Embed Size (px)
Citation preview

HIV Antiretroviral (ART) Medications Class Generic Brand Preparations Combo Pill Dosing Side Effects
Drug Interactions
Comments
Nucleoside / N
ucleotide Re
verse Tran
scrip
tase Inhibitors -‐ N
RTI
Nucleoside / Nucleotide Reverse Transcriptase Inhibitors MOA: Analogues of nucleo(t)side which replace a base during reverse transcription of viral RNA to DNA à chain termination Resistance: -‐ Needs only one resistant base pare mutation to acquire resistance -‐ If using two analogues, and both were same analogue, resistant would waste drugs à use 2 NRTIs that are different analogues. Long half lives. Renal Dosing: Try to avoid NRTIs all together, it’d be best Class Interaction: Ribavirin (hepatotoxicity)
Abacavir Guanosine analogue ABC Ziagen
300 mg tab ViiV
Kivexa 1 QD Triumeq 1 QD
Trizivir 1 BID
300 mg po BID 600 mg po QD
can safely use in CKD
Common: • Headache • N/D • Malaise
Serious: • Hypersensitivity reaction (HR) in 8%
↓[Methadone]
ü Black Box: Only Rx for HLA-‐B*5701 negatives à Testing predicts HR in Caucasians. Rechallenge in HR patients C/I à life threatening
ü Sings of HR: fever, rash, tired, upset stomach, vomit, belly pain, flu-‐like sx, sore throat, cough. Occurs < 6 wks after start (mean 11 days). Stop drug right away & see MD.
ü Meta-‐analysis à no signal for increased MI à but if higher MI risk, ABC not best choice
ü Can cause hepatitis and lactic acidosis esp in women and obese
Lamivudine Cytidine analogue 3TC Heptovir
3TC
150, 300 mg tab GSK
Kivexa 1 QD Triumeq 1 QD
Trizivir 1 BID
Combivir 1 BID
150 mg po BID 300 mg po QD
Renal
Well Tolerated • Headache begging • N/D/Abd pain transient • Insomnia uncommon • Pancreatitis more peds
Emtricitabine [X] à both Cytosine analogues (no point in using both)
ü Some people have headache in first few days, stick with it and use Tylenol and Advil if needed
Tenofovir Adenosine analogue
Only Nucleotide Reverse Transcriptase
Inhibitor (NtRTI)
TDF TAF
Viread TDF
150, 200, 250, 300 mg tab
40 mg/g powder Gilead
Truvada TDF 1 QD Descovy TAF 1 QD Stribild TDF 1 QD Genvoya TAF 1 QD Complera TDF 1 QD Odefsey TAF 1 QD Atripla TDF 1 QD
300 mg po QD Renal
avoid TDF in CKD
Mostly Well Tolerated • N/V/D/Gas • Renal impairmentTDF • Reduced bone density TDF
↓[atazanavir] ↑[didanosine -‐ ddi] Clinically not used with TDF anyways any longer
ü TDF = tenofovir disoproxil fumarate (pro-‐drug), efficacy of TDF = TAF ü TAF = tenofovir alafenamide fumarate (targeted pro-‐drug), less bone &
renal issues (TAF safe till CrCl 30 mL/min, TDF safe till CrCl 70 mL/min) ü Preferred over ABC due to activity in cases Hep B virus co-‐infection and
not needing HLA testing ü Favorable lipid profile
Emtricitabine Cytidine analogue FTC Emtriva
200 mg cap Gilead
200 mg po QD cap 240 mg po QD sol’n
Renal
Well Tolerated • Headachecommon, dizziness • N/D • Rash, skin pig’n
Lamuvidine [X] à both Cytosine analogues (no point in using both)
ü Black Box: severe exacerbation of hep B on stopping drug in pts w Hep B ü Only part of combos w Tenofovir in Canada ü Rarely pts may experience bad diarrhea. Headache most common s/e.
Zidovudine Thymidine analogue
AZT Retrovir
100, 250 mg cap 10 mg/mL syrup 10 mg/mL inject
ViiV
Trizivir 1 BID
Combivir 1 BID 300 mg po BID
Also I.V. form
Not Well Tolerated • Headache 62% • N 50% / V 17% / Anorexia 20% • Insomnia • Nail pigmentation • Hematologic tox
stavudine [X] also a thymidine analogue
ü Black Box: hematologic toxicity, myopathy, anemia, granulocytopenia, thrombocytopenia
ü Used in 1980s as one of the earliest HIV drugs, when people were dying from AIDS.
