Embed Size (px)
Citation preview

HIV care engagement among people with a history of injection drug use
Ann N. Burchell, PhD Scientist, Dept of Family and Community Medicine and Li Ka Shing Knowledge Institute St. Michael’s Hospital
Ontario Harm Reduction Conference October 26, 2015
Collaborators
Ann N. Burchell2,3, Sandra Gardner1,2, Beth Rachlis1, Lucia Light1, Tony Antoniou3, Jean Bacon1, Anita Benoit2, Jeff Cohen7, Tracy Conway1, Curtis Cooper5, Patrick Cupido1, Tony DiPede1, Claire Kendall4, Mona Loutfy2, Frank McGee4, James Murray4, Janet Raboud2, Anita Rachlis2, Wendy Wobeser6, Sean B. Rourke1 for the OHTN Cohort Study Team
1) Ontario HIV Treatment Network 2) University of Toronto 3) St. Michael's Hospital 4) AIDS Bureau, Ontario Ministry of Health and Long Term Care 5) University of Ottawa 6) Kingston Hotel Dieu Hospital 7) Windsor Regional Hospital
HIV Care Continuum Project Team

Continuum of HIV care (“Cascade”)
HIV-Infected HIV-Diagnosed
Linked to HIV care
Engaged or Retained in
HIV care
On Antiretroviral
Therapy
Achieved Viral
Suppression
In HIV Care

What are the benefits of optimal HIV care engagement?
• Regular contact with HIV care promotes – Starting antiretroviral treatment (ART) – Better ART adherence – Better primary care including early detection and management of co-
infections and other co-morbidities
• Being on ART prevents HIV progression
• Positive prevention suppressed viral load prevents transmission to partner
• All of the above predicts better survival

Aims
• What are the patterns of HIV care engagement
– Among people attending specialty HIV clinics?
– Among people with HIV who have a history of IDU?
– Among people with HIV who continue to use substances?

OHTN Cohort Study (OCS)
Ongoing follow-up study of persons in HIV care in Ontario
Eligibility Criteria • Positive HIV-antibody test or other laboratory evidence of HIV
infection • Patients at participating specialty HIV clinic • Aged 16 years or older • Capable of providing informed consent
Data • Medical charts, electronic medical records, face-to face interviews • Data linkage with Public Health Ontario Laboratories
6,408 participants ever enrolled as of December 2013
Rourke et al. Cohort profile. Int J Epidemiol, 2013

Recruitment & follow-up at hospital-based specialty HIV clinics and primary care practices across Ontario

Characteristics of participants at their first interview (N=3,571)
Mean age (SD)
45.9 (10.1)
Born in Canada 68.5%
Sex/Orientation MSM Heterosexual male Female
69.0% 13.6% 17.5%
Ethnicity White Aboriginal African/Black/Caribbean Other
62.9%
9.2% 16.4% 11.5%
Median year of HIV diagnosis (IQR)
1998 (1992-2004)
Income <$20,000 $20,000 to < $40,000 $40,000 to< $60,000
$60,000+
44.0% 21.2% 16.5% 18.3%
Employment status Employed Unemployed-seeking Not in the labour force Disability
47.1%
6.2% 17.1% 29.7%
Education Some high school or less Completed high school Trade/Some college
College/Some university University degrees
14.2% 17.5% 13.5% 27.4% 27.5%

History of drug use among participants
12 14 3
0
20
40
60
80
100
Ever injected drugs Used substances in past 6months (but did not inject)
Injected drugs in past 6months
Compare to all diagnosed with HIV in Ontario, of whom 11% report injection drug use as a risk factor 1
1. Remis 2011. http://www.ohemu.utoronto.ca/doc/PHERO2011_report_preliminary.pdf 2. As reported at interviews in 2007/08 onwards
2 2

Recent drug use (past 6 months) among people with a history of IDU, by year of interview
53% 45%
50%
41% 41% 38%
23% 18%
24% 18%
24% 22%
0%
20%
40%
60%
80%
100%
2008 2009 2010 2011 2012 2013Year of interview
Any substance use Injection drug use

Specific Drugs Reported by Drug Users Pe
rcen
t
1 6
35
47
20
35
16 7 8
0
10
20
30
40
50
60
70

Continuum of HIV care (“Cascade”)
HIV-Infected HIV-Diagnosed
Linked to HIV care
Engaged or Retained in
HIV care
On Antiretroviral
Therapy
In HIV Care
Achieved Viral Suppression

