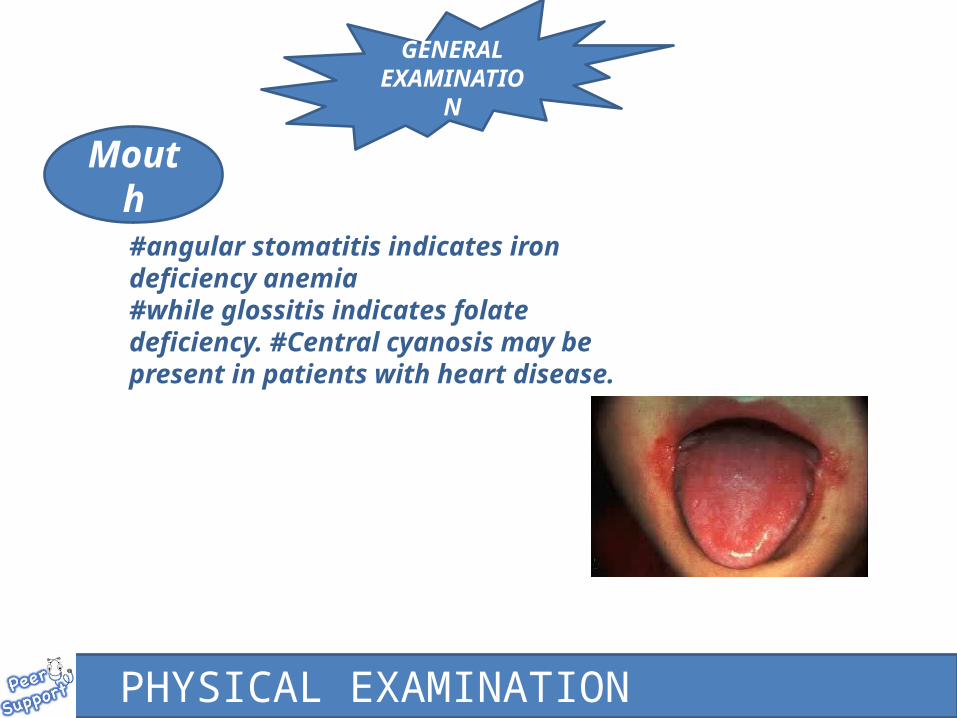
#angular stomatitis indicates iron deficiency anemia#while glossitis indicates folate deficiency. #Central cyanosis may be present in patients with heart disease.
Mouth

PHYSICAL EXAMINATION
GENERAL EXAMINATION
Thyroid
#The thyroid may sometimes be enlarged, reflecting increase metabolism in pregnancy

PHYSICAL EXAMINATION
GENERAL EXAMINATION
Legs
#Examine the legs for peripheral oedema. This sign is elicited by pressing the examining finger on the skin over tibia for 10 seconds#The presence of peripheral oedema may be physiological in pregnancy, where hands and feet are involved#It may be pathological in more severe degree where it involves the face and sacral area

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
#Patient should lie flat or in a semi– recumbent position, with the head rested on one pillow (Beware of supine hypotension)
#Patient abdomen should be exposed from the xiphisternum to just below the symphysis pubis, to display the suprapubic and inguinal regions with sheet covering the legs up to just below the symphysis pubis
A-inspection : we inspect for abdominal distension or enlargement (symmetrical or non symmetrical) , linea nigra , striae gravidarum( indicate current abdominal distension may be due to pregnancy), striae albicans (indicate previous abdominal distension either due to pregnancy or other cause),surgical scars which should be described in details ( site , shape , length signs of infectin if present) , dilated veins and hernias .

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
B- PALPATION : you should be gentle and keep looking on the patient face during palpation to be sure you are not causing pain.

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
1- superficial palpation…usually we start from the left lower quadrant using the flat of the hand and move gently around the abdomen looking for points of tenderness or rigidity or guarding.
#If there is rigidity, try to differentiate betwwen true regidity and voluntary one (due to nervous )rigidity by asking the patient to draw up her knees, this action will relax the abdominal muscle.
#If there is tenderness, try to induce rebound tenderness, by asking the patient to cough Or to push the abdominal wall against the examining hand. This will stretch the peritoneum out and cause discomfort in cases of peritoneal irritation or inflammation
Note : sudden withdrawal of the hand to induce rebound tenderness should be avoided coz it may coz significant distress to the patient .