ü Place for therapy: IV form and syrup still used in MTCT in pregnancy and delivery and infants with HIV
Didanosine Adenosine analogue ddi Videx
EC
125, 200, 250, 400 mg EC cap
2, 4 g oral sol’n bottles Bristol-Myers
None
400 mg po QD
> 60kg
take ½ hr before or 2 hr after meal
Not Well Tolerated • Lipoatrophy very common • D/N/Abd pain • Rash • Headache, Fever • Hyperuricemia • Peripheral neuropathy
↑[conc] of: • Allopurinol (avoid)
↓[conc/abs] of: • Methadone • Rifampin, FLQ • Itra/ketoconazole
Black Box: fatal pancreatitis esp w d4T +/-‐ hydroxyurea If 25-‐60 kg then 250 mg QD DDinx w Ethanol, lamivudine, pentamidine à ↑pancreatitis
ü Lipodistrophy: ↑ metabolic issues (TG, LDL, sugars) & fat wasting in cheeks, hips, arms, legs, but fat gain tissue in abdo area MOA: all the NRTIs look like nucleosides, can also target mitochondrial polymerase. DNA replicate in mitochondria à polymerase in mitochondria inhibited (more lactic acid, more cell apaptosis, if mitochondrial in nerve cell led to neuropathy, if in fat cell lipodistrophy)
Stavudine Thymidine analogue d4T Zerit
15,20,30,40 mg cap
1 mg/mL oral Bristol-Myers
None 40 mg po q12h > 60 kg
• Lipoatrophy very common • Headache • N/V/D • Peripheral neuropathy
Dapson, INH Ribavirin Zidovudine
Black Box: fatal pancreatitis esp w d4T, fatal lactic acidosis
Fusion Inhibitor Enfuvirtide ENF Fuzeon 90 mg vial Genentech
None 90 mg SC BID • Inj site reaction • Bacterial pneumonia • Hypersensitivity
ü Was historically used in era between 1st and 2nd generation PIs ü Unstable drug, dose needs to be prepared before administering each
dose

Class Generic Brand Preparations Combo Pill Dosing Side Effects Drug Interactions Comments Non
-‐nucleoside RT
Inhibitors -‐ NNRT
I NNRTI ___vir___ MOA: NNRTIs bind allosterically in a pocket located near the catalytic site in the palm domain of the p66 subunit site of the Reverse Transcriptase (RT) enzyme Resistance: Single point attachments, easy for mutant to make attachment not happen, easy resistance “low generic barrier to resistance” K103N Mutation
Rilpivirine RPV Edurant 25 mg tab
Janssen
Complera TDF 1 QD Odefsey TAF 1 QD
25 mg po QD w food ++
• Rash 3% • Headache 3% • Insomnia • Depression 8% • Hyperlipidemia • Hepatotoxicity
↓[Edurant] with: Inducers of 3A Drugs inc pH
ü Among smallest HIV tablets ü Best absorbed with a good meal (350 cal) ü PPI contraindicated, H-‐2 blockers need dose reduction. ü Favorable lipid profile ü Lower virologic efficacy, not suggested for VL < 100,000 & CD4 > 200 ü Being studies (Phase 3 with CAB) as long-‐acting injectable
Efavirenz EFV Sustiva 600 mg tab
50, 200 mg cap Bristol-Myers
Atripla TDF 1 QD
600 mg po QD
avoid fatty meals on empty stomach
(inc abs’n leading to s/e)
CNS S/E 52%
• Dizziness, vivid dreams • Insomnia, somnolence • Impaired concentration • Hyperlipidemia
• Rash 26% (can treat through it mostly)
↑[Cocain]
↓[conc] of: • Benzos (-‐olam are issues, -‐pams are ok)
• most opioids • methadone (monitor response, don’t dose adjust in beginning)
ü let MD know if history of psych illness à should avoid this med ü Vivid dreams bothersome to some, enjoyable to some other ü CNS s/e worst after 1st or 2nd dose, get better in 2-‐4 weeks ü if you’re on methadone, you may need higher doses of it ü May cause false +ve cannabinoid test ü Avoid if hx of HIV-‐associated dementia (HAD) ü Not favourable in pregnancy (neural tube defects in animal studies, not
as significant in humans)
Nevirapine NVP Viramune 200 mg IR tab 400 mg SR tab
Boehringer
None 200 mg QD X 14
days then 200 mg po BID
• Rash 37% • Hepatic failure • Fever • Nausea
CYP3A4 substrate inducers/inhibitors of 3A4 will interact
ü Black Box: severer rash & hepatotoxicity ü higher CD4 associated w hypersensitivity à can treat through rash, but if
w fever and inc LFTs sign of hyperactivity ü Lead-‐in phase to reduce rash, occurs in 1st 6 wks, more in women… also
drug is auto inducer (will reduce its own level) ü XR version (400 mg QD) more common
Etravirine ETR Intelence 100, 200 mg tab
Janssen
None 200 mg po BID or 400 mg po QD
• Rash 9% • Dyslipidemia • Nausea • Rhabdomyolysis uncommon
CYP3A4, 2C9, 2C19 substrate inducers/inhibitors
will interact
ü Tabs are large; dissolve very readily in water (can help with swallowing). Also chucky and swallowing not easy of whole tab.