Percent in continuous care among participants in annual HIV care, by IDU status
83.7 83.5 90.1 87.3
0
20
40
60
80
100
2002 2012
IDUNon-IDU
-7.4% -3.8%
Continuous care defined as ≥2 HIV laboratory tests (viral load or CD4 cell count) at least 3 months apart
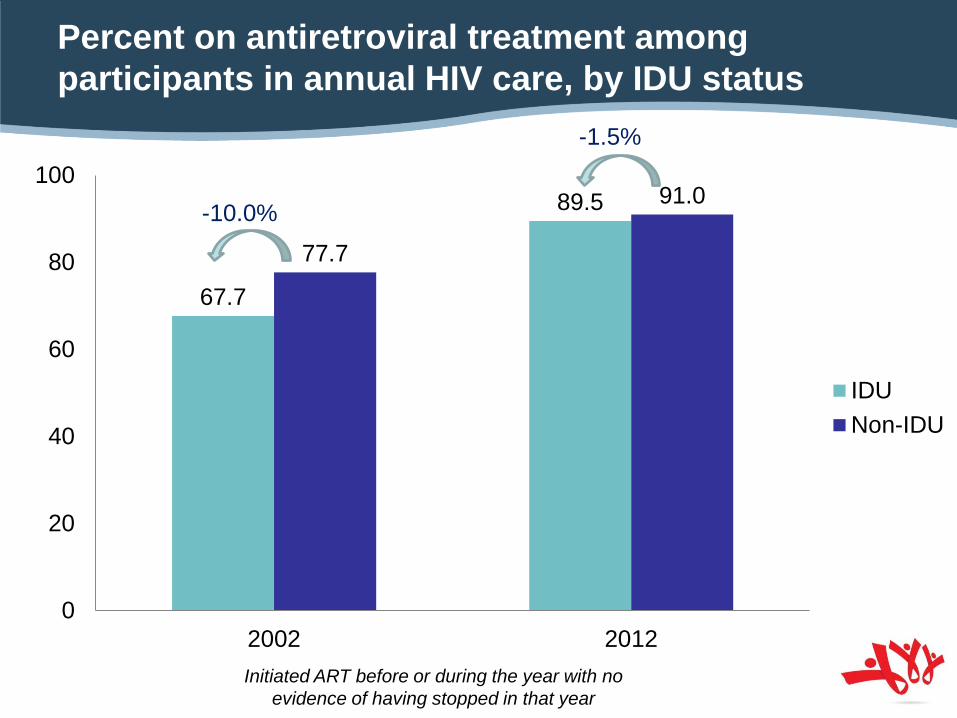
Percent on antiretroviral treatment among participants in annual HIV care, by IDU status
67.7
89.5
77.7
91.0
0
20
40
60
80
100
2002 2012
IDUNon-IDU
-10.0%
-1.5%
Initiated ART before or during the year with no evidence of having stopped in that year

Continuum of HIV care (“Cascade”)
HIV-Infected HIV-Diagnosed
Linked to HIV care
Engaged or Retained in
HIV care
On Antiretroviral
Therapy
Achieved Viral
Suppression
In HIV Care

Percent with suppressed viral load (<200 copies/mL) among participants on antiretroviral treatment, by IDU status
48.2
84.6
59.9
90.7
0
20
40
60
80
100
2002 2012
IDUNon-IDU
-11.7%
-6.1%

Adherence among participants on ART, by IDU status
25%
75%
11%
89%
14%
86%
0%
20%
40%
60%
80%
100%
Yes No
Have you missed any of your doses of ART medications over the past 4 days?
Current IDU (n=12) Past IDU (n=54) Non-IDU (n=904)

Ongoing substance use & suppressed viral load
Tobacco p<0.0001
Substance use p<0.0001
Binge drinking p=0.06
90.2 92.2
96.3 95.0 94.1 94.0 92.5 89.4 94.5
91.1
82.2
50
60
70
80
90
100
Source: Sandra Gardner
Pattern held even after accounting for smoking, drinking, income, housing & mental health concerns

Engagement in care among people with a history of IDU ever enrolled in OCS, 2001-2012
0
20
40
60
80
100
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012In care Continuous care On ART Undetectable VL
• “On ART” increased from 56% to 73% • Undetectable VL increased from 34% to 65%

Engagement in care among all people ever enrolled in OCS, 2001-2012
0
20
40
60
80
100
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012In care Continuous care On ART Undetectable VL
• “On ART” increased from 67% to 77% • Undetectable VL increased from 42% to 73%

Interpretation
• Since early 2000s, dramatic gains in viral suppression Why?
• ART regimen improvements (tolerability, dosing) • Guidelines (earlier initiation, no treatment interruption)
• Patients with history of IDU generally had lower HIV care engagement • Driven by ongoing substance use
• Not explained by differences in income, housing, employment, ethnicity, nor a host of other factors

Interpretation
• Better access to high quality harm reduction, addictions treatment, mental health care may have far reaching benefits • Better HIV care engagement, adherence
• Lower viral load, less disease progression, less transmission
• Longer lives