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
2- deep palpation … we gently try to feel for organomegally and In case of pregnancy we feel the uterus and check either if it is soft and non tender or it is rigid and tender , also we check for uterine size , fetus and liquor.#we also feel for the liver, epigastric and loin tenderness . #if there is a pelvic or abdominal mass : site , size , shape , consistency , mobility and tenderness should be determined.# we check for the presence of ascites ,a- shifting dullness :percussion from midline to laterally untill thepercussion changes from resonance to dull , we keep the hand in this point and rool the patient 45 degrees , then we repeat percussion over this point which changes to reasonance in the presence of ascites .b- transmitted thrill.

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
Symphysio– fundal
height
#It is the distance between the fundus of uterus to top of symphysis pubis.#It can be estimated clinically or measured in centimeters#Clinical estimation of uterine size is done as below: At 12 weeks of gestation, the fundus is just above the symphysis pubis At 16 weeks, the fundus is equidistance between the symphysis pubis and umbilicus At 22 weeks of gestation, the fundus is at umbilicus At 30 weeks, the fundus is equidistance between the xiphisternum and umbilicus At 36 weeks, the fundus is at xiphisternum, To measure (SFH) in centimeterfirst centralize the uterus if it is deviated then a tape is used to measure the distance between the Fundus of uterus and the uppermost part of symphysis pubis .After 20 weeks the SFH approximates to the number of weeksMeasurement of SFH cannot be done if pregnancy is less than 20 weeks.

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
Symphysio– fundal height

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
THE NUMBER OF FETUSES
#Face the patient head and palpate the fundus and letral walls of uterus using the flat of both hands to determine the No of fetal poles , then face the patient feet and papate the lateral walls toward symphysis pubis . Single fetus has 2 poles , presence of more than 2 poles indicate multiple pregnancy , also may indicate singleton pregnancy with uterine fibroid or ovarian mass.
PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
THE NUMBER OF FETUSES

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
Fetal lie
#The relationship between the long axes of the fetus to that of the mother#It can be longitudinal , transverse or oblique# fetal lie is determined after determination of fetal poles .

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
Fetal presentation
…the fetal part that is foremost in the birth canal ,,#By facing the patient’s feet, apply lateral palpation to the presenting part gently pressing fingers of each hands towards the pelvis to determine whether the presenting part is cephalic (fetal head is hard and round) or breech( fetal breech is soft and not so round) and whether it is fixed or mobile #With trans- verse or oblique lie, we may feel either shoulder or arm.

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
Fetal parts
#The fetal parts is assessed by performing lateral palpation to dtermine on which Side the back of the fetus(firm) located, and fetus belly (soft) and limbs are located

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION

PHYSICAL EXAMINATION
c- percussion.
ABDOMINAL EXAMINATION

PHYSICAL EXAMINATION
ABDOMINAL EXAMINATION
D- auscultation :auscultation of fetral heart using Pinard fetal stethoscope depends on fetal presentation and location of fetal backA- If the presenting part is cephalic, the fetal heart will be heard over the lower right or lower left of the maternal abdomenB-If the presenting part is breech, the fetal heart will be heard over the upper right or upper left of the maternal abdomen.# we auscult also for bowel sound , silent abdomen indicate intestinal paralysis .

#pelvic examination :
• Patient placed in dorsal position with both knees bend and apart.
• A- inspection : we inspect for , swelling , inflammation , masses , lesions , discharges , trauma, skin tags , hemorrhoids and fissures.
• B- speculum examination : done with the patient either in dorsal or lateral position. The cervix is inspected for the presence of masses , discharge and ulcerations.
• C- vaginal examination : its done with lubricated gloves , vaginal walls palpated for the presence of masses , uterine cervix is felt for it,s position , presence of masses , in cases of pregnancy whether its closed or dilated , consistency , degrees of dilatation , condition of fetal membranes , presenting part and station of presenting part.

D- bimanual examination : fingers of right hand placed in the vagina and the left hand is placed over
the abdomen above symphysis pubis and bellow the umblicus . # cervix is identified and moved gently to asses for excitation pain # palpation of uterus : fingers of right hand placed under the cervix and
gently push up on the cervix to tilt the uterus upward and be felt between the two hands , in pregnant women uterus is soft as lips , while in non-pregnant women the uterus is firm like the tip of the nose . # position of the uterus : in anteverted uterus the cervix is directed in posterior position and the anterior lip of the cervix is felt 1st , while in retroverted uterus , the cervix is directed in anterior position and the posterior lip of the cervix is felt 1st .

# the adenxae is palpated for tenderness or masses , if mass present , its size ,
consistency , mobility , shape and tenderness should determined. # finally , size , shape , consistency and mobility of ovaries should be determined .

Thank you





