ü Sever rash reported
Delavirdine DLV Rescriptor 300 mg tab
ViiV
None 400 mg po TID • Rash 18% • N/V/D • Headache
CYP3A4 substrate inducers/inhibitors of 3A4 will interact
ü Completely not used at, cumbersome dosing
INST
I
Integrase Inhibitors ___tegravir Resistance: Low genetic barrier to R Class Interaction: 2 hrs before 6 hrs after cations
Raltegravir RAL Isentress 400 mg tab
Merck
None
400 mg po BID 1200 mg po QD
new study QDMRK w or w/o food
Well Tolerated • Rash, hypersensitivity • N/D, Headache • Insomnia • ↑ LFTs, ↑ CK, rhabdo
No CYP3A4 inx -‐ Rifampin may
reduce [ralteg] à 800 mg BID of RAL -‐ Al & Mg antacids
ü 1st to market INSTI à Being studied: 1200 mg po QD (given as 2X 600mg) ü More favourable lipid profile ü Aluminum or Magnesium antacids reduce abs’n RAL (use Ca antacid) ü Lower genetic barrier to resistance than PIs or DTG à can spare DTG,
start with RAL first & if resistance happened, change to DTG
Dolutegravir DTG Tivicay 50 mg tab
ViiV
Triumeq 50 mg po QD 50 mg po BID*
Well Tolerated • Insomnia • Headache • ↑ SCr small
No CYP3A4 inx -‐ Metformin (inc 2 fold [metformin]) -‐ C/I Dolfodelide
ü No food requirements J ü Inhibits renal tubular secretion of creatinine, SCr “falsely” increases ü Higher barrier to resistance than EVG or RAL ü Diarrhea uncommon ü BID dosing for heavily tx experienced, INSTI resistant, or given w rifampin
Elvitegravir EVG Vitekta 85, 150 mg tab
Gilead
Stribild Genvoya
85-‐150 mg po QD boosted
w small food
Well Tolerated • Hyperlipidemia • D/N • Headache
CYP3A4 substrate inducers/inhibitors of 3A4 will interact
ü Better absorption w food/snack ü More favourable lipid profile ü Must be given with PI, RTV or another ARV
Cabotegravir CAB TBD
? 200 mg/mL inj
30 mg tab ViiV
TBD 400 mg CAB + 600 mg RPV IM q4w
(TBD) TBD TBD ü As of Sept 2016 in phase 3 trials à LATTE-‐2 & FLAIR Phase 3 studies
ü 1st long acting injectable ART, nuc sparing regimen under study with RPV

Class Generic Brand Preparations Combo Pill Dosing Side Effects Drug Interactions Comments Protease In
hibitors -‐ PI
Protease Inhibitor _____avir Class S/E: Hyperlipidemia MOA: PI bind to active site in center of molecular complex of protease, locks in at multiple points and won’t allow the protease to cleave à high genetic barrier to mutation
Ritonavir PK booster RTV Norvir
100 mg tab/cap 80 mg/mL oral
Abbott
Kaletra 100-‐400 po/day
• Bitter aftertaste • Numbness around mouth at HIV doses
• N/V/D • ↑ LFTs, ↑ TG
Inducer of: • 1A2, 2B6, 2C9
Inhibitor of: • 3A4 strong 2C8, 2C9
ü Black Box: many drug interactions: 3A4, 2D6 à life threatening ü Extremely strong inhibition 3A4 & PGP ü HIV active at higher doses but toxicity & inx (not used for HIV treatment) ü 100 mg per dose to boost (e.g. if using with BID drug, give 100 mg BID) ü Fluorinated steroids (even inhaled) can lead to cushing’s syndrome
Darunavir DRV Prezista
Prezista: 600, 800 mg tab
Prezcobix: 800 mg + 150 mg COB tab
Janssen
Prezcobix w cobicistat 1 QD
600 mg po BID or 800 mg po QD
w food
+ RTV 100 mg BID
• Rash 10% • Headache • N/D • ↑ amylase • Hepatotoxic • Kidney stones?