OCS Acknowledgments
We thank all participants and the interviewers, data collectors, research associates and coordinators, nurses and physicians who provide support for data collection and extraction
OCS Study Team Sean B Rourke (PI), Ann N Burchell, Ahmed M Bayoumi, John Cairney, Jeffrey Cohen, Curtis Cooper, Fred Crouzat, Sandra Gardner, Kevin Gough, Don Kilby, Mona Loutfy, Nicole Mittmann, Janet Raboud, Anita Rachlis, Edward Ralph, Sergio Rueda, Irving E Salit, Roger Sandre, Marek Smieja, Wendy Wobeser
OHTN Staff Jason Globerman, Madison Giles, Robert Hudder, Lucia Light, Veronika Moravan, Nahid Qureshi
OCS Scientific Steering Committee Leighton McDonald, Ann N Burchell, Curtis Cooper, Sergio Rueda, Barry Adam, Tony Antoniou, Adrian Betts, John Cairney, Tracey Conway, Sandra Gardner, Trevor Hart, Mona Loutfy, Peggy Millson, Kelly O’Brien, Janet Raboud, Anita Rachlis, Sean Rourke, Sergio Rueda, Wendy Wobeser
OCS Governance Committee Patrick Cupido (Chair), Adrian Betts, Anita Benoit, Les Bowman, Tracey Conway, Tony Di Pede, Michael Hamilton, Brian Huskins, Clemon George, Troy Grennan, Claire Kendall, Nathan Lachowsky, Joanne Lindsay, John MacTavish, Shari Margolese, Colleen Price, Rosie Thein
Funding AIDS Bureau, Ontario Ministry of Health and Long Term Care CIHR New Investigator Salary Award to ANB
Data Linkage Public Health Ontario Laboratories
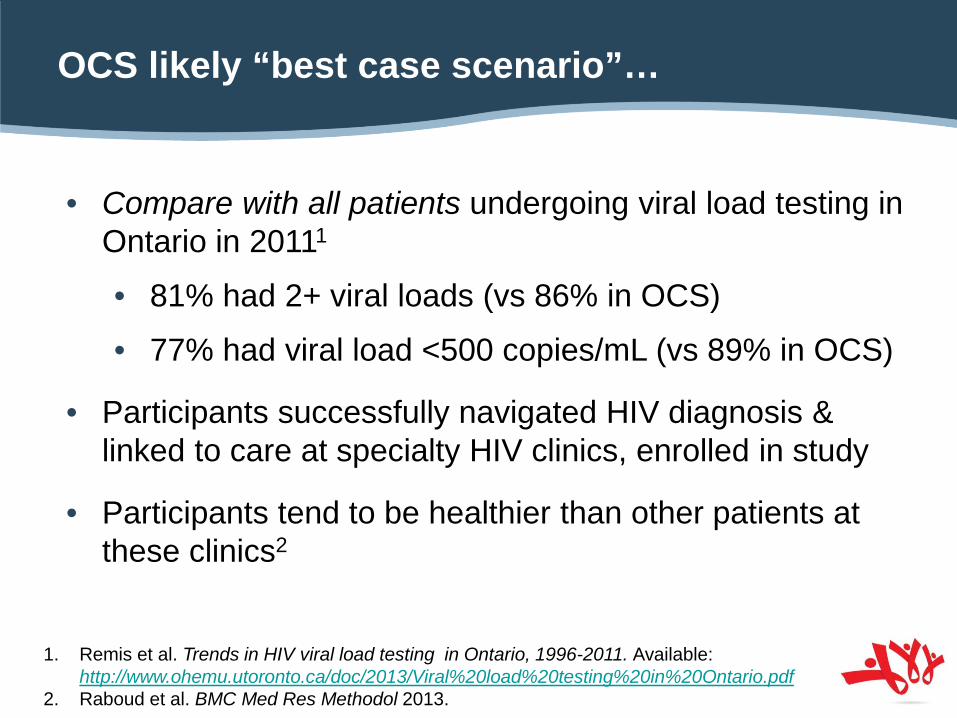
OCS likely “best case scenario”…
• Compare with all patients undergoing viral load testing in Ontario in 20111
• 81% had 2+ viral loads (vs 86% in OCS)
• 77% had viral load <500 copies/mL (vs 89% in OCS)
• Participants successfully navigated HIV diagnosis & linked to care at specialty HIV clinics, enrolled in study
• Participants tend to be healthier than other patients at these clinics2
1. Remis et al. Trends in HIV viral load testing in Ontario, 1996-2011. Available: http://www.ohemu.utoronto.ca/doc/2013/Viral%20load%20testing%20in%20Ontario.pdf
2. Raboud et al. BMC Med Res Methodol 2013.


























![Knowledge about hiv aids among nurses [compatibility mode]](https://img.pdfslide.net/doc/110x75/55783fcfd8b42a1f5b8b4e9a/knowledge-about-hiv-aids-among-nurses-compatibility-mode.jpg)