Failure of contraceptives
ü Currently highest prescribed PI: 2nd Gen PI ü Works in those who are R to other PIs ü Cobicistat will cause tubular creatinine reabsorption à SCr “pseudo” rise
of 10-‐30 mmol/L from pts normal baseline ü Needs RTV boosting ü 800 QD + 100 mg RTV for naïve, [600 mg + 100 RTV] BID for experienced ü Contains Sulfa moiety
Atazanavir ATV Reyataz
Reyataz: 150, 200,
300mg tab
Evotaz: 300 mg + 150 mg COB tab
Bristol-Myers
Evotaz w cobicistat
300 mg po QD boosted w RTV 100 mg 400 mg po QD
unboosted w food
• Kidney stone 10 fold inc • Increased billi 60% (cosmetic, not harmful)
• D/N/Abd pain • Headache 6% • Rash 20%
CYP3A4 substrate inducers/inhibitors of 3A4 will interact
ü 2X150 mg (300 mg) + RTV 100 mg daily (TDF increases excretion of ATZ) ü 2X200 mg (400 mg) unboosted with Kivexa (needs RTV boost w others) ü Nuc sparing: w Raltegravir (boost each other) à ATZ 300 mg + RAL 400
mg BID (each) ü Increased QTc, PR, more torsads ü Jaundice as result of increased direct bilirubin à not harmful, pt may
decide to switch for cosmetic reason
Lopinavir / RTV
LPV Kaletra 200 mg + 50 mg
RTV tab Abbott
Kaletra 4 QD 400 mg po BID 800 mg po QD
• Diarrhea 24% • N • ↑ LFTs, billi, Lipids, MI
Many ↑ [benzos] Fentanyl Phenytoin
ü Deathly interaction with fentanyl . ü Funky interaction with phenytoin à RTV inhibitor, LPV inducer of CYP.
Unpredictable pheny level (unpredictable) ü +++ diarrhea, worse with q24h ü May need higher doses if tx experienced
Tipranavir TPV Aptivus 250 mg cap
100 mg/mL oral Boehringer
None 500 mg po BID • D/N/Abd pain • Rash >10% esp women • ↑ Lipids
Many à Inducer AND
inhibitor of CYP
ü Black Box: hepatitis, fatal hepatic failure, intracranial hemorrhage ü Contains Sulfa moiety ü Not clinically used due to cerebral bleeds and many drug interactions
Indinavir IDV Crixivan 200,400 mg cap
Merck
800 mg po q12h w RTV 100 mg
• Kidney stone hydration • ↑MI, LFTs, billi 15% • N/V/D/Metallic taste • Ingrown nail, dry skin
ü Lots of resistance to it! ü Need > 2 glasses water per dose! Otherwise kidney disease. ü Had to be on empty stomach ü Historically unboosted as q8h w restrict adherence needed à but
boosting removed all this requirement
Nelfinavir NFV Viracept 250, 625 mg tab
Roche
1250 mg po BID w lots of food
• Diarrhea 24% • N • Rash
ü Takes 5 tablets to make a dose! Not used routinely anymore. ü Place in therapy: Paediatric population
CC
R-5
CCR-‐5 Co Receptor Antagonists
Maraviroc MVC Celsentri 150, 300 mg tab
ViiV
None
150-‐600 mg po BID
Dose depends on DDinx
• cough 13 • Rash 10% , Abdo pain • Dizziness, myalgia • Ortho hypo, syncope • Upper resp infection
CYP3A4 substrate inducers/inhibitors of 3A4 will interact
ü Black Box: hepatotoxicity, inc MI? ü Used later in tx only for CCR-‐5-‐tropic HIV virus, cannot use for CXCR-‐4-‐
tropic virus which is seen more and more in advance dx
Tool Created by: Afshin Azami, PharmD, RPh, ACPR(c) ~ Chief Editor: Linda Robinson, BSc.Phm, RPh, AAHIVP (HIV Pharmacotherapy Specialist) ~ Windsor Regional Hospitals (WRH) ~ Sept 2016 References: 1) AIDSinfo Guidelines 2016 2) Stanford Guide to HIV/AIDS Therapy 2015-‐16 3) Lexi-‐Comp Drug Monographs for each respective drug 4) “Antiretroviral Therapy for HIV Infection” Johnson et al. IAS-‐USA Vol. 23 Iss 5: 161-‐167 (Jan 2016)
Tool Created by: Afshin Azami, PharmD, RPh, ACPR(c) ~ Chief Editor: Linda Robinson, BSc.Phm, RPh, AAHIVP (HIV Pharmacotherapy Specialist) ~ Windsor Regional Hospitals (WRH) ~ Sept 2016 References: 1) AIDSinfo Guidelines 2016 2) Stanford Guide to HIV/AIDS Therapy 2015-‐16 3) Lexi-‐Comp Drug Monographs for each respective drug 4) “Antiretroviral Therapy for HIV Infection” Johnson et al. IAS-‐USA Vol. 23 Iss 5: 161-‐167 (Jan 2016)
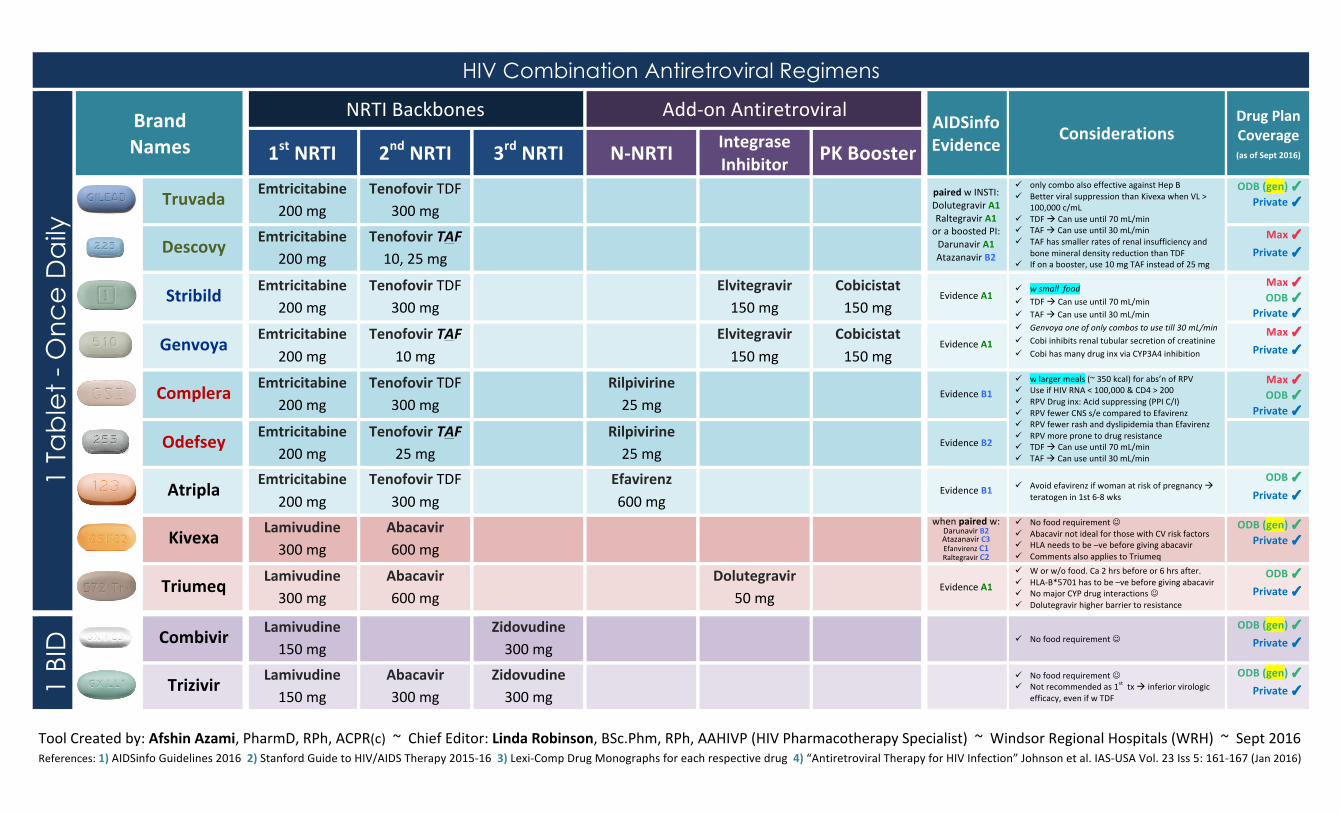
HIV Combination Antiretroviral Regimens 1
Tab
let
- O
nc
e D
aily
Brand Names
NRTI Backbones Add-‐on Antiretroviral AIDSinfo Evidence Considerations
Drug Plan Coverage
(as of Sept 2016) 1st NRTI 2nd NRTI 3rd NRTI N-‐NRTI Integrase Inhibitor PK Booster
Truvada Emtricitabine 200 mg
Tenofovir TDF 300 mg
paired w INSTI: Dolutegravir A1 Raltegravir A1 or a boosted PI: Darunavir A1 Atazanavir B2
ü only combo also effective against Hep B ü Better viral suppression than Kivexa when VL >
100,000 c/mL ü TDF à Can use until 70 mL/min ü TAF à Can use until 30 mL/min ü TAF has smaller rates of renal insufficiency and
bone mineral density reduction than TDF ü If on a booster, use 10 mg TAF instead of 25 mg
ODB (gen) ✓ Private ✓
Descovy Emtricitabine 200 mg
Tenofovir TAF 10, 25 mg
Max ✓
Private ✓
Stribild Emtricitabine 200 mg
Tenofovir TDF 300 mg
Elvitegravir 150 mg
Cobicistat 150 mg
Evidence A1
ü w small food ü TDF à Can use until 70 mL/min ü TAF à Can use until 30 mL/min ü Genvoya one of only combos to use till 30 mL/min ü Cobi inhibits renal tubular secretion of creatinine ü Cobi has many drug inx via CYP3A4 inhibition
Max ✓ ODB ✓
Private ✓
Genvoya Emtricitabine 200 mg
Tenofovir TAF 10 mg
Elvitegravir 150 mg
Cobicistat 150 mg
Evidence A1
Max ✓ Private ✓
Complera Emtricitabine 200 mg
Tenofovir TDF 300 mg
Rilpivirine 25 mg
Evidence B1 ü w larger meals (~ 350 kcal) for abs’n of RPV ü Use if HIV RNA < 100,000 & CD4 > 200 ü RPV Drug inx: Acid suppressing (PPI C/I) ü RPV fewer CNS s/e compared to Efavirenz ü RPV fewer rash and dyslipidemia than Efavirenz ü RPV more prone to drug resistance ü TDF à Can use until 70 mL/min ü TAF à Can use until 30 mL/min
Max ✓ ODB ✓
Private ✓
Odefsey Emtricitabine 200 mg
Tenofovir TAF 25 mg
Rilpivirine 25 mg
Evidence B2
Atripla Emtricitabine 200 mg
Tenofovir TDF 300 mg
Efavirenz 600 mg
Evidence B1 ü Avoid efavirenz if woman at risk of pregnancy à teratogen in 1st 6-‐8 wks
ODB ✓ Private ✓
Kivexa Lamivudine 300 mg
Abacavir 600 mg
when paired w:
Darunavir B2 Atazanavir C3 Efanvirenz C1 Raltegravir C2
ü No food requirement J ü Abacavir not ideal for those with CV risk factors ü HLA needs to be –ve before giving abacavir ü Comments also applies to Triumeq
ODB (gen) ✓ Private ✓
Triumeq Lamivudine 300 mg
Abacavir 600 mg
Dolutegravir
50 mg Evidence A1
ü W or w/o food. Ca 2 hrs before or 6 hrs after. ü HLA-‐B*5701 has to be –ve before giving abacavir ü No major CYP drug interactions J ü Dolutegravir higher barrier to resistance
ODB ✓ Private ✓
1 BI
D
Combivir Lamivudine 150 mg
Zidovudine 300 mg
ü No food requirement J ODB (gen) ✓
Private ✓
Trizivir Lamivudine 150 mg
Abacavir 300 mg
Zidovudine 300 mg
ü No food requirement J ü Not recommended as 1st tx à inferior virologic
efficacy, even if w TDF
ODB (gen) ✓ Private ✓